Embed Size (px)
Citation preview

Risk assessment of selected opportunisticpathogens in drinking water.
Item Type Dissertation-Reproduction (electronic); text
Authors Chaidez Quiroz, Cristobal,1969-
Publisher The University of Arizona.
Rights Copyright © is held by the author. Digital access to this materialis made possible by the University Libraries, University of Arizona.Further transmission, reproduction or presentation (such aspublic display or performance) of protected items is prohibitedexcept with permission of the author.
Download date 05/05/2018 07:04:31
Link to Item http://hdl.handle.net/10150/191233

RISK ASSESSMENT OF SELECTED OPPORTUNISTIC PATHOGENS IN
DRINKING WATER
by
Cristobal Chaidez Quiroz
A Dissertation Submitted to the Faculty of the
GRADUATE INTERDISCIPLINARY PROGRAM IN NUTRITIONAL SCIENCES
In Partial Fulfillment of the Requirements For the Degree of
DOCTOR OF PHILOSOPHY
In the Graduate College
THE UNIVERSITY OF ARIZONA
1999
1 h L. Price
(0 ,tA-0-n) V.Lightner
2
THE UNIVERSITY OF ARIZONAGRADUATE COLLEGE
As members of the Final Examination Committee, we certify that we have
read the dissertation prepared by Cristobal Chaidez Quiroz
entitled Risk Assessment of Selected Opportunistic Pathogens
in Drinking Water
and recommend that it be accepted as fulfilling the dissertation
requirement for the Degree of Doctor in Philosophy
rCha P. Ger ap
/.
142 49Date
I / ze Mc",Date
V 31-/c0 Date
Ag-/q9 Date
( 2 99DaLe
Final approval and acceptance of this dissertation is contingent uponthe candidate's submission of the final copy of the dissertation to theGraduate College.
I hereby certify that I have read this dissertation prepared under mydirection and recommend that it be accepted as fulfilling the dissertationrequirement.
,L$ 1,7Dissertation Director
Charles P. Gerba
1 /2-9Date

STATEMENT BY THE AUTHOR
This dissertation has been submitted in partial fulfillment of requirements for anadvance degree at The University of Arizona and is deposited in the University Library tobe made available to borrowers under rules of the Library.
Brief quotation from this dissertation are allowable without special permission,provided that accurate acknowledgment of source is made. Request for permission forextended quotation from or reproduction of this manuscript in hole or in part may begranted by the head of the major department or the Dean of the Graduate College when,in his or her judgment, the proposed use of the material is in the interests of scholarship.In all other instances, however, permission must be obtained by the author.
3
Signed:

ACKNOWLEDGMENTS
I would like to express my sincere acknowledge to Dr. Charles P. Gerba, mymajor advisor, for the guidance and encouragement he provided throughout the course ofthis research.
I would also extend my thanks to Dr. Pat A. Rusin, Dr. Donald V. Lightner, Dr.Glenn J. Songer and Dr. Ralph Price for their service as the advisory committee as well astheir suggestions and insights toward the completion of this work.
Special thanks are for Mr. Jaime Naranjo. I would not be able to finish my work,without your help. Thanks for everything Jaime (my friend).Also my appreciation is for Dr. (Don) Carlos Enriquez. Your suggestion and friendshipmeant a lot to me.
My sincere thanks to my buddy Jorge Sandoval. I will never forget those days wespent talking about "the wonder years".
I would like to thank Dr. Adela Allen and Geraldine Olds (from the Graduatecollege) for being so helpful.
And finally, the Gerbais (Dr. Gerba's students): Thanks a lot to the Mexican crew:Dr. Maria Quifionez, Juan Antonio Vidales, Pablo Gortarez, Tomas Sepulveda y RicardoEnriquez. And also thanks to Pam, Patricia, Faezeh, Amy, Cherry, Jeanette, Denise , Luis.Mohammad, Absar, Frank and Hiroshi. And also for the old gang: Edlin, Manuella, Danaand Seema.
Thanks to all of you for being my friends all this time and making this task much easier.I will never forget those days at Gerba's lab.
4

DEDICATION
This work is dedicated to my parents, Cristobal Chaidez Medina and Leonor
Quiroz de Chaidez, to my sisters, Rosa Delia and Silvia Patricia, and for their kids
(Genessys, Daniel and Hansel), who were my constant inspiration during all those years.
I would also extend this dedication to my friend and lovely wife, Dr. Marcela
Vergara for your patience and support during the preparation of this work. I will love
you forever.
5
6
TABLE OF CONTENTSI. LIST OF FIGURES 8
II. LIST OF TABLES 9
ABSTRACT 11
III. INTRODUCTION 13
Problem Definition 13
Literature Review 14
The Risk Assessment 14
Microbial Risk Assessment 15
Opportunistic Pathogens in Water 19
Dissertation Format 45
IV. PRESENT STUDY 46
APPENDIX 1: MICROBIOLOGICAL QUALITYOF WATER VENDING MACHINES 48
APPENDIX 2: MICROBIOLOGICAL SURVEYOF PRIVATE ROOF WATER TANKS INCULIACAN, MEXICO 68
APPENDIX 3: MICROBIOLOGICALCOMPARISON OF THE QUALITY OFPOU-TREATED WATER, TAP WATER,AND BOTTLED WATER 85

TABLE OF CONTENTS-Continued
APPENDIX 4: AEROMONAS HYDROPHILAAND PSELTDOMONAS AERUGINOSA INDRINKING WATER FROM VARIOUSSOURCES: A RISK ASSESSMENT 113
APPENDIX 5: CONCLUSION 139
APPENDIX 6: BACTERIAL DATA 142
REFERENCES 154
7
LIST OF FIGURES
FIGURE 1.1, Percentage of positive samplesfor Pseudomonas aeruginosa (CFU/500 mL),total coliforms (CFU/100 mL) and heterotrophicplate count (HPC) bacteria greater than 500 CFU/mL 57
FIGURE 2.1, Percentage of samples positivefor Pseudomonas aeruginosa (CFU/500 mL),total and fecal coliforms (CFU/100 mL) andheterotrophic plate count (HPC) bacteria greaterthan 500 CFU/mL 77
FIGURE 3.1, Mean HPC bacteria densities (CFU/mL) 109
FIGURE 3.2, Mean Pseudomonas aeruginosadensities (CFU/500 mL) 110
FIGURE 3.3, Mean Aeromonas hydrophiladensities (CFU/500 mL) 111
FIGURE 3.4, Mean total coliforms densities (CFU/100 mL) 112
8

LIST OF TABLES
TABLE 1.1, Bacteriological quality of waterfrom vending machines 58
TABLE 1.2, Weekly sampling of three watervending machines 59
TABLE 1.3, Nozzle swab test results of fifteenwater vending machines 59
TABLE 1.4, Drain swab test results of fifteenwater vending machines 60
TABLE 1.5, Maximum and minimum valuesfor the physico-chemical parameters in analyzedwater from vending machines 61
TABLE 2.1, Bacteriological quality of waterfrom household roof tanks 78
TABLE 2.2, Average, maximum andminimum values for the physico-chemicalparameters in analyzed water from householdroof tanks 79
TABLE 3.1, General characteristics ofpoint-of-use (POU)-devices (faucet-mounted units) 91
TABLE 3.2, Percentage bacterial occurrencein POU-treated water, tap water (with POU),tap water (without POU), and bottled water 104
TABLE 3.3, Average, maximum, minimumvalues of bacteria in drinking water sources 105
9
TABLE 3.4, Occurrence of the HPC in drinkingwater sources 106
LIST OF TABLES-Continued
TABLE 3.5, Bacteria isolated and identified indrinking water samples 107
TABLE 3.6, Average (ave), maximum (max),and minimum (min) values for the physico-chemicalparameters in analyzed water (POU-treated water,tap water with POU, tap water without POU,and bottled water) 108
TABLE 4.1, Isolation of A. hydrophila fromdrinking water sources (CFU or %) 124
TABLE 4.2, Isolation of P. aeruginosa fromdrinking water sources (CFU or %) 125
TABLE 4.3, Risk of infection of Aeromonashydrophila and Pseudomonas aerugin osa inselected drinking water sources (2L/day/person) 127
TABLE 4.4, Risk of infection of Aeromonashydrophila and Pseudomonas aeruginosa inselected drinking water sources (4L/day/person) 128
TABLE 4.5, Risk of infection of A. hydrophilain bottled water excluding one high value 128
TABLE 4.6, Daily bacterial concentrations usedfor the risk of infection based on two and fourliter consumption 129
10

11
ABSTRACT
Water as a route of opportunistic bacterial disease transmission has not been well
established. The use of epidemiological evidence linking drinking water bacterial
contamination to health effects in a population is lacking and very costly to obtain. Also,
the significance of exposure to low-level contamination is difficult to determine
epidemiologically. This makes it difficult to estimate the impact on a community. The
use of risk assessment approach allows an understanding of low-level exposure; and to
define it in a more quantitative fashion. Microbial risk assessment was employed to
determine the risks associated with exposure to selected opportunistic bacterial pathogens
(Aeromonas hydrophila and Pseudomonas aeruginosa) present in drinking water from
various sources. An extensive analysis was conducted on drinking water obtained from
various sources including point-of-use (POU)-treated water, tap water with POU-
connection, tap water, bottled water, and water from vending machines and storage tanks.
Enumerated bacteria included: A. hydrophila, heterotrophic plate count (HPC) bacteria,
Mycobacteriuni spp., Plesiomonas shigelloides, P. aeruginosa, and total and fecal
coliforms. It was found that opportunistic pathogens were present in small numbers in
drinking water. Neither fecal coliforms nor P. shigelloides were found in the drinking
water samples. The annual risks of colonization based on the consumption of
2L/day/person for drinking water were determined to be as high as 7.9x10 - ' and 9.9x10 -4
for A. hydrophila and P. aeruginosa, respectively at exposure levels ranging from 90 to
12
10 CFliimL. respectively. The results obtained indicates that the risk of colonization is a
transient process, and the probability of infection may be very but could result in the most
vulnerable (very young, the elderly and immunocompromised).
More studies are needed on the occurrence of opportunistic pathogens in drinking
water from various sources and animal andjor human feeding studies to better define
dose-response in both healthy and immunocomprimised individuals. There is no doubt
that the greatest need for microbial risk assessment is the occurrence data. Therefore,
national surveys in drinking water from various sources will help in the developing of
microbial risk assessment for opportunistic bacterial pathogens. The use of conventional
methods as well as molecular approaches are recommended in order to obtain a more
accurate identification of waterborne bacterial pathogens.

CHAPTER 1
INTRODUCTION
The purpose of this dissertation was to assess the risks associated with the
exposure to selected opportunistic bacterial pathogens in drinking water from various
sources using a microbial risk assessment approach. This was accomplished by
determining the occurrence and concentration of selected opportunistic bacterial
pathogens in various drinking water sources.
Problem Definition
Opportunistic bacterial pathogens continues to occur in the United States despite
present technologies available for water treatment. This may be due to a breakdown in
treatment such as inability of the treatment process to remove all of the pathogenic
organisms present in the raw water, contamination after treatment, or bacterial re-growth
in the distribution system. Opportunistic bacterial pathogens are capable of surviving on
minimal nutrients, in pipes sediments, and becoming participants of biofilm formation.
Segments of the population particularly at risk of infection are newborn babies, the
elderly and immunocompromised individuals. However, their public health significance
13

14
with regard to the population at large is not well known. It is difficult. to determine the
human health significance of exposure to low-level contamination of water supplies.
Furthermore, data are limited on the occurrence of specific opportunistic pathogens in
drinking water. Better quantification of the occurrence of opportunistic bacteria is
necessary to understand the human health risk associated with exposure.
Literature Review
The Risk Assessment
Risk may be defined as the probability or likelihood of an adverse effect occurring
due to consequences set forth from a particular hazard (chemical, landfill, biologically-
contaminated food or water, or even a person's own behavior). The science of risk
assessment involves evaluating the risks posed to a society or to the environment in order
to better understand the scope of the problems that may result from the exposure to
particular hazards. Information learned through risk assessments can be used to help
policy-makers make informed decisions concerning the risks posed from a given hazard.
Risks analysis is the process of evaluating risks and risk issues. The process
involves risk assessment, risk management, and risk communication (NRC, 1994). The
risk assessment is the first step of the risk analyses process.
There are four fundamental steps in the risk assessment framework: 1) hazard
identification: 2) dose-response assessment; 3) exposure assessment; and, 4) risk
15
characterization (Rose et al.. 1991). The hazard identification step is the most easily
followed. Basically, a substance is determined as harmful or not based on laboratory and
field data as well as information obtained from epidemiological studies. The dose-
response assessment involves determining the relationship between the dose of the hazard
and the incidence of the adverse health effect. This step uses animal studies and requires
the extrapolation from high to low doses and from animals to humans (Macler and Regli,
1993).
The objective of the exposure assessment step is to measure the frequency and
intensity of the exposure, the route of exposure, and the population exposed. The
objective of the risk characterization step (which can be qualitative or quantitative) is to
estimate the risk of an adverse health effect occurring based on exposures determined in
the exposure assessment.
The use of risk assessment framework to estimate risks associated with
environmental exposure to microorganisms is of more recent development and is
discussed in the following section.
Microbial Risk Assessment
Risk assessment methodology has been developed to better understand the
significance of exposure to microorganisms in water. Epidemiological data obtained
from waterborne outbreaks provide information on the human health impacts of microbial
contaminated water. However, it is difficult to understand the impacts associated with
16
exposure to low levels of contamination (Rose et al., 1991). Risk assessment helps to
understand the significance of exposure to low-levels of microorganisms in water.
The four-tiered approach is used in the risk assessment framework. Hazard
identification, dose-response assessment, exposure assessment, and risk characterization
(NRC, 1983), can also be applied to assessing risks associated with exposure to
microorganisms. Hazard identification is the identification of the microbial agent as well
as the spectrum of the human illness and disease associated with the specific
microorganisms. Dose-response is the characterization of the relationship between the
dose administered and the probability of infection or disease on the exposed population.
Exposure assessment determines the size and the nature of the population exposed and
the route. Risk characterization is the integration of the three steps in order to estimate
the magnitude of the public health problem (NRC, 1983).
Two mathematical models have been shown to adequately describe the infection
process demonstrated in the dose-response studies of pathogenic microorganisms (Haas,
1983; Rusin et al., 1997). The exponential model:
Pi = 1 - e -(1/K) (N);
Where Pi = the probability of infection, 1/k= the fraction of ingested microorganisms
that survive to initiate infection, and N= number of microorganisms ingested or inhaled.

17
The beta-Poisson model.
Pi = 1 -(1 ± N/I3
Where Pi = the probability of infection, N= the number of microorganisms ingested, and
B represents the parameters of the host-virus interaction. Risk estimates illness and death
can also be computed from these models by incorporating morbidity and mortality ratios
of that particular microorganism (Haas et al., 1993).
Exposure assessment determines the amount of water consumed by an individual
as well as the concentration of microorganisms (e.g. bacteria). The USEPA uses two
liter/person/day for risk estimates of drinking water (Roseberry and Burmaster, 1992).
Risk assessment has been used recently to evaluate the human health impact of exposure
to microorganisms in food and various water supplies (Hass, 1983; Gerba and Haas,
1988; Rose et al., 1991; Regli et al., 1991; Rusin et al., 1997). The USEPA recommends
that microbial risks of infection should not exceed 1/10,000 (10) for drinking water for a
yearly exposure (Macler and Re2li, 1993).
The application of the risk assessment framework to viruses as a group has been
reviewed (Gerba and Haas, 1988; Regli et al., 1991; Haas et al., 1996). Rose et al.,
(1991) developed a risk assessment model to estimate the risk of infection after exposure
to treated waters contaminated with Giardia cysts. More recently, a risk assessment of
rotavirus has been conducted (Gerba et al., 1996). Rusin et al., (1997) estimated the daily
risk of bacterial (heterotrophic plate count) infection using the exponential model. Daily
18
risk were based on the consumption of 2 liters of water per day. Rusin et al., (1997)
summarized that the probability of infection is low and emphasized that further research
is needed to determine the occurrence of selected opportunistic pathogens in drinking
water.
Dose-response studies using human volunteers have been conducted for several
microorganisms including Pseudomonas aeruginosa (Buck and Cooke, 1969),
Aeromonas hydrophila (Morgan et al., 1985). Mycobacterium avium (Murphey et al.,
1983), rotavirus (Ward et al., 1986), hepatitis A virus (Ward et al., 1958), poliovirus
(Koprowski. 1956), and Cryptosporidium (Dupont et al., 1995). More data are needed on
the quantitative occurrence of opportunistic bacterial pathogens in drinking water.
The application of risk assessment methodology to estimate risks posed by
specific bacteria would provide a better understanding of the significance of bacterial
waterborne disease. This methodology can be applied to drinking water in both
developed and developing countries.
An Extensive literature review on opportunistic bacterial pathogens is presented in
the next section. Opportunistic pathogens were selected for this study. The research
reported here is original, hence, no such information are available from previously
reported studies.

19
A eromonas hydrophila
The genus Aeromonas occur as straight cells that are rod-shaped with rounded
ends. Their size range is 0.3 to 1.0 i_tm in diameter and 1.0 to 3.5 lam in length and they
exist singly, in pairs or short chains. They are Gram-negative, facultative anaerobes and
generally motile by a single polar flagellum. Metabolism of glucose is both fermentative
and respiratory. They are oxidase and catalase-positive, reduce nitrates to nitrites, and
utilize carbohydrates with the production of acid with gas. They are resistant to the
vibriostatic agent 0/129 with optimum growth temperature of 22-28°C (Rippey and
CabeIli, 1979).
While Aeromonas are undoubtedly more commonly isolated from patients with
gastroenteritis, reports of Aeromonas sepsis, wound and ocular infections have appeared
increasingly in the literature (Janda and Duffey, 1988). Unlike gastroenteritis, these
infections are often reported to have serious debilitating outcomes (George et al., 1985).
The highest seasonal incidence of A. hvdrophilcz diarrhea in the Unites States
occurs during summer months, some studies indicate that A. hydrophila infection is the
second or third leading cause of bacterial gastroenteritis during these months (Moyer,
1987; LeChevallier et al., 1982). Seidler et al., (1980) found Aeromonas in distribution
water systems during the summer months. Evidence suggests that this species is an
enteric pathogen around the world. However, the incidence of Aeromonas associated
diarrhea is relatively low in developed countries (Havelaar and Vonk, 1988).
Gastroenteritis due to A. hydrophila resembles that of shigellosis, in which the stool

20
specimen is bloody in appearance and numerous fecal leukocytes are present (George et
al., 1985). Since 1968, A. hydrophda species have been recognized as an opportunistic
pathogen that affects young children, elderly people and the immunocompromised host
( Von Gravenitz and Mensh, 1968). The pathogenicity of A. hydrophda has been
associated with the production of exotoxins. Clinical and environmental strains of A.
hydrophda have been reported to produce both heat-labile and heat-stable cytotoxins that
have enterotoxic activities (Janda, 1991). Despite the production of extracellular enzymes
and toxins, the pathogenesis of A. hydrophila infections remains unclear (Handfield et al.,
1996).
The bacteria can be cultured on a wide range of agar media containing ampicillin.
Handfield et al., (1996) efficiently used ampicillin-dextrin agar with a standard
membrane filtration procedure for isolating A. hydrophda from drinking water. The
choice of a specific medium for isolation of Aeromonas spp. will depend on the type of
sample to be examined and whether a detection or quantitative determination is needed
(Jeppesen, 1995). Conventional biochemical tests help to identify Aeromonas (Janda et
al., 1995). Chromogenic substrates (API systems) and carbohydrate utilization (BIOLOG
GN microplates) are utilized (Janda et al., 1995). Aeromonas strains can also be identified
by fingerprinting (multilocus enzyme electrophoresis) (Altweg et al., 1991), ribotyping
(Martinetti and Altwegg, 1992), and protein electrophoresis (Kuijper et al., 1989).
Aeroinonas can survive standard chlorination and thus re-colonize the water
distribution networks after the chlorination process (Van der Kooij, 1988). Aeromonas
21
have been isolated from chlorinated water systems, where they persist as a component of
biofilms (Van der Kooij, 1991). They represent from 17 to 25% of the total indicator
bacteria recovered (Clark et al., 1982). The bacterium has been found to survive for up to
60 days and proliferate to levels >10 5 CFU/mL in water stored at room temperature
(Warburton, 1994b).
A. hydrophila is a ubiquitous bacterium frequently isolated from food, drinking
water, and aquatic environments (Holmberg et al., 1986). It has been recovered from 0.6-
18.2% of natural fresh water samples at concentration range of 0.1-3600 CFU/mL (Rusin
et al., 1997). Handfield et al., (1996) recovered 94 CFU of A. hydrophila from
chlorinated and unchlorinated drinking-water supplies. Small numbers of A. hydrophila
(6.6 to 12 °A) have been recovered from tap water (Chaidez and Gerba, 1998; Levesque et
al., 1994)
Chaidez and Gerba, (1998) and Tsai and Yu, (1997) recovered small numbers (1.4
to 6.9%) of the bacterium from bottled water. Two European studies from Spain and
Portugal have identified A. hydrophila (6.6 to 50%) in bottled mineral waters (Gonzalez
et al., 1987; Manaia et al., 1990). Hunter (1994) failed to recover the bacterium from
bottled water samples obtained from the United Kingdom. A. hydrophila as well as other
opportunistic pathogens have been encountered in plumbing system biofilms (Dennis et
al., 1989). Levesque et al., (1994) observed the bacterium in the water cooler biofilms
and recovered it from 22% of the samples tested.

22
Volunteer feeding studies with large oral doses (up to 10 10 CFU) have failed to
produce human illness (Morgan et al., 1985). Two subjects showed symptoms of
diarrhea with doses of 10' CFU, but the organism did not appear in the stools. There is
controversy as to whether the organism is a cause of human gastroenteritis. It possesses
several attributes that may act as a pathogen for humans. Also, the presence in the stools
of individuals with diarrhea suggests that the bacterium may be an infectious agent to
humans.
Coliform bacteria
The coli form group consists of several genera of bacteria belonging to the family
Enterobacteriaceae (Bitton, 1994). Traditionally these genera include Escherichia,
Citrobacter, Enterobacter and Klebsiella. However, using more modern taxonomical
criteria, the group is heterogenous and includes non-fecal lactose-fermenting bacteria as
well as other species which are rarely found in feces but are capable of multiplication in
water (Gleeson and Gray, 1997).
The coliform group is normally defined as compromising all aerobic and
facultative anaerobic, Gram-negative, non-spore forming, rod-shaped bacteria that
develop a red colony with a metallic sheen within 24 h at 35°C on an Endo type medium
containing lactose (APHA, 1995). They are also oxidase-negative, non-spore forming
and display beta-galactosidase activity. The coliform group also includes the
then-notolerant fecal coliforms. These are defined as being able to ferment lactose at

23
44.5 'C (WHO. 1993), and not only include E. cou, but also species of the Klebsiella,
Enterobacter and Citrobacter genera (Bitton, 1994). E. colt is considered to be the only
true fecal coliform as other thermotolerante coliforms can be derived from non-fecally
contaminated water (Gleeson and Gray, 1997).
The coliform index is still widely considered to be reliable indicator for potable
water (Gleeson and Gray, 1997). However, its use has been questioned as a measure of
water quality. The coliform group have several deficiencies as indicator organisms: re-
growth in aquatic environments and distribution systems, suppression by high
background bacterial growth, not indicative of health threat, a lack of correlation between
protozoan and viral numbers, and the occurrence of false-positive and false-negative
results (Gleeson and Gray, 1997; Bitton, 1994).
In the bacteriological examination of drinking water, emphasis is often placed on
frequent sampling and simpler, cheaper tests as opposed to occasional sampling by more
expensive methods (Gleeson and Gray, 1997). As both the multiple tube method and
membrane filtration (MF) techniques are recognized as being relatively simple and
inexpensive they have tended to become the leader of microbiological water assessment
worldwide. Both of these methods are based on the ability of coliforms to produce acid
and gas from lactose-based media (Gleeson and Gray, 1997). Despite their widespread
use, it is recognized that both methods suffer from inherent faults; the MPN is
fundamentally inaccurate, whereas the sensitivity of the MF procedure can be affected by
a number of variables (Bitton, 1994).

24
Rapid tests that can currently be performed for detecting coliforms have little
specificity and may include non-viable cells (PCR, Gene Probes), and false-positive
results (Colilert system) (Bitton, 1994).
Over the years. several groups of bacteria have been suggested as alternative of
fecal indicators. Organisms such as fecal streptococci and Clostridium perfringens have
widely used as indicator of fecal pollution (Geldreich, 1996; Payment et al., 1997). Many
proposed indicator organisms involve complex and expensive methodologies which are
beyond the means of capabilities of smaller utilities and developing countries and,
therefore, can not be applied as a routine basis (Gleeson and Gray, 1997). It would
therefore appear that currently used bacterial indicators will go on being used throughout
the world until an alternative is found that meets all the criteria established for indicator
organisms and that is acceptable in terms and simplicity (Bitton, 1994).
In conclusion, it would appear that there is still a place for the coliform as a
measure of treatment effectiveness; however, their presence in water should no longer
remain the sole source criterion on which the microbiological quality of water is based.
Heterotrophic plate count (HPC)
The first edition of Standard Methods for the Examination of Water and
Wastewater was published in 1905 and included methods for counting bacteria on agar
media, also known as standard plate count bacteria and currently referred to as the
heterotrophic plate count (HPC) bacteria (Rusin et al., 1997).

95
HPC bacteria in drinking water are composed of many transient organisms that
never colonize the distribution system, while other associate organisms are more
opportunistic, being capable of surviving on minimal nutrients, attachment to pipes
sediments, and becoming participants in the development of biofilms (Geldreich, 1996).
HPC bacteria represent the aerobic and facultative anaerobic bacteria that derive their
carbon and energy from organic compounds (Bitton, 1994). The number of recovered
bacteria depends on medium composition, period of incubation (1-7 days), and
temperature of incubation (20-35°C) (Reasoner, 1990). This group includes Gram-
negative bacteria belonging to the following genera: Pseudomonas, Aeromonas,
Mycobacterium, Klebsiella, Flavobacterium, Enterobacter, Citrobacter, Serratia,
Acinetobacter, Proteus, Alcaligenes, and Morallexa. Some members of this group are
opportunistic pathogens (Aeromonas, Flavobacterium, Pseudomonas and
Mycobacterium), but little is known about the effects of high numbers of HPC bacteria on
human health (Bitton, 1994). In drinking water, the number of HPC bacteria may vary
from less than one CFU/mL to more than 104 CFU/mL, and they are influenced mainly
by the temperature, presence of chlorine residual, and level of assimilable organic matter.
HPC bacteria levels should not be high due to the possible decrease in sensitivity of the
coliform test, the masking of health significant bacteria (EPA, 1989), and increased of
risk for exposure, especially to the infirm, the elderly and the young (Geldreich et al.,
1975; Payment et al., 1991).

26
Heterotrophic bacteria densities in most municipal water supplies are generally
below 100 organisms per mL except at static water locations in buildings where densities
are often one or two log higher because of warm ambient temperatures (Geldreich, 1986).
HPC bacteria are not of immediate public health significance, but upon amplification in a
protected habitat become the source of taste and odor complaints or emerge as an
opportunistic pathogen threat (Geldreich, 1996). Reasoner (1989), defined the use of
HPC bacteria in the water treatment process:
• Monitoring the efficiency of water treatment process (primarily disinfection).
• Evaluation of levels of HPC bacteria that may interfere with coliform
monitoring.
• Evaluation of finished water quality during storage and distribution.
• Evaluation of microbial growth on materials used in construction of potable
water treatment and distribution system.
• Evaluation of bacterial re-growth in treated drinking water.
• Evaluation of changes in the population of bacteria during changes in
treatment.
Bacteria in drinking water supplies are generally not physiologically vigorous.
Many of these organisms have been stressed by recent passage of surface water through
the disinfection process or are starved because of minimal nutrient concentrations of
available nutrients in the water (McFeters, 1990). Survivors that reach the distribution
system may adjust to low-nutrient conditions, and slowly colonize a biofilm (Reasoner,

27
1990). Therefore. cultivation requires careful consideration. The use of R2A agar in the
spread plate method is recommended as the medium of choice (Reasoner and Geldreich,
1985). The incubation time is interrelated with selection of temperature. As a general
rule, for the detection of a greater portion of HPC bacteria, it is necessary to use of 28°C
for at least 7 days (Lombardo et al., 1985).
A characteristic of some bacteria found in water supplies is the ability to form
brightly colored non-photosynthetic, non-diffusible pigments (Geldreich, 1996). The
pigmented bacteria may compromise 80-100% of the HPC bacteria not only in
distribution system, but also in bottled water and a variety of attachment devices
including drinking water fountains, water vending machines, ice machines, and point-of-
use-treated waters (Chaidez et al., 1997; Geldreich et al., 1985; Reasoner et al., 1989;
Ridgway and Olson, 1982). Pigmented bacteria appear to adapt well to the distribution
system environment, with at least two populations, the yellow and orange pigmented
groups, being always present in slow-flow and dead-end sections of the pipe network
(Geldreich, 1996).
Flavobacterium
The natural habitat of these bacteria are soil, plants, and water sources.
Flavobacterium form bright-yellow colonies. Flavobacterium can be opportunistic
pathogens and have been implicated in human infections including meningitis (infants),
pneumonia, endocarditis, and septicemia (Dooley et al., 1980). The most important

28
clinical species is F. meninç,Yosepticum (Rusin et al.. 1997). F. meningosepticum has been
recovered from a variety of water system attachment devices including nebulizers,
distilled water systems, sink faucets, and drinking water fountains (Werthamer and
Weiner, 1972). In the United States the cases of neonatal meningitis due to F.
meningosepticum are very rare, only 0.04% per year (Rusin et al., 1997).
A cinetobacter
Acinetobacter is isolated in very low numbers and it is considered to be of low
virulence. Humans carry the bacterium as a normal flora of the skin, being the site source
for most outbreaks of hospitals infections. Acinetobacter is involved in nosocomial and
community-acquired infections. Predisposing factors including malignancy, burns,
immunosuppression, major surgery are necessary to trigger the infection (Rusin et al.,
1997).
Acinetobacter can be isolated from many different water sources. LeChevallier et
al.. (1980) analyzed water from the distribution systems and found that from 5-97% of the
samples contained the bacterium. Acinetobacter has been recovered from bottled water
and water coolers (Gonzalez et al., 1987 and Levesque et al., 1994). Studies on the
infective dose are scarce. The lethal dose to mice is 10 6-10 8 when injected
intraperitoneally (Bergogne-Berezin, 1994).

29
VIoraxella
illoraxella appears as a normal flora of the respiratory tract as well as human skin.
Moraxella species cause upper respiratory infections and eye infections , they can also
produce septicemia and meningitis (Rusin et al., 1997). Moraxella species are present in
water sources, including distribution system, bottled water and water coolers (Payment et
al., 1988; Edberg et al.. 1996 and Levesque et al., 1994). No studies on the infective dose
have been done.
Xanthomonas
Most of the members of this group are non-pathogenic to humans, but may be
harmful to plants. X maltophila is the only member of this group that may cause disease
to humans. The diseases include septicemia, pneumonia, and wound infection.
Antibiotic treatment and cancer therapy are the two risk factors associated with
this bacterium. Xanthomonas occur in the water environment at low numbers. It
compromises 5.7% of the HPC population found in raw surface water samples (Rusin et
al., 1997). The bacterium has been recovered from bottled waters and water coolers
(Manaia et al., 1990 and Levesque et al., 1994). High numbers (10 6-109) are required to
colonize the intestine of mice, but no signs of infection have been described (George et
al., 1989).
30
.11ycobacteria
It is common knowledge that some Mycobacteria are agents of chronic diseases in
humans and other animals, but it is not always recognized that most Mycobacteria are
free-living saprophytes which form part of the balanced microbial community in natural
habitats such as water or soils (Kubica and Wayne, 1984).
Mycobacteria are aerobic acid-alcohol that usually form slightly curved or straight
rods with a size range between 0.2-0.6 and 1.0-10 tm. Occasionally extensively
branched filaments may occur. The organisms are non-motile, and do not form
endospores, spores or capsules. Mycobacteria have cell walls with a high lipid content
that includes waxes (mycolic acids). They are not readily stained by the Gram method
but they are considered Gram-positive organisms (Kubica and Wayne, 1984).
Growth rates of Mycobacteria are slow with generation times varying by species
and ranging from 2 to >20h. Visible colonies may be produced after 2d to 8 weeks of
incubation under optimal conditions (depending the species). Optimal temperatures vary
widely among species, ranging from 30 to 45°C.
The most important pathogens are non-pigmented, including M tuberculosis, M
(MUM complex (avium and intracellulare), M asiaticum, and M. malmoense (Nolte and
Metchock, 1995).
31
The Mycobacterium avium complex (MAC) are composed of a serological group
consisting of 28 serovars of two species, M avium and M intracellulare. MAC are
ubiquitous organisms that cause disseminated disease, pulmonary disease, and cervical
lymphadenitis in the immunocompromised and to a lesser extent in normal individuals
(Korvick, 1996; Collins et al., 1984). Disseminated MAC infection is a progressive
illness, characterized by intermittent fever, sweating, weakness, anorexia, and weight
loss. Pulmonary disease due to MAC presents symptoms similar to those of tuberculosis,
with productive cough, fatigue, fever, weight loss, and night sweats. Pulmonary disease
caused by MAC was to be found as common as pulmonary tuberculosis in many areas of
the United States (Rosenweig and Schlueter, 1981). Cervical lymphadenitis usually
affects children less than 12 years of age, and is the leading cause of lymphadenitis in this
age group.
MAC becomes particularly invasive in susceptible individuals with predisposing
factors (elderly, newborns, burn cases, dialysis, AIDS patients, and individuals receiving
organ transplants). Furthermore, it has been recently shown that MAC infections also
affect normal individuals without predisposing factors (Glover et al., 1994). Studies
conducted by Prince et al., (1989) showed that M avium infection can also cause
osteomyelitis and septic arthritis in people with no known predisposing factors (Jones et
al., 1995; Prince et al., 1989). In the United States, many infections are asymptomatic
and occur early in life; 12% of the population has been infected by MAC (Von Reyn et
32
al., 1993). However, disease by MAC can be lethal and is difficult treat because it is
resistant to many antimycobacterial agents (Rusin et al., 1997).
M. avium has been frequently associated with disease in humans (Collins et al.,
1984). M avium is a waterborne opportunistic pathogen (Du Moulin et al., 1985).
However, the precise mode of transmission remains undetermined. Infection with M
avium is thought to occur from colonization of the gastrointestinal or respiratory tract
(Chin et al., 1994).
Several methods can be used to culture M avium from water sources. However,
the most popular and effective is membrane filtration, using 7H11 selective agar (Difco
Laboratories). Glover et al., (1994) successfully recovered MAC from Los Angeles tap
water following this method. Du Moulin and Stottmeier, (1978) concluded that treating
water samples with cetylpyridinium chloride (CPC) for 24 h reduced the contamination
and increased the recovery of Mycobacteria.
Mycobacteria are difficult to stain. Although they are classified as Gram-
positives organisms, the large amount of lipids present in their cell walls makes it
difficult to the dyes used in the Gram stain (Nolte and Metchock, 1995). Special staining
procedure is used to promote the uptake of dye in Mycobacteria (Auramine-O-acridine
orange, Ziehl-Neelsen and Kinyoun). Serology has been previously applied to the
identification of Mvcobacteria recovered from tap water. Graham et al., (1988) identified
M avium serovar 4 from one laboratory and four hospital wards, using the Shaeffer
seroagglutination method. PCR has been widely used for the differentiation of M. avium

33
and M intracellulare from clinical specimens (D,vadyk et al., 1994: Yamamoto et al.,
1993).
MAC can be isolated from numerous sources in the environment, including water,
aerosols, and soil (Kirschner et al., 1992). Evidence suggests a higher incidence of MAC
infections due to M avium than M intracellulare. For example, Korvick, (1996)
mentioned that over 98% of cases of MAC infections in AIDS patients are caused by M.
avium serotypes, particularly 1, 4, and 8, rather than M. intracellulare. Glover et al.,
(1994) found a high incidence of M. avium serotypes 1 and 8 from hospital water in the
Los Angeles area. These results coincide with those reported by Yakrus and Good,
(1990) in which it was found that serotype 8 was the predominant serotype among
clinical isolates in Los Angeles area. The environmental reservoirs and route of
acquisition of the organism are most likely water and aerosols. Hospital water systems
often harbor MAC (Horsburgh, 1991), and may be a source of nosocomial infections
(Von Reyn et al., 1994).
Glover et al., (1994) examined Los Angeles tap water and found M avium in 70%
of hospitals, 9% of dwellings, and 15% of reservoirs. Chaidez and Gerba, (1998) found
that 43% of the tap water analyzed had acid-fast organisms. It has also been found in up
to 50% of municipal and private drinking water samples at concentrations of 0.01-5.2
CFU/mL (Rusin et al., 1997). Collins et al., (1984) mentioned that MAC is particularly
resistant to chlorination of water. Surucu and Haas, (1976) and Goslee and Wolinsky,
(1976) reported that M. aviuin was resistant to the usual chlorine doses that inactivate
34
conforms and viruses. Mycobacteria were also more resistant than E. colt to inactivation
by chloramines and by ozone (Severin, 1976; Goslee and Wolinsky, 1976). The
resistance of those microorganisms to chlorine disinfection in water may be a particularly
important factor in the occurrence of MAC infections (Geldreich, 1996). MAC have been
isolated from water samples with temperatures ranging from 2 to 57.2°C, and residual
chlorine concentrations of 0.02 to 0.3 mg/L (Du Moulin et al., 1988; George et al., 1980).
Little information has been obtained about the presence of Mycobacteria in
bottled water. Caroli et al., (1985) reported the presence of Mycobacteria in 9 samples of
84 bottled water samples tested, but, none were M avium. The acid-fast bacilli isolated
were M gordonae, M flavescens, M phlei, and Nocardia sp. Similarly, Chaidez and
Gerba, (1998) identified acid-fast organisms from 13% of the bottled water samples
analyzed. Holtzman et al., (1997) examined 20 brands of bottled water and no acid-fast
organisms were found. The reason for this variation could be that not all bottled water
are processed by the same method and some could contain significant contaminants.
However further studies are required to elucidate such variation.
Point-of-Use (POU)-devices attached to building plumbing systems may even
enhance the growth of Mycobacteria (Geldreich, 1996). POU-devices might be expected
to remove Mycobacteria by physical methods, but it is also possible that the organism
might colonize and multiply in the filter's biofilm and, thereafter, appear in the product
water (Collins et al., 1984). Chaidez and Gerba, (1998) found acid-fast organisms in
33.3% of POU product water.

35
Chaidez et al., (1997) conducted a study on water obtained from vending
machines and found acid-fast organisms in the product water. Water vending machines
are connected to an approved local water supply system and processed the water by
reverse osmosis, carbon filters, and ultraviolet light (Lynkins et al., 1992). Studies have
shown that Mycobacteria are among the first organisms to colonize reverse osmosis
membranes (Geldreich, 1996). Ridgway et al., (1985) suggested that the hydrophobic
cell surface of Mycobacteria may play an important role in the bacterial adhesion to
reverse osmosis membranes.
It has been shown that tap water can harbor M. avium and that it may be the
vehicle responsible for transmission to AIDS patients, and to non-AIDS patients with
predisposing factors (Glover et al., 1994; Von Reyn et al., 1994; Mansfield and Lackner,
1997). Von Reyn et al., (1993) isolated M avium from 32% of the samples from water
supply systems in the United States. Peters et al., (1995) found M avium in 2% of the
samples obtained from tap water in Germany. Mycobacteria are important components
of biofilms in tap water distribution systems, being found in 90% of the biofilm samples
with densities ranging from 10 3 to 104 CFU/cm2 (Schulze-Robbecke et al.,
1992).
The infective dose of M. avium is quite high according to laboratory studies by
Bermudez et al., (1992). Five oral doses of 10 8 CFU of MAC resulted in bacteremia in
45% of the animals with 26% mortality. The use of alcohol (ingestion of ethanol) aided
to a significant increase the number of M avium recovered from the liver, spleen, and
36
appendix (Bermudez et al., 1992). Studies in human volunteers are scarce and no
publications are available that provide the infectious dose in humans.
Plesiomonas shigelloides
Plesiomonas shigelloides, a member of the family Vibronaceae, is a facultative
anaerobic, Gram-negative, nonspore-forming rod that measure 0.8 to 1.0 by 3.0 1AM and
can occur singly, in pairs, or in short chains (Janda et al., 1995). They are usually motile
by two or five lophotrichous polar flagella and are catalase, oxidase, and nitrate positive.
They ferment D-glucose and a few other carbohydrates but without production of gas
(Freund et al., 1988).
Infections attributed to P. shigelloides are almost exclusively restricted to two
clinical settings: The most common presentation is watery diarrheal illness often found
in individuals with a history of freshwater contact, seafood consumption, exposure to
amphibia or reptiles, or travel to developing countries (Janda et al., 1995); The
gastroenteritis is usually a mild self-limiting disease with fever, chills, abdominal pain,
nausea, or vomiting (Holmberg et al., 1986). The peak season of P. shigelloides
associated diarrheal disease appear to be similar to that of Aeromonas-associated diarrhea
(warner months). The second well-recognized syndrome associated with P. shigelloides
is septicemia, often accompanied by meningitis (Janda et al., 1995). Most published
cases of Plesiomonas-meningitis have occurred in newborn babies whose deliveries
which been complicated by various medical conditions, including prolonged rupture of
37
the mother's membranes. The fatality rate in such instances approaches 70% (Janda et
al., 1995).
The link between P. shigelloides and diarrhea appears to be rather weak.
Liesenfeld et al., (1993) found P. shigelloides in stool samples in only 0.014% of
diarrheal patients in Germany. This frequency is not much higher than the carrier rate of
0.0078% described by Arai et al., (1980) in healthy humans. Rautelin et al., (1995)
isolated 20/13,027 (0.15%) from stool samples in Helsinki. All except 2/20
Plesiomonas-positive patients had diarrhea; 13 patients had onset of illness after foreign
travel and 5 patients had chronic diarrhea with symptoms lasting 2 months. Morbidity
and Mortality Weekly Report (MMWR) described an outbreak in associated with
contaminated water supply in Livignstone County, NY. Thirty persons became ill
(diarrhea), due to the presence of P. shigelloides and Salmonella in the drinking water
source (MMWR, 1998).
P. shigelloides has been isolated using routine clinical procedures for the
Enterobactericeae which includes MacConkeys, Salmonella-Shigella, Deoxycholate,
Hektoen, and XLD agars (Cooper and Brown, 1968). The organism grows well on
enteric agars and can easily be mistaken as a member of the Enterobactericeae (Miller
and Koburger, 1985). There are several selective media proposed for the isolation of the
bacterium (Jeppesen. 1995). However, for routine analysis of environmental and food
samples inositol brilliant green bile salts (IBB) and Plesiomonas (PL) agar are
recommended for best results (Jeppesen, 1995).

38
P. shigelloides is widespread in nature and has been isolated in many different
countries (Miller and Koburger, 1985). Hernandez and Rodriguez de Garcia, (1997)
found a prevalence of 59% in surface water from Venezuela during the warmer months.
Tsukamoto et al., (1978) surveyed water samples in Japan and found that P. shigelloides
was present in 60% of pond water and 35.7% of river water samples. In Nigeria, well
waters were sampled for the presence of P. shigelloides and 7.4% of the wells were
positive (Kwaga et al., 1988). Medema and Schets, (1993) found P. shigelloides in 30 of
42 samples in fresh water in the Netherlands. P. shigelloides showed a positive
correlation with the presence of fecal pollution (E. cou). Others authors have reported the
occurrence of P. shigelloides in surface water around the world including Australia
(Cooper and Brown, 1968), and the United States (Rutala et al., 1982). P. shigelloides is
considered as a waterborne opportunistic pathogen (Tsukamoto, 1978). It is found most
often in fresh surface waters, but there are some reports of its presence in seawater
(Cabelli, 1978). Chaidez and Gerba, (1998) analyzed various water sources including
bottled water, tap water, and point-of-use treated water and found that P. shigelloides was
absent from those sources.
Animal and human feeding studies have been conducted for P. shigelloides.
Herrington et al., (1987), conducted human feeding studies using young healthy humans.
None of the volunteers developed diarrhea or any other disease symptoms. Pretreatment
with ampicillin did not enhance colonization. In rabbit feeding studies, it was found that
only one rabbit developed diarrhea, but when re-tested, none of the five strains could

39
induce diarrhea. Oral doses of P. shigelloides produced disease in a semi-consistent
manner only when administered to gnotobiotic piglets. Oral doses of 109 CFU produced
diarrhea within 6 days in 3 of 3 piglets while a higher dose of 10 10 CFU induced shock in
2 of 2 piglets (Rusin et al., 1997).
Pseudomonas aerugin osa
Pseudomonas species are Gram-negative, straight or slightly curved rods, motile
with polar flagella (Hoadley, 1977). They are oxidase and catalase-positive. The size
ranges between 1 to 5 im long and 0.5 to 1.0 p.m wide. They are obligate aerobes, with a
respiratory metabolism in which oxygen is the terminal electron acceptor (Gilligan,
1995). Some isolates may grow under anaerobic conditions if nitrate is present (Hoadley,
1977). The nutritional versatility of Pseudomonas aid to utilize carbohydrates, alcohols,
and aminoacids as a carbon source (Gilligan, 1995). Certain species have distinctive
colony morphologies or pigmentation. Some species can multiply at 4°C, but most are
mesophilic, with optimal growth temperatures between 30 and 37°C (Palleroni, 1984). P.
aeruginosa is capable of growing at 41°C (Hoadley, 1977).
The genus Pseudomonas contains several well-recognized pathogens, including
Pseudomonas mallei, P. pseudomallei, P. cepacia, and P. aeruginosa. The Pseudomonas
most commonly associated with food and water is P. aeruginosa (Stiles, 1989). P.
40
aeruginosa represents special hazard in patients requiring instrumentation (i.e. catheter,
aerators. respiratory therapy equipment) which can introduce bacteria to susceptible
tissues, also in lesions containing necrotic tissues (burns) or fluids (urine) in which the
organism can grow rapidly, from small inocula to potentially invasive numbers (Fick,
1993). In addition to its nosocomial sources, the bacterium may be found in swimming
pools, hot tubs, and contact lens solutions (Gilligan, 1995).
It rarely causes problems in healthy persons, but it has been implicated in
epidemic diarrhea in infants (Hunter and Ensign, 1947). In hospitalized and
immunocompromised patients the organism has the ability to produce serious diseases,
including endocarditis, meningitis, pneumonia, and septicemia (Bodey et al., 1983). The
infection causes a sudden onset of fever, abdominal distention, and pain that gradually
increases (Stiles, 1989). It also causes nosocomial urinary tract infections, wound
infections, and bacteremia (Favero et al., 1971). Other serious infections involves eyes,
ear, skin and nose (Geldreich, 1996). The CDC reported an outbreak in which
individuals who were bathed in a hot tub developed folliculitis and otitis due to P.
aeruginosa (CDC, 1982).
P. aeruginosa is a common pathogen in the U.S., this bacterium alone has
accumulated some impressive figures: Up to two thirds of hospitalized patients,
particularly the critically ill, become colonized with P. aerugin osa, this often presages
more invasive disease. Two thirds of pneumonias are hospital-acquired, and P.
aeruginosa is listed as the leading cause of nosocomial respiratory tract infection (Fick,

41
1993). The mortality of nosocomial pneumonias remains as high as 70% (Celis et al.,
1988). Cystic fibrosis (CF) is the most common lethal genetic disease of Caucasians, and
chronic Pseudonionas respiratory infections complicate 90% of CF patients leading to
respiratory failure and death (Gilligan, 1991).
In 1946, an epidemic of acute P. aeruginosa gastroenteritis was reported in which
milk was implicated. There were 409 cases with symptoms of diarrhea, cramps, nausea,
and vomiting. Symptoms were more severe in infants and children, and there were nine
deaths in infants (Hunter and Ensign, 1947). In 1974, an outbreak of P. aeruginosa
foodborne illness was reported in a school; 7.7% of the infected developed weakness,
dizziness, and arthralgia, but without diarrhea (Meitert et al., 1984).
Bert et al., (1998) reported an outbreak of P. aeruginosa in hospital tap water;
nine patients were diagnosed with urinary tract infections, pneumonia and sinusitis. An
outbreak of funicular sepsis (infection of the umbilical cord resulting in bacteremia) in 10
newborns in a hospital of Germany was reported with P. aerugionsa the organism
isolated (Weber et al., 1971). There is some evidence that such infections are caused by
consumption of contaminated water. However, the information in this study was scarce
and the evidence was circumstantial (Rusin et al., 1997).
The presence of P. aeruginosa in surface waters has been associated with sewage
discharges (Alonso et al., 1989). Counts of the bacterium in sewage often exceed 10 5 per
100 mL (Hoadley, 1977). Its presence may be considered as an indicator of such
pollution (Warburton et al., 1994; Geldreich, 1986). Up to 15% of the normal human
42
population are fecal carriers of P. aeruginosa. The isolation rate from feces of
hospitalized patients is 20% or greater, and recovery rates occur in patients with longer
times of hospitalization (Sloodley and Thom, 1970). Colonized patients are at greater
risk of infection (Bodey et al., 1983). The most important mode of transmission is
person-to-person, but it can also occur from common environmental sources, including
water, soil, and foods (Shooter et al., 1969).
Several methods have been employed to enumerate or confirm the presence of this
bacterium in waters. However, the membrane filtration technique has been the most
widely applied for the isolation of P. aeruginosa (Hoadley, 1977). P. aeruginosa isolates
are easily recognized on primary isolation media on the basis of colony morphology,
production of pigments and grape-like odor (Gilligan, 1995). Culture media facilitate the
isolation from environmental sources. Generally, bacterial growth showing blue-green
fluorescence after 24h at 37°C on cetrimide is virtually always P. aeruginosa (Hoadley,
1977). The bacterium can be identified on the basis of a positive oxidase test, and triple
sugar iron (TSI) agar reaction (Gilligan, 1995). Most of the commercial kit systems can
identify P. aeruginosa (Gilligan, 1995) However, such kits are expensive and the results
are not 100% accurate (Gilligan, 1995).
P. aeruginosa is able to multiply in low nutrient water and can therefore, colonize
a variety of drinking water sources (bottled water, water vending machines, mineral
water) (Gonzalez et al., 1987; Chaidez et al.. 1997; and Manaia et al., 1990).

43
P. aeruginosa can be recovered in low numbers in drinking water (Hardalo and
Edberg, 1997). Hoadley, (19 7 ') found that the occurrence of this microorganism is
usually low in water, especially in treated (chlorinated) drinking water (3.7%). Similarly,
Edberg et al., (1996) found that 3% of drinking water samples (bottled water, water
coolers units, and tap water) contained P. aeruginosa. Five isolates from the green
pigmented colonies were satisfactorily identified as strains of P. aeruginosa from bottled
water from Nigeria (Ogan, 1992). Manaia et al., (1990) identified P. aeruginosa in 29%
of Portuguese bottled water and Fewtrell et al., (1997) found the bacterium in 1.2% of
bottled water from England. Chaidez and Gerba (1998) found P. aeruginosa in 8.3% of
bottled water collected from Costa Rica, Mexico, U.S., Japan, Korea, Greece, and
Panama. On the other hand, Hernandez-Duquino and Rosenberg, (1987) did not isolate
P. aeruginosa from both German and American bottled waters nor did Hunter, (1994) in
bottled water obtained from England.
Levesque et al., (1994) did not detect P. aeruginosa in water cooler samples. In
contrast, P. aeruginosa was found in 23% of the water vending machines (WVM) water
samples (Chaidez et al., 1997). Point-of-Use (POU) home devices may be very effective
initially for some specific contaminants, however their usefulness may become limited.
Chaidez and Gerba, (1998) found P. aeruginosa in POU devices during a six weeks
sampling. This indicate that colonization is not transient and may be due to the ability of
P. aeruginosa to form biofilms in water pipes (Brown and Gauthier, 1993; Geldreich,
1996). P. aeruginosa has the ability to multiply in process units such as sand and
44
activated carbon filters (Grabow et al., 1980). P. aeruginosa use trace nutrients present
either in the water or attached to the carbon filters to grow (TamaE,rini and Gonzalez,
1997). P. aeruginosa can be also recovered often in high numbers, in common food,
especially vegetables. Tomato salad may contain 5x10 3 organisms per serving size
(Kominos et al., 1972).
It is apparent that P. aerugin osa can cause both foodborne and waterborne illness
(Meitert et al., 1984; Bert et al., 1998). Contaminated water supply might be a more
significant source of infection than foods, especially for infants (Weber et al., 1971). The
presence of P. aeruginosa in water does not justify specific attention for healthy people,
but in the hospital environment, especially for immunocompromised individuals, special
precautions would be justified (Stiles, 1989). Although acquired immunodeficiency
syndrome (AIDS) patients are immunocompromised, P. aeruginosa is not predominant
opportunistic pathogen for this population (Rusin et al., 1997).
Larger numbers are required to colonize the respiratory tract of healthy
individuals. The infective dose for P. aeruginosa is quite high according to Buck and
Cooke, (1969). They found that oral doses of >1.5x106 CFU are required to colonize
healthy volunteers. Volunteers with ampicillin treatment excrete 2x10 8 of P. aeruginosa
for up to 14 days. The selective pressure of antibiotic treatment could extend the
incidence and time of colonization. Excretion was limited to 6 days by volunteers not
taking ampicillin. Colonization by P. aeruginosa in hospitalized individuals may occur

45
by ingesting less than 10 3 to 104 of the organism (Pollack, 1990). Although P.
aerugin osa is sometimes found as a normal flora in man, the prevalence of colonization
in healthy adults outside the hospital are low (2.6-24%), and the probability of infection
in healthy individuals appears to be very low (Rusin et al., 1997). Hospitalization leads
to greatly increased rates of carriage, especially in patients with serious burns.
Colonization of a hospital patient often presages disease (Rusin et al., 1997).
Dissertation Format
The research presented in the appendices of this dissertation consists of four
related studies designed and undertaken by the candidate: 1) The microbiological quality
of water from vending machines; 2) A survey of the microbial quality of water from
storage tanks; 3) Microbiological comparison of the water quality of point-of-use treated
water, tap water, and bottled water; and 4) Aeromonas hydrophila and Pseudomonas
aeruginosa in drinking water from various sources: a risk assessment.
Dr. Charles P. Gerba is a co-author on all of the papers and served as an advisor to
the candidate's research. The Department of Nutritional Sciences requires that each
candidate submit their original research to peer-reviewed scientific journals for
publication. By using this dissertation format, the candidate's research is presented as
four separate papers.

46
CHAPTER 2
PRESENT STUDY
The methods. results and conclusions of this study are presented in the articles
appended to this dissertation. The following is a summary of the most important
findings.
The first article is a study conducted on the microbiological quality of drinking
water from vending machines. The information obtained from this study can be used to
identify the bacterial quality of the water dispensed from such machines. Opportunistic
bacterial pathogens data were used for the elaboration of microbial risk assessment.
The second article presents a survey of the microbial drinking water quality of
storage tanks. The information obtained here helped to inform and persuade the
community to the importance of maintenance of water storage tanks (WST). Also,
Pseudomonas aerugmosa data obtained in this study was used to conduct a microbial
risks assessment.
The third article is an extensive study on the bacterial quality of the drinking
water obtained from point-of-use (POU) devices, tap water with POU-connection, and
bottled water. The information was utilized to perform the microbial risk assessment.
A formal microbial risk assessment was conducted using the data obtained from
the three articles appended to this dissertation. Aeromonas hydrophila and P. aeruginosa
47
data were selected to estimate risk associated with exposure to opportunistic bacterial
pathogens in drinking water. The results and the conclusions are presented in the fourth
article. Estimated annual risks of colonization for drinking water from selected sources
were determined to be as high as 10 and 10' for A. hydrophda and P. aeruginosa,
respectively.

APPENDIX 1:
MICROBIOLOGICAL QUALITY OF WATER VENDING MACHINES
Cristobal Chaidez Quiroz 1 , Pat Rusin', Jaime Naranjo', and Charles P. Gerba* I '"
Department of Nutritional Sciences', Department of Soil, Water, and EnvironmentalSciences',
The University of Arizona, Tucson, AZ., 85721.
48
*Corresponding author
Abstract
Consumption of water from vending machines has recently increased in the
United States. However, studies describing the bacteriological quality of these machines
are scarce. In this study, bacteriological analyses were performed on samples from 30
water vending machines (WVM), three of which were sampled weekly for three weeks.
Bacteriological analyses were also conducted on the nozzle dispensers and the drains of
fifteen WVM. Heterotrophic bacteria, total and fecal coliforms, and Pseudomonas
aeruginosa were enumerated. Physico-chemical parameters such as pH, temperature,
turbidity, and residual chlorine were also examined. P. aeruginosa was found in 23% of
the water samples and coliform bacteria in 20%. Heterotrophic plate count (HPC)
bacteria were found in all samples and 73% had numbers greater than 500 colony forming
units (CFU)/mL. The HPC bacteria ranged from 9 to 48,000 CFU/sampled area on the
dispensing nozzle. Total coliforms and Escherichia coli were detected in the drain
samples with HPC bacterial concentrations from 1,000 to 56,000 CFU/sampled area. No
significant correlation was found between the physico-chemical and bacteriological
parameters. Regular cleaning and maintenance procedures should be implemented to
reduce bacterial concentrations in the product water.
Keywords: Water vending machines; bacteria; coliform; Pseudomonas aeruginosa;
heterotrophic bacteria.
49
Introduction
The water vending machine (WVM) industry has experienced an increase in growth over
the past few years (Lynkins et al., 1992). Likewise public awareness of water quality has
increased significantly. People use WVM as an alternative drinking water supply
because they believe it tastes better, is safer, and free of contaminants. There are many
factors that lead consumers to obtain drinking water from sources other than the tap.
Health risks, both real and perceived, are often the main reason why people use WVM as
a source of drinking water. Tucson, Arizona has large numbers of WVM located at high
traffic locations such as supermarkets, drugstores, and variety stores. Water is delivered,
by these machines, in volumes (3.7 liters) to the consumer's containers. The Food and
Drug Administration (FDA) considers WVM as food vendors and regulates them
according to the Food and Beverage Model Ordinance. However, the state of Arizona
has no specific regulations regarding WVM unless a complaint is received. Since water
from vending machines must come from an approved municipal source, the assumption is
that the water should meet Environmental Protection Agency (EPA) standards (Gelt,
1996). According to Lynkins et al., (1992) WVMs follow a typical POU/POE (point-of-
use/point-of-entry) technology that require little technical service. The carbon filters are
changed as required, the ultraviolet lamp is replaced annually, and the reverse osmosis
(RO) membrane is replaced every 2-3 years. The WVMs surveyed in this study are
50

51
connected to an approved local water supply system and processed the water by reverse
osmosis, carbon filtration, and ultraviolet light.
Drinking water contains heterotrophic bacteria including Acinetobacter,
Flavobacterium, Moraxella, Çvtophoga, Achromobacter, Pseudomonas, and Alcaligenes
spp. (McFeters, 1990). Some of these genera include opportunistic pathogens such as
Pseudomonas aeruginosa, Alcaligenes faecalis, Acinetobacter baumanii, and
Flavobacterium meningosepticum species that can cause nosocomial and community-
acquired infections (Bitton, 1994). Of these, P. aeruginosa is the pathogen most common
associated with documented illnesses (Rusin et al., 1997). Favero et al., (1971) described
P. aeruginosa as an important nosocomial pathogen that is associated with hospital
equipment contamination. Contaminated foods and water supplies have also been
implicated as routes of transmission in the hospital environment (Shooter et al., 1969),
although never conclusively shown to be a source. P. aeruginosa is responsible for 9%
of all nosocomial infections (Hoadley, 1977), being the leading cause of nosocomial
respiratory tract infections. It also causes nosocomial urinary tract infections, wound
infections, and bacteremia (Murray et al., 1995).
Other factors affecting the microbial quality of WVM product water are the
carbon filters and RO membranes. While carbon filters may be very effective initially
removing specific contaminants, studies have shown (Taylor et al., 1979) that
heterotrophic plate count (HPC) bacteria can colonize the carbon filters in a short period,
contributing high levels of bacteria to the final product water. According to Taylor et al.,
52
(1979) carbon filters in point-of-use devices resulted in a one to two log increase of
bacterial concentrations over those found in public tap water samples. Wallis et al.,
(1974) warned against the incorporation of charcoal filters into water systems after
observing that bacterial densities increased in treated (chlorinated) waters following an
overnight period of non-use. In the WVM, initial counts of HPC are low, but can
increase rapidly if there is inadequate cleaning of the carbon filters, RO-membrane, or
ultraviolet lamp (Hunter, 1994). Payment et al., (1991) found that water treated by
reverse osmosis units may produce an increase in the HPC bacterial counts of
approximately 1,000 to 10,000 CFU/mL in the product water.
The microbial quality of water produced by point-of-use devices is extremely
variable, being a function of the contamination of the water, the service life of the filter,
water temperature, and the frequency of static water conditions (Geldreich, 1989). In
England, Hunter and Burge, (1986) conducted a study on the bacteriological quality of
water and soft drinks from automatic vending machines and showed that 44% of 25
drinking water samples and 6% of the soft drinks contained coliforms and 84% and 39%
had HPC bacterial levels greater than 1,000 organisms per mL, respectively. Automatic
vending machines are described as units that dispense water or soft drinks into disposable
cups. Some machines contain water filtration system to improve the taste of the product
water (Hunter, 1992). The presence of coliforms should not be ignored because these
bacteria are consistently present in high numbers in feces (human and wildlife) and are a
significant warning of a potential risk for pathogen exposure from a contaminated water
53
source (Geldreich. 1996).
To our knowledge no previous bacteriological studies have been conducted on
water vending machines. The purpose of the study was to determine the occurrence P.
aeruginosa, total and fecal coliforms, and HPC bacteria in WVM product water, and their
correlation to each other in the WVM product water. Others factors such as pH,
temperature, chlorine, and turbidity were measured and correlated with the presence these
of bacteria, and are also reported here.
Materials and Methods
Thirty water samples were collected from WVM, three of which were sampled for
three consecutive weeks. Locations throughout the Tucson area were selected with the
majority of these outside (against the entrance side of the building) of supermarkets.
Water samples were collected in sterile one-liter plastic bottles containing 2 mL of sterile
10% sodium thiosulfate to neutralize any residual chlorine. To ensure that the samples
were representative of the water consumed, the outer surface of the WVMs' nozzle were
not sanitized. The samples were transported refrigerated to the laboratory for processing
within one hour. Biofilms were observed in some of the machines outer nozzle and drain.
Therefore, biofilm samples were collected from the nozzle and drain of fifteen WVM.
Sterile cotton swabs were used to collect biofilm samples and placed in 2 mL of sterile
universal neutralizer (polysorbate 80, 0.3%, sodium thiosulfate, 0.5%. L-histidine, 0.1%,
and phosphate buffer, 0.25N) for transport to the laboratory, according to The Official
54
Methods of Analysis of the Association of Official Analytical Chemist (1984).
P. aeruginosa, total and fecal coliforms in water samples were enumerated by the
membrane filtration method, according to the Standard Methods for the Examination of
Water and Wastewater (1992) (0.45 um, Gelman Science, Ann Arbor, MI), using
Pseudomonas agar base (Oxoid, Hampshire, England), m-Endo, and m-FC agar (Difco
laboratories, Detroit, MI), respectively. P. aeruginosa samples were incubated a 37°C for
24 h; total and fecal coliforms were incubated at 37°C and 44.5°C for 24 h, respectively.
HPC bacteria were enumerated by the spread plate method using R2A agar (Difco
laboratories), and incubation at 25°C for 7 days, according to the Standard Methods for
the Examination of Water and Wastewater (1992). Presumptive identification of P.
aerugin osa was based on the production of green pigmentation, a positive oxidase test,
the ability to grow at 42°C and 4°C, and the ability to oxidize dextrose. Confirmation was
conducted using the API2OE system (Biomurex Vitek, Hazelwood, MO). Confirmation
of total and fecal coliform bacteria were conducted using the Colilert test (IDEXX,
Westbrook, ME).
Biofilm swab samples from drain and nozzle sites were placed in sterile universal
neutralizer, vortexed and immediately plated on m-Endo, m-FC, and R2A agar for the
detection of total coliforms, fecal coliforms, and HPC bacteria, respectively. The Colilert
test was utilized to assess the presence of total coliforms and Escherichia coll. The
approximate sampled area for nozzle and drain surfaces was 3 and 20 cm 2 , respectively.
Factors such as pH, temperature, turbidity, and residual chlorine that may
55
influence the quality of the water dispensed by the VvvVM were also measured. These
procedures were performed according to Standard Methods for the Examination of Water
and Wastewater (1992).
Finally, the relationship between physico-chemical and bacteriological parameters
were analyzed by regression analysis using STAT101 computer software (1993).
Results
Microbiological analyses
Bacteriological results of water samples from 30 WVM are shown in Table 1. P.
aeruginosa was found in 23% of the samples and total coliforms in 20%. HPC bacteria
were found in all samples with 73% having numbers greater than 500 organisms per mL.
The percentage of samples that were positive are shown in Figure 1. During three
consecutive weeks, three WVM were concurrently tested. P. aeruginosa was present in
most of the samples except one (Table 2). Total coliforms were found in only one
sample. Concentrations of HPC bacteria varied with 50% of the samples containing
greater than 500 CFU/mL. The results from the nozzle swab test are shown in Table 3.
Total coliforms were not detected using either m-Endo agar or the Colilert test in the
nozzle samples. HPC concentrations varied from 9 to 48,000 CFU/ sampled area.
Total and fecal coliforms were detected in the drain biofilms using Colilert test

56
and m-Endo agar in ten of the fifteen samples (Table 4). HPC counts were found to
range from 1,000 to 56.000 CFU/sampled area.
Physical and Chemical analyses
The maximum and minimum levels of physico-chemical parameters of 30 WVM
are shown in Table 5. The temperature of the WVM water samples varied from 25 to
32°C. This variation may have been due to location of the WVM as some were exposed
directly to sunlight whereas others were located in shaded areas and the product water
remained at a lower temperature. The pH range was between 6.0 and 7.4, with no
obvious explanation for such variation. Turbidity varied from 0.15 to 3.00 NTU. Such
variation might be explained by the presence of dust and biofilm in some of the WVMs'
nozzles; however, further studies are required to elucidate the source of turbidity in the
water. Finally, total and free chlorine was absent in all of the machines except one,
which contained 0.07 mg/L of free chlorine.
Analysis by regression method
Regression analysis revealed that there were no statistical correlation between
physico-chemical and microbiological parameters (p<0.05) (STAT computer software
1993).
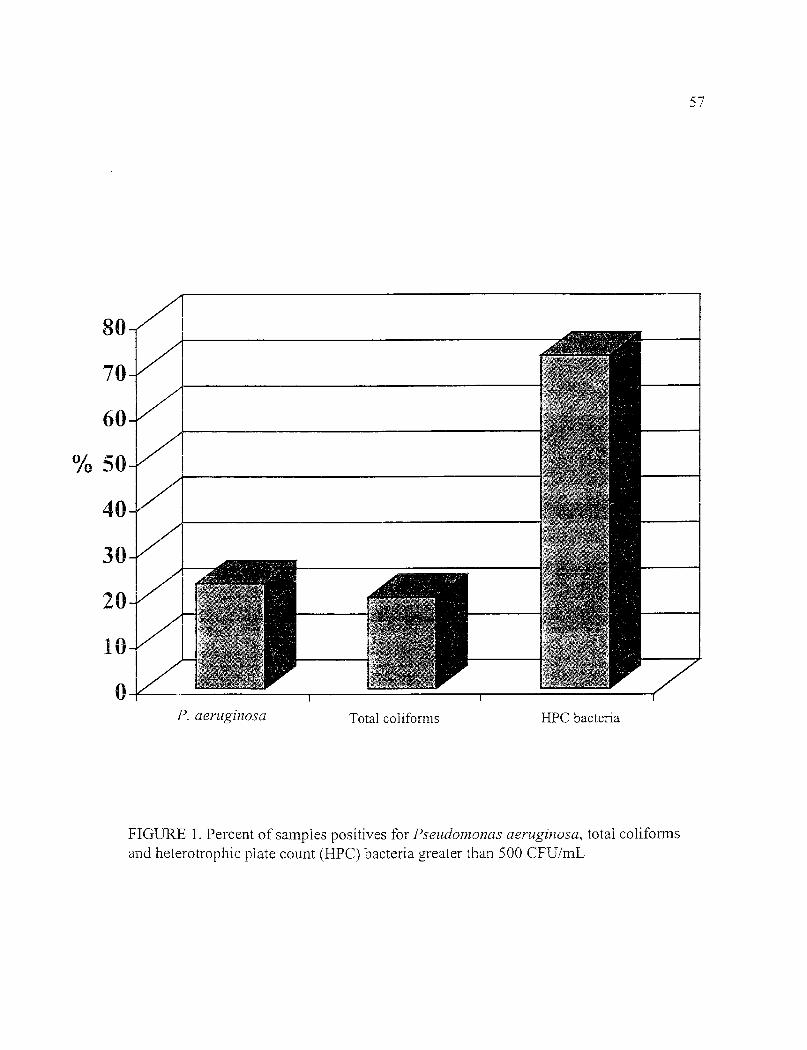
P. aeruginosa Total coliforms HPC bacteria
20
10
57
FIGURE 1. Percent of samples positives for Pseudoznonas aerzzginosa, total coliformsand heterotrophic plate count (HPC) bacteria greater than 500 CFU/mL

TABLE 1. Bacteriological quality of water from vending machines
Vending machine P. aeruginosce Total coliformsb HPC bacteria'
1 0 0 4,0001 25 0 6,5003 0 0 3104 0 0 1,3005 7 0 4,0006 0 0 1,3007 0 2 2,1008 0 0 1,3009 0 3 1,80010 0 5 1,80011 0 3 2012 0 0 L00013 0 0 3,00014 0 0 2,00015 0 0 13016 21 0 8,60017 0 0 20018 0 0 3,00019 0 0 80/0 0 0 81021 0 3 6,00022 22 0 5,20023 0 0 8,00024 2 0 <1025 79 0 6,00026 0 1 35027 0 0 1,00028 0 0 2029 0 0 5,20030 2 0 1,000
' CFU/500mLb CFU/100mL
CFU/mL
58
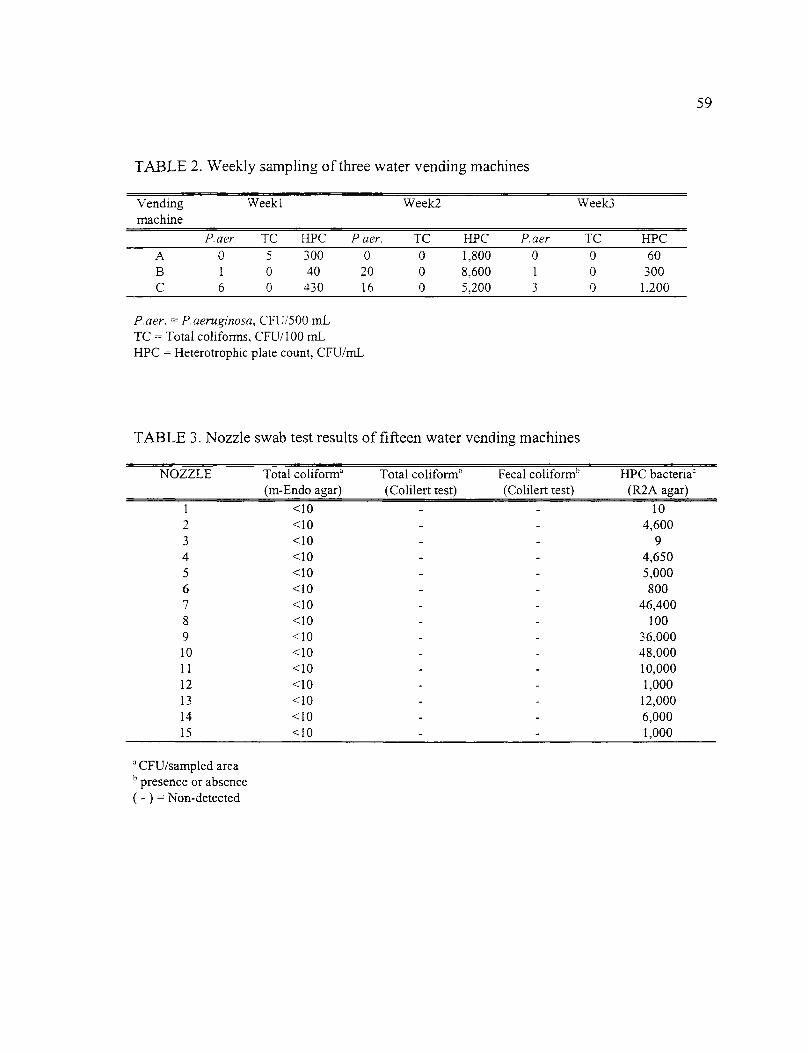
TABLE 2. Weekly sampling of three water vending machines
Vendingmachine
Weekl Weelc2 Week3
P.aer. TC HPC P. aer. IC HPC P. aer TC HPCA 0 5 300 0 0 1,800 0 0 60B 1 0 40 20 0 8,600 1 0 300C 6 0 430 16 0 5,200 3 0 1,200
P. aer. = P. aeruginosa, CFU/500 m.LIC = Total coliforms, CFU/100 mLHPC = Heterotrophic plate count, CFU/mL
TABLE 3. Nozzle swab test results of fifteen water vending machines
NOZZLE Total coliforma Total coliformb Fecal coliformb
(m-Endo agar) (Colilert test) (Colilert test)HPC bacteria'
(R2A agar)
1 <10 102 <10 4,6003 <10 94 <10 4,6505 <10 5,0006 <10 8007 <10 46,4008 <10 1009 <10 36,00010 <10 48,00011 <10 10,00012 <10 1,00013 <10 12,00014 <10 6,00015 <10 1,000
CFU/sampled areapresence or absence
( - ) = Non-detected
59

60
TABLE 4. Drain swab test results of fifteen water vending machines
DRAIN Total conform'(m-Endo agar)
Total conform'(Colilert test)
Fecal conform'(Colilert test)
HPC bacteria'(R2A agar)
1 10 — — 3,9002 500 4_ 4,2503 20 + 2,8004 <10 _ 4,3505 6,000 + 4,6506 120 + 56,0007 2,800 + + 36,0008 <10 6,0009 8,000 + 480,00010 3,000 + 400,00011 1.000 — 480,00012 10 + + 32,00013 <10 - 16,00014 <10 1,60015 <10 1,000
CFU/sampled areab presence or absence
CFU/sampled area( + ) = Detected( - ) = Non-detected

61
TABLE 5. Maximum and minimum values for the physico-chemical parameters inanalyzed water from vending machines
Conditions
Maximum MinimumResidual chlorine (mg/L) 0.07 0pH 7.4 6.0Temperature (°C) 32 25Turbidity (NTU) 3.00 0.08
Discussion
The WVM tested in the Tucson area use ultraviolet light to disinfect the dispensed
water. However, this study demonstrates that high numbers of bacteria may colonize the
product water. This may be partially explained by the fact that U.V. treatment leaves no
residual in the water. The EPA recommends that HPC bacteria should not exceed 500
CFU/mL in drinking water in order to reduce interference with the detection of coliform
bacteria and as a general measure of water quality (Bitton, 1994). The findings in this
study indicate that 73% of water samples from WVM did not meet that recommendation
(Figure 1). These results coincide with those found by Hunter and Burge, (1986) in their
study on the bacteriological quality of water and soft drinks from automatic vending
machines, in which HPC bacteria concentrations greater than 1,000 CFU/mL were found
in 84% and 39% of the product samples respectively.
Total coliforms are often used as indicator organisms of the presence of human
and animal feces although, some species occur naturally in the aquatic environment,
62
being common to soil and vegetation (Geldreich, 1996). Total coliform bacteria have
also been found in insects (Burgess et al., 1973). However, the presence of total
coliforms is a significant warning of a potential risk for pathogens from a contaminated
water source. Their presence should never be ignored (Mack, 1977). In this study, 20%
of the product water contained total coliforms (Figure 1). These findings are similar to a
study done by Levesque et al., (1994) in which coliforms were detected in 30% of water
samples from water coolers located in residences and workplaces.
P. aeruginosa is an important opportunistic pathogen and agent of nosocomial
disease. Hoadley, (1977) identified in his study that P. aeruginosa is a potential hazard
in water, but the occurrence of this microorganism is usually low, especially in treated
(chlorinated) drinking water (3.7%). Similarly, Edberg et al., (1996) found that only 2 to
3% of drinking water samples (bottled water, water coolers units, and tap water)
contained P. aeruginosa. Levesque et al., (1994) did not detect P. aeruginosa in water
cooler samples. In contrast, P. aeruginosa was found in 23% of the WVM water samples
in our study (Figure 1). P. aeruginosa was detected in 2 of 3 WVM's during three
consecutive weeks (Table 2), indicating that colonization is not transient (Geldreich,
1996). This may be due to the ability of P. aeruginosa to form biofilms in water pipes
(Brown and Gauthier, 1993). The nutritional versatility of P. aeruginosa enables it to
grow using trace nutrients present either in the water or attached to the carbon filters
(Tamagini and Gonzalez, 1997). Larger numbers are required (>1.5x106 CPU) to

63
colonize the respiratory tract of healthy individuals (Buck and Cooke, 1969), and
colonization by P. aeruginosa is a presage of disease (Pollack. 1990). However, the
probability of infection to healthy individuals is very low (Rusin et al., 1997).
The results obtained from nozzle and drain biofilm samples indicate that
contamination of these sites could play an important role in the quality of the water from
these machines. Previous studies (Levesque et al., 1994), showed that nozzles of water
coolers were colonized by total coliforms and fecal coliforms 44 and 20% of the time,
respectively. Neither total nor fecal coliforms were detected in the WVM nozzles in this
study (Table 3). However, only a limited number of nozzles were sampled. Numerous
HPC bacteria were found in the nozzle biofilm scrapings, which were consistent with
high numbers found in many of the product water samples. The numbers of HPC bacteria
in the drain biofilm (Table 4) were higher than those found in the nozzle. In addition, 10
of the 15 samples were positive for both total and fecal coliforms in the latter case.
Kneller et al., (1990) conducted a study done on the drain of automatic vending machines
and showed HPC counts ranging from 8 to 10 6 CFU/sampled area, and also reported the
isolation of E. coui from 23% of the samples.
The bacterial biofilm population in the present study may be due to inappropriate
cleaning and/or contamination of the nozzle area by consumers. Hunter and Burge,
(1986) indicated that inadequate cleaning of vending machines dispensing soft drinks and
drinking water may result in biofilm formation contributing to the bacterial population in
the water samples. The biofilm formation may also be exacerbated by the exposure of the

64
drain to fomites (i.e. containers used by the consumer to collect the water from the
vending machines) transmitting bacteria that may proliferate on the moist surfaces.
Burgess et al., (1972) mentioned that coliforms may be carried to the drain surfaces via
insects (cockroaches and flies), and demonstrated that E. coli is harbored and transmitted
by cockroaches. Khalil et al., (1994) showed that flies also serves as reservoir of E. cou.
Cockroaches also have been shown to carry P. aeruginosa and to excrete the organism in
high numbers (Fotedar et al., 1993). The presence of coliforms in the drain area might not
pose a risk to the WVM product water, however, inadequate cleaning practices by trained
personnel may increase the risk of contamination of the WVM product water (Hunter,
1992).
The question remains whether any of these findings have any relevance to public
health. The authors' knowledge there has not been an outbreak of disease linked to
WVM product water. However, there have been no studies that have attempted to
identify any adverse effects.
In conclusion, these results indicate that one should be aware of the
microbiological quality of the water dispensed from the WVM. Although the WVM is
well-designed and poses effective treatment for the water dispensed (reverse osmosis,
carbon filters, and UV light), the manufacturer should be aware of the need for regular
maintenance of the WVM and emphasize the importance of controlling bacterial growth
in such units.

65
References to Appendix 1
American Public Health Association. 1992. Standard Methods for the Examination ofWater and Wastewater. 18' ed. Washington, DC. American Public Health Association.
Bitton, G. 1994. Microbiological Aspects of Drinking Water Treatment and Distribution.p. 261-292. In Wiley-Liss, (ed.) Wastewater Microbiology. New York, NY.
Brown, L.M. and J.J. Gautheir. 1993. Testing of home use carbon filters. J. Amer. WaterWorks Assoc. 71:577-579.
Burgess, N.R.H., Mcdermott, S.N. and J. Whiting. 1973. Laboratory transmission ofenterobacteriaceae by the oriental cockroach, Blatta orientalis. J. Hyg. 71:9-14.
Edberg, S.C., Gallo, P. and C. Kontnick. 1996. Analysis of the virulence characteristicsof bacteria isolated from bottled water, and tap water. Microbial Ecol. Hlth. Dis. 9:67-77.
Favero, M.S, Carson, L.A., Bond, W.W. and N.J. Petersen. 1971. Pseudomonasaeruginosa: growth in distilled water from hospitals. Science. 173:836-838.
Fotedar, R., Banerjee, U. and Shriniwas. 1993. Vector potential of the German cockroachin dissemination of Pseudomonas aeruginosa. J. Hosp. Infect. 23:55-59.
Geldreich, E.E. 1996. Creating microbial quality in drinking water. p 80-90. In CRC (ed.)Microbial Quality of Water Supply in Distribution Systems. Boca Raton, FL.
Geldreich, E.E. 1989. Drinking water microbiology-new directions toward water qualityenhancement. hit. J. Food Microbiol. 9:295-312.
Gelt, J. 1996. Consumers increasingly use bottled water, home water system, watervending machines to avoid direct tap water. Arroyo. 9:1-12.
Hoadley, A.W. 1977. Potentially health hazards associated with Pseudomonasaeruginosa. p. 80-114. In Hoadley and Dutka (ed.) American Society for Testing andMaterials.
Hunter, P.R. 1994. The microbiology of drinks' vending machines. Microbiol. Europe.2:8-10.

66
Hunter, P.R. 1992. Bacteriological, hygienic, and public health aspects of food and drinkfrom vending machines. Critical Rev. Environ. Control. 22:151-167.
Hunter, P.R. and S.H. Burge. 1986. Bacteriological quality of drinks from vendingmachines. J. Hyg. Camb. 97:497-500.
Khalil, K., Lindblom, G.B., Mazhae, K. and B. Kaijser. 1994. Flies and water asreservoirs for bacterial enteropathogens in urban and rural areas in and around Lahore,Pakistan. Epidemiol. Infect. 133:435-444.
Kneller, P.B., Jayasawal, R.K. and L.M. Eils. 1990. Sanitation control for cold cup softdrink vending machines . Diary Food Environ. Sanitation. 10:449.
Levesque, B., Simard, P., Gauvin. D., Gringas, S., Dewally, E. and R. Letarte. 1994.Comparison of the microbiological quality of the water coolers and that of municipalwater systems. Appl. Environ. Microbiol. 60:1174-1178.
Lynkins, B.W., Clark, R.M. and J.A. Goodrich. 1992. Point-Of-Use/Point-Of-Entry forDrinking Water Treatment. Lewis, eds. Chelsea, MI.
Mack, W.N. 1977. Total Coliform Bacteria. Bacterial Indicators/health hazards associatedwith water. p. 59-64. In Hoadley and B.J. Dutka, (ed.) American Society for Testing andMaterials.
McFeters, G.A. 1990. Microbiology of drinking water distribution. p. 40-45. In SpringerVerlag (ed.) Drinking Water Microbiology. New York, NY.
Murray, P.R., Baron, E.J., Pfaller, M.A., Tenover, F.C. and R.H. Yolken. 1995.Pseudomonas and Burkhordelia. p. 510-511. In ASM press (ed.) Manual of ClinicalMicrobiology. Washington DC.
Payment, P., Franco, E., Richardson, L and J. Siemiatycki. 1991. Gastrointestinal healtheffects associated with the consumption of drinking water produced by point-of-usedomestic reverse osmosis filtration units. Appl. Environ. Microbiol. 57:945-948.
Rusin, P.A., Rose, J.B., Haas, C.H. and C.P. Gerba. 1997. Risk assessment ofopportunistic bacterial pathogens in drinking water. Rev. Environ. Contam. Toxicol.152:57-83.
Shooter, R.A., Cooke, E.M., Gaya, H., Kumar, P., Patel, M.T., Thom, B.T. and D.R.France. 1969. Food and medicaments as possible sources of hospital strains ofPseudomonas aeruginosa. LANCET. 1:1221-1229.

67
Statistics Software for Today's Students. Release 1.1. Copyright 1993. log Minitab Inc.
Tamagini, L.M. and R.D. Gonzalez. 1997. Bacteriological stability and growth kinetics ofP. aeruginosa in bottled water. J. Appl. Microbiol. 83:91-94.
Taylor, R.H., Allen, M.J. and E.E. Geldreich. 1979. Testing home use carbon filters. J.Amer. Water Works Assoc. 71:577-579.
The Official Methods of Analysis of the Association of Official Analytical Chemist. 14 th
ed. (1984).
Wallis, C., Stagg, H. and J.L. Melnick. 1974. The hazards of incorporating charcoalfilters into domestic water systems. Wat. Res. 8:111-113.

APPENDIX 2:
MICROBIOLOGICAL SURVEY OF PRIVATE ROOF WATER TANKS INCULIACAN, MEXICO
Cristobal Chaidez Quiroz l* , Aurora Candi12 , and Charles P. Gerba'
Department of Nutritional Sciences', Facultad de Ciencias Quimico-Biologicas', andDepartment of Soil, Water and Environmental Sciences'.
Universidad Autonoma de Sinaloa, MexicoThe University of Arizona, Tucson, AZ 85721
68
*Corresponding author

Abstract
A survey was conducted in Culiacan, Mexico on the water quality of private roof
water tanks (PRWT). In Culiacan, the house water connection is provided to nearly
100% of the urban population; however, the scarcity of water, especially in the summer,
obligates the water authority to ration potable water. As a result, people store water from
the public distribution system in PRWT. Little is known about the microbiological water
quality of the PRWT therefore, this study assessed the quality of the water after storage in
PRWT. Heterotrophic bacteria, total and fecal coliforms, Pseudomonas aeruginosa,
enteroviruses, and protozoa (Cryptosporidium and Giardia) were enumerated. Physico-
chemical parameters such as pH, temperature, turbidity, and residual chlorine were also
examined. P. aeruginosa was found in 28% of the samples; 32% also contained total
coliforms, and 20% Escherichia co/i. Heterotrophic plate count (HPC) bacteria were
found in all of the samples with numbers between 10 2 and 10 5 CFU/mL. No enteroviruses
or protozoan parasites were detected suggesting adequate protection from human or large
animal contamination. Inappropriate cleaning of the private roof water tanks may
account for high levels of bacteria.
69

Introduction
The purpose of a water supply distribution system is to deliver safe drinking water
that is adequate in quantity and acceptable in terms of taste, odor, and appearance (WHO,
1993). The Water supply released into the distribution system becomes altered during its
passage through pipes , open reservoirs, standpipes, and storage tanks (Geldreich, 1996).
Every effort should be made to achieve a drinking water quality as high as
practicable. Failure to do so exposes the population to waterborne diseases. Those at
greatest risk are the very old, the very young, and patients in hospitals (burn and
immunosuppressed patients) (WHO, 1993). Risk of disease must be controlled at the
community level by provision of uncontaminated water and basic sanitation (Ford and
Colwell, 1996). In developing countries, fast growing populations combined with poor
living conditions in rural areas have forced many people to migrate to cities in search of
better living conditions (Mintz et al., 1995). Urbanization affects water availability and
quality, this growing demand for urban water has placed much emphasis on storing water
from the public distribution system into private water storage tanks (PWST).
In Mexico, tap water is stored in private roof water tanks (PRWT) as a backup for
household use, including bathing, cooking, and drinking purposes. In Culiacan, Mexico,
the water distribution system reaches almost 100% of the urban population. However,
because of the intermittent delivery during summer, nearly all households store water in
70

71
PRWT. The urban population of Culiacan reaches almost 700,000 inhabitants (INTEGI,
census 1990). A study was conducted on the microbiological quality of the municipal
reservoirs and distribution system and showed that potable water in Culiacan is of
satisfactory quality (Candil et al., 1990). However, that study did not cover the bacterial
quality of water stored in PRWT. Storing water may contribute dramatically to the water
quality deterioration due to water stagnation (Mintz et al., 1995). Municipal water has
been shown to be further contaminated when the water is stored at home (Myo Han et al.,
1989). In Peru a study was conducted in which fecal coliform counts from water
household's storage containers were 10-fold higher than levels in the tap from which they
had been drawn, indicating that water was being contaminated further during storage
(Swerdlow et al., 1992). A sanitary survey was conducted in drinking water reservoirs
from Jordan, and 20% were contaminated with E. coli (Rabi and Abo-Shehada, 1995).
Reservoirs should be covered to avoid contamination of the supply with bird excrement
and surface run-off. Birds may be infected with intestinal pathogens such as Salmonella
and E. coli which may be pathogenic to man (Geldreich, 1996).
Organic and inorganic suspended particles may protect microorganisms from
disinfectants and may provide a suitable substratum for bacterial proliferation (Schreiber
and Schoenen, 1994), which could result in a colonization of the stored water (Silverman
et al., 1993). In many developing countries, municipal water is unsafe because of
inadequately maintained pipes, low pressure, intermittent delivery, and clandestine
connections (Ford and Colwell, 1996), implying possible consequences to the
79
microbiological quality of the drinking water itself. The risk of diarrheal disease due to
contamination of drinking water during household storage was noted in surveys
conducted by the World Health Organization (WHO) in the 1960s (Van Zilj, 1996).
Since PRWT are widely used and few studies on the microbiological quality have
been conducted, the objectives of the study were to determine the sanitary condition of
the PRWT in Culiacan, and to determine the types of microorganisms (bacteria, parasites,
and enteroviruses) colonizing them.
Materials and Methods
Sample collection
Drinking water samples from storage tanks were collected in the city of Culiacan,
Mexico. Residences located within the urban area were chosen as the only criteria to
participate in the study. Water in Culiacan is obtained from wells along the river shore
extracted by a pumping system to be stored in five municipal reservoirs. Public access is
strictly prohibited, and run off is channeled away from the reservoirs. Water is treated by
conventional processes that include flocculation, sedimentation, filtration, and
chlorination. For sampling purposes, the city was divided into five sectors and
randomized sampling was carried out in each of the sectors. For each sector, five
representative houses were chosen to obtain a total of 25 water samples for bacteria
analyses and 5 samples for virus and parasite analyses.

73
Roof water tanks made of concrete or polyvinyl chloride (PVC), and had a
capacity of 300 to 500 L. Tanks are usually covered and constructed with an inlet and
outlet pipe, floating valve, and drainage pipe. Water is drawn from the main water supply
source provided to the house. The stored water serves as a reserve water source when
interruptions to the municipal system occur.
Bacteriological analyses
Water samples were collected in sterile one-liter plastic bottles containing 2mL of
10% sodium thiosulfate to neutrilize any residual chlorine. Water samples were placed
on ice and analyzed within 2 to 3 h after sampling. All bacteriological analyses were
carried out according to the Standard Method for the Examination of Water and
Wastewater (APHA, 1995). Pseudomonas aeruginosa and total and fecal coliforms were
enumerated by the membrane filtration method (0.45 1.tm, Gelman Science, Ann Arbor,
MI) using Pseudomonas agar base (Oxoid, Hampshire, England), m-Endo and mFC agar
(Difco laboratories, Detroit. MI), respectively. P. aeruginosa samples were incubated at
37°C for 36 h. total and fecal coliforms were incubated at 37°C and 44.5°C for 24 h,
respectively. The heterotrophic plate count (HPC) bacteria were enumerated by the
spread plate method using R2A agar (Difco laboratories), and incubated at 25°C for seven
days. Identi fi cation of P. aeruginosa and coliform bacteria were conducted by the
API2OE system (Biomurex Vitek, Hazelwood, MO).
Virological and parasitological analyses
Storage water samples were analyzed for the presence of human enteroviruses and
Giardia cysts and Cryptosporidium oocysts, according to the Standard Method for the
Examination of Water and Wastewater (APHA, 1995). For viruses, a volume of 378 L
(100 gallons) of stored water was concentrated by passage through a MK filter (Zeta plus,
CUNO, Meriden, CT). The filter was eluted with 900 mL of 1.5% beef extract V (Becton
Dickinson, Cockeysville, MD), buffered with 0.05 M glycine, pH 9.5 (Ma et al., 1994).
Reconcentration of the eluate was via flocculation (Katzenelson et al., 1976). The eluate
was resuspended on 0.1M NaJIPO 4 , and adjusted to pH 7.2-7.3 with 1N HC1 and 1N
NaOH. Concentrates were treated with Freon 113 to reduce toxicity and assayed on the
BGM cell line. The cells were cultivated on minimal essential medium (MEM)
supplemented with 10% fetal calf serum in 75 cm2 tissue culture flasks. The flasks were
incubated at 37°C for 7-10 days before being frozen at -20°C and small amount of
supernatant fluid from each flask was transferred to a new monolayer of BGM cells.
There were observed for 10-14 days for the development of viral cytopatic effect (CPE).
For parasite samples, the same volume was processed (378 L), by passing it
through yarn-wound polypropylene cartridge filters (CUNO, Meriden, CT). The filters
were cut in half, teased and washed in a 1% Tween 80 solution. Eluents were
reconcentrated by centrifugation, and purified by sucrose-Percoll flotation (Sigma
-74
75
Chemical, St. Louis. MO), collected on membrane filters and analyzed for Giardia cysts
and CiTyptosporidium oocysts by immunofluorescence using specific mouse monoclonal
antibodies (Meridian, Cincinnati. OH), and subsequently stained with goat anti-mouse
antibodies conjugated to a fluorescent dye (Kyrkegaard and Perry Laboratories Inc.,
Gaithersburg,, MD). Membranes were mounted on glass slides, and examined with the
aid of an epifluorescence microscope. The cysts and oocyts were identified by their size,
shape, and green fluorescence around the walls, and confirmed by observation for internal
structures by differential phase contrast microspcopy (Rose et al., 1988).
Physico-chemical analyses
Physico-chemical analyses were performed according to the Standard Method for
the Examination of Water and Wastewater (APHA, 1995). The pH, temperature,
turbidity, and residual chlorine were determined. A database was prepared using the
Excel 4.0 computer program software. Regression analyses were performed on physico-
chemical and microbiological parameters.
Results
Bacteriological results are summarized in Table 1. P. aeruginosa was found in
28% of the samples, total and fecal coliforms in 32% and 20% , respectively (Figure 1).
76
HPC bacteria were found in all of the samples with numbers between 10 : and 10'
CR.,7mL. P. aeruginosa isolates were confirmed by the API2ONE system (Biomurex),
and selected colonies for m-Endo were confirmed by the API2OE system (Biomurex).
The predominant coliform bacteria were E. coui and Serratia marcencens. Enteroviruses,
Giardia cysts, and Cryptosporidium oocysts were not detected in the water obtained from
any PRWT.
Results of physico-chemical parameters are summarized in Table 3. The
temperature of the water varied from 17 to 35°C. An explanation of such variation may
be the different types of roof storage tanks tested (concrete and PVC), some roof tanks
tested were also protected from the sunlight by trees and therefore the water remained at
lower temperatures. The pH ranged from between 6.9 and 9.5. Such variation is
probably influenced by the materials used in construction. Turbidity varied from 0.38 to
135 NTU, such variation might be due to dust and biofilm accumulation in the storage
tank, and some tanks also had broken or unfitted covers allowing the accumulation of
large particles. Total and free chlorine were present in all of the samples with values
from 0.1 to 4.5 and from 0.1 to 4 mg/L, respectively.
Regression analyses revealed that there were no statistical significance among physico-
chemical and microbiological parameters (P<0.05).

0 % of samples positive
77
P. aerziginosa
Total conforms Fecal coliforms HPC bacteria
FIGURE 1. Percentage of samples positive for Pseudomonas aeruginosa (CFU/100 mL),total and fecal coliforms (CFU/100 mL) and heterotrophic plate count (HPC) bacteria(>500 CFU/mL)

TABLE 1. Bacteriological quality of water from household roof tanks
Roof tank P. aeruginosaCFU/100mL
Total coliformsCFU/100mL
Fecal coliformsCFU/100mL
HPC bacteriaCFU/mL
Zone-A1 0 1 l) 625007 0 7 0 195003 0 0 0 725004 100 1 1 2240005 3 0 0 17000
Zone-B1 ') 0 0 500000) 0 20 20 2000003 10 10 10 2180004 3 0 0 4000005 5 120 0 6300
Zone-C1 0 0 0 230002 0 0 0 200003 0 0 0 12504 0 0 0 1420005 0 0 0 1550
Zone-D1 0 0 0 3000-,- 1 0 0 1520003 0 15 15 1000004 0 0 0 3020005 0 15 3 6000
Zone-E1 0 0 0 27107 0 0 0 5603 0 0 0 88004 0 0 0 80005 0 0 0 2500
78
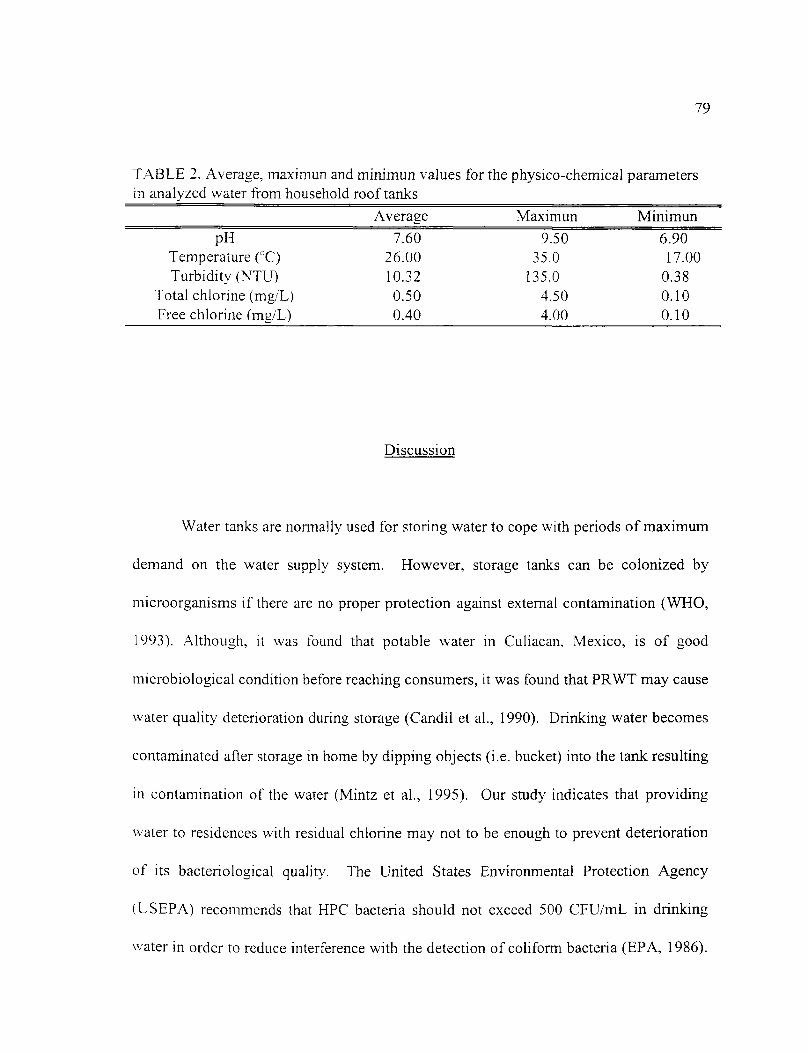
79
TABLE 2. Average, maximun and minimun values for the physico-chemical parametersin analyzed water from household roof tanks
Average Maximun Minimun
pH 7.60 9.50 6.90Temperature (°C) 26.00 35.0 17.00Turbidity (NTU) 10.32 135.0 0.38
Total chlorine (mg/L) 0.50 4.50 0.10Free chlorine (mg/L) 0.40 4.00 0.10
Discussion
Water tanks are normally used for storing water to cope with periods of maximum
demand on the water supply system. However, storage tanks can be colonized by
microorganisms if there are no proper protection against external contamination (WHO,
1993). Although, it was found that potable water in Culiacan, Mexico, is of good
microbiological condition before reaching consumers, it was found that PRWT may cause
water quality deterioration during storage (Candil et al., 1990). Drinking water becomes
contaminated after storage in home by dipping objects (i.e. bucket) into the tank resulting
in contamination of the water (Mintz et al., 1995). Our study indicates that providing
water to residences with residual chlorine may not to be enough to prevent deterioration
of its bacteriological quality. The United States Environmental Protection Agency
(USEPA) recommends that HPC bacteria should not exceed 500 CFU/mL in drinking
water in order to reduce interference with the detection of coliform bacteria (EPA, 1986).
80
Higher numbers are often the results of bacterial regrowth. particularly in distribution
systems and storage water containers (Geldreich, 1996). HPC bacteria are capable of
surviving on minimal nutrients, attach to pipe sediments, and participate in the biofilm
formation (Geldreich, 1996). There is a generalized concern regarding the public health
risk of some members of the HPC bacteria (LeChevallier et al., 1985; Payment et al.,
1988). However, health risk with HPC bacteria have not been established.
Sediments in drinking water reservoirs have been evaluated and colony counts of
up to 3x10 5 CF1i/mL using standard plate agar have been reported (Schreiber and
Schoenen, 1994). In our study we did not attempt to analyze the sediments in the
household tanks, however the water itself had between 10 2 and 10 CFU/mL. The purpose
of quantifying indicator organisms is to predict the possible occurrence of specific
pathogens and assess the sanitary quality of the water (Ford and Colwell, 1996). Total
coliforms are often used as indicator organisms for the presence of human and animal
excreta. However, indicator organisms such as E. co/i can grow in the absence of fecal
contamination , and therefore their usefulness is sometimes limited (Rivera et al., 1988).
Some strains are common in soil and vegetation (Geldreich, 1996), and insects may be
carriers of E. coli (Burgess et al., 1973). In this study, 32 and 20% of the water samples
contained total and fecal coliforms, respectively (Figure 1), E. co/i and Serratia
marcescens being the predominant coliform bacteria identified in this study.
Enterobacter cloacae and Citrobacter fretindii were detected in the outlet of open

81
holding reservoirs containing chlorinated water (Paspaliaris and Hodgson, 1994). In Iraq,
a study was conducted on tap water and
storage tanks which found that Enterobacter cloacae and Klebsiella pneumoniae were the
predominant organisms, respectively (Sameer et al., 1988).
P. aerugin osa is the most prevalent pathogen in the genus Pseudomonas. P.
aeruginosa is predominantly a nosocomial pathogen (Pollack, 1990), but it is present in
many environments including swimming pools, whirpools, hot tubs, contact lenses
solutions and other water-related reservoirs (Rusin et al., 1997). In this study, P.
aeruginosa was found in 28% of the water storage tanks (Figure 1). It has also been
isolated from water distribution systems, and 3% of the time in tap water (Geldreich and
Allen, 1975). It is able to form biofilms on several surfaces including PVC and carbon
filters (Geldreich and Allen, 1975). The nutritional versatility of P. aeruginosa enables it
to grow using trace nutrients presents in water (Tamagini and Gonzalez, 1997). The
presence of P. aeruginosa in storage tanks did not coincide with a study in which P.
aeruginosa was present in low numbers (3.7%), especially in chlorinated tap water
(Hoadley, 1977).
The absence of enteroviruses and protozoan parasites suggests that the coliforms
and fecal coliforms are not from human fecal material. It also suggests that the enteric
bacteria which were detected may have originated from birds, other small animals, or
debris that gained access into the tanks. The PRWT examined had covers but only a few
firmly fitted which may contribute to the high contamination level.

82
Our bacteriological results indicate that water from storage tanks in Culiacan,
Mexico, did not meet drinking water standards for bacterial indicators. However, the
health risk associated with the presence of bacteria in the storage tank is probably low as
no human parasite or viral pathogens were detected.
References to Appendix 2:
Allen, M.J. and E.E. Geldreich. 1975. Bacteriological criteria for ground waterquality. Ground Water. 13:45-52.
American Public Health Association. 1995. Standard Methods for the Examination ofWater and Wastewater. le ed. Washington, DC.
Burgess, N.R.H., Mcdermott, S.N., and J. Whiting. 1973. Laboratory transmission ofEnterobacteriaceae by oriental cockroach, Blatta orientalis. J Hyg. 71:9-14.
Candil-Ruiz, A.. Uribe, M., Diaz, S.P., De Leon, R., Naranjo, J., and C.P. Gerba. 1990.Calidad microbiologica del agua de la zona centro de Sinaloa. Sociedad Mexicana deIngieneria Sanitaria Ambiental, A. C. Congreso Nacional. 25-26. Oaxaca, Oax.
Environmental Protection Agency (EPA). 1986. Ambient water quality criteria forbacteria. EPA 44015-84-002. Washington, DC.
Ford, T.E. and R.R. Colwell. 1996. A global decline in microbiological safety of water: acall for action. American Academy of Microbiology. Washington, DC.
Geldreich, E.E. 1996. Microbial Quality of Water Supply in Distribution Systems.Boca Raton, FL.
Hoadley, A.W. Potentially health hazards associated with Pseudomonasaeruginosa, bacterial indicator/health hazards associated with water. American Societyfor Testing and Materials. Hoadley and Dutka (ed.) Atlanta, GA. 1977.

83
Instituto Nacional de Estadistica, Geografia e Infounatica (INEGI). 1990. XI CensoGeneral de Poblacion y Vivienda. Mexico.
Katzenelson, E., Fattal, B., and T. Hostovesky. 1976. Organic flocculation: an efficientsecond-step concentration method for the detection of viruses in tap water. App!. Environ.Microbiol. 32:638-639.
LeChevallier, M.W.. Singh, A., Schiemann, D.A., and G.A. McFeters. 1985. Changes invirulence of waterborne enteropathogens with chlorine injury. App!. Environ. Microbiol.50:412-419.
Ma, J., Naranjo, J., and C.P Gerba. 1994. Evaluation of MK filters for recovery ofenteroviruses from tap water. App!. Environ. Microbiol. 60:1974-1977.
Mintz, E.D., Reiff, E.M., and R.V. Tauxe. 1995. Safe water treatment and storage in thehome: A practical new strategy to prevent waterborne disease. J Amer. Med. Assoc.273:848-953.
Myo Han, A., Nwe 00, K., Midorikawa, Y., and S. Shwe. 1987. Contamination ofdrinking water during collection and storage. Trop. Geograph. Med.. 41:138-140.
Paspaliaris, P. and B. Hodgson. 1994. The role of cypress leaves in promoting growth ofcoliform organisms in holding reservoirs. Wat. Res. 28:2147-2151.
Payment, P., Gamache, F. and G. Paquette. 1988. Microbiological and virologicalanalysis of water from two water filtration plants and their distribution systems. Can. J.Microbiol. 34:1304-1309.
Pollack, M. 1990. Pseudomonas aeruginosa. p. 1673-1687. In Mandell, G.H., DouglasR.G. Jr., Benett, J.E. (ed.) Principles and practice of infectious diseases. Livingstone, NY.
Rabi, A.Z. and M.N. Abo-Shehada. 1995. Sanitary survey of private drinking waterreservoirs in Northern Jordan. Int. J. Environ. Hlth. Res. 5:255-261.
Rivera, S.C., Hazen, T.C. and G.A. Toranzos. 1988. Isolation of fecal coliforms frompristine sites in a tropical rain forest. App!. Environ. Microbiol. 54:513-517.
Rose, J.B., Darbin, H. and C.P. Gerba. 1988. Correlations of the protozoa,Cryptosporidium and Giardia with water quality variables in a watershed. Wat. Sci. Tech.20:271-276.
84
Rusin, P.A., Rose, J.B., Haas, C.H. and C.P Gerba. 1997. Risk assessment ofopportunistic bacterial pathogens in drinking water. Rev. Environ. Con tam. Toxicol.152:57-83.
Sameer, F.J., Zainab, A., Al, D. and T.A. Haddad. 1988. Antibiotic resistance coliformand fecal coliform bacteria in drinking water. Wat. Air Soil Poll. 39:377-382.
Schreiber, H. and D. Schoenen. 1994. Chemical, bacteriological and biologicalexamination and evaluation of sediments from drinking water reservoirs. ZbL Hyg.196:153-169.
Silverman, S., Nagy, L.A. and B.H. Olson. 1983. Variations in particulate matter, algae,and bacteria in uncovered finished drinking water reservoirs. J Amer. Water WorksAssoc. 75:191-195.
Swerdlow, D.L., Mintz, E.D., Rodriguez, M., Tejeda, E., Ocampo, C., Espejo, L.,Greene, K.D., Saldana, W., Seminario, L., Tauxe, R.V., Wells, J.G., Bean, N.H., Ries,A.A., Pollack, M., Vertiz, B. and P.A. Blake. 1992. Waterborne transmission of epidemiccholera in Trujillo, Peru: lessons for a continent at risk. LANCET. 340:28-32.
Tamagini, L.M. and R.D. Gonzalez. 1997. Bacteriological stability and growth kinetics ofP. aeruginosa in bottled water. J. App!. Microbiol. 83:91-94.
Van Zilj, W.J. 1966. Studies on diarrhoea! in seven countries by the WHO diarrhoealdisease study team. Bull. Wld. Organ. 35:249-261.
World Health Organization Guidelines for drinking water quality. 2" d ed. Geneva,Switzerland. 1993.

APPENDIX 3:
MICROBIOLOGICAL COMPARISON OF THE QUALITY OF POINT-OF-USE(POU)-TREATED WATER, TAP WATER, AND BOTTLED WATER
Cristobal Chaidez Quiroe and Charles P. Gerba'
Department of Nutritional Sciences and Department of Soil, Water, and EnvironmentalSciences'.
The University of Arizona, Tucson, AZ. 85721
85
*Corresponding author

86
Abstract
The water quality of point-of-use (POU) water treatment devices, and that of tap
water with POU-connections, tap water, and bottled water were compared. Heterotrophic
plate count (HPC) bacteria, total and fecal coliforms, and acid-fast organisms
(Itlycobacteria spp.) as well as the opportunistic bacterial pathogens Aeromonas
hydrophila, Plesiomonas shigelloides, and Pseudomonas aeruginosa were enumerated.
The highest concentration of bacteria was found in POU-treated water. P. aerziginosa,
acid-fast organisms, and total coliforms were present in 38.5, 43.8, and 82.4% of the
samples, respectively. HPC bacteria were present in all of the POU-treated water
samples, with concentrations ranging from 10 2 to 10 CFU/mL. Neither fecal coliforms
nor P. shigelloides were recovered from any samples. Tap water with a POU-connection
also had higher numbers of bacteria than tap and bottled water samples. It was concluded
that tap and bottled water had lower numbers of A. hydrophila, acid-fast organisms, HPC
bacteria, P. aeruginosa and coliforms than POU-treated water, and tap water with a POU-
connection. The use of POU-devices may amplify the bacteria present in the distribution
system by promoting biofilm formation. Regular maintenance of POU-devices is
recommended to minimize the numbers of bacteria.
87
Introduction
In the past decade there has been a growing concern by public health officials,
regulatory agencies, and the general public about the safety of drinking water supplies
(Geldreich, 1996). A growing segment of the public is convinced that many health risks
may emerge from the water distribution system. An available alternative to this threat is
bottled water, or point-of-use (POU)-treated water (Geldreich, 1996; McFeters, 1990).
In North America, the market for bottled water is large, with an annual growth
rate estimated at 25% in recent years. The consumption of bottled water in the United
States has risen from four gallons per person per year in 1984 to 9.7 gallons per year in
1994. In 1995, Americans bought 2.8 billion gallons of bottled water, and in 1996 they
spent $2 billion on drinking water (Swanson, 1996; Holtzman et al., 1997). Overall, 10
to 15% of the U.S. households drink bottled water on a regular basis (Symons, 1997).
Bottled water is intended to be used as a beverage, however, it has also been
marketed as ideal for infant formula preparation, or nursery drinking water, for use in
reconstituting other foods, for cleaning contact lenses, for skin care, and for humidifiers
(Warburton et al., 1992). Thus, bottled water should be of better microbiological quality
than most foods, especially if intended for use by vulnerable populations (pregnant
women, the infirm, the elderly, and the very young) (Warburton, 1993).
Bottled water may contain bacteria that enters as contaminants, including a wide
range of saprophytic species and human pathogens (Warburton et al., 1993). It has been
88
shown that many shallow and deep aquifiers contain microorganisms, sometimes at levels
as high as 10 5 -10 CFU/mL (Warburton, 1993). Sometimes, bottled water industry uses
potable water as a source water, and indigenous bacteria from the municipal source may
appear in the product water (Warburton, 1993).
The point-of-use (POU) devices industry has experienced a growth increase over
the past years. In the United States, the Water Quality Association has reported that there
are at least 325 manufacturers of POU home water treatment devices. The annual sales in
1990 rose to nearly $1 billion and these products were serving more than 5 million
families nationwide (McFeters, 1990).
Water purifiers are treatment devices designed to remove contaminats from the
water (Lynkins et al., 1992). POU-devices use a wide range of treatments to control
contaminants in drinking water. Treatments include: adsorption, ion-exchange, and
disinfection such as chlorination, ozonation, silver salts, and ultraviolet light. In some
designs, the treatment package consists of several processes in series to achieve better
removal and control of water contaminants (Lynkins et al., 1992; McFeters, 1990).
However, studies have shown that these units can deteriorate the microbial water quality
(Geldreich, 1996). The microbial quality of the water produced by these devices is
influenced by input water flora, service life of the filter, physico-chemical water quality
(i.e. temperature), and frequency of static water conditions (Geldreich et al., 1985).
Amplification of the heterotrophic bacterial population in POU-devices is of concern.
Opportunistic pathogens can be found as part of the heterotrophic plate count (HPC)
89
bacteria in drinking water (Rusin et al., 1997a). Therefore, their growth may threat
vulnerable segments of the population (very young, pregnant women, and
immunocompromised).
A variety of bacteria occur in drinking water by entering during water line repairs,
in open finished water reservoirs, in blackflows from pipelining projects, and new pipe
network (Payment et al., 1997; Geldreich, 1996). Most of these bacteria are not of
immediate public health significance, but some can represent a health risk (Geldreich,
1996). Higher numbers are often the result of bacterial re-growth, particularly in
distribution systems (Geldreich, 1996; Olson and Nagy, 1984), and in water treatment
devices (Geldreich et al., 1985; Payment, 1989; Reasoner et al., 1987; Snyder et al.,
1995). Bacterial densities in water effluents from POU-devices can be expected to
increase by one or two logs over the number detected in water supplies (Taylor et al.,
1979). Wallis et al., (1974) observed that bacterial densities increased in filters devices
after an overnight period of non-use. This proliferation depends on certain conditions
such as seasonal changes, temperature and free chlorine concentration (Geldreich, 1996).
Public water supplies were never intended to provide a sterile product, but to
supply safer drinking water. However, before reaching the consumer, the microbial
quality of potable water is modified in composition through treatment processes,
colonization in the distribution system, and selectively amplification in attachment
devices (Geldreich, 1986). These changes are caused to a large extent by a variety of

90
microbiological activities that occur as water passes through the distribution network
(Bitton, 1994).
Studies on the bacteriological quality of the POU-devices under laboratory
settings have been extensively conducted (Naranjo et al., 1997; Geldreich et al., 1985;
Geldreich and Reasoner, 1989; Tobin et al., 1981). However, field studies are limited.
Previous field studies have been conducted (Snyder et al., 1995), but differentiation and
concentration of selected opportunistic pathogens have not been performed. The
purposes of the study reported here were : 1) to evaluate the microbiological quality of
the water dispensed by POU-devices, tap water with POU-connection tap water, and
bottled water, 2) to compare the quality of each of the drinking water sources, and 3) to
determine the occurrence of selected opportunistic pathogens.
Materials and Methods
Sample collection
Point-of-use (POU) devices were installed in 10 private homes in January of
1998, in Tucson, AZ. The units were connected to the faucet that delivers cold water.
The faucet-mounted units provide an easy access to both filtered and unfiltered (tap)
water by a simply twist from the vertical (filtered water) to the horizontal position
(unfiltered water). Thus, an influent (unfiltered) and an effluent (filtered) water sample

91
were collected from the installed POU-devices. Table 1 describes the general
characteristics of the POU-devices used in this study.
Table 1. General characteristics of point-of-use (POU) devices (faucet mounted units)
Unit Model Filtration system Service life(gallons)
PUR FM-2000 Micron carbon 300PUR FM-2000 Micron-carbon 300PUR FM-2000 Micron-carbon 300PUR FM-2000 Micron-carbon 300PUR FM-2000 Micron-carbon 300
PUR-plus RF-30520 Micron-carbon 1000Teledyne pik FM-1 Carbon 300
Culligan FM-15 Carbon 200Culligan FM-15 Carbon 200
Nordic ware NW-78100 Carbon 500
Sample collection procedures are critical to obtain a representation of water
quality within the POU-device. Therefore, to make sure that the samples were
representative of the water consumed, neither the POU-treated water nor the tap water
were flushed before sampling and there was no attempt to sterilize the outer surface of
both sites. First-draw water samples were collected aseptically in sterile 1-liter plastic
bottles from both POU-device and the tap water. A total of four liters of water were
obtained from each site. Each bottle sample contained 2 mL of sterile sodium thiosulfate
to neutralize any residual chlorine. Samples were stored in a plastic cooler and packed
with ice for transport to the laboratory for immediate processing.

9?
The sampling was carried out over a period of six weeks. Every week a sample
was obtained from both POU-treated water and tap water. Also, samples from other tap
home-owners (without POU-device connection) were obtained to determine if the POU-
device exert an influence on the bacteriological quality of the tap water. Samples were
collected every week to obtain a total of thirty water samples. They were collected in
sterile plastic bottles containing 2 mi, of sterile sodium thiosulfate. Tap water samples
from homes without POU-devices were used as the baseline value.
Bacteriological analysis were conducted on 72 brands of retail bottled water from
7 countries (Costa Rica, Greece, Japan, Korea, Mexico, Panama, and US). Container
sizes ranges from 300 to 3785 mL. The types of water were: distilled, spring, and
purified water. Samples were placed at room temperature before analysis.
Bacteriological analyses
Bacterial analyses were performed on POU-treated water, tap water with POU-
connection, tap water, and bottled water according to the Standard Methods for the
Examination of Water and Wastewater (APHA, 1995), unless otherwise indicated. HPC
bacteria were determined using the spread plate method by placing 0.1 mL of the sample
onto R2A agar plates (Difco Laboratories, Detroit, MI). These plates were incubated at
25°C for 7 days. Membrane (0.45 pm pore size) filtration technique (Gelman Science
Laboratories, Ann Arbor, MI) was used for the enumeration of Aeromonas hydrophila,
acid-fast organisms, Pseudomonas aeruginosa, Plesionzonas shigelloides, and total and
93
fecal coliforms. Five-hundred mL of water samples were used for A. hydrophila, P.
aerugin osa, and P. shigelloides, the membranes (Gelman Sciences Laboratories) were
placed onto Aeromonas agar (Difco Laboratories), Pseudomonas agar (Oxoid
Laboratories, Hampshire, England), and inositol brilliant green bile salts (IBB) agar
(Jeppensen, 1995), respectively. Membranes were incubated at 37°C for 36 h. One-
thousand mL samples were collected for the enumeration of acid-fast organisms. The
membranes were decontaminated with 0.04% of Cetylpiridinium chloride (CPC) for 2h
and placed onto 7H11 agar (Difco Laboratories) at 37°C for four weeks at 5% CO,
environment. One-hundred mL samples were obtained to enumerate total and fecal
coliforms. Membranes were placed onto m-Endo at 37°C and mFc agar at 44.5°C for 24
h, respectively.
API2OE and API2ONE (Biomurex Vitek, Hazelwood, MO) systems were utilized
for the identification of fermentative and non-fermentative bacteria. The acid-fast
(Kinyoun) stain was used for the identification of the acid-fast organisms.
Physico-chemical analyses
Physico-chemical analyses were performed according to the Standard Method for
the Examination of Water and Wastewater (APHA, 1995). Turbidity, pH, temperature
and residual chlorine were monitored in the POU-treated water, tap water with POU-
connection and tap water, and bottled water.
94
Statistical method
Water quality data were analyzed by the Pearson correlation and the linear
regression with the aid EXCEL computer software (Microsoft Co., Redmond, WA).
Results
Results of bacteriological analyses from the POU-treated water, tap water with
POU-connection, tap water, and bottled water are shown in Table 2. The average
concentration of A. hydrophila, P. aeruginosa, and total coliforms are presented in Table
3. The results of the HPC bacteria for POU-treated water, tap water with POU-
connection, tap water, and bottled water are presented in Table 4. Table 5 shows the
identification of selected bacterial isolates from the drinking water sources. Physico-
chemical parameters are summarized in Table 6.
The numbers of HPC bacteria were compared among POU-treated water, tap
water with POU-connection, and tap water (Figure 1). Data were collected over a period
of six weeks. POU-devices were colonized by bacteria shortly after installation, and the
numbers were much higher than those found in tap water with POU-connection and tap
water. P. aeruginosa densities of POU-treated water, tap water with POU-connection,
and tap water are shown on Figure 2. The average number of A. hydrophila was also
compared in Figure 3. The average of total coliforms is summarized and compared in
Figure 4.

95
Correlation and regression analyses were perfolined on bacteriological and
physico-chemical data, however, no significant differences were found.
Discussion
Bacterial colonization of POU-devices occurred shortly after installation. POU-
treated water showed the highest bacterial contamination when compared with other
drinking water sources (Table 2). The average concentration of A. hydrophila was low in
POU-treated water (29.5/mL) (Table 3). This might be due to the fact that A. hydrophila
is not able to grow extensively in nutrient-poor waters, and is not able to compete
efficiently with the heterotrophic bacteria (Holmes et al., 1996). Moreover, it has been
suggested that heterotrophic bacteria might be inhibitory to A. hydrophila (Hunter, 1993).
In contrast, P. aeruginosa and total coliforms were recovered at much higher
concentrations (102 and 139 CFU/mL, respectively) in POU-treated water than other
drinking water sources (Table 3). The explanation of this is that P. aeruginosa and total
coliforms participate in biofilm formation and they are able to co-exist in the biofilm
surfaces (Geldreich, 1996). Geldreich, (1996) mentioned that organisms that reside in
biofilms are expected to be more consistently found in the product water. POU-treated
water had higher concentrations of acid-fast bacilli (based on the acid-fast stain),
followed by tap water with POU-connection, tap water and bottled water (Table 2).
Acid-fast organisms are also able to participate in biofilm formation and have been

96
recovered from chlorinated tap water and bottled water (Bullin et al., 1970; Geldreich,
1996; Caroli et al., 1985).
The greatest concentration of HPC bacteria were found in POU-treated water,
followed by tap water with POU-connection, tap water, and bottled water (Table 4). The
microbial flora of bottled water is altered as water is extracted from the source and passes
through the bottling plant. Warburton et al., (1998) found that 5.5% of the bottled water
tested exceeded 1x104 CFU/mL. The HPC bacteria found in POU-treated water, tap
water with POU-connection and tap water are compared in Figure 1. POU-treated water
and tap water with POU-connection maintained high constant numbers of HPC bacteria
during the six weeks of the sampling. Tap water and bottled water had similar
concentrations of HPC bacteria, indicating that the use of POU-devices may promote the
proliferation of heterotrophic bacteria and might then have had an influence on the water
source (tap water connection). This might be explained by the fact that water filters may
support biofilm formation. These results coincide with those found by Levesque et al.,
(1994), in their study of the bacteriological quality of tap water and water coolers. They
found that the water taken from water coolers were much more contaminated than the tap
water. They suggested that water coolers might affect the microbial quality of the bottled
water obtained from the faucets. In contrast, Snyder et al., (1995) analyzed the
bacteriological quality of 24 domestic ground water supplies treated with powdered
activated carbon filters (POU-PAC). They found that POU-PAC did not have an effect
on the bacteriological quality of drinking obtained from underground sources.
97
Hunter, (1994) states that bottled water must be free of coliforms (0/100 mL) and
P. aeruginosa (0/250 mL). In the current study P. aeruginosa was present in 8.3% and
coliforms in 15.2% of the bottled water tested at concentrations of 0.6 and 4.4 CFU/mL,
respectively (Table 2). A. hydrophda and acid-fast organisms (based on acid-fast stain)
must be absent as well (Geldreich, 1996; Warburton et al., 1994), but they were identified
in 8.7% and 11.4% of the samples, respectively (Table 2). Caroli et al., (1985) reported
the isolation of acid-fast organisms in nine bottle water samples. Slade et al., (1986)
isolated A. hydrophila from 41 of 95 (43%) bottles of mineral water in Saudi Arabia.
Opportunistic bacterial pathogens, total coliforrns, and HPC bacteria were
detected in the bottled waters (Table 2). The results are similar to those reported by
others authors (Edberg et al., 1996; Ogan, 1992; Fewtrell et al., 1997; Gonzalez et al.,
1987; Tsai and Yu, 1997; Hunter, 1994; Manaia et al., 1990; Caroli et al., 1985). Low
numbers of opportunistic pathogens were detected in bottled water, except one sample
obtained from Costa Rica that contained 90 CFIJ/mL of A. hydrophda. Warburton et al.,
(1994) mentioned that this organism is able to survive and proliferate to levels of 1000
CFU/mL in bottled water stored at room temperature. Bacterial contamination can be
attributed to several factors including contamination during bottling and storage
(Geldreich, 1986). Prolonged storage at room and refrigeration temperatures allow
multiplication of bacteria to numbers >1x10 5 (Bischofberger et al., 1990; Geldreich et al.,
1975; Warburton et al., 1992).

98
The presence of P. aeruginosa , A. hydrophila, and total coliforms may indicate
contamination by pollution and human fecal matter, and is an indication of a poor
manufacturing practices (Hoadley, 1977; Warburton et al., 1992).
Overall, opportunistic pathogens were present in all of the drinking water sources.
Although, the numbers of cells necessary for an infective dose is relatively high for
opportunistic pathogens (ranging from 1 x10 6 to 1x10' ° CFU), the volume of water
consumed could conceivably deliver an infective dose during serial exposures
(Warburton et al., 1992). Adverse health effects is dependent upon, the bacteria involved,
the number of bacteria ingested and the individual's general health including resistant to a
particular organisms (McFeters, 1990).
The United States Environmental Protection Agency (EPA) has suggested that
HPC bacteria counts in drinking water should not exceed 500 CFU/mL, primarily
because of the interference of coliforms detection (EPA, 1989). In this study, drinking
water often failed to meet such a recommendation. HPC bacteria were often present in
numbers that reached lx 1 0 3 to 1x10 7 CFU/mL. Caution is needed when interpreting the
public health significance of HPC bacteria in drinking water. Although, it has been
suggested that these bacteria may be potentially pathogenic to the most vulnerable
individuals including infants and immunocompromised (McFeters, 1990), the potential
for adverse health effects appear to be low (Rusin et al., 1997a)
Various studies have shown that home treatment devices are effective in the
removal of contaminants in drinking water (microbiological and chemical), but the

99
effectiveness might be short-lived (McFeters, 1990). In this study, POU devices
efficiently removed chlorine from the tap water source (Table 6). However, the microbial
quality of the water produced from these devices was extremely variable. This may be a
function of service life of the filter, water static conditions in distribution systems, and
water line repairs rather than the municipal water treatment (Geldreich et al., 1986).
On the basis of the results obtained in this study, bottled water and municipal tap
water were superior in bacterial quality when compared with the water dispensed by
POU-devices and the tap water with POU-connection. This results indicated that the use
of POU-devices might increase the numbers of bacteria in drinking water, promote
biofilm formation, and might have an influence on the bacterial quality of the connected
tap water.
The results obtained in this study suggest that microbial contamination might be
derived from the plumbing system (sediment deposition, static water zones, and warm
water), and POU-devices may allow bacteria to proliferate in the filter device. Therefore,
the larger the water standing in the distribution system, the greater the potential there is
for bacteria to accumulate in the POU-device. Regular maintenance of the filter
(changing filter cartridge at least as frequently as recommended by the manufacturers)
may enhance the water quality of the water dispensed from POU-device.

100
References to Appendix 3:
American Public Health Association (APHA). 1995. Standard Methods for theExamination of Water and Wastewater, 1 8th ed. Washington, DC.
Bischofberger, T. Cha, S.K., Schmitt, R., Konig, B. and W. Schmidt-Lorenz. 1990. Thebacterial flora of non-carbonated, natural mineral water from springs to reservoir andglass and plastic bottles. Int. I Food Microbiol. 11:51-72.
Bitton, G. 1994. Wastewater Microbiology. Wiley-Liss. NY.
Bullin, C.H., Tanner, E.I. and C.H. Collins. 1970. Isolation of Mycobacterium xenopeifrom water taps. I Hyg. Camb. 68:97-100.
Caroli, G., Levre, E., Armani, G., Biffi-gentili, S. and G. Molonari. 1985. Search for acid-fast in bottled water. J. App!. Bacteriol. 58:461-464.
Collins, C.H., Grange, J.M. and M.D. Yates. 1984. Mycobacteria in water. J. Appl.Bacteriol. 57:193-211.
Difco laboratories. 1984. Difco manual: dehydrated culture media and reagentsfor microbiology, 10 6' ed. Difco laboratories, Detroit, MI.
Edberg, S.C., Gallo, P. and C. Kontnick. 1996. Analysis of the virulence characteristicsof bacteria isolated from bottled water, water cooler, and tap water. Microbial Ecol. Hlth.Dis. 9:67-77.
Environmental Protection Agency (EPA). 1989. Drinking water health effects task force.Health effects of drinking water treatment technologies. Lewis Pubs. Chelsea, MI.
Fewtrell, L., Kay, D., Wyer, M., Godfree, A. and G. O'neall. 1997. Microbiologicalquality of bottled water. Wat. Sci. Tech. 35:47-53.
Geldreich, E.E. 1996. Microbial quality of water supply in distribution systems. CRC,Boca Raton, FL.
Geldreich, E.E. and D.J. Reasoner. 1989. Home water treatment devices and waterquality, p. 147-167. In G.A McFeters, Springer-verlag (ed.). Drinking watermicrobiology. New York, NY.

101
Geldreich, E.E. 1986. Potable water: new directions in microbiological regulations. ASM
News. 52:530-534.
Geldreich, E.E., Taylor, R.H., Blannon, J.C. and D.J. Reasoner. 1985. Bacterial
colonization of point-of-use water treatment devices. J. Amer. Water Works. Assoc.
77:72-80.
Geldreich, E.E., Nash, H.D., Reasoner, D.J. and R.H. Taylor. 1975. The necessity of
controlling bacterial population in potable water-bottled water, and emergency water
supplies. J. Amer. Water Works Assoc. 67:117-124.
Gonzalez, C. Gutierrez, C. and T. Grande. 1987. Bacterial flora in bottled uncarbonated
mineral drinking water. Can. J. Microbiol. 33:1120-1125.
Hoadley, A. W. 1977. Pseudomonas aeruginosa in surface waters. p. 31-57. In young,
V.M. Raven press (ed.) Pseudomonas aeruginosa: ecological aspects and patients
colonization., New York, NY.
Holmes, P., Niccolls, L.M. and D.P. Sartory. 1996. The ecology of mesophilic
Aeromonas in aquatic environment. p. 126-150. In Wiley (ed.) The genus Aeromonas.
New York, NY.
Holtzman, A.E., Aronson, T.W., Glover, N., Froman, S., Stelma, G.N., Sebata, S.N.,Boian, M.G. and O.G.W. Berlin. 1997. Examination of bottled water for non-tuberculous
Mycobacteria. J. Food Protect. 60:185-187.
Hunter, P.R. 1993. The microbiology of bottled natural mineral waters. J. App!.
Bacteriol. 74:345-352.
Hunter, P.R. 1994. Bottled natural mineral water and other bottled waters. Microbiol.
Europe. 2:8-10.
Jeppesen, C. 1995. Media for ileromonas spp., Plesiomonas spp. and Pseudomonas spp.
from and the environment. Int. J. Food Microbiol. 26:25-41.
Levesque, B., Pierre, S., Gauvin, D., Gingras, S., Dewailly, E. and R. Letarte. 1994.
Comparison of the microbiological quality of water coolers and that of municipal water
systems. App!. Environ. Microbiol. 60:1171-1178.
Lynkins, B.U., Clark, R.M. and A.G. James. 1992. Point-of-use/point-of-entry for
drinking water treatment. Lewis, Chelsea, MI.

102
Manaia, C.M., Nunes, 0.C., Morais, P.V. and M.S. Da Costa. 1990. Heterotrophic platecounts and the isolation of bacteria from mineral waters on selective andenrichment media. J. App!. Bacteriol. 69:871-876.
McFeters, G.A. 1990. Drinking water microbiology. G.A. McFeters (ed.), SpringerVerlag. New York, NY.
Naranjo, J.E., Chaidez, C., Quinonez, M. Gerba, C.P., Olson, J. and J. Dekko. 1997.Evaluation of portable water purification system for the removal of enteric pathogens.Wat. Sci. Tech. 35:55-58.
Ogan, M. 1992. Microbiological quality of bottled water sold in retail in Nigeria. I App!.Bacteriol. 73:175-181.
Olson, B.H. and L.G. Nagy. 1984. Microbiology of potable water. Adv. Appl. Microbiol.30:73-132.
Payment, P., Franco, E. and Siemiatycki. 1991. Gastrointestinal health effects associatedwith the consumption of drinking water produced by point-of-use domestic reverseosmosis filtration units. App!. Environ. Microbiol. 57:945-948.
Payment, P., Siemiatycki, J., Richardson, L., Renaud, G., Franco, E. and M. Prevost.1997. A prospective epidemiological health effects due to the consumption of drinkingwater. Int. i Environ. Hit/i. Res. 7:5-31.
Payment, P. 1989. Bacterial colonization of domestic reverse-osmosis filtration units.Can. J. Microbiol. 35:1065-1067.
Reasoner, D.J., Blarmon, J.C. and E.E. Geldreich. 1987. Microbiological characteristicsof third-faucet point-of-use devices. J. Amer. Water Works Assoc. 79:60-66.
Rusin, P.A., Rose, J.B., Haas, C.H. and C. P. Gerba. 1997. Risk assessment ofopportunistic bacterial pathogens in drinking water. Rev. Environ. Con tam. Toxicol.152:57-83.
Rusin, P.A., Rose, J.B. and C.P. Gerba. 1997b. Health significance of pigmented bacteriain drinking water. Wat. Sci. Tech. 32:21-27.
Slade, P.J., Falah, M.A. and A.M. Al-Ghady. 1986. Isolation of Aeromonas hydrophilafrom bottled waters and domestic water supplies in Saudi Arabia. J. Food Protect.49:471-476.
103
Snyder, J.W., Craig, N.M., Anderson, R.E and G.K. Bissonnette. 1995. Effect on point-of-use, activated carbon filters on the bacteriological quality of rural groundwatersupplies. Appl. Environ. Microbiol. 61:4291-4295.
Swanson, S. 1996. International bottled water association: an update. Water Cond. Purif.38:40-41.
Symons, M.J. 1997. Home facts. Texas A&M University Press, Texas.
Taylor, R.H., Allen, M.J. and E.E. Geldreich. 1979. Testing of home use carbon filters.Amer. Water Works Assoc. 71:577-579.
Tobin, R.S., Smith, D.K. and J.A. Lindsay. 1981. Effects of activated carbon andbacteriostatic filters on microbiological quality of drinking water. Appl. Environ.Microbiol. 41:646-651.
Tsai, G.J. and S.C. Yu. 1997. Microbiological evaluation of bottled water uncarbonatedmineral water in Taiwan. Int. I Food Microbiol. 37:137-143.
Warburton, D.W., Dodds, K.L., Burke, R., Johnston, M.A. and P.J. Laffey. 1993. Areview of the microbiological quality of bottled water sold in Canada between 1981 and1989. Can. J. Microbiol. 38:12-19.
Warburton, D.W. 1993. A review of the microbiological quality of bottled water sold inCanada. Part2. The need for more stringent standards and regulations. Can. I Microbiol.39:158-168.
Warburton, D.W., McCormick, J.K. and B. Bowen. 1994. Survival and recovery ofAeromonas hydrophila in water: development and methodology for testing bottled waterin Canada. Can. I Microbiol. 40:145-148.
Wallis, C., Stagg, C.H. and J.L. Melnick. 1974. The hazards of incorporating charcoalfilters into domestic water systems. Wat. Res. 8:111-113.

104
Table 2. Percentage bacterial occurrence in POU-treated water, tap water (with POU), tapwater (without POU), and bottled water
Percentage of bacteria (%)
Organisms POU-treatedwater(57)e
Tap withPOU(57)
Tap withoutPOU(30)
Bottledwater(72)
A. hydrophilaa 7.0 10.5 6.6 6.9P. aeruginosaa 38.5 33.3 16.6 8.3
Acid-fast organisms' 43.8 35 16.6 5.5Total coliformse 82.4 33.3 6.6 15.2
1-1PCd 87.7 61.4 43.3 65.3CFU/500 mLAcid fast stain positivesCFU/100 mL
d Heterotrophic plate count bacteria greater than 500 CFU per rriLe Number of samples
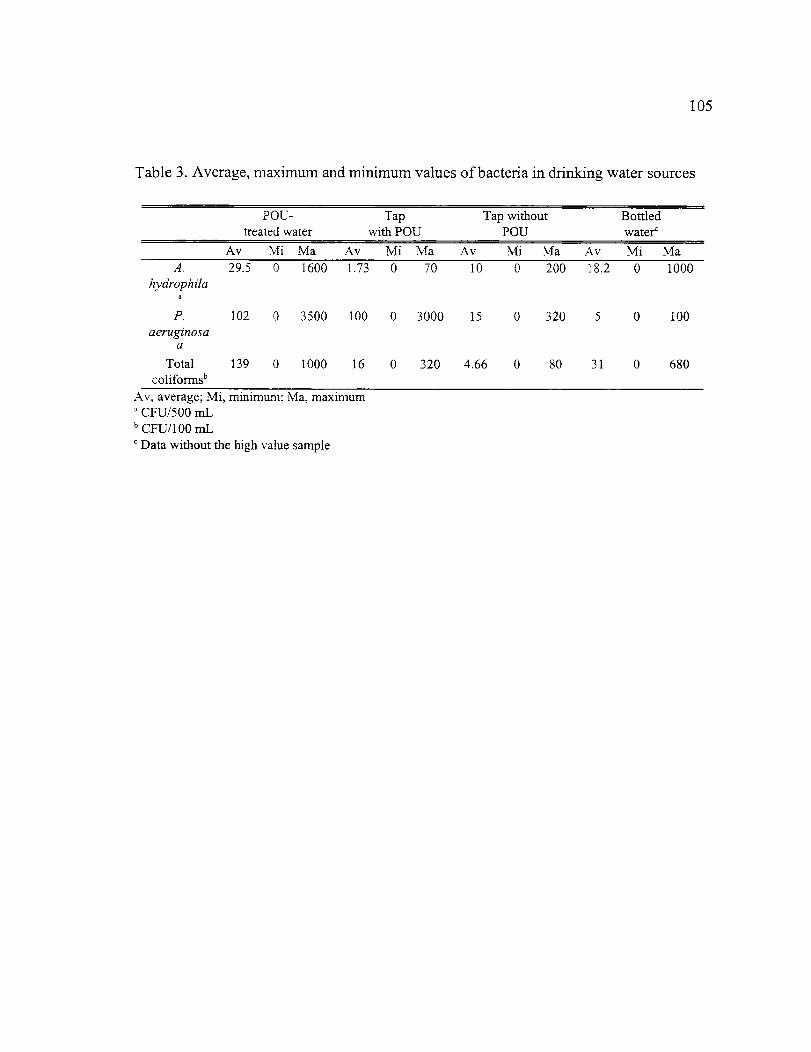
105
Table 3. Average, maximum and minimum values of bacteria in drinking water sources
POU-treated water
Tapwith POU
Tap withoutPOU
Bottledwater`
Av Mi Ma Av Mi Ma Av Mi Ma Av Mi MaA.
hydrophdaa
29.5 0 1600 1.73 0 70 10 0 200 18.2 0 1000
P.aeruginosa
a
102 0 3500 100 0 3000 15 0 320 5 0 100
Totalcoliformsb
139 0 1000 16 0 320 4.66 0 80 31 0 680
Av, average; Mi, minimum; Ma, maximumCFU/500 mL
b CFU/100 mLData without the high value sample

Table 4. Occurrence of the HPC in drinking water sources
Heterotrophic plate count bacteria (%)
HPCCFU/mLa
POU-treatedwater(57)d
Tapwith POU(57)
Tap withoutPOU(30)
Bottledwater(72)
<1 0 0 5.51-10 0 0 3.3 5.5
11- 100 1.7 7.0 26.6 15.3101 - 1,000 24.6 47.4 30.0 12.5
1,001 - 10,000 42.1 26.3 16.6 34.710,001 - 100,000 15.7 10.5 23.3 25
> 100,000 15.7 8.7 0 0Range' 100 - 4x10 7 40- 2x10' 10 - 5x10 4 <1 - 9x104
Median' 4000 700 300 1750Geometric mean' 9692 1841 642 906
Heterotrophic plate count bacteria (7d incubation time at 25°C)All values are percent of samplesNumber of bacteria per mLNumber of samples
106

Table 5. Bacteria isolated and identified in drinking water samples
Organisms POU-treatedwater
Tap water(with POU)
Tap water(without POU)
Bottledwater
Acinetobacter` XEnterobacter
cloacae'X X X X
Enterobacteraglomerans"
X X X
Klebsiella oxytocaa X X XKlebsiella
pnetunoniaeaX X X
Moraxella sp.' XPseudomonas putida b X X XSerratia marcencensb X X X
a Total coliforms"Pigmented bacteria' Heterotrophic bacteria
107

108
Table 6. Average, maximum and minimum values for the physico-chemical parameters inanalyzed water (POU-treated water, tap water with POU, tap water without POU, andbottled water)
POU-treatedWater
Tap with POU Tap withoutPOU
Bottled water
Av Mi Ma Av Mi Ma Av Mi Ma Av Mi MapH 7.6 6.6 8.7 7.8 7.1 8.6 7.8 7.4 8.2 7.3 5.6 8.3
Temperature 23 22 25 24 22 26 23 22 24 n/a nia nia(°C)
Turbidity 0.8 0.2 4.6 0.6 0.2 2.3 0.9 0.2 2.4 0.4 0.1 1.2(NTU)Total
chlorine
(mg/L)
0 0 0 0.3 0 0.8 0.3 0 0.9 0 0 0
Freechlorine
0 0 0 0.2 0 0.7 0.3 0 0.8 0 0 0
(1110-)Av, average; Mi, minimum; Ma, Maximumnia (Not available)

21P 0U-water
Tap welfP OU
Tap witho ut P OU
3 4
weeks
5 6
109
Fig 1. Mean HPC bacteria densities (CFU/mL)

6 —+-- FCUmater
--II-- Tap Wth
—it— Tap withat FCUwaek
110
Fig 2. Mean Pseudomonas aeruginosa densities (CFU/500 mL)

weeksP 0U-water
Tap with P OU
Tap witho ut P OU I
2.5
-0.5
111
Fig 3. Mean Aeromonas hydrophila densities (CFU/500mL)
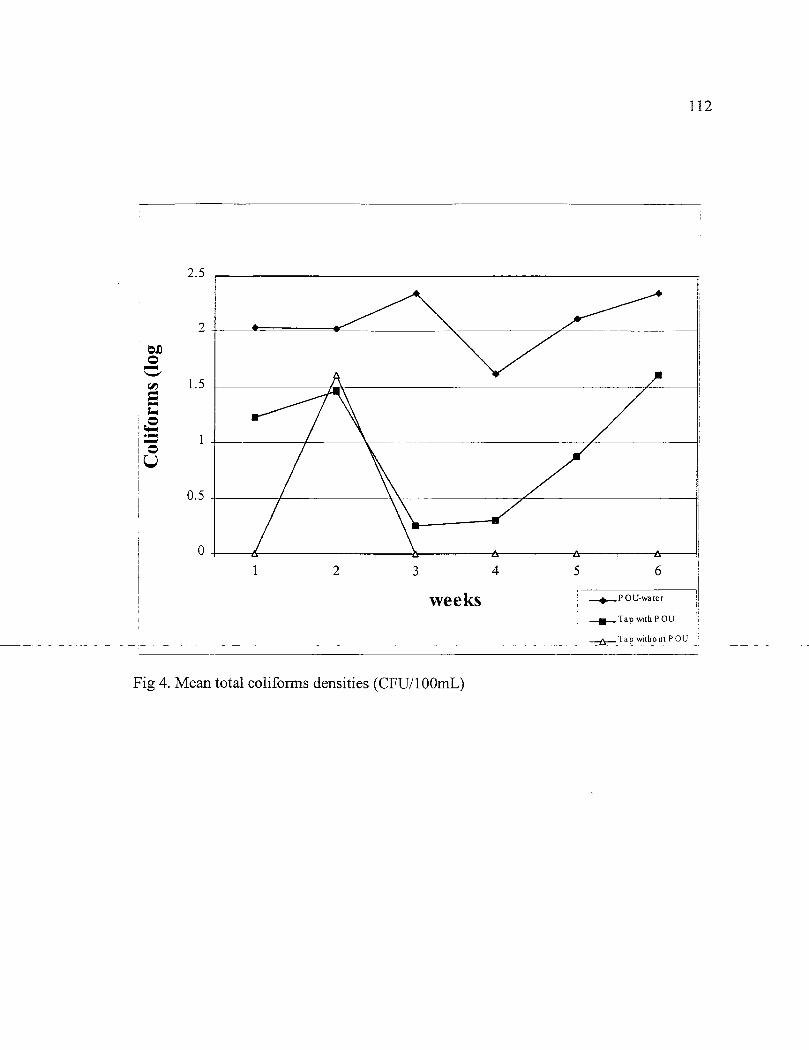
•
111
. A A. A
1 2 3
weeks4 5 6
—40— POU-water
2.5
0
2
0 5
112
Tap with P OU
Tap without P OU
Fig 4. Mean total conforms densities (CFU/100mL)

113
APPENDIX 4:
AEROMONAS HYDROPHILA AND PSEUDOMONAS AERUGINOSA IN DRINKINGWATER FROM VARIOUS SOURCES: A RISK ASSESSMENT
Cristobal Chaidez Quiroz i and Charles P. Gerba* 2
Department of Nutritional Sciences' and Department of Soil, Water and EnvironmentalSciences'
The University of ArizonaTucson, Arizona 85721
*Corresponding author

114
Abstract
The opportunistic bacterial pathogens, Aeromonas hydrophila and Pseudomonas
aeruginosa have been detected worldwide in drinking water and are associated with a
number of human infections. There have been concern that the presence of these
organisms in drinking water may represent a public health threat. The purpose of this
work was to assess the potential risk of infection (colonization) of these organisms from
exposure to various sources of drinking water (POU-treated water, tap water with POU-
connection, bottled water and water from vending machines and household storage
tanks). Water samples were collected from described sources and tested.
Based on data obtained from human dose-response studies the exponential model
{Pi = 1 - e HiNxENDI was chosen to be used in this risk assessment. The model was used to
develop a microbial risk assessment to estimate daily and yearly risks of infection
(colonization) for the exposure of opportunistic pathogens via drinking water. Analysis
indicate that risks of colonization ranged from 5x10' - 1.6x10 for A. hydrophila, and
7.7x10 -9 - 1.8x10' for P. aeruginosa could result for drinking water from the sources
studied based on the consumption of 2L/day/person. In general, the risk of colonization
may be associated with the most vulnerable (very young, the elderly and
immunocompromised).
Introduction
Risk assessment has been used for setting standards for toxic chemicals in water
and foods (Rose and Gerba, 1991). This process attempts to identify the risks and
quantify the degree of risk to exposed individuals or populations. Risk assessment has
only been used on a limited scale to determine and evaluate the risks involved with
exposure to waterborne pathogenic microorganisms (Haas, 1983; Gerba and Haas, 1988;
Rose et al., 1991; Rose and Gerba, 1991; Regli et al., 1991; Rusin et al., 1997).
Opportunistic bacterial pathogens are members of the heterotrophic bacteria and often are
found in low numbers in drinking water. The risks these may pose to consumers has been
subject to much debate. This debate has centered on the importance of high numbers of
heterorophic (HPC) bacteria in drinking water. It has been suggested that drinking water
should not exceed 500 CFU per mL (EPA, 1989). This recommendation is based on the
findings that this level interferes with the detection of coliform bacteria which are used to
judge the sanitary quality of drinking water. No epidemiological data is available to
indicate that this or higher levels of HPC bacteria in drinking water are harmful. The
premise of this study is that the concentration of specific opportunistic pathogens are
more important than HPC bacteria as a whole. Thus, the occurrence of two common
HPC bacteria (A. hydrophila and P. aeruginosa) in various sources of drinking water
(point-of-use -POU- treated water, tap water with POU-connection. tap water, bottled
115

116
water, water from vending machines, and water from household storage tanks from
Mexico) were studied.
A. hydrophila has been isolated from humans since the early 1950s (Carnahan and
Altwegg, 1996). A. hydrophila is commonly isolated from patients with gastroenteritis.
It has also been found in wound and ocular infections (Janda and Abbot, 1996).
Aeromonads are oxidase positive, facultatively anaerobic, glucose fermenting, Gram-
negative bacilli (Hazen et al., 1978). They are a straight rod that measures 0.3 to 1.0 by
1.0 to 3.5 l_tm. Three species have been associated with human gastroenteritis, however
the exact mechanisms for diarrhea is not well defined (A. hydrophila, A. sobria, and A.
caviae) (Holmberg et al., 1986).
Pseudomonas species are Gram-negative, straight or slightly curved rods, motile
with polar flagella (Hoadley, 1977). The genus Pseudomonas contains well-recognized
pathogens (P. malle', P. cepacia, and P. aeruginosa). The source of infection is often
difficult to trace, but colonization has been associated with hospital equipment as well as
water-related reservoirs outside the hospital (i.e. swimming pools, hot tubs and contact
lenses ) (Rusin et al., 1997). P. aeruginosa can be introduced to susceptible tissues of
patients requiring instrumentation (i.e. catheter, aerators and respiratory therapy
equipment) posing a health threat (Fick, 1993).
Risk assessment involves four basic steps: 1) hazard identification; 2) dose-
response assessment; 3) exposure assessment; and, 4) risk characterization (NRC, 1983).
The purpose of the present study was to use the four-tiered approach to evaluate the

117
microbiological hazard from ingestion of drinking water. The data were obtained from
the previously cited studies of the occurrence of A. hydrophila and P. aeruginosa in
drinking water (POU-treated water, tap water with POU-connection, tap water, bottled
water, water vending machines and water storage tanks) (Chaidez et al., 1997; Chaidez et
al., 1998; Chaidez and Gerba, 1998). The risk assessment steps were followed to assess
the risks of acquiring an opportunistic bacterial infection (colonization) from
contaminated drinking water.
Materials and Methods
A. hydrophila and P. aeruginosa were selected for the study due to the importance
as opportunistic pathogens in drinking water and their common occurrence in drinking
water sources. The association of these organisms with water-related illness was also
evaluated.
Quantitative dose-response models were developed using information involving
human volunteer feeding studies (Bergogne-Berezin, 1994; Buck and Cooke, 1969).
Different mathematical models have been developed for evaluating microbial risk
assessment (Haas, 1983; Rose, 1997). However, the exponential model provided the best
fit-value to be used in estimating daily (Pi) and yearly (Pyea) risks of infection for the
study organisms (Rusin et al., 1997). The exponential model is as follow : Pi 1 - e
(1/10x(N)

118
The exposure assessment was conducted by collecting the data obtained in the
three previously cited studies (Chaidez et al., 1997; Chaidez et al., 1998; Chaidez and
Gerba, 1998). This information was then analyzed to perform the risk characterization.
Result
Hazard identification
Aeromonas hydrophila
Bacterial gastroenteritis due to A. hydrophila has been described (Moyer, 1987).
However, the exact mechanisms of diarrhea has not been elucidated. The virulence
factors that may be responsible include cytotoxin related to the cholera toxin, heat-labile
and heat-stable enterotoxins, hemagglutinins and hemolysin (Rusin et al., 1997). A.
hydrophda cause several types of clinical illnesses including diarrhea, wound infections,
endocarditis, meningitis, pneumonia, osteomyelitis, peritonitis, conjuntivitis,
thrombophlebitis, and cholecyititis (Janda et al., 1995; Janda and Duffey, 1988).
Septicemia due to A. hydrophda may be life-threatening. In the U.S. the overall
frequency is low (<1%) (Janda and Abbot, 1996). Common symptoms include fever (94-
95%) and chills (70%) (Harris et al., 1985). Patients who become septic with Aeromonas
often exhibit signs of gastrointestinal involvement, including abdominal pain, nausea,
vomiting and diarrhea (Dryden and Munro, 1989).

119
The health significance of Aeromonas in drinking water is not well understood as
few outbreaks are documented and establishing epidemiological links is difficult. Burke
et al., (1984) suggested a connection between cases of Aeromonas-associated diarrhea
and the numbers of Aeromonas in drinking water. It is accepted that some strains of
Aeromonas are enteropathogens possessing a range of virulence factors (enterotoxins,
cytotoxins, hemolysins and invasive ability) (Kirov, 1993) which can be expressed by
both environmental and clinical strains of Aeromonas (Cahill, 1990). Enteropathogens
strains of A. hydrophila, A. sobria and A. caviae have all been isolated from cases of
gastroenteritis (Deodhar et al., 1991). Ghanem et al., (1993) considered that potable
water was the source of Aeromonas infections after 90% of the samples were positive for
the organism. A. hydrophila isolated from a private unchlorinated well was proposed as
the cause of a long-term diarrhea in an 18-month-old child (Krovaceck and Peterz, 1989).
In a long-term care institution, there were 17 patients involved in acute diarrheal
episode presumably due to contaminated food or drinking water. Four patients were
positive for A. hydrophila, and a fatality was observed in one patient. It was concluded
that previous predisposing factors were associated with such fatality (Bloom and Bottone,
1990). Although Aeromonas are frequently isolated from drinking water systems, and
some strains may exhibit enterotoxic properties, further epidemiological studies are
required to ascertain whether there is any relationship between cases of Aeromonas-
associted diarrhea and the presence of these organisms in drinking water.

120
Pseudomonas aeruginosa
P. aeruginosa is the most important nosocomial pathogen responsible for 9% of
all hospital-acquired infections (Pollack, 1990). The mortality of nosocomial
pneumonias remains as high as 70% (Celis et al., 1988). Cystic fibrosis (CF) is the most
common lethal genetic disease of Caucasians, and chronic Pseudomonas respiratory
infections complicate 90% of CF patients leading to respiratory failure and death
(Gilligan, 1991). Hospitalization leads to greatly increased rates of carnage, especially in
patients with serious burns. Hoadley, (1977) reported that the rate of infection is about
25% in burn patients. Other infections occur due to P. aeruginosa including ear
infections (e.g. otitis externa), especially among swimmers (Hoadley, 1977).
The nutritional requirements of P. aeruginosa are extremely simple, favoring
growth in almost any moist environment (e.g. sinks, weak antiseptic solutions, eye drops,
anesthesia and resuscitation equipment, humidifiers, and stored distilled water)
(Steigbigel et al., 1968). P. aeruginosa may be transmitted by contaminated water, soil,
and vegetables. Kominos et al., (1972) demonstrated that vegetables may be the source
of P. aeruginosa in hospital kitchens. Shooter et al., (1969) implicated foods and
medicines as route of transmission in the hospital environment.
A group of people developed otitis after they were bathed in a wooden hot tub
containing P. aeruginosa (CDC, 1982). In 1947, an epidemic of acute P. aeruginosa
gastroenteritis was reported in a newborn nursery in which milk was implicated.
Symptoms were described as diarrhea, cramps, nausea, and vomiting, being more severe

121
in infants (Hunter and Ensign, 1947). Contaminated drinking water was traced as the
source of P. aeruginosa causing an outbreak of funicular sepsis. Ten newborn in a
hospital of Germany were infected by the bacterium (Weber et al., 1971). The
information of this study was scarce thus, the evidence lacks of credibility. P. aeruginosa
was isolated from a hospital tap water causing urinary tract infections, pneumonia and
sinusitis in nine hospitalized individuals (Bert et al., 1998).
The human body uses a complex cellular interaction to attack P. aeruginosa
infection. P. aeruginosa has a wide variety of virulence factors. These virulence factors
can be divided into two general groups: 1) cell surface components (pili,
lipopolysaccharide-LPS-) and 2) extracellular products (exotoxin A, proteases, and
lecithinase) (Peterson, 1980). No single host factor is of paramount importance in host
defense against P. aeruginosa which depends upon the integrated functions of the
epithelial cells barriers, antibodies, the complement system, phagocytic cells, and
lymphocytes (Peterson, 1980).
Dose-response
The development of a quantitative dose-response relationship is a primary step
in performing a risk analysis (Rose et al., 1991). The dose-response model describes
the quantitative relationship between the dose of a microorganism (the exposure) and
the response of the exposed population (the occurrence of infection). Human and
animal studies have been conducted to elaborate dose-response models (Macler, 1993).

122
In the environment, exposures to microorganisms are usually at doses that are too low to
measure via direct dose-response experiments (Rose et al., 1991). Thus, it is necessary
to use high concentration of pathogenic microorganism in order to observe high
frequencies of infections with a minimum numbers of volunteers. High exposures are
extrapolated down to doses that are representative of environmental scenarios by using
mathematical models (Rose and Gerba, 1991).
The exponential model provides the best fit exposure to A. hydrophila and P.
aeruginosa in drinking water (Rusin et al., 1997). The exponential model may be
expressed as:
Pi = 1 - el 4" )x(Nn
Where Pi is the probability of infection, 1/k is the fraction of ingested
microorganisms that survive to initiate infection, and N is the number of organisms
ingested. The model assumes a random distribution of microorganisms and that one
single microorganism is capable of initiating an infection (Haas, 1983). Yearly risk
were calculated using the following equation:
year = 1 - ( 1 - Pi)365
Exposure assessment
Aeromonas hydrophila
A. hydrophila is an ubiquitous bacterium frequently isolated from drinking water
and aquatic environments (Table 1). Chaidez and Gerba, (1998) found A. hydrophila in

123
6.6% of tap water samples at average concentration of 0.6 CFU/mL, and Levesque et
al., (1994) recovered the bacterium from 12% of the tap water samples. It has also been
recovered in 25% of distribution water samples at an average concentration of 0.001-94
CFU/mL (Millership and Chattopadhyay, 1985; Knocheland and Jeppesen, 1990;
Handfield et al., 1996; LeChevallier et al., 1982; Krovaceck et al., 1992). Taps with a
POU-connection (Faucet-mounted units) have shown to increase bacterial
concentrations when compared with tap water collected without filter device
connection. A. hydrophila was present in 10.5% of tap water samples with a POU-
connection at concentrations ranging from 0.006 to 0.14 CFU/mL (Chaidez and Gerba,
1998). POU-devices connected in households taps had A. hydrophila at concentrations
that ranged from 0.1 to 3.2 CFU/mL (Chaidez and Gerba, 1998). This data suggests
that POU-devices encourage the growth of A. hydrophila to levels greater than that
found in the tap water.
Bottled water has been shown to contain A. hydrophila. Chaidez and Gerba,
(1998) recovered the bacterium in 6.9% of the bottled water tested at concentrations
ranging from 0.1 to 0.3 CFU/mL. This excludes, one bottled water sample obtained
from Costa Rica which had a concentration of 90 CFU/mL. Others studies have
reported the isolation of this bacterium from bottled water, however the actual
concentrations were not provided (Tsai and Yu, 1997; Gonzalez et al., 1987; Manaia et
al., 1990; Slade et al.. 1986). The bacterium was present in 10% of water from vending
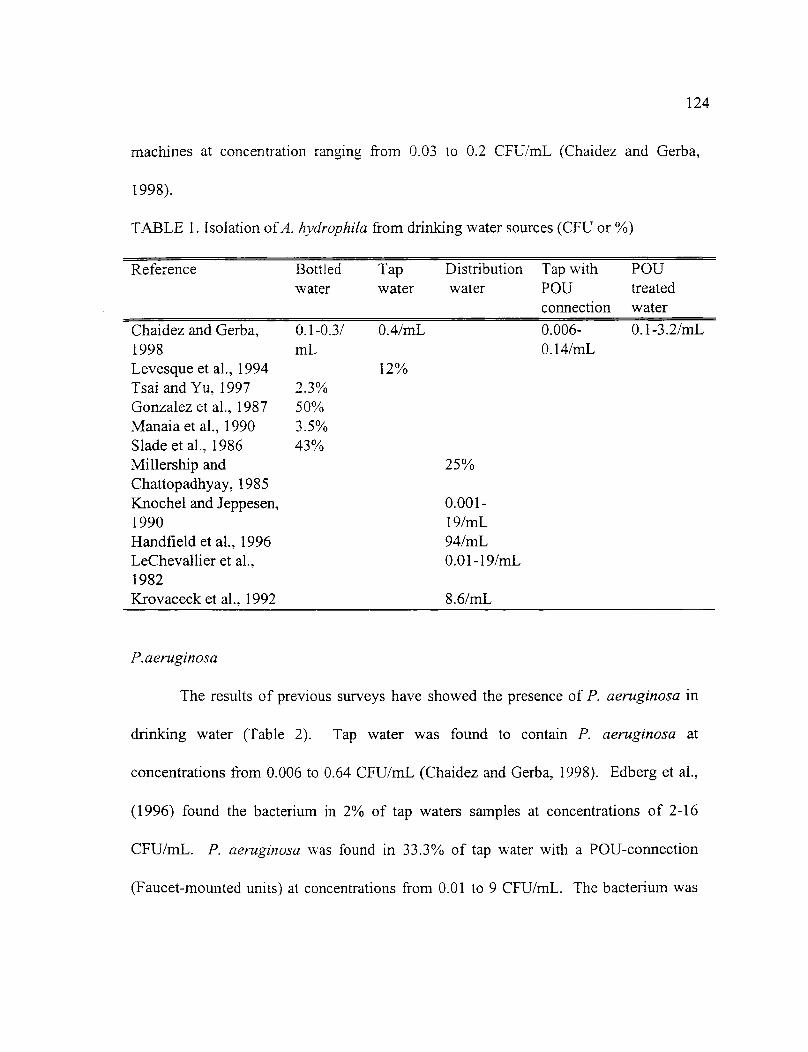
124
machines at concentration ranging from 0.03 to 0.2 CFU/mL (Chaidez and Gerba,
1998).
TABLE 1. Isolation of A. hydrophda from drinking water sources (CFU or %)
Reference
Bottled Tap Distribution Tap with POUwater water water POU treated
connection water
Chaidez and Gerba, 0.1-0.3/ 0.4/mL 0.006-1998 mL 0.14/mLLevesque et al., 1994 12%Tsai and Yu, 1997 2.3%Gonzalez et al., 1987 50%Manaia et al., 1990 3.5%Slade et al., 1986 43%Millership and 25%Chattopadhyay, 1985ICnochel and Jeppesen, 0.001-1990 19/mLHandfield et al., 1996 94/mLLeChevallier et al., 0.01-19/mL1982Krovaceck et al., 1992 8.6/mL
0.1-3.2/mL
P.aeruginosa
The results of previous surveys have showed the presence of P. aeruginosa in
drinking water (Table 2). Tap water was found to contain P. aeruginosa at
concentrations from 0.006 to 0.64 CFU/mL (Chaidez and Gerba, 1998). Edberg et al.,
(1996) found the bacterium in 2% of tap waters samples at concentrations of 2-16
CFU/mL. P. aeruginosa was found in 33.3% of tap water with a POU-connection
(Faucet-mounted units) at concentrations from 0.01 to 9 CFU/mL. The bacterium was

125
found in 38.5% of POU-devices mounted on household water taps at concentrations
from 0.008 to 10 CFU/mL (Chaidez and Gerba, 1998).
Chaidez and Gerba, (1998) found P. aeruginosa in 8.3% of bottled water tested
at concentrations from 0.01 to 0.2 CFU/mL. Fewtrell et al., (1997) reported that P.
aeruginosa was present in 12% of bottled water at an average concentration of 0.05
CFU/mL. Manaia et al., (1990) identified P. aeruginosa in 29% of the bottled waters
tested, and Edberg et al., (1996) found that 3% of bottled water contained the bacterium.
P. aeruginosa was found in water from vending machines at concentrations from 0.004
to 0.2 CFU/mL (Chaidez et al., 1997). Drinking water from storage tanks showed the
presence of the bacterium in 28% of the samples at concentrations from 0.002 to 0.6
CFU/mL (Chaidez et al., 1998).
TABLE 2. Isolation of P. aeruginosa from drinking water sources (CFU or %)
Reference Bottled Tap Tap with POU WVMa WSTb
water water POU treatedconnection water
Chaidez and 0.1- 0.006- 0.01-9/mL 0.008-Gerba, 1998 0.2/mL 0.64 10/mL
/mLEdberg et al., 3% 2-16/mL1996Fewtrell et al., 0.05/m1997Manaia et al., 29%1990Chaidez et al.,1997Chaidez et al.,1998
0.004-0.2/mL
0.002-0.6/mL
a Water vending machinesb Water storage tanks

126
During the exposure assessment, the amount of water consumed must also be
considered. An ingestion of 2 Upersoniday for the general population and 4
Li/person/day for the elderly for drinking water exposure was applied (Roseberry and
Burmaster, 1992).
Risk Characterization
Daily risks of colonization based on the consumption of 2L/day/person for A.
hydrophda ranged from 5x10 -1° for tap water with POU-connection to 2.2x10 -7 in
bottled water. On the annual basis the risks ranged from 1.8x10 -7 for tap water with
POU-connection to 7.9x10 -5 for bottled water (Table 3).
Daily risks of colonization based on the consumption of 2L/day/person for P.
aeruginosa ranged from 3x10 -7 for tap water to 2.7x10-6 for POU-treated water. On an
annual basis, the risks ranged from 4.8x10 -5 for water from storage tanks and to 9.9x10-4
for tap water with POU-connection (Table 3).
Also, the risk of colonization based on the consumption of 4L/day/person was
evaluated (Table 4). Daily risks for A. hydrophila ranged from 6.7x10 -9 for tap water to
4.3x10-7 for bottled water, and on the annual basis the risks ranged from 4x10-7 for tap
with POU-connection to 1.6x10 -4 for bottled water. A very low risk of colonization was
observed for bottled water excluding one sample containing high numbers of A.

127
hydrophila (Table 5). For P. aeruginosa. the daily risks ranged from 7.7x10' for water
from vending machines to 5.5x10 -6 for POU-treated water, and on the annual basis from
2.8x10 -6 for water from vending machines to 1.9x10 -3 for POU-treated water. Table 6
shows the bacterial concentration used for the risk of infection analysis.
TABLE 3. Risk of infection of Aeromonas hydrophila and Pseudomonas aeruginosa inselected drinking water sources (2L/day/person)
ORGANISMS RISK (DAY) RISK (YEAR)
POU-treated waterA. hydrophila 9.9x10-9 3.6x10-6P. aeruginosa 2.7x10-6 9.9x10'
Tap water (with POU-connection)A. hydrophila 5x10-1° 1.8x10-7P. aeruginosa 2.6x10-6 9.7x10-4
Tap water (without POU-connection)A. hydrophila 3.3x10' 1.2x10-6P. aeruginosa 3.9x10-7 1.4x10-4
Bottled waterA. hydrophila 2.2x10-7 7.9x10-5P. aeruginosa 1.2x10-7 4.4x10-5
Water from vending machinesA. hydrophila 1.6x10' 5.8x10-7P. aeruginosa 3x1 07 1.1x10-5
Water from storage tanksA. hydrophila Not available Not availableP. aeruginosa 1.3x10-7 4.8x10-5

TABLE 4. Risk of infection of A. hydrophila and P. aeruginosa in selected drinkingwater sources (4L/day/person)
128
ORGANISMS
A. hydrophilaP. aeruginosa
A. hydrophilaP. aeruginosa
A. hydrophilaP. aeruginosa
A. hydrophilaP. aeruginosa
A. hydrophilaP. aeruginosa
A. hydrophilaP. aeruginosa
RISK (DAY) RISK (YEAR)POU-treated water
1.9x10 -8 7.3x10-65.5x10 -6 1.9x10-3Tap water (with POU-connection)
1.1x10 -9 4x10-75.3x10 -6 1.95x10-3Tap water (without POU-connection)6.7x10 -9 2.4x10-67.8x10 -7 2.8x10-4
Bottled water4.3x10-7 1.6x10-42.4x10-7 8.8x10-5
Water from vending machines3.3x10 -9 1.2x10-67.7x10 -9 2.8x10-6
Water from storage tanksNot available Not available
2.6x10-7 9.6x10-5
TABLE 5. Risk of infection of A. hydrophila in bottled water excluding one high value*
RISK (DAY) RISK (YEAR)Bottled water2L/day/person
6.1x10-9 2.2x10-64L/day/person
1.2x10 -8 4.4x10-6*One bottle contained 90 CFU/mL

129
TABLE 6. Daily bacterial concentrations used for the risk of infection based on two andfour liter consumption
ORGANISMS Bacterial concentration
POU-treated waterTwo liters Four liters
A. hydrophila(57)a 6732`(118.1) b 13464(236.2)P. aeruginosa(57) 23340(409.5) 46680(818.2)
Tap water (with POU-connection)A. hydrophila(57) 396(6.9) 792(13.9)P. aeruginosa(57) 22800(400) 45600(800)
Tap water (without POU-connection)A. hydrophila(30) 1200(40) 2400(80)P. aeruginosa(30) 1752(58.4) 3504(116.8)
Bottled waterA. hydrophila(72) 185160(2571.6) 370320 (5143.3)P. aeruginosa(72) 1308(18.2) 2616(36.3)
Water from vending machinesA. hydrophila(30) 588(19.6) 1176(39.2)P. aeruginosa(30) 1380(46) 2760(92)
Water from storage tanksA. hydrophila(25) Not available Not availableP. aeruginosa(25) 496(19.8) 992(39.7)
a Total of number of samples analyzed (N value)Arithmetic averageHighest bacterial concentration
Discussion
Aeromonas hydrophila and Pseudomonas aeruginosa, are well-recognized
opportunistic pathogens and have been responsible for waterborne (Burke et al., 1984;
CDC, 1982) and foodbome (Bloom and Bottone, 1990; Hunter and Ensign, 1947)
outbreaks . Most of the HPC bacteria in drinking water are not human pathogens.
However, some bacteria including A. hydrophila and P. aeruginosa cause human
infections.

130
The microbial risk assessment approach attempts to address the uncertainity of
environmental contamination, generally at low levels of exposure and the potential for
resulting health effects. Although the assessment is made through the use of
assumptions, resulting in quantitations with large range of variation and uncertainity,
the method is useful for ranking the risks, comparing different environmental sources
and different approaches to control (Rose et al., 1991; Rose and Gerba, 1991).
A number of assumptions were used in the application of the selected
mathematical models to drinking water data. First random distribution (poisson)
governs the occurrence of the drinking water microorganisms, the population is equally
susceptible to a single exposure and the exposure is defined as the consumption of
2L/day/person or 4L/day/person (Rose and Gerba, 1991; Haas, 1993).
Risk estimates using existing data would tend to underestimate actual risks as
the culture methods for concentration of opportunistic pathogens are not 100% efficient
and will not detect viable but non-culturable organisms. Risks may be overestimated by
assuming a specific volume of ingestion (2 or 4 L of drinking water), especially for
developing countries where access to drinking water is often difficult (Gerba et al.,
1996; Crabtree, 1996). This assumption may not also be adequate for everyone, as
some persons may consume more or less.
One of the more controversial areas surrounding the modeling is the potential for
a single organism to initiate an infection. However, current scientific data support the

131
"independent-action" (or single-organism) hypothesis (Rubin, 1987). A single
bacterium, or virus, or protozoan can reproduce is a known biological phenomenon
which has been proven in laboratory studies. While it is clear that the host defense
(cellular and humoral immunity) does play a critical role in the determination of which
individuals may develop infection, it has been also suggested that these do not provide
the complete explanation (Rubin, 1987). The evaluation of the dose-response data sets
also support the independent-action hypothesis as in almost every case the exponential
or beta models provided a statistically significant improvement in fit over the log-
normal which could be used to predict a threshold (Haas, 1983). No experimental data
support a threshold phenomenon.
Conclusions
A concern has been generated regarding the health risks associated with
opportunistic bacterial pathogens in drinking waters. Opportunistic bacteria continue to
occur in the United States and other developed countries. It has been recommended that
the microorganisms present a risk no greater than 1:10,000 per year of infection from
drinking water (EPA, 1989). From this assessment, P. aeruginosa collected from POU-
treated water had the greatest risk of colonization (1.9:1,000 per year), and with a lesser
risk from A. hydrophila from any of the drinking water sources. However, the risk of
colonization by opportunistic bacterial pathogens is very low when compared with a

132
waterborne pathogen. Unknown agents, viruses and the protozoa rank as the most serious
threats to water quality. For instance, the annual risk of infection of rotavirus for the
general population is of 8.34x10 -1 (8.34:10 per year)(Crabtree, 1996).
Colonization of the gastrointestinal tract by P. aeruginosa does not confirm that is
a prerequisite for pneumonia or other associated infections. To further narrow the risk to
human health only certain specific hosts are at risks, including patients with profound
neutropenia, cystic fibrosis, severe burns, and those subject to foreign device installation
(Hardalo and Edberg, 1997). A. hydrophila isolated from drinking water rarely infect the
human gastrointestinal tract and the majority of Aeromonas strains occurring in drinking
water differ from those found in diarrhea stools (Havelaar et al., 1992). Apparently, A.
hydrophila which infect humans are from a great variety of environmental sources
including food.
In general, the risk of colonization from opportunistic pathogens is seen as a
transient process. The probability of infection may be very low, and the chances of
illness may be associated to the most vulnerable (very young, the elderly and
immunocompromised). Also, it must be kept in mind that the dose-response models
predict colonization and not disease.
Research needs
Future research should include the comparison of the risk data from various sources of
exposure. For instance , the risk of colonization from POU-treated water was 10 times

133
greater than tap water without POU-connection. Also, more surveys of drinking water
from various sources for specific opportunistic bacterial pathogens should need to be
conducted.
References of Appendix 4:
Altwegg, M., G. Martinetti, J. Luthy-hottenstein, J. and M. Rohrbach. 1991. Aeromonas-associated gastroenteritis after consumption of contaminated shrimp. Ezir. I Clin.Microbiol. Infect. Dis. 10:44-45.
Bergogne-Berezin, E. 1994. Acinetobacter spp., saprophytic organisms of increasingpathogenic importance. Zentralbl. Bakteriol. 281:389-405.
Bert, F., Maubec, E., Bruneau, B. and N. Lambert-Zechovosky. 1998. Multi-resistantPseudomonas aeruginosa outbreak associated with contaminated tap water in aneurosurgery intensive care unit. J. Hosp. Infect. 39:53-62.
Bloom, H.G. and E.J. Bottone. 1990. Aeromonas hydrophila diarrhoea in a long-termcare setting. J. Amer. Geriatr.Soc. 38:804-806.
Buck, A.C. and E.M. Cooke. 1969. The fate of ingested Pseudomonas aeruginosa innormal persons. J. Med. Microbiol. 2:521-525.
Burke, V., Robinson, J., Gracey, M., Peterson, D. Meyer, N. and V. Haley. 1984.Isolation of Aeromonas spp. from unchlorinated domestic water supply. Appl. Environ.Microbiol. 48:367-370.
Carnahan, A.N. and M. Altwegg. 1996. Taxonomy. p.1. In Wiley (ed.) The genusAeromonas. Chichester, England.
Cahill, M.M. 1990. Virulence factors in motile Aeromonas species. J. Appl. Bacteriol.69:1-16.
Center for Disease Control. 1982. Otitis due to Pseudomonas aeruginosa 0:01 associatedwith a mobile redwood tub system-North Carolina. Morb. Mortal. Weekly Report.31:541-542.

134
Celis, R., Tones, A., Gate11, J.M. and M. Alnela. 1988. Nosocomial pneumonia amultivariate analyses of risk and prognosis. Chest. 93:318-324.
Chaidez, C., Candil, A., Uribe, M. and C.P. Gerba. 1998. Microbiological survey ofprivate roof water tanks in Culiacan, Mexico. J Environ. Sci. Hlth. In press.
Chaidez, C. and C.P. Gerba. 1998. Microbiological comparison of the quality of POU-treated water, tap water, and bottled water. University of Arizona, Tucson, AZ.(unpublished report).
Chaidez, C., Rusin, P.A., Naranjo, J. and C.P. Gerba. 1997. Microbiological quality ofwater vending machines. Int. J Food Microbial. In press.
Crabtree, K.D. 1996. Risk assessment of viruses in water. Ph.D. dissertation. Universityof Arizona. Tucson, AZ.
Deodhar, L.P., Saraswathi, K. and A. Vardukar. 1991. Aeromonas spp. and theirassociation with human diarrheal diseases. J. Clin. Microbial. 29:853-856.
Dryden, M. and R. Munro. 1989. Aeromonas septicemia: relationship of species andclinical features. Pathol. 21:111-114.
Edberg, S.C., Gallo, P. and C. Kontnick. 1996. Analysis of the virulence characteristicsof bacteria isolated from bottled water, water cooler, and tap water. Microbial EcoL Hlth.Dis. 9:67-77.
Environmental Protection Agency (EPA). 1989. Drinking water health effects task force.Health effects of drinking water treatment technologies. Lewis Pubs. Chelsea, MI.
Fewtrell, L., Kay, D., Wyer, M., Godfree, A. and G. O'neall. 1997. Microbiologicalquality of bottled water. Wat. Sci. Tech. 35:47-53.
Fick, R.B. 1993. Pseudomonas aeruginosa: The opportunist. CRC press.
Flynn, T.J. and I.G. Knipp. 1995. Seafood shucking as an etiology for Aeromonashydrophila infection. Arch. Intern. Med. 147:1816-1817.
Gerba, C.P. and C. N. Haas. 1988. Assessment of risks associated with enteric viruses incontaminated drinking water. American society for testing and materials. Philadelphia.
Gerba, C.P., J.B. Rose, C.N. Haas and K.D. Crabtree. 1996. Waterborne rotavirus: a riskassessment. Wat. Res. 30:2929-2940.

135
Ghanem, E.H., Mussa, M.E. and H.M. Eraki. 1993. Aeromonas-associated gastroenteritisin Egypt. Zentralbl. Mikrobiol. 148:441-447.
Gilardi, G.L. 1980. Medical Microbiology. p. 25-30. In Hans Huber (ed.) Pseudomonasaeruginosa, the organism. Switzerland.
Gilligan, P.H. 1995. Pseudomonas and Burkholderia. p. 509-519. In ASM press (ed.)Manual of clinical microbiology. Washington, DC.
Gilligan, P.H. 1991. Microbiology of airway disease in patients with cystic fibrosis. Clin.Microbiol. Rev. 4:35-51.
Glover, D., Ross, A. and J. Lugsdin. 1992. Gastroenteritis outbreak at an industrial camp-British Columbia. Can. Commun. Dis. Rep. 18:66-68.
Gonzalez, C. Gutierrez, C. and T. Grande. 1987. Bacterial flora in bottled uncarbonatedmineral drinking water. Can. I Mierobiol. 33:1120-1125.
Haas, C.N. 1983. Estimation of risk due to low doses of microorganisms: a comparison ofalternatives methodologies. Amer. I EpidemioL 118:537-582.
Handfield, M., Simard, P., Coullard, M. and R. Letarte.1996. Aeromonas hydropilaisolated from food and drinking water: Hemaglutination, hemolysis, and cytotoxity for ahuman intestinal cell line (HT-29). App!. Environ. Microbiol. 62:3459-3461.
Hardalo, C. and S.C. Edberg. 1997. Pseudomonas aeruginosa: Assessment of risk fromdrinking water. Crit. Rev. Microbiol. 23:47-75.
Harris, R.L., Fainstein, V., Elting, L., Hopfer, R.L. and G.P. Bodey. 1985. Bacteremiacaused by Aeromonas species in hospitalized cancer patients. Rev. Infect. Dis. 7:314-320.
Hazen, T.C., Flierman, G.B., Hirsch, R.P. and G.W. Esch. 1978. Prevalence anddistribution of Aeromonas hydrophila in the United States. App!. Environ. Microbiol.36:731-738.
Havelaar, A.H., Schets, F.M., Van Silfhout, A., Jasen, W.H., Wieten, G. and D. Van DerKooij. 1992. Typing Aeromonas strains from patients with diarrhoea and from drinkingwater. I Appl. Bacteriol. 72:435-444.

136
Hoadley, A. W. 1977. Pseudomonas aeruginosa in surface waters. p. 31-57. In young,V.M. Raven press. (ed.) Pseudomonas aentginosa: ecological aspects and patientscolonization. New York, NY.
Holmberg, S.D., Shell, W.L., Fanning, G.R., Wachsmoth, I.K., Hiickman, Brenner, F.W.and P.A. Blake. 1986. Aeromonas intestinal infections in the United States. Ann. Intern.Med. 105:109-114.
Hunter, C.A. and P.R. Ensign. 1947. An epidemic of diarrhea in a newborn nurserycaused by Pseudomonas aeruginosa. Amer. J. Public Hlth. 37:1166-1169.
Janda, J.M. and S.L. Abbott. 1996. Human pathogens. p. 151-173. In Wiley (ed.) Thegenus Aeromonas. Chichester, England.
Janda, J.M., Abbott, S.L. and A.M. Carnahan. 1995. Aeromonas and Plesiomonas. p.477-482. In ASM press (ed.) Manual of clinical microbiology. Washington, DC.
Janda, J.M. and P.S. Duffey. 1988. Mesophilic Aeromonads in human disease: Currenttaxonomy, laboratory and infections disease spectrum. Rev. Infect. Dis. 10:980-997.
Kirov, S.M. 1993. The public health significance of Aeromonas spp. in foods. Mt. J.Food Microbiol. 20:179-198.
Knochel, S. and C. Jeppesen. 1990. Distribution and characteristics of Aeromonas in foodand drinking water in Denmark. Mt. J Food Microbiol. 10:317-322.
Kominos, S.D., Copeland, C.E., Grosiak, B. and B. Postic. 1972. Introduction ofPseudomonas aeruginosa into a hospital via vegetables. Appl. Microbiol. 24:567-570.
Krovaceck, K. Dumontet, S., Ericksson, E. and S.B. Balada. 1995. Isolation and virulenceprofiles of Aeromonas hydrophila implicated in an outbreak of food poisoning inSweden. Microbiol. Immunol. 39:655-661.
Krovaceck, K., Faris, A., Baloda, S.B., Lindberg, T., Peterz, M. and I. Mansson. 1992.Isolation and virulence profiles of Aeromonas spp. from different municipal drinkingwater supplies in Sweden. Food Microbiol. 9:215-222.
Krovaceck, K. and M. Peterz. 1989. Enterotoxigenicity and drug sensitivity ofAeromonas hydrophila isolated from well water in Sweden: a case study. Mt. J. FoodMicrobiol. 8:149-154.

137
LeChevallier, M.W., Evans, T.M., Seidler, R.J., Daily, 0.P., Merrell, B.R., Rollins, D.M.and S.W. Joseph. 1982. Aeromonas sobria in chlorinated drinking water supplies.Microb. Ecol. 8:325-333.
Levesque, B., Pierre, S., Gauvin, D., Gingas, S., Dewailly, E. and R. Letarte. 1994.Comparison of the microbiological quality of water coolers and that of municipal watersystems. Appl. Environ. Microbiol. 60:1171-1178.
Macler, B.A. and S. Regli. 1993. Use of microbial risk assessment in setting UnitedStates drinking water standards. Int. J. Food Microbiol. 18:245-256.
Manaia, C.M., Nunes, 0.C., Morais, P.V. and M.S. Da Costa. 1990. Heterotrophic platecounts and the isolation of bacteria from mineral waters on selective andenrichment media. J. Appl. Bacteriol. 69:871-876.
Millership, S.E. and B. Chattopadhyay. 1985. Aeromonas hydrophila in chlorinated watersupplies. J. Hosp, Infect. 6:75-80.
Moyer, N.D. 1987. Clinical significance of Aeromonas species isolated from patientswith diarrhea. J. Clin. Microbiol. 25:2044-2048.
National Research Council. 1983. Risk assessment in the federal government: managingthe process. National Academy Press, Washington, DC.
Peterson, P.K. 1980. Host defense against Pseudomonas aeruginosa. p. 103-118. In HansHuber (ed.) Pseudmonas aeruginosa, the organism. Switzerland.
Pollack, M. 1990. Pseudomonas aeruginosa. p. 1673-1687. In Mandell, G.H., DouglasR.G. Jr., Benett, J.E. (ed.) Principles and practice of infectious diseases. Livingstone, NY.
Regli, S., Rose, J.B., Haas, C.N. and C.P. Gerba. 1991. Modeling the risk from Giardiaand viruses in drinking water. J. Amer. Water Works. Assoc. 83:76-84.
Rose, J.B. and C.P. Gerba. 1991. Use of risk assessment for the development of microbialstandards. Wat. Sci. Tech. 24:29-34.
Rose, J.B., Haas, C.N. and S. Regli. 1991. Risk assessment and control of waterbornegiardiasis. Amer. J. Pub. Hlth. 1:709-713.
Rose, J.B. 1997. Environmental ecology of Cryptosporodium and public healthimplications. Annu. Rev. Public Hlth. 18:135-161.

138
Roseberry, A.M. and D.E. Burmaster. 1992. Lognormal distribution for water intake bychildren and adults. Risk Anal. 12:99-104.
Rubin, L.G. 1987. Bacterial colonization and infection resulting from multiplication of asingle organism. Rev. Infect. Dis. 9:488-493.
Rusin, P.A., Rose, J.B., Haas, C.H. and C. P. Gerba. 1997. Risk assessment ofopportunistic bacterial pathogens in drinking water. Rev. Environ. Contam. Toxicol.152:57-83.
Sims, R.V., Hauser, R.J., Adewale, A.O., Maislin, G., Skeie, S., Lavizzo-Mourey, R.J.and H. Rubin. 1995. Acute gastroenteritis in three community-based nursing homes. J.Gerontol. A. Biol. Sci. Med. Sci. 50:M252-256.
Shooter, R.A., Cooke, E.M., Gaya, H., Kumar, P., Patel, N., Parker, T., Tham, T. andD.R. France. 1969. Food and medicaments as possible sources of hospital strains ofPseudomonas aeruginosa. LANCET. 1:1227-1229.
Slade, P.J., Falah, M.A. and A.M. Al-Ghady. 1986. Isolation of Aeromonas hydrophilafrom bottled waters and domestic water supplies in Saudi Arabia. J. Food Protect.49:471-476.
Steigbigel, N.H., Kislak, J.W., Tilles, J.G. and M. Finland. 1968. Clinical evaluation ofcephaloridine. Arch. Mt. Med. 121:24-38.
Tsai, G.J. and S.C. Yu. 1997. Microbiological evaluation of bottled water uncarbonatedmineral water in Taiwan. Mt. J. Food Microbiol. 37:137-143.
Weber, G., Werner, H.P. and H. Matsching. 1971. Death cases in newborns caused byPseudomonas aeruginosa contaminated drinking water. Zentralbl. Bakteriol. 216:210-214.

APPENDIX 5:
CONCLUSION
Cristobal Chaidez Quiroz
Department of Nutritional SciencesThe University of Arizona
Tucson, AZ. 85721
139

140
Microbial risk assessment is relatively new and has many potential applications in
risk management decisions. It can be used to evaluate treatment options and objectives,
guidelines and standards, as well as cost benefit analysis, and to competing risks. The
presented study in this dissertation shows how microbial risk assessment can be applied
to microbial water quality. Data from various drinking water sources were obtained for
microbial risk assessment. Quantitative microbial risk assessment was applied to offer
risk managers another means of interpreting water quality data. Attending the needs for
specific occurrence data, opportunistic bacterial pathogens were identified from point-of-
use (POU)-treated water, tap water with POU-connection, tap water, bottled water, and
water from vending machines and households storage tanks. The data were designed to
be used in the microbial risk assessment. The opportunistic bacterial pathogens, as
potential waterborne pathogens, were placed in a framework for use in risk
characterization.
Microbial risk assessment has only been used on a limited scale for assessing the
risk of infection from waterborne pathogens. Dose-response models for two specific
opportunistic bacterial pathogens (Aeromonas hydrophda and Pseudomonas aeruginosa)
have previously modeled (Rusin et al., 1997), and were applied to perform the risk
characterization in this study. The selected bacterial pathogens belong to the

141
heterotrophic plate count (HPC) bacteria and are commonly found in water. However,
there is no clear-cut evidence that EIPC bacteria as a whole pose a significant public
health risk. Therefore, it is necessary to evaluate specific opportunistic bacterial
pathogens when assessing drinking water quality. Opportunistic bacterial pathogens
continue to occur in drinking water and may pose a threat to segments of the population.
Opportunistic bacterial pathogens requires very specific immune defects in order for
people to become infected (colonized). Infection (colonization) outside these well-
defined groups are very rare. Therefore, under normal circumstances, the risk to the
general population from opportunistic bacteria is not significant. However in the specific
compromised patient, prevention, or early detection, and eradication of colonization are
likely to be more effective than attempting to control the number of opportunistic bacteria
due to the ubiquitous nature of the species, it is not practical to eliminate the species from
the drinking water.
More data is needed on the occurrence of specific opportunistic bacterial
pathogens in selected drinking water sources to fully assess the risks of HPC bacteria in
drinking water. Conventional methods as well as Molecular approaches should be
applied to identify clinical and environmental isolates. Although the assessment is made
based on assumptions. resulting in a large range of variations and uncertainity, the use of
microbial risk assessment approach can provide a better understanding of the public
health significance of the occurrence of bacteria in drinking water.

APPENDIX 6:
BACTERIAL DATA
Cristobal Chaidez Quiroz
Department of Nutritional SciencesThe University of Arizona
Tucson, AZ. 85721
142
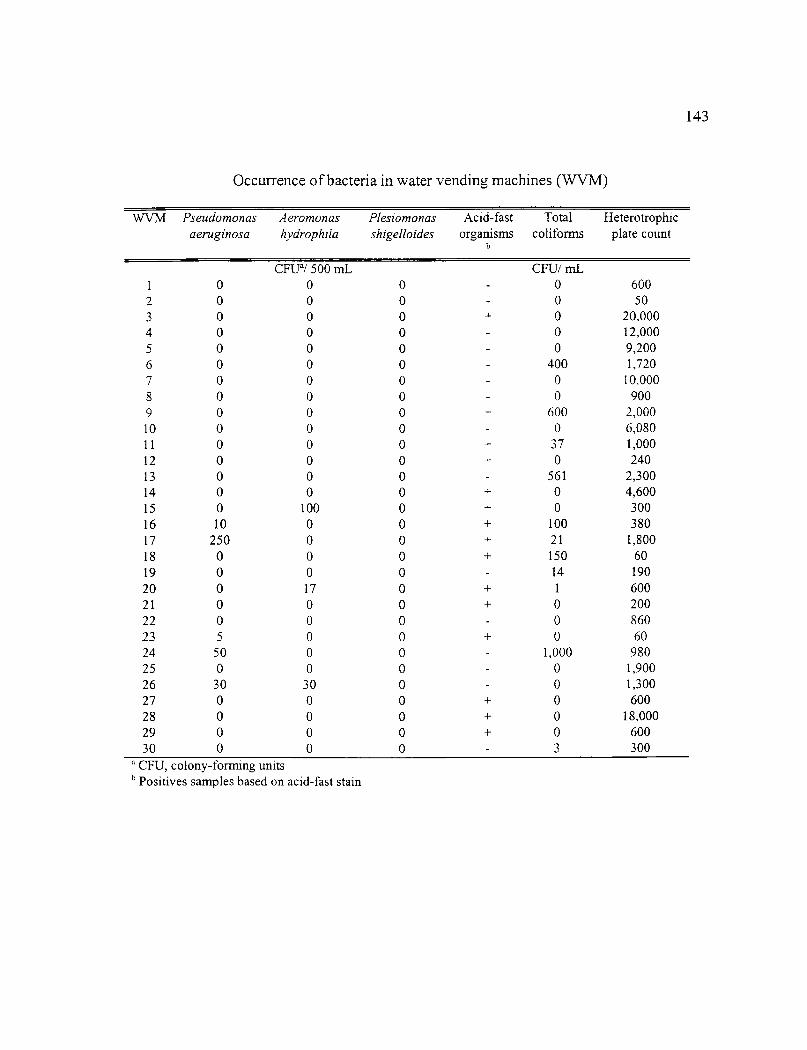
Occurrence of bacteria in water vending machines (WVM)
WVM Pseudomonasaeruginosa
Aeromonashydrophila
Plesiomonasshigelloides
Acid-fastorganisms
Totalcoliforms
Heterotrophicplate count
CFUa/ 500 mL CFU/ mL1 0 0 0 0 6002 0 0 0 0 503 0 0 0 + 0 20,0004 0 0 0 0 12,0005 0 0 0 0 9,2006 0 0 0 400 1,7207 0 0 0 0 10,0008 0 0 0 0 9009 0 0 0 + 600 2,00010 0 0 0 0 6,08011 0 0 0 + 37 1,00012 0 0 0 + 0 24013 0 0 0 561 2,30014 0 0 0 + 0 4,60015 0 100 0 + 0 30016 10 0 0 + 100 38017 250 0 0 + 21 1,80018 0 0 0 + 150 6019 0 0 0 14 19020 0 17 0 + 1 60021 0 0 0 + 0 20022 0 0 0 0 86023 5 0 0 + 0 6024 50 0 0 1,000 98025 0 0 0 0 1,90026 30 30 0 0 1,30027 0 0 0 + 0 60028 0 0 0 + 0 18,00029 0 0 0 + 0 60030 0 0 0 3 300
CFU, colony-forming unitsPositives samples based on acid-fast stain
143

144
Occurrence of bacteria in water storage tanks (WST)
Vv'STP. aeruginosaCFUa/100mL
Total coliformsCFU/100rnL
Fecal coliformsCFU/100mL
HPC bacteriaCFU/mL
1 0 1 0 625001 0 2 0 195003 0 0 0 725004 100 1 1 224000:_ 3 0 0 170006 2 0 0 5000007 0 20 20 2000008 10 10 10 2180009 3 0 0 40000010 5 120 0 63001 1 0 0 0 2300012 0 0 0 2000013 0 0 0 125014 0 0 0 14200015 0 0 0 155016 0 0 0 300017 1 0 0 15200018 0 15 15 10000019 0 0 0 30200020 0 15 3 600021 0 0 0 271022 0 0 0 56023 0 0 0 880024 0 0 0 800025 0 0 0 2500
' CFU, colony-forming units
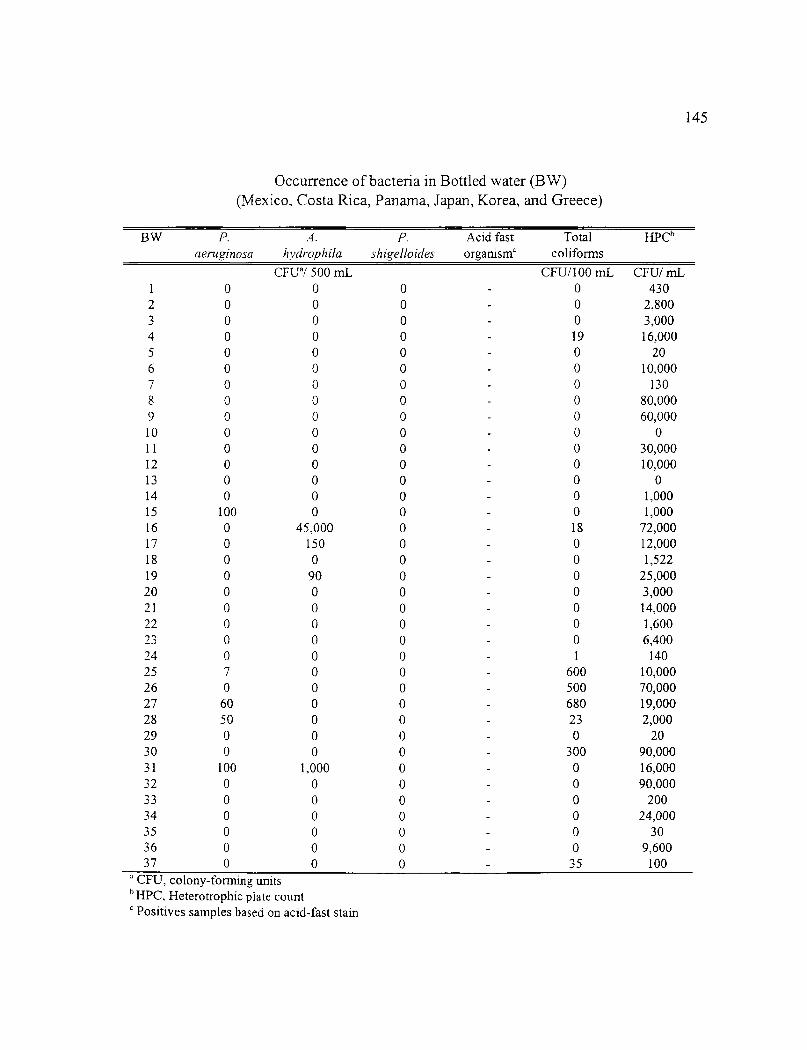
Occurrence of bacteria in Bottled water (BW)(Mexico, Costa Rica, Panama, Japan, Korea, and Greece)
BW P.aeruginosa
A.hydrophila
P. Acid fastshieelloides organism'
Totalcoliforms
HPC6
OE -Pi 500 mL CFU/100 mL CFU/ mL1 0 0 0 0 4302 0 0 0 0 2,8003 0 0 0 0 3,0004 0 0 0 19 16,0005 0 0 0 0 206 0 0 0 0 10,0007 0 0 0 0 1308 0 0 0 - 0 80,0009 0 0 0 - 0 60,00010 0 0 0 0 011 0 0 0 0 30,00012 0 0 0 - 0 10,00013 0 0 0 0 014 0 0 0 0 1,00015 100 0 0 0 1,00016 0 45,000 0 - 18 72,00017 0 150 0 - 0 12,00018 0 0 0 0 1,52219 0 90 0 0 25,00020 0 0 0 0 3,00021 0 0 0 0 14,00022 0 0 0 - 0 1,60023 0 0 0 - 0 6,40024 0 0 0 1 14025 7 0 0 600 10,00026 0 0 0 500 70,00027 60 0 0 - 680 19,00028 50 0 0 23 2,00029 0 0 0 0 2030 0 0 0 300 90,00031 100 1,000 0 0 16,00032 0 0 0 - 0 90,00033 0 0 0 - 0 20034 0 0 0 - 0 24,00035 0 0 0 - 0 3036 0 0 0 0 9,60037 0 0 0 - 35 100
a CFU, colony-forming unitsb HPC, Heterotrophic plate count
Positives samples based on acid-fast stain
145

Occurrence of bacteria in bottled water (BW)(United States)
(BW) P.aeruginosa
A.hydrophila
P.shigelloides
Acid-fastorganismsb
Totalcoliforms
Heterotrophicplate count
CFliaf 500 mL CFUI 100mL CFU/mL1 0 0 0 0 4,2002 0 0 0 0 1,1003 0 0 0 2 2,0004 0 0 0 0 15 0 0 0 0 106 0 0 0 0 207 0 0 0 -4- 0 1,9008 0 0 0 0 1,2009 0 0 0 + 0 0lo 0 0 0 + 0 2011 0 0 0 0 1,30012 0 0 0 0 4,00013 0 0 0 0 1014 0 0 0 + 0 3015 0 0 0 0 15016 10 0 0 0 28,00017 0 0 0 0 6018 0 0 0 0 4019 0 0 0 0 1020 0 0 0 0 2021 0 0 0 0 1,00022 0 0 0 0 1,20023 0 0 0 0 10,08024 0 0 0 0 30025 0 50 0 0 9,20026 0 0 0 0 90027 0 0 0 0 2,80028 0 0 0 0 20,00029 0 0 0 0 3,00030 0 0 0 0 26,80031 0 0 0 0 3032 0 0 0 0 033 0 0 0 0 3,60034 0 0 0 0 6,20035 0 0 0 - 60 8,000
CFU, colony-forming unitsb Positives samples based on acid-fast stain
146

Occurrence of bacteria in tap water (TW)(TUCSON, AZ)
TW P.aeruginosa
A.hydrophila
P. Acid fastshigelloides organisms .'
Totalcoliforms
Heterotrophicplate count
CFUa/500
Week #1
CFU/100mL
CFU/mL
1 0 0 0 0 202 0 0 0 0 3003 0 0 0 0 104 0 0 0 + 0 305 0 0 0 0 60
Week #26 0 0 0 + 0 38,0007 0 0 0 0 40,0008 0 0 0 0 50,0009 0 0 0 60 4,00010 0 100 0 80 50,000
Week #311 0 0 0 - 0 50,00012 0 0 0 0 20,00013 100 0 0 0 12,00014 0 0 0 0 15015 0 0 0 0 100
Week #416 10 0 0 0 13017 0 0 0 - 0 20018 0 0 0 - 0 30019 320 0 0 0 15020 0 0 0 0 20
Week #521 0 0 0 0 4,00022 0 0 0 0 15023 5 0 0 + 0 5,20024 0 0 0 + 0 10025 0 0 0 0 1,600
Week #626 0 0 0 0 35027 0 200 0 0 2028 0 0 0 0 6029 0 0 0 - 0 1,00030 3 0 0 0 1,200
a CFU, colony-forming unitsh Positives samples based on acid-fast stain
147
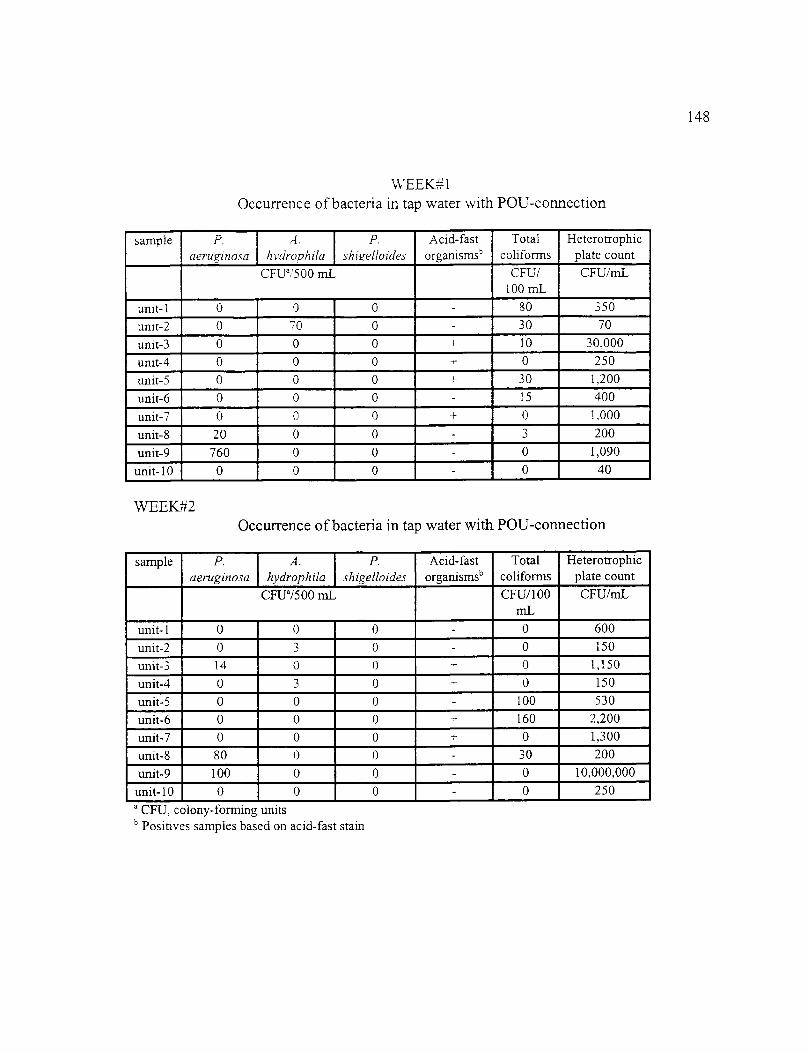
WEEK#1Occurrence of bacteria in tap water with POU-connection
sample P.aeruzinosa
.4.hydrophda
P.shigelloides
Acid-fastorganisms'
Totalcoliforms
Heterotrophicplate count
CFUa/500 mL CFU/100 mL
CFU/rnL
unit-1 0 0 0 - 80 350
unit-2 0 70 0 - 30 70
unit-3 0 0 0 + 10 30,000
unit-4 0 0 0 0 250
unit-5 0 0 0 30 1,200
unit-6 0 0 0 - 15 400
unit-7 0 0 0 0 1,000
unit-8 20 0 0 - 3 200
unit-9 760 0 0 - 0 1,090
unit-10 0 0 0 - 0 40
WEEK#2Occurrence of bacteria in tap water with POU-connection
sample P.aeruginosa
A.hydrophila
P.shigelloides
Acid-fastorganisms'
Totalcoliforms
Heterotrophicplate count
CHP/500 mL CFU/100niL
CFU/mL
unit-1 0 0 - 0 - 0 600
unit-2 0 3 0 - 0 150
unit-3 14 0 0 .,- 0 1,150
unit-4 0 3 0 0 150
unit-5 0 0 0 - 100 530
unit-6 0 0 0 160 2,200
unit-7 0 0 ' 0 + 0 1,300
unit-8 80 0 0 - 30 200
unit-9 100 0 0_ - 0 10,000,000
unit-10 0 0 0 - 0 250
CFU, colony-forming unitsPositives samples based on acid-fast stain
148
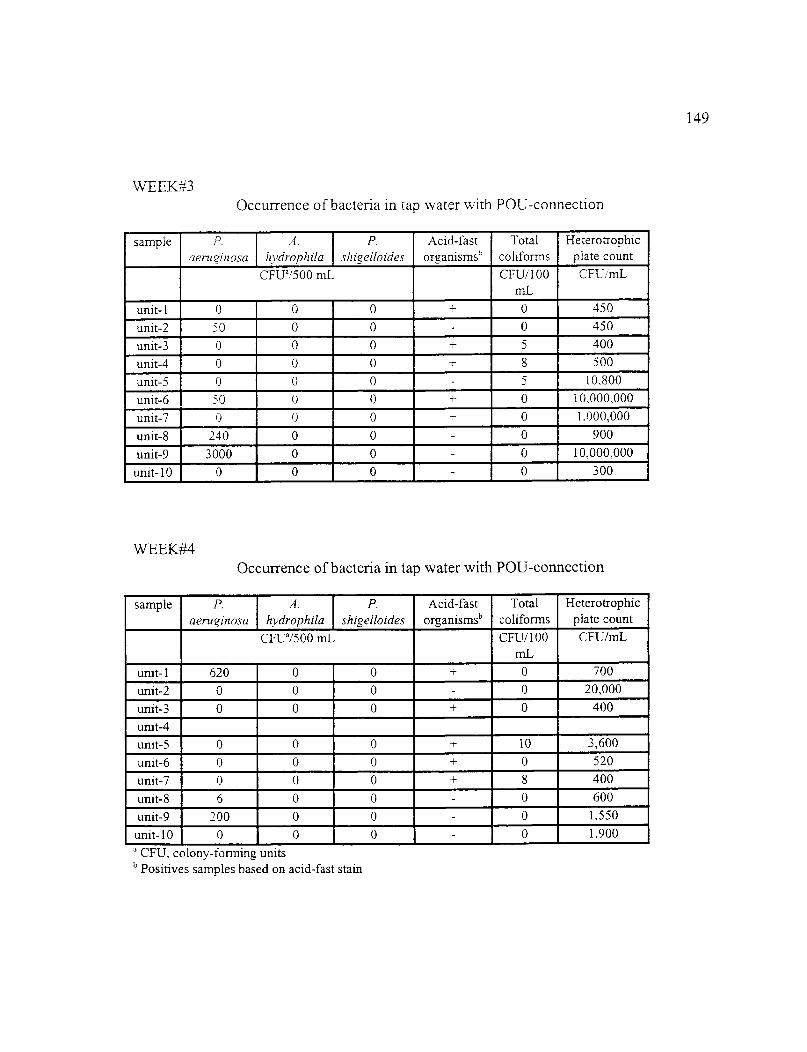
VvIEK#3Occurrence of bacteria in tap water with POU-connection
sample P.aeruginosa
A.hydrophda
P.shigeiloides
Acid-fastorganisms'
Totalcoliforms
Heterotrophicplate count
CFUa/500 mL CFU/100raL
CFU/ML
unit-1 0 0 0 A- 0 450
unit-2 50 0 0 - 0 450
unit-3 0 0 0 5 400
unit-4 0 0 0 8 500
unit-5 0 0 0 5 10,800
unit-6 50 0 0 -,- 0 10,000,000
unit-7 0 0 0 0 1.000,000
unit-8 240 0 0 - 0 900
unit-9 3000 0 0 - 0 10,000,000
unit-10 0 0 0 - 0 300
WEEK#4Occurrence of bacteria in tap water with POU-connection
sample P.aeruginosa
A.hydrophda
P.shigelloides
Acid-fastorganisms'
Totalcoliforms
Heterotrophicplate count
CFUa/500 mL CFU/100mL
CFU/mL
unit-1 620 0 0 0 700
unit-2 0 0 0 - 0 20,000
unit-3 0 0 0 + 0 400unit-4unit-5 0 0 0 + . 10 3,600
unit-6 0 0. 0- + 0 520
unit-7 0 0 0 + 8 400
unit-8 6 0 0 0 600
unit-9 200 0 0 - 0 1,550
unit-10 0 0 0 - 0 1,900
CFU, colony-forming unitsb Positives samples based on acid-fast stain
149

WEEK#5Occurrence of bacteria in tap water with POU-connection
sample P.aeruginosa
.4.hydrophda
P.shigelloides
Acid-fastorganisms b
Totalco1iforms
Heterotrophicplate count
CFL;a/500 mL CPU/100mL
CFU/mL
unit-1 0 0 0 0 1,500
unit-2 0 5 0 - 0 200
unit-3 0 0 0 - 0 4,000
unit-4unit-5 30 0 0 - 10 2,000
unit-6 200 0 0 - 0 3,500
unit-7 0 0 0 - 0 380
unit-8 10 0 0 - 0 500
unit-9 300 0 0 - 57 2,500
unit-10 0 0 0 - 0 100
WEEK#6Occurrence of bacteria in tap water with POU-connection
sample P.aeruginosa
A._ hydrophila
P.shigelloides
Acid-fastorganisms b
Totalconforms
Heterotrophicplate count
CFtia/500 mL CFU/100rnL
CFU/mL
unit-1 0 0 0 - 30 450unit-2 0 10 0 - 0 20,000,000
unit-3 0 0 0 + 0, 100
unit-4 .unit-5 60 8 0 - 320 14,000
unit-6 80 — 0 0 -_
0 16,000unit-7 0 0 0 - - 0 1,600
unit-8 0 0 0 - 0 4,000
unit-9 120 - 0 0 - 15 16,000unit-10 0 0 - 0 - 0 200
CFU, colony-forming unitsb Positives samples based on acid-fast stain
150

WEEK#1Occurrence of bacteria in Point-Of-Use (POU)-treated water
sample P.aeruginosa
A.hydrophila
P.shigelloides
Acid-fastorganisms'
Totalcoliforms
Heterotrophicplate count
CFUN500 mL CFU/100mL
CFU/mL
unit-1 0 0 0 100 700
unit-2 0 0 0 - 14 400
unit-3 0 0 0 - 16 10,000
unit-4 0 0 0 + 5 150unit-5 0 0 0 - 260 30,000,000
unit-6 30 0 ' 0 340 2,000,000
unit-7 0 0 0 - 0 2,600unit-8 0 0 0 - 240 1,200unit-9 240 0 0 - 0 4,000
unit-10 400 0 0 + 100 120
WEEK#2Occurrence of bacteria in Point-Of-Use (POU)-treated water
sample P.aeruginosa
A.hydrophila
P.shigelloides
Acid-fastorganisms'
Totalcoliforms
Heterotrophicplate count
CFUa/500 rnL CFU/100mL
CFU/mL
unit-1 0 () 0 - 200 80,000unit-2 4 2 8 0 - 70 30,000unit-3 25 0 0 + 35 30,000,000
unit-4 0 0 0 + 62 40,000unit-5 150 0 0 — 140 100
unit-6 74 0 0 + 260 7,400unit-7 0 0 0 - 0 30,000,000unit-8 0 0 0 - 145 1,400unit-9 100 0 0. -. 0 510
unit-10 0 0 0 - 150 4,000CFU, colony-forming units
b Positives samples based on acid-fast stain
151

"vVEEK#3Occurrence of bacteria in Point-Of-Use (POU)-treated water
sample P.aeruginosa
A.hydrophda
P.shigelloides
Acid-fastorganisms'
Totalcoliforms
Heterotrophicplate count
CFUa/500 mL CFU/100mL
CFU/mL
unit-1 0 0 0 — 800 8,000
unit-2 15 0 0 — 35 350
unit-3 100 0 0 180 4,000unit-4 0 0 0 62 900
unit-5 0 0 0 - 10 4,700
unit-6 100 0 0 161 28,000
unit-7 0 0 0 - 507 900
unit-8 0 0 0 - 3 750
unit-9 3500 0 0 - 0 4,000
unit-10 0 0 0 -1- 480 3,200
WEEK#4Occurrence of bacteria in Point-Of-Use (POU)-treated water
sample P.aeruginosa
A.hydrophila
P.shigelloides
Acid-fastorganisms'
Totalcoliforms
Heterotrophicplate count
CFUa/500 mL CFU/100mL
CFU/mL
unit-1 0 0 0 0 4,560
unit-2 6 0 . 0 - 10 25,000,000
unit-3 0 0 - 0 - 10 1,800unit-4
unit-5 0 0 0, 80 6,400
unit-6 10 0 0, + 20 40,000,000
unit-7 0 0 0 - 130 1,000unit-8 0 0 0 - 62 2,000
unit-9 190 0 0 - 0 8,800unit-10 0 0 0 - 60 7,600CFU, colony-forming units
" Positives samples based on acid-fast stain
152

WEEK#5Occurrence of bacteria in Point-Of-Use (POU)-treated water
sample P.aerueinosa
A.hvdrophila
P.shigelloides
Acid-fastorganisms'
Totalcoliforms
Heterotrophicplate count
CR. /500 m_L CFU/100mL
CFU/mL
unit-1 10 0 0 ± 17 500unit-2 100 25 0 500 2,500unit-3 0 0 0 - 25 5,600unit-4
unit-5 0 0 0 194 18,000unit-6 100 0 0 + 32 15,000unit-7 0 0 0 100 1.200unit-8 0 0 0 + 0 10,000,000unit-9 266 0 0 - 0 400
unit-10 0 0 0 -t- 300 6,000
WEEK#6Occurrence of bacteria in Point-Of-Use (POU)-treated water
sample P.aeruginosa
A.hydrophila
P.shigelloides
Acid-fastorganisms'
Totalcoliforms
Heterotrophicplate count
CFUa/500 mL CFU/100rnL
CFU/mL
unit-1 0 0 0 + 130 12,000unit-2 100 1,600 0 - 50 20,000,000unit-3 0 0 0 - 0 1,000unit-4
unit-5 0 30 0 - 1,000 16,800unit-6 120 0 0 610 16,400unit-7 0 0 0 - 84 2,400unit-8 0 0 0 - 5 4,400unit-9 180 0 0 - 30 2,000,000
unit-10 0 0 0 - 80 400CFU, colony-forming unitsPositives samples based on acid-fast stain
153
154
REFERENCES
Alonso, J.L., Garay, E. and E. Hernandez. 1989. Membrane filter procedure for theenumeration of Pseudomonas aeruginosa in water. Wat. Res. 23:1499-1502.
Altwegg, M., Reeves, R., Altwegg-Bissig, R. and D.J. Brenner. 1991. Multilocus enzymeanalysis of the genus Aeromonas and its use for specific identification. Zentralbl.Bakteriol. 257:28-45.
American Public Health Association (APHA). 1995. Standard Methods for theExamination of Water and Wastewater, 18 ed. Washington, DC.
Arai, T., Ikejima, N., Itoh, T., Sakai, S., Shimada, T. and R. Sakazaki. 1980. A survey ofPlesiomonas shigelloides from aquatic environments, domestic animals, pets andhumans. 1 Hyg. Camb. 84:203-211.
Bermudez, L.E., Petrotsky, M., Koloski, P. and L.S. Young. 1992. An animal model ofMycobacterium avium complex disseminated infection after colonization of the intestinaltract. J. Infect. Dis. 165:75-79.
Bergogne-Berezin, E. 1994. Acinetobacter spp., saprophytic organisms of increasingpathogenic importance. Zentralbl. Bakteriol. 281:389-405.
Bert, F., Maubec, E., Bruneau, B. and N. Lambert-Zechovosky. 1998. Multi-resistantPseudomonas aeruginosa outbreak associated with contaminated tap water in aneurosurgery intensive care unit. J. Hosp. Infect. 39:53-62.
Bitton, G. 1994. Wastewater Microbiology. Wiley-Liss. NY.
Bodey, G.P., Bolivar, R., Faisten, V. and L. Jadeja. 1983. Infections caused byPseudomonas aeruginosa. Rev. Infect. Dis. 5:279-313.
Brown, L.M. and J. Gauthier. 1993. Cell density and growth phase as factor in theresistant of a biofilm of Pseudomonas aeruginosa (ATCC 27853) to iodine. Appl.Environ. Microbiol. 59:2320-2322.
Buck, A.C. and E.M. Cooke. 1969. The fate of ingested Pseudomonas aeruginosa innormal persons. J. Med. Microbiol. 2:521-525.
Cabelli, V.J. 1978. Swimming-associated disease outbreaks. Water Poll. Control Fed. J50:1374-1377.

155
Caroli, G., Levre, E., Armani. G., Biffi-gentili, S. and G. Molonari. 1985. Search for acid-fast in bottled water. J. Appl. Bacteriol. 58:461-464.
Celis, R., Torres, A., Gatell, J.M. and M. Alnela. 1988. Nosocomial pneumonia amultivariate analyses of risk and prognosis. Chest. 93:318-324.
Center for Disease Control. 1982. Otitis due to Pseudomonas aeruginosa 0:10 associatedwith a mobile redwood tub system-North Carolina. Morbid. Mortal. Weekly Rep. 31 :541-542.
Chaidez, C. and C.P. Gerba. 1998. Microbiological comparison of the quality of POU-treated water, tap water, and bottled water. University of Arizona, Tucson, AZ.(unpublished report).
Chaidez, C., Rusin, P.A., Naranjo, J. and C.P. Gerba. 1997. Microbiological quality ofwater vending machines. Int. I Environ. Hlth. In press.
Chin, D.P. Hopewell, P.C., Yajko, D.M., Vittinghoff, E., Horsburgh, C.R. jr., Hadley,W.K., Stone, E.N., Nassos, P.S., Ostroff, S.M., Jacobsono, M.A., Matkin, C.C. and A.L.Reingold. 1994. Mycobacterium avium complex in the respiratory or gastrointestinal tractand the risk of M avium bacteremia in patients with human immunodeficiency virusinfection. J. Infect. Dis. 169:289-295.
Clark, J.A., Burger, C.A. and L.E. Sabatinos. 1982. Characterization of indicator bacteriain municipal raw water, drinking water and new main water samples. Can. J. Microbiol.28:1002-1013.
Collins, C.H., Grange, J.M. and M.D. Yates. 1984. Mycobacteria in water. J. App!.Bacteriol. 57:193-211.
Cooper, R.G. and G.W. Brown. 1968. Plesiomonas shigelloides in south Australia. J.Clin. Pathol. 21:715-718.
Dennis, P.J.L., Lee, J.V., Walker, J.T., West, A.A. and C.W. Keevil. 1989. Biofilms:Detection, implications, and solutions. Watershed 89: The future for water quality inEurope. Vol. II. Pergamon press. New York, NY.
Difco laboratories. 1984. Difco manual: dehydrated culture media and reagentsfor microbiology, 10' ed. Difco laboratories, Detroit, MI.
Dooley, J.R., Nims, L.J., Lipp, V.H., Beard, A. and L.T. Delancy. 1980. Meningitis ofinfants caused by Flavobacterium meningosepticum. I Trop. Ped. 26:24-30.

156
Du Moulin, G.C., Sherman, I.H., Hoaglin, D.C. and K.D. Stottmeier. 1985.Mycobacterium avium complex, an emerging pathogen in Massachusetts. J. Clin.Microbiol. 22:9-12.
Du Moulin, G.C., Stottmeier, K.D., Pelletier, P.A., Tsang, A.Y. and J. Hedley-White.1988. Concentration of Mycobacterium avium by hospital hot water systems. JAMA.260:1599-1601.
Du Moulin, G.C. and K.D. Stottmeier. 1978. Use of cetylpiridinium chloride in thedecontamination of water for culture of Mycobacteria. App!. Environ. Microbiol. 36:771-773.
Dupont, H.L., C. Chappell, C. Sterling, P. Okhuysen, J.B. Rose and W. Jakubowski.1995. Infectivity of Cryptosporidium parvum in healthy individuals volunteers. N. Eng. J.Med. 332, 885, 1.
Edberg, S.C., Gallo, P. and C. Kontnick. 1996. Analysis of the virulence characteristicsof bacteria isolated from bottled water, water cooler, and tap water. Microbial Eco!. Hlth.Dis. 9:67-77.
Environmental Protection Agency (EPA). 1989. Drinking water health effects task force.Health effects of drinking water treatment technologies. Lewis Pubs. Chelsea, MI.
Favero, M.S., Carson, L.A. Bond, W.W. and N.J. Petersen. 1971. Pseudomonasaeruginosa: Growth on distilled water from hospitals. Science. 173:836-838.
Fewtrell, L., Kay, D., Wyer, M., Godfree, A. and G. O'neall. 1997. Microbiologicalquality of bottled water. Wat. Sci. Tech. 35:47-53.
Fick, R.B. 1993. Pseudomonas aeruginosa: The opportunist. CRC press.
Freund, S.M., Koburger, J.A. and C.I. Wei. 1988. Enhanced recovery of Plesiomonasshigelloides following an enrichment technique. J. Food Protect. 51:110-112.
Geldreich, E.E. 1996. Microbial quality of water supply in distribution systems. CRC,Boca Raton, FL.
Geldreich, E.E. 1986. Potable water: New directions in microbial regulations. ASM news.52:530-534.

157
Geldreich, E.E., Nash, H.D., Reasoner, D.J. and R.H. Taylor. 1975. The necessity ofcontrolling bacterial population in potable water-bottled water, and emergency watersupplies. J. Amer. Water Works Assoc. 67:117-124.
Gerba, C.P. and C. N. Haas. 1988. Assessment of risks associated with enteric viruses incontaminated drinking water. American society for testing and materials. Philadelphia, p.489-494.
Gerba, C.P., J.B. Rose, C.N. Haas and K.D. Crabtree. 1996. Waterborne rotavirus: a riskassessment. Wat. Res. 30:2929-2940.
George, S.E., Kohan, M.J., Walsh, D.B., Stead, A.G. and L.D. Claxton. 1989.Polychlorinated phenyl-degrading Pseudomonads: Survival in mouse intestines andcompetition with normal flora. J. Toxicol. Environ. Hlth. 26:19-37.
George, W.L., Nakata, M.M., Thompson, J. and M.L. White. 1985. Aeromonas-relateddiarrhea in adults. Arch. Intern. Med. 145:2207-2211.
George, K.L., Parker, B.C., Grufth, H. and J.O. Falkinham III. 1980. Epidemiology ofinfection by non-tuberculous Mycobacteria. Am. Rev. Respir. Dis:122:89-94.
Gilligan, P.H. 1995. Pseudomonas and Burkholderia. p. 509-519. In ASM press (ed.)Manual of clinical microbiology. Washington, DC.
Gilligan, P.H. 1991. Microbiology of airway disease in patients with cystic fibrosis. Clin.Microbiol. Review. 4:35-51.
Gleeson, C. and N. Gray. 1997. The Coliform Index and Waterborne Disease. E and FNSpon (ed.). U.K.
Glover, N., Holtzman, A., Aronson, T., Fromm, S., Brolin, 0.G.W., Dominguez, P.,Kunkel, K.A., Overturf, G., Stelma, G., Smith, C. and M. Yakrus. 1994. The isolation andidentification of Mycobacterium avium complex (MAC) recovered from Los Angelespotable water, a possible source of infection in AIDS patients. Mt. J. Environ. Hlth. Res.4:63-72.
Gonzalez, C. Gutierrez, C. and T. Grande. 1987. Bacterial flora in bottled uncarbonatedmineral drinking water. Can. J. Microbiol. 33:1120-1125.
Goslee, S. and E. Wolinsky. 1976. Water as a source of potentially pathogenicMycobacteria. Am. Rev. Respir. Dis. 113:287-292.

158
Grabow, W.O.K., Burger, J.S. and E.M. Nupen. 1980. Evaluation of acid-fast bacteria,Candida albicans, enteric viruses and conventional indicators for monitoring wastewaterreclamation system. Prog. Water Tech. 12 :803-817.
Graham, L., Warren, N.G., Tsang, A.Y. and H.P. Dalton. 1988. Mycobacterium aviumcomplex pseudobacteriuria from a hospital water supply. J. Clin. Microbiol. 26:1034-1036.
Haas, C.N. 1983. Estimation of risk due to low doses of microorganisms: a comparison ofalternatives methodologies. Amer. J Epidemiol 118:537-582.
Haas, C.N., J.B. Rose, C.P. Gerba and S. Regli. 1993. Risk assessment of virus indrinking water. Risk Anal. 13:545-552.
Haas, C.N., C.S. Crockett, J.B. Rose, C.P. Gerba and A.M. Fazil. 1996. Assessing therisk posed by oocysts in drinking water. J Amer. Water Assoc. 9:131-136.
Handfield, M., Simard, P., Coullard, M. and R. Letarte.1996. Aeromonas hydropilaisolated from food and drinking water: Hemaglutination, hemolysis, and cytotoxity for ahuman intestinal cell line (HT-29). App!. Environ. Microbiol. 62:3459-3461.
Hardalo, C. and S.C. Edberg. 1997. Pseudomonas aeruginosa: Assessment of risk fromdrinking water. Critical Rev. Microbiol. 23:47-75.
Havelaar, A.H. and M. Vonk. 1988. The preparation of ampicillin dextrin agar for theenumeration of Aeromonas in water. Lett. App!. Microbiol. 7:169-171.
Hernandez-Duquino, H. and I.A. Rosenberg. 1987. Antibiotic resistant Pseudomonas inbottled drinking water. Can. J Microbiol. 33:286-289.
Hernandez, P. and R. Rodriguez de Garcia 1997. Prevalence of Plesiomonas shigelloidesin surface waters. Arch. Lat. Nutr. 47:47-49.
Herrington, D.A., Tzipori, S., Robins-Browne, R.M., Tall, B.D. and M.M. Levine. 1987.In vitro and in vivo pathogenicity of Plesiomonas shigelloides. Infect. Immun. 55:979-985.
Hoadley, A. W. 1977. Pseudomonas aeruginosa in surface waters. p. 31-57. In young,V.M. Raven press (ed.) Pseudomonas aeruginosa: ecological aspects and patientscolonization. New York, NY.
159
Holmberg, S.D., Shell. W.L., Fanning, G.R., Wachsmoth, I.K., Hiickman, Brenner, F.W.and P.A. Blake. 1986. Aeromonas intestinal infections in the United States. Ann. Intern.Med. 105:109-114.
Holtanan, A.E., Aronson, T.W., Glover, N., Froman, S., Stelma, G.N., Sebata, S.N.,Boian, M.G. and 0.G.W. Berlin. 1997. Examination of bottled water for non-tuberculousMycobacteria. J Food Protect. 60:185-187.
Horsburgh, C.R. 1991. Mycobacterium avium complex infection in the acquiredimmunodeficiency syndrome. N. Engl. J. Med. 19:1332-1338.
Hunter, P.R. 1994. Bottled natural mineral water and other bottled waters. Micro biol.Europe. 2(4):8-10.
Hunter, C.A. and P.R. Ensign. 1947. An epidemic of diarrhea in a newborn nurserycaused by Pseudomonas aeruginosa. Amer. J. Public Hlth. 37:1166-1169.
Janda, J.M. 1991. Recent advances in the study of the taxonomy, pathogenicity, andinfectious syndromes associated with the genus Aeromonas. Clin. MicrobioL Rev.4:397-410.
Janda, J.M., Abbott, S.L. and A.M. Carnahan. 1995. Aeromonas and Plesiomonas. p.477-482. In ASM press (ed.) Manual of clinical microbiology. Washington, DC.
Janda, J.M. and P.S. Duffey. 1988. Mesophilic Aeromonads in human disease: Currenttaxonomy, laboratory and infections disease spectrum. Rev. Infect. Dis. 10:980-997.
Jeppesen, C. 1995. Media for Aeromonas spp., Plesiomonas spp.and Pseudomonas spp.from and the environment. Int. J. Food Microbiol. 26:25-41.
Jones, A.R., Bartlett, J. and J.G. McCormack. 1995. Mycobacterium avium complex(MAC) osteomyelitis and septic arthritis in immunocompetent host. J. Infect. 30:59-62.
Kirschner, R.A. jr., Parker, B.0 and J.O. III Falkinham. 1992. Mycobacterium avium,Mycobacterium intracellulare, and M scrofulaceum in acid brown-water swamps of thesoutheastern United States and their association with environmental variables. Am. Rev.Respir. Dis. 145:271-275.
Kominos, S.D., Copeland, C.E., Grosiak, B. and B. Postic. 1972. Introduction ofPseudomonas aerugmosa into a hospital via vegetables. App!. Microbiol. 24:567-570.
160
Koprowski, H. 1956. Immunization against poliomyelitis with living attenuated virus.JAMA 160:954-966.
Korvick, J. 1996. Mycobacterium avium complex infection. Marcel Dekker (ed.), NewYork, NY.
Kubica. G.P. and L.G. Wayne. 1984. The Mycobacteria. Marcel Dekker (ed.), New York,NY.
Kuijper, E.J., Van Alphen, L., Leenders, E. and H.C. Zanen. 1989. In vitro susceptibiltiesof tropical strains of Aeromonas species from Queensland, Australia. to 22 antimicrobialagents. J Clin. Microbiol. 27:1280-1285.
Kwaga, J.K., Adesiyun, A.A., Bello, C.S. and S.U. Abdullahi. 1988. Occurrence ofPlesiomonas shigelloides in humans and water in Zaria, Nigeria. Microbiologica. 11:165-167.
LeChevallier, M.W., Evans, T.M., Seidler, R.J., Daily, 0.P., Merrell, B.R., Rollins, D.M.and S.W. Joseph.1982. Aeromonas sobria in chlorinated drinking water supplies. Microb.Ecol. 8:325-333.
LeChevallier, M.W., Seidler, R.J. and T. M. Evans. 1980. Enumeration andcharacterization of standard plate count bacteria in chlorinated and raw water supplies.App!. Environ. Microbiol. 40:922-930.
Levesque, B., Pierre, S., Gauvin, D., Gingras, S., Dewailly, E. and R. Letarte. 1994.Comparison of the microbiological quality of water coolers and that of municipal watersystems. Appl. Environ. Microbiol. 60:1171-1178.
Liesenfeld, O., Weinke, T. and H. Hahn. 1993. Three-year prevalence ofenteropathogenic bacteria in an urban population in Germany. Infect. 21:101-105.
Lombardo, L.R., West, P.R. and J.L. Holbrook. 1985. A comparison of various mediaand incubation temperatures used in the heterotrophic plate count analysis. Water Quai.Tech. Conf, Amer. Water Works Assoc. Denver, CO. p.251-270.
Lynkins, B.U., Clark, R.M. and A.G. James. 1992. Point-of-use/point-of-entry fordrinking water treatment. Lewis, Chelsea, MI.
Macler, B.A. and S. Regli. 1993. Use of microbial risk assessment in setting UnitedStates drinking water standards. Int. J Food MicrobioL 18:245-256.

161
Manaia, C.M., Nunes, O.C. , Morais, P.V. and M.S. Da Costa. 1990. Heterotrophic platecounts and the isolation of bacteria from mineral waters on selective andenrichment media. J. Appl. Bacteriol. 69:871-876.
Mansfield, K.G. and A.A. Lackner. 1997. Simian immunodeficiency virus-inoculatedmacaques acquire Mycobacterium avium from potable water during AIDS. J Infect.175:184-187.
Martinetti, L. and M. Altwegg. 1992. rRNA gene restriction pattern as taxonomic toolsfor the genus Aeromonas. Int. J. Syst. Bacteriol. 24:384-389.
McFeters, G.A. 1990. Drinking water microbiology. G.A. McFeters (ed.), SpringerVerlag. New York, NY.
Medema, G. and C. Schets. 1993. Occurrence of Plesiomonas shigelloides in surfacewater: relationship with fecal pollution and trophic state. Zentralbl. Hyg. Umweltmed.194:398-404.
Meitert, E.A., Vlad, A. and E. Sima. 1984. Food Poisoning associated with Pseudomonasaeruginosa. Arch. Roum. Pathol. Exp. Microbiol. 43:115-119.
Miller, L.M. and J.A. Koburger.1985. Plesiomonas shigelloides: An opportunistic foodand waterborne pathogen. J. Food Protect. 48:449-457.
Morbidity and Mortality Weekly Report (MMWR). 1998. Plesiomonas shigelloides andSalmonella serotype Hartford infections associated with contaminated water supply-Livingstone County, NY. MMWR. 47:349-396.
Morgan, D.R., Johnson, P.C., DuPont, H.L., Satterwhite, T.K. and L.V. Wood. 1985.Lack of correlation between known virulence properties of Aeromonas hydrophila andenteropathogenicity for humans. Infect. Immun. 50:62-65.
Moyer, N.D. 1987. Clinical significance of Aeromonas species isolated from patientswith diarrhea. J Clin. Microbiol. 25:2044-2048.
Murphey, S.A, Jungkind, D.L. and E. Adams. 1983. Mycobacterium avium-intracellularein a hospital hot water system: epidemiological investigation. In: Proceedings andabstracts of the 2nd Interscience Conference on Antimicrobial Agents and Chemotherapy,Las Vegas. Washington, DC: American Society for Microbiology, p. 277.
National Research Council. 1983. Risk assessment in the federal government: managingthe process. National Academy Press, Washington, DC.

162
National Research Council. 1994. Science and judgment in risk assessment. NationalAcademy Press, Washington, DC.
Nolte, F. and B. Metchock. 1995. Mycobacterium. p. 400-437. In Murray R.R. (ed.).Manual of clinical microbiology. American society for microbiology. Washington DC.
Ogan, M. 1992. Microbiological quality of bottled water sold in retail in Nigeria. J App!.Bacteriol. 73:175-181.
Palleroni, N.J. 1984. Genus I Pseudomonas migula 1894, 237AL , p. 141-199. In N.R.Kreig and J.G. Holt (ed.) Bergey's Manual of Systematic Bacteriology. Baltimore.
Payment, P., Franco, E. and Siemiatycki. 1991. Gastrointestinal health effects associatedwith the consumption of drinking water produced by point-of-use domestic reverseosmosis filtration unites. App!. Environ. Microbiol. 57:945-948.
Payment, P., Gamache, F. and G. Paquette. 1988. Microbiological and virologicalanalysis of water from two filtration plants and their distribution system. Can. J.Microbiol. 34:1304-1309.
Payment, P., Siemiatycki, J., Richardson, L., Renaud, G., Franco, E. and M. Prevost.1997. A prospective epidemiological health effects due to the consumption of drinkingwater. Int. J. Environ. Hlth. Res. 7:5-31.
Peters, M., Muller, C., Rusch-Gerdes, S., Seidel, C., Gobe!, U., Pohle, H.D. and B. Ruf.1995. Isolation of atypical Mycobacteria from tap water in hospitals and homes: Is this apossible source of disseminated MAC infection in AIDS patients. J. Infect. 31:39-44.
Pollack, M. 1990. Pseudomonas aeruginosa. p. 1673-1687. In Mandell, G.H., DouglasR.G. Jr., Benett, J.E. (ed.) Principles and practice of infectious diseases. Livingstone, NY.
Prince, D.S., Peterson, D.D., Steiner, R.M., Gottlieb, J.E., Scott, R., Israel, H.L.,Figueroa, W.G. and J.E. Fish. 1989. Infections with Mycobacterium avium complex inpatients without predisposing factors conditions. N. Engl. J. Med. 321:863-868.
Rautelin, H., Sivanen, A., Kuikka, A., Renkonen, U.V., Valtonen, V. and T.V. Kosunen.1995. Enteric Plesiomonas shigelloides infections in Finnish patients. Scand. J. Infect.Dis. 27:495-498.
Reasoner, D.J. 1990. Monitoring heterotrophic bacteria in potable water. p. 452-477 InDrinking water microbiology. Gordon A. McFeters (ed.) Spring-Verlag. NY.

163
Reasoner, D.J., Blannon, J.C., Geldreich, E.E. and J. Barnick. 1989. Non-photosyntheticpigmented bacteria in a potable water treatment and distribution system. App!. Environ.Microbiol. 55:912-921.
Reasoner, D.J. and E.E. Geldreich. 1985. A new medium for the enumeration andsubculture of bacteria from potable water. App!. Environ. Microbiol. 49:1-7.
Regli, S., Rose, J.B.. Haas, C.N. and C.P. Gerba. 1991. Modeling the risk from Giardiaand viruses in drinking water. J. Amer. Water Works. Assoc. 83:76-84.
Ridgway, H.F. and B.H. Olson. 1982. Chlorine resistant patterns of bacteria from twodrinking water distribution systems. App!. Environ. Microbiol. 44:972-987.
Ridgway, H.F., Rigby, M.G. and D.G. Argo. 1985. Bacterial adhesion and fouling ofreverse osmosis membranes. J Amer. Water Works Assoc. 97:106-109.
Rippey, S.R. and V.J. Cabelli. 1979. Membrane filter procedure for enumeration ofAeromonas hydrophila in fresh water. App!. Environ. Ann. Intern. Med. 38:180-113.
Rose, J.B. and C.P. Gerba. 1991. Use of risk assessment for the development of microbialstandards. Wat. Sci. Tech. 24:29-34.
Rose, J.B., Haas, C.N. and S. Regli. 1991. Risk assessment and control of waterbornegiardiasis. Amer. J. Pub. Hlth. 1:709-713.
Roseberry, A.M. and D.E. Burmaster. 1992. Lognormal distribution for water intake bychildren and adults. Risk Anal. 12:99-104.
Rosenzweig, D.Y. and D.P. Schlueter. 1981. Spectrum of clinical disease in pulmonaryinfections with Mycobacterium avium-intracellulare. Rev. Infect. Dis. 3:1046-1052.
Rusin, P.A., Rose, J.B., Haas, C.H. and C. P. Gerba. 1997. Risk assessment ofopportunistic bacterial pathogens in drinking water. Rev. Environ. Contam. Toxicol.152:57-83.
Rutala, W.A., Sarubbi, F.A. jr., Finch, C.S., MacCormack, J.N. and G.E. Steinkraus.1982. Oyster-associated outbreak of diarrhoeal disease possibly caused by Plesiomonasshigelloides. LANCET. 27:739.
Schulze-Robbecke, R., Janning, B. and R. Fischerder. 1992. Occurrence of Mycobacteriain biofilms samples. Tub. Lung Dis.73:141-144.
164
Seidler, R.J., Allen, D.A, Lockman, H., Colwell, R.R., Joseph, S.W. and O.P. Daily.1980. Isolation, enumeration, and characterization of Aeromonas from polluted watersencountered in diving operations. Appl. Environ. Microbiol. 39:1010-1018.
Severin, B.F. 1976. Inactivation of new indicators organisms of disinfection efficiency.Part II. Combined chlorine as chloramines. Presented at the 96th annual meeting. Amer.Water Works Assoc. New Orleans, LO.
Shooter, R.A., Cooke, E.M., Gaya, H., Kumar, P., Patel, N., Parker, T., Tham, T. andD.R. France. 1969. Food and medicaments as possible sources of hospital strains ofPseudomonas aeruginosa. LANCET 1:1227-1229.
Sloodley, B.J. and B.T. Thom.1970. Observations on the intestinal carriage ofPseudomonas aeruginosa. J Med. Microbiol. 3:367-375.
Stiles, M.E. 1989. Less recognized or presumptive foodborne pathogenic bacteria. p.689-692. In Foodbome bacterial pathogens. Marcel Dekker (ed.). NY.
Surucu, F. and C.N. Haas. 1976. Inactivation of new indicator organisms of disinfectionefficiency. Part I. Free available chlorine species kinetics. Presented at the 96th annualmeeting. Amer. Water Works Assoc. New Orleans, LO.
Tamagini, L.M. and R.D. Gonzalez. 1997. Bacteriological stability and growth kinetics ofPseudomonas aeruginosa in bottled water. J Appl. Microbiol. 83:91-94.
Tsai, G.J. and S.C. Yu. 1997. Microbiological evaluation of bottled water uncarbonatedmineral water in Taiwan. Int. J. Food Microbiol. 37:137-143.
Tsukamoto, T., Kinoshita, Y., Shimada, T. and R. Sakazaki. 1978. Two epidemics ofdiarrhoeal possibly caused by Plesiomonas shigelloides. J Hyg. Camb. 80:275-280.
Van Der Kooij, D. 1988. Properties of Aeromonas and their occurrences and hygienicsignificance in drinking water. Zentralbl. BakterioL MikrobioL Hyg. Ser. B. 187:1-17.
Van Der Kooij, D. 1991. Nutritional requirements of Aeromonads and theirmultiplication in drinking water. Experientia. 47:444-446.
Von Gravenitz, A. and A.H. Mensh. 1968. The genus Aerornonas in human bacteriology:Report of 30 cases and review of the literature. N. Eng. J. Med. 278:245-249.

165
Von Reyn, C.F., Barber, T.W., Arbeit, R.D., Sox, C.H., Oconnor, G.T., Brindle, R.J.,Gilks, C.F., Hakkarainen, K., Ranki, A., Bartholomew, C., Edwards, J., Tostesson,A.N.A. and M. Magnusson. 1993. Evidence of previous infection with Mycobacteriumavium-M intracellulare complex among healthy subjects: An international study ofdominant mycobacterial skin test reactions. J. Infect. Dis. 168:1553-1558.
Von Reyn, C.F., Manslow, J.N., Barber, T.W., Falkinham III, J.O. and R.D. Arbeit. 1994.Persistent colonization of potable water as a source of Mycobacterium avium infection inAIDS. LANCET. 343:1137-1141.
Warburton, D.W., Bowen, B. and A. Konkle. 1994a. The survival and recovery ofPseudomonas aeruginosa and its effects upon Salmonellae in water: Methodology to testbottled water in Canada. Can. J. Microbiol. 40:987-992.
Warburton, D.W., McCormick, J.K. and B. Bowen. 1994b. Survival and recovery ofAeromonas hydrophila in water: Development of methodology for testing bottled waterin Canada. Can. J Microbiol. 40:145-148.
Ward, R.L., S. Krugman, J. Giles, M. Jacobs and O. Bodansky. 1958. InfectiousHepatatis-studies of its natural history and prevention. N. Eng. J Med. 258:402-416.
Ward, R.L., D.I. Bernstein and E.C. Young. 1986. Human Rotavirus studies in volunteersof infectious dose and serological response to infection. J. Infect. Dis. 154:871-877.
Weber, G., Werner, H.P. and H. Matsching. 1971. Death cases in newborns caused byPseudomonas aeruginosa contaminated drinking water. Zentralbl. Bakteriol. 216:210-214.
Werthamer, S. and M. Weiner. 1972. Subacute bacterial endocarditis due toFlavobacterium meningosepticum. Amer. J. Clin. Pathol. 57:410-412.
World Health Organization (WHO). 1993. Guidelines for the drinking water quality. 2'd
edition. Geneva, Switzerland.
Yakrus, M.A. and R.C. Good. 1990. Geographic distribution, frequency, and specimensource of Mycobacterium avium complex serotypes isolates from patients with acquiredimmunodefieciency syndrome. J. Clin. Microbiol. 28:926-929.
Yamamoto, T., Shibagaki, T., Yamori, S., Saito, H., Yamada, H., Ichiyama, S. and K.Shimokata. 1993. Polymerase chain reaction for the differentiation of Mycobacteriumintracellulare and M. avium. Tub. Lung dis. 74:342-345.

166
Zwadyk, P., Down, J.A., Myers, N. and M.S. Dey. 1994. Rendering of Mycobacteria safefor molecular diagnostic studies and developmental of lysis method for stranddisplacement amplification and PCR. J. Clin. Microbiol. 32:2140-2146.





























