Embed Size (px)
Citation preview
1
Texas Resilience & Recovery Services Statement of Work
Collin County Mental Health and Mental Retardation dba LifePath Systems (“LifePath” or “Local Authority”) is the Department of State Health Services (“DSHS”) designated Local Authority established to plan, coordinate, develop policy, develop and allocate resources, supervise, and ensure the provision of community based mental health and intellectual and developmental disabilities services for the residents of Collin County, Texas. SECTION I.
A. PURPOSE: 1. To provide treatment services that facilitate recovery from mental health
disorders to clients who do not require a more structured environment such as residential services to meet treatment goals.
B. PRIORITY POPULATION: 1. Adult Mental Health (MH) Priority Population
a) Adult Mental Health (MH) Priority Population - Adults who have severe and persistent mental illnesses such as schizophrenia, major depression, bipolar disorder, post-traumatic stress disorder, obsessive compulsive disorder, anxiety disorder, attention deficit/hyperactivity disorder, delusional disorder, bulimia nervosa, anorexia nervosa or other severely disabling mental disorders which require crisis resolution or ongoing and long-term support and treatment.
b) An individual age 18 or older who has a diagnosis of: (1) Schizophrenia as defined in the following Diagnostic and Statistical
Manual, Fifth Edition (DSM-5) diagnostic codes: F20.81, F25.0,F20.9, F25.1
(2) Bipolar disorder as defined in the following DSM-5 diagnostic codes: F31.0, F31.9, F31.11, F31.12, F31.13, F31.2, F31.73, F31.71, F31.74, F31.72, F31.31, F31.32, F31.4, F31.5, F31.75, F31.76, F31.89, F31.81
(3) Major Depression as defined in the following DSM-5 diagnostic codes: F32.9, F32.0, F32.1, F32.2, F32.3F32.4, F32.5, F33.9, F33.0, F33.1, F33.2, F33.3, F33.41, and F33.42; with a Global Assessment of Functioning (GAF) of 50 or below at intake.
c) An individual age 18 or older who has a mental health diagnosis other than those listed in (e) below and whose current Global Assessment of Functioning (GAF) is 50 or less and needs on-going MH services; or
d) An individual age 18 or older who was served in children’s MH services and meets the children’s MH priority population definition prior to turning 18 is considered eligible for one year.
e) Individuals with only the following diagnoses are excluded from this provision: (1) Substance Related Disorders as defined in the following DSM-5
diagnostic codes: F10.10, F10.121, F10.129, F10.14, F10.159, F10.180, F10.181, F10.20, F10.221, F10.229, F10.231, F10.232, F10.239, F10.24, F10.259, F10.26, F10.27, F10.280, F10.281, F10.182 F10.288, F10.921, F10.929, F10.94, F10.959, F10.96, F10.97, F10.980, F10.981, F10.982, F10.988, F10.99, F11.10, F11.121, F11.122, F11.129, F11.14, F11.181, F11.188, F11.20, F11.221, F11.222, F11.229, F11.23, F11.24, F11.182, F11.281, F11.282, F11.288, F11.921, F11.922, F11.929, F11.94, F11.981, F11.982, F11.988, F11.99, F12.10, F12.121, F12.122, F12.129, F12.159,
2
F12.180, F12.188, F12.20, F12.221, F12.222, F12.229, F12.259, F12.280, F12.288, F12.921, F12.922, F12.929, F12.959, F12.980, F12.988, F12.99, F13.10, F13.121, F13.129, F13.14, F13.159, F13.180, F13.181, F13.182, F13.20, F13.221, F13.229, F13.231, F13.232, F13.239, F13.24, F13.259, F13.27, F13.280, F13.281, F13.282, F13.288, F13.921, F13.929, F13.94, F13.959, F13.97, F13.980, F13.981, F13.982, F13.988, F13.99, F14.10, F14.121, F14.122, F14.129, F14.14, F14.159, F14.180, F14.181, F14.182, F14.188, F14.20, F14.221, F14.222, F14.229, F14.23, F14.24, F14.259, F14.280, F14.281, F14.282, F14.288, F14.921, F14.922, F14.929, F14.94, F14.959, F14.980, F14.981, F14.982, F14.988, F14.99, F15. 229, F15.10, F15.121, F15.122, F15.129, F15.14, F15.159, F15.180, , F15.181, F15.188, F15.20, F15.221, F15.222, F15.23, F15.24, F15.259, F15.280, F15.281, F15.288, F15.921, F15.922, , F15.929, F15.93, F15.94, F15.959, F15.980, F15.981, F15.988, F15.99, F16.10, F16.121, F16.129, F16.14, F16.159, F16.180, F16.20, , F16.221, F16.229, F16.24, F16.259, F16.280, F16.921, F16.929, F16.94, F16.959, F16.980, F16.983, F16.99, F17.200, F17.203, F17.208, F17.209, F18.10, F18.121, F18.129, F18.14, F18.159, F18.17, F18.180, F18.188, F18.20, F18.221, F18.229, F18.24, F18.259, F18.27, F18.280, F18.288, F18.921, F18.929, F18.94, F18.959, F18.97, F18.980, F18.988, F18.99, F19.10, F19.121, F19.129, F19.14, F19.159, F19.17, F19.180, F19.181, F19.182, F19.188, F19.20, F19.221, F19.229, F19.231, F19.239, F19.24, F19.259, F19.27, F19.280, F19.281, F19.282, F19.288, F19.921, F19.94, F19.959, F19.97, F19.980, F19.981, F19.982, F19.988, F19.99, Z72.0.
f) IDD as defined in the following DSM-5diagnostic codes: F70, F71, F72, F73, F79
g) Autism spectrum disorder as defined in the following DSM-5 diagnostic code: F84.0.
2. Child and Adolescent Mental Health (MH) Priority Population a) Child and Youth Mental Health (MH) Priority Population – children/youth ages
3 through 17 with a diagnosis of mental illness (excluding a single diagnosis of substance abuse, IDD, autism or pervasive development disorder) who exhibit serious emotional, behavioral or mental health disorders and who:
(1) Have a serious functional impairment; or (2) Are at risk of disruption of a preferred living or child care environment
due to psychiatric symptoms; or (3) Are enrolled in a school system’s special education program because of
serious emotional disturbance. b) CMH Ineligible Codes:
(1) Ineligible single diagnoses of substance abuse: (same as AMH) (a) Substance Related Disorders as defined in the following DSM-5
diagnostic codes: F10.10, F10.121, F10.129, F10.14, F10.159, F10.180, F10.181, F10.20, F10.221, F10.229, F10.231, F10.232, F10.239, F10.24, F10.259, F10.26, F10.27, F10.280, F10.281, F10.182 F10.288, F10.921, F10.929, F10.94, F10.959, F10.96, F10.97, F10.980, F10.981, F10.982, F10.988, F10.99, F11.10, F11.121, F11.122, F11.129, F11.14, F11.181, F11.188, F11.20, F11.221, F11.222, F11.229, F11.23, F11.24, F11.182, F11.281, F11.282, F11.288, F11.921, F11.922, F11.929, F11.94, F11.981, F11.982, F11.988, F11.99, F12.10, F12.121, F12.122, F12.129,
3
F12.159, F12.180, F12.188, F12.20, F12.221, F12.222, F12.229, F12.259, F12.280, F12.288, F12.921, F12.922, F12.929, F12.959, F12.980, F12.988, F12.99, F13.10, F13.121, F13.129, F13.14, F13.159, F13.180, F13.181, F13.182, F13.20, F13.221, F13.229, F13.231, F13.232, F13.239, F13.24, F13.259, F13.27, F13.280, F13.281, F13.282, F13.288, F13.921, F13.929, F13.94, F13.959, F13.97, F13.980, F13.981, F13.982, F13.988, F13.99, F14.10, F14.121, F14.122, F14.129, F14.14, F14.159, F14.180, F14.181, F14.182, F14.188, F14.20, F14.221, F14.222, F14.229, F14.23, F14.24, F14.259, F14.280, F14.281, F14.282, F14.288, F14.921, F14.922, F14.929, F14.94, F14.959, F14.980, F14.981, F14.982, F14.988, F14.99, F15. 229, F15.10, F15.121, F15.122, F15.129, F15.14, F15.159, , F15.180, F15.181, F15.188, F15.20, F15.221, F15.222, F15.23, F15.24, F15.259, F15.280, F15.281, F15.288, F15.921, F15.922, , F15.929, F15.93, F15.94, F15.959, F15.980, F15.981, F15.988, F15.99, F16.10, F16.121, F16.129, F16.14, F16.159, F16.180, F16.20, F16.221, , F16.229, F16.24, F16.259, F16.280, F16.921, F16.929, F16.94, F16.959, F16.980, F16.983, F16.99, F17.200, F17.203, F17.208, F17.209, F18.10, F18.121, F18.129, F18.14, F18.159, F18.17, F18.180, F18.188, F18.20, F18.221, F18.229, F18.24, F18.259, F18.27, F18.280, F18.288, F18.921, F18.929, F18.94, F18.959, F18.97, F18.980, F18.988, F18.99, F19.10, F19.121, F19.129, F19.14, F19.159, F19.17, F19.180, F19.181, F19.182, F19.188, F19.20, F19.221, F19.229, F19.231, F19.239, F19.24, F19.259, F19.27, F19.280, F19.281, F19.282, F19.288, F19.921, F19.94, F19.959, F19.97, F19.980, F19.981, F19.982, F19.988, F19.99, Z72.0.
(2) Ineligible diagnoses for IDD (same as AMH): F70, F71, F7 (3) Ineligible diagnosis for Autism spectrum disorder: F84.0
C. SERVICE REQUIREMENTS: 1. Administrative Requirements:
a) Contractor shall serve as a Comprehensive Service Provider located in Collin County, providing the services listed in this statement of work.
b) Meet the qualifications of the DSHS performance contract: http://www.dshs.state.tx.us/mentalhealth.shtm and local plan www.lifepathsystems.org.
c) Demonstrate one’s ability to provide services in compliance with DSHS contract requirements.
d) Comply with TRR (Texas Resiliency and Recovery) @ http://www.dshs.state.tx.us/mhsa/trr/.
e) Be able to provide services in the language as dictated by the person receiving services and/or utilization of translator at the Contractor’s sole expense. Required to use at least a Level One certified sign language interpreter and to use a Level Three certified sign language interpreter, if available, for persons with hearing impairments who request sign language interpreter services.
f) Engage and involve consumers, legally authorized representatives, and families in the policy and practice levels within the applicant’s organization or individual practice.
4
g) Have the ability to accept routine appointments within 10 days and urgent appointments within 2 days for all new referrals until the applicant’s capacity is reached or utilization/referral is not indicated.
h) Contractor and its employees, as applicable, are responsible, at Contractor’s sole expense, to comply with all training requirements the Local Authority mandates and in accordance with the Texas Administrative Code.
i) Contractor shall maintain all original documentation reflecting service provision regarding treatment and/or services rendered to the Local Authority’s individuals with mental illness, and allow the Local Authority access to such records upon request.
j) Contractor must submit encounters within 2 business days for provision of service via Local Authority’s on-line web-based portal.
k) Contractor must submit monthly invoices for payment as designated in current version of LifePath Provider Manual.
l) Ensure client has an appointment scheduled with a physician or designee authorized by law to prescribe needed medications, if the Continuing Care Plan, as defined in 25 TAC Chapter 412, Subchapter D, Mental Health Services – Admission, Continuity, and Discharge, indicates that the LMHA is responsible for providing or paying for psychotropic medications.
(1) The appointment shall be on a date prior to the earlier of the following events:
(a) The exhaustion of the client’s supply of medications; or (b) The expiration of 14 days from the client’s discharge or furlough
from a State Mental Health Facility (SMHF). Contractor is required to comply with all state and federal laws regarding the confidentiality of consumers’ records and nondiscrimination.
(c) Provide individuals a choice of qualified physicians or designees authorized by law to prescribe needed medications through face-to-face encounters or via telemedicine to the maximum extent possible. This shall be accomplished by the following, listed in order of priority:
i. Employing a qualified physician or designee authorized by law to prescribe needed medications; or
ii. Contracting with a qualified physician or designee authorized by law to prescribe needed medications; or
iii. Notifying Local Authority within one business day if both employing and contracting with a qualified physician or designee authorized by law to prescribe needed medications is not possible for any period of time during the contract period.
m) Offer each Level of Care (LOC) as outlined in the Texas Resilience and Recovery (TRR) Utilization Management Guidelines and this Statement of Work and provide the core services available within each LOC to individuals through face-to-face encounters or via telemedicine/telehealth. This shall be accomplished by the following, listed in order of precedence:
(1) Employing staff who meet the qualifications (i.e. licensure, training, and/or competency) to provide the core service; or
(2) Contracting with providers who meet the qualifications (i.e. licensure, training, and/or competency) to provide the core service.
n) Specific Requirements for Medicaid Recipients –
5
(1) General - Contractor shall deliver services to an individual who is a Medicaid recipient and has an identified need for Targeted Case Management or Mental Health Rehabilitative Services.
(2) Mental Health Rehabilitative and Mental Health Targeted Case Management Services (both Intensive and Routine) - Medicaid recipients who are eligible for full Medicaid benefits shall not be placed on a waiting list for medically necessary Targeted Case Management or Mental Health Rehabilitative Services. Contractor shall make these services available to the individual whenever such services are indicated by the uniform assessment and in accordance with the Texas Resilience and Recovery Utilization Management Guidelines. If the Uniform Assessment process recommends that an individual receive a LOC that includes one or both of these services and a Licensed Practitioner of the Healing Arts (LPHA) determines that the service or services are not medically necessary, the LPHA shall document the reasons that the service is not indicated.
(3) Other Medicaid Mental Health Services - For Medicaid recipients who are eligible for full Medicaid benefits and have an identified need for medically necessary mental health services other than Mental Health Rehabilitative Services and Targeted Case Management (such as counseling or physician’s services), Contractor shall provide these services to the individual or refer the individual to other local Medicaid providers. Contractor shall provide assistance with the referral if requested by the client. Contractor shall document actions taken on behalf of the client.
o) Contractor shall participate in Local Authority’s Quality Management Program:
(1) Assist in the completion of Mental Health Adult Client or Child and Family surveys as required by Local Authority and DSHS.
(2) Participate in the collection of grievance, appeal, fair hearings, and expedited hearings, mortality, and incident/accident data as part of the Quality Management process;
(3) Participate in measuring, assessing, and improving Contractor’s functions;
(4) Participate in development of processes to systematically monitor, analyze, and improve performance of quality management activities, administrative services, client services and outcomes for individuals;
(5) Participate in the review of provider treatment to determine whether it is consistent with DSHS’ approved evidence-based practices, accuracy of assessments, and treatment planning;
(6) Participate in the ongoing monitoring of the quality of access to services, service delivery, and continuity of services;
(7) Allow Local Authority oversight to ensure compliance with and the quality of the TRR practices to include monitoring fidelity to the service models defined by Local Authority and DSHS and requiring providers to participate in oversight; including an annual continuous quality improvement measurement of the fidelity of evidence-based practices (EBP) for children and adolescent services utilizing the EBP fidelity tools approved by DSHS.
(a) Fidelity monitoring is required for the following CMH EBPs:
6
i. TF-CBT ii. Seeking Safety
iii. Aggression Replacement Techniques (b) Fidelity monitoring is recommended for the following CMH EBPs
and promising practices: i. Wraparound Planning
ii. Nurturing Parenting iii. Safety Planning Intervention: The Safety Plan
Intervention (SPI; Stanley & Brown, 2011) is a brief 20 to 45 minute intervention that provides an individual with a set of steps that can be used progressively to attempt to reduce risk and maintain safety when suicidal thoughts emerge. SPI should follow a comprehensive risk assessment after strong rapport has been developed. Safety plans should be developed within a collaborative process among the provider, the individual at risk, and his or her close family or friends. Safety planning can be a stand-alone intervention, utilized during crisis contacts (e.g., in emergency departments, mobile crisis contacts) or as a part of an on-going treatment relationship.
(8) Ensure mechanisms to measure, assess, and reduce incidents of client abuse, neglect and exploitation and improving the client rights protection processes;
(9) Ensue Risk Management processes such as competency determinations and the management and reporting of incidents and deaths;
(10) Coordination of activities and information with the UM Program including participation in UM oversight activities as defined and scheduled by Local Authority, including but not limited to submitting data and supporting documentation, performance and submitting results of self-audits, and participating in Local Authority onsite reviews.
p) Ensure all providers are implementing TRR, as specified by Local Authority and DSHS and providing evidence-based practices in accordance with the Fidelity Manual. Providers who do not meet adequate implementation shall submit a Plan of Improvement (POI) for identified problems and meet the following standards:
(1) Within five business days after receipt of a request from Local Authority, develop a POI that adequately addresses the correction of any critical health, safety, rights, abuse and neglect issues identified by Local Authority and/or DSHS, that includes a description of local oversight activities to monitor and maintain the correction of the identified problem, and submit to Local Authority for approval; and
(2) Within 14 business days after receipt of a request from Local Authority, develop a POI that adequately addresses the correction of organizational, clinical or compliance problems identified by Local Authority during oversight activities and that includes a description of local oversight activities to monitor and maintain the improvement of the identified problem, and submit to Local Authority for approval in accordance with the Submission Calendar.
7
q) If applicable, submit to Local Authority evidence of initial or continued accreditation by a national accreditation organization (e.g., American Association of Suicidology, Joint Commission, Commission on Accreditation of Rehabilitation Facilities (CARF), and The Council on Quality and Leadership (CQL), in accordance with the Submission Calendar. The submission shall include the accreditation review report and any plan of improvement created by Contractor in response to the accreditation review report.
r) Ensure that Contractor’s buildings and associated properties are compliant with the Texas Accessibility Standards (TAS), Texas Health and Safety Code, Texas Department of Licensing and Regulation requirements, National Fire Protection Association (NFPA) Life Safety Code or the International Fire Code.
s) Ensure that Contractor’s Americans with Disabilities Act (ADA) Self-Evaluation and Transition Plan (ADA Plan) is reviewed by Contractor at least annually and updated as necessary, and ensure that the following information is posted prominently at each service location:
(1) The name, address, telephone number, TDD telephone number, fax number and e-mail address of the ADA and the Rehabilitation Act of 1973 Coordinator(s);
(2) The location at which the ADA Plan may be viewed; and (3) The process for requesting and obtaining copies of the ADA Plan.
D. ADULT SERVICES 1. Community Services
a) Contractor shall provide the community-based services outlined Exhibit B. b) Service Determination:
(1) In determining services to be provided to the priority and target populations, the choice of and admission to medically necessary services is determined jointly by the individual seeking service and the Local Authority.
(2) Criteria used to make these determinations are the recommended LOC (LOC-R) of the individual as derived from the UA, the needs of the individual, Texas Resilience and Recovery Utilization Management Guidelines, and the availability of resources. Clients authorized for care by the Local Authority through a clinical override are eligible for the duration of the authorization.
(3) The initial assessment is the clinical process of obtaining and evaluating historical, social, functional, psychiatric, developmental or other information from the individual seeking services in order to determine specific treatment and support needs.
(4) All individuals seeking services must go to Local Authority for Eligibility and Intake.
(5) Individuals will be able to choose a provider once the Local Authority assigns a Level of Care.
c) Continued Eligibility for Services: (1) Reassessment by the Contracted provider and reauthorization of
services by Local Authority determines continued need for services. This activity is completed according to the UA protocols and Texas Resilience and Recovery Utilization Management Guidelines.
(2) Assignment of diagnosis in CMBHS is required at any time the Axis I diagnosis changes and at least annually from the last diagnosis entered into CMBHS.
8
(3) The LPHA’s determination of diagnosis shall include a face-to-face or via telemedicine/telehealth interview with the individual.
(4) Eligibility for clients whose diagnosis is Major Depression includes a GAF of 50 or below at intake only. Changes in GAF scores after the initial eligibility determination do not make clients ineligible.
d) Documentation Required: (1) In order to assign a diagnosis across all 5 axes to an individual,
documentation of the required diagnostic criteria, as well as the specific justification of GAF score, shall be included in the client record. This information shall be included as a part of the required assessment information.
e) UA Requirements: (1) The DSHS-approved UA for Adults includes the following instruments:
(a) Adult Needs and Strengths Assessment (ANSA). (b) Diagnosis-Specific Clinical Rating Scales; (c) Community Data; and. (d) Authorized LOC – to be completed by the Local Authority.
(2) The above instruments are required to be completed at the initial assessment (by the Local Authority) and at reassessment (by the Contractor).
(3) Staff administering the instruments must have documented training in said instruments and must be a QMHP-CS, with the exception of the Diagnosis-Specific Clinical Rating Scales which may be administered by a QMHP-CS or Licensed Vocational Nurse (LVN). Staff administering the instruments must have documentation of certification in the ANSA or CANS;
(4) The UA shall be administered according to the timeframes delineated in Information Item C at http://www.dshs.state.tx.us/mhcontracts/ContractDocuments.shtm.
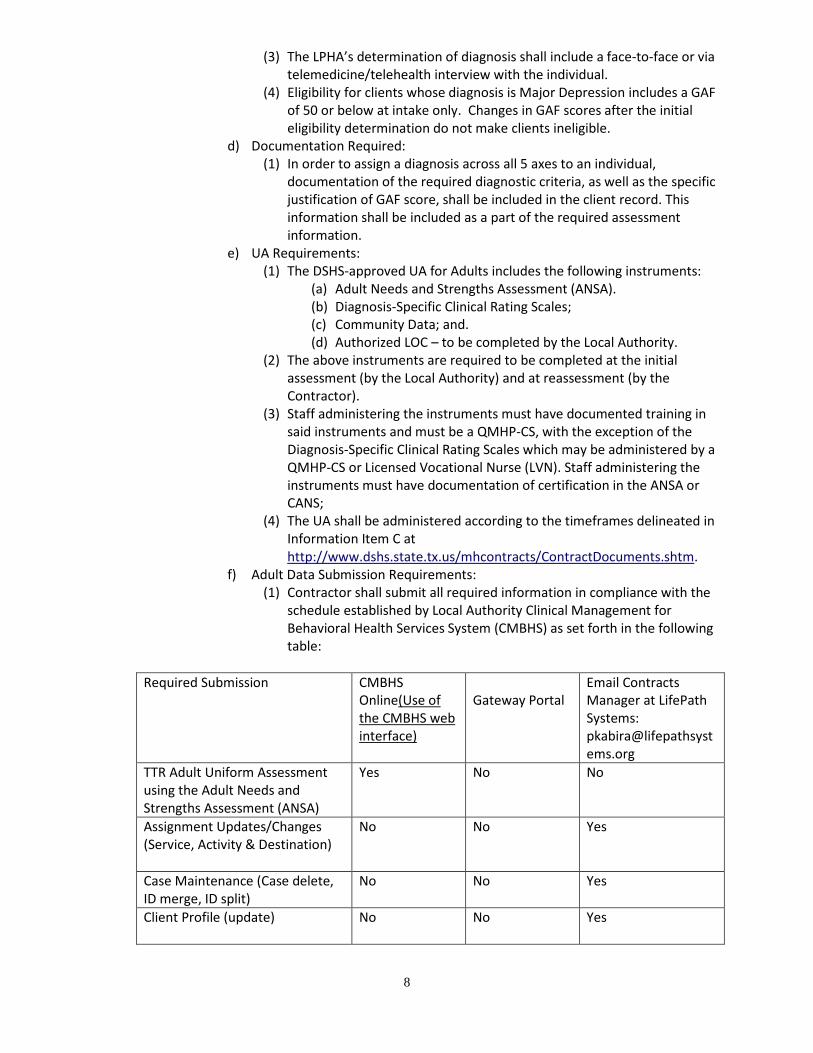
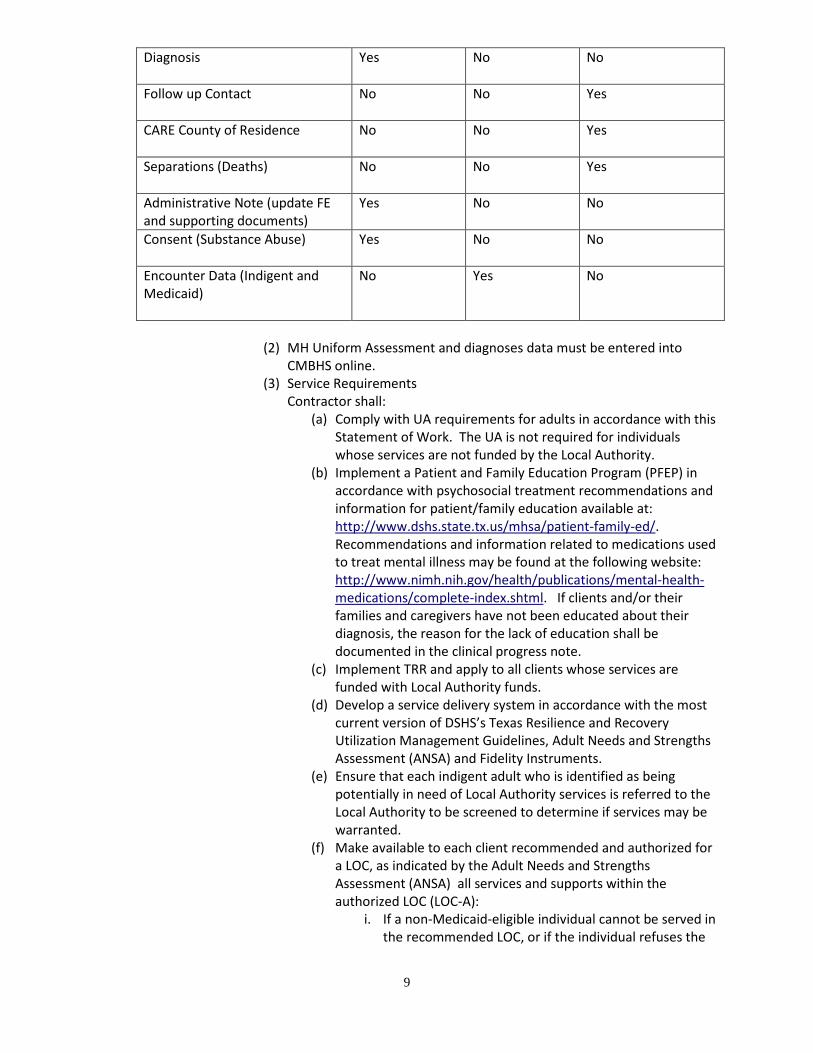
f) Adult Data Submission Requirements: (1) Contractor shall submit all required information in compliance with the
schedule established by Local Authority Clinical Management for Behavioral Health Services System (CMBHS) as set forth in the following table:
Required Submission CMBHS
Online(Use of the CMBHS web interface)
Gateway Portal
Email Contracts Manager at LifePath Systems: [email protected]
TTR Adult Uniform Assessment using the Adult Needs and Strengths Assessment (ANSA)
Yes No No
Assignment Updates/Changes (Service, Activity & Destination)
No No Yes
Case Maintenance (Case delete, ID merge, ID split)
No No Yes
Client Profile (update)
No No Yes
9
Diagnosis
Yes No No
Follow up Contact
No No Yes
CARE County of Residence
No No Yes
Separations (Deaths)
No No Yes
Administrative Note (update FE and supporting documents)
Yes No No
Consent (Substance Abuse)
Yes No No
Encounter Data (Indigent and Medicaid)
No Yes No
(2) MH Uniform Assessment and diagnoses data must be entered into
CMBHS online. (3) Service Requirements
Contractor shall: (a) Comply with UA requirements for adults in accordance with this
Statement of Work. The UA is not required for individuals whose services are not funded by the Local Authority.
(b) Implement a Patient and Family Education Program (PFEP) in accordance with psychosocial treatment recommendations and information for patient/family education available at: http://www.dshs.state.tx.us/mhsa/patient-family-ed/. Recommendations and information related to medications used to treat mental illness may be found at the following website: http://www.nimh.nih.gov/health/publications/mental-health-medications/complete-index.shtml. If clients and/or their families and caregivers have not been educated about their diagnosis, the reason for the lack of education shall be documented in the clinical progress note.
(c) Implement TRR and apply to all clients whose services are funded with Local Authority funds.
(d) Develop a service delivery system in accordance with the most current version of DSHS’s Texas Resilience and Recovery Utilization Management Guidelines, Adult Needs and Strengths Assessment (ANSA) and Fidelity Instruments.
(e) Ensure that each indigent adult who is identified as being potentially in need of Local Authority services is referred to the Local Authority to be screened to determine if services may be warranted.
(f) Make available to each client recommended and authorized for a LOC, as indicated by the Adult Needs and Strengths Assessment (ANSA) all services and supports within the authorized LOC (LOC-A):
i. If a non-Medicaid-eligible individual cannot be served in the recommended LOC, or if the individual refuses the
10
recommended LOC, individual may be served at the next most appropriate LOC. If no services are available at the next most appropriate LOC, notify Local Authority for referral or recommendation;
ii. Medicaid-eligible individuals may not have services denied, reduced, suspended, or terminated due to lack of available resources; and
iii. If a Medicaid eligible individual refuses the recommended LOC, the individual may be served at the next most appropriate LOC as long as the services within that LOC are appropriate and medically necessary to address the individual’s mental illness.
(g) Ensure Medicaid eligible individuals are provided with any medically necessary Medicaid funded MH services within the recommended LOC without undue delay.
(h) Ensure that Cognitive-Behavioral Therapy (CBT) is provided by an LPHA, practicing within the scope of a license, or when appropriate and not in conflict with billing requirements, by an individual with a master’s degree in a human services field (e.g., psychology, social work, family therapy or counseling) who is pursuing licensure under the direct supervision of an LPHA. The LPHA providing CBT shall meet DSHS competency requirements as outlined in the Information Item A (CBT Competency Policy).
(i) Ensure that providers of services and supports within TRR are trained in the DSHS-approved evidence-based practices prior to the provision of these services and supports. DSHS-approved evidence-based practices are:
i. Counseling: Cognitive Behavioral Therapy; ii. Psychosocial Rehabilitation: SAMHSA Illness
Management and Recovery; iii. Supported Employment: Dartmouth Psychiatric
Research Center – Individual; Placement and Support or SAMHSA Supported Employment; and
iv. Supported Housing: SAMHSA Permanent Supported Housing;
v. Co-Occuring Psychiatric and Substance Use Disorders (COPSD)
(j) Ensure that supervisors of services and supports within TRR are trained as trainers in the DSHS-approved evidence-based practices, are trained in the evidence-based practices, or have provided the evidence–based practices prior to the supervision of the evidence-based practices. Supervisors must complete this requirement within 180 days of assuming a supervisory position. If supervisors are unable to complete this requirement within 180 days of assuming the supervisory position, the Contractor must submit a plan to the Local Authority outlining how the supervisor will fulfill this requirement.
(k) Use the uniform assessment and other relevant clinical information reassess current clients in services when update
11
assessments are due or significant changes in functioning occur, to determine the recommended LOC for a client.
(l) Utilize information from the Adult Needs and Strengths Assessment (ANSA) and other relevant clinical information to:
i. Recommend a LOC; ii. Determine whether the client should be transferred to
another provider; and iii. Determine if a client should be discharged from
services. (m) Contractor shall maintain access to CMBHS.
(4) Submit encounter data for all Indigent and Medicaid services according to the procedures, instructions and schedule established by Local Authority, including all required data fields and values in the current version of the Local Authority Community Mental Health Service Array.
(5) Comply with the following Medicaid-related items: (a) Contract with Managed Care Organization to be a provider of
Medicaid MH Rehabilitative Services; (b) Contract with Managed Care Organization to be a provider of
Medicaid MH Case Management; (c) Recognize that funding earned through billings to Texas
Medicaid and Healthcare Partnership (TMHP) for Medicaid MH Case Management and Medicaid MH Rehabilitative Services represents the federal share and the State match; and
(d) Submit encounter data for all Medicaid services through the gateway portal for the provision Community Mental Health Services.
(6) Utilize non-contract funds and other funding sources (e.g., any person or entity who has the legal responsibility for paying all or part of the services provided, including commercial health or liability insurance carriers, Medicaid, or other Federal, State, local, and private funding sources) whenever possible to maximize Contractor’s financial resources. This includes:
(a) Enroll in the CHIP and bill CHIP for services covered under that plan;
(b) Become a Medicaid provider and bill Medicaid for services covered under that plan;
(c) Notify Local Authority to provide assistance to individuals to enroll in such programs when the screening process indicates possible eligibility for such programs;
(d) Comply with the Charges for Community Services Rule as set forth in Title 25, Part 1, Chapter 412, Subchapter C of the Texas Administrative Code to maximize reimbursement from individuals with an ability to pay for services provided;
(e) Bill all other funding sources for services provided under this Contract before submitting any request for reimbursement to Local Authority; and
(f) Provide all billing functions at no cost to the client. (7) Provide services to all clients without regard to the client’s history of
arrest, charge, fine, indictment, incarceration, sentence, conviction,
12
probation, deferred adjudication, or community supervision for a criminal offense.
(8) Develop and implement written procedures to identify clients with Co-Occurring Psychiatric and Substance Use Disorders (COPSD), identify available resources, provide referrals and continuity of care for ongoing services as necessary to address the client’s unmet substance use treatment needs in accordance with 25 TAC, Chapter 411, Subchapter N. Nothing herein shall prohibit a physician from considering a client’s substance use in prescribing medications.
g) Conduct all initial and on-going diagnostic assessments face-to-face or by telemedicine/telehealth with the individual to determine priority population eligibility.
h) Submit update financial data regarding co-pays, deductibles, and premiums related to Medicare Part D or other information related to expenditures for medications as requested by Local Authority and in the form and format prescribed by Local Authority.
E. CHILDREN’S SERVICES 1. Community Services
a) Contractor shall provide the community-based services outlined in Exhibit B. b) Service Determination:
(1) In determining services and supports to be provided to the child/youth and family, the choice of and admission to medically necessary services and supports are determined jointly by the child/youth and family seeking services and supports and by Local Authority.
(2) Criteria used to make these determinations are from the recommended LOC (LOC-R) of the individual as derived from the UA, the needs of the individual, Texas Resilience and Recovery Utilization Management Guidelines and the availability of resources.
(3) The Global Assessment of Functioning (GAF) is not used to determine eligibility for CMH services; and
(4) Children/Youth authorized for care by Local Authority through a clinical override are eligible for the duration of the authorization. A clinical override for ineligible children/youth may not exceed a maximum of two consecutive authorizations.
(5) The initial assessment is the clinical process of obtaining and evaluating historical, social, functional, psychiatric, developmental or other information from the individual seeking services in order to determine specific treatment and support needs.
(6) All individuals seeking services must go to Local Authority for Eligibility and Intake.
(7) Individuals will be able to choose a provider once the Local Authority assigns a Level of Care.
c) Continued Eligibility for Services: (1) Reassessment by the provider and reauthorization of services by Local
Authority determines continued need for services. This activity is completed according to the UA protocols and Texas Resilience and Recovery Utilization Management Guidelines;
(2) Assignment of diagnosis in CMBHS is required at any time the Axis I diagnosis changes and at least annually from the last diagnosis entered into CMBHS; and
13
d) The LPHA’s determination of diagnosis shall include an interview with the individual conducted either face-to-face or via telemedicine/telehealth. Documentation required:
(1) In order to assign a diagnosis across all five axes to an individual, documentation of the required diagnostic criteria, as well as the specific justification of GAF score, shall be included in the client record. This information shall be included as part of the required assessment information.
e) UA requirements (1) DSHS-approved UA for children and youth includes the following
instruments: (a) Child and Adolescent Needs and Strengths Assessment (CANS) ;
and (b) Community Data; and (c) Authorized LOC – to be completed by Local Authority
(2) The above instruments are required to be completed at the initial assessment (by the Local Authority) and at reassessment (by the Provider).
(3) Staff administering the instruments shall be a QMHP-CS and have documented training in the use of the instruments; Staff administering the instruments must have documentation of current certification in the CANS or ANSA. Certification must be updated annually through a DSHS approved entity.
(4) The UA shall be administered according to the timeframes delineated in Information Item C located at http://www.dshs.state.tx.us/mhcontracts/ContractDocuments.shtm Child Data Submission Requirements.
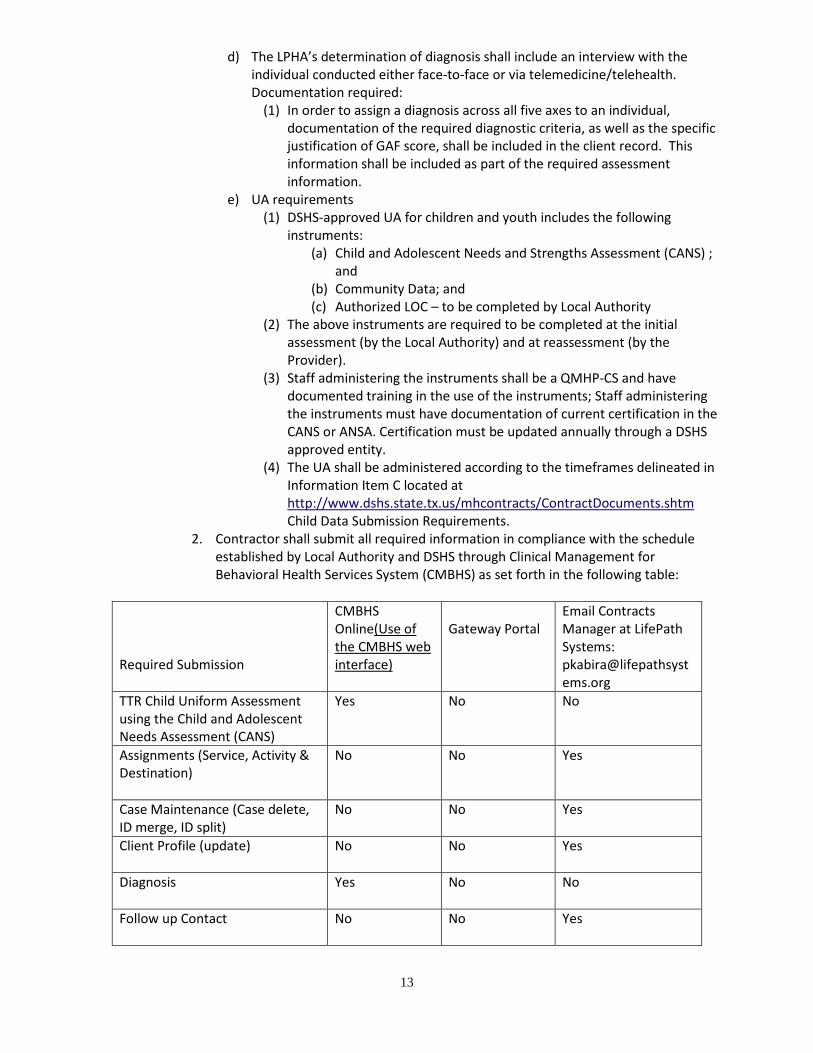
2. Contractor shall submit all required information in compliance with the schedule established by Local Authority and DSHS through Clinical Management for Behavioral Health Services System (CMBHS) as set forth in the following table:
Required Submission
CMBHS Online(Use of the CMBHS web interface)
Gateway Portal
Email Contracts Manager at LifePath Systems: [email protected]
TTR Child Uniform Assessment using the Child and Adolescent Needs Assessment (CANS)
Yes No No
Assignments (Service, Activity & Destination)
No No Yes
Case Maintenance (Case delete, ID merge, ID split)
No No Yes
Client Profile (update)
No No Yes
Diagnosis
Yes No No
Follow up Contact
No No Yes
14
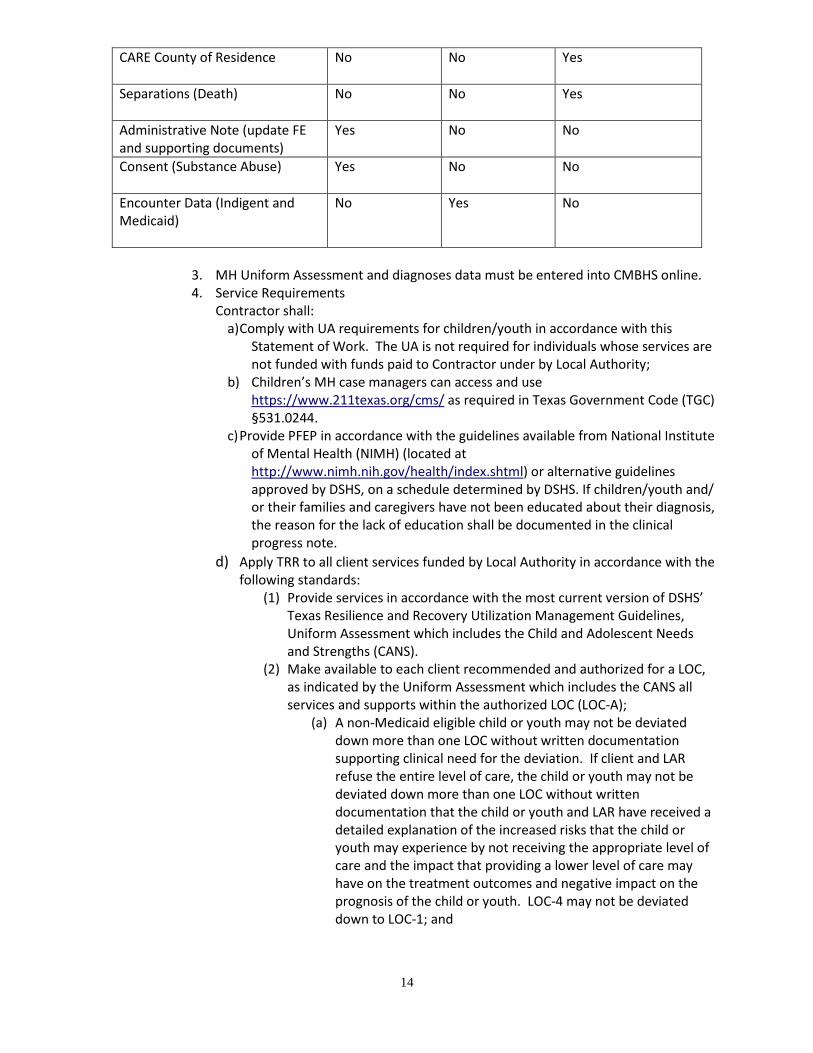
CARE County of Residence
No No Yes
Separations (Death)
No No Yes
Administrative Note (update FE and supporting documents)
Yes No No
Consent (Substance Abuse)
Yes No No
Encounter Data (Indigent and Medicaid)
No Yes No
3. MH Uniform Assessment and diagnoses data must be entered into CMBHS online. 4. Service Requirements
Contractor shall: a) Comply with UA requirements for children/youth in accordance with this
Statement of Work. The UA is not required for individuals whose services are not funded with funds paid to Contractor under by Local Authority;
b) Children’s MH case managers can access and use https://www.211texas.org/cms/ as required in Texas Government Code (TGC) §531.0244.
c) Provide PFEP in accordance with the guidelines available from National Institute of Mental Health (NIMH) (located at http://www.nimh.nih.gov/health/index.shtml) or alternative guidelines approved by DSHS, on a schedule determined by DSHS. If children/youth and/ or their families and caregivers have not been educated about their diagnosis, the reason for the lack of education shall be documented in the clinical progress note.
d) Apply TRR to all client services funded by Local Authority in accordance with the following standards:
(1) Provide services in accordance with the most current version of DSHS’ Texas Resilience and Recovery Utilization Management Guidelines, Uniform Assessment which includes the Child and Adolescent Needs and Strengths (CANS).
(2) Make available to each client recommended and authorized for a LOC, as indicated by the Uniform Assessment which includes the CANS all services and supports within the authorized LOC (LOC-A);
(a) A non-Medicaid eligible child or youth may not be deviated down more than one LOC without written documentation supporting clinical need for the deviation. If client and LAR refuse the entire level of care, the child or youth may not be deviated down more than one LOC without written documentation that the child or youth and LAR have received a detailed explanation of the increased risks that the child or youth may experience by not receiving the appropriate level of care and the impact that providing a lower level of care may have on the treatment outcomes and negative impact on the prognosis of the child or youth. LOC-4 may not be deviated down to LOC-1; and
15
(b) Medicaid-eligible children and youth may not have services denied, reduced, suspended, or terminated due to lack of available resources. If a Medicaid-eligible child, youth or the LAR of a child or youth refuses the recommended LOC, the child or youth may be served at the next most appropriate LOC as long as the services within that LOC are appropriate and medically necessary to address the child or youth’s emotional disturbance. The LOC should not be reduced if the child, youth, or LAR refuses Family Partner services or family support groups only.
(3) Medicaid-eligible children and youth shall be provided with any medically necessary Medicaid-funded MH services within the recommended LOC without undue delay.
(4) Meet and require TRR services subcontractors to meet the training requirements for the DSHS-approved evidence-based practices prior to the provision of these services and supports as outlined in Exhibit D. Completion of the training requirements shall be documented and maintained by Contractor and subcontractor.
(5) Wraparound Treatment Planning: This is a required component of Intensive Case Management and shall be implemented as outlined in 25 TAC Chapter 412, Subchapter I. Training requirements are outlined in Exhibit D.
(6) Counseling: Counseling services shall be provided by an LPHA, practicing within the scope of a license, or when appropriate and not in conflict with billing requirements, by an individual with a master’s degree in a human services field (e.g., psychology, social work, counseling) who is pursuing licensure under the direct supervision of an LPHA. Training and/or competency requirements are outlined in Exhibit D. The allowable models of counseling and practice requirements are:
(a) Cognitive Behavioral Therapy (CBT): Providers of CBT must deliver the approved protocols as outlined in the Texas Resilience and Recovery Utilization Management Guidelines
(b) Trauma-Focused Cognitive Behavioral Therapy (TF-CBT): TF-CBT is a required protocol. Contractor shall document completed training and clinical consultations as outlined in Exhibit D and according to UM Guidelines.
(c) Parent-Child Psychotherapy (Dyad Therapy): This is an allowable model of counseling that may be delivered to children 3-5 years of age. To deliver this protocol, Contractor shall document completed training in one of the DSHS approved models of Parent-Child Psychotherapy as outlined in Exhibit D.
(7) Ensure that supervisors of services and supports within TRR are trained as trainers in the DSHS-approved evidence-based practices, are trained in the evidence-based practices, or have provided the evidence–based practices prior to the supervision of the evidence-based practices. Supervisors must complete this requirement within 180 days of assuming a supervisory position. If supervisors are unable to complete this requirement within 180 days of assuming the supervisory position, the Contractor must submit a plan to the Local Authority outlining how the supervisor will fulfill this requirement. Clinical supervisors for a
16
QMHP-CS providing Skills Training and Development services must be at least a QMHP-CS.
(8) Use the Uniform Assessment which includes the Child and Adolescent Needs and Strengths Assessment (CANS) to:
(a) reassess current children/youth in services when update assessments are due or when service needs have changed to determine the recommended LOC for a child/youth;
(9) Hire or contract with a Certified Family Partner to provide peer mentoring and support to parents/primary caregivers of children and youth. Certified Family Partners hired or contracted must meet the following qualifications:
(a) Is 18 years of age or older; (b) Has received either:
i. A high school diploma; or ii. A high school equivalency certificate issued in
accordance with the laws applicable to the issuing agency;
(c) Has at least one year of lived experience raising a child or adolescent with an emotional or mental health issue as a parent or LAR;
(d) Has at least one year of experience navigating a child-serving system (e.g. mental health, juvenile justice, social security, or special education) as a parent or LAR; and
(e) Has the ability to perform the duties of a Family Partner as outlined in the Texas Resilience and Recovery Utilization Management Guidelines.
(f) Has successfully completed the certified Family Partner training and passed the certification exam recognized by the department within one year of the date of hire for the role of Family Partner.
(10) Family Partner Supports are available in all LOCs, but Contractor shall serve a minimum of 54.90% of children and youth receiving services in LOC 4.
(11) Ensure the Family Partner receives the appropriate training and supervision;
(12) Contractor shall make family support groups available to the caregivers of children and youth with serious emotional disturbances; and
(13) Maintain access to CMBHS. e) Submit encounter data for all Indigent and Medicaid services according to the
procedures, instructions and schedule established by Local Authority, including all required data fields and values in the current version of the Local Authority and DSHS Community Mental Health Service Array.
f) Comply with the following Medicaid-related items: (1) Contract with Managed Care Organization to be a provider of Medicaid
MH Rehabilitative Services; (2) Contract with Managed Care Organization to be a provider of Medicaid
MH Case Management. (3) Recognize that funding earned through billings to Texas Medicaid and
Healthcare Partnership (TMHP) for Medicaid MH Case Management and
17
Medicaid MH Rehabilitative Services represents the federal share and the State match; and
(4) Submit encounter data for all Medicaid services through the gateway portal for the provision Community Mental Health Services.
g) Utilize non-contract funds and other funding sources (e.g., any person or entity who has the legal responsibility for paying all or part of the services provided, including commercial health or liability insurance carriers, Medicaid, or other Federal, State, local, and private funding sources) whenever possible to maximize Contractor’s financial resources. Contractor shall comply with the following requirements:
(1) Enroll in the CHIP and bill CHIP for services covered under that plan; (2) Become a Medicaid provider and bill Medicaid for services covered
under that plan; (3) Provide assistance to individuals to enroll in such programs when the
screening process indicates possible eligibility for such programs; (4) Allow clients that are otherwise eligible for Local Authority funded
services, but that cannot pay a deductible required by a third party payor, to receive services up to the amount of the deductible and to use Local Authority funds to pay for the deductible;
(5) Maintain appropriate documentation from the third party payor reflecting attempts to obtain reimbursement;
(6) Bill all other funding sources for services provided under this Statement of Work before submitting any request for reimbursement to Local Authority; and
(7) Provide all billing functions at no cost to the client. h) Provide services to all clients without regard to the client’s history of arrest,
charge, fine, indictment, incarceration, sentence, conviction, probation, deferred adjudication, or community supervision for a criminal offense.
SECTION II. SERVICE AREA
A. Counties: Collin County SECTION III. PAYMENT
A. Compensation will be a monthly case rate per client seen each month. Adult Case Rate Payment will be $175 per month per member served with a face to face service. Child/Adolescent Case Rate Payment will be $200 per month per member served with a face to face service. Actual count is determined by taking the count of any Member with an active Uniform Assessment and authorization with an Exhibit A service encounter successfully submitted into Local Authority’s online web portal within the month, less the total amount of MAP (Maximum Ability to Pay) payments that Contractor was responsible for collecting during the month, based on Local Authority data. Additionally, Contractor is required to submit encounters totaling at least 90% of the total case rate payment. If encounter claims submitted are below threshold percentage, then Local Authority may reduce the payment to reflect the difference between the encounter value and 90% of the case rate value.
B. It is the goal of LifePath Systems for all clean claims to be paid within 30 days of receipt.
SECTION IV. PERFORMANCE TARGETS A. See Exhibit E for the DSHS Performance Targets. Contractor will be responsible for assisting the
Local Authority to meet these Performance Targets. Any Penalties assessed on the Local

18
Authority for not meeting Performance Targets will be assessed across contracted providers based on performance during the period in question.
19
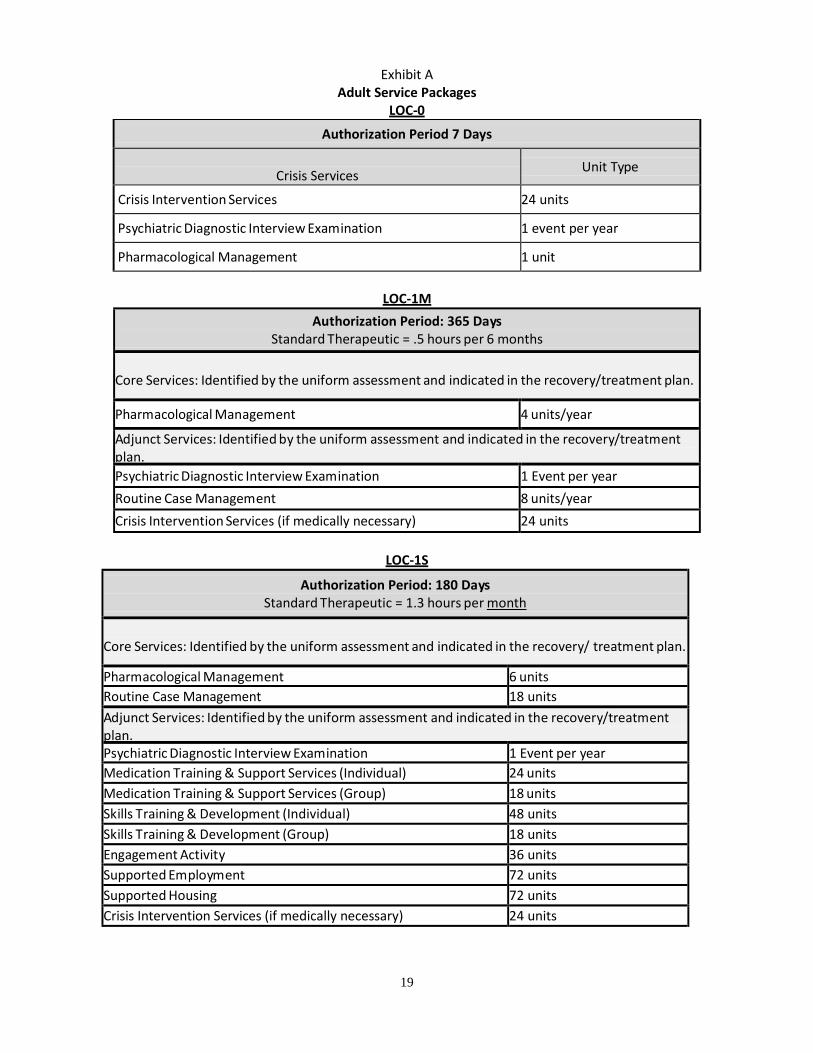
Exhibit A
Adult Service Packages LOC-0
Authorization Period 7 Days
Crisis Services Unit Type
Crisis Intervention Services 24 units
Psychiatric Diagnostic Interview Examination 1 event per year
Pharmacological Management 1 unit
LOC-1M
Authorization Period: 365 Days Standard Therapeutic = .5 hours per 6 months
Core Services: Identified by the uniform assessment and indicated in the recovery/treatment plan. Pharmacological Management 4 units/year
Adjunct Services: Identified by the uniform assessment and indicated in the recovery/treatment plan. Psychiatric Diagnostic Interview Examination 1 Event per year Routine Case Management 8 units/year Crisis Intervention Services (if medically necessary) 24 units
LOC-1S
Authorization Period: 180 Days Standard Therapeutic = 1.3 hours per month
Core Services: Identified by the uniform assessment and indicated in the recovery/ treatment plan. Pharmacological Management 6 units Routine Case Management 18 units Adjunct Services: Identified by the uniform assessment and indicated in the recovery/treatment plan. Psychiatric Diagnostic Interview Examination 1 Event per year Medication Training & Support Services (Individual) 24 units Medication Training & Support Services (Group) 18 units Skills Training & Development (Individual) 48 units Skills Training & Development (Group) 18 units Engagement Activity 36 units Supported Employment 72 units Supported Housing 72 units Crisis Intervention Services (if medically necessary) 24 units
20
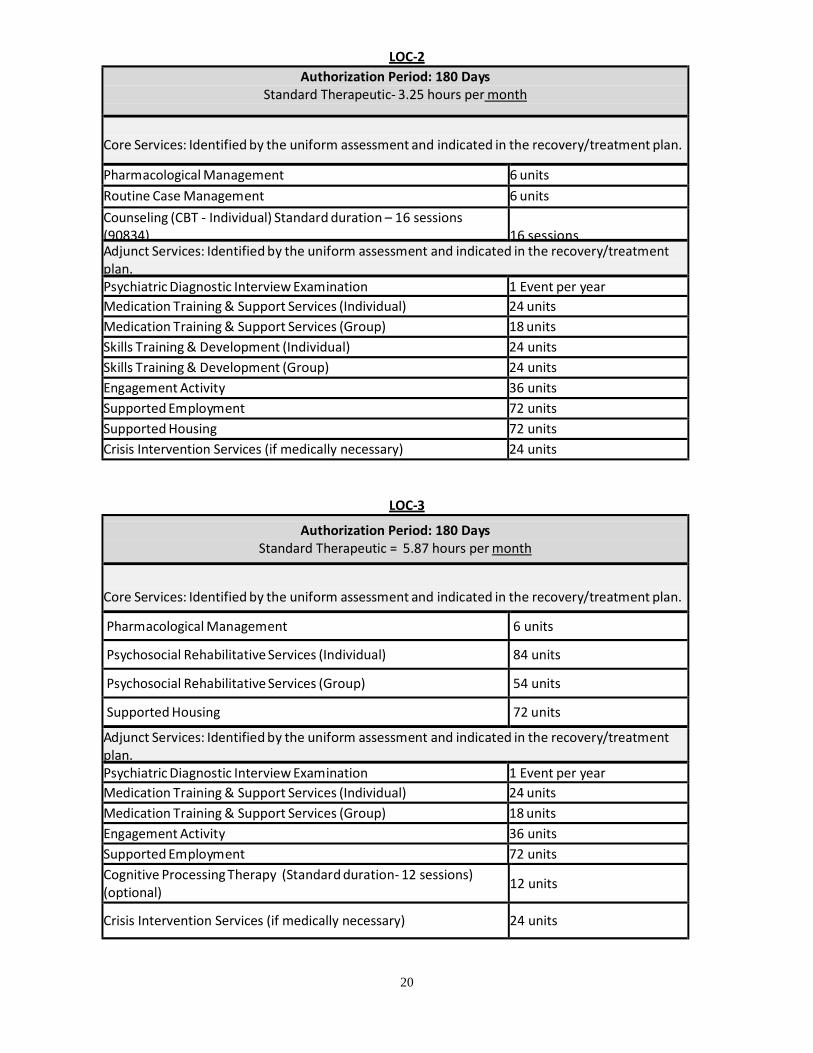
LOC-2 Authorization Period: 180 Days
Standard Therapeutic- 3.25 hours per month
Core Services: Identified by the uniform assessment and indicated in the recovery/treatment plan.
Pharmacological Management 6 units Routine Case Management 6 units Counseling (CBT - Individual) Standard duration – 16 sessions (90834)
16 sessions
Adjunct Services: Identified by the uniform assessment and indicated in the recovery/treatment plan. Psychiatric Diagnostic Interview Examination 1 Event per year Medication Training & Support Services (Individual) 24 units Medication Training & Support Services (Group) 18 units Skills Training & Development (Individual) 24 units Skills Training & Development (Group) 24 units Engagement Activity 36 units Supported Employment 72 units Supported Housing 72 units Crisis Intervention Services (if medically necessary) 24 units
LOC-3
Authorization Period: 180 Days Standard Therapeutic = 5.87 hours per month
Core Services: Identified by the uniform assessment and indicated in the recovery/treatment plan.
Pharmacological Management 6 units
Psychosocial Rehabilitative Services (Individual) 84 units
Psychosocial Rehabilitative Services (Group) 54 units
Supported Housing 72 units
Adjunct Services: Identified by the uniform assessment and indicated in the recovery/treatment plan. Psychiatric Diagnostic Interview Examination 1 Event per year Medication Training & Support Services (Individual) 24 units Medication Training & Support Services (Group) 18 units Engagement Activity 36 units Supported Employment 72 units Cognitive Processing Therapy (Standard duration- 12 sessions) (optional) 12 units
Crisis Intervention Services (if medically necessary) 24 units
21
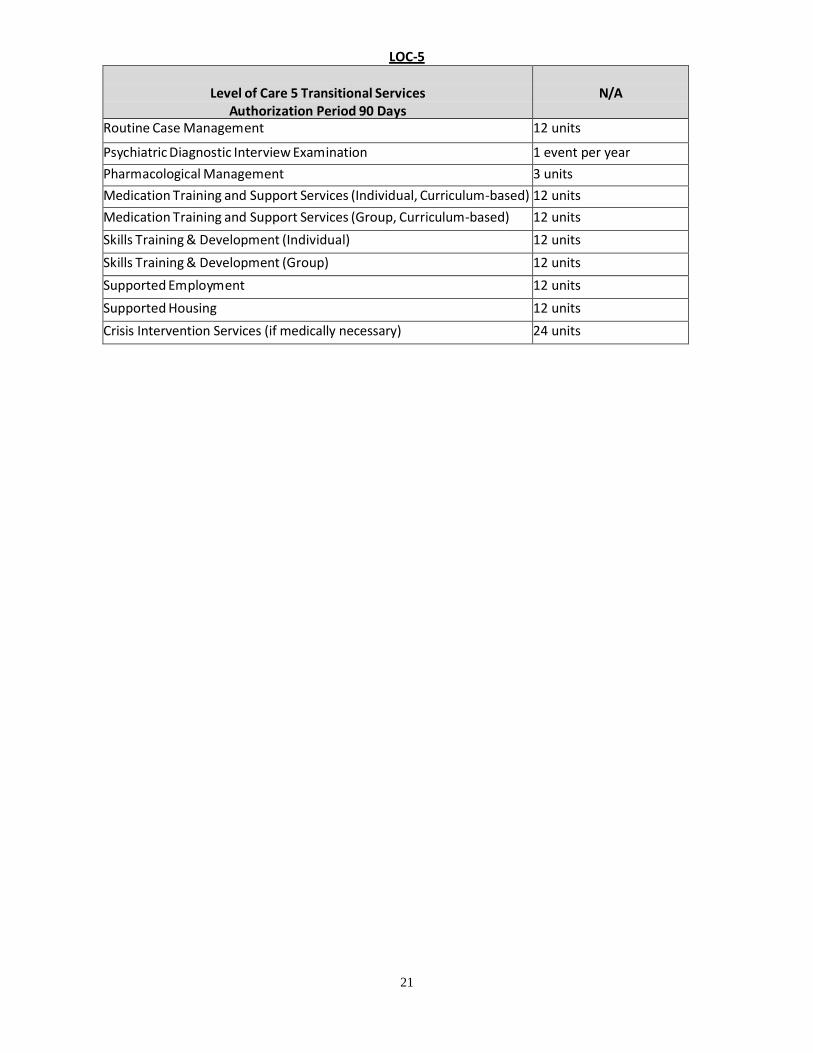
LOC-5
Level of Care 5 Transitional Services Authorization Period 90 Days
N/A
Routine Case Management 12 units
Psychiatric Diagnostic Interview Examination 1 event per year Pharmacological Management 3 units Medication Training and Support Services (Individual, Curriculum -based) 12 units Medication Training and Support Services (Group, Curriculum -based) 12 units Skills Training & Development (Individual) 12 units Skills Training & Development (Group) 12 units Supported Employment 12 units Supported Housing 12 units Crisis Intervention Services (if medically necessary) 24 units
22
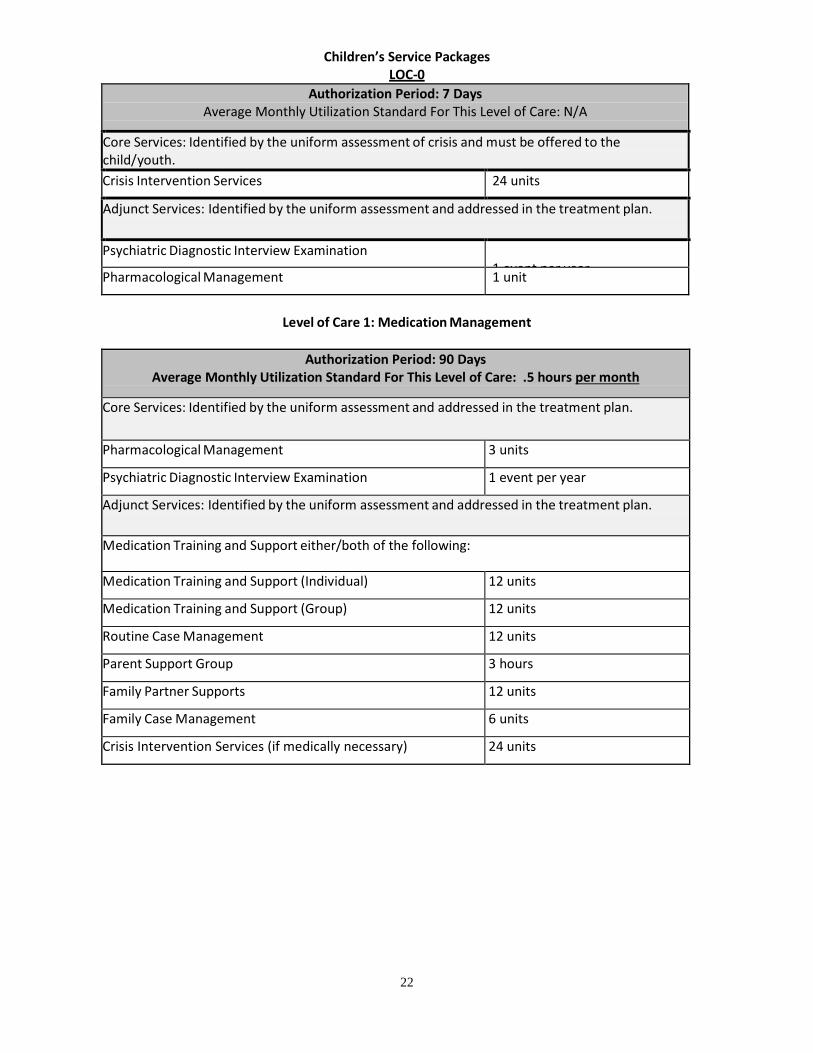
Children’s Service Packages LOC-0
Authorization Period: 7 Days Average Monthly Utilization Standard For This Level of Care: N/A
Core Services: Identified by the uniform assessment of crisis and must be offered to the child/youth. Crisis Intervention Services 24 units
Adjunct Services: Identified by the uniform assessment and addressed in the treatment plan.
Psychiatric Diagnostic Interview Examination 1 event per year Pharmacological Management 1 unit
Level of Care 1: Medication Management
Authorization Period: 90 Days
Average Monthly Utilization Standard For This Level of Care: .5 hours per month
Core Services: Identified by the uniform assessment and addressed in the treatment plan.
Pharmacological Management 3 units
Psychiatric Diagnostic Interview Examination 1 event per year
Adjunct Services: Identified by the uniform assessment and addressed in the treatment plan.
Medication Training and Support either/both of the following:
Medication Training and Support (Individual) 12 units
Medication Training and Support (Group) 12 units
Routine Case Management 12 units
Parent Support Group 3 hours
Family Partner Supports 12 units
Family Case Management 6 units
Crisis Intervention Services (if medically necessary) 24 units
23
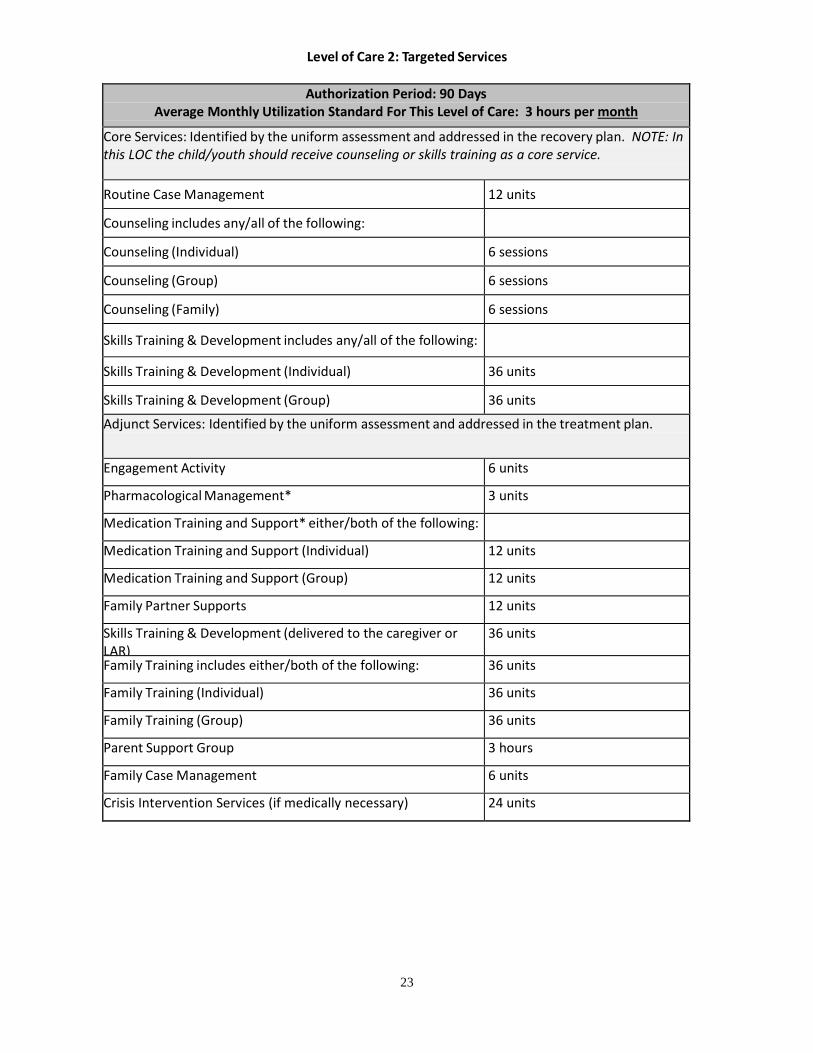
Level of Care 2: Targeted Services
Authorization Period: 90 Days Average Monthly Utilization Standard For This Level of Care: 3 hours per month
Core Services: Identified by the uniform assessment and addressed in the recovery plan. NOTE: In this LOC the child/youth should receive counseling or skills training as a core service.
Routine Case Management 12 units
Counseling includes any/all of the following:
Counseling (Individual) 6 sessions
Counseling (Group) 6 sessions
Counseling (Family) 6 sessions
Skills Training & Development includes any/all of the following:
Skills Training & Development (Individual) 36 units
Skills Training & Development (Group) 36 units
Adjunct Services: Identified by the uniform assessment and addressed in the treatment plan.
Engagement Activity 6 units
Pharmacological Management* 3 units
Medication Training and Support* either/both of the following:
Medication Training and Support (Individual) 12 units
Medication Training and Support (Group) 12 units
Family Partner Supports 12 units
Skills Training & Development (delivered to the caregiver or LAR)
36 units
Family Training includes either/both of the following: 36 units
Family Training (Individual) 36 units
Family Training (Group) 36 units
Parent Support Group 3 hours
Family Case Management 6 units
Crisis Intervention Services (if medically necessary) 24 units
24
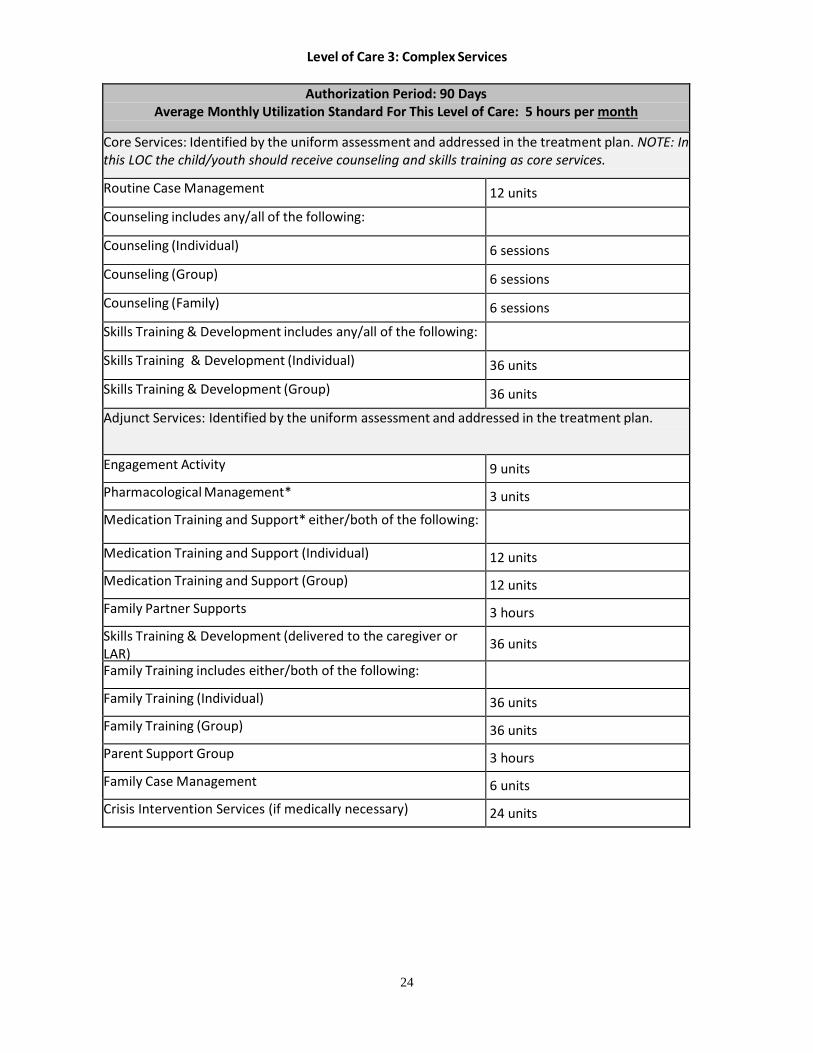
Level of Care 3: Complex Services
Authorization Period: 90 Days Average Monthly Utilization Standard For This Level of Care: 5 hours per month
Core Services: Identified by the uniform assessment and addressed in the treatment plan. NOTE: In this LOC the child/youth should receive counseling and skills training as core services.
Routine Case Management 12 units
Counseling includes any/all of the following:
Counseling (Individual) 6 sessions
Counseling (Group) 6 sessions
Counseling (Family) 6 sessions
Skills Training & Development includes any/all of the following:
Skills Training & Development (Individual) 36 units
Skills Training & Development (Group) 36 units
Adjunct Services: Identified by the uniform assessment and addressed in the treatment plan.
Engagement Activity 9 units
Pharmacological Management* 3 units Medication Training and Support* either/both of the following:
Medication Training and Support (Individual) 12 units Medication Training and Support (Group) 12 units
Family Partner Supports 3 hours
Skills Training & Development (delivered to the caregiver or LAR)
36 units
Family Training includes either/both of the following:
Family Training (Individual) 36 units
Family Training (Group) 36 units Parent Support Group 3 hours
Family Case Management 6 units
Crisis Intervention Services (if medically necessary) 24 units
25
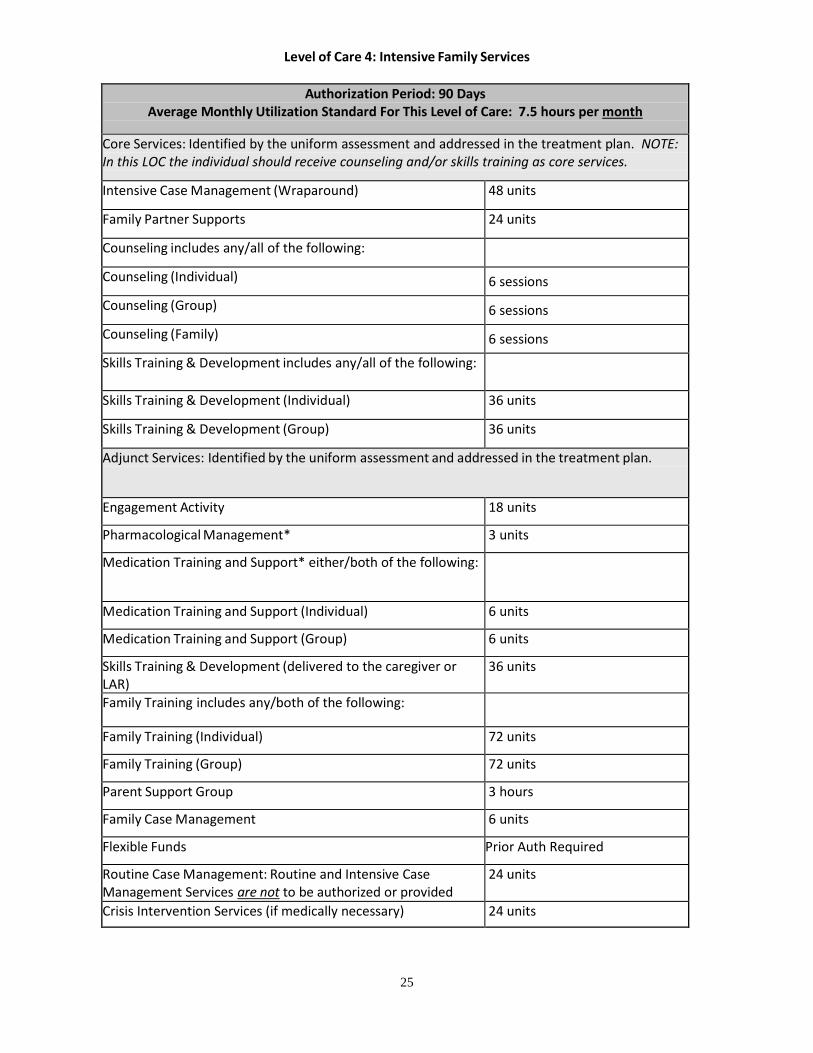
Level of Care 4: Intensive Family Services
Authorization Period: 90 Days Average Monthly Utilization Standard For This Level of Care: 7.5 hours per month
Core Services: Identified by the uniform assessment and addressed in the treatment plan. NOTE: In this LOC the individual should receive counseling and/or skills training as core services.
Intensive Case Management (Wraparound) 48 units
Family Partner Supports 24 units
Counseling includes any/all of the following:
Counseling (Individual) 6 sessions
Counseling (Group) 6 sessions
Counseling (Family) 6 sessions
Skills Training & Development includes any/all of the following:
Skills Training & Development (Individual) 36 units
Skills Training & Development (Group) 36 units
Adjunct Services: Identified by the uniform assessment and addressed in the treatment plan.
Engagement Activity 18 units
Pharmacological Management* 3 units
Medication Training and Support* either/both of the following:
Medication Training and Support (Individual) 6 units
Medication Training and Support (Group) 6 units
Skills Training & Development (delivered to the caregiver or LAR)
36 units
Family Training includes any/both of the following:
Family Training (Individual) 72 units
Family Training (Group) 72 units
Parent Support Group 3 hours
Family Case Management 6 units
Flexible Funds Prior Auth Required
Routine Case Management: Routine and Intensive Case Management Services are not to be authorized or provided
24 units
Crisis Intervention Services (if medically necessary) 24 units
26
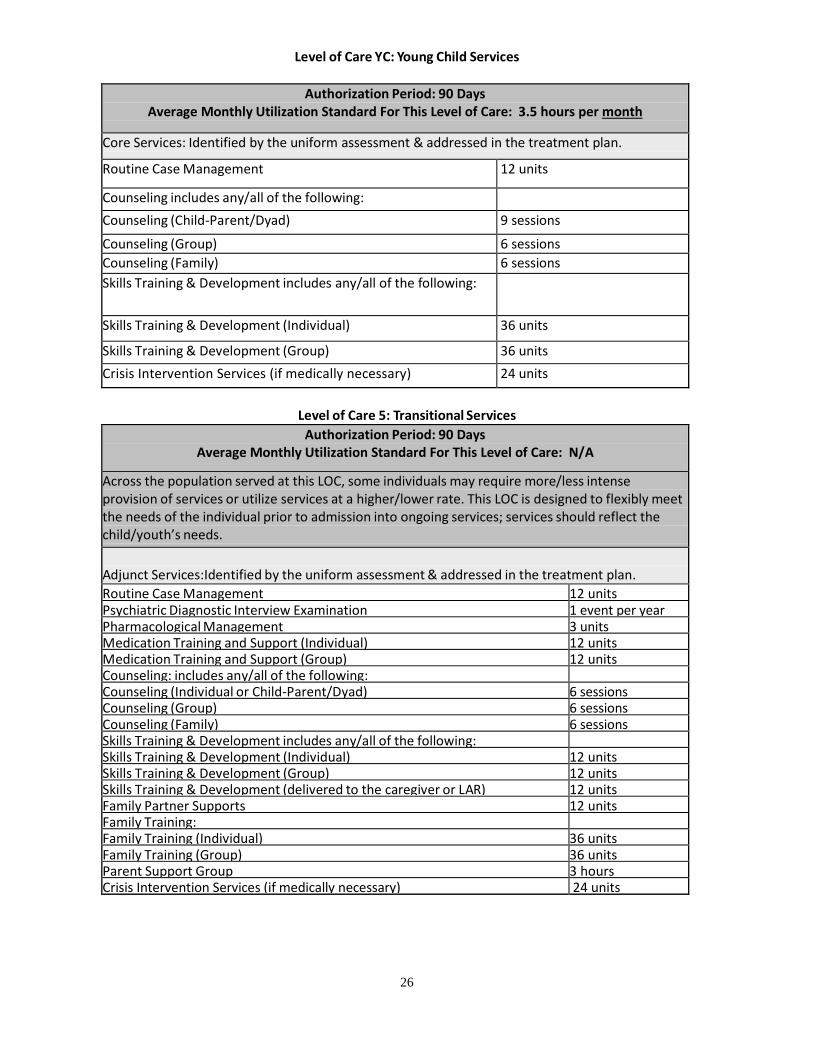
Level of Care YC: Young Child Services
Authorization Period: 90 Days Average Monthly Utilization Standard For This Level of Care: 3.5 hours per month
Core Services: Identified by the uniform assessment & addressed in the treatment plan.
Routine Case Management 12 units
Counseling includes any/all of the following: Counseling (Child-Parent/Dyad) 9 sessions
Counseling (Group) 6 sessions Counseling (Family) 6 sessions Skills Training & Development includes any/all of the following:
Skills Training & Development (Individual) 36 units
Skills Training & Development (Group) 36 units Crisis Intervention Services (if medically necessary) 24 units
Level of Care 5: Transitional Services
Authorization Period: 90 Days Average Monthly Utilization Standard For This Level of Care: N/A
Across the population served at this LOC, some individuals may require more/less intense provision of services or utilize services at a higher/lower rate. This LOC is designed to flexibly meet the needs of the individual prior to admission into ongoing services; services should reflect the child/youth’s needs. Adjunct Services:Identified by the uniform assessment & addressed in the treatment plan. Routine Case Management 12 units Psychiatric Diagnostic Interview Examination 1 event per year Pharmacological Management 3 units Medication Training and Support (Individual) 12 units Medication Training and Support (Group) 12 units Counseling: includes any/all of the following: Counseling (Individual or Child-Parent/Dyad) 6 sessions Counseling (Group) 6 sessions Counseling (Family) 6 sessions Skills Training & Development includes any/all of the following: Skills Training & Development (Individual) 12 units Skills Training & Development (Group) 12 units Skills Training & Development (delivered to the caregiver or LAR) 12 units Family Partner Supports 12 units Family Training: Family Training (Individual) 36 units Family Training (Group) 36 units Parent Support Group 3 hours Crisis Intervention Services (if medically necessary) 24 units
27
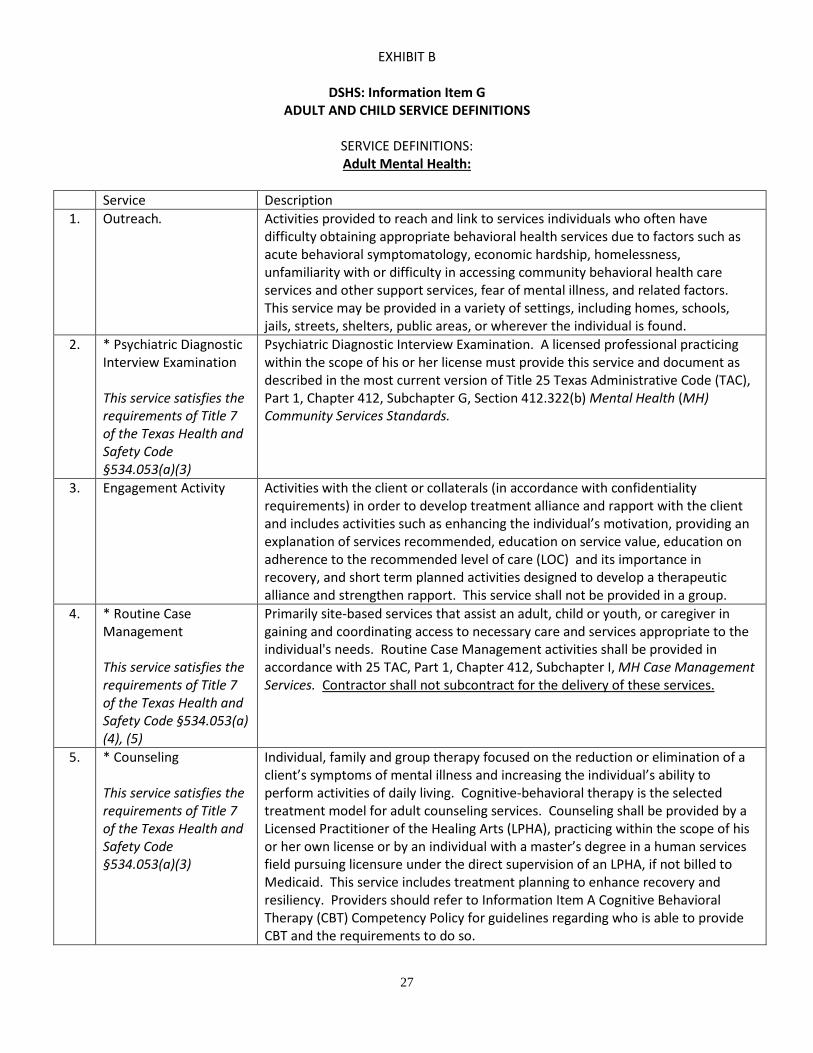
EXHIBIT B
DSHS: Information Item G ADULT AND CHILD SERVICE DEFINITIONS
SERVICE DEFINITIONS: Adult Mental Health:
Service Description
1. Outreach. Activities provided to reach and link to services individuals who often have difficulty obtaining appropriate behavioral health services due to factors such as acute behavioral symptomatology, economic hardship, homelessness, unfamiliarity with or difficulty in accessing community behavioral health care services and other support services, fear of mental illness, and related factors. This service may be provided in a variety of settings, including homes, schools, jails, streets, shelters, public areas, or wherever the individual is found.
2. * Psychiatric Diagnostic Interview Examination This service satisfies the requirements of Title 7 of the Texas Health and Safety Code §534.053(a)(3)
Psychiatric Diagnostic Interview Examination. A licensed professional practicing within the scope of his or her license must provide this service and document as described in the most current version of Title 25 Texas Administrative Code (TAC), Part 1, Chapter 412, Subchapter G, Section 412.322(b) Mental Health (MH) Community Services Standards.
3. Engagement Activity Activities with the client or collaterals (in accordance with confidentiality requirements) in order to develop treatment alliance and rapport with the client and includes activities such as enhancing the individual’s motivation, providing an explanation of services recommended, education on service value, education on adherence to the recommended level of care (LOC) and its importance in recovery, and short term planned activities designed to develop a therapeutic alliance and strengthen rapport. This service shall not be provided in a group.
4. * Routine Case Management This service satisfies the requirements of Title 7 of the Texas Health and Safety Code §534.053(a) (4), (5)
Primarily site-based services that assist an adult, child or youth, or caregiver in gaining and coordinating access to necessary care and services appropriate to the individual's needs. Routine Case Management activities shall be provided in accordance with 25 TAC, Part 1, Chapter 412, Subchapter I, MH Case Management Services. Contractor shall not subcontract for the delivery of these services.
5. * Counseling This service satisfies the requirements of Title 7 of the Texas Health and Safety Code §534.053(a)(3)
Individual, family and group therapy focused on the reduction or elimination of a client’s symptoms of mental illness and increasing the individual’s ability to perform activities of daily living. Cognitive-behavioral therapy is the selected treatment model for adult counseling services. Counseling shall be provided by a Licensed Practitioner of the Healing Arts (LPHA), practicing within the scope of his or her own license or by an individual with a master’s degree in a human services field pursuing licensure under the direct supervision of an LPHA, if not billed to Medicaid. This service includes treatment planning to enhance recovery and resiliency. Providers should refer to Information Item A Cognitive Behavioral Therapy (CBT) Competency Policy for guidelines regarding who is able to provide CBT and the requirements to do so.
28
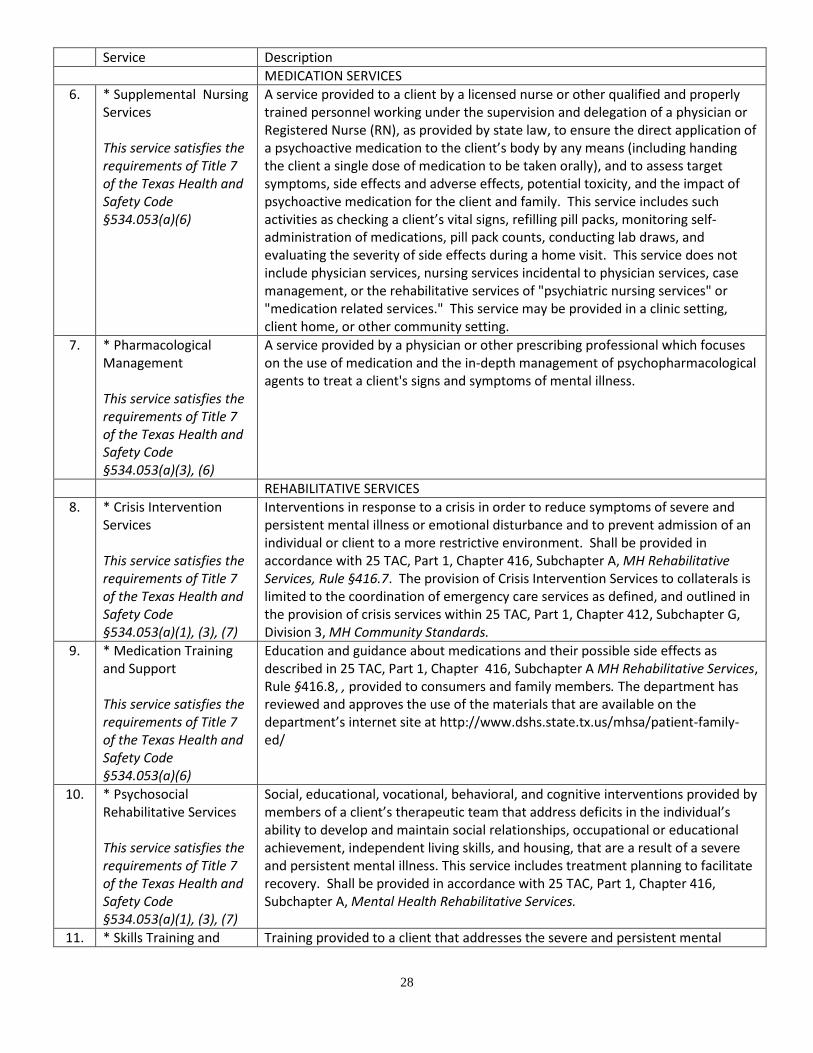
Service Description MEDICATION SERVICES
6. * Supplemental Nursing Services This service satisfies the requirements of Title 7 of the Texas Health and Safety Code §534.053(a)(6)
A service provided to a client by a licensed nurse or other qualified and properly trained personnel working under the supervision and delegation of a physician or Registered Nurse (RN), as provided by state law, to ensure the direct application of a psychoactive medication to the client’s body by any means (including handing the client a single dose of medication to be taken orally), and to assess target symptoms, side effects and adverse effects, potential toxicity, and the impact of psychoactive medication for the client and family. This service includes such activities as checking a client’s vital signs, refilling pill packs, monitoring self-administration of medications, pill pack counts, conducting lab draws, and evaluating the severity of side effects during a home visit. This service does not include physician services, nursing services incidental to physician services, case management, or the rehabilitative services of "psychiatric nursing services" or "medication related services." This service may be provided in a clinic setting, client home, or other community setting.
7. * Pharmacological Management This service satisfies the requirements of Title 7 of the Texas Health and Safety Code §534.053(a)(3), (6)
A service provided by a physician or other prescribing professional which focuses on the use of medication and the in-depth management of psychopharmacological agents to treat a client's signs and symptoms of mental illness.
REHABILITATIVE SERVICES 8. * Crisis Intervention
Services This service satisfies the requirements of Title 7 of the Texas Health and Safety Code §534.053(a)(1), (3), (7)
Interventions in response to a crisis in order to reduce symptoms of severe and persistent mental illness or emotional disturbance and to prevent admission of an individual or client to a more restrictive environment. Shall be provided in accordance with 25 TAC, Part 1, Chapter 416, Subchapter A, MH Rehabilitative Services, Rule §416.7. The provision of Crisis Intervention Services to collaterals is limited to the coordination of emergency care services as defined, and outlined in the provision of crisis services within 25 TAC, Part 1, Chapter 412, Subchapter G, Division 3, MH Community Standards.
9. * Medication Training and Support This service satisfies the requirements of Title 7 of the Texas Health and Safety Code §534.053(a)(6)
Education and guidance about medications and their possible side effects as described in 25 TAC, Part 1, Chapter 416, Subchapter A MH Rehabilitative Services, Rule §416.8, , provided to consumers and family members. The department has reviewed and approves the use of the materials that are available on the department’s internet site at http://www.dshs.state.tx.us/mhsa/patient-family-ed/
10. * Psychosocial Rehabilitative Services This service satisfies the requirements of Title 7 of the Texas Health and Safety Code §534.053(a)(1), (3), (7)
Social, educational, vocational, behavioral, and cognitive interventions provided by members of a client’s therapeutic team that address deficits in the individual’s ability to develop and maintain social relationships, occupational or educational achievement, independent living skills, and housing, that are a result of a severe and persistent mental illness. This service includes treatment planning to facilitate recovery. Shall be provided in accordance with 25 TAC, Part 1, Chapter 416, Subchapter A, Mental Health Rehabilitative Services.
11. * Skills Training and Training provided to a client that addresses the severe and persistent mental
29
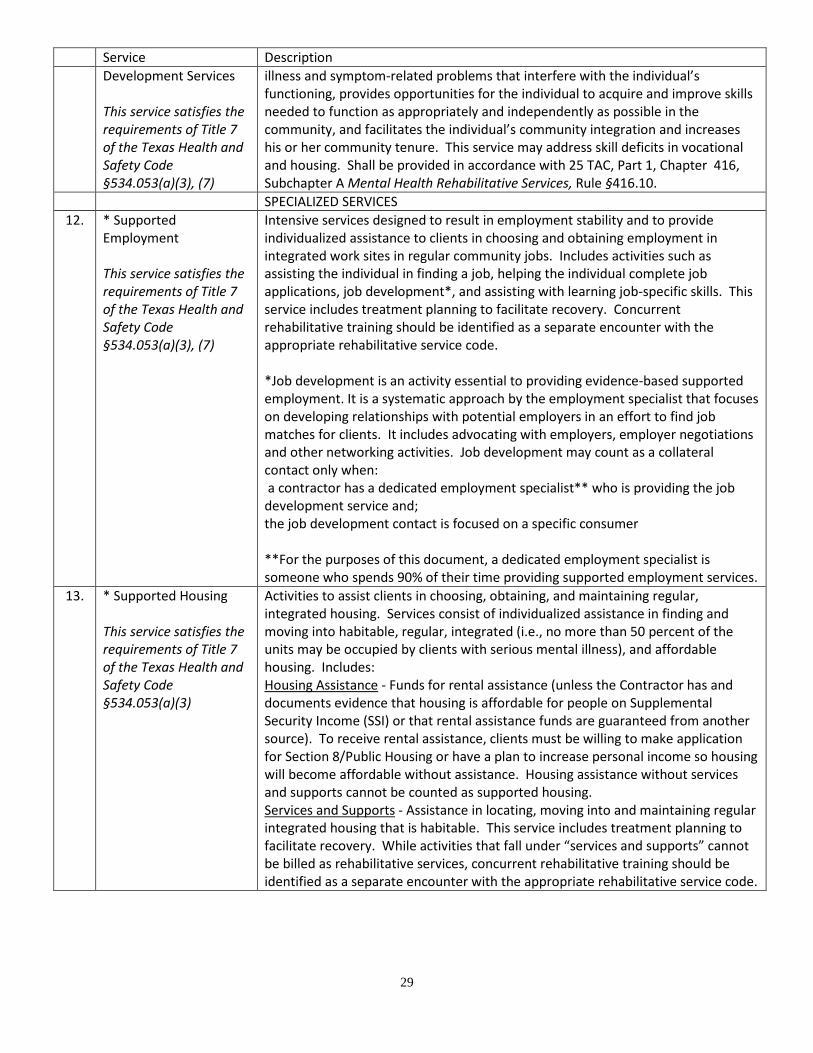
Service Description Development Services This service satisfies the requirements of Title 7 of the Texas Health and Safety Code §534.053(a)(3), (7)
illness and symptom-related problems that interfere with the individual’s functioning, provides opportunities for the individual to acquire and improve skills needed to function as appropriately and independently as possible in the community, and facilitates the individual’s community integration and increases his or her community tenure. This service may address skill deficits in vocational and housing. Shall be provided in accordance with 25 TAC, Part 1, Chapter 416, Subchapter A Mental Health Rehabilitative Services, Rule §416.10.
SPECIALIZED SERVICES 12. * Supported
Employment This service satisfies the requirements of Title 7 of the Texas Health and Safety Code §534.053(a)(3), (7)
Intensive services designed to result in employment stability and to provide individualized assistance to clients in choosing and obtaining employment in integrated work sites in regular community jobs. Includes activities such as assisting the individual in finding a job, helping the individual complete job applications, job development*, and assisting with learning job-specific skills. This service includes treatment planning to facilitate recovery. Concurrent rehabilitative training should be identified as a separate encounter with the appropriate rehabilitative service code. *Job development is an activity essential to providing evidence-based supported employment. It is a systematic approach by the employment specialist that focuses on developing relationships with potential employers in an effort to find job matches for clients. It includes advocating with employers, employer negotiations and other networking activities. Job development may count as a collateral contact only when: a contractor has a dedicated employment specialist** who is providing the job development service and; the job development contact is focused on a specific consumer **For the purposes of this document, a dedicated employment specialist is someone who spends 90% of their time providing supported employment services.
13. * Supported Housing This service satisfies the requirements of Title 7 of the Texas Health and Safety Code §534.053(a)(3)
Activities to assist clients in choosing, obtaining, and maintaining regular, integrated housing. Services consist of individualized assistance in finding and moving into habitable, regular, integrated (i.e., no more than 50 percent of the units may be occupied by clients with serious mental illness), and affordable housing. Includes: Housing Assistance - Funds for rental assistance (unless the Contractor has and documents evidence that housing is affordable for people on Supplemental Security Income (SSI) or that rental assistance funds are guaranteed from another source). To receive rental assistance, clients must be willing to make application for Section 8/Public Housing or have a plan to increase personal income so housing will become affordable without assistance. Housing assistance without services and supports cannot be counted as supported housing. Services and Supports - Assistance in locating, moving into and maintaining regular integrated housing that is habitable. This service includes treatment planning to facilitate recovery. While activities that fall under “services and supports” cannot be billed as rehabilitative services, concurrent rehabilitative training should be identified as a separate encounter with the appropriate rehabilitative service code.
30
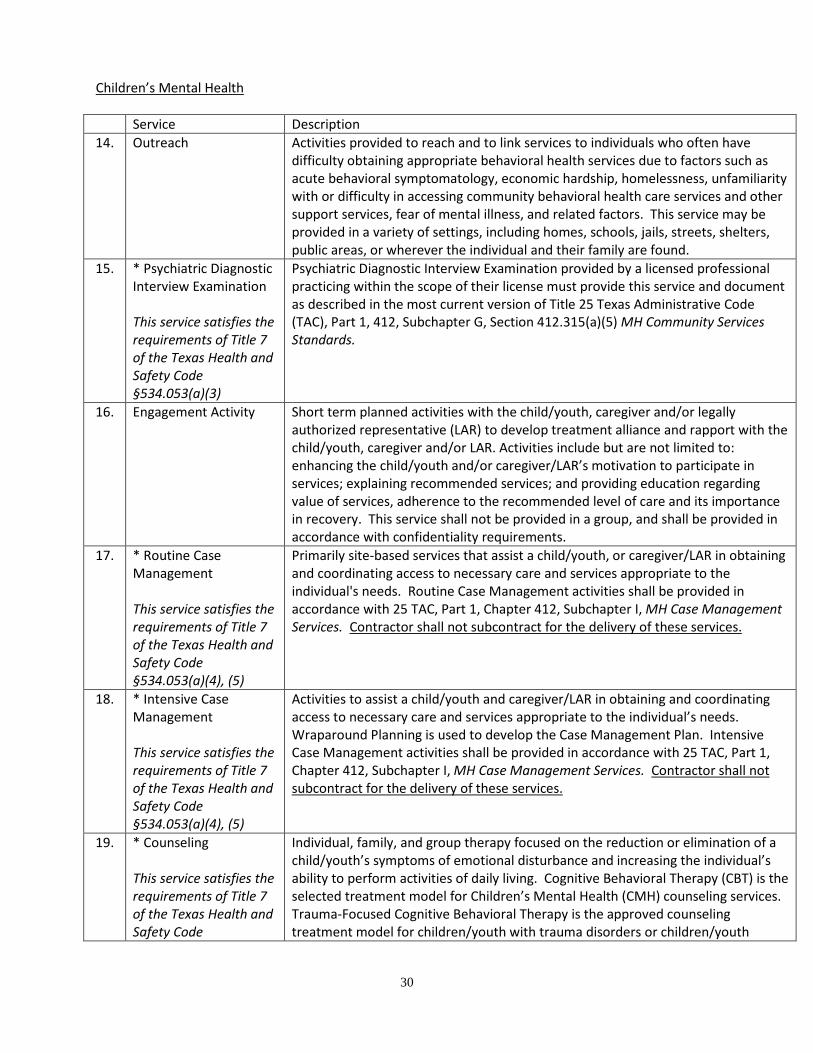
Children’s Mental Health
Service Description 14. Outreach Activities provided to reach and to link services to individuals who often have
difficulty obtaining appropriate behavioral health services due to factors such as acute behavioral symptomatology, economic hardship, homelessness, unfamiliarity with or difficulty in accessing community behavioral health care services and other support services, fear of mental illness, and related factors. This service may be provided in a variety of settings, including homes, schools, jails, streets, shelters, public areas, or wherever the individual and their family are found.
15. * Psychiatric Diagnostic Interview Examination This service satisfies the requirements of Title 7 of the Texas Health and Safety Code §534.053(a)(3)
Psychiatric Diagnostic Interview Examination provided by a licensed professional practicing within the scope of their license must provide this service and document as described in the most current version of Title 25 Texas Administrative Code (TAC), Part 1, 412, Subchapter G, Section 412.315(a)(5) MH Community Services Standards.
16. Engagement Activity
Short term planned activities with the child/youth, caregiver and/or legally authorized representative (LAR) to develop treatment alliance and rapport with the child/youth, caregiver and/or LAR. Activities include but are not limited to: enhancing the child/youth and/or caregiver/LAR’s motivation to participate in services; explaining recommended services; and providing education regarding value of services, adherence to the recommended level of care and its importance in recovery. This service shall not be provided in a group, and shall be provided in accordance with confidentiality requirements.
17. * Routine Case Management This service satisfies the requirements of Title 7 of the Texas Health and Safety Code §534.053(a)(4), (5)
Primarily site-based services that assist a child/youth, or caregiver/LAR in obtaining and coordinating access to necessary care and services appropriate to the individual's needs. Routine Case Management activities shall be provided in accordance with 25 TAC, Part 1, Chapter 412, Subchapter I, MH Case Management Services. Contractor shall not subcontract for the delivery of these services.
18. * Intensive Case Management This service satisfies the requirements of Title 7 of the Texas Health and Safety Code §534.053(a)(4), (5)
Activities to assist a child/youth and caregiver/LAR in obtaining and coordinating access to necessary care and services appropriate to the individual’s needs. Wraparound Planning is used to develop the Case Management Plan. Intensive Case Management activities shall be provided in accordance with 25 TAC, Part 1, Chapter 412, Subchapter I, MH Case Management Services. Contractor shall not subcontract for the delivery of these services.
19. * Counseling This service satisfies the requirements of Title 7 of the Texas Health and Safety Code
Individual, family, and group therapy focused on the reduction or elimination of a child/youth’s symptoms of emotional disturbance and increasing the individual’s ability to perform activities of daily living. Cognitive Behavioral Therapy (CBT) is the selected treatment model for Children’s Mental Health (CMH) counseling services. Trauma-Focused Cognitive Behavioral Therapy is the approved counseling treatment model for children/youth with trauma disorders or children/youth
31
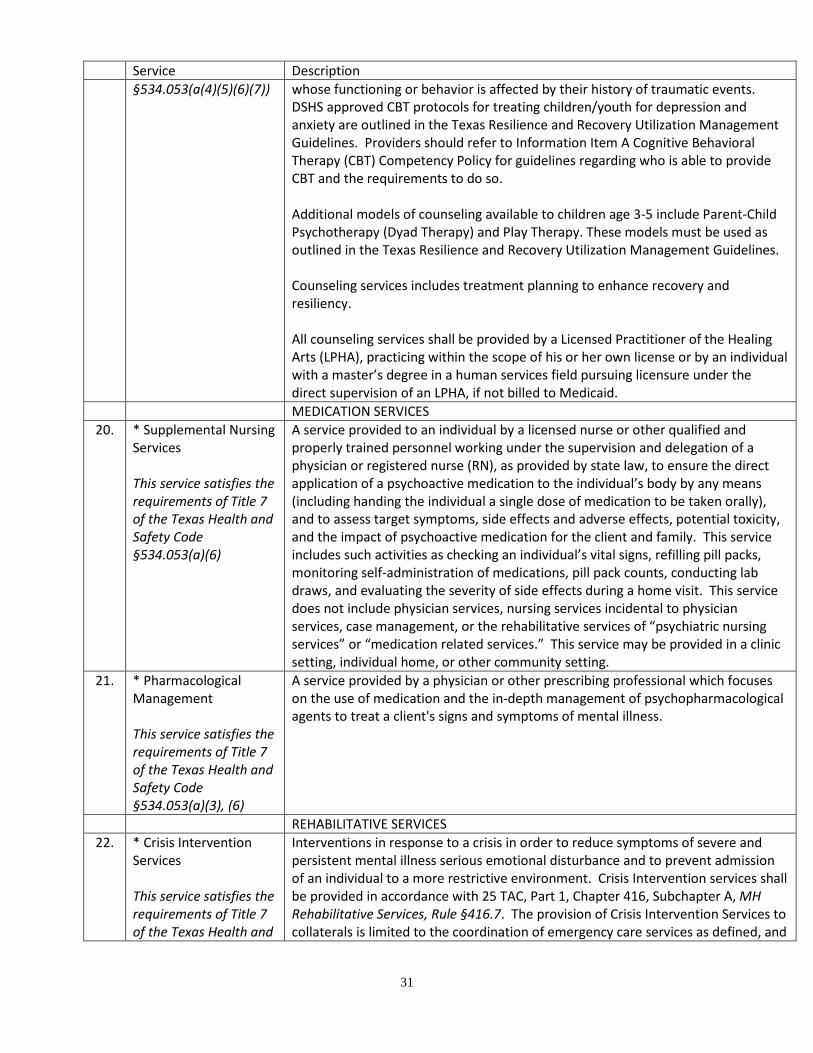
Service Description §534.053(a(4)(5)(6)(7)) whose functioning or behavior is affected by their history of traumatic events.
DSHS approved CBT protocols for treating children/youth for depression and anxiety are outlined in the Texas Resilience and Recovery Utilization Management Guidelines. Providers should refer to Information Item A Cognitive Behavioral Therapy (CBT) Competency Policy for guidelines regarding who is able to provide CBT and the requirements to do so. Additional models of counseling available to children age 3-5 include Parent-Child Psychotherapy (Dyad Therapy) and Play Therapy. These models must be used as outlined in the Texas Resilience and Recovery Utilization Management Guidelines. Counseling services includes treatment planning to enhance recovery and resiliency. All counseling services shall be provided by a Licensed Practitioner of the Healing Arts (LPHA), practicing within the scope of his or her own license or by an individual with a master’s degree in a human services field pursuing licensure under the direct supervision of an LPHA, if not billed to Medicaid.
MEDICATION SERVICES 20. * Supplemental Nursing
Services This service satisfies the requirements of Title 7 of the Texas Health and Safety Code §534.053(a)(6)
A service provided to an individual by a licensed nurse or other qualified and properly trained personnel working under the supervision and delegation of a physician or registered nurse (RN), as provided by state law, to ensure the direct application of a psychoactive medication to the individual’s body by any means (including handing the individual a single dose of medication to be taken orally), and to assess target symptoms, side effects and adverse effects, potential toxicity, and the impact of psychoactive medication for the client and family. This service includes such activities as checking an individual’s vital signs, refilling pill packs, monitoring self-administration of medications, pill pack counts, conducting lab draws, and evaluating the severity of side effects during a home visit. This service does not include physician services, nursing services incidental to physician services, case management, or the rehabilitative services of “psychiatric nursing services” or “medication related services.” This service may be provided in a clinic setting, individual home, or other community setting.
21. * Pharmacological Management This service satisfies the requirements of Title 7 of the Texas Health and Safety Code §534.053(a)(3), (6)
A service provided by a physician or other prescribing professional which focuses on the use of medication and the in-depth management of psychopharmacological agents to treat a client's signs and symptoms of mental illness.
REHABILITATIVE SERVICES 22. * Crisis Intervention
Services This service satisfies the requirements of Title 7 of the Texas Health and
Interventions in response to a crisis in order to reduce symptoms of severe and persistent mental illness serious emotional disturbance and to prevent admission of an individual to a more restrictive environment. Crisis Intervention services shall be provided in accordance with 25 TAC, Part 1, Chapter 416, Subchapter A, MH Rehabilitative Services, Rule §416.7. The provision of Crisis Intervention Services to collaterals is limited to the coordination of emergency care services as defined, and

32
Service Description Safety Code §534.053(a)(1), (3), (7)
outlined in the provision of crisis services within 25 TAC, Part 1, Chapter 412, Subchapter G, Division 3, MH Community Standards.
23. * Medication Training and Support This service satisfies the requirements of Title 7 of the Texas Health and Safety Code §534.053(a)(6)
Education and guidance about medications and their possible side effects as described in 25 TAC, Part 1, Chapter 416, Subchapter A MH Rehabilitative Services, Rule §416.8, , provided to children, youths, and caregivers and/or LAR. The department has reviewed and approves the use of the materials that are available on the department’s internet site at http://www.dshs.state.tx.us/mhsa/patient-family-ed/
24. * Skills Training and Development Services This service satisfies the requirements of Title 7 of the Texas Health and Safety Code §534.053(a)(3), (7)
Training provided to an individual and/or the primary caregiver or legally authorized representative (LAR) that addresses the serious emotional disturbance and symptom-related problems that interfere with the individual’s functioning, provides opportunities for the individual to acquire and improve skills needed to function as appropriately and independently as possible in the community, and facilitates the individual’s community integration and increases his or her community tenure. For 17-year-old youth, skills training and development may also include supported employment and supported housing services delivered as defined above for Adult Mental Health Services. Must be provided in accordance with 25 TAC, Part 1, Chapter 416, Subchapter A MH Rehabilitative Services, Rule §416.10.
SPECIALIZED SERVICES 25. * Family Case
Management This service satisfies the requirements of Title 7 of the Texas Health and Safety Code §534.053(a)(3), (4)
Activities to assist the individual’s family members in accessing and coordinating necessary care and services appropriate to the family members’ needs. The need for Family Case Management shall be documented in the individual’s Case Management Plan.
26. * Family Training This service satisfies the requirements of Title 7 of the Texas Health and Safety Code §534.053(a)(4)
Training provided to the individual’s primary caregivers to assist the caregivers in coping and managing with the individual’s emotional disturbance. This includes instruction on basic parenting skills and other forms of guidance that cannot be considered rehabilitative skills training. Concurrent rehabilitative training should be identified as a separate encounter with the appropriate rehabilitative service code.
27. * Family Partner Supports This service satisfies the requirements of Title 7 of the Texas Health and Safety Code §534.053(a)(4)
Peer mentoring and support provided by Certified Family Partners to the primary caregivers of a child who is receiving mental health community services. This may include introducing the family to the treatment process; modeling self-advocacy skills; providing information, making referrals; providing non-clinical skills training; assisting in the identification of natural/non-traditional and community supports. Family Partners are the parent or LAR of a child or youth with a serious emotional disturbance and have at least one year of experience navigating a child-serving system (e.g. mental health, juvenile justice, social security, special education) as the LAR to that child or youth. (TAC Title 25 Part 1 Chapter 412 Subchapter G Division 1)
28. * Parent Support Routinely scheduled support and informational meetings for the individual’s
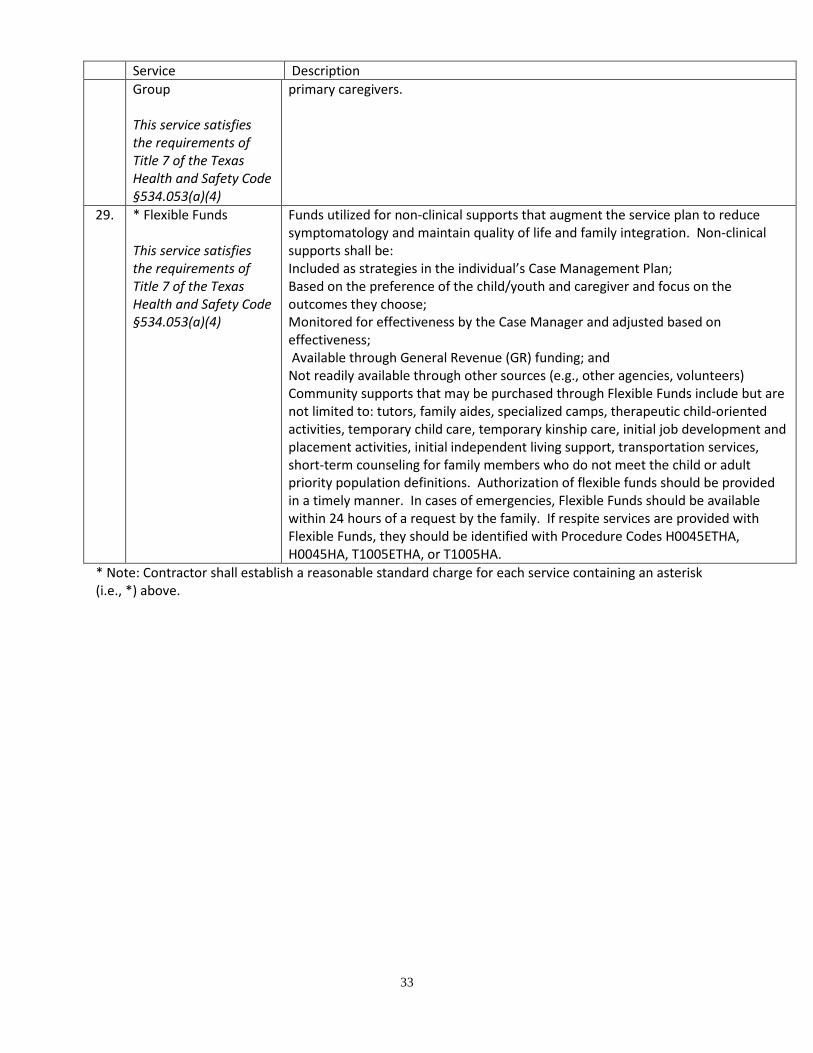
33
Service Description Group This service satisfies the requirements of Title 7 of the Texas Health and Safety Code §534.053(a)(4)
primary caregivers.
29. * Flexible Funds This service satisfies the requirements of Title 7 of the Texas Health and Safety Code §534.053(a)(4)
Funds utilized for non-clinical supports that augment the service plan to reduce symptomatology and maintain quality of life and family integration. Non-clinical supports shall be: Included as strategies in the individual’s Case Management Plan; Based on the preference of the child/youth and caregiver and focus on the outcomes they choose; Monitored for effectiveness by the Case Manager and adjusted based on effectiveness; Available through General Revenue (GR) funding; and Not readily available through other sources (e.g., other agencies, volunteers) Community supports that may be purchased through Flexible Funds include but are not limited to: tutors, family aides, specialized camps, therapeutic child-oriented activities, temporary child care, temporary kinship care, initial job development and placement activities, initial independent living support, transportation services, short-term counseling for family members who do not meet the child or adult priority population definitions. Authorization of flexible funds should be provided in a timely manner. In cases of emergencies, Flexible Funds should be available within 24 hours of a request by the family. If respite services are provided with Flexible Funds, they should be identified with Procedure Codes H0045ETHA, H0045HA, T1005ETHA, or T1005HA.
* Note: Contractor shall establish a reasonable standard charge for each service containing an asterisk (i.e., *) above.
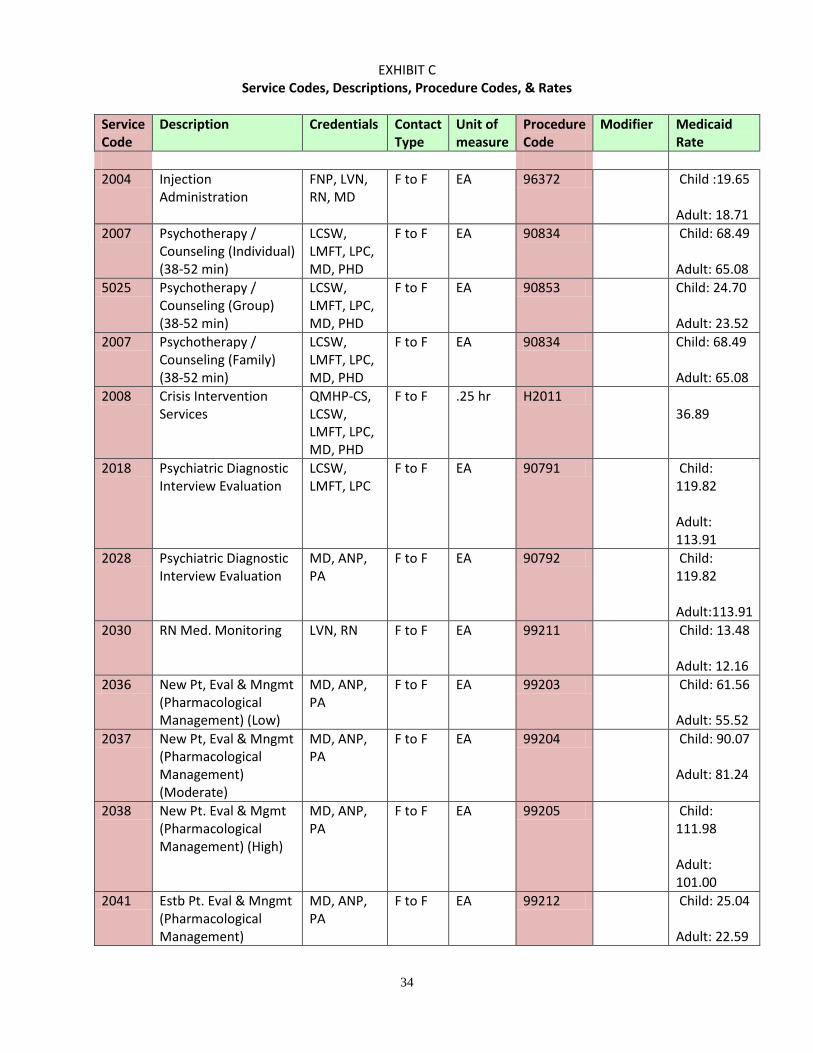
34
EXHIBIT C Service Codes, Descriptions, Procedure Codes, & Rates
Service Code
Description Credentials Contact Type
Unit of measure
Procedure Code
Modifier Medicaid Rate
2004 Injection
Administration FNP, LVN, RN, MD
F to F EA 96372 Child :19.65 Adult: 18.71
2007 Psychotherapy / Counseling (Individual) (38-52 min)
LCSW, LMFT, LPC, MD, PHD
F to F EA 90834 Child: 68.49 Adult: 65.08
5025 Psychotherapy / Counseling (Group) (38-52 min)
LCSW, LMFT, LPC, MD, PHD
F to F EA 90853 Child: 24.70 Adult: 23.52
2007 Psychotherapy / Counseling (Family) (38-52 min)
LCSW, LMFT, LPC, MD, PHD
F to F EA 90834 Child: 68.49 Adult: 65.08
2008 Crisis Intervention Services
QMHP-CS, LCSW, LMFT, LPC, MD, PHD
F to F .25 hr H2011 36.89
2018 Psychiatric Diagnostic Interview Evaluation
LCSW, LMFT, LPC
F to F EA 90791 Child: 119.82 Adult: 113.91
2028 Psychiatric Diagnostic Interview Evaluation
MD, ANP, PA
F to F EA 90792 Child: 119.82 Adult:113.91
2030 RN Med. Monitoring LVN, RN F to F EA 99211 Child: 13.48 Adult: 12.16
2036 New Pt, Eval & Mngmt (Pharmacological Management) (Low)
MD, ANP, PA
F to F EA 99203 Child: 61.56 Adult: 55.52
2037 New Pt, Eval & Mngmt (Pharmacological Management) (Moderate)
MD, ANP, PA
F to F EA 99204 Child: 90.07 Adult: 81.24
2038 New Pt. Eval & Mgmt (Pharmacological Management) (High)
MD, ANP, PA
F to F EA 99205 Child: 111.98 Adult: 101.00
2041 Estb Pt. Eval & Mngmt (Pharmacological Management)
MD, ANP, PA
F to F EA 99212 Child: 25.04 Adult: 22.59
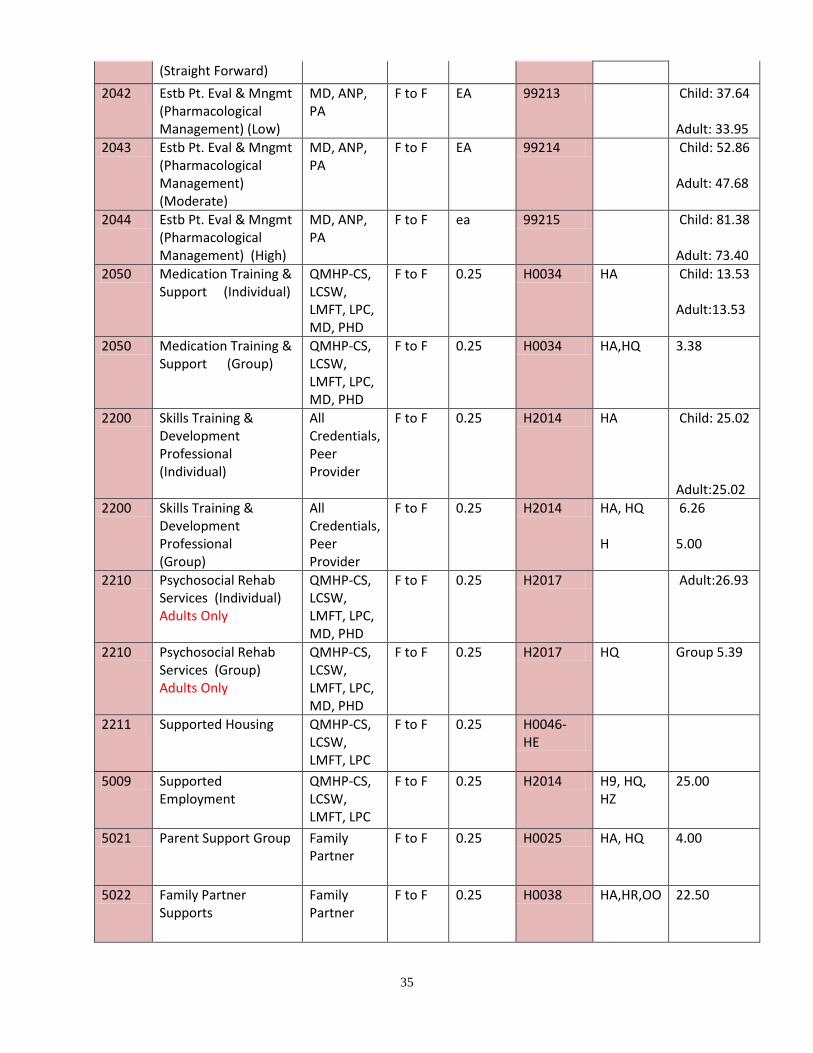
35
(Straight Forward) 2042 Estb Pt. Eval & Mngmt
(Pharmacological Management) (Low)
MD, ANP, PA
F to F EA 99213 Child: 37.64 Adult: 33.95
2043 Estb Pt. Eval & Mngmt (Pharmacological Management) (Moderate)
MD, ANP, PA
F to F EA 99214 Child: 52.86 Adult: 47.68
2044 Estb Pt. Eval & Mngmt (Pharmacological Management) (High)
MD, ANP, PA
F to F ea 99215 Child: 81.38 Adult: 73.40
2050 Medication Training & Support (Individual)
QMHP-CS, LCSW, LMFT, LPC, MD, PHD
F to F 0.25 H0034 HA Child: 13.53 Adult:13.53
2050 Medication Training & Support (Group)
QMHP-CS, LCSW, LMFT, LPC, MD, PHD
F to F 0.25 H0034 HA,HQ 3.38
2200 Skills Training & Development Professional (Individual)
All Credentials, Peer Provider
F to F 0.25 H2014 HA Child: 25.02 Adult:25.02
2200 Skills Training & Development Professional (Group)
All Credentials, Peer Provider
F to F 0.25 H2014 HA, HQ H
6.26 5.00
2210 Psychosocial Rehab Services (Individual) Adults Only
QMHP-CS, LCSW, LMFT, LPC, MD, PHD
F to F 0.25 H2017 Adult:26.93
2210 Psychosocial Rehab Services (Group) Adults Only
QMHP-CS, LCSW, LMFT, LPC, MD, PHD
F to F 0.25 H2017 HQ Group 5.39
2211 Supported Housing QMHP-CS, LCSW, LMFT, LPC
F to F 0.25 H0046- HE
5009 Supported Employment
QMHP-CS, LCSW, LMFT, LPC
F to F 0.25 H2014 H9, HQ, HZ
25.00
5021 Parent Support Group Family Partner
F to F 0.25 H0025 HA, HQ 4.00
5022 Family Partner Supports
Family Partner
F to F 0.25 H0038 HA,HR,OO 22.50

36
5023 Family Training (Individual)
Family Partner
F to F 0.25 H2019 HA 22.50
5023 Family Training (Group)
Family Partner
F to F 0.25 H2019 HA, HQ 4.00
5024 Family Case Management
Family Partner
F to F 0.25 T1016 HA, HE, HS
19.00
5010 Routine Case Management (Adult/Child)
QMHP-CS, LCSW, LMFT, LPC, MD, PHD
F to F 0.25 T1017 TF HA, TF
Adult: 19.83 Child: 24.07
5015 Outreach/Engagement Activity
QMHP-CS, LCSW, LMFT, LPC, MD, PHD
F to F 0.25 H0023 18.00
5020 Intensive Case Management (Child)
QMHP-CS, LCSW, LMFT, LPC, MD, PHD
F to F 0.25 T1017 HA, TG Child:31.69
37
Exhibit D
DSHS: Information Item A I. Cognitive Behavioral Therapy Competency Policy: DSHS has developed a competency-based approach for the delivery of Cognitive Behavioral Therapy (CBT) in our community mental health service delivery system. Every practitioner that provides CBT for adult mental health services or children mental health services must comply with this policy. CBT Competency Standards: A. Existing Staff
1. Submission of a tape to be reviewed and rated by one of the following entities: a) Beck Institute for Cognitive Behavioral Therapy http://www.beckinstitute.org/ b) Academy of Cognitive Therapy http://www.academyofct.org/ c) Reach Institute (Child & Adolescent Providers Only) http://www.thereachinstitute.org/
2. Existing practitioners shall score a 40 or greater to be considered competent (rating is done using the Cognitive Therapy Rating Scale by Beck). This documentation should be maintained in the employee’s personnel file. All practitioners providing CBT must pass the competency review and are subject to limitations regarding their ability to continue to provide CBT services if they do not pass the competency review.
3. Practitioners who have submitted tapes for review to one of the endorsed entities, without passing with a score of 40 within the 12th month of eligibility to pass the CBT competency, will be allowed to provide CBT counseling services until they have gained competency under the following conditions:
a) The practitioner must attend and complete a DSHS approved CBT training conducted by The Academy of Cognitive Therapy (ACT), The Beck Institute, or the REACH Institute every year until practitioner gains CBT competence.
b) The practitioner must practice CBT under the supervision of a practitioner who has passed the CBT competency review. The supervision must include at least weekly supervision meetings that involve practice tape reviews with real clients. The supervision must be documented by supervisor, and must be available per request of DSHS.
c) The practitioner must attempt to pass the CBT competency review by submitting a tape (as indicated in A.1), at least every six months, until practitioner gains CBT competence.
4. A practitioner will be allowed an exception for approved leave, such as military duty, family and medical leave act (FMLA), or other approved leave. When approved leave has been granted, the practitioner will be allowed an extension equal to the time they were away for leave.
B. New Hires
1. All new hires have one year from the date of hire to demonstrate competency as outlined in the competency standards. (For the purposes of this Information Item section, a person is a new hire if they are an external hire or if they move from a different role within the organization to provide CBT counseling services).
2. It is a best practice that new hires submit a tape for competency review within 6 months of hire. 3. Practitioners that have submitted tapes for review to one of the endorsed entities within 1 year,
but have not passed with a score of 40 by the identified timeline are subject to items A.3 and A.4 of this policy.
38
C. Staff Pursuing Independent Licensure
1. Staff with non-independent licenses (i.e. Licensed Professional Counselor-Intern, Licensed Master Social Worker, Licensed Psychological Associate, Licensed Marriage and Family Therapist-Associate) may provide CBT in the event they are under the supervision of a fully licensed clinician that meets the criteria to be a Licensed Professional of the Healing Arts (LPHA) and meets the supervisor requirements as outlined in this policy. Please reference Texas Administrative Code (TAC) Code §412.303 to determine the disciplines that meet the criteria for LPHA.
2. Staff with non-independent licenses must be actively seeking full licensure as a LPHA. 3. Staff with non-independent licenses should refer to their respective Texas state licensing board
requirements regarding frequency of supervision. 4. Upon acquisition of full licensure staff will have 1 year to demonstrate competency per the
competency standards as set forth in this document. If the practitioner has not obtained competency within one year, see items A.3 and A.4 above.
D. Grandfathering Grandfathering is permitted if there is documentation of any one of the following:
1. Any practitioner that has been trained as a trainer by Dr. Monica Basco. Please note that practitioners that attended the CBT training workshops with Dr. Basco in the past do not meet this requirement. A practitioner must have been trained as a trainer in order to be grandfathered.
2. Any practitioner that has been certified by the Academy of Cognitive Therapy. 3. Any practitioner that has been certified as a trainer by the REACH Institute.
E. Supervisors The following requirement(s) must be met to provide supervision to clinicians providing CBT:
1. Supervisors must have attended or viewed the webinar ‘Demystifying the Tape Rating Process’ or viewed the training video ‘Cognitive Therapy Rating Scale (CTRS) Adherence Workshop’ and meet one of the following requirements: a) Supervisors must have attended the 3-day training in CBT by Dr. Basco or a Dr. Basco
trainer; or b) Supervisors must be trained by the Beck Institute, the REACH Institute, or certified by The
Academy of Cognitive Therapy in CBT. NOTE: Supervisors may substitute the above requirement(s) by passing the competency review or if they meet any of the grandfathering requirements. If a supervisor has attended the CBT training facilitated by the Beck Institute and hosted by the Centralized Training Infrastructure for Evidence-based Practices (CTI-EBP), has been trained by the REACH Institute, or has been certified by The Academy of Cognitive Therapy, then he or she has fulfilled the training requirement outlined in item E.1.b. of this policy. F. Additional Considerations
1. It is a best practice that practitioners get training and supervision in CBT while preparing for their tape review.
2. Training requirements are left up to the discretion of each individual center for clinicians that will be delivering CBT.
3. Trainers in adult CBT may serve as a resource in preparing providers for the competency review. 4. The Centralized Training Infrastructure for Evidence-based Practices (CTI-EBP) will serve as a
training resource for providers needing training in CBT.
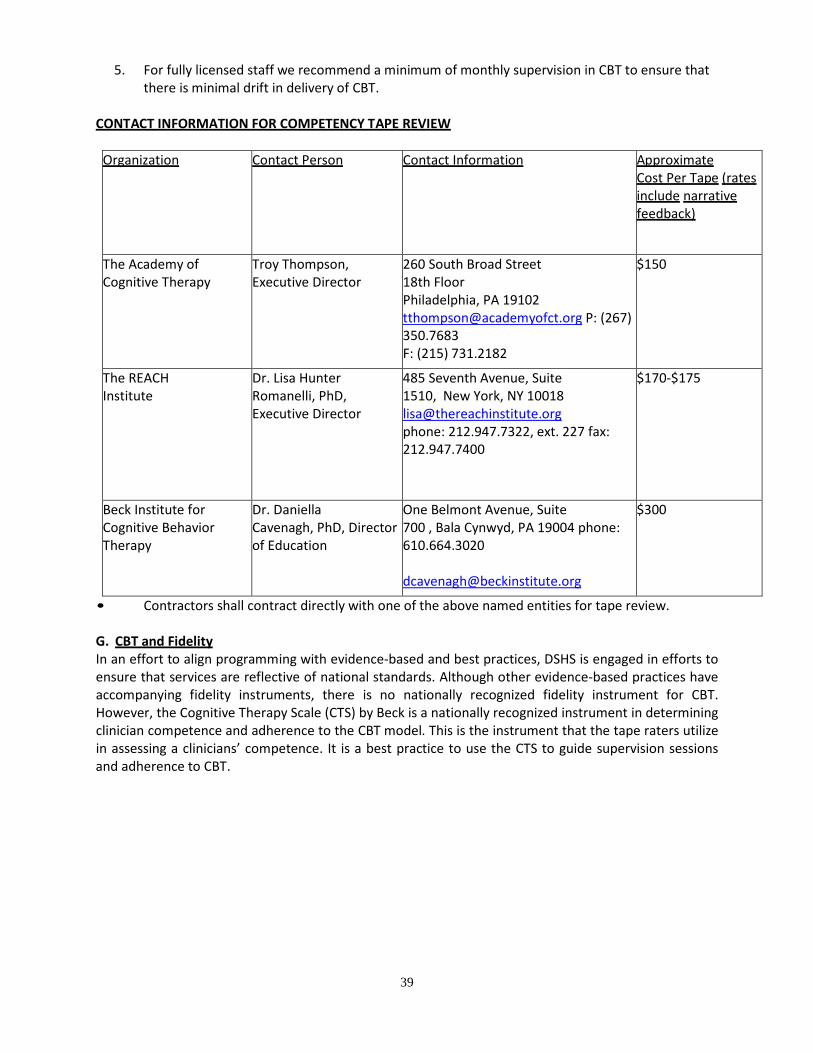
39
5. For fully licensed staff we recommend a minimum of monthly supervision in CBT to ensure that there is minimal drift in delivery of CBT.
CONTACT INFORMATION FOR COMPETENCY TAPE REVIEW
Organization Contact Person Contact Information Approximate Cost Per Tape (rates include narrative feedback)
The Academy of Cognitive Therapy
Troy Thompson, Executive Director
260 South Broad Street 18th Floor Philadelphia, PA 19102 [email protected] P: (267) 350.7683 F: (215) 731.2182
$150
The REACH Institute
Dr. Lisa Hunter Romanelli, PhD, Executive Director
485 Seventh Avenue, Suite 1510, New York, NY 10018 [email protected] phone: 212.947.7322, ext. 227 fax: 212.947.7400
$170-$175
Beck Institute for Cognitive Behavior Therapy
Dr. Daniella Cavenagh, PhD, Director of Education
One Belmont Avenue, Suite 700 , Bala Cynwyd, PA 19004 phone: 610.664.3020 [email protected]
$300
• Contractors shall contract directly with one of the above named entities for tape review. G. CBT and Fidelity In an effort to align programming with evidence-based and best practices, DSHS is engaged in efforts to ensure that services are reflective of national standards. Although other evidence-based practices have accompanying fidelity instruments, there is no nationally recognized fidelity instrument for CBT. However, the Cognitive Therapy Scale (CTS) by Beck is a nationally recognized instrument in determining clinician competence and adherence to the CBT model. This is the instrument that the tape raters utilize in assessing a clinicians’ competence. It is a best practice to use the CTS to guide supervision sessions and adherence to CBT.
40
H. Additional Resources DSHS Cognitive Therapy Resources Page http://www2.hhsc.state.tx.us/CentralOffice/BehavioralHealthServices/CTMain.html I. Adult Mental Health A. Cognitive Process Therapy (CPT) Training Requirements and Obtaining “Approved Provider” Status In order for practitioners to provide CPT they must complete the following multi-phase process:
1. Training Phase: Practitioners will complete the DSHS approved 2-Day classroom training on CPT or an equivalent training, such as Veteran’s Administration training on CPT.
2. Consultation Phase: Practitioners will participate in the consultation phase of the training process by attending the scheduled consultation calls with qualified trainers/consultants and concurrently conducting CPT with clients. To complete this phase, the clinician must document attendance of at least 19.5 hours of consultation calls during the consultation period within one year of the classroom training.
3. Counseling Phase: The counseling phase requires practitioners complete two 12- session cases of CPT during the consultation phase within one year of the training.
Following completion of the consultation phase and the required two cases, providers may apply to be added to the CPT registry in the DSHS Training Infrastructure. Once added to the CPT Registry, the clinician in now in approved status. Being added to the registry creates a permanent record of those practitioners approved to provide CPT in Texas. II. Child and Adolescent Mental Health Contractor shall meet and require Texas Resilience and Recovery (TRR) services subcontractors to meet the following training requirements for the DSHS- approved evidence-based practices prior to the provision of these services and supports. Completion of the requirements listed below shall be documented and maintained by Contractor or subcontractor. DSHS-approved evidence-based practices and training requirements are as follows: Training and Competency Standards: A. Skills Training and Development
1. Aggression Replacement Techniques utilizing the Aggression Replacement Training® curriculum: Aggression Replacement Techniques are required for the delivery of skills training and development in all CMH Levels of Care in which skills training and development services are available. Aggression Replacement Techniques shall be used as outlined in the TRR Utilization Management Guidelines. To deliver skills training and development services utilizing Aggression Replacement Techniques the following training requirements must be met:
a) Completion of at least a one-day live training hosted by any of the following: The Behavioral Institute for Children and Adolescents, G&G Consultants, Education and Treatment Alternatives, Inc., or an individual or entity designated as approved trainers by the aforementioned institutes; or
b) Documented completion of the “Aggression Replacement Training® DVD and the first five DVDs of the 6-DVD set workshop series “Teaching Prosocial Behavior to Antisocial Youth: A Live Workshop Presentation” by Dr. Arnold P. Goldstein,” as evidenced by signature of CMH Director (or designee) in the employee file, and
41
c) Completion of one of the following A.R.T.® curriculum fidelity observation forms within one year of completion of training: Anger Control Fidelity Form, Skillstreaming Fidelity Form, Moral Reasoning Fidelity Form.
2. Barkley’s Defiant Child and Barkley’s Defiant Teen: This protocol is currently required and shall be used as outlined in the TRR Utilization Management Guidelines. It is recommended for providers to complete a 6 hours training on this protocol by an approved trainer by Dr. Russell A. Barkley developer of this protocol.
3. Nurturing Parenting: Nurturing Parenting is a required protocol and shall be used as outlined in the TRR Utilization Management Guidelines. To deliver this protocol, completion of a 3-day training on Nurturing Parenting by a trainer who has been certified as an Organizational Trainer or National Trainer by Nurturing Parenting Programs® is required.
4. Seeking Safety: Seeking Safety is a required protocol and shall be used as outlined in the TRR Utilization Management Guidelines. To deliver this protocol, the following training requirements must be met:
a) Attendance at a 1-day live training on Seeking Safety by a trainer or training entity that has been designated as a trainer by Seeking Safety®; or
b) Documented completion of the 4 DVD set “Video Training Series on Seeking Safety” workshop as evidenced by signature of CMH Director (or designee) in the employee file; and
c) Completion of the fidelity form “Seeking Safety Adherence Scale” within one year of completion of training.
5. Preparing Adolescents for Young Adulthood (PAYA): PAYA is a required protocol and shall be used as outlined in the TRR Utilization Management Guidelines. There are no training requirements for this contracting period.
6. Wraparound Planning Process: Wraparound care planning process is required for Level of Care (LOC) 4 and the provision of Intensive Case Management (ICM). Facilitators must meet the following training requirements:
a) Ensure that Wraparound Process Planning is provided by an employee of the provider who is a QMHP-CS, CSSP, or LPHA. Providers must ensure that the employee has achieved Wraparound Facilitator training through a DSHS approved entity; and
b) Providers must ensure that Wraparound Facilitators have completed, or are in the process of completing, each of the core trainings listed below in the order in which they are listed. These trainings must be provided by a person/entity that has been certified as a training entity by the National Wraparound Initiative (NWI) standards:
i. Introduction to Wraparound ii. Engagement in the Wraparound Process
iii. Intermediate Wraparound: Improving Wraparound Practice c) At least once per month, Wraparound Facilitators must receive ongoing
Wraparound supervision from a Wraparound Supervisor who has completed the following training which must be provided by a person/entity that has been certified as a training entity by the National Wraparound Initiative (NWI):
i. Advancing Wraparound Practice—Supervision and Managing to Quality B. Counseling
1. Counseling services shall be provided by an LPHA, practicing within the scope of a license, or when appropriate and not in conflict with billing requirements, by an individual with a masters degree in human services field (e.g., psychology, socialwork, counseling) who is pursuing licensure under the direct supervision of an LPHA. The allowable models of counseling and practice requirements are:
42
a) Cognitive Behavioral Therapy (CBT): CBT is a required protocol. Providers of CBT must deliver the approved protocols as outlined in the TRR Utilization Management Guidelines and must meet the CBT Competency Policy outlined in Section I: Cognitive Behavioral Therapy Competency Policy of this Information Item;
b) Trauma-Focused Cognitive Behavioral Therapy (TF-CBT): TF-CBT is a required protocol. To deliver this protocol, the following training requirements must be satisfied:
i. Documentation of completed training from the DSHS TF-CBT Training (2009, 2010 Trainings) with Dr. Susana Rivera; or
ii. Completion of Basic Online Training on TF-CBTWeb© from the Medical University of South Carolina; and
iii. Completion of Online Training on Complex Traumatic Grief on TF- CBTWeb© from the Medical University of South Carolina; and
iv. Completion of at least 2 days of face-to-face TF-CBT training by a National Approved TF-CBT Trainer as designated by the Medical University of South Carolina or the developers of TF-CBT (Dr. Judith Cohen, Dr. Anthony Mannarino, or Dr. Esther Deblinger), and
v. Completion, or in process of completion, of 12 clinical consultation calls as required by the trainer. During the clinical consultation calls, the trainee must do at least one case presentation. Trainees are required to provide TF-CBT to at least one client during their clinical consultation period. A provider must have trainer approval of completion of all requirements or exceptions. A nationally approved trainer may require additional clinical consultations of a provider who does not demonstrate competency during the clinical consultation training period. Providers who complete the required two days of live- training after December 31, 2014 must complete the clinical consultation requirements within 12 months of the end of their live- training.
vi. Grandfathering consultation calls: Providers who completed TF-CBT training and clinical consultations prior to FY 13 (September 1, 2012) will be grandfathered if they completed the clinical consultation requirements that were the national standards during their training period.
2. Providers who completed TF-CBT training between FY 13 and FY 14 are required to complete a minimum of 9 of their 12 consultation calls, as was required nationwide during that period.
3. TF-CBT Providers who completed the live-training prior to December 31, 2014 but did not complete the required consultation calls or did not participate in clinical consultation calls after their live-training must complete the 12 clinical consultation call within 12 months after December 31, 2014.
i. Supervisors: Staff in a supervisory role who do not provide TF-CBT or counseling services are required to participate in the trainings and clinical consultation calls but are not required by DSHS to do a case presentation. However, staff in supervisory roles are not allowed to provide TF-CBT counseling services unless they have completed clinical consultation according to subsection III.B.2.v of this information Item. If a staff member in an administrative supervisory role with required credentials wants to provide TF-CBT, the staff member must complete an additional 12 clinical consultation calls inclusive of a case presentation and provide TF-CBT during the consultation period according to national standards.
43
ii. National Certification: DSHS does not require TFCBT National Therapist Certification. A national certification as a TF-CBT certified therapist, approved by the national developers of TF-CBT, surpasses and supersedes all DSHS training and competency requirements for TF-CBT. More information about national certification can be found at: https://tfcbt.org/
iii. Providing TF-CBT services: A provider is allowed to start providing TF- CBT once he or she has completed all the online and live-training requirements while they complete the clinical consultation requirements as stated in this Information Item.
c) Parent-Child Psychotherapy (Dyad Therapy): This is an allowable model of counseling that may be delivered to children 3-7 years of age. To deliver this protocol, Contractor shall document completed training in one of the following DSHS approved models of Parent-Child Psychotherapy:
i. Certificate for training from the DSHS/Early Childhood Mental Health ii. Training with Dr. Sarah Hinshaw-Fuselier (2006-2009 Trainings); or
iii. Certificate for training from the Early Childhood Mental Health Online iv. Training with Dr. Neil Boris and Dr. Hinshaw-Fuselier (2011); or v. Parent-Child Psychotherapy certification from a DSHS approved university
based institute, program; or vi. Certified in Parent-Child Interaction Therapy (PCIT) by a PCIT International
Certified Trainer or training entity that follows the current PCIT training guidelines as outlined by PCIT International® or by the developer of PCIT (Dr. Sheila Eyberg from the University of Florida).
C. Supervision
1. Supervisors of services and supports within TRR must be trained as trainers in the DSHS-approved evidence-based practices, be trained in evidence-based practices, or have provided the evidence–based practices prior to the supervision of the evidence- based practices. Supervisors must complete this requirement within 180 days of assuming a supervisory position. If supervisors are unable to complete this requirement within 180 days of assuming the supervisory position, the LMHA must submit a plan to the department outlining how the supervisor will fulfill this requirement.
III. Assessment Training Requirements A. Child and Adolescent Needs and Strengths (CANS) Assessment / Adult Needs and Strengths
Assessments (ANSA) 1. Providers must complete the CANS or ANSA online training or live-training and pass the
training with a score of .70 or above in order to administer and score the CANS and ANSA. 2. Providers must maintain annual certification of CANS or ANSA from the Praed Foundation
documented in their personnel file at their Local Mental Health Authority. B. CANS/ANSA Super User
1. Complete CANS/ANSA online with a score of .80 or above, and a) Attend a live training for CANS/ANSA Super User b) Bring to live training a scored written case vignette; c) Bring to live training a presentation to about why the CANS or ANSA is important to
their organization. 2. A Super User has to maintain annual Super User certification documented in their personnel
file at their Local Mental Health Authority.

44
3. A Super User is not required to complete both trainings for CANS or ANSA. The completion for all the training requirements for either CANS or ANSA Super User Training will suffice for the staff to have a Super User role at the LMHA.
Exhibit E
FY 2016 Information Item C Page Info. C - 1
I. Adult Services .................................................................................... 2 A. Adult Service Target ........................................................................................ 2 B. Adult Uniform Assessment (UA) Completion Rate ....................................... 2 C. Adult Counseling Target ................................................................................. 3 D. ACT Target ....................................................................................................... 3 E. Resilience and Recovery Outcomes - Adult Mental Health Measures ........ 3 F. Resilience and Recovery Outcomes - Crisis Measures Applicable to Adult
and Children’s Mental Health .......................................................................... 7 G. TANF Transfer to Title XX Services: ............................................................. 10
II. Child and Youth Services ................................................................ 11 A. Child and Youth Service Target .................................................................... 11 B. Child and Youth Uniform Assessment (UA) Completion Rate ................... 12 C. Family Partner Support Services ................................................................. 12 D. Resilience and Recovery Outcomes – Children’s Mental Health Measures
......................................................................................................................... 13 G. TANF Transfer to Title XX Services: ............................................................. 17
III. Performance Measures Assessed Within CARE ........................... 18 A. Community Support Plan .............................................................................. 18 B. Follow-Up Within Seven Days ...................................................................... 19 C. Long-Term Services and Support Screen ................................................... 20
IV. Crisis Response System Outcomes ............................................... 20 A. Community Linkage ....................................................................................... 21 B. Crisis Follow-Up............................................................................................. 21
V. Uniform Assessment Instructions .................................................. 21 A. Adult Uniform Assessment ........................................................................... 21 B. Child & Adolescent Uniform Assessment Instructions .............................. 23
VII. Glossary of Terms ........................................................................... 25
Information Item C
FY 2016 Information Item C Page Info. C - 2
I. Adult Services Measured Semi Annually A. Adult Service Target
Explanation: The statewide performance level for the adult service target is 100%.
Calculation: (Numerator/Denominator)*100 a. Numerator: The total number of Client Months in which a client was
authorized in a FLOC. b. Denominator: The target assigned to the contractor times six months.
Exclusion(s)/Exception(s): N/A
Sanctions and Remedies: Will be based on Contractor’s current six month adult MH allocation. NOTE: LMHAs may contact their assigned contract manager to notify DSHS of any potential impact on the LMHA’s ability to meet contractual requirements resulting from a significant change in local funding.
Data Source: Clinical Management for Behavioral Health Services (CMBHS) system and Mental Retardation and Behavioral Health Outpatient Warehouse (MBOW).
B. Adult Uniform Assessment (UA) Completion Rate
Explanation: The percentage of adults served or authorized for services during the six month period with a completed and current Uniform Assessment (UA) shall be ≥ 95%.
Calculation: (Numerator/Denominator)*100. a. Numerator: Total number of adults registered in CARE with a completed
UA. b. Denominator: Unduplicated number of adults with a completed UA or a
service encounter. Exclusion(s)/Exception(s):
a. The following are not included in the calculation of this measure: i. Delivery of a Screening Service or Assessment Service encounter
without a completed UA. ii. 100% of service hours by Third Party Payer as noted by field #12,
FIRST_BILLED_PAYER_CD on all encounter records for the month. iii. Individuals without a registration in CARE.
Sanctions and Remedies: Will be based on the contractor’s current six month adult MH allocation.
Data Source: CMBHS system. MBOW report found in the CA Contract Performance Measures folder.
Information Item C
FY 2016 Information Item C Page Info. C - 3
C. Adult Counseling Target Explanation: The monthly average of all adults authorized into LOC-2 is
greater than or equal to 12% of adults recommended for LOC-2. Calculation: (Numerator/Denominator)*100
a. Numerator: The number of adults recommended and authorized into LOC-2 during the fiscal year.
b. Denominator: The number of adults recommended for LOC-2 during the fiscal year.
Exclusion(s)/Exception(s): N/A Sanctions and Remedies: Will be based on the terms included in the PCN
Scope of Work or Article VII. of the Local Mental Health Authority Special Conditions.
D. ACT Target
Explanation: The monthly average of all adults recommended for LOC 4 and authorized into LOC-3 or LOC-4 is greater than or equal to 54.0%.
Calculation: (Numerator/Denominator)*100 a. Numerator: The number of adults recommended for LOC-4 and authorized
into LOC-3 or LOC-4 during the fiscal year. b. Denominator: The number of adults recommended for LOC-4 during the
fiscal year. Exclusion(s)/Exception(s): N/A Sanctions and Remedies: Will be based on the terms included in the PCN
Scope of Work or Article VII. of the Local Mental Health Authority Special Conditions.
E. Resilience and Recovery Outcomes - Adult Mental Health Measures
Measured Semi Annually
Employment a. Target: The percentage of adults served with an Adult Uniform
Assessment Community Data Section 4. B. Paid Employment Type score of 1 (Independent/Competitive/Supported/Self Employment) shall be ≥9.8% per measurement period.
b. Calculation: (Numerator/Denominator)*100 i. Numerator—The number of adults recommended and authorized for
a FLOC with an Adult Uniform Assessment Community Data Section 4. B. Paid Employment Type score of 1.
ii. Denominator—All adults recommended and authorized for a FLOC. c. Exclusion(s)/Exception(s): Intake Assessments. d. Sanctions and Remedies: Rider 78, Mental Health Outcomes and
Accountability, requires 10% withhold of funds in strategies B.2.1, B.2.2 and B.2.3 with payment contingent upon achievement of outcome performance. Performance assessed and payments made on a six-month
Information Item C
FY 2016 Information Item C Page Info. C - 4
interval. e. Data Source: CARE, CMBHS and MBOW
Adult Community Tenure a. Target: The percentage of adults in a FLOC that avoid hospitalization in a
DSHS Operated or Contracted Inpatient Bed after authorization into a FLOC shall be > 96.4% per measurement period.
b. Calculation: (Numerator/Denominator)*100 i. Numerator—All adults authorized in a FLOC during the measurement
period who avoid hospitalization in a DSHS Operated or Contracted Inpatient Bed after authorization into a FLOC.
ii. Denominator—All adults authorized in a FLOC during the measurement period.
c. Exclusion(s)/Exception(s): Crisis Stabilization Units (CSU) - including Hill Country, Extended Observation Units (EOU), Crisis Respite, Crisis Residential and Rusk and Vernon forensic locations. Measurement period is six months.
d. Sanctions and Remedies: Rider 78, Mental Health Outcomes and Accountability, requires 10% withhold of funds in strategies B.2.1, B.2.2 and B.2.3 with payment contingent upon achievement of outcome performance. Performance assessed and payments made on a six-month interval.
e. Data Source: CARE, CMBHS and MBOW.
Adult Improvement a. Target: 20.0% or more of all adults authorized into a FLOC shall show
reliable improvement in at least one of the following ANSA domains/modules: Risk Behaviors, Behavioral Health Needs, Life Domain Functioning, Strengths, Substance Use, Adjustment to Trauma. Reliable Improvement is defined as a calculated value of the Reliable Change Index (RCI) that exceeds a benchmark value of -1.645 in the negative direction (indicating fewer problematic symptoms) over the measurement period.
b. Calculation: (Numerator/Denominator)*100 i. Numerator: Number of adults enrolled in a FLOC meeting or exceeding
the RCI in one of the identified ANSA domains/modules whose first and last Uniform Assessments are at least 90 days apart.
ii. Denominator: All adults enrolled in a FLOC whose first and last Uniform Assessments, including ANSA domains/modules, are at least 90 days apart.
d. Exclusion(s)/Exception(s): e. Sanctions and Remedies: Rider 78, Mental Health Outcomes and
Accountability, requires 10% withhold of funds in strategies B.2.1, B.2.2
Information Item C
FY 2016 Information Item C Page Info. C - 5
and B.2.3.with payment contingent upon achievement of outcome performance. Performance assessed and payments made on a six-month interval.
f. Data Source: CMBHS and MBOW. 5. Adult Monthly Service Provision
a. Target: The percentage of adults authorized in a FLOC receiving at least one face to face, telehealth, or telemedicine encounter of any service per month of any length of time shall be ≥ 65.6% per measurement period. FLOCs included in this measure are LOC-1S, LOC-2, LOC-3, and LOC-4. Individuals both recommended and authorized for LOC-A1S are excluded from this measure. Encounters must be delivered face-to-face or via telehealth or telemedicine.
b. Calculation: (Numerator/Denominator)*100 i. Numerator: Total number of persons authorized in a FLOC
receiving at least one face to face, telehealth, or telemedicine encounter of any service per month of any length of time.
ii. Denominator: Total number of persons authorized in a FLOC that month.
iii. On a semi-annual basis, the percentage for each of the six months within that time period will be averaged to calculate whether the measure is met.
c. Exclusion(s)/Exception(s): i. Individuals enrolled in LOC-1M; ii. Individuals with both LOC-R=A1S and LOC-A=A1S; iii. Non face-to-face, GJ modifiers, and telephone contact encounters;
and iv. Partially Authorized Months and their associated hours
d. Sanctions and Remedies: Rider 78, Mental Health Outcomes and Accountability, requires 10% withhold of funds in strategies B.2.1, B.2.2 and B.2.3 with payment contingent upon achievement of outcome performance. Performance assessed and payments made on a six-month interval.
e. Data Source: CARE, CMBHS, and MBOW. FY16 will serve as a benchmarking year for the following Resilience and Recovery Outcomes.. There will be no sanctions assessed for these outcomes during the FY16 benchmarking year:
6. Employment
a. Target: The percentage of adults authorized in a FLOC with acceptable or improved employment performance.
b. Calculation: (Numerator/Denominator)*100 i. Numerator: # of adults authorized in a FLOC who meet or exceed
the RCI benchmark in the direction of improvement for the ANSA Employment item (i.e., ≤ -1.645, indicating fewer problematic symptoms) or who have ANSA Employment item scores of 0, 1 at
Information Item C
FY 2016 Information Item C Page Info. C - 6
both First and Last Active UAs within the fiscal year. First and Last Active UAs must be at least 90 days apart and must include ANSA Employment item scores at both assessments.
ii. Denominator: # of adults authorized in a FLOC with First and Last Active UAs within the fiscal year occurring at least 90 days apart, with ANSA Employment item scores at both assessments.
c. Exclusion(s)/Exception(s): d. Sanctions and Remedies: N/A e. Data Source: CMBHS and MBOW
7. Residential Stability
a. Target: The percentage of adults authorized in a FLOC with acceptable or improved residential stability.
b. Calculation: (Numerator/Denominator)*100 i. Numerator: # of adults authorized in a FLOC who meet or exceed
the RCI benchmark in the direction of improvement for the ANSA Residential Stability item (i.e., ≤-1.645, indicating fewer problematic symptoms) or who have ANSA Residential Stability item scores of 0,1 at both First and Last Active UAs within the fiscal year. First and Last Active UAs must be at least 90 days apart.
ii. Denominator: # of adults authorized in a FLOC with First and Last Active UAs within the fiscal year occurring at least 90 days apart.
c. Exclusion(s)/Exception(s): d. Sanctions and Remedies: N/A e. Data Source: CMBHS and MBOW
8. Strengths
a. Target: The percentage of adults authorized in a FLOC with acceptable or improved strengths.
b. Calculation: (Numerator/Denominator)*100 i. Numerator: # of adults authorized in a FLOC who meet or exceed
the RCI benchmark in the direction of improvement for the ANSA Strengths domain (i.e., ≤-1.645, indicating fewer problematic symptoms) or who have ANSA item scores of 0,1 for all Strengths domain items at both First and Last Active UAs within the fiscal year. First and Last Active UAs must be at least 90 days apart.
ii. Denominator: # of adults authorized in a FLOC with First and Last Active UAs within the fiscal year occurring at least 90 days apart.
c. Exclusion(s)/Exception(s): d. Sanctions and Remedies: N/A e. Data Source: CMBHS and MBOW
9. Life Domain Functioning
a. Target: The percentage of adults authorized in a FLOC with acceptable or improved life functioning.
b. Calculation: (Numerator/Denominator)*100 i. Numerator: # of adults authorized in a FLOC who meet or exceed
Information Item C
FY 2016 Information Item C Page Info. C - 7
the RCI benchmark in the direction of improvement for the ANSA Life Domain Functioning domain (i.e., ≤-1.645, indicating fewer problematic symptoms) or who have ANSA item scores of 0,1 for all Life Domain Functioning domain items at both First and Last Active UAs within the fiscal year. First and Last Active UAs must be at least 90 days apart.
ii. Denominator: # of adults authorized in a FLOC with First and Last Active UAs within the fiscal year occurring at least 90 days apart.
c. Exclusion(s)/Exception(s): d. Sanctions and Remedies: N/A e. Data Source: CMBHS and MBOW
10. Educational or Volunteering Strengths
a. Target: The percentage of adults authorized in a FLOC with acceptable or improved employment-preparatory skills as evidenced by Educational or Volunteering Strengths.
b. Calculation: (Numerator/Denominator)*100 i. Numerator: # of adults authorized in a FLOC who meet or exceed
the RCI benchmark in the direction of improvement for either the ANSA Educational or the Volunteering Strengths item (i.e., ≤-1.645, indicating fewer problematic symptoms), or who have ANSA item scores of 0,1 for either the Educational or the Volunteering Strengths item at both First and Last Active UAs within the fiscal year. First and Last Active UAs must be at least 90 days apart.
ii. Denominator: # of adults authorized in a FLOC with First and Last Active UAs within the fiscal year occurring at least 90 days apart.
c. Exclusion(s)/Exception(s): d. Sanctions and Remedies: N/A e. Data Source: CMBHS and MBOW
F. Resilience and Recovery Outcomes - Crisis Measures Applicable to Adult
and Children’s Mental Health 1. Hospitalization
a. Target: The equity-adjusted rate of adult and child inpatient DSHS Operated or Contracted psychiatric Inpatient Beds for the population of the local service area shall be ≤ 1.9% per measurement period.
b. Calculation: (Numerator/Denominator)*100 i. Numerator: The number of DSHS Operated or Contracted Inpatient
Bed Days for the population in the local service area multiplied by the LMHA’s equity factor.
ii. Denominator: Total population of the local service area. iii. Equity factor: The LMHA’s per capita funding rate (excluding funding
for hospital beds and Hospitality House) divided by the per capita funding rate of the LMHA with the highest per capita funding rate.
c. Exclusion(s)/Exception(s): Crisis Stabilization Units (CSU) - including Hill Country, Extended Observation Units (EOU), Crisis Respite, Crisis Residential and Rusk and Vernon forensic locations.
Information Item C
FY 2016 Information Item C Page Info. C - 8
i. Children in LOC-Y (YES Waiver). d. Sanctions and Remedies: Rider 78, Mental Health Outcomes and
Accountability, requires 10% withhold of funds in strategies B.2.1, B.2.2 and B.2.3 with payment contingent upon achievement of outcome performance. Performance assessed and payments made on a six-month interval.
e. Data Source: CARE, CMBHS and MBOW f. Example: Local
Service Area
Population
Reported Inpatient
Bed Days
Per Capita
Funding
Per Capita
Funding of
highest ranking LMHA
Calculation Equity-adjusted
Performance
500,000 10,000 $20.00 $30.00 �(10,000) ∗ �20.0030.00��
500,000 .013 or 1.3%
Effective Crisis Response a. Target: The percentage of individuals receiving crisis services who avoid
admission to a DSHS Operated or Contracted Inpatient Bed within 30 days of the start of the crisis episode shall be > 75.1% per measurement period.
b. Calculation: (Numerator/Denominator)*100 i. Numerator: The number of persons with crisis episodes that avoid
admission into DSHS Operated or Contracted Inpatient Beds within 30 days of the first day of the crisis episode.
ii. Denominator: The number of crisis episodes c. Exclusion(s)/Exception(s):
i. Crisis Stabilization Units (CSU) - including Hill Country, Extended Observation Units (EOU), Crisis Respite, Crisis Residential and Rusk and Vernon forensic locations.
ii. Children in a LOC-Y (YES Waiver). d. Sanctions and Remedies: Rider 78, Mental Health Outcomes and
Accountability, requires 10% withhold of funds in strategies B.2.1, B.2.2 and B.2.3 with payment contingent upon achievement of outcome performance. Performance assessed and payments made on a six-month interval.
e. Data Source: CARE, CMBHS and MBOW.
Frequent Admissions a. Target: The percentage of adults and children authorized in a FLOC who
are admitted 3 or more times within 180 days to a DSHS Operated or
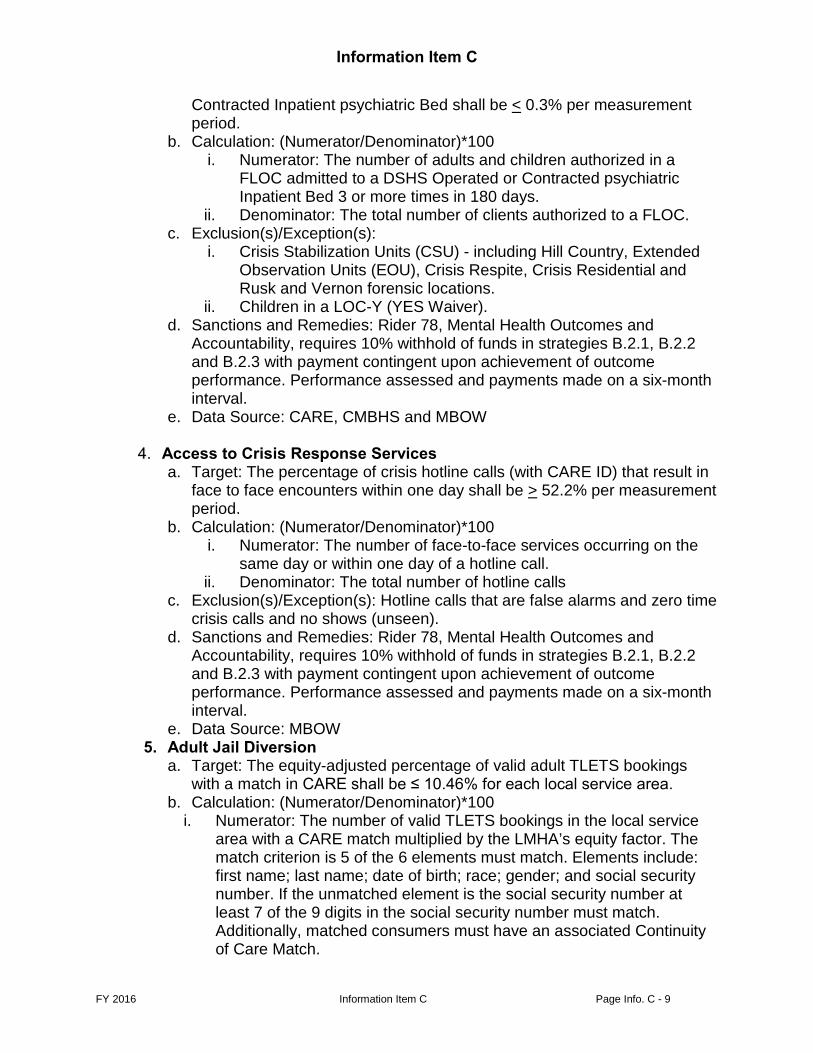
Information Item C
FY 2016 Information Item C Page Info. C - 9
Contracted Inpatient psychiatric Bed shall be < 0.3% per measurement period.
b. Calculation: (Numerator/Denominator)*100 i. Numerator: The number of adults and children authorized in a
FLOC admitted to a DSHS Operated or Contracted psychiatric Inpatient Bed 3 or more times in 180 days.
ii. Denominator: The total number of clients authorized to a FLOC. c. Exclusion(s)/Exception(s):
i. Crisis Stabilization Units (CSU) - including Hill Country, Extended Observation Units (EOU), Crisis Respite, Crisis Residential and Rusk and Vernon forensic locations.
ii. Children in a LOC-Y (YES Waiver). d. Sanctions and Remedies: Rider 78, Mental Health Outcomes and
Accountability, requires 10% withhold of funds in strategies B.2.1, B.2.2 and B.2.3 with payment contingent upon achievement of outcome performance. Performance assessed and payments made on a six-month interval.
e. Data Source: CARE, CMBHS and MBOW
Access to Crisis Response Services a. Target: The percentage of crisis hotline calls (with CARE ID) that result in
face to face encounters within one day shall be > 52.2% per measurement period.
b. Calculation: (Numerator/Denominator)*100 i. Numerator: The number of face-to-face services occurring on the
same day or within one day of a hotline call. ii. Denominator: The total number of hotline calls
c. Exclusion(s)/Exception(s): Hotline calls that are false alarms and zero time crisis calls and no shows (unseen).
d. Sanctions and Remedies: Rider 78, Mental Health Outcomes and Accountability, requires 10% withhold of funds in strategies B.2.1, B.2.2 and B.2.3 with payment contingent upon achievement of outcome performance. Performance assessed and payments made on a six-month interval.
e. Data Source: MBOW 5. Adult Jail Diversion
a. Target: The equity-adjusted percentage of valid adult TLETS bookings with a match in CARE shall be ≤ 10.46% for each local service area.
b. Calculation: (Numerator/Denominator)*100 i. Numerator: The number of valid TLETS bookings in the local service
area with a CARE match multiplied by the LMHA’s equity factor. The match criterion is 5 of the 6 elements must match. Elements include: first name; last name; date of birth; race; gender; and social security number. If the unmatched element is the social security number at least 7 of the 9 digits in the social security number must match. Additionally, matched consumers must have an associated Continuity of Care Match.
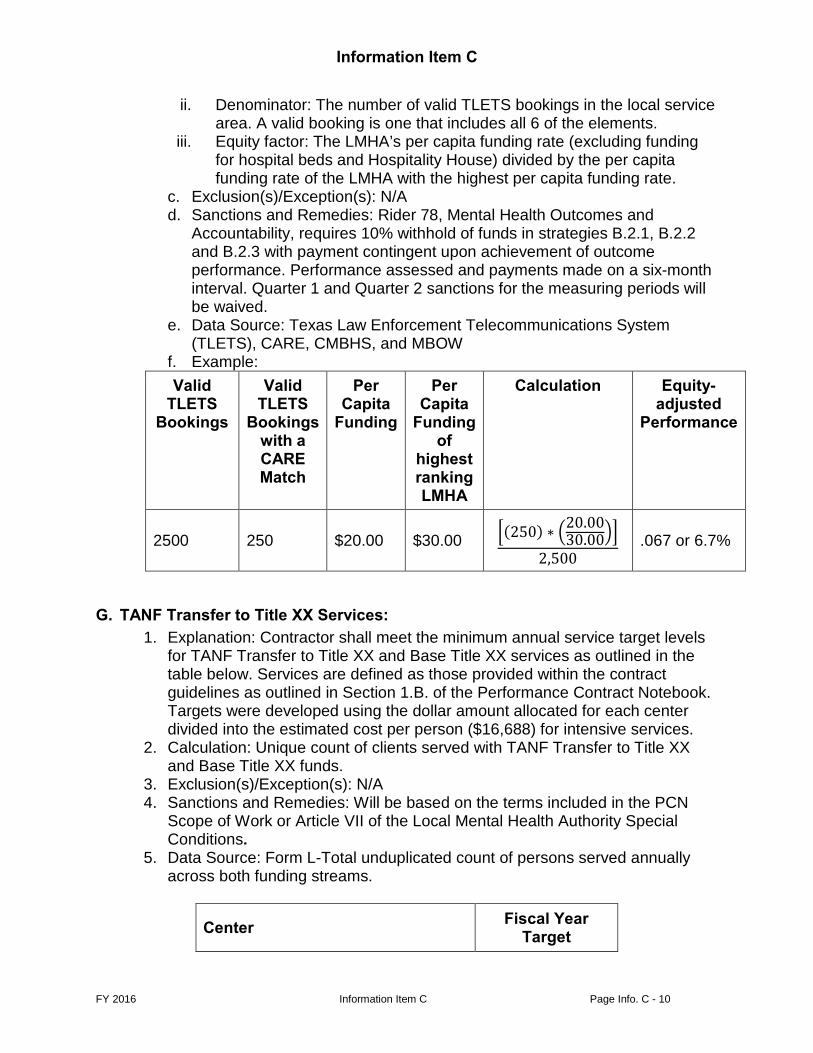
Information Item C
FY 2016 Information Item C Page Info. C - 10
ii. Denominator: The number of valid TLETS bookings in the local service area. A valid booking is one that includes all 6 of the elements.
iii. Equity factor: The LMHA’s per capita funding rate (excluding funding for hospital beds and Hospitality House) divided by the per capita funding rate of the LMHA with the highest per capita funding rate.
c. Exclusion(s)/Exception(s): N/A d. Sanctions and Remedies: Rider 78, Mental Health Outcomes and
Accountability, requires 10% withhold of funds in strategies B.2.1, B.2.2 and B.2.3 with payment contingent upon achievement of outcome performance. Performance assessed and payments made on a six-month interval. Quarter 1 and Quarter 2 sanctions for the measuring periods will be waived.
e. Data Source: Texas Law Enforcement Telecommunications System (TLETS), CARE, CMBHS, and MBOW
f. Example: Valid
TLETS Bookings
Valid TLETS
Bookings with a CARE Match
Per Capita
Funding
Per Capita
Funding of
highest ranking LMHA
Calculation Equity-adjusted
Performance
2500 250 $20.00 $30.00 �(250) ∗ �20.0030.00��
2,500 .067 or 6.7%
G. TANF Transfer to Title XX Services: 1. Explanation: Contractor shall meet the minimum annual service target levels
for TANF Transfer to Title XX and Base Title XX services as outlined in the table below. Services are defined as those provided within the contract guidelines as outlined in Section 1.B. of the Performance Contract Notebook. Targets were developed using the dollar amount allocated for each center divided into the estimated cost per person ($16,688) for intensive services.
2. Calculation: Unique count of clients served with TANF Transfer to Title XX and Base Title XX funds.
3. Exclusion(s)/Exception(s): N/A 4. Sanctions and Remedies: Will be based on the terms included in the PCN
Scope of Work or Article VII of the Local Mental Health Authority Special Conditions.
5. Data Source: Form L-Total unduplicated count of persons served annually across both funding streams.
Center Fiscal Year Target
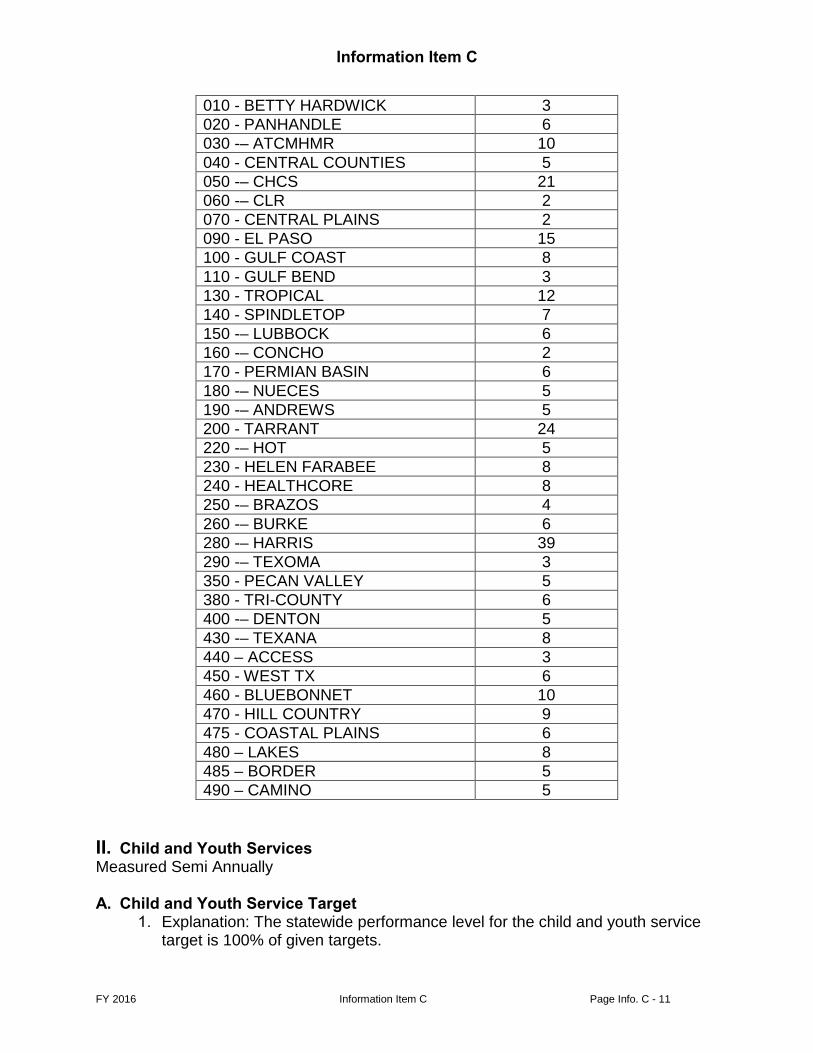
Information Item C
FY 2016 Information Item C Page Info. C - 11
010 - BETTY HARDWICK 3 020 - PANHANDLE 6 030 -– ATCMHMR 10 040 - CENTRAL COUNTIES 5 050 -– CHCS 21 060 -– CLR 2 070 - CENTRAL PLAINS 2 090 - EL PASO 15 100 - GULF COAST 8 110 - GULF BEND 3 130 - TROPICAL 12 140 - SPINDLETOP 7 150 -– LUBBOCK 6 160 -– CONCHO 2 170 - PERMIAN BASIN 6 180 -– NUECES 5 190 -– ANDREWS 5 200 - TARRANT 24 220 -– HOT 5 230 - HELEN FARABEE 8 240 - HEALTHCORE 8 250 -– BRAZOS 4 260 -– BURKE 6 280 -– HARRIS 39 290 -– TEXOMA 3 350 - PECAN VALLEY 5 380 - TRI-COUNTY 6 400 -– DENTON 5 430 -– TEXANA 8 440 – ACCESS 3 450 - WEST TX 6 460 - BLUEBONNET 10 470 - HILL COUNTRY 9 475 - COASTAL PLAINS 6 480 – LAKES 8 485 – BORDER 5 490 – CAMINO 5
II. Child and Youth Services Measured Semi Annually
A. Child and Youth Service Target
Explanation: The statewide performance level for the child and youth service target is 100% of given targets.
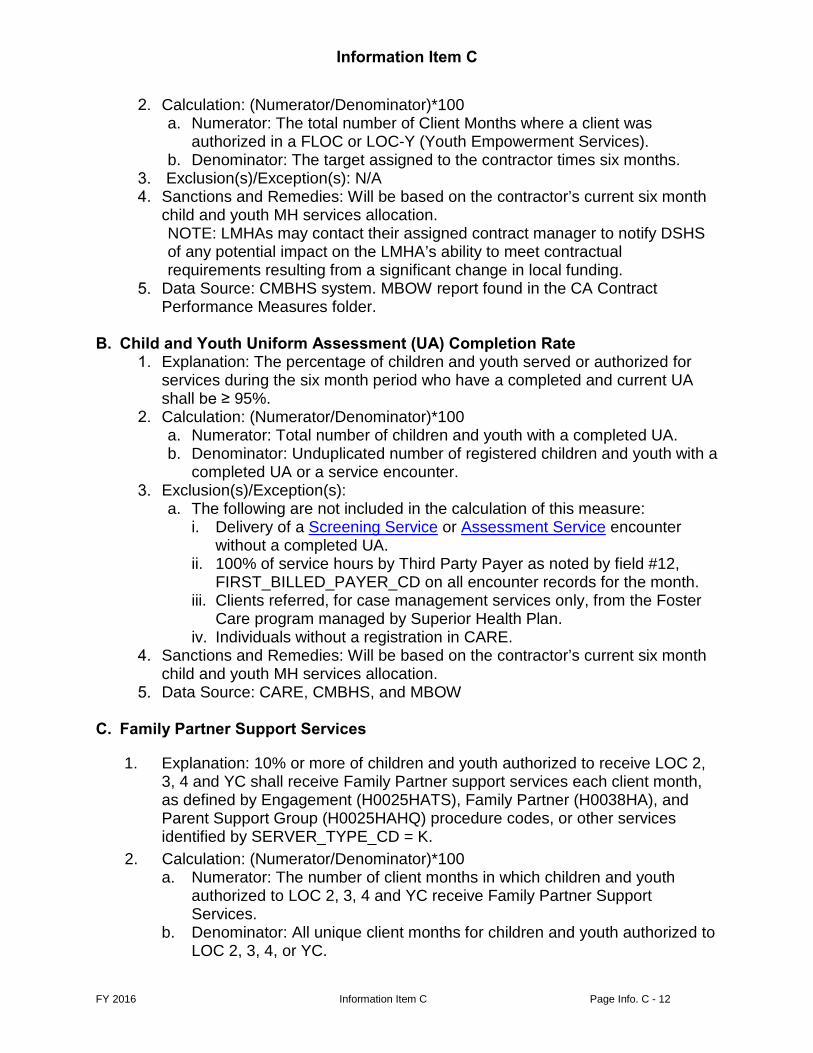
Information Item C
FY 2016 Information Item C Page Info. C - 12
Calculation: (Numerator/Denominator)*100 a. Numerator: The total number of Client Months where a client was
authorized in a FLOC or LOC-Y (Youth Empowerment Services). b. Denominator: The target assigned to the contractor times six months.
Exclusion(s)/Exception(s): N/A Sanctions and Remedies: Will be based on the contractor’s current six month
child and youth MH services allocation. NOTE: LMHAs may contact their assigned contract manager to notify DSHS of any potential impact on the LMHA’s ability to meet contractual requirements resulting from a significant change in local funding.
Data Source: CMBHS system. MBOW report found in the CA Contract Performance Measures folder.
B. Child and Youth Uniform Assessment (UA) Completion Rate
Explanation: The percentage of children and youth served or authorized for services during the six month period who have a completed and current UA shall be ≥ 95%.
Calculation: (Numerator/Denominator)*100 a. Numerator: Total number of children and youth with a completed UA. b. Denominator: Unduplicated number of registered children and youth with a
completed UA or a service encounter. Exclusion(s)/Exception(s):
a. The following are not included in the calculation of this measure: i. Delivery of a Screening Service or Assessment Service encounter
without a completed UA. ii. 100% of service hours by Third Party Payer as noted by field #12,
FIRST_BILLED_PAYER_CD on all encounter records for the month. iii. Clients referred, for case management services only, from the Foster
Care program managed by Superior Health Plan. iv. Individuals without a registration in CARE.
Sanctions and Remedies: Will be based on the contractor’s current six month child and youth MH services allocation.
Data Source: CARE, CMBHS, and MBOW C. Family Partner Support Services
1. Explanation: 10% or more of children and youth authorized to receive LOC 2, 3, 4 and YC shall receive Family Partner support services each client month, as defined by Engagement (H0025HATS), Family Partner (H0038HA), and Parent Support Group (H0025HAHQ) procedure codes, or other services identified by SERVER_TYPE_CD = K.
2. Calculation: (Numerator/Denominator)*100 a. Numerator: The number of client months in which children and youth
authorized to LOC 2, 3, 4 and YC receive Family Partner Support Services.
b. Denominator: All unique client months for children and youth authorized to LOC 2, 3, 4, or YC.
Information Item C
FY 2016 Information Item C Page Info. C - 13
3. Exclusion(s)/Exception(s): Only children and youth authorized to LOC 2, 3, 4 and YC are included in the calculation of this measure. The following are not included in the calculation of this measure: a. Partially Authorized Months; and b. Children and youth referred, for case management services only, from the
Foster Care program managed by Superior Health Plan. c. Children in LOC-Y (Yes Waiver).
4. Sanctions and Remedies: Will be based on Contractor’s current six month child and youth MH services allocation.
5. Data Source: CMBHS system and MBOW. MBOW report found in the CA Contract Performance Measures folder.
D. Resilience and Recovery Outcomes – Children’s Mental Health Measures 1. Juvenile Justice Avoidance
a. Explanation: 95.0% of children/youth enrolled in a FLOC showing no arrests (acceptable) or a reduction of arrests (improving) from time of first assessment to time of last assessment within the measurement period (with assessments occurring at least 75 days apart).
b. Calculation: (Numerator/Denominator)*100 i. Acceptable Juvenile Justice Involvement Avoidance
(1) Numerator: The number of children and youth recommended and authorized for a FLOC, whose latest number of arrests is 0 and whose previous number of arrests is 0.
(2) Denominator: All children and youth recommended and authorized for a FLOC who have at least two number of arrests ratings.
ii. Improving Juvenile Justice Involvement Avoidance (1) Numerator: The number of children and youth recommended and
authorized for a FLOC, whose latest number of arrests rating is less than their previous number of arrests rating.
(2) Denominator: All children and youth recommended and authorized for a FLOC who have at least two number of arrests ratings.
c. Exclusion(s)/Exception(s): Children in LOC-Y (Yes Waiver). d. Sanctions and Remedies: Will be based on Contractor’s current six month
child and youth MH services allocation. e. Data Source: This measure utilizes the Arrests Item from the community
data section of the Uniform Assessment.
Child and Youth Community Tenure a. Explanation: The percentage of children and youth in a FLOC avoiding
psychiatric hospitalization in a DSHS Purchased Inpatient Bed after authorization into a FLOC shall be > 98.1%.
b. Calculation: The percentage of children/youth authorized in a FLOC who avoid hospitalization in a DSHS Purchased Inpatient Bed Day after authorization into a FLOC. i. Numerator- The number of children and youth authorized in a FLOC
Information Item C
FY 2016 Information Item C Page Info. C - 14
who avoided hospitalization in a DSHS Purchased Inpatient Bed after authorization into a FLOC.
ii. Denominator- All children and youth authorized in a FLOC during the measurement period.
c. Exclusion(s)/Exceptions(s): Children in LOC-Y (Yes Waiver) d. Sanctions and Remedies: Rider 78, Mental Health Outcomes and
Accountability, requires 10% withhold of funds in strategies B.2.1, B.2.2 and B.2.3 with payment contingent upon achievement of outcome performance. Performance assessed and payments made on a six-month interval.
e. Data Source: CMBHS and MBOW
Child and Youth Improvement a. Explanation: 25.0% or more of all children/adolescents authorized into a
FLOC will show reliable improvement in at least one of the following CANS domains/modules: Child Strengths, Behavioral and Emotional Needs, Life Domain Functioning, Child Risk Behaviors, Adjustment to Trauma, School Performance, Substance Use. Reliable Improvement is defined as a calculated value of the Reliable Change Index (RCI) that exceeds a benchmark value of -1.645 in the negative direction (indicating fewer problematic symptoms) over the measurement period.
b. Calculation i. Numerator: Number of children/youth enrolled in a FLOC meeting or
exceeding the RCI in one of the identified CANS domains/modules whose first and last Uniform Assessments are at least 75 days apart. .
ii. Denominator: All children/youth enrolled in a FLOC whose first and last Uniform Assessments, including CANS domains/modules, are at least 75 days apart.
c. Exclusion(s)/Exception(s): d. Children in LOC-Y (Yes Waiver).Sanctions and Remedies: Rider 78,
Mental Health Outcomes and Accountability, requires 10% withhold of funds in strategies B.2.1, B.2.2 and B.2.3 with payment contingent upon achievement of outcome performance. Performance assessed and payments made on a six-month interval.
e. Data Source: CMBHS and MBOW
Child and Youth Monthly Service Provision a. Target: The percentage of children and youth authorized in a FLOC or
LOC-Y (Yes Waiver) receiving at least one face to face, telehealth or telemedicine encounter of any service per month of any length of shall be > 65 % the target for the measurement period. LOCs included in this measure are LOC-1, LOC-2, LOC-3, LOC-4, LOC-YC and LOC-Y. An encounter must be delivered face-to-face or via telehealth or telemedicine.
b. Calculation: The average monthly percentage of children and youth receiving at least one face to face, telehealth or telemedicine encounter of any service per month of any length of time.
Information Item C
FY 2016 Information Item C Page Info. C - 15
i. Numerator – Total number of children and youth authorized in a FLOC or LOC-Y (Yes Waiver) receiving at least one face to face, telehealth or telemedicine encounter of any service per month of any length of time.
ii. Denominator – Total number of children and youth authorized in a FLOC or LOC-Y that month.
iii. On a six month basis, the six months will be averaged to calculate whether the measure is.
c. Exclusion(s)/Exception(s): i. Children and youth on extended review; ii. Non face-to-face, GJ modifiers, and telephone contact encounters; and iii. Partially Authorized Months and their associated hours.
d. Sanctions and Remedies: Rider 78, Mental Health Outcomes and Accountability, requires 10% withhold of funds in strategies B.2.1, B.2.2 and B.2.3 with payment contingent upon achievement of outcome performance. Performance assessed and payments made on a six-month interval.
e. Data Source: CARE, CMBHS and MBOW. FY16 will serve as a benchmarking year for the following Resilience and Recovery Outcomes.. There will be no sanctions assessed for these outcomes during the FY16 benchmarking year: 5. School
a. Target: The percentage of children and youth authorized in a FLOC with acceptable or improved school performance.
b. Calculation: (Numerator/Denominator)*100 i. Numerator: # of children and youth authorized in a FLOC who meet
or exceed the RCI benchmark in the direction of improvement for the CANS School module (i.e., ≤-1.645, indicating fewer problematic symptoms) or who have CANS item scores of 0,1 for all School module items at both first and last UAs. If the child or youth does not experience any difficulties in school (or has completed school) and therefore does not trigger the school module via a score >0 on the CANS School item, then the default mean score for the module is 0. First and last UAs must be at least 75 days apart.
ii. Denominator: # of children and youth authorized in a FLOC with first and last UAs at least 75 days apart.
c. Exclusion(s)/Exception(s): d. Sanctions and Remedies: N/A e. Data Source: CMBHS and MBOW
Assessment of CANS Acceptable/Improved School Functioning for Children in a full LOC
6. Family and Living Situation
a. Target: The percentage of children and youth authorized in a FLOC with
Information Item C
FY 2016 Information Item C Page Info. C - 16
acceptable or improved family and living situations. b. Calculation: (Numerator/Denominator)*100
i. Numerator: # of children and youth authorized in a FLOC who meet or exceed the RCI benchmark in the direction of improvement for the ANSACANS Family and Living Situation items (i.e., ≤-1.645, indicating fewer problematic symptoms) or who have CANS Family and Living Situation item scores of 0,1 at both first and last UAs. First and last UAs must be at least 90 days apart.
ii. Denominator: # of children and youth authorized in a FLOC with first and last UAs at least 75 days apart.
c. Exclusion(s)/Exception(s): If the child/youth does not have a family unit, the family item will be marked as not applicable. This item should only be evaluated for children and youth with a score on both items.
d. Sanctions and Remedies: N/A e. Data Source: CMBHS and MBOW
7. Strengths a. Target: The percentage of children and youth authorized in a FLOC with
acceptable or improved strengths. b. Calculation: (Numerator/Denominator)*100
i. Numerator: # of children and youth authorized in a FLOC who meet or exceed the RCI benchmark in the direction of improvement for the CANS Strengths domain (i.e., ≤-1.645, indicating fewer problematic symptoms) or who have CANS item scores of 0,1 for all Strengths domain items at both first and last UAs. First and last UAs must be at least 90 days apart.
ii. Denominator: # of children and youth authorized in a FLOC with first and last UAs at least 75 days apart.
c. Exclusion(s)/Exception(s): d. Sanctions and Remedies: N/A e. Data Source: CMBHS and MBOW
8. Life Domain Functioning a. Target: The percentage of children and youth authorized in a FLOC with
acceptable or improved life functioning. b. Calculation: (Numerator/Denominator)*100
i. Numerator: # of children and youth adults authorized in a FLOC who meet or exceed the RCI benchmark in the direction of improvement for the ANSACANS Life Domain Functioning domain (i.e., ≤-1.645, indicating fewer problematic symptoms) or who have ANSACANS item scores of 0,1 for all Life Domain Functioning domain items at both first and last UAs. First and last UAs must be at least 90 days apart.
ii. Denominator: # of children and youth authorized in a FLOC with first and last UAs at least 75 days apart.
c. Exclusion(s)/Exception(s): d. Sanctions and Remedies: N/A e. Data Source: CMBHS and MBOW
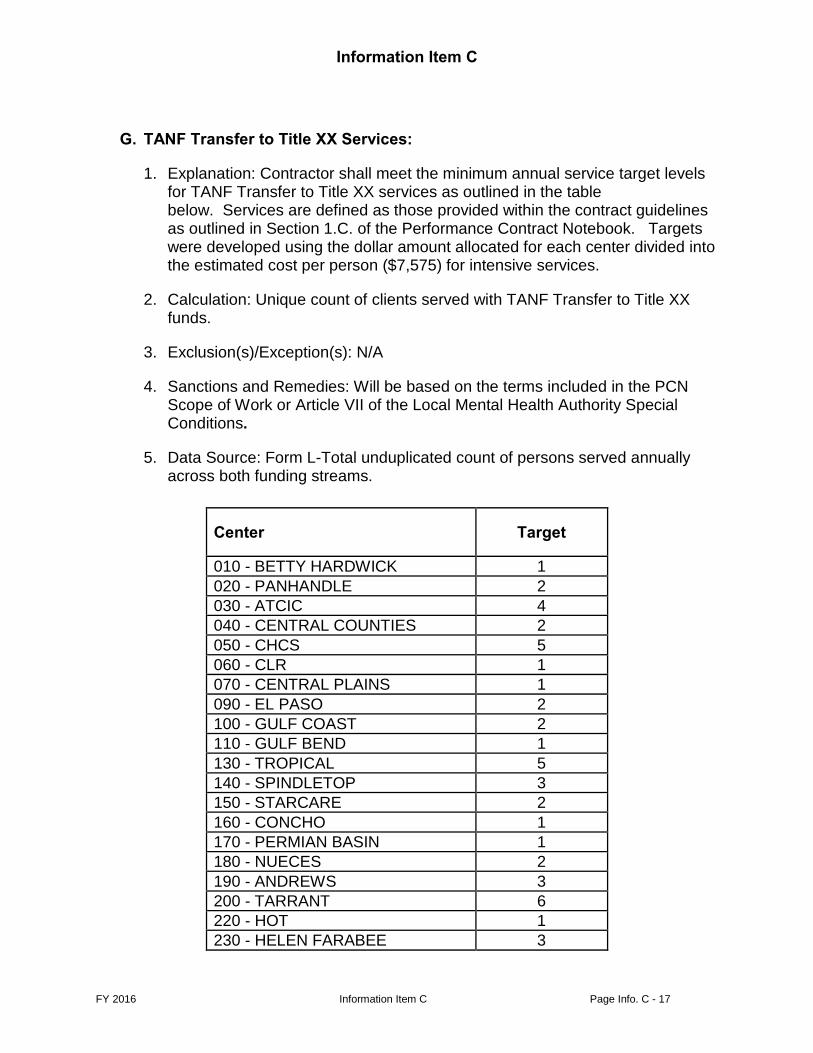
Information Item C
FY 2016 Information Item C Page Info. C - 17
G. TANF Transfer to Title XX Services:
1. Explanation: Contractor shall meet the minimum annual service target levels for TANF Transfer to Title XX services as outlined in the table below. Services are defined as those provided within the contract guidelines as outlined in Section 1.C. of the Performance Contract Notebook. Targets were developed using the dollar amount allocated for each center divided into the estimated cost per person ($7,575) for intensive services.
2. Calculation: Unique count of clients served with TANF Transfer to Title XX funds.
3. Exclusion(s)/Exception(s): N/A
4. Sanctions and Remedies: Will be based on the terms included in the PCN Scope of Work or Article VII of the Local Mental Health Authority Special Conditions.
5. Data Source: Form L-Total unduplicated count of persons served annually across both funding streams.
Center Target
010 - BETTY HARDWICK 1 020 - PANHANDLE 2 030 - ATCIC 4 040 - CENTRAL COUNTIES 2 050 - CHCS 5 060 - CLR 1 070 - CENTRAL PLAINS 1 090 - EL PASO 2 100 - GULF COAST 2 110 - GULF BEND 1 130 - TROPICAL 5 140 - SPINDLETOP 3 150 - STARCARE 2 160 - CONCHO 1 170 - PERMIAN BASIN 1 180 - NUECES 2 190 - ANDREWS 3 200 - TARRANT 6 220 - HOT 1 230 - HELEN FARABEE 3
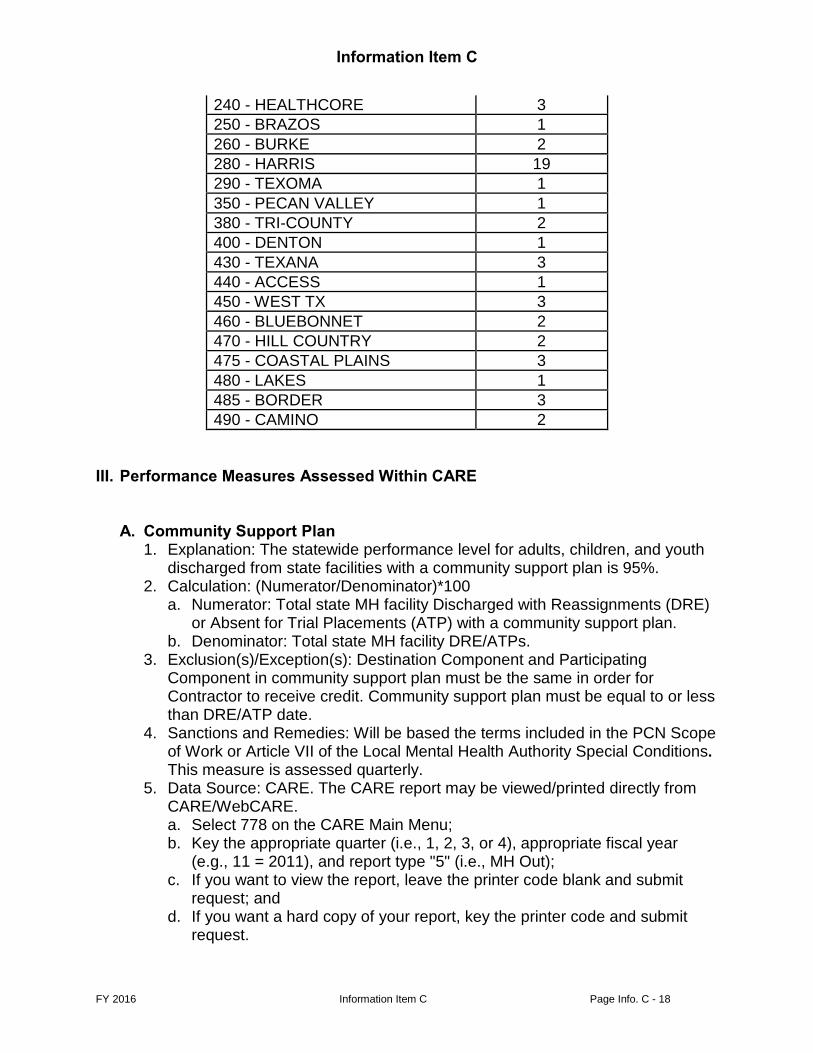
Information Item C
FY 2016 Information Item C Page Info. C - 18
240 - HEALTHCORE 3 250 - BRAZOS 1 260 - BURKE 2 280 - HARRIS 19 290 - TEXOMA 1 350 - PECAN VALLEY 1 380 - TRI-COUNTY 2 400 - DENTON 1 430 - TEXANA 3 440 - ACCESS 1 450 - WEST TX 3 460 - BLUEBONNET 2 470 - HILL COUNTRY 2 475 - COASTAL PLAINS 3 480 - LAKES 1 485 - BORDER 3 490 - CAMINO 2
III. Performance Measures Assessed Within CARE
A. Community Support Plan
1. Explanation: The statewide performance level for adults, children, and youth discharged from state facilities with a community support plan is 95%.
2. Calculation: (Numerator/Denominator)*100 a. Numerator: Total state MH facility Discharged with Reassignments (DRE)
or Absent for Trial Placements (ATP) with a community support plan. b. Denominator: Total state MH facility DRE/ATPs.
3. Exclusion(s)/Exception(s): Destination Component and Participating Component in community support plan must be the same in order for Contractor to receive credit. Community support plan must be equal to or less than DRE/ATP date.
4. Sanctions and Remedies: Will be based the terms included in the PCN Scope of Work or Article VII of the Local Mental Health Authority Special Conditions. This measure is assessed quarterly.
5. Data Source: CARE. The CARE report may be viewed/printed directly from CARE/WebCARE. a. Select 778 on the CARE Main Menu; b. Key the appropriate quarter (i.e., 1, 2, 3, or 4), appropriate fiscal year
(e.g., 11 = 2011), and report type "5" (i.e., MH Out); c. If you want to view the report, leave the printer code blank and submit
request; and d. If you want a hard copy of your report, key the printer code and submit
request.
Information Item C
FY 2016 Information Item C Page Info. C - 19
6. Data Source: CARE. The CARE report may be viewed/printed directly B. Follow-Up Within Seven Days
1. Explanation: The statewide follow-up performance level for adults, children, and youth discharged from a state facility, privately operated and state funded facility (i.e., Montgomery County Mental Health Treatment Facility and University of Texas Health Science Center at Tyler), or private psychiatric hospital funded through a Private Psychiatric Bed (PPB) or Community Mental Health Hospital (CMHH) contract is 75% for face-to-face follow-up, and 95% with any follow-up disposition.
2. Calculation: (Numerator/Denominator)*100 a. Numerator: Number of face-to-face follow-ups (i.e., F001, F002 and FR01)
entered in CARE. b. Numerator: Number of any follow-up disposition (i.e., F001, F002, FR01,
F005, and FR03) entered in CARE. c. Denominator: Number of ATPs/DREs.
3. Exclusion(s)/Exception(s): a. CARE searches for adults discharged (ATP or DRE) from a state MH
facility (hospital, state center), excluding the following situations at discharge: i. Arrest to Jail; ii. Court Release; iii. Children’s Protective Services; iv. Involuntary Unauthorized Departure; v. Jail; vi. Medical Inpatient; vii. Out of State; viii. Private Provider; ix. Private Psychiatric Hospital; x. Private Residential Treatment Center; xi. Single Diagnosis Substance Abuse; xii. State Funded Community Hospital; xiii. State Hospital; xiv.State School; xv. Substance Abuse Treatment Center (Inpatient); xvi.Veterans Administration Inpatient; xvii. Veterans Administration Outpatient; and xviii. Voluntary Unauthorized Departure.
b. If the client returns to campus from ATP w/n 7 days and no follow-up entered, client is not counted in Denominator. If a follow-up is entered, CARE counts person in Numerator and Denominator.
c. If ATP followed by DRE, then CARE checks for a follow-up from the ATP. d. If a client is DRE and ADM to campus in less than 7 days, follow-up will be
expected on the DRE. If a follow-up was completed on both ATP and DRE, then CARE counts only the ATP follow-up.
e. If ATP, followed by a Return from Absence (RET) in more than 7 days, followed by DRE, then CARE expects a follow-up for both ATP and DRE
Information Item C
FY 2016 Information Item C Page Info. C - 20
and counts two discharges and up to two follow-ups. f. Contractor may report to CARE a service type FR01 (face-to-face contact
with discharged individual within 7 days; individual refuses enrollment into community services). Date of refusal must be within 7 days following end date of assignment.
g. Contractor may report to CARE a service type FR03 (individual refuses community services via contact with individual, family member, legal guardian, or other collateral). Good faith efforts to provide face-to-face contact must be documented. Contractor may report to CARE a service type F005 (unable to locate individual within 7 days). Good faith efforts to provide face-to-face contact must be documented. Date of refusal must be within 7 days following end date of assignment from state mental health facility (SMHF). Entry of these two service types do not fall into Numerator a. for this measure and therefore do not get credited as face-to-face follow-ups entered.
4. Sanctions and Remedies: Will be based the terms included in the PCN Scope of Work or Article VII of the Local Mental Health Authority Special Conditions. This measure is assessed quarterly.
5. Data Source: CARE. The CARE report may be viewed/printed directly from CARE/WebCARE. a. Select 778 on the CARE Main Menu; b. Key the appropriate quarter (i.e., 1, 2, 3, or 4), appropriate fiscal year
(e.g., 11 = 2011), and report type "5" (i.e., MH Out); c. If you want to view the report, leave the printer code blank and submit
request; and d. If you want a hard copy of your report, key the printer code and submit
request.
C. Long-Term Services and Support Screen
1. Explanation: Contractor shall act upon referrals within 15 calendar days of receipt from the Long-term Services and Supports (LTSS) Screen.
2. Contractor shall demonstrate successful action a referral by utilizing the H0023 procedure code (grid code 100) for adults and the H0023HA procedure code (grid code 200) for children.
3. Allowable Server Types: All (A-R) 4. Contact Type: Contractor coding T (telephone), F (face-to-face), or D
(documentation) on the procedure code will be demonstrating successful action the referral.
5. Calculation The numerator will be the number of successfully acted upon referrals divided by the denominator of total referrals received multiplied by 100. The proposed calculation for passing this measure shall be 70%.
6. Data Source: MBOW IV. Crisis Response System Outcomes
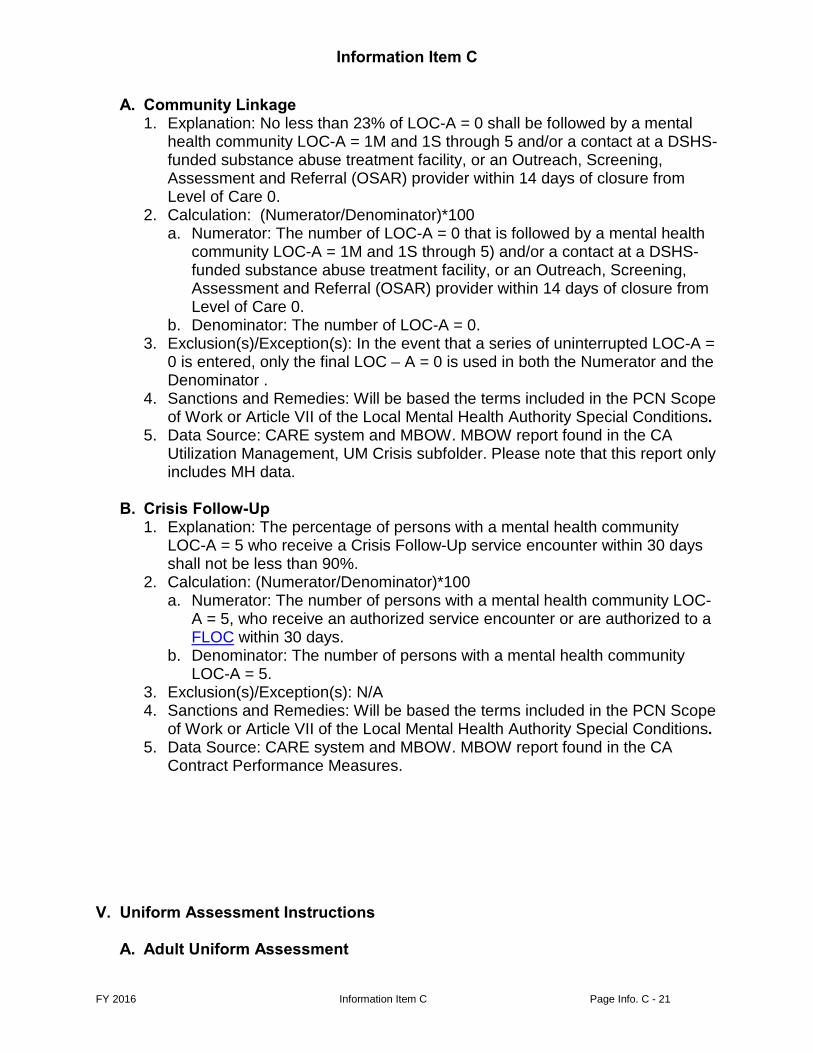
Information Item C
FY 2016 Information Item C Page Info. C - 21
A. Community Linkage 1. Explanation: No less than 23% of LOC-A = 0 shall be followed by a mental
health community LOC-A = 1M and 1S through 5 and/or a contact at a DSHS-funded substance abuse treatment facility, or an Outreach, Screening, Assessment and Referral (OSAR) provider within 14 days of closure from Level of Care 0.
2. Calculation: (Numerator/Denominator)*100 a. Numerator: The number of LOC-A = 0 that is followed by a mental health
community LOC-A = 1M and 1S through 5) and/or a contact at a DSHS-funded substance abuse treatment facility, or an Outreach, Screening, Assessment and Referral (OSAR) provider within 14 days of closure from Level of Care 0.
b. Denominator: The number of LOC-A = 0. 3. Exclusion(s)/Exception(s): In the event that a series of uninterrupted LOC-A =
0 is entered, only the final LOC – A = 0 is used in both the Numerator and the Denominator .
4. Sanctions and Remedies: Will be based the terms included in the PCN Scope of Work or Article VII of the Local Mental Health Authority Special Conditions.
5. Data Source: CARE system and MBOW. MBOW report found in the CA Utilization Management, UM Crisis subfolder. Please note that this report only includes MH data.
B. Crisis Follow-Up
1. Explanation: The percentage of persons with a mental health community LOC-A = 5 who receive a Crisis Follow-Up service encounter within 30 days shall not be less than 90%.
2. Calculation: (Numerator/Denominator)*100 a. Numerator: The number of persons with a mental health community LOC-
A = 5, who receive an authorized service encounter or are authorized to a FLOC within 30 days.
b. Denominator: The number of persons with a mental health community LOC-A = 5.
3. Exclusion(s)/Exception(s): N/A 4. Sanctions and Remedies: Will be based the terms included in the PCN Scope
of Work or Article VII of the Local Mental Health Authority Special Conditions. 5. Data Source: CARE system and MBOW. MBOW report found in the CA
Contract Performance Measures.
V. Uniform Assessment Instructions
A. Adult Uniform Assessment
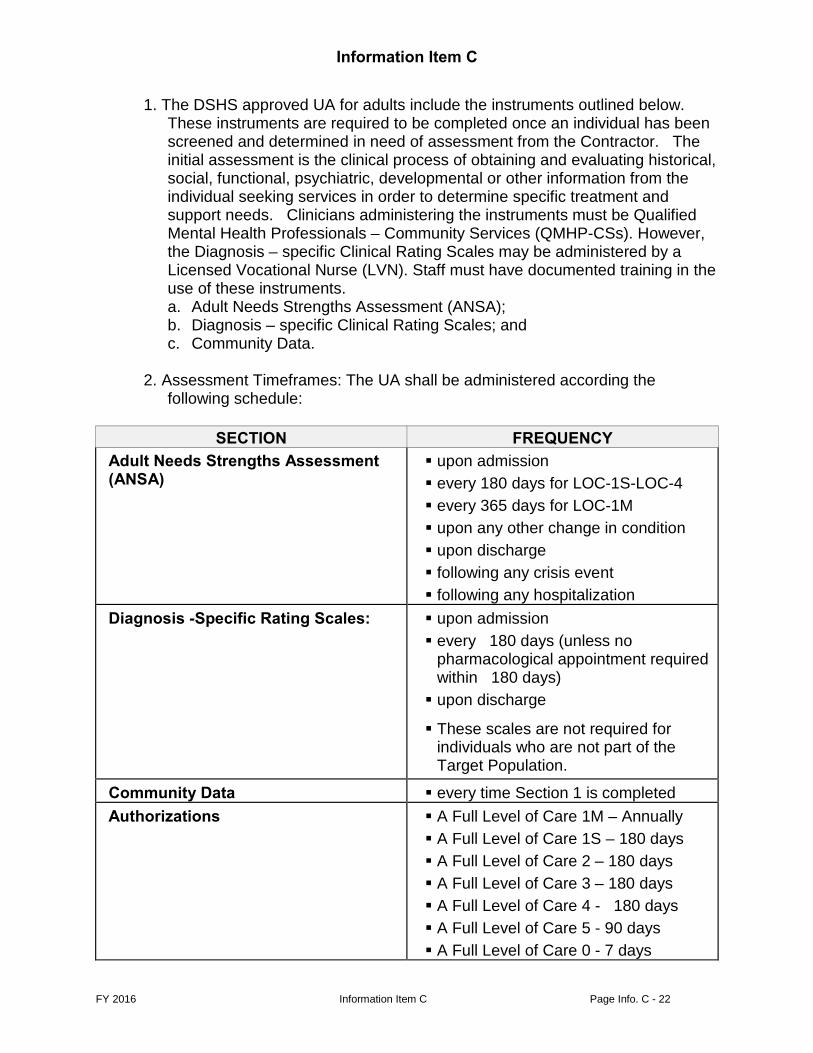
Information Item C
FY 2016 Information Item C Page Info. C - 22
1. The DSHS approved UA for adults include the instruments outlined below. These instruments are required to be completed once an individual has been screened and determined in need of assessment from the Contractor. The initial assessment is the clinical process of obtaining and evaluating historical, social, functional, psychiatric, developmental or other information from the individual seeking services in order to determine specific treatment and support needs. Clinicians administering the instruments must be Qualified Mental Health Professionals – Community Services (QMHP-CSs). However, the Diagnosis – specific Clinical Rating Scales may be administered by a Licensed Vocational Nurse (LVN). Staff must have documented training in the use of these instruments. a. Adult Needs Strengths Assessment (ANSA); b. Diagnosis – specific Clinical Rating Scales; and c. Community Data.
2. Assessment Timeframes: The UA shall be administered according the
following schedule:
SECTION FREQUENCY Adult Needs Strengths Assessment (ANSA)
upon admission every 180 days for LOC-1S-LOC-4 every 365 days for LOC-1M upon any other change in condition upon discharge following any crisis event following any hospitalization
Diagnosis -Specific Rating Scales: upon admission every 180 days (unless no
pharmacological appointment required within 180 days) upon discharge
These scales are not required for individuals who are not part of the Target Population.
Community Data every time Section 1 is completed Authorizations A Full Level of Care 1M – Annually
A Full Level of Care 1S – 180 days A Full Level of Care 2 – 180 days A Full Level of Care 3 – 180 days A Full Level of Care 4 - 180 days A Full Level of Care 5 - 90 days A Full Level of Care 0 - 7 days
Information Item C
FY 2016 Information Item C Page Info. C - 23
Assessments in CARE/CMBHS: Data must be submitted through WebCARE/ CMBHS or through an approved batch to the CARE/CMBHS system according to the schedule and formats established by DSHS.
B. Child & Adolescent Uniform Assessment Instructions
The DSHS approved Child and Adolescent Needs and Strengths (CANS) Assessment is a component of the Uniform Assessment for children and youth. The Protocol Matrix for the Uniform Assessment includes the items that must be completed once a child or youth has been screened and determined to need an assessment by the LMHA. The Uniform Assessment is completed per the following Protocol Matrix. The person administering the Uniform Assessment must be at a minimum a Qualified Mental Health Professional – Community Services (QMHP-CS); additionally, the person administering the CANS must have documented current certification in the use of the CANS.
Information Item C
FY 2016 Information Item C Page Info. C - 24
Uniform Assessment Protocol Matrix: SECTION FREQUENCY
Child and Adolescent Needs and Strengths (CANS) Assessment
upon admission every 90 days (unless child or youth is approved for 180-Day Extended Review authorization) upon discharge following any crisis event following any hospitalization 180-Day Extended Review Authorization: for LOC-1 once a child has been assessed and authorized three consecutive times to LOC-1 when LOC-R and LOC-A = LOC-1, a reassessment can be done every 180 days thereafter when: both the LOC-R and LOC-A equal
LOC-1 and; the preceding LOC-R and LOC-A
equal LOC-1 and; the Extended Review box has been
checked and approved.
Community Data every time Section 1 is completed
Authorizations every 90 days (except as noted below) For LOC-1 may be done every 180 days when 180-Day Extended Review Authorization has been approved. (See above Section 1: Child and Adolescent Needs and Strengths (CANS) Assessment)
Residential Treatment Center Placement (excluding Waco Center for Youth)
if a child is placed in a DSHS-funded residential treatment center (RTC) bed outside of the LMHA service area, ongoing diagnostic assessments may be provided by phone, utilizing data collected from the child, child’s LAR, and child’s RTC therapist
Assessments in CARE/CMBHS: Data must be submitted through WebCARECMBHS online or through an approved batch to the CARE/CMBHS system according to the schedule and formats established by DSHS.
Information Item C
FY 2016 Information Item C Page Info. C - 25
VII. Glossary of Terms
1. ANSA: Adult Needs and Strengths Assessment 2. Assessment Service: Includes psychiatric diagnostic interview examination,
pre-admission QMHP-CS assessment, and psychological or neuropsychological testing.
3. CANS: Child and Adolescent Needs and Strengths assessment 4. CARE: Client Assignment and Registration System 5. Client Month: Refers to a count of clients and months for the measured
reporting period. For example, a client with activity in 3 months of a measured period counts as 3, those with activity only in 1 month counts as 1.
6. Clinical and Support Services: Services that have been identified as those that provide support and foster recovery. The clinical and support services refers to all approved TRR services delivered face to face or via telehealth/telemedicine as listed in the LOCs in the Um Guidelines. The services categories include the following: Pre-Admission Assessment, Psychiatric Diagnostic Interview, Routine Case Management, Psychosocial Rehabilitation Services, Engagement Activity, Consumer Peer Support, Pharmacological Management, Med Training and Supports, Individual/Family Counseling, Group Counseling, Supported Employment, Skills Training and Development, and Supportive Housing Services and Supports.
7. CMBHS: Clinical Management for Behavioral Health Services 8. Crisis Client Month: A client who has any time reported as crisis in a
calendar month. 9. Crisis Episode: A crisis episode begins when a crisis service is provided to
an individual where there are no other crisis services provided to that individual within the previous seven days.
10. Crisis Redesign: The 81st Legislature appropriated new crisis funding to DSHS to support a statewide initiative to enhance the crisis service delivery system. This ongoing DSHS initiative is known as Crisis Redesign. The policies and expectations for the enhanced crisis system were initially based on specifications in Rider 65 of the General Appropriations Act, 81st Legislature. The Legislature has continued to allocate this funding to DSHS. Based on the positive outcomes attained during the biennium when Rider 65 specifically appropriated the new crisis funding, DSHS will continue to fund Crisis Redesign in keeping with the policies and expectations reflected in Rider 65.
11. Crisis Service: A crisis service includes both inpatient and outpatient service procedure codes that either contain an ET modifier (ex., psychosocial rehabilitative services in response to a crisis = H2017ET), or are uniquely defined as a crisis service (ex., crisis residential = H0018).
12. DSHS Purchased Inpatient Bed: Refers to accommodation at a state hospital, Montgomery County Mental Health Treatment Facility, DSHS funded community hospitals (i.e., Harris County Psychiatric Center, Sunrise Canyon, and Galveston Community Hospital) documented using CARE
Information Item C
FY 2016 Information Item C Page Info. C - 26
assignment codes H035, and TC07, or local hospitalizations paid for with DSHS funding and reported as encounters using procedure codes = T2048 and T2048HA, It excludes Crisis Stabilization Units (CSU) - including Hill Country, Extended Observation Units (EOU), Crisis Respite, Crisis Residential and Rusk and Vernon forensic locations.
13. DSHS Purchased Inpatient Bed Day: Refers to a day in a DSHS Purchased Inpatient Bed. Generally the count includes each day in the facility that crossed midnight except for same day admissions and discharges which count as one day.
14. Family Partner support services include the following: Engagement (H0025HATS), Family Partner (H0038HA), and Parent Support Group (H0025HAHQ) procedure codes, or other services identified by SERVER_TYPE_CD = K.
15. Full Client Month: A calendar month in which a client receives services within the same LOC from the first through the last day of the same month.
16. Full Level of Care (FLOC): Refers to Texas Resilience and Recovery (TRR) levels of care that are intended for ongoing service delivery, specifically adult levels of care A1M, A1S, A2, A3, and A4 and children and youth levels of care C1, C2, C3, C4, and Young Child (YC).
17. Improvement: Significant change over time, with a Reliable Change Index (RCI) score exceeding the benchmark value of ±1.645.
18. Level of Care (LOC): Refers to Texas Resilience and Recovery (TRR) levels of care for any service.
19. LOC-Y: Youth Empowerment Services (YES) Waiver clients. 20. MBOW: Mental retardation and Behavioral health Outpatient Warehouse 21. Measured Month: The month for which the DSHS Contract Manager
performs a compliance review. 22. Mental Health (MH) Hourly Service: Includes all mental health services
reported via encounter data that are counted towards contact performance measures. It includes only services where the reporting unit is measured in hours (daily or residential services are excluded.) In addition, the following hourly services are excluded: • Telephone contacts; and • Services with a ‘GJ’ procedure code modifier.
23. Monthly Service Provision: This measure is intended to determine the amount of clients who receive any mental health hourly service. These services must be delivered face-to-face or via telehealth or telemedicine.
24. Partially Authorized Months: Refers to months when a client was not authorized and being served in the community for the entire calendar month. Specifically, months where a client: • Is admitted to service after the first day of the month; • Is discharged from services; • Changes authorized Level of Care; or • Has a DSHS Purchased Inpatient Bed Day.
25. RCI: Reliable Change Index. This value is calculated to determine
Information Item C
FY 2016 Information Item C Page Info. C - 27
significant change over time using the formula: 𝐑𝐑𝐑𝐑𝐑𝐑 = (𝑿𝑿𝟐𝟐−𝑿𝑿𝟏𝟏)𝑺𝑺𝑺𝑺𝑺𝑺𝑺𝑺𝑺𝑺𝑺𝑺
, where SEdiff =
𝐒𝐒𝐒𝐒 ∗ �𝟏𝟏 − 𝒓𝒓𝒙𝒙𝒙𝒙. X1 = data value at time 1, X2 = data value at time 2, SD = Standard Deviation of the data observations (generated using first administrations of the test), and rxx = inter-rater reliability (this is a correlation representing consistency in use of the tool across multiple users of the tool).
26. Screening Service: Includes screening, hotline, crisis follow-up and relapse prevention, benefit eligibility determination, and continuity of services.
27. Texas Law Enforcement Telecommunications System: (TLETS) 28. Under Served: Refers to clients who are authorized to a less intensive
Level of Care than the Level of Care recommended by the DSHS approved uniform assessment calculator.
29. Valid TLETS Booking: Refers to a request issued by the DPS TLETS system to perform a match of consumers in the mental health data system that has been logged in CARE. As duplicate matches are issued at times, only the first match is retained each date of request per jail facility name, County and set of match elements (first name, last name, date of birth gender, SSN, race).
30. Continuity of Care Match: Consumers who have any of these activities within the last 3 fiscal years: • An open authorization to a FLOC, level of care 5, 8 or YES; • An MH service encounter other than those services with procedure
codes H0030 (crisis hot line), H0002 (screening) or GJ modifiers (false alarm);
• A hospital discharge; or • A new generation medication assignment.





























