Embed Size (px)
Citation preview
Texas Medicaid Basics
Barry S. Lachman, MD, MPHOctober, 2012
What is Medicaid?
Jointly funded state-federal program providing health coverage to low-income and disabled individuals.
Federal agency: Centers for Medicare and Medicaid Services (CMS)
State agency: Health and Human Services Commission (HHSC)
Medicaid is entitlement program
Federal law requires coverage for certain populations and services.
States are allowed to cover additional populations.
Eligibility is based on income, age and certain eligibility categories
Guaranteed coverage for eligible services to eligible individuals.
Medicaid EligibilityMedicaid serves:
Low-income families
Children
Related caretakers of dependent children
Pregnant women
Elderly
Individuals with disabilities
Eligibility criteria:
Residency in Texas
U.S. citizen or qualified aliens legally admitted for permanent residency
Income and resource limits
Functional and medical criteria for long-term services and support
Most child applicants must be under age of 19
Medicaid Caseload
Services for the aged, blind, and disabled are the largest share of program costs
50% of all enrollees are in FFS & PCCM models thatwere not designed to manage costs.
66% are children
currently serves about 3.3 million people
Federal Poverty Level
FPLis the definition of poverty used by the federal government as the reference point to determine Medicaid eligibility
is the income level below which a person is officially considered to lack adequate financial resources and to be living in poverty
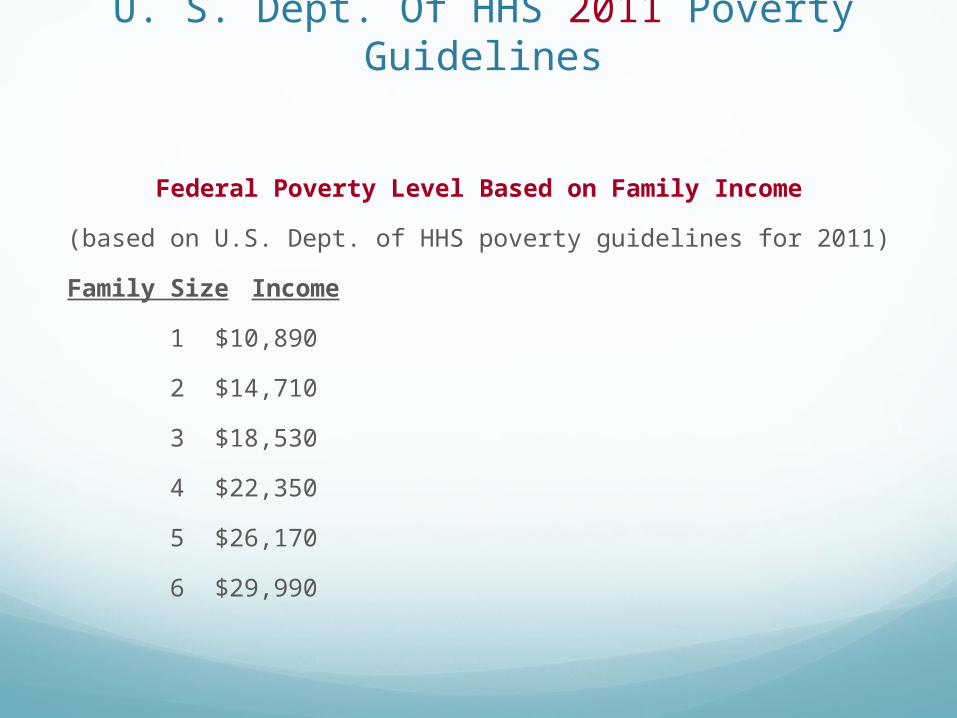
U. S. Dept. Of HHS 2011 Poverty Guidelines
Federal Poverty Level Based on Family Income
(based on U.S. Dept. of HHS poverty guidelines for 2011)
Family Size Income
1 $10,890
2 $14,710
3 $18,530
4 $22,350
5 $26,170
6 $29,990
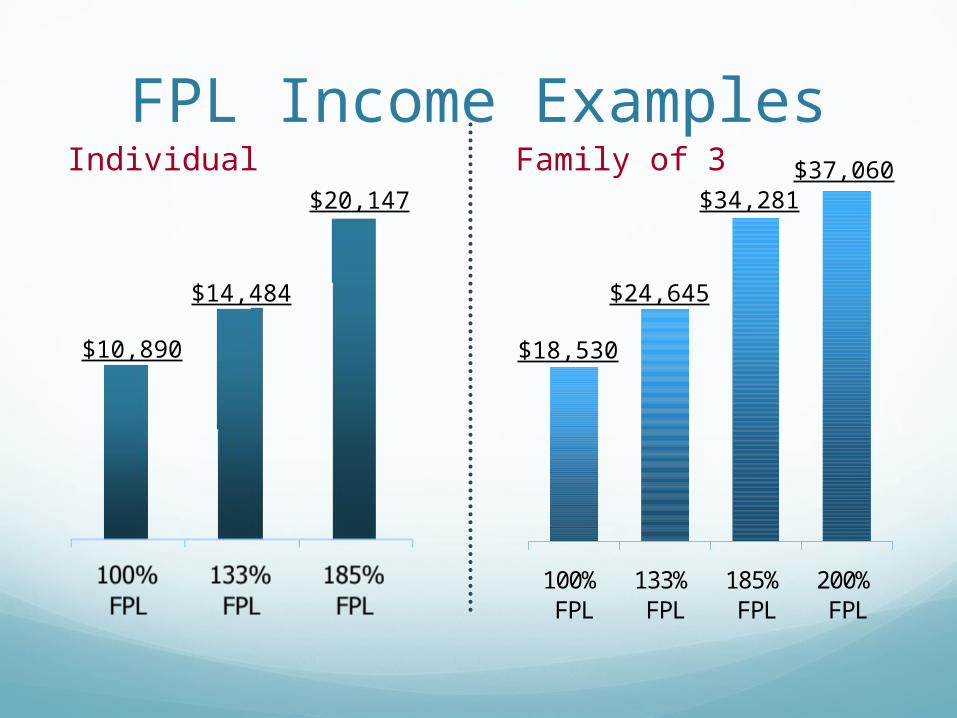
FPL Income ExamplesIndividual
100%FPL
133%FPL
185%FPL
200%FPL
$10,890
$14,484
$20,147
Family of 3
$18,530
$24,645
$34,281$37,060
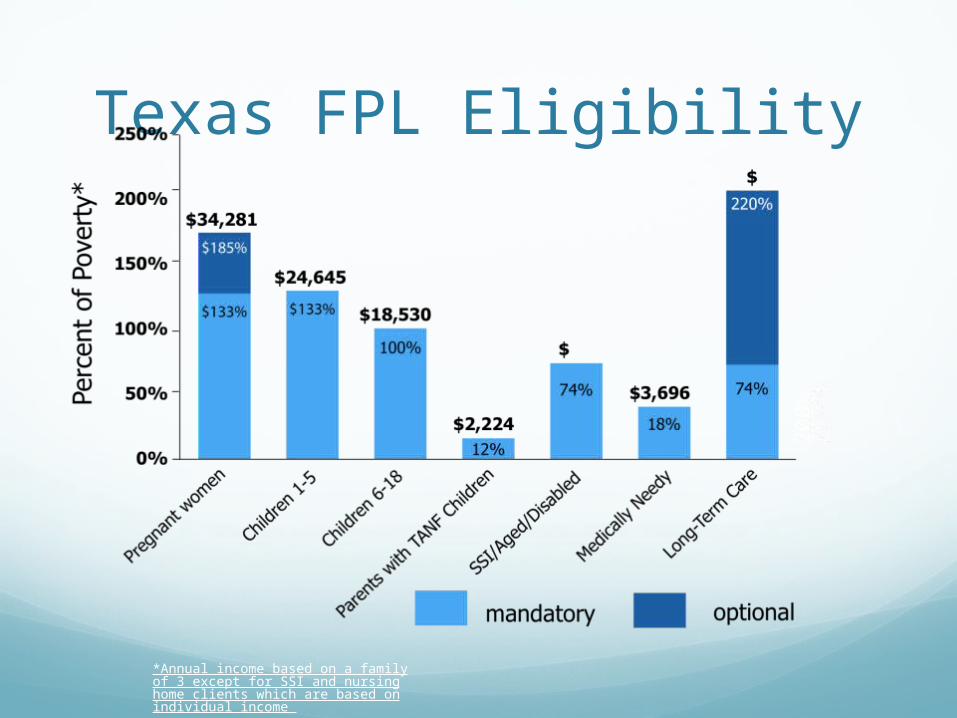
Texas FPL Eligibility
*Annual income based on a family of 3 except for SSI and nursing home clients which are based on individual income
20
0%
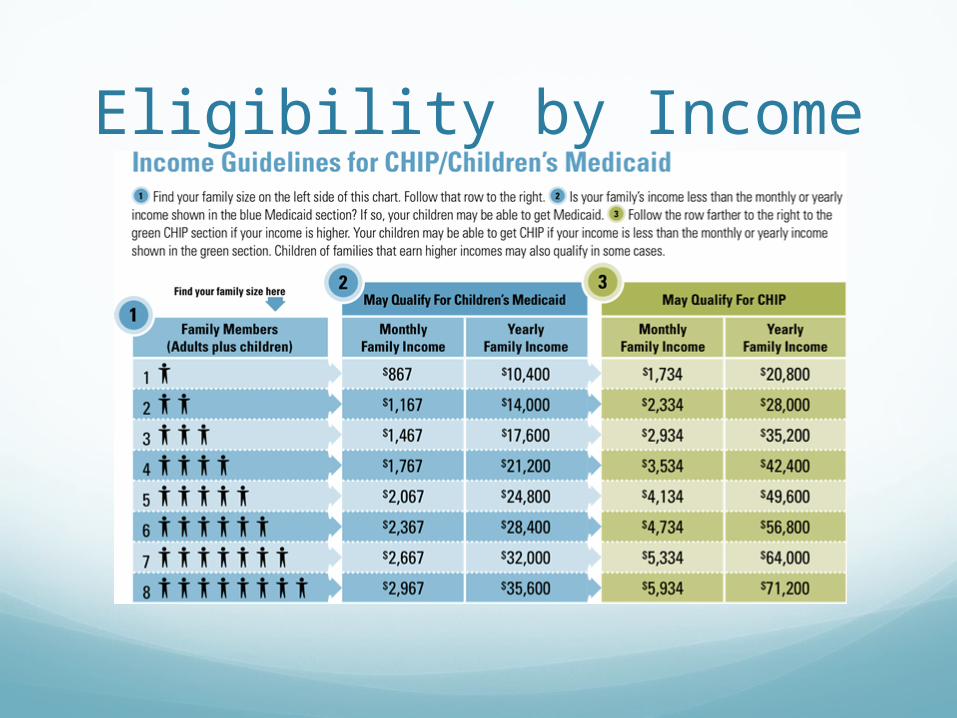
Eligibility by Income
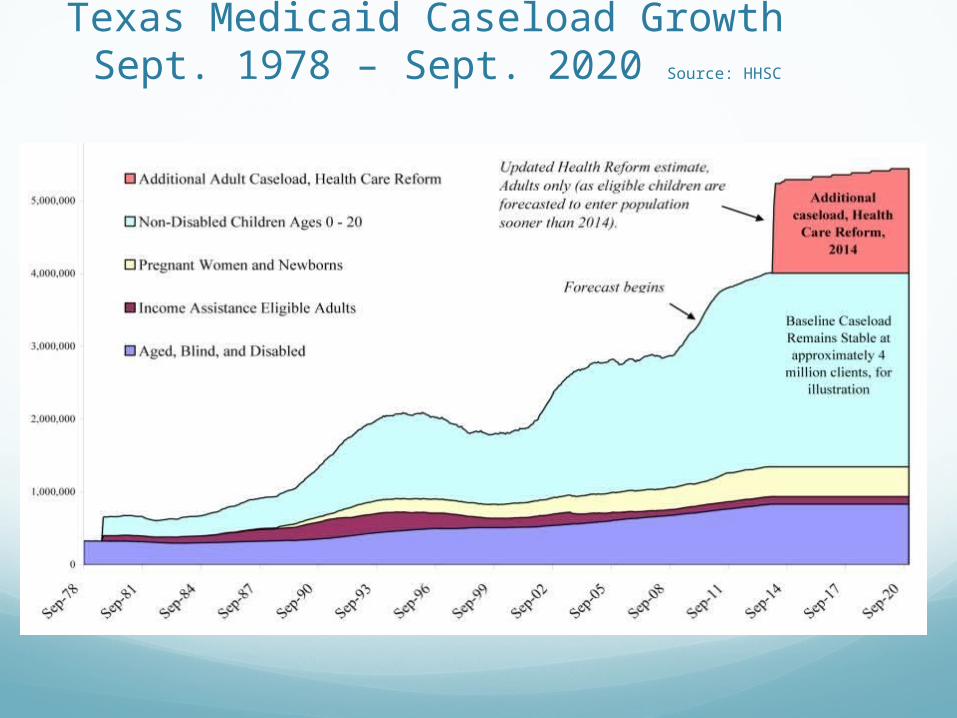
Texas Medicaid Caseload Growth Sept. 1978 – Sept. 2020 Source: HHSC
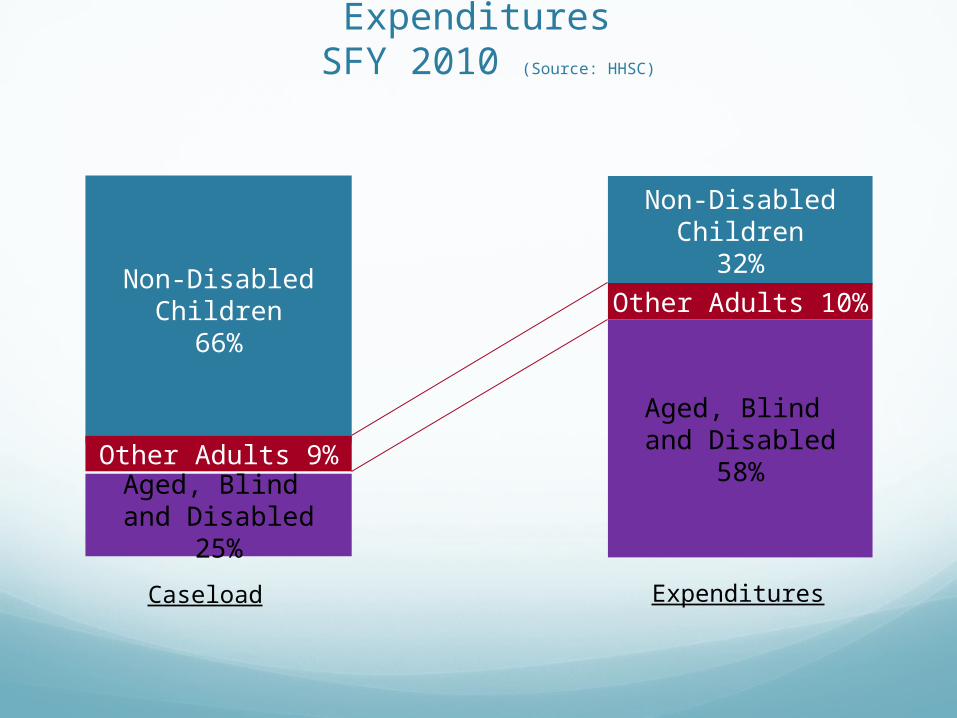
Texas Medicaid Beneficiaries & Expenditures SFY 2010 (Source: HHSC)
Non-DisabledChildren
66%
Non-DisabledChildren
32%
Other Adults 9%
Other Adults 10%
Aged, Blind and Disabled
25%
Aged, Blind and Disabled
58%
Caseload Expenditures
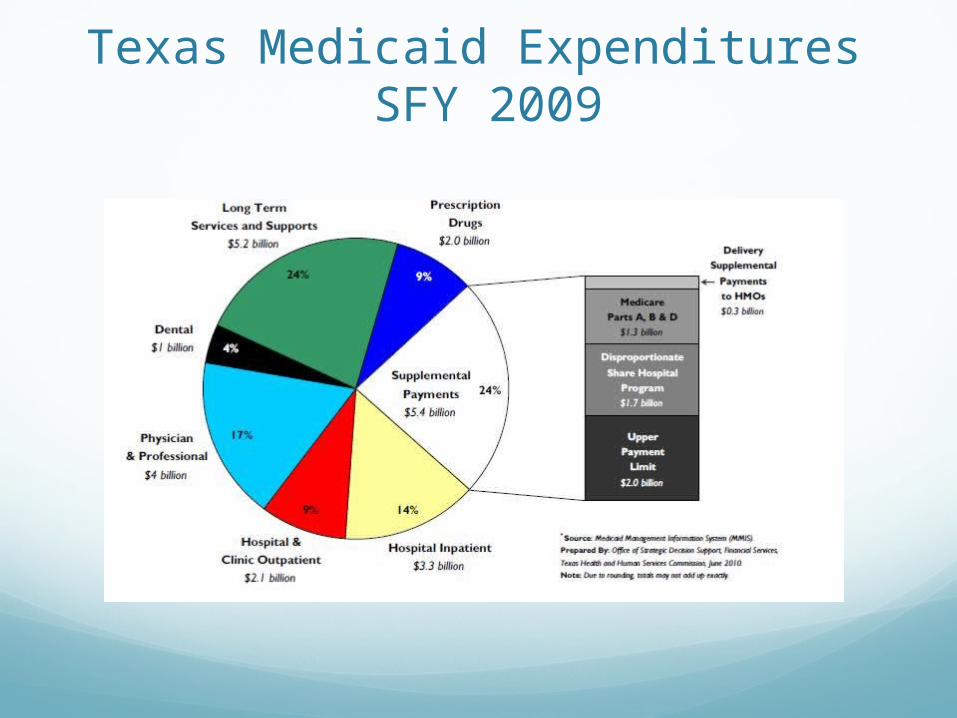
Texas Medicaid Expenditures SFY 2009
Medicaid BenefitsMandatory Benefits
The services states are federally required to offer as part of state program
Optional Benefits
Federally approved additional services that states can offer under Medicaid program

Services Covered
Covers basic health care servicesphysician services inpatient, outpatient care pharmacy, lab and x-ray long term care services for the aged and disabled

How is Medicaid Funded?Medicaid is funded by both state and federal
governments.
Federal share is based on Federal Medical Assistance Percentage (FMAP)
FMAP is based on state’s per capita personal income compared to the U. S. average.
Texas receives FMAP of approximately 60% meaning 60/40 split for most client services.
Supplemental Federal Funding
Upper Payment Limit (UPL) – payments made to hospitals and physicians to make up the difference between what Medicaid pays for services and what Medicare would have paid for the same care.
Disproporionate Share Hospital Program (DSH) – special payments made to hospitals that serve a disproportionately large number of Medicaid and low-income patients.
Health Reform: Myth and Truth
Barry S. Lachman, MD, MPH
Why is Medicaid ImportantSafety Net for the underserved and vulnerable
Key cog in assuring universal coverage for those under 133% of poverty
Medicaid Myths and Reality
Myth: Federal Program – actually much State control
Benefits are very generous – true, more than any commercial insurance or Medicare. However, covers those with disabilities who are more expensive.
Fiscally unsustainable – State budgets are challenged; however, we are already paying for these services. 40% of health expenditures are wasted (IOM, 2012)
Medicaid is a failure – fales. It has narrowed gap on health disparities. Multiple good studies show improved health outcomes in those served
Could just move them into commercial insurance – false. Has been tried. It does not work.
The State of the Healthcare System
Costs out of control
Over 40 million uninsured
Poor quality – Overall Texas is at or near the bottom on almost all measures
Ration based on income
Employer based model in rapid decline
Insurance unaffordable for many
Very inefficient system
Multiple problems not just access
21
The Uninsured Over 40 million uninsured (US Census Bureau, New York Times,
Austin American Statesman, Lubbock Times
Texas highest uninsured rate in US (same)
Texas highest number of uninsured children (KFF, US Census Bureau) Over 1 million uninsured children in Texas (Kids Count Survey)
Dallas has second most uninsured of any city – 1.4 million (TMA)
Over 90% of uninsured in Dallas are US citizens (CPPP)
1 in 5 women in Dallas uninsured (Dallas Women’s Foundation)
Most are low income (Census Bureau, CPPP, Dallas Women’s Foundation, KFF)
22
Texas Health Statistics 47th in % of insured children (KFF)
47th in % of insured adults (KFF)
2nd in number of uninsured adults (KFF)
2nd in Total Uninsured (KFF)
1st in number of uninsured children (KFF)
Public Mental Health expenditures (48th)
Infectious Disease – 46th
Lack of Health Insurance – 50th
Early Prenatal Care – 50th
Affordable or NotTexas cost cover 80% of uninsured for 1%
increase in State Health Care Spending CPPP
CMS (DMN 6/14/2012) – cover 30 million (75%) for 0.1% increase per year in costsDoes not include any savings from billDoes not look at NPV of investment – what is the
cost of not doing it over time
Supreme Court RulingUpholds all challenged parts of ACA except
Medicaid Expansion to 133% of poverty level (it is optional)
ACA HighlightsNear universal coverage through Medicaid,
Exchanges, Medicare, private health insurance
Eliminates preexisting condition for coverage and continuation
Eliminates ending coverage for honest errors on application
Extends dependent coverage to age 27
Clinical trials coverage
Small employer tax credits
More ACA HighlightsGrants available to states: (1) to set up an Office of Health
Insurance Consumer Assistance (2) to establish health insurance exchanges. TX applied and will get both!
Begins new $11 billion investment in Community Health Centers.
New funding for training primary care docs, nurses, other professionals.
No copays on preventive servicesMinimum and essential benefitsMedicaid payments to doctors must be equal to Medicare
Limits excessive profits by insurers
28
2010: Closing the Rx “Doughnut Hole”: Shrinks Doughnut Hole by $250 in 2010 (rebate), 50% discount on brand-name drugs in the remaining gap; closes doughnut hole entirely by 2020
Jan. 2011: New preventive benefits: adds comprehensive annual check-up plus other prevention benefits, with no out-of-pocket costs.
Adds 12 more years to Medicare Trust Fund Solvency: Not by cutting current Medicare benefits or doctor fees, but slowing growth in Medicare spending from 2010 to 2019.
New Access to Community-Based Services and Supports: Medicare today does not cover community-based services to help seniors remain in their homes. A new voluntary insurance program (CLASS) will provide community-based assistance services and support. Starts in 2012 or 2013; 5 years to qualify for benefits.
The “cuts” are largely limits on insurer profits in ACA whereas cuts in the “Ryan Budget” are real cuts to benefits and payments
.
Making Medicare Stronger
29
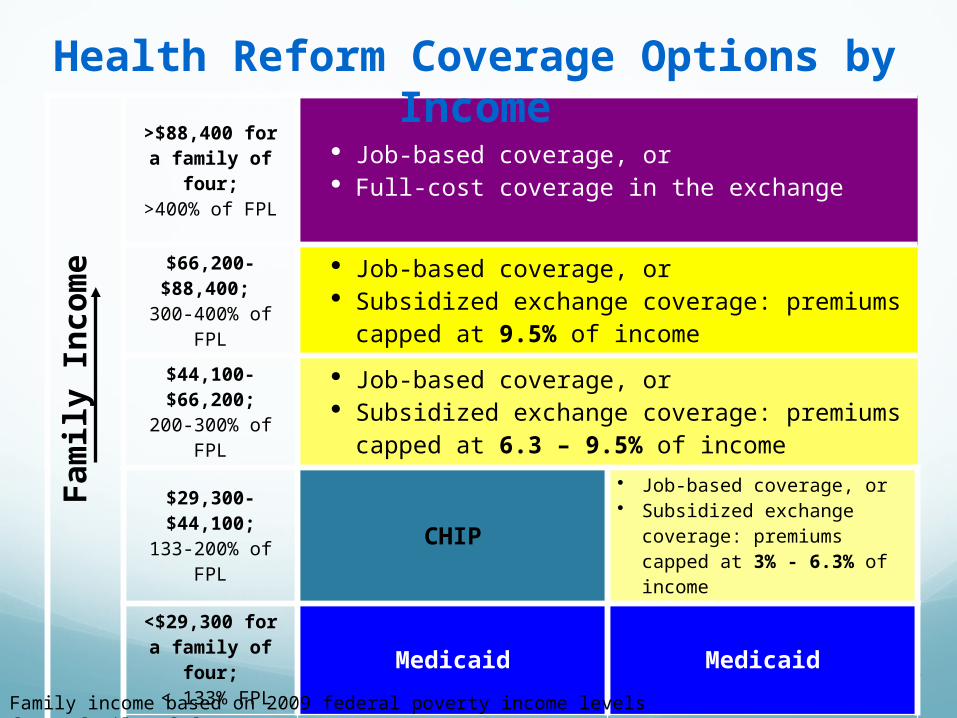
>$88,400 for a family of four;>400% of FPL
Job-based coverage, or Full-cost coverage in the exchange
$66,200-$88,400; 300-400% of FPL
Job-based coverage, or Subsidized exchange coverage: premiums capped
at 9.5% of income
$44,100-$66,200;200-300% of FPL
Job-based coverage, or Subsidized exchange coverage: premiums capped
at 6.3 – 9.5% of income
$29,300-$44,100;133-200% of FPL CHIP
• Job-based coverage, or• Subsidized exchange coverage:
premiums capped at 3% - 6.3% of income
<$29,300 for a family of four; < 133% FPL
Medicaid Medicaid
Children Adults (non-disabled adults,
not eligible for Medicare)
Fam
ily
Inco
me
Health Reform Coverage Options by Income
Family income based on 2009 federal poverty income levels for a family of four
Medicaid and Faith
Tikkun Olam(Healing the World)
Jewish theologic concept dating to early Rabbinic Period
Maimonides expanded to society as a whole
Luria expounded the concept most clearly as part of the mystic tradition (Kabbalah)
Jewish tradition celebrates and honors our obligations to the community
Maimonides – Hierarchy of charitable acts
Seventh Noachite commandment links Jewish tradition to social justice
Christian and MoslemJesus ministry to the poor
Islam – Zakah – clearly linked to social justice