Embed Size (px)
DESCRIPTION
The Winter 2016 edition of the quarterly magazine of the Texas Academy of Family Physicians.
Citation preview
Presorted StandardU.S. Postage
PAID Austin, TXPermit No. 1450
TEXAS FAMILY PHYSICIANVOL. 67 NO. 1 WINTER 2016
PLUS:What You Need To KnowAbout Medicare’s New Merit-Based Incentive Payment System And Alternative Payment Models
Report, Photos From Annual Session & Primary Care Summit
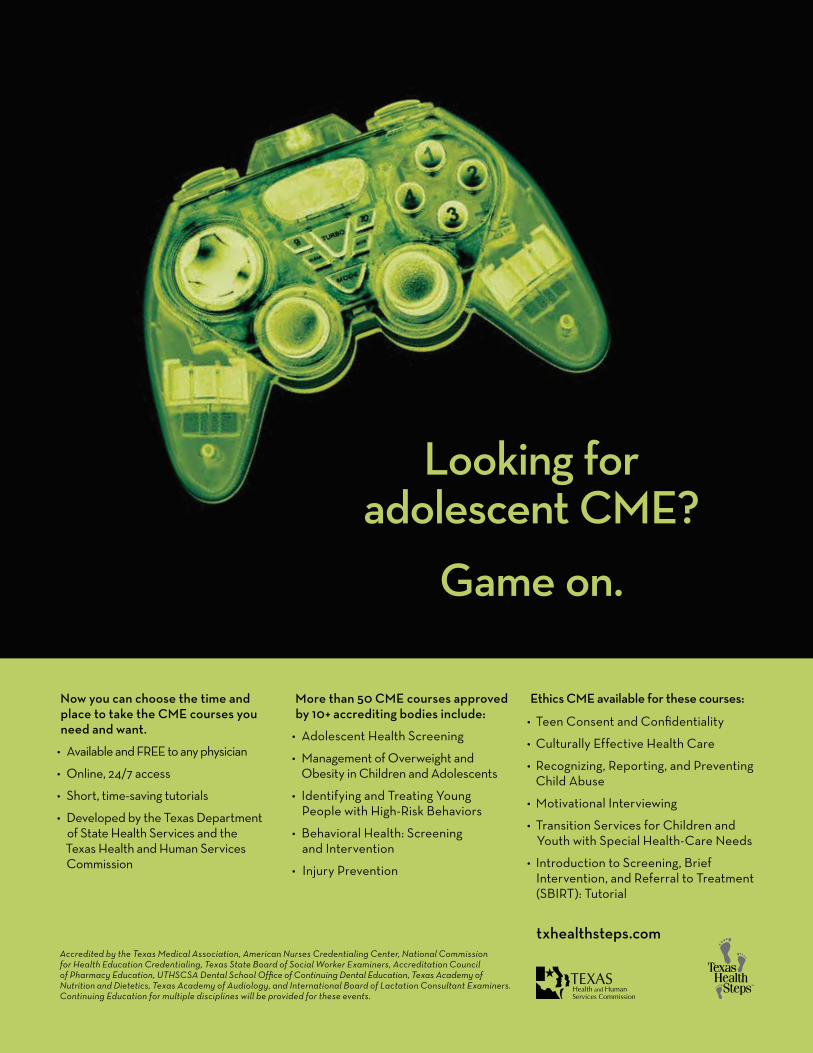
Texas Family Physician Of The Year ANTONIO FALCON, MD
Accredited by the Texas Medical Association, American Nurses Credentialing Center, National Commission for Health Education Credentialing, Texas State Board of Social Worker Examiners, Accreditation Council of Pharmacy Education, UTHSCSA Dental School Office of Continuing Dental Education, Texas Academy of Nutrition and Dietetics, Texas Academy of Audiology, and International Board of Lactation Consultant Examiners. Continuing Education for multiple disciplines will be provided for these events.
txhealthsteps.com
Now you can choose the time and place to take the CME courses you need and want.
• AvailableandFREEtoanyphysician
• Online,24/7access
• Short,time-savingtutorials
• DevelopedbytheTexasDepartmentofStateHealthServicesandtheTexasHealthandHumanServicesCommission
More than 50 CME courses approved by 10+ accrediting bodies include:
• AdolescentHealthScreening
• ManagementofOverweightandObesityinChildrenandAdolescents
• IdentifyingandTreatingYoungPeoplewithHigh-RiskBehaviors
• BehavioralHealth:ScreeningandIntervention
• InjuryPrevention
Ethics CME available for these courses:
• TeenConsentandConfidentiality
• CulturallyEffectiveHealthCare
• Recognizing,Reporting,andPreventingChildAbuse
• MotivationalInterviewing
• TransitionServicesforChildrenandYouthwithSpecialHealth-CareNeeds
• IntroductiontoScreening,BriefIntervention,andReferraltoTreatment(SBIRT):Tutorial
Looking for adolescent CME?
Game on.
INSI
DE
16
TEXAS FAMILY PHYSICIANVOL. 67 NO. 1 2016
16 The richest man in the worldMeet the 2015-2016 Texas Family Physician of the Year: Antonio Falcon, MD. Born and bred in Rio Grande City,
Falcon knew he wanted to return to the small town to practice family medicine after finishing residency. He saw the need there for more physicians and wanted to help. He has been in the border town ever since, growing a bustling practice and raising a family.By Samantha White
14 MEMBER NEWSAnnual Session highlights and photos| In memoriam: Glen Journeay, MD, PhD
27 HHSC NEWSNew tool makes finding Medicaid patient records easy.
30 FOUNDATION FOCUSThanks to 2015 TAFP Foundation donors.
30 TAFP PERSPECTIVESkipping the negative and accepting the maybe
22 After the SGR: Alternative payment modelsWith the sustainable growth rate gone, now is the time to
familiarize yourself with what the Centers for Medicare and Medicaid Services are bringing online next.By Jim Walton, DO, MBA
24 MACRA FAQAAFP’s practice management experts present another excel-
lent resource. Here’s what you need to know about the new payment models in the Medicare Access and CHIP Reauthorization Act of 2015.By AAFP Staff
6 FROM YOUR PRESIDENT An adaptation of the 2015-2016 incoming president’s address
8 NEWS FROM AAFPThe end of Medicare bonuses for primary care underlines the need for new payment models.
SAM
AN
TH
A W
HIT
E

69957 AD TAFP.indd 2 12/9/15 12:31 PM
6 TEXAS FAMILY PHYSICIAN WINTER 2016
greetings colleagues. I am humbled and honored to serve as president of this extraor-dinary Academy and I want to thank all of those leaders and physicians who have men-tored me and guided me along the way as well as my wonderful family for their stead-fast support.
I became involved in the Texas Academy in my second year of prac-tice because it equipped me with the tools to make my practice better. As you know, TAFP provides some of the best CME available and is produced for family physicians by family phy-sicians. The Academy has helped me maintain board certification, which as you all are aware is an important process and not easy to do. The Academy also provides a range of practice support services to help my practice be more efficient. At our statewide meetings I get the chance to network with other family physicians to hear about the latest trends in health care delivery and payment—what’s working and what’s not working.
But perhaps most impor-tantly, the Academy gives us the opportunity to do things collectively that we can’t do individually—whether it is to support a medical student interested in becoming a family physician or to influence public policy decisions. The Academy gives us a voice.
So, what do we want to say and how should we go about saying it? It’s through our involvement that our message is shaped, that our ideas are generated, and our Acad-emy is strengthened. By joining commit-tees and commissions, attending section meetings, coming to CME conferences and
meeting your colleagues, we both get what we need from our association and we enable our association to provide ever greater sup-port for our specialty.
That’s what membership is all about, and so I encourage you to get involved and to stay involved. If you’re already involved—thank you, keep it up, we need you. If you are sitting
on the sidelines and waiting for the right moment, now is the time to suit up.
Let me give you a recent personal example of why it is so important to be involved and how TAFP helped me.
Over the last year I’ve spent a good deal of time learning about alternative payment models—account-able care organizations or ACOs, in particular. After much thought and consider-ation, our practice decided to join two ACOs in our city—a hospital-directed ACO and a physician-led ACO.
I was asked to serve on the board of the hospital ACO, while my partner joined a committee on the other one.
Now let me give you a little background on our hospital ACO. Their board is comprised of five physicians, two of whom are primary
care doctors and I’m the only family physician.So I probably don’t need to tell you how the
conversation went when we began discuss-ing how money should be distributed when it came to things like shared savings. I think the last four decades of payment in the health care industry provide a pretty good guide.
But quite to my surprise, after getting some advice from TAFP staff and coaching from a couple of past TAFP leaders, I was able to make a compelling argument to the board and my specialist colleagues that pri-
PRESIDENT’S COLUMN
TEXAS FAMILY PHYSICIANVOL. 67 NO. 1 WINTER 2016
The Texas Academy of Family Physicians is the premier membership organization dedicated to uniting the family doctors of Texas through advocacy, education, and member services, and empowering them to provide a medical home for patients of all ages. TEXAS FAMILY PHYSICIAN is published quarterly by TAFP at 12012 Technology Blvd., Ste. 200, Austin, Texas 78727. Contact TFP at (512) 329-8666 or [email protected].
OFFICERS
president Ajay Gupta, MD
president-elect Tricia Elliott, MD
vice president Javier “Jake” Margo, MD
treasurer Janet Hurley, MD
parliamentarian Rebecca Hart, MD
immediate past president Dale Ragle, MD
EDITORIAL STAFF
managing editor Jonathan L. Nelson
associate editor Samantha White
chief executive officer and executive vice president Tom Banning
chief operating officer Kathy McCarthy, CAE
advertising sales associate Michael Conwell
CONTRIBUTING EDITORS
Janet Hurley, MDJim Walton, DO, MBA
Robert Wergin, MD
cover photograph Samantha White
SUBSCRIPTIONSTo subscribe to TEXAS FAMILY PHYSICIAN, write to TAFP Department of Communications, 12012 Technol-ogy Blvd., Ste. 200, Austin, Texas 78727. Subscriptions are $20 per year.
Articles published in TEXAS FAMILY PHYSICIAN represent the opinions of the authors and do not neces-sarily reflect the policy or views of the Texas Academy of Family Physicians. The editors reserve the right to review and to accept or reject commentary and adver-tising deemed inappropriate. Publica tion of an adver-tisement is not to be considered an endorsement by the Texas Academy of Family Physicians of the product or service involved. TEXAS FAMILY PHYSICIAN is printed by AIM Printing and Marketing, Austin, Texas.
LEGISLATIVE ADVERTISING Articles in TEXAS FAMILY PHYSICIAN that mention TAFP’s position on state legislation are defined as “legislative advertising,” according to Texas Govt. Code Ann. §305.027. The person who contracts with the printer to publish the legislative advertising is Tom Banning, CEO, TAFP, 12012 Technology Blvd., Ste. 200, Austin, Texas 78727.
© 2016 Texas Academy of Family Physicians
POSTMASTER Send address changes to TEXAS FAMILY PHYSICIAN, 12012 Technology Blvd., Ste. 200, Austin, TX 78727.
Our membership in TAFP gives us the opportunity
to do things collectively that
we can’t do individually—whether it is to
support a medical student interested
in becoming a family physician or to influence public policy
decisions. The Academy gives us
a voice.
Strength in numbersAn adaptation of the 2015-2016 incoming president’s address
By Ajay Gupta, MDTAFP President
www.tafp.org 7
Your Full Turnkey Partner for Chronic Care Management
Your Practice is Already Doing the Work With New CPT 99490
Now Get Paid for it!
23501 Cinco Ranch Blvd., Ste H120#130, Katy, TX 77494 www.medi-code.com 832-437-2029 email: [email protected]
EMERGENCY MEDICINE OPPORTUNITY AVAILABLE NOWSTEPHENVILLE, TEXAS
Emergency Medicine, Family Practice, or Internal Medicine Trained/Boarded Physicians
• 98-bed acute care, level IV trauma center • New 12-bed ED set within 9,500 square feet• 18,000 annual ED patient visits • Two, 12-hour physician shifts • Scribe coverage 7 days a week • EPIC – electronic health record • Independent contractor status with excellent
fee-for-service compensation
Located 70 miles southwest of downtown Fort Worth, Stephenville is a steadily growing, diversified community and also home to Tarleton State University. As a part of the Texas Health Resources System, you will have access to the expertise and specialty services of varying medical specialties.
• Stephenville
Contact me today for more information.
Crystal Mundine(817) 507-1786 [email protected]
Loan repayment option available
mary care needed to be fairly and appropri-ately compensated in any shared savings.
As you can imagine things got a little tense. I was even asked at one point what would happen if specialists did not join the ACO. I retorted that primary care was doing the majority of the work to earn any shared savings, so what would happen if there were no primary care physicians to create the savings for everyone to share?
In the final accounting, my voice was heard and the outcome was much more favorable then it would have been had I not been involved in our Academy and had I not had the resources and counsel TAFP provided me.
Our collective voice was also heard when the U.S. Congress finally repealed the Medicare SGR. Our work, however, is not done. Starting in 2019, Medicare will insti-tute two bonus payment tracks for physi-cians: a Merit-Based Incentive Payment System that consolidates existing Medicare fee-for-service physician incentive pro-grams and a separate pathway to reward physicians for participating in alternative payment models, including ACOs and the patient-centered medical home.
Our members need to be preparing now to choose a pathway or face penalties. Your Academy will be launching an aggressive education campaign, developing CME, webi-nars, and other resources to help its members make the best decision for their practice.
Now is not the time to rest on our lau-rels. We need to continue to remind every-one that family medicine is the best hope to mend our broken health care system. We provide the best value out there, the most comprehensive care. The essence of our specialty is the key to fixing the system. We are compassionate. We treat the whole patient. It is who we are.
Get involved in the Academy. Continue to make a difference with your patients, your community, and the health care system. Don’t let others decide what is best for family medicine and our patients.
I appreciate the opportunity to serve as president of the Texas Academy of Family Physicians. I will provide all my effort to serve our state and national health care system. It will take all of us working together to improve health care in America. I’m excited to lead the path into a new chapter.
8 TEXAS FAMILY PHYSICIAN WINTER 2016
C. Frank Webber Lectureship & Interim SessionApril 15-16, 2016Omni Austin Hotel at Southpark Austin, Texas
Texas Family Medicine SymposiumJune 3-5, 2016La Cantera Hill Country ResortSan Antonio, Texas
Annual Session and Primary Care SummitNov. 4-6, 2016Nov. 2-3: Business meetings and preconference workshops
The Westin Galleria Dallas, Texas
TAFP2016
CME SCHEDULE
AAFP NEWS
more than just the calendar year ended on Dec. 31. The new year also marked the end of the Primary Care Incentive Program.
The PCIP, created in 2010 as part of the Patient Protection and Affordable Care Act, pays family physicians and other primary care providers bonuses equal to 10 percent of the amount Medicare paid them for primary care services if they met certain conditions. This bonus was an overdue step toward recognizing the value of primary care.
The program paid $664 million to primary care practices in 2012, but how much it will be missed depends somewhat on whom you ask. A survey of primary care physi-cians found that half were unaware of the program’s existence. Some physicians
“boutique” their practices, limiting their number of Medicare patients. But many practices in rural and underserved areas can’t do this, and they benefited greatly from the bonus pay-ments. Practices with large Medicare panels certainly will feel the hit. Qualifying primary care physicians received an average of nearly $4,000 a year.
Although the AAFP and other primary care advocates fought for an extension of the program, Congress showed little inter-est in prolonging a bonus program based on the fee-for-service model. As we have seen in the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA)—the law passed earlier this year that repealed the flawed Medicare sustainable growth rate formula—legislators are more interested in linking increased physician payments to certain quality and perfor-mance standards.
If you haven’t already, I strongly encour-age you to start making yourself familiar with the alternative payment models and the merit-based incentive payment system, or MIPS, described in the new law. By 2019,
all physicians participating in Medicare will fall into one category or the other.
MIPS, while attempting to promote quality and added value, still is based on fee-for-service. And as we have seen, that model continues to be a popular target for spending cuts. A multi-year federal budget agreement led to a 2 percent cut to Medicare payments in 2013 and further incremental reductions for several years,
and Congress allowed the Medicaid parity program—a provision of the ACA that raised Medicaid physician payments in line with Medicare—to expire in December 2014.
The 2016 physician fee schedule called for a modest 0.5 percent increase in the physician payment conver-sion rate. However, other legal mandates made even that minimal increase too tall a task for CMS because it failed to identify and adjust a required percentage of overvalued CPT codes. As a result, the Medicare physi-cian fee schedule will see a
fractional decrease in the conversion factor in 2016, rather than a half-percent increase.
What it boils down to is that alternative payment models are the path forward that will provide stability and give our practices the greatest opportunity to thrive. One-third of family physicians already are pursu-ing value-based payments.
The AAFP recently submitted detailed responses to 126 questions as part of a CMS request for information on how to imple-ment new payment models associated with MACRA. Early in 2016, the Academy will be rolling out materials that will help family physicians better understand the choices, deadlines and challenges that MACRA pres-ents. Stay tuned.
Robert Wergin, MD, is Board Chair of the AAFP.
Source: AAFP Leader Voices Blog, Dec. 23, 2015. © American Academy of Family Physicians.
End of Medicare bonuses underlines need for new payment models
By Robert Wergin, MD
What it boils down to is that
alternative payment models
are the path forward that will provide
stability and give our practices the greatest
opportunity to thrive.
CDC recommendation:Test everyone born from
1945-1965 for Hepatitis C
People born from 1945-1965 account for 3 out of every 4 people with
Hepatitis C, and more are unaware of their infection.
l Testing only patients with elevated ALT’s may miss 50% of infection
l Hepatitis C is a leading cause of liver cancer and liver transplants
l Care and treatment can help prevent Hepatitis C-related disease and deaths
hep c ads final 7.5 X 4.75.indd 1 12/17/14 6:18 PM
When you need it in Texas.
ProAssurance.com
Medical professional liability insurance specialists providing a single-source solution in Texas
10 TEXAS FAMILY PHYSICIAN WINTER 2016
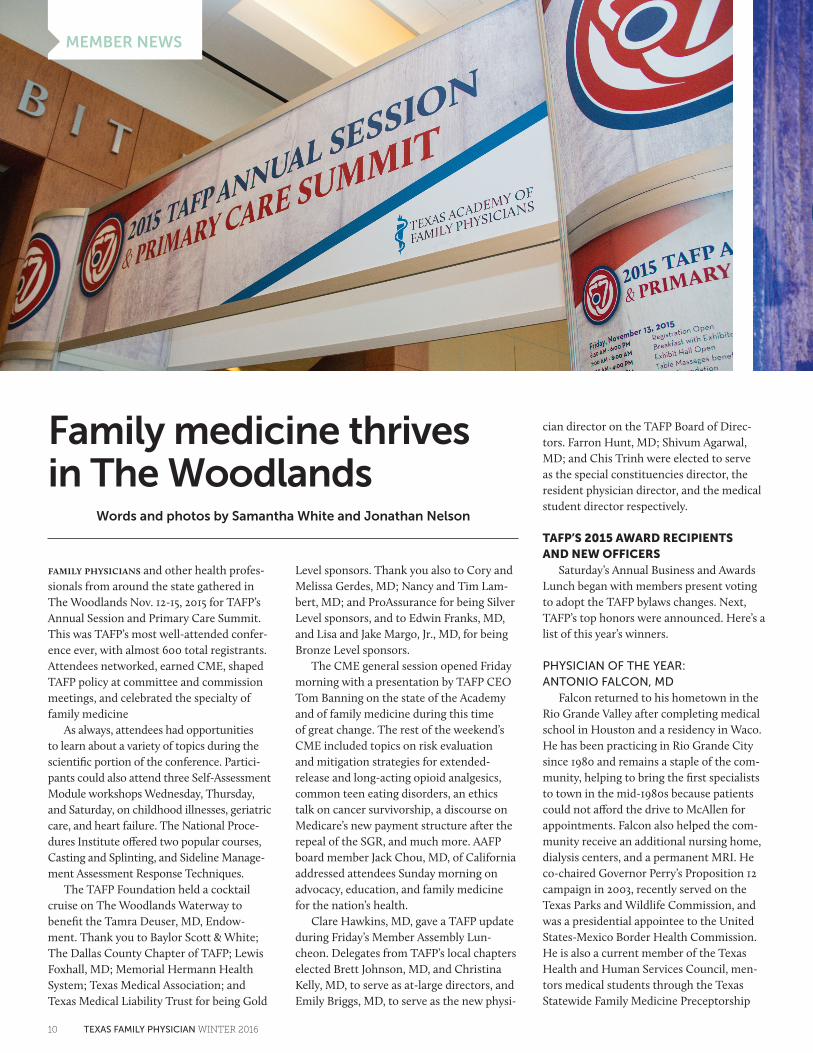
Family medicine thrives in The Woodlands
Words and photos by Samantha White and Jonathan Nelson
family physicians and other health profes-sionals from around the state gathered in The Woodlands Nov. 12-15, 2015 for TAFP’s Annual Session and Primary Care Summit. This was TAFP’s most well-attended confer-ence ever, with almost 600 total registrants. Attendees networked, earned CME, shaped TAFP policy at committee and commission meetings, and celebrated the specialty of family medicine
As always, attendees had opportunities to learn about a variety of topics during the scientific portion of the conference. Partici-pants could also attend three Self-Assessment Module workshops Wednesday, Thursday, and Saturday, on childhood illnesses, geriatric care, and heart failure. The National Proce-dures Institute offered two popular courses, Casting and Splinting, and Sideline Manage-ment Assessment Response Techniques.
The TAFP Foundation held a cocktail cruise on The Woodlands Waterway to benefit the Tamra Deuser, MD, Endow-ment. Thank you to Baylor Scott & White; The Dallas County Chapter of TAFP; Lewis Foxhall, MD; Memorial Hermann Health System; Texas Medical Association; and Texas Medical Liability Trust for being Gold
Level sponsors. Thank you also to Cory and Melissa Gerdes, MD; Nancy and Tim Lam-bert, MD; and ProAssurance for being Silver Level sponsors, and to Edwin Franks, MD, and Lisa and Jake Margo, Jr., MD, for being Bronze Level sponsors.
The CME general session opened Friday morning with a presentation by TAFP CEO Tom Banning on the state of the Academy and of family medicine during this time of great change. The rest of the weekend’s CME included topics on risk evaluation and mitigation strategies for extended-release and long-acting opioid analgesics, common teen eating disorders, an ethics talk on cancer survivorship, a discourse on Medicare’s new payment structure after the repeal of the SGR, and much more. AAFP board member Jack Chou, MD, of California addressed attendees Sunday morning on advocacy, education, and family medicine for the nation’s health.
Clare Hawkins, MD, gave a TAFP update during Friday’s Member Assembly Lun-cheon. Delegates from TAFP’s local chapters elected Brett Johnson, MD, and Christina Kelly, MD, to serve as at-large directors, and Emily Briggs, MD, to serve as the new physi-
cian director on the TAFP Board of Direc-tors. Farron Hunt, MD; Shivum Agarwal, MD; and Chis Trinh were elected to serve as the special constituencies director, the resident physician director, and the medical student director respectively.
TAFP’S 2015 AWARD RECIPIENTS AND NEW OFFICERS
Saturday’s Annual Business and Awards Lunch began with members present voting to adopt the TAFP bylaws changes. Next, TAFP’s top honors were announced. Here’s a list of this year’s winners.
PHYSICIAN OF THE YEAR: ANTONIO FALCON, MD
Falcon returned to his hometown in the Rio Grande Valley after completing medical school in Houston and a residency in Waco. He has been practicing in Rio Grande City since 1980 and remains a staple of the com-munity, helping to bring the first specialists to town in the mid-1980s because patients could not afford the drive to McAllen for appointments. Falcon also helped the com-munity receive an additional nursing home, dialysis centers, and a permanent MRI. He co-chaired Governor Perry’s Proposition 12 campaign in 2003, recently served on the Texas Parks and Wildlife Commission, and was a presidential appointee to the United States-Mexico Border Health Commission. He is also a current member of the Texas Health and Human Services Council, men-tors medical students through the Texas Statewide Family Medicine Preceptorship
MEMBER NEWS

www.tafp.org 11
Clockwise from top left
Antonio Falcon, MD, accepts the 2015 Texas Family Physician of the Year Award at Saturday’s Business and Awards Lunch.
Dale Ragle, MD, gives the Physician Emeritus Award to H. David Pope, Jr., MD.
Lloyd Van Winkle, MD, and Mary Nguyen, MD: “Family physician, because freakin’ awesome is not an official job title.”
TAFP Foundation members Justin Bartos, MD, Doug Curran, MD, TAFP COO Kathy McCarthy, and Leah Raye Mabry, MD, serve breakfast to attendees in the exhibit hall.
Program, and serves as a clinical assistant professor for UTMB.
After accepting the award, Falcon gave a little advice to his colleagues. “Always be kind to the patients. It’s just incredible how one act of kindness can be worth more than 10 prescription drugs. Don’t ever forget to tell your patient something nice about them when they are in that office with you. And don’t forget to touch them. Sometimes we forget how important the human touch is.”
Read more on Falcon’s life in this issue’s cover story on page 16.
PHYSICIAN EMERITUS: H. DAVID POPE, JR., MD
After graduating high school second in his class, getting his medical degree from Tulane, an Air Force internship, flight surgeon school, and a residency at a charity hospital, Pope fulfilled his calling and became a practicing
family physician in 1961. Over the years he worked in solo practice, a multi-specialty clinic, a 100-bed Catholic hospital, Christian missions worldwide, as medical director for numerous nursing homes, and more. He was vital in the creation of the Texas A&M Family Medicine Residency program in Bryan, and TAFP’s Brazos Valley Chapter. Pope still travels to the Texas-Mexico border multiple times a year for Christian missions, serves as Physician of the Day during the Texas Legislature every session, and is active in his church and community.
PATIENT ADVOCACY AWARD: BLAIR CUSHING, DO
Cushing completed a public policy rota-tion with TAFP as a medical student during the 84th Texas Legislature, helping develop policy options for legislators to consider involving physician workforce. Her efforts

12 TEXAS FAMILY PHYSICIAN WINTER 2016
resulted in the passage of Senate Bill 18 by Sen. Jane Nelson, R-Flower Mound, which prioritized the creation of new primary care residency positions and funding for the Texas Statewide Primary Care Preceptorship Pro-gram. Cushing graduated from the University of North Texas Health Science Center and is a family medicine resident at Natividad Medical Center in Salinas, California.
PUBLIC HEALTH AWARD:BRIAN SMITH, MD, MPH
Smith served as the Regional Medical Director for the Texas Department of State Health Services Region 11 for 17 years, and for five additional years as the communi-cable disease clinician. In this role, he was responsible for 19 counties in South Texas, dealing with tuberculosis, diabetes, ebola, and other cross-border issues, and provided emergency preparedness for many hurri-canes along the coast. Before joining DSHS, he practiced medicine in South Texas com-munity health centers, with the Cherokees and Choctaws in Oklahoma, and in various countries including Guatemala and Nigeria.
EXEMPLARY VOLUNTEER TEACHING AWARD: ADRIAN BILLINGS, MD, PHD
Billings is a professor for both the UTMB and Texas Tech Permian Basin, and has been a preceptor in the Texas Statewide
Family Medicine Preceptorship Program for many years, precepting about 100 medical students total. He recently became the pro-gram’s director. He also hosts residents in the Big Bend area, working alongside them to demonstrate true rural family medicine. He is known for incorporating the students and residents into every aspect of his prac-tice. His community has seen three former trainees return to the area to practice.
EXEMPLARY TEACHING AWARD:NORA GIMPEL, MD
Gimpel is an assistant professor of family and community medicine and chief of the Community Medicine Division in the Department of Family Medicine at UT Southwestern. She is the director of numer-ous training programs at UT Southwestern including a predoc training program and a postdoc training program in community medicine. Gimpel is also on the advisory board for the Texas Area Health Education Center East DFW Region.
SPECIAL CONSTITUENCY LEADERSHIP AWARD: CHRISTINA KELLY, MD
Kelly has been active in AAFP since her time as a medical student and after moving to Texas in 2011, she immediately got involved with TAFP. After serving the National Con-ference of Special Constituencies as new phy-
sician co-convener, she was elected convener for the newly renamed National Conference of Constituency Leaders. While her time as a new physician is now over, her nominator is sure Kelly will remain a strong, female leader to both TAFP and AAFP.
TAFP FOUNDATION PHILANTHROPIST OF THE YEAR: NANCY AND DR. PATRICK LEUNG
Leung has practiced family medicine in Midland since 1980 where Nancy, a registered nurse, manages their office. They want to attract more medical students to the family medicine, ensuring that the next generation of doctors includes enough family physicians for the population. Earlier this year the Leungs made a generous dona-tion to the TAFP Foundation to fully endow the Patrick Leung, MD, Medical Student Scholarship. It was awarded this summer to a student who had just finished his first year of medical school and participated in a family medicine preceptorship.
TAFP POLITICAL ACTION COMMITTEE AWARD: TROY FIESINGER, MD
Fiesinger is a longtime advocate for family medicine, working hard to develop local rela-tionships with his elected officials. Not only does he serve as a key contact, but he is also regarded as an expert in health policy. He is

www.tafp.org 13
Clockwise from top left
TAFP 2015-2016 officers, left to right: Parliamentarian Rebecca Hart, MD; Treasurer Janet Hurley, MD; Immediate Past President Dale Ragle, MD; President-Elect Tricia Elliott, MD; President Ajay Gupta, MD; and Vice President Javier “Jake” Margo, Jr., MD.
Drs. Justin Bartos, Jack Chou, Rebecca Hart, and T. David Greer enjoy casino night at the President’s Party.
Dale Ragle, MD, presents Christina Kelly, MD, with the Special Constituency Leadership Award.
TAFP members Irvin Sulapas, MD, and Thomas Kim, MD, MPH, network with AAFP board member Jack Chou, MD, and TAFP guest and CME speaker Mike Sevilla, MD.
Attendees gather at Friday night’s student and resident reception.
active with TAFP’s Political Action Commit-tee and currently serves on AAFP’s Commis-sion on Governmental Advocacy.
Following the presentation of awards Chou installed TAFP’s 2015-2016 officers. They are President Ajay Gupta, MD; President-elect Tricia Elliott, MD; Vice President Javier “Jake” Margo, Jr., MD; Treasurer Janet Hurley, MD; and Parliamentarian Rebecca Hart, MD.
In his inaugural address, Gupta thanked the many physician leaders who have gone before him and several mentors who have guided him along his path. He encouraged family physicians to become involved in the Academy for the sake of the specialty as well as their own fulfillment. “I appreci-ate the opportunity to serve as president of
the Texas Academy of Family Physicians,” he told the audience. “I will provide all my effort to serve our state and national health care system. It will take all of us working together to improve health care in America. I’m excited to lead the path into a new chap-ter.” Read an excerpt of his address in this issue’s President’s Column on page 6.
Mark your calendars now for upcom-ing symposia. The 2016 C. Frank Webber Lectureship will be held April 15-16 at the Omni Austin Hotel at Southpark. The Texas Family Medicine Symposium will be June 3-5, 2016 at La Cantera Hill Country Resort and Spa in San Antonio, and next year’s Annual Session and Primary Care Summit will be Nov. 4-6, 2016 at The Westin Galleria Dallas. For the full 2016 schedule, go to www.tafp.org/professional-development.

14 TEXAS FAMILY PHYSICIAN WINTER 2016
SEEKING FAMILY PHYSICIAN
Opportunity waits for a BC/BE Family Practice Physician looking to practice in the Alamo Heights area of San Antonio. When you join this
team, you will be working with a busy Board Certified Orthopedic Surgeon who’s been in private practice for 10 years. Seeking a
competitive, driven individual who wants an opportunity to succeed. Benefits include, but not limited to, competitive salary, health and life insurance, vacation and a retirement plan. Experience in sports
medicine a plus. Bilingual is a plus as well. For more information about our practice, please visit our website www.ossmsa.com. Please
send CV to [email protected].
adv e r t i s ement
JOIN THE COASTAL HEALTH & WELLNESS HEALTHCARE TEAM!
Excellent federally-qualified primary care clinics on the coast in Galveston County seeking PRIMARY CARE PHYSICIANS to join our clinician team serving residents of all ages. Family practice training
and certification preferred. Excellent work hours and benefits. SALARY NEGOTIABLE! Applications and additional information may be found at http://www.gchd.org/hr/job.htm. Or by contacting HR at apply@
gchd.org or (409) 938-2260.HR at [email protected] or (409) 938-2260.
adv e r t i s ement
MEMBER NEWS
tafp past president Glen Journeay, MD, PhD, passed away at the age of 90 after bat-tling pancreatic cancer. Journeay served as TAFP president in 1983-1984 and was a life member. He practiced in Austin for 30 years and taught biomedical engineering at the University of Texas for 35 years.
Journeay earned two undergraduate degrees from Rice University, one while participating in the NROTC V-12 program. He later served on the USS Barnegat AVP-10 and was discharged from active duty in 1946. After receiving a doctorate in chem-istry from UT and working in the research department of Monsanto Chemical in Texas
City, Journeay returned to school to receive his medical degree from the University of Texas Medical Branch at Galveston.
He practiced family medicine in Texas City until the Journeay family home was flooded by Hurricane Carla in 1961, when he returned to Austin and began his prac-tice there.
Journeay married the girl next door, Betty Jo Cooper, in 1948 while earning his PhD from UT. His is survived by his wife and their five children: Carol Journeay, David Journeay, Stephen Journeay, Nancy Jackson, and Janet Slack, as well as twelve grandchildren and eight great-grandchildren.
In memoriam: Glen Journeay, MD, PhD
Supported in part by a grant from the American Academy of Family Physicians Foundation.
more than 3,500 children will try their
first cigarette.
Stop kids from starting.Volunteer to be a
Tar Wars presenter.
Today
www.tarwars.org
TW hlf vert.10_v2.indd 1 9/3/10 11:57 AM
Are you plugged in to your academy?Visit tafp.org and plug in to what your Academy is doing for you!ww
w.ta
fp.o
rg
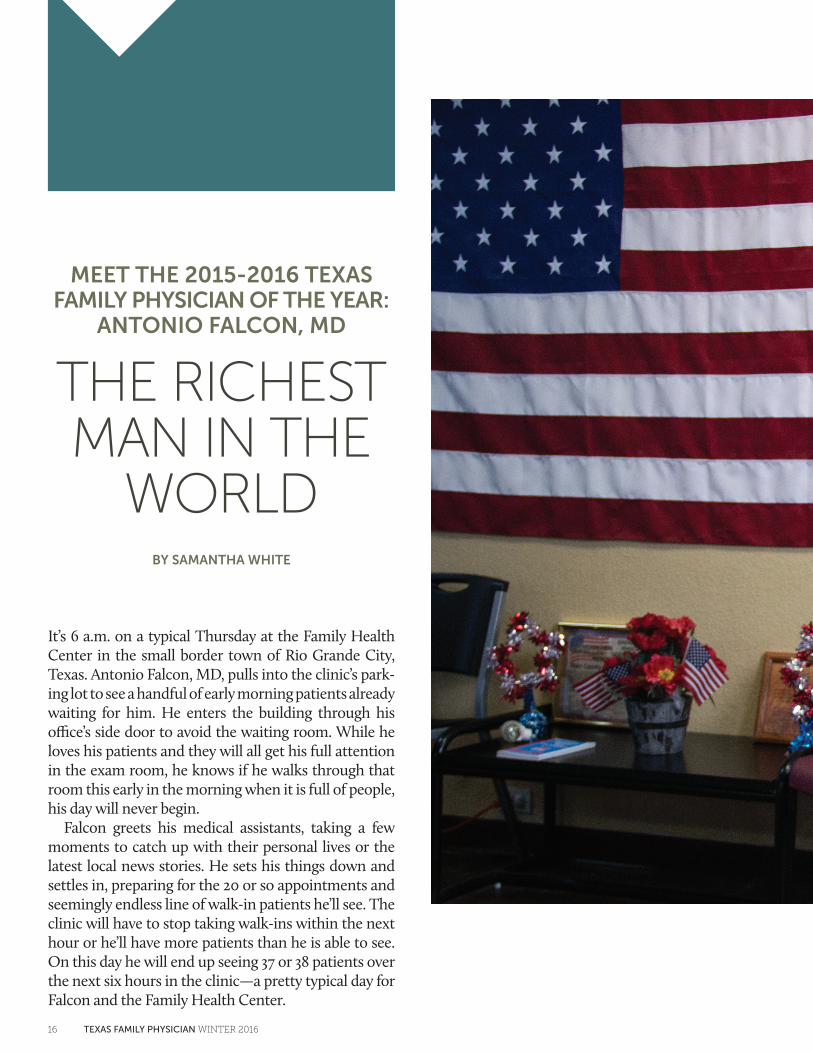
MEET THE 2015-2016 TEXAS FAMILY PHYSICIAN OF THE YEAR:
ANTONIO FALCON, MD
THE RICHEST MAN IN THE
WORLDBY SAMANTHA WHITE
It’s 6 a.m. on a typical Thursday at the Family Health Center in the small border town of Rio Grande City, Texas. Antonio Falcon, MD, pulls into the clinic’s park-ing lot to see a handful of early morning patients already waiting for him. He enters the building through his office’s side door to avoid the waiting room. While he loves his patients and they will all get his full attention in the exam room, he knows if he walks through that room this early in the morning when it is full of people, his day will never begin.
Falcon greets his medical assistants, taking a few moments to catch up with their personal lives or the latest local news stories. He sets his things down and settles in, preparing for the 20 or so appointments and seemingly endless line of walk-in patients he’ll see. The clinic will have to stop taking walk-ins within the next hour or he’ll have more patients than he is able to see. On this day he will end up seeing 37 or 38 patients over the next six hours in the clinic—a pretty typical day for Falcon and the Family Health Center.
16 TEXAS FAMILY PHYSICIAN WINTER 2016

The Family Health Center in Rio Grande City invites patients to bring in photos of loved ones who have previously served
or are currently serving in U.S. military forces as a way to honor community members. The photos line the clinic’s waiting
room walls, alongside a colossal American flag. Falcon has a long line of family members who have served in the armed
forces, including his son who is a brigade surgeon.
www.tafp.org 17
Family medicine isn’t just about filling prescriptions and con-ducting well visits, though family docs spend a lot of time on both. It’s not just delivering babies and diagnosing the common cold, though both happen frequently. It’s more than geriatrics and pediatrics, and it’s more than caring for
multiple generations of one family. “I think the most important thing is not to forget patients have
feelings,” Falcon says. He knows family medicine is so much more than the actual medicine itself.
“Being sensitive to their needs is probably the most critical thing. I don’t think patients ever expect you to have everything right, but I think they expect you to listen.”
Listening to patients and showing them you care is just as vital as prescribing medications, Falcon explains. Touching them, greeting them with a hug or a quick peck on the cheek, smiling—all simple acts of kindness that can go a long way in the exam room he says.
“I’m one of those who feels that touching a patient is very impor-tant. Especially the older individuals. Sometimes nobody ever gives them a hug or tells them they look nice or they smell nice. Sometimes when you’re in that age group of your 70s and 80s, sometimes people forget that you need strokes of kindness, and the family doctor can do that. One act of kindness in the examining room can be worth a ton of medications.”
“I try to compliment my patients as much as possible. Sometimes the little grandmothers that are 90 are never told that their blue hair is cute. It’s okay to do that and they love it! It’s an easy thing to do. It costs you absolutely nothing.”
Other lines of work might frown upon getting to know your patients personally, but Falcon thinks it makes family doctors even better physicians.
“Never giving up hope for the patient is another thing. You can get involved and emotional with your patients. You can hurt when they hurt. I think when you do that they feel closer to you. They have a greater tendency to follow your advice. They’ll listen to your words and if you give encouraging words and words of comfort, you’ve done 99 percent of what a good family doctor will do.”
Falcon, the 2015-2016 Texas Family Physician of the Year, was born in Edinburg and raised in Rio Grande City, where he continues to practice today. He only left his hometown for long enough to attend school and complete his residency.
A long line of Falcon’s family members attended the University of Texas at Austin for their undergraduate education, and Falcon had
plans to do the same. It was just after Vietnam though, and his educa-tor father felt there would be too many distractions in Austin. Falcon instead attended Baylor for his undergraduate degree, Baylor College of Medicine in Houston for his medical degree, then he completed a family medicine residency back in Waco. After his father passed away in 1972, Falcon became the father figure to his three younger brothers.
While in Houston he met a nurse named Kathy, who relocated from Vermont after nursing school. The two married during his second year of residency. We he had completed his residency, the Falcons returned to Rio Grande City in 1980 and he began practicing.
He became a father that same year when Kathy gave birth to their only son, James. Over the next decade, four daughters followed: Sarah, Emily, Kelly, and Patty. Raising their five children is obviously the Fal-cons’ proudest achievement in life. All five are now successful in their respective careers: A brigade surgeon in the U.S. Army, a family physi-cian, a speech pathologist, an attorney, and realtor.
Though his office’s physical location and practice type has changed a few times over the last three and a half decades, he never saw himself leaving his hometown to practice anywhere else.
“I saw the need here,” Falcon says. “I grew up here and saw that the area was desperate for more practitioners. When I came to Starr County it was labeled the poorest county in the country.”
In his acceptance speech at TAFP’s Annual Session and Primary Care Summit, he talked about moving back home to the poverty-stricken Rio Grande Valley to not only practice family medicine, but to raise a family.
“I went to the poorest county in the country and became the richest man,” Falcon said. “I say that because I am absolutely blessed with richness from my family.”
Falcon went on to humbly thank his peers for nomi-nating him for the award and give medical students and residents in the audience some tips on being a family physician.
“Don’t forget that it’s not about the money. It’s about what happens in your heart. It’s about the relationship with your patients.”
Just like many other family physicians across the country, “family doc” isn’t Falcon’s only job title. Falcon served as the local high school’s team physician for mul-tiple decades and served for nine years on the school board. He is an active preceptor in the Texas Statewide
Family Medicine Preceptorship Program. He is a clinical assistant professor for the University of Texas Medical Branch Department of Family Medicine. He served as the emergency medical services direc-tor for Starr County Memorial Hospital for many years. He is active in the Hidalgo-Starr County Medical Society and once served as presi-dent of the TAFP Valley Chapter. He spent many years on the Texas Medical Association’s Foundation Board and TMA’s Political Action Committee.
Falcon is not only a humble, small town physician. He’s also a politically active heavy hitter with strong governmental ties. In 2003, Governor Rick Perry appointed Falcon as co-chair to the Proposition 12 campaign, a tort reform that fought to protect physicians from lawsuits by capping malpractice suit payouts. In 2007, Falcon was appointed by President Bush to the United States-Mexico Border Health Commission where he collaborated with other states and both countries’ federal governments to give recommendations to the Sec-retary of Health and Human Services on border health. More recently, Gov. Perry once again appointed Falcon, this time to the state’s Health and Human Services Council, a duty he is currently fulfilling.
“I went to the poorest county in the country and became the richest man. I say that because I am absolutely blessed with richness from my family.” — Antonio Falcon, MD
18 TEXAS FAMILY PHYSICIAN WINTER 2016

One of Falcon’s favorite professional accomplishments is having served on the Texas Parks and Wildlife Commission for seven years. Whereas the Health and Human Services Council is strictly advisory, the parks commission was given direction from the legislative branch and actually put laws into place. He says seeing how the government works from the inside broadened his outlook on the state of Texas and that he was honored to serve a bigger community in all of these capacities.
“To be in a leadership position where you can make changes, rules, regulations, that affect the everyday life of an individual, is critical. There’s nobody in better positions in small communities than family docs to do that.”
Falcon also stresses the importance of rural physicians specifically being active members of the political landscape to fight for their com-munities.
“Sometimes the family docs are the only people who are going to advocate for patients out in rural areas. The only ones who are really going to understand out in rural areas are the rural practitioners because they live in town. I think it’s absolutely critical that family docs continue to participate and be a voice in state government. It’s important to be heard, to be loud when you have to be loud, and to not be afraid to say what you think.”
Rural medicine has its ups and downs for sure Falcon says, but it is also the only type of medicine he can imagine himself doing.
“There are difficulties in rural medicine. You really have to love it. On the other hand, it’s super rewarding to be involved with the com-munity and to know the community.”
Over the years Falcon saw more and more patients unable to make the drive to McAllen to meet with specialists. They couldn’t afford the gas, couldn’t take the time off work, or didn’t have a car, among other reasons. The sensible solution was to bring the specialists to town, so that’s what he did. On his suggestion, multiple specialists set aside a half day outside of their clinics to travel the 40 miles from McAllen to Rio Grande City and see patients. It started with nephrologists, then expanded to cardiologists, optometrists, and pediatricians. There are also now two dialysis centers, an additional nursing home, and a per-manent MRI in the area, all of which Falcon had a strong hand in.
It’s this type of concern for and action to better the community that makes Falcon a local leader. Audencio Garza has lived next to the Falcons for over 15 years now and says relating to his patients cultur-ally allows Falcon to be the best possible physician.
“If you’re born here, raised here, you know the conditions, you know the people,” Garza says. “The better doctor would be somebody who is locally grown because he or she would know what’s needed for the community.”
Having only left for a handful of years, Falcon was already active in the South Texas community when he returned to practice medi-cine. Many people were already familiar with him, or at least with the Falcon name. The Falcon family has been in the Rio Grande Valley for multiple generations and many Falcons hold notable positions in the area. His brothers alone, now all retired, were the county’s emergency coordinator, a longtime teacher, and a border patrol officer. Everyone in the community knows the Falcon name one way or another.
Falcon celebrates receiving the award with his family at November’s Annual Session and Primary Care Summit.
www.tafp.org 19

Another homegrown local physician, Jake Margo, Jr., MD, is active in TAFP, currently serving as the organization’s vice presi-dent and the Valley Chapter’s president. Margo echoes Falcon’s sentiments on the importance of docs being active community members.
“It’s not enough to be a physi-cian,” Margo says. “You’re looked up to in the community. You are expected to be involved. Your opinion matters, not just when it comes to medical issues, but local politics, schools.”
Seeing a homegrown resident become a family doc like Falcon inspires younger residents. Stella Winters, a third-year resident at the John Peter Smith Family Residency Program, grew up in Rio Grande City and is currently rotating there. She credits Falcon with supporting her pursuit of education to become a physi-cian, by mentoring her as she volunteered at the hospital and financially helping her attend a pre-med conference, both while she was still in high school.
“He’s been very inspirational to the young people, the next generation,” Winters says. “He’s the role-model-type figure saying ‘this is possible, you can do this, somebody from here has done it.’ He’s been very supportive in developing potential for young people here in this small city.”
It’s difficult to find someone in Rio Grande City who doesn’t know and love Falcon. Margo first met Falcon as a kid when he sprained his ankle. He says Falcon has always been casual, making you feel relaxed and like you are part of the Falcon family. His young-est daughter, Patty, says that’s what makes him a good family doctor —his ability to make patients feel so comfortable they feel like a part of his family.
A patient and friend of Falcon, Ivo Perez, had a stroke in 2011 and now comes to the clinic to get his blood pressure checked twice a week, a service Falcon doesn’t charge him for despite its frequency. Perez is grateful to have Falcon as a friend and physician.
“Like they say, you only have friends when you’re in jail, when somebody passes away, and when you’re in the hospital,” Perez says. After the stroke Perez suffered, he says Falcon came to the hospital and checked on him often. “To me he’s a good friend.”
“All his care is patient-oriented and often includes the entire family for the betterment of the patient,” Margo says. “This often includes seeing several family members at once for their conve-
nience. How else could he instill such loyalty in his patients that they would often rather go back home than be seen by someone else in the clinic?”
Rosa Garza has been a medi-cal assistant with Falcon for 11 years. When she was hired she only planned on staying for a year or two before finding another career. She says Falcon is the reason she has stayed in the pro-fession for so long. “I love work-ing with Dr. Falcon so much it’s like, why leave?”
“He’s very down to earth,” Garza says, “and patients can actually talk to him. When I go to the doctor I feel intimidated and scared, but Dr. Falcon is so down to earth. You just feel so much…he’s not even a doctor. He’s just your friend.”
His willingness to listen to patients is a gift from God, Fal-con’s brother Gene says.
“So many of his patients always tell me, ‘after I saw Dr. Falcon I feel so much better.’ I ask them if he gave them medi-cine. ‘No, we just talked,’ they say. ‘After I left, I felt great!’”
Nanette Garcia, another family friend, says Falcon has a way of making you feel good even at your worst times. He helped Garcia through her mother’s stroke and death in 2015, visiting her McAl-len nursing home weekly. He’s a people person, she says.
“People tend to gravitate toward him. He knows how to make everybody feel comfort-able. I don’t think it’s something
he does on purpose, it’s just part of his personality.”Long-time patient Yolanda doesn’t know what she will do if Falcon
ever retires. They grew up together, working in the melon sheds as kids, and she can’t imagine anyone else as her health care provider.
“He has helped me a lot when I couldn’t afford it. I didn’t have insurance or anything, but it didn’t matter to him. He looks after his patients. He knows you, and he hears you.”
It’s now Thursday evening and after spending his afternoon working on paperwork and fielding calls from people asking for medical advice, Falcon is enjoying a dinner out with his wife. They discuss the events of the day and what’s to come in the next few weeks—a visit with his friends from his undergrad days at Baylor, a daughter’s wedding in Austin, and the upcoming birth of their sixth granddaughter. The satisfaction in Falcon’s smile when discussing these family milestones says it all. In this moment, Falcon is the rich-est man in the world.
“To be in a leadership position where you can make changes, rules, regulations, that affect the everyday life of an individual, is critical. There’s nobody in better positions in small communities than family docs to do that.” — Antonio Falcon, MD
Falcon receives the 2015-2016 Texas Family Physician of the
Year Award from TAFP Immediate Past President Dale Ragle,
MD, at TAFP’s Annual Session and Primary Care Summit.
20 TEXAS FAMILY PHYSICIAN WINTER 2016
The Core Content Review of Family Medicine
Why Choose Core Content Review?
• CD and Online Versions available for under $250!
• Cost Effective CME
• For Family Physicians by Family Physicians
• Print Subscription also available
• Discount for AAFP members
• Money back guarantee if you don’t pass the Board exam
• Provides non-dues revenue for your State Chapter
North America’s mostwidely-recognized program for:•Family Medicine CME•ABFM Board Preparation •Self-Evaluation
• Visit www.CoreContent.com • Call 888-343-CORE (2673) • Email [email protected]
22 TEXAS FAMILY PHYSICIAN WINTER 2016
last year the much maligned sustainable growth rate cost control scheme used by The Center for Medicare and Medicaid Services was repealed. If you are like me, you are cel-ebrating this legislative victory, which took too many years to achieve. It is estimated that the cost of repealing SGR would be $150 billion over 10 years, because in the simplest terms, the SGR law attempted to control growth in Medicare costs by reducing the reimbursement rate for each unit of service provided by physicians. But as Joel White, president of the Council for Affordable Health Coverage reports, the SGR resulted in a reflexive increase in the volume of ser-vices as physicians attempted to maintain revenues. Where SGR failed, new strategies, rules, and regulations are now being rolled out for our profession.
As we enter the post-SGR phase of CMS’ attempt to control the burgeoning baby boomers’ impact on the total cost obliga-tions of the federal budget, CMS is launching its new strategy, and we should all become familiar with its new terminology: “alterna-tive payment models.” Through APMs, CMS and Medicare have made a commitment to value-based payments, incentivizing provid-
ers to adopt this model to promote better health outcomes at lower costs.
Some familiar examples of APMs include:
• Accountable care organizations• Capitated and bundled-based
payments• Patient-centered medical homes
We must recognize that in the wake of the SGR repeal, Medicare has accelerated its transition away from fee-for-service as its sole mechanism for reimbursing physicians. To ease the transition for physicians, there is a narrow window of time in which Medi-care will provide standard annual FFS rate increases of half a percent, from July 2015 through 2019. In the APM strategy, which will start in 2019, CMS has committed to rewarding physicians who achieve the transi-tion to quality improvement and cost reduc-tion in an APM contract.
Physicians and their Medicare patients who do not participate in APMs will be cap-tured in a value-based financial reward pro-gram called Merit-based Incentive Payment System. Starting in 2019, the standard FFS rate increases will be replaced by MIPS, rewarding
Jim Walton, DO, MBA, is president and CEO of Genesis Physician Group, and he is president of the Dallas County Medical Society. He is board certified in internal medicine.
This article first appeared as the “President’s Page” in the Oct. 2015 issue of the Dallas Medical Journal.
After the SGR: ALTERNATIVE PAYMENT MODELS
Jim Walton, DO, MBA
10%
5%
0%
-5%
-10%
2019 2020 2021 2022 2023 2024 2025
Reward Penalty
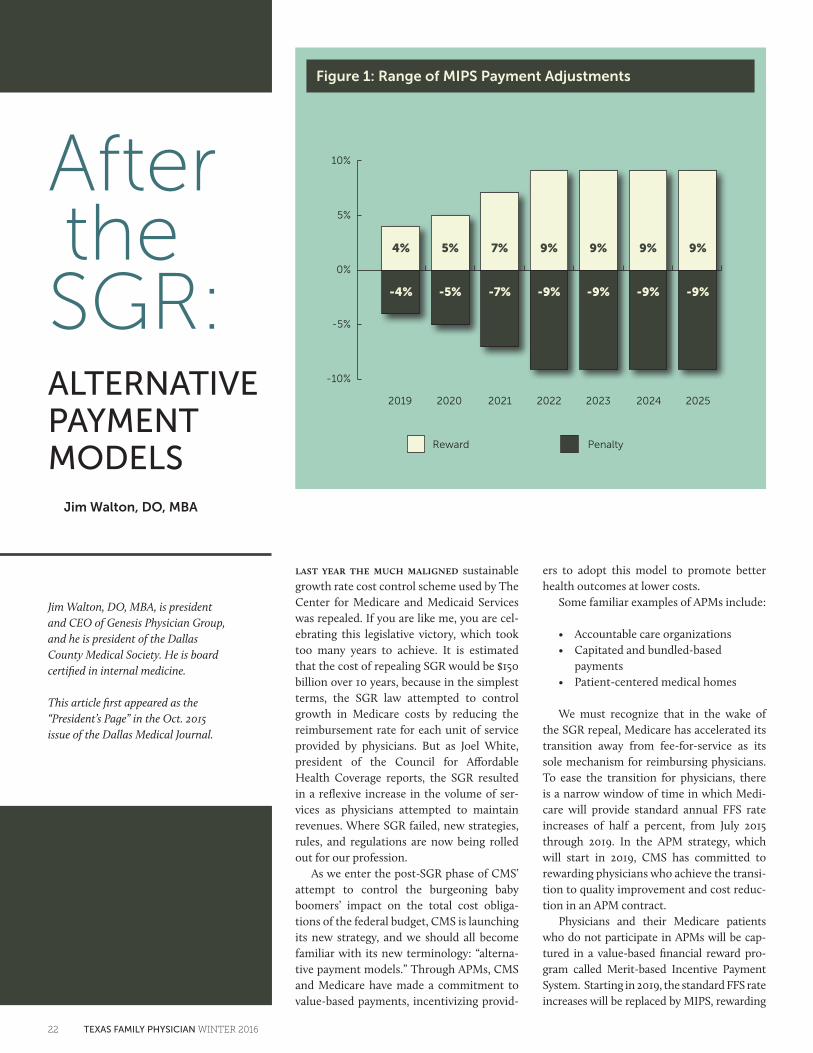
Figure 1: Range of MIPS Payment Adjustments
5%4% 7% 9% 9% 9% 9%
-4% -5% -7% -9% -9% -9% -9%
www.tafp.org 23
physicians based on how they perform on many of the now familiar quality measures outlined in the current quality payment pro-grams. The MIPS will consolidate the follow-ing Medicare quality payment programs:
• Physician Quality Reporting System • Electronic Medical Record Meaning-
ful Use • Value-based Payment Modifier
Figure 1 illustrates the potential financial rewards or penalties for physicians treating Medicare patients beginning in 2019.
As you can see, the range of MIPS-related payment adjustments begin at 4 percent in FY-19 and peaks at 9 percent a short four years later. The MIPS program differs from current PQRS and MU incentives that are “all or nothing.” The MIPS program also rewards those with exceptional performance (top quartile) with separate bonuses.
Important exceptions are:
• Physicians may opt out of the MIPS-related payment adjustments if they choose to be engaged in the APM programs noted above.
• Physicians choosing to participate in APMs and receive a substantial share of Medicare revenues through an APM will receive FFS bonus payments of 5 percent annually for six years.
• Physicians participating in APMs may also be eligible for shared savings bonuses (typically paid six months after the end of the calendar year).
In the immediate future, physicians will be weighing the decision to become more engaged in APMs. It is also fairly certain that commercial insurers will be following the same basic formula to control costs. With all this change where should we look for good news?
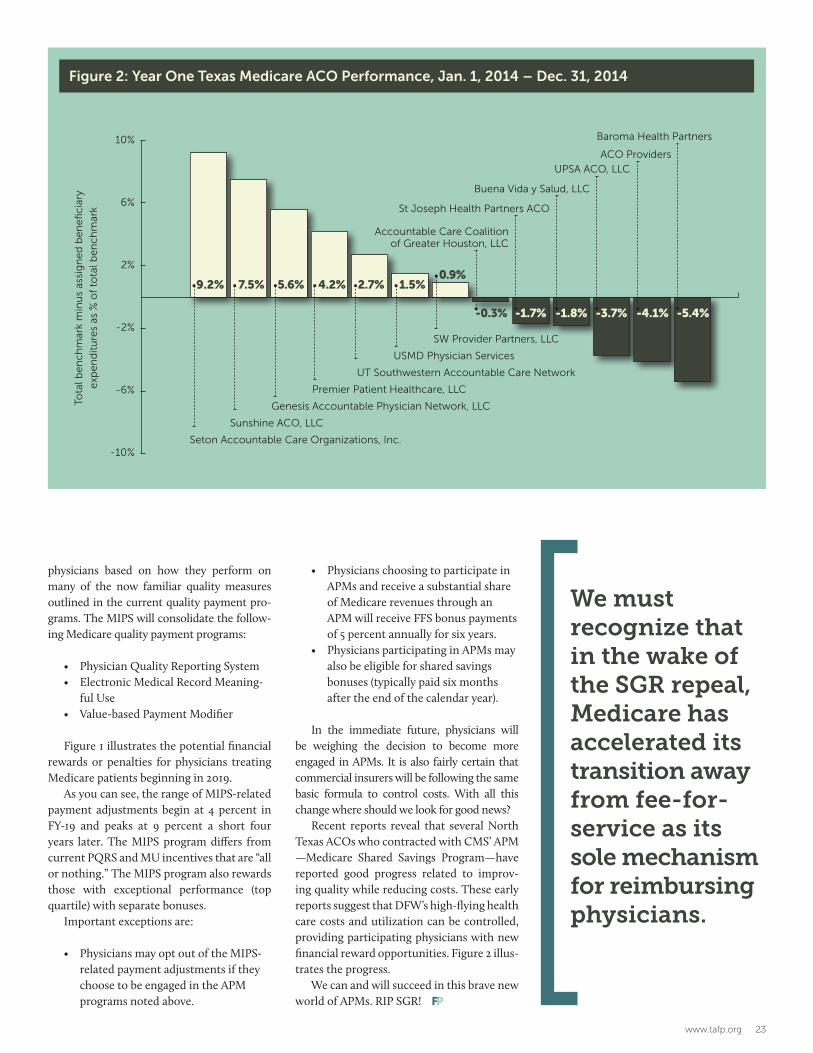
Recent reports reveal that several North Texas ACOs who contracted with CMS’ APM —Medicare Shared Savings Program—have reported good progress related to improv-ing quality while reducing costs. These early reports suggest that DFW’s high-flying health care costs and utilization can be controlled, providing participating physicians with new financial reward opportunities. Figure 2 illus-trates the progress.
We can and will succeed in this brave new world of APMs. RIP SGR!
We must recognize that in the wake of the SGR repeal, Medicare has accelerated its transition away from fee-for-service as its sole mechanism for reimbursing physicians.
10%
6%
2%
-2%
-6%
-10%
Figure 2: Year One Texas Medicare ACO Performance, Jan. 1, 2014 – Dec. 31, 2014
9.2% 7.5% 5.6% 4.2% 2.7% 1.5%0.9%
Tota
l be
nc
hm
ark
min
us
assi
gn
ed
be
ne
fic
iary
exp
en
dit
ure
s as
% o
f to
tal b
en
ch
mar
k
-0.3% -1.7% -1.8% -3.7% -4.1% -5.4%
Seton Accountable Care Organizations, Inc.
Sunshine ACO, LLC
Genesis Accountable Physician Network, LLC
Premier Patient Healthcare, LLC
UT Southwestern Accountable Care Network
USMD Physician Services
SW Provider Partners, LLC
Baroma Health Partners
ACO Providers
UPSA ACO, LLC
Buena Vida y Salud, LLC
St Joseph Health Partners ACO
Accountable Care Coalition of Greater Houston, LLC
24 TEXAS FAMILY PHYSICIAN WINTER 2016
1 How does the Medicare Access and
CHIP Reauthori-zation Act of 2015 impact my Medi-care payments?
This law repeals the flawed Medicare
sustainable growth rate formula that
calculated payment cuts for physicians.
MACRA establishes an alternative set of
predictable annual baseline payment
updates and two payment tracks: the
Alternative Payment Model track and
the Merit-Based Incentive Payment
System track.
The following is a timeline for MACRA
implementation:
July 2015 through December 2015: Medicare physician payments
increase by 0.5 percent.
2016 through 2019: Medicare physi-
cian payments increase by 0.5
percent each year.
January 2019: Based on eligibility, phy-
sicians enter either the APM track or
the MIPS track.
2020 through 2025: Medicare physician
fee-for-service payments remain at
2019 levels with no updates.
2 What is an alternative payment
model?
MACRA defines any of the following as
an alternative payment model:
• An innovative payment model
expanded under the Center for Medi-
care & Medicaid Innovation, including
Comprehensive Primary Care initia-
tive participants but not Health Care
Innovation Award recipients
• A Medicare Shared Savings Program
accountable care organization
• Medicare Health Care Quality Dem-
onstration Program or Medicare
Acute Care Episode Demonstration
Program, or another demonstration
program required by federal law
3 Does MACRA specify additional
qualifying criteria for APMs?
Yes. An APM must require participants
to meet all of the following criteria:
• Uses quality measures comparable
to measures under the MIPS
• Uses certified electronic health
record technology
• Bears more than nominal financial
risk or is a medical home expanded
under the CMMI
• Has increasing percentage of
payments linked to value through
Medicare or all-payer APMs
4The Com-prehensive Primary
Care initiative is an APM option for practices of all sizes. What are the expectations of that program?
The aim of the CPC initiative is to
strengthen primary care in order to
support better care, lower costs, and
improved population health. Through
collaboration between the Centers for
Medicare & Medicaid Services and com-
mercial and state health insurance plans,
participating primary care practices in
seven U.S. regions receive population-
based care management fees and
shared savings opportunities. In return
for this financial support, each practice
is expected to provide a core set of five
“comprehensive” primary care functions:
• Access and continuity
• Planned care for chronic conditions
and preventive care
• Risk-stratified care management
• Patient and caregiver engagement
• Coordination of care across the
medical neighborhoodFreq
uen
tly
Ask
ed Q
ues
tio
ns:
Med
icar
e A
cces
s an
d C
HIP
Rea
uth
ori
zati
on
Act
of 2
015
MACRA FAQP
RA
CT
ICE
MA
NA
GE
ME
NT
www.tafp.org 25
Is your practice managing you, or are you managing your practice?
Reiner Consulting & AssociatesPractice ManageMent ServiceS
Bradley reiner, Bareiner consulting & associates
212 covered Wagon Way, Driftwood, texas 78619
p (512) 858-1570 | m (512) 413-5678 | f (512) 858-1580 fax
www.bkrconsulting.org
Specializing in:• Practice assessments• Billing and coding audits• Documentation reviews• Managed care contract negotiation• recruitment• interim Management• Personnel and Work Flow issues• new Practice Set-ups
Payer audits are at an all-time high. Have us review and validate that your records are consistent with cMS and commercial coding requirements. Let us educate and protect you from potential refunds and overpayments.
Exclusive discount for TAFP members!
5How would I be paid under an APM?
If you are eligible and choose to par-
ticipate in a qualifying APM, you will
receive a 5 percent lump-sum bonus
on your Medicare payments for 2019
through 2024. Beginning in 2026, you
will qualify for a 0.75 percent increase
in your payments each year.
6What is the Merit-Based Incentive
Payment System?
The Merit-Based Incentive Pay-
ment System is a new program in the
Medicare fee-for-service payment
system. It consolidates three existing
programs—Meaningful Use, the Physi-
cian Quality Reporting System, and the
Value-Based Payment Modifier—into a
single program.
The MIPS will assess individual physi-
cian performance in four categories to
generate a composite score on a 0- to
100-point scale. The categories are:
• Quality
• Resource use
• Meaningful use of certified EHR
technology
• Clinical practice improvement
activities
7How would I be paid under the MIPS?
Beginning in 2019, physicians partici-
pating in the MIPS will be eligible for
positive or negative Medicare payment
adjustments that start at 4 percent and
gradually increase to 9 percent for
2022. The threshold for these payment
adjustments will be the mean compos-
ite score for all MIPS-eligible profes-
sionals during the previous performance
period. Distribution of payment adjust-
ments will follow a bell-shaped curve.
[cont. on 26]
26 TEXAS FAMILY PHYSICIAN WINTER 2016
Quality people. Quality care. Quality of LIFE.
Contact: Craig McGovern, Physician Recruiter at 727-437-0846 or [email protected] me about our referral program! Refer a provider. Receive a bonus. It’s that simple!
EmCare is seeking Family Practice Physicians for our ERs throughout the state of Texas and nationwide!
We’re seeking Emergency Medicine, Family Practice and Internal Medicine physicians, with emergency medicine experience, to join our team. We have multiple locations
available, ranging from low to high volume.
Rates up to $245 an hour. Sign-on bonus available.
Candidates must be BC/BP in Emergency Medicine, Family Practice or Internal Medicine. FP/IM with Emergency Medicine experience.
Full time, part time, per diem and travel opportunities available.
with EmCareFind the Perfect Opportunity
8How does MACRA help small
practices?
The law allocates $100 million for the
U.S. Department of Health and Human
Services to support organizations (e.g.,
quality improvement organizations,
regional extension centers) that pro-
vide technical assistance to practices
with 15 or fewer eligible professionals
participating in an APM or the MIPS. 9What is the AAFP doing to help me?
As always, we’re committed to keeping
you informed, developing resources
to support your quality improve-
ment efforts, and helping you provide
cost-effective care. We also want to
know more about your experience with
MACRA, and your decisions about APMs
and the MIPS. As information, tools, and
resources to help you comply with and
benefit from MACRA become available,
we will update AAFP.org and spread the
word through AAFP News and Family
Practice Management.
We will also tell the Secretary of Health
and Human Services what family physi-
cians think about provisions within
MACRA. In particular, we will continue to
advocate vigorously for the following:
• Improved payment for primary care
• Administrative simplification
• Harmonization of measures across
all private and public payers
• Reasonable reporting requirements
10What can I do now to pre-
pare for MACRA implementation?
If you haven’t reported data on quality
measures through the PQRS or as part
of meaningful use, start as soon as
possible. Penalties for not reporting
or for low quality may impact you this
year. More information on Medicare
penalties is available. Go to www.aafp.
org/practice-management/regulatory/
bonus-penalty.html.
• Physicians who score at the thresh-
old (i.e., earn the mean composite
score) will receive no payment
adjustment.
• Physicians whose composite score
is above the mean will receive a
positive payment adjustment on
each claim for the following year.
• Physicians whose composite score
is below the mean will receive a
negative payment adjustment on
each claim for the following year.
Physicians with high composite scores
will be eligible for a positive payment
adjustment that is up to three times the
baseline positive payment adjustment for
a given year. For example, the baseline
positive payment adjustment for 2019
will be 4 percent, so high performers
will be eligible for a positive payment
adjustment of up to 12 percent. For 2019
through 2024, an additional positive pay-
ment adjustment of up to 10 percent will
be available to exceptional performers.
Beginning in 2026, all physicians
participating in the MIPS will be eligible
for a 0.25 percent increase in their pay-
ments each year.
Priority will be given to practices in
rural areas, health professional short-
age areas, and medically underserved
areas, and to practices with low com-
posite scores. The allocated money
will not fund changes at the individual
practice level.
Watch TAFP’s EMBRACING CHANGE videos at www.tafp.org/practice-resources/change/video1.
[cont. from 25]
www.tafp.org 27
Come to work. . . where your work makes a difference!
Exciting and challenging job opportunities await you at a state supported living center.
There are positions available at facilities located around the state. We are looking for
psychiatrists, physicians, pharmacists, dentists, nurse practitioners, RNs, LVNs, therapists, dieticians and direct support professionals.
Excellent benefits package, includes:l Competitive salaries l Health and retirement benefitsl Paid vacation leave l Up to 15 paid holidays annuallyl Shift differential pay
l Flexible schedules
Contact: Laura Hunter at [email protected] 512-438-3268 or 512-348-0503
For information, or to apply online go to
www.dads.state.tx.us/employment/
Medicaid providers can now find their patients' medical histories on YourTexas-BenefitsCard.com. Medicaid Eligibility and Health Information Services added the Blue Button to the site in September.
Once a provider or office staff receives a client's consent, they can log in to the site and click on the Blue Button to see and download the client's health information. The informa-tion can then be saved as a Portable Docu-ment Format document, a Clinical Document Architecture data file, or a simple text file. Once saved, it can be imported into the pro-vider's health management tool.
The YourTexasBenefitsCard Blue Button is assembled from client data found in the
current database and claims data stored in the Medicaid Claims Administrator System. It generates easily accessible patient records on the website for providers to download, import, or print.
Having access to reliable health informa-tion gives providers a more complete picture of their patients’ health. Having the ability to view, print, and export the client’s health information could make it easier to transfer information when referring patients and taking on new ones. It keeps everyone on the same page when multiple doctors are treat-ing a patient. For more information, email Alessandra Reyes at [email protected].
Blue Button makes finding Medicaid patient records simple
11Where can I find more
information on MACRA?
Information, tools, and resources
to help you comply with and ben-
efit from MACRA are available from
the AAFP and from FPM. Go to www.
aafp.org/practice-
management/payment/medicare-
payment.html and www.aafp.org/
journals/fpm.html.
The latest news about MACRA and
other payment reform topics is avail-
able from AAFP News at www.aafp.org/
news/government-medicine.html.
12How can I get answers
to my practice-specific questions?
AAFP members can contact an AAFP
subject matter expert at www.aafp.org/
practice-management/administration/
ask.mem.html or call (800) 274-2237.
If you submitted quality data during
the last calendar year, you should have
access to your Quality and Resource Use
Report. This report will help you under-
stand your performance in terms of cost
and quality so you can prioritize potential
areas for improvement.
If your practice doesn’t provide chronic
care management services, consider
starting now. Medicare began paying
for CCM codes on January 1, 2015. By
offering CCM services, your practice
will be a step closer to implement-
ing the five comprehensive primary
care functions promoted by the CPC
initiative. You may also qualify to
participate in the APM track. Informa-
tion on chronic care management and
resources to help you start providing
CCM services in your practice are avail-
able. Go to www.aafp.org/
practice-management/payment/
coding/ccm.html.
HHSC NEWS
28 TEXAS FAMILY PHYSICIAN WINTER 2016
FOUNDATION FOCUS
Baylor Scott & White Health
Memorial Hermann Health System
ProAssurance
TAFP Dallas Chapter
Texas Medical Association
Texas Medical Liability Trust
Shivum Agarwal, MD
Ruben Aleman, MD
★ Trisha A. Allamon, MD
Victor Lee Allen, MD
Gary R. Allen, MD
Dale Crawford Allison, MD
★ Erick Fernando Alvarez Mosqueira, MD
Adanna Juliet Amechi-Obigwe, MD
Ichabod L. Balkcom, IV, MD
★ Maria Diana Ballesteros, MD
Madhumita Banga, MD
★ Tom Banning
★ Lynda Jayne Barry, MD
★ Justin V. Bartos, MD
David W. Bauer, MD, PhD
★ Stephen Douglas Benold, MD
★ Teddy and Henry Julius Boehm, Jr., MD
Robert John Bolster, MD
★ Lindsay Kathryn Botsford, MD, MBA
★ Emily D. Briggs, MD, MPH
★ Dennis L. Brown, MD
Raul Niduaza Calvo, MD
★ Chinglin Lillian Chan, MD
★ C. Mark Chassay, MD
Joanna Clark
Jill Clay, MD
Oscar Cortes, MD, MBA
★ Seth B. Cowan, MD
Alice Dilling Cox, MD
Michael Avery Crouch, MD
Douglas W. Curran, MD
Darnel Viray Dabu, MD, MPH
★ Kenneth Gayle Davis, MD
Manuel De Los Santos, MD
Paula L. Denson, MD
★ Tamra K. Deuser, MD
★ Chrisette M. Dharmagunaratne, MD
Darrell R. Dixon, MD, MBA
★ Jorge Duchicela, MD
★ Tamarah L. Duperval-Brownlee, MD
Carolyn Eaton, MD
★ Bruce Alan Echols, MD
★ Tricia C. Elliott, MD
Sheridan Scott Evans, MD
Christopher S. Ewin, MD
★ Robert Floyd Ezell, MD
★ Antonio Falcon, MD
★ Troy Treanor Fiesinger, MD
★ Aimee Lyn Flournoy, MD
★ Lewis Emory Foxhall, MD
Edwin R. Franks, MD
★ Kelly A. Gabler, MD
Oscar Garza, MD
★ Melissa Susan Gerdes, MD
★ Lisa Biry Glenn, MD
★ Roland A. Goertz, MD
Ty Lee Gore, MD
Geraldine Gossard, MD
★ John Edward Green, MD
★ Thomas David Greer, MD
★ Ajay Kumar Gupta, MD
★ Natalia Gutierrez, MD
★ Lesca C. Hadley, MD
★ Suhaib W. Haq, MD
★ Rebecca Eileen Hart, MD
Bill and Gail Hartin
Sharon Hausman-Cohen, MD
Clare Arnot Hawkins, MD, MSc
★ James Michael Henderson, MD
Harriet Nailor Hilliard, MD
★ Terrance S. Hines, MD
★ Farron Cheryl Hunt, MD
★ Janet L. Hurley, MD
Lee Janson, MD
★ Audrey Lee Jones, DO
Brian D. Jones, MD
★ David Arthur Katerndahl, MD
★ Christina Marie Kelly, MD
★ Shelley Kohlleppel, MD
★ Kaparaboyna Ashok Kumar, MD, FRCS
★ Cyrus Timothy Lambert, MD
★ Don A. Lawrence, DO
Huong Le, MD
Patrick Ys Leung, MD
Kathy and Paul Locus, MD
Donald E. Lovering, MD
★ Leah Raye Mabry, MD
McDavid Michael Mahaffey, MD
Ernesto Malave, MD
★ Javier D. Margo, MD
James Charles Martin, MD
★ Kathy McCarthy, CAE
Jimmy Eugene McCoy, MD
★ William Mike McCrady, MD
★ John M. McCullough, MD
★ Susan Clymer McMullen, MD
Victor O. Mendiola, MD
★ Gary R. Mennie, MD
★ Jessica Miley
Kavitha Moolamalla, MD
★ Carol and Dale C. Moquist, MD
★ Graciela Moreno, MD
★ Mary Helen Morrow, MD
★ Estela Mota, MD
Bonnie Eugenia Muncy, MD
James A. Murphy, MD
W. Darell Murphy, MD
Nancy Naghavi, DO
Jonathan Nelson
★ Mary S. Nguyen, MD
Donald R. Niño, MD
★ Paul B. Oliver, MD
Didier F. Piot, MD
★ Henry David Pope, MD
Teresita Ramirez-Scott, PA
★ John R. Richmond, MD
★ Shelley Poe Roaten, MD
Leon Rochen
Alex Salazar, MD
★ Sarah Samreen, MD
Ramiro Sanchez, MD
★ M. Sandra Scurria, MD
★ Stephanie Segal, MD
Jennifer Cobb Seger, MD
Puja Anil Sehgal, MD
Mike Sevilla, MD
★ Amer Shakil, MD
H. Kyle Sheets, MD
★ Zafreen Arfeen Siddiqui, MD
★ Linda Marie Siy, MD
★ Mary Carmen Spalding, MD
★ Charles Stern, MD
★ Sharon Stern, MD
★ Donald E. Stillwagon, MD
★ Paul and Erica Swegler, MD
Thuy Hanh Thi Trinh, MD, MBA, FAAHPM
★ Ashok Tripathy, MD
★ Thao Minh Truong, MD
★ Lloyd Van Winkle, MD
Samuel C. Wang, MD
★ Isaac A. Watemberg, MD
★ Sally Pyle Weaver, MD
Judge Marcia Weiner
★ Jim and Karen White
Walter D. Wilkerson, MD
★ Hugh H. Wilson, MD
Keith Allen Wixtrom, MD
★ Khalida Yasmin, MD
★ Robert Allen Youens, MD
★ Richard A. Young, MD
2015 TAFP Foundation donors★ = TAFP Foundation monthly donor
Thank you to these 2015 TAFP Foundation donors, whose contributions fund scholarships for Texas medical students, family medicine research grants, and travel scholarships for residents to attend continuing professional development activities.
Representation before the Texas Medical Board, The Texas Medical Foundation and Medical Staff Peer Review.
Medical Practice Act and Medical Board Actions(hearings, settlement conferences and licensure) • Personal Counsel in Medical Liability Cases
• Probation Modification / Termination • Managed Care Exclusions • Licensure
• Reinstatement • Medico-legal Issues• Expert Review • Telemedicine
• Medicare/Medicaid Appeals• Medical Ethics Opinions
• Physician Assistants.
* Board Certified in Administrative Law by the Texas Board of Legal Specialization.
Confidential and experienCedLEgAL REPRESEnTATIOn FOR TExAS PhySICIAnS
MIChAELShARP*
COuRTnEynEwTOn
ChRIS ShARP Of Counsel
TOnyCOBOS*
ShARP & COBOS, LLP, Attorneys At LAw4705 SPICEwOOd SPRIngS ROAd • SuITE 100• AuSTIn, TExAS 78759 • 512 473 2265 • FAx: 512 473 8525 • www.sharpcobos.com
SharpLLPGSAd12_09.indd 1 12/21/09 2:52:24 PM
Early diagnosis and treatment of HIV
saves money and improves health outcomes.
Routine HIV testing in health care settings is as cost effective as
other screening programs, including type 2 diabetes and breast
cancer mammography.
Learn more at
www.testtexashiv.org
Krentz HB, Auld MC, Gill MJ. The high cost of medical care for patients who present late (CD4 < 200 cells/μL) with HIV infection.
HIV Medicine. 2004;5:93-8.
message no 6 tafp.indd 1 6/12/11 7:18:42 PM

30 TEXAS FAMILY PHYSICIAN WINTER 2016
in my leadership duties for the Texas Academy of Family Physicians and within my personal job as family physician and operational chief of primary care for Trinity Mother Frances Health System, I continue to see pockets of skepti-cism, frustration, and fear among my primary care physician colleagues. In some of my most difficult assignments, I have felt that the greatest barrier occurs when some physicians go straight to the negative with their thoughts as we begin discussions.
Our specialty is rife with physicians that go straight to the negative. When we consider the high rates of physician burnout in our country we begin to under-stand why this is true. Primary care physicians have felt overworked and underpaid for quite some time. The current fee-for-service pay-ment system has created inefficient patient management practices that prevent care for simple conditions over the phone, lead to unneces-sary follow-up appointments, and encourage physicians to pack more patients into their clinic day to gen-erate volume. Transitioning these practices to a value-based payment world is truly a challenge.
When family medicine leaders reach out to constituents in private practices, we commonly find that physicians do not trust their nearby hospital administrators, they see neighboring practices as competi-tion, and they are quick to blame insurance companies for most of their payment problems. While a lot of this frustra-tion is justified, it hinders their ability to make the necessary changes in their practice that will make them viable in the medical marketplace of the future. I propose another way of thinking. What if instead of going straight to the negative, we begin accepting the maybe.
Maybe hospitals really do understand the need for a strong primary care infrastructure within the community to provide good care to the patients they serve. Maybe their appeal to provide EMR support, shared savings benefits, or other ame-nities to local physicians is generated with honest intent.
Maybe insurance companies really do want to partner with us to create a higher quality, lower cost health-delivery product for our communities. While we realize every busi-ness needs to make money to stay afloat, maybe we can begin to believe that insurers see patients as more than covered lives.
Maybe we will realize that employers are the true custom-ers in the insurance marketplace and they value our ability to see their employees efficiently so they can receive the needed
treatments and get back to work. Maybe we will realize our desire
for autonomy must also come with accountability. The future health care marketplace will demand a commitment to following evi-dence-based guidelines and provid-ing reports on quality. We should realize that patients are demand-ing this and they are becoming much more sophisticated in their research efforts and physician selec-tion. We should be motivated by a desire to improve and not offended because people ask about our cre-dentials and quality ratings.
Maybe we can accept that there is strength in numbers and that integrating with neighboring inde-pendent primary care physicians or health systems will make the transition to these changes more palatable.
Maybe we will realize our true cus-tomers are our patients and they are
demanding these health care changes as much as anyone else. Once local primary care physicians begin to have col-
legial discussions with hospitals, insurers, or employers, maybe these other entities will begin to trust that the physicians care more about their patients and the commu-nity than their own bottom line. And maybe, just maybe, primary care physicians will once again enjoy being doctors.
Janet Hurley, MD, is TAFP Treasurer and the operational chief for primary care for Trinity Mother Frances Health System, South Region. Read her blog at http://acceptingthemaybe.blogspot.com/.
PERSPECTIVE
Accepting the maybeBy Janet Hurley, MD
Many physicians do not trust their nearby hospital
administrators, they see neighboring practices as
competition, and they are quick to blame insurance
companies for most of their payment problems. While
a lot of this frustration is justified, it hinders
their ability to make the necessary changes in their
practice that will make them viable in the medical marketplace of the future.
As a physician, you understand
that health is everything.
TMA Insurance Trust advisors have decades of
experience matching Texas physicians with the
health insurance coverage that meets their unique
and individual needs. If you need help securing
coverage during the annual ACA open enrollment,
or coverage for your employees, our advisors will
shop the open market and choose from the major
insurance carriers to find a suitable plan for you.
Call us today 1-800-880-8181
or visit us at www.TMAIT.org.
NPINSTITUTE.COM
NatioNal Procedures iNstitute
Teaching procedural skills to enhance medical practice since 1989
The Texas Academy of Family Physicians presents:
Want
from your practice
Invest in yourself by enhancing your procedural skills from NPI and have the practice you’ve always wanted!
By learning new procedural skills through NPI, you can:• Increase your earning power,• Provide comprehensive services,• Earn CME credits,• Stop “referring” revenue away, and• Improve continuity of care for your patients.
JULY 21 – 24, 2016 | AUSTIN, TEXASOmni Austin Hotel at Southpark | (800) 843-6664 | 144/$164 per night
See what NPI can offer you.
Find our full schedule and register
online at www.NPInstitute.com or call (866) 674-2631
or (866) NPI-CME1 today.
UPCOMING SCHEDULE
Aesthetic Procedures July 21-22 $1,295
Colonoscopy July 21-22 $1,350
Dermatologic Procedures July 21-22 $1,495
Allergy Testing and Immunotherapy for Primary Care Physicians July 22 $795
Sclerotherapy July 22 $1,050
Advanced Colonoscopy July 23 $1,100
Anti-Aging Medicine: Advances in Hormone Replacement July 23-24 $1,295
Exercise Stress Testing July 23-24 $1,095
Hospitalist Procedures July 23-24 $1,495
Joint Exam and Injections July 23-24 $1,295
SEPTEMBER 8 – 11, 2016HOUSTON, TEXASWestin Galleria Hotel
DECEMBER 8 – 11, 2016LAS VEGAS, NevadaRed Rock Casino, Resort & Spa
Full Page NPI ad July 2016.indd 1 1/20/2016 3:40:40 PM