Embed Size (px)
Citation preview

SCLAFANI-GRAND ROUNDS SAMPLE
GRAND ROUNDS:Guess what I saw today!
Louise A. Sclafani, OD, FAAOCOPE#24602-SD
Cases will be presented in a grand rounds mannerwith audience participation determining
management.Classic and unusual conditions will be discussed in
detail from diagnosis to treatment.Examples are included
Patient History and ClinicalFindings are Presented
Age, Race, Gender POHX: Patient Ocular History PMHX: Patient Medical History FO/MHX: Family Ocular and Social History CC: Chief Complaint Are there any other questions Always look at the fellow eye Survey the family history More is revealed when someone else asks
Tests IncludeBasic Tests BVA: Best
corrected vision Pupils/Motility SLX: Slit Lamp
evaluation IOPs DFE: Dilated
fundus evaluation
Additional Tests Office procedures
– Color, Vital Dye Lab tests Imaging VF, OCT, FANG
Differential Diagnosis What are the most likely causes of
your findings based on the patientspresentation and history.
Include the most common and thosethat are rare.
What are the trends and include yourpast experience
TREATMENT PLAN Include medical and surgical options What is your scope of practice What is standard of care Is there consent When is the follow-up
If you would like the backgroundinformation for the cases presented today,
please email me:

SCLAFANI-GRAND ROUNDS SAMPLE
Patient History and ClinicalFindings are Presented
Age, Race, Gender POHX: PMHX: FO/MHX: CC: BVA: SLX: IOPs DFE:
Other tests:
What is your DDX? What are the ClinicalFindings of this condition?
How would you treatthis condition? NOTES

SCLAFANI-GRAND ROUNDS SAMPLE
PATIENT HISTORY 67 yo WF c/o reduced vision and sees a white floating
line in center of vision OS PoHx: cataracts, LPI OS, floaters, DES PmHx: Capillary Leak Syndrome, HTN,
cholesterol, asthma, allergy, fibromyalgia Meds: Darvocet, Effexor, Benicar, Seravent,
fosamax, Lipitor, AT FoHx: brother and sister with glaucoma Referred to me by retinal service/ general
ophtho
EXAM FINDINGS VARE 20/60 LE 20/50 mono.dip BVA RE 20/50 -1.00 +.75 x 173
LE 20/30 - .75 + 2.00 170 ** IOPS 23,23 SLX 2-3+ NS/CS OU OS
Patent LPI OTHER TESTS
OTHER TESTS
Trial frame improves symptomsof monocular diplopia but “wavy
line” persists.
Consistent Finding

SCLAFANI-GRAND ROUNDS SAMPLE
DIFFERENTIALDIAGNOSIS
Posterior VitreousDetachment
ERM or othermacular condition
TESTS TO R/O– DFE– OCT
DIFFERENTIALDIAGNOSIS
Posterior Vitreous Detachment ERM or other macular condition Cortical Cataract Post-op effects of YAG laser
– PVD secondary to Pilocarpine use– PVD or rapid cataract progression due to
shock wave (energy + 5.8 mj)– Visual symptoms due to LPI
Contact Lens TrialCooperVision Prosthetic
Series No. 3, BO ( back tint,
open pupil) Eliminates symptoms
of line and some ofblur when combinedwith trial frame
No longer availablefrom CV: Marietta Lab
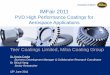
PURPOSE:
PURPOSE: Patients experience visual
disturbances after LP 1st study to evaluate them and
determine if there was anassociation of lid position andsize.
172 eyes, 92 controls
J Glaucoma, Volume 14, October2005
CONCLUSION:Visual symptoms related to LPI
occur in 7%
More likely to occur in patientswho have exposure, and mostlikely if it is partial. Fully
Eye (2006)
Glare from PI

SCLAFANI-GRAND ROUNDS SAMPLE
RESULTS
full
DIFFERENTIALDIAGNOSIS
Post-op effects of YAG laser– PVD secondary to Pilocarpine use– PVD or rapid cataract progression due to shock wave (Nd:YAG =
energy + 5.8 mj– Visual symptoms due to the LPI
Visual symptoms LPI hole vs. Tear Mensicus– Weintraub and Burke, Ophthalmology 1992
Pt reports that when she lifts the lid away (exposing entire PI)the symptoms go away.
Symptoms also relieved when looking down Therefore symptoms not related to aperture, but due to light
rays being refracted by the tear film at the edge of the upperlid and then passing through PI.
TREATMENT Occluder Contact Lens Cataract surgery first
– Cataracts are significant, however patient isanxious
– Eliminate narrow angles– Iris will be repositioned and reduce symptoms– McCannel closure preferred vs. Morcher
segment Corneal Tattoo
– Tattoo should always be done after cataractsurgery so as not to hinder view
Therapeutic Tattoo Coloring: organic, gold dust, india ink etc
– Pfeiffer describes anterior stromal micropuncturetechnique using commercially available dyes
– Risk of full thickness puncture, inflammatory reaction inwhich cells eat up dye, non-uniform results, RCE
– Long term safety unknown: possible toxicity (arsenic,Cl) Use of Intacs channel dissector to distribute dye
– Risk of non-uniform or limited surface area– Awdeh suggests use of Intralase to create flap/paint
stromal cap Chemical reaction involving precipitated pigment
brought about by metallic salts
Filter paper soakedwith sterile platinumchloride solution isinserted into 2 mmstromal pocket anteriorto PI
The reducing agent,hydrazine hydrate wasadded under paperand excess solutionremoved.
Over time, reduced toplatinum black :
20 months later
PATIENT HISTORY c/o wants cataract removed to see if there is vision
potential/ improve cosmesis BVA: OD NLP OS 20/20 sc PoHx: Trauma OD > 20 yrs, strabismus sx OD
>10yrs, cryo sx OS for retinal hole > 5 yrs LEE > 5yrs
PmHx: UTI, +RA Meds: IV AB, d/c pred and methotrexate CLHx: wears SCL opaque lenses purchased at
beauty supply store. Uses Visine weekly. EW.Present lens 3 months old. Pays $25 per pair.
Social: “gypsy”

SCLAFANI-GRAND ROUNDS SAMPLE
Patient History and ClinicalFindings are Presented
Age, Race, Gender POHX: PMHX: FO/MHX: CC: BVA: SLX: IOPs DFE:
Other Tests:
What is your DDX? What are the ClinicalFindings of this condition?
How would you treatthis condition? NOTES

SCLAFANI-GRAND ROUNDS SAMPLE
PATIENT HISTORY 30 YO WM H/O sudden RE eye pain, redness, blur CLHx: Ciba N/D, OptiFree Express OMD: 3 days after RE symptoms he began
Vigamox TID -OD. Some improvement soresumed CL wear. One day later, severeeye pain OU.
PmHX and FoHX: negative Social: cleans portable toilets, cleans CLS
at work
LE 5 circular epithelial defects in acurva-linear pattern across cornearanging in size .1 to 2.1 mm withsurrounding infiltrate. RE had one
Feathery appearance: DDX?/ Tests?
DIFFERENTIALDIAGNOSIS
Corneal Abrasion or Trauma Sterile Infiltrate Microbial Keratitis
– Bacterial– Fungal– Viral– Protozoan
SterileInfection
Mild pain Small Multiple or arcuate Peripheral No discharge Epithelium intact* Elevated AC quiet Focal Accumulation
of inflammatory cells
Moderate to extreme Large Individual lesions Central Discharge Epithelial staining Flat or excavated AC reaction Localized edema
Stein RM, Clinch TE, Cohen EJ,Genvert GI, Arentsen JJ, Laibson PR:
Infected vs. sterile corneal infiltrates in contact lenswearers.
Am J Ophthalmol 1988, 105(6);632-636
Infiltrative KeratitisDifferential diagnosis is critical
LAS
Most Likely Organismsin CL Wearers
Pseudomonas aeruginosa: gram -– 50% of CL related ulcers, also post sx or trauma– Can penetrate an intact cornea & perforate in 24 h
Staphylococcus aureus (gram + non mobile)– Colonizes eyes, nose axillae
Serratia marcesens (gram - bacteria)– Develops over time and requires a break in epithelium
Acanthamoeba (protozoa)– A minor corneal break allows it to enter from
contaminated CL solutions, cases, or tap water. Ring

SCLAFANI-GRAND ROUNDS SAMPLE
TREATMENT PLAN Vigamox increased to q 2h OU ( seemed to
improve symptoms previously) Natamycin q 4 hours ( high suspicion FK) Cultures Taken
– Cornea: no growth– CLS/Case/Solution: -gram colonies of
Alcaligenes xylosoxidans. Later confirmed withPCR
– Case series showed a 92% sensitivity alcaligensto systemic trimethaprim-sulmethoxazole
– Started Polytrim (polymyxin B/trimethoprin) qhand continue Natamycin. D/C Vigamox
Improvement over Time Symptoms improved
after 2 days: Polytrimtapered q 4 x 5 days,then QID x 10 days
d/c Natamycin 1 week BVA 20/25 at 10 days Residual scar at 3 wks
Achromobacterxylosoxidans
Motile, aerobic,gram-negative,non-fermentativestraight rod with aperitrichousflagella*
DDX: PA Urine, blood, ears,
respiratory tract,and spinal fluid
Opportunisticpathogen tocompromised tissue
Water pathogen foundin pools, chlorhexidine
Reports: post-PKP,EKC, steroid use,NVGTherapeutic BCL
Resistant to many AB Sensitive to Polytrim
Patel, Saidel, UC ARVO 2008
SIGNIFICANCE OFCASE
There are only 15 reports of ocular infectionfrom Achromobacter xylosoxidans and thisis the first to be confirmed with PCRtechnique
VITEK 2 rapid panel assays which can ddxfrom PA and determine specificities
Recent study showed (excluding PA) a highconcordance rate of gram negative rodsbetween +CL cultures and – cornealscrapings
Our patient Extensive daily wear use (15 – 20 hours) A.xylosoxidans isolated from sewage sludge His case and solution was exposed at work
making colonization possible, and uponexposure under stress infection can result.
Cultures revealed A.xylosoxidans to beresistance to aminoglycosides,cephalosporins and first-generation FQ.Perhaps the low dose Vigamox was enoughto render cornea culture negative, butenough to eliminate infection.

SCLAFANI-GRAND ROUNDS SAMPLE
Patient History and ClinicalFindings are Presented
Age, Race, Gender POHX: PMHX: FO/MHX: CC: BVA: SLX: IOPs DFE:
Other Tests:
What is your DDX? What are the ClinicalFindings of this condition?
How would you treatthis condition? NOTES

SCLAFANI-GRAND ROUNDS SAMPLE
Patient M.C.
HPI: 34 year old female with: Red swollen left eye Purulent discharge Central corneal opacity Suicidal ideation
Additional HPI: History severely limited by patient
agitation/intoxication Last used crack cocaine today Seen at OSH 4 days ago for “corneal
abrasion.” Prescribed abx butnoncompliant.
Varied patient response regardinglength of problem OS - 4 days, 2months or 2 years???
Medical History PMH: Bipolar disorder, hepatitis B and C Ocular History: Unknown Meds: Depakote, Trazadone (non-
compliant) Allergies: NKDA SHx: +EtOH, +crack cocaine, +tobacco FHx: Non-contributory
Visual Examination VASC: CF@ 2ft OD; LP OS Pupils: 6mm unreactive to light OD; hazy
view OS, ~4mm unreactive to light; ?Reactive to near
Motility and CVF: Unable to cooperate External exam: Photo Anterior segment: Photo DFE: Normal OD; no view OS; Bscan –
retina flat
Differential Diagnosis Corneal ulcer
– Bacterial– Fungal– Parasitic– Neurotrophic
Corneal melt Corneal burn Self-induced trauma Toxic exposure
Clinical Course Admitted to hospital for psychiatric
observation Lid and corneal cultures sent in ER Tobramycin q1h; Vancomycin q1h –
alternating q30min Eye culture: One colony coagulase (-)
Staph; one colony Corynebacterium,(normal flora)
Fungal/AK cx negative

SCLAFANI-GRAND ROUNDS SAMPLE
Additional LaboratoryStudies
Utox: +cocaine Head CT: normal RPR: non-reactive HIV: negative
Additional historyobtained
Uses $100/day of crack cocaine(smokes)
Works as prostitute Unable to see out of left eye for >2
years Non-compliant with follow-up Denies history of contact lens wear,
surgery, head trauma OS
Clinical Course f/u VA 20/100 OD; LP OS IOP 20 OD; 21 OS Denies any symptomatic improvement No clinical improvement in corneal
defect, size of infiltrate Seidel negative; no evidence of
perforation Started Doxycycline and Vitamin C Recommended FTA-ABS
Future TreatmentStrategies
Prevention of corneal melt– Doxycycline– Vitamin C– Topical medroxyprogesterone– 10% sodium citrate
Tarsorrhaphy Amniotic membrane graft Corneal transplant Substance abuse counseling
Eye Complications ofCocaine Abuse
Angle closure glaucoma Retinal hemorrhages Optic neuropathy Ocular motility disturbances Nasolacrimal duct obstruction Orbital cellulitis Corneal epithelial defects SPK Corneal ulcers Corneal perforation
If you would like the backgroundinformation for the cases presented today,
please email me: