Embed Size (px)
Citation preview

Testosterone Replacement in
Adults
John A. Seibel, MD, MACE

History of Testosterone Rx
• Ancient Europe and Asia
– Castrated males had no secondary sex charistics
– Used as eunichs to guard Women
• 1765 Hunter Transplanted Tissue in Animals
• 1849 Berthold “Results of Castration Caused
by a substance secreted from testicles.

Dr. Brown-Sequard
Auto Injected Extract
• “…a radical change took place in me….I fully
regained my old powers….My limbs…showed
a decided gain of strength. With regard to
the facility of intellectual labour,…a return to
my previous ordinary condition became quite
manifest during and after the first two or
three days of my experiments.”
• Called Testosterone “the Elixir of Life”.

Brown-Sequard 1889
• Immediately 12,000 Physicians began injecting
“testosterone extract”
• Unfortunately it had little testosterone and
the effects were placebo.
•

Sergio Veronoff 1920
• Began transplanting animal testes into men.
• Others used goat and sheep testicles.
• Uniformly rejected by the body and the only
effects were placebo

Synthetic Testosterone
• 1935 David isolated testosterone
• 1939 Kock used Used 40 pounds of bull testes to
get 20 mg of testosterone
• 1939 Butenandt and Ruzika received Nobel Prize
in Medicine for synthesizing Testosterone
• Testosterone injections began
• 1990 patch is introduced.

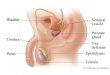
Role of Testosterone in
Male Health

The Impact of Testosterone
Skin
Hair growth, balding,
sebum production
Liver
Synthesis of serum
proteins
Male Sexual Organs
Penile growth,
spermatogenesis, prostate
growth, and function
Brain
Libido, mood
Muscle
Increase in
strength and
volume
Kidney
Stimulation of
erythropoietin
production
Bone Marrow
Stimulation of
stem cellsBone
Accelerated linear
growth, closure of
epiphyses
Guyton AC. In: Textbook of Medical Physiology. 8th ed. 1991:891-895.

TESTOSTERONE SECRETION

Testosterone Production
Adapted from Bagatell CJ, Bremner WJ. N Engl J Med. 1996;334:707-714.
GnRH
LH FSHTestosterone
Testosterone
Sperm
Hypothalamus
Pituitary
Testis

Production and Regulation of Testosterone
Hypothalamus
Pituitary
Testes
Leydig cells
LH
GnRH
FSH
FSH = follicle-stimulating hormone; GnRH = gonadotropin-releasing hormone;
LH = luteinizing hormone; T = testosterone.
Costanzo LS. Physiology. 3rd ed. Saunders Elsevier; 2006:449.
+
+ –
–
TT
Sertoli cells

Definition of Male Hypogonadism
“ … clinical syndrome that results from failure of the testes to produce
physiological levels of testosterone … due to disruption of one or more levels
of the hypothalamic-pituitary-gonadal (HPG) axis.”
Endocrine Society Guideline (2006)
“ … inadequate gonadal function, as manifested by deficiencies in …the
secretion of gonadal hormones.”
American Association of Clinical Endocrinologists Guidelines (2002)
Bhasin S, et al. J Clin Endocrinol Metab. 2006;91(6):1995-2010.
Petak SM, et al. Endocr Pract. 2002;8(6):440-456.

13
Definition of Hypogonadism
• Male gonadal dysfunction
• Low levels of testosterone
• May be congenital or acquired
Winters SJ. Arch Fam Med. 1999;8:257-263; Petak SM, et al. AACE Clinical Practice Guidelines.
Available at: http://www.aace.com/clin/guidelines/hypogonadism.pdf. Accessed October 16,
2003;
Tenover JL. Endocrinol Metab Clin North Am. 1998;27:969-987.

Signs And Symptoms of Low T
• Loss of muscle mass and strength• Loss of libido and erectile function• Depression• Fatigue• Osteoporosis• Hot Flashes, Sweats
• Some regression of secondary sexual
characteristics• Oligospermia or azoospermia
• Tenover JL. Endocrinol Metab Clin North Am. 1998;27:969-987.
• Petak SM, et al. AACE Clinical Practice Guidelines. Available at: http://www.aace.com/clin/guidelines/jypogonadism.pdf•

Incidence of Hypogonadism

Prevalence of Low Testosterone
13.8 Million Men in the US
34%
40.2% 39.9%
45.5%50%
38.7%
0
10
20
30
40
50
60
70
45 to 54 55 to 64 65 to 74 75 to 84 85+ Total
Pre
va
len
ce o
f H
yp
og
on
ad
ism
Patient Age Range
Overall, 38.7% of men ≥≥≥≥45 years had
testosterone levels <300 ng/dL
Mulligan T, et al. Int J Clin Pract. 2006;60(7):762-769..
Patients recruited for study from 2003-2004.

17
Prevalence and Treatment of
Hypogonadism
10-14 Million Men with Hypogonadism
Adapted from US Food and Drug Administration Updates. Skin patch replaces
testosterone.
Available at: http://www.fda.gov/fdac/departs/196_upd.html. Accessed May 23, 2003.
10%of men arecurrently treated

Low Testosterone Is Increasingly
Common as Men Age
• Men in their 40s and 50s1 in 10
• Men in their 60s1 in 5
• Men in their 70s1 in 4
However, less than 10% are being
treated for low testosterone
Available at: http://www.fda.gov/fdac/departs/196_upd.html Accessed March 20, 2009.

Conditions
Associated with
Hypogonadism

Prevalence of Low Testosterone in
Other Conditions
ED = erectile dysfunction
1. Daniell HW. J Pain. 2002;3:377-384; 2. Mulligan T, et al. Int J Clin Pract. 2006;60:762-769; 3. Grinspoon S, et al. Ann Intern
Med. 1998;129:18-26; 4. Dobs AS. Baillière’s Clin Endocrinol Metab. 1998;12:379-390; 5. Bodie J, et al.
J Urol. 2003;169:2262–2264.

Chronic Opioid Use
• Direct Effect on Hypothalamus
– Decreases GhRH Production & Release
• Direct Effect on Testes
– Decreases Production of Testosterone and
Androgenic Binding Proteins
• Effect begins almost immediately

Prevalence of Low Testosterone in
HIV and AIDS• 30% of men with HIV and
50% of men with AIDS are
hypogonadal1,2
• Mechanisms of
hypogonadism in men with
HIV and AIDS are complex
and not fully understood2
1Grinspoon SK, et al. N Engl J Med. 1992;327-1360-1365; 2Dobs AS, et al. J Clin Endocrinol Metab. 1996;81:4108-4112.

23
Acquired Causes or Conditions
• Pituitary adenoma
• Inflammatory diseases (rheumatoid arthritis, Crohn’s disease,
ulcerative colitis)
• Respiratory disorders (asthma, COPD, sleep apnea)
• Iatrogenic (ketoconazole, glucocorticoids, spironolactone, cimetidine,
phenytoin, flutamide, opioids)
• Other endocrine disorders (hyperprolactinemia, hypothyroidism)
• Alcohol or anabolic steroid abuseWinters SJ. Arch Fam Med. 1999;8:257-263; Tenover JL. Endocrinol Metab Clin North Am. 1998;27:969-987; Gordon GG, et al. J Clin Endocrinol Metab. 1975;40:1018-1026; Doerr P, Pirke KM. J Clin Endocrinol Metab. 1976;43:622-629; Tengstrand B, Carlstrom K, Hafstrom I. Rheumatology (Oxford). 2002;41:285-289.

24
Primary Hypogonadism (Primary Testicular Disorder):
Acquired Causes
• Medications
• Obesity
• Severe systemic illness
• Castration
• Hemochromatosis
• Mumps orchitis
• Idiopathic
• Neurodegenerative
illnesses
• Malnutrition
• Respiratory disorders
• Trauma
Winters SJ. Arch Fam Med. 1999;8:257-263.Tenover JL. Endocrinol Metab Clin North Am. 1998;27:969-987.Gordon GG. J Clin Endocrinol Metab. 1975;40:1018-1026.Doerr P, Pirke KM. J Clin Endocrinol Metab. 1976;43:622-629.Tengstrand B, Carlstrom K, Hafstrom I. Rheumatology (Oxford). 2002;41:285-289.

Diabetes/Metabolic Syndrome
and Low Testosterone Levels• Men with metabolic syndrome or type 2 diabetes may
have concurrent low testosterone
• In three major studies with >2800 patients, patients with metabolic syndrome or type 2 diabetes were more likely to be in the lowest testosterone quartile1-3
– Laaksonen et al. Diabetes Care. 2004; Kupelian et al. J Clin Endocrinol Metab. 2006; Muller et al. J Clin Endocrinol Metab. 2005
• Serum testosterone should be measured in men with type 2 diabetes with symptoms suggestive of testosterone deficiency4
1Laaksonen DE, et al. Diabetes Care. 2004;27:1036–1041; 2Kupelian V, et al. J Clin Endocrinol Metab. 2006;91:843-850; 3Muller M, et al. J
Clin Endocrinol Metab. 2005;90:2618-2623.; 4Wang C, et al. C, et al. Int J Impot Res. 2009;21:1-8.

Association Between Hypogonadism, Obesity, and Insulin Resistance
Leydig cells� Increased insulin resistance affects cells
Low testosterone
Adipose tissue� Increased number of adipocytes in obese and type-2 diabetic men
� Greater aromatase activity
� Increased metabolism of testosterone to estradiol
Pituitary and hypothalamus� Estradiol inhibits LH/FSH secretion
FSH = follicle stimulating hormone; LH = luteinizing hormoneCohen PG. Med Hypotheses. 1999;52(1):49-51; Kapoor D, et al. Clin Endocrinol (Oxf). 2005;63(3):239-250;
Pitteloud N, et al. J Clin Endocrinol Metab. 2005;90(5):2636-2641.

Role of Testosterone in Erectile
Function• Screening
– 19% of men with ED are known to have low testosterone1
– 23-50% of patients are non-responsive to PDE5 inhibitors2
– Patients failing PDE5 inhibitors may warrant screening for low testosterone
• Causes of ED include several factors3
– Psychogenic
– Neurogenic
– Endogenic
– Vasculogenic
• Animal models suggest that the erectile pathway is testosterone dependent4
– Nitric oxide is necessary for penile erection
1. Bodie J, et al. J Urol. 2003;169:2262–2264; 2. Salonia A, et al. Curr Med Res Opin. 2003; 19:241-262;
3. Yassin AA, Saad F. J Androl. 2008; 29:593-604; 4. Shabsigh R. Aging Male. 2004; 7:312-318.

Number Treated
• 2009 1.2 million
• 2013 2.3 million
Endocrine Today : April 2016
Source FDA

FDA Concerns Prompt New Warning
• FDA Concerns Have Decreased
• Use of TRT
• • Risk of CVD, VTE and stroke – FDA
• requires boxed warning on all TRT
• products since 6/14, 3/15.
• • Decision made based on 4 trials (Vigen, Finkle,
• Basaria, Xu).
• • All with methodological flaws or misleading
• results.
• • Concern with inappropriate use and use in
• aging men

Increased Use of TRT
• Increased opioid use
Increased incidence of co-morbidities
• • Obesity
• • DM
• • HIV/AIDS
• • Increased steroid abuse
• • Stress

Heart and Testosterone

Testosterone & the Heart
• 4 Studies Concluded Increased CV Risk
• Vigen et al
– Concluded that there was a doubling of risk
– 29 different Medical groups demaned it be
retracted for faulty design & Calculation
– The group admitted errs and came out with
correct conclusions
– Results the opposite of original conclusions

Basaria et al
Showed Increased CV Events
• Mean age was 74
• Subjects had Serious Chronic Diseases
– High Percentage of Subjects
– Diabetes, Abn. Lipids, HTN, Obesity and Pre-
existing Heart Disease
• Selected Patients with Mobility Problems

The Studies that prompted FDA
• Finkle Study:
– Too small to be significant
• Xu Study
– Meta analysis that was flawed

Hypogonadal Males Treated with
Testosterone
• Shores et al studied 1031 Males at VA
– Showed increased mortality in the untreated
group compared to treated group
• 20.75 compared to 10.3%
• Glueck et al. showed that males with
undiagnosed hypercoaguable states had more
DVTs and PE in the treated group

Morganthaler AnalysisMayo Clinic
• Reviewed over 100 studies.
– Found the same 4 suggesting Increased CV Risk
• The rest had no evidence of increased CV risk.
– Showed improved CV Function.
– Increased Benefit for older men.
Morganthaler, A et al Mayo Clin Proceed Feb 2015;2:p224-251

Medical Letter
• Adverse reactions to TRT include:
• Gynecomastia
• Acne
• Edema
• Polycythemia
• No Convincing evidence of increased Prostate Cancer
• Needs further study for CVD
JAMA Vol: 315#14; pp12-14

QTc interval
• Felt to be measure of Cardiac Repolarization
– Short QTc goes with fewer cardiac problems
• Shortens in Men age 9-50
• Starts to prolong at age 60 or with low T
• Studies show Men with Low T have long QTc
• Charbit, van Noord & Picori Giraldi have
shown hypogonadal males treated with
Testosterone have short QTc intervals

Hypogonadal Males Treated with
Testosterone
• Shores et al studied 1031 Males at VA
– Showed increased mortality in the untreated
group compared to treated group
• 20.75 compared to 10.3%
• Glueck et al. showed that males with
undiagnosed hypercoaguable states had more
DVTs and PE in the treated group

J.Brent Muhlestein, MD
Intermountain Heart Institute
American Heart Ass. Scientific Session
March 2016
• No increase in major CV events including MI
or CVAs in healthy men > age 50.
– 1472 men age 52 – 63 followed for 3 years
• Decrease in MI, CVA and death was seen.
• European Heart Journal 2015

Mayo Clinic Study
30 day Re Hospitalization Rate
• 6372 non surgical Pts. age 66+ with Low T
Re hospitalization rate
• 9.8% re hospitalization for pts on TRT
• 13% for those not treated with TRT
Mayo Clin Proc 5,2016:91(5) 587-595

Wallis Study
• 10,311 men aged 66+ on TRT for 5 years
• Men on TRT had lower death rate and CV
events.
• Short term Rx increased Mortality & CV
• Long Term Associated with lower Death rate
and CV events
Wallis CJ et al Lancet Diabetes Endocrionol
http://dxdoi.org/10.1016/s2213-8587(16)00112-1

Multiple Articles Show Benefit of TRT49
• Low levels of endogenous testosterone and increased mortality 8
• Low testosterone levels and increased incidence of coronary
• artery disease 6
•
• Low testosterone level correlates with increased severity of
• coronary artery disease 4
•
• Low endogenous testosterone level and increased carotid
• intima-media thickness 8
•
• TRT decreases obesity 6
• TRT improved cholesterol levels (meta- analysis) 3
• TRT improves glycemic control 6
• TRT decreases markers of inflammation 8

Corona Meta-analysis of TRT and
CV events (MACE)
• Available evidence “does not support a causal
• Role between testosterone supplemental and
adverse CV events when hypogonadism is
properly diagnosed and replacement therapy
correctly preformed”.
• Corona G, et al. Expert Opin Drug Saf. 2014;13: 1327-51.

American Association of Clinical
Endocrinologists and American college
of Endocrinology
• There is no compelling evidence that testosterone
• therapy either increases or decreases cardiovascular
• risk.
• • Large-scale prospective randomized controlled trials
• on testosterone therapy, focusing on cardiovascular
• benefits and risks, are clearly needed.
• • As with therapeutics in general, common sense,
• experience, and an individualized approach are
• recommended
• Endocr Pract. 2015;21:1066-1073

50 + Years of Testosterone Rx
• Why After 50 years do we need more studies?
• 2 very Large VA Studies had shown:
1. Decreased Mortality in Men Using T
2. No Increase in CVD Incidents
• Could it be the Advent of the more Expensive
Patch and Gel?
•

50 + Years of Testosterone Rx
• Steven Nissen?
– This story should not be about the use of
testosterone therapy, it should be about the abuse
of testosterone therapy“
– “I think until proven otherwise, we should
consider these supplements to be unsafe for
men”.
– “More studies are needed”

Have you or a loved one suffered a Heart
attack, Stroke or DEATH from Testosterone
replacement?
Injured by Testosterone Supplements?
Call now for money you deserve.

The Legal Examiner
• Cleveland Clinic Dr. Warns about Testosterone Risks
• Posted by Gregory SpizerOctober 29, 2014 11:23 AM
• Comments Off
• inShare
• Renowned Cleveland Clinic cardiologist Steven Nissen, MD is advising men to stop taking medication to treat low testosterone (low-T) caused by aging.
• In his recent article, “Why Your Low-T Medications May Not Be Safe,” Nissen warns men looking to counteract the effects of aging not to start taking low-T medications, and he suggests current users discontinue use.
• A U.S. Food and Drug Administration (FDA) advisory panel recently recommended that doctors limit the use of testosterone drugs to men diagnosed with low-T as a result of a medical condition, such as pituitary or testicular disease.
• The panel’s recommendations would exclude millions of men who are taking low-T drugs to treat low testosterone levels caused by aging.
• The FDA panel also recommends that low-t drug makers explore possible testosterone-related heart attack and stroke risks. A 2014 Journal of the American Medical Association (JAMA) study suggested that men taking testosterone had an increased risk of suffering a heart attack or stroke.
• Nissen recommends that men taking testosterone drugs talk to their doctor to determine whether it is medically necessary. He discourages men from relying on it to feel or look younger, as they may be putting their health at risk.
• A number of men who suffered a heart attack or stroke while taking low-T drugs have filed testosterone lawsuits. Men who want to take legal action after suffering a testosterone heart attack or stroke are urged to contact a testosterone lawyer to discuss their legal rights.
• Tags: testosterone heart attack, testosterone lawyer, testosterone stroke

Signs of Low Testosterone
• Incomplete sexual development
• Breast discomfort, gynecomastia
• Increased body fat
• Reduced muscle bulk and strength
• Lack of effect of PDE5 inhibitors for erectile dysfunction
• Low BMD
• Loss of body hair (auxiliary and pubic), reduced shaving
• Low or zero sperm count
•
Adapted from Bhasin S, et al. J Clin Endocrinol Metab. 2006;91:1995-2010.

1. Do you have a decrease in libido (sex drive)?
2. Do you have a lack of energy?
3. Do you have a decrease in strength and/or endurance?
4. Have you lost height?
5. Have you noticed a decreased enjoyment of life?
6. Are you sad and/or grumpy?
7. Are your erections less strong?
8. Have you noticed a recent deterioration in your ability to play sports?
9. Are you falling asleep after dinner?
10. Has there been a recent deterioration in your work performance?
Screening for Low T
If the answer is yes to question 1 or 7, or at least three of the other questions, low
testosterone may be present.
Morley JE, et al. Metabolism. 2000;49(9):1239-1242.
Androgen Deficiency in Aging Males (ADAM) Questionnaire

Symptoms of Low Testosterone
Adapted from Bhasin S, et al. J Clin Endocrinol Metab. 2006;91:1995-2010.

Male Hormonal StatusChanges With Age as SHBG Increases
Gray A, et al. J Clin Endocrinol Metab. 1991;73:1016-1025.
nm
ol/
L
0
10
20
30
40
50
60
70
80
<3435-44 45-54 55-64 65-74 >75
Age (y)
Total Testosterone SHBG
~288 ng/dL ~576 ng/dL
As SHBG increases with age, levels of free testosterone decrease

Diurnal Variation in Serum Total
Testosterone LevelsTo
tal
Test
ost
ero
ne
(n
g/d
L)
Time
8 am noon 4 pm 8 pm midnight 4 am 8 am
Older Men
Young Men
Bremner WJ et al. J Clin Endocrinol Metab. 1983;56:1278-1281.
400
500
600
700
800

SHBG = sex-hormone binding globulin.
Adapted from Braunstein GD. In: Basic & Clinical Endocrinology. 5th ed. Stamford, Conn: Appleton & Lange; 1997:422-
452.
Circulating Testosterone
2% 38% 60%

Diagnosing Hypogonadism
• Signs and symptoms1
• Clinical laboratory diagnostic tests1
– Total testosterone levels (<300 ng/dL)*
– Bioavailable testosterone (<70 ng/dL)
– Free testosterone (<50 pg/mL)
• Screening tools
– ADAM (Androgen Deficiency in the Aging Male) Questionnaire2
– AMS (Aging Males' Symptoms) Scale3
– MMAS (Massachusetts Male Aging Study) Questionnaire4
*Most frequently used lab test for the diagnosis of hypogonadism.
1. AACE Hypogonadism Task Force. Endocrinol Pract. 2002;8:439-456; 2. Morley JE, et al. Metabolism. 2000;49:1239-1242; 3.
Moore C, et al. Eur Urol. 2004;46:80-87; 4. Smith KW, et al. Clin Endocrinol. 2000;53:703-711.

57
Additional Tests
• LH and FSH
– To ascertain whether cause is primary or
secondary
• Serum prolactin
– High prolactin levels may suggest presence of
pituitary tumor
Braunstein GD. Testes. In: Basic & Clinical Endocrinology. 5th ed. Stamford, CT: Appleton &
Lange; 1997:403-433. Tenover JL. Endocrinol Metab Clin North Am. 1998;27:969-987.

Further Diagnostic Recommendations
Primary Hypogonadism� Karyotype to rule out Klinefelter syndrome
Secondary Hypogonadism� Measure serum prolactin, iron saturation, and other pituitary hormones
� Obtain MRI if
� Severe secondary hypogonadism (TT <150 ng/dL)
� Hyperprolactinemia
� Other pituitary-hormone deficiency (panhypopituitarism)
� Symptoms/signs of tumor-mass effect(headache, visual-field defect, or impairment)
TT = total testosterone
MRI = magnetic resonance imaging.
Bhasin S, et al. J Clin Endocrinol Metab. 2006;91(6):1995-2010.

Testosterone Replacement Therapy
TRT

Testosterone-Replacement Therapy
Dosing and Administration
Intramuscular Injection
�Testosterone enanthate or cypionate
�75-100 mg weekly or 150-200 mg every 2
weeks
Transdermal Patches (Nonscrotal)
�2.5-7.5 mg applied nightly for 24 hours*
Transdermal Gels 1%
5-10 g applied daily (5-10 mg testosterone systemically
absorbed)
Buccal Tablets
�30 mg tablet applied to the buccal mucosa
every 12 hours
Pellets
�150-450 mg implanted subcutaneously every
3-6 months†

Transdermal Gels Are the Most
Commonly Prescribed Form of TRT
IMS NPA; 2008.

*Schematic representation; not an actual study.
Testosterone Levels After
Replacement With Gel or Injection*
Gel Injection
Time (d)
0
0 3 5 7 12 17 21 30 34
Normal range of
testosterone
Testosterone
Sub-therapeutic levels
of testosterone
300 ng/dL
1000 ng/dL

TRT Replacement
• Injections
– Mood swings
– Polycythemia – Strokes or AMI
• Oral Tablets – Methyl Testosterone
– Toxic Hepatitis
• Skin Patches
– Skin Reactions
• Pellets
– Infection
• Gels
– Transference to partner

Monitoring After Initiation of
Testosterone Replacement Therapy
Adapted from Bhasin, et al. J Clin Endocrinol Metab. 2006;91:1995-2010 and Rhoden EL, et al. N Engl J Med.
2004;350:482-492.

What About Prostate Cancer?
• Geriatric patients may be at an increased risk for prostatic
hyperplasia and prostatic carcinoma
• PSA levels in hypogonadal men are often abnormally low1,2
– TRT may increase PSA levels reflecting normalization and typically
plateau within 12 months of initiating therapy
– Increases in PSA levels beyond this warrant further screening
1. Bhasin, et al. J Clin Endocrinol Metab. 2006;91:1995-2010; 2. Miner M, et al. Postgrad Med. 2008;120:130-153.

Original Basis for Concern• Castration caused prostate cancer regression, and T administration caused progression
(Huggins C, et al., 1941)
• Case reports of conversion of occult cancer into clinically apparent lesions
Current View• Prevalence rate of prostate cancer in TRT patients similar (1.1%) to that found in general
population (over 6-36 months)
• Despite decades of work, there is no compelling evidence that testosterone has a causative
role in prostate cancer
• Prostate cancer prevalence increases as T levels decline
• Studies show no significant differences in testosterone levels between those who develop
prostate cancer and those who do not
Future Direction
• The Institute of Medicine and National Institute of Aging are embarking on studies to further
evaluate causality
Testosterone and Prostate Cancer Concerns and Current Views
T = testosterone; TRT = testosterone-replacement therapy.Huggins C, Hodges CV. Cancer Res. 1941;1:293-297; Liverman CT, Blazer DG. Executive Summary. In: Testosterone
and Aging: Clinical Research Directions. Washington DC: The National Academies Press; 2004:1-9.
Rhoden EL, Morgentaler A. N Engl J Med. 2004;350(5):482-492.

� Serum PSA concentration >4 ng/mL
� An increase in serum PSA >1.4 ng/mL within any 12-month period of T
replacement
� A PSA velocity of >0.4 ng/mL/yr using the PSA level at 6 months after
initiation of T replacement as the reference
� Only applicable if PSA data are available for a period
>2 years
� Detection of prostatic abnormality on DRE
AUA = American Urological Association; DRE = digital rectal exam; IPSS = International Prostate
Symptom Score; PSA = prostate specific antigen.
Bhasin S, et al. J Clin Endocrinol Metab. 2006;91(6):1995-2010.
Reasons for Urological Consultation

Benefits of TRT

• Testosterone
• and Depression
• An overview of older studies shows
• mixed results regarding the relationship
• between testosterone levels in men and
• depression1
• However several well-controlled studies
• indicate that endogenous testosterone
• levels are lower in depressed aging men
• than in healthy subjects *2,3
• In particular, low bioavailable
• testosterone levels in aging men
• correlate strongly with depression *3
• 1 Margolese HC, J Geriatr Psychiatry Neurol 2000;13(2):93-101.
• 2 Schweiger et al. Psychosom Med 1999;61(3):292-6 .
• 3 Barrett-Connor et al. J Clin Endocrinol Metab 1999;84(2):573-7.
• Testosterone
• and Cognitive Function
• Cognitive measures demonstrate significant
• correlation with plasma bioavailable
• testosterone levels in some, but not all
• studies
• Plasma testosterone levels influence the
• performance of cognitive tasks with positive
• correlations with spatial tests and negative
• correlations with verbal tests
• Plasma testosterone is lower in men with
• Alzheimer’s Disease than in healthy men
• 1Yliskoski et al. 1999.2Morley et al., 1997.3Perry et al.
• 2001.4Kimura et al., 1994. 5Christiansen and Knussmann,
• 1987.6Ahlbom et al. 2001.7Hammond et al. 2001.8Hogervorst et
• al. 2001.

70
Goals and Benefits of Testosterone
Replacement Therapy
• Improve libido and improve erectile function
• Improve body mass and strength
• Improve bone mineral density
• Improve energy level
• Improve mood/sense of well-being
Petak SM, et al. AACE Clinical Practice Guidelines. Available at: http://www.aace.com/clin/guidelines/hypogonadism.pdf.Tenover JL. Endocrinol Metab Clin North Am. 1998;27:969-987.Wang C, et al. J Clin Endocrinol Metab. 2000;85:2839-2853. Katznelson L. Baillières Clin Endocrinol Metab. 1998;12:453-470.

Improvement in Sexual Function
Parameters• 90-day study in 406 hypogonadal men
– Randomized, multidose, multicenter, active, and placebo controlled
• Significant improvement from baseline vs placebo included
– Motivation (P<0.05)
– Performance (P<0.05)
– Desire (P<0.01)
– Spontaneous erections (P<0.001)
• An additional open-label extension study supported these
data
Steidle C, et al. J Clin Endocrinol Metab. 2003; 88:2673-2681.

Dean J, et al. Rev Urol. 2004;(suppl 6):S22–S29.
Significant and Sustained Improvement in Sexual
Performance* With TRT(in 12-month extension study following 90-day pivotal trial)
Me
an
We
ek
ly S
core
(Se
lf-r
ep
ort
ed
Qu
est
ion
na
ire
)1.6
0 3 9 12
1.4
1.2
1
0.8
6
*Based on average number of days with orgasm, ejaculation,
intercourse, masturbation, or erection in response to sexual activity.
Open-label Extension Study Month
↑↑↑↑ 76.6%P<0.001

Significant Improvement in Body
Composition With TRT(in 12-month extension study following 90-day pivotal trial)
Dean J, et al. Rev Urol. 2004; 6(suppl 6):S22–S29.
Fat Mass
Me
an
Ch
an
ge
Fro
m B
ase
lin
e (
lb)
0 3 6 9 12
0
-1.1
-2.2
-3.3
-4.4
-5.5
Lean Body Mass
Me
an
Ch
an
ge
Fro
m B
ase
lin
e (
lb)
5.5
4.4
3.3
2.2
1.1
0
0 3 6 9 12
Open-label Extension Study Month
−4.84 lbP<0.0001
↓↓↓↓3.96 lbP<0.0001
Open-label Extension Study Month

74
Results after 36 Months of
TRT Therapy: Sexual Function
Sexual desire
0
1
2
3
4
5
0 6 12 18 24 30 36
Month
Se
xua
l d
esi
re (
0-7
)
Satisfaction with erection
0
1
2
3
4
5
6
0 6 12 18 24 30 36
Month
Sa
tisf
act
ion
(0
-7)
p=0.000
1
p=0.000
1
Wang C, et al. J Clin Endocrinol Metab. 2004;89(5):2085-2098.

75
Results after 36 Months TRT Therapy: Bone Mineral Density
Change Hip BMD
−−−−0.01
0.00
0.02
0.03
0.04
0 6 12 18
Month
Ch
an
ge
hip
BM
D (
g/c
m2)
363024
0.01
Change Spine BMD
0.00
0.02
0.04
0.06
0 6 12 18
Month
Ch
an
ge
sp
ine
BM
D (
g/c
m2)
363024
Wang C, et al. J Clin Endocrinol Metab. 2004;89(5):2085-2098.

76
Results after 36 Months of TRT Therapy: Effect on
Mood
Positive Moods
4.5
5.0
5.5
Month
Po
siti
ve
mo
od
s (0
-7)
Negative Moods
1.00
1.25
1.50
1.75
2.00
Ne
ga
tiv
e m
oo
ds
(0-7
)
p=0.0022p=0.0013
0 6 12 18 24 30 360 6 12 18 24 30 36Month
Wang C, et al. J Clin Endocrinol Metab. 2004;89(5):2085-2098.

77
Contraindications and Relative Contraindications of Testosterone Replacement Therapy
• Known or suspected prostate cancer
• Known or suspected carcinoma of the breast
• Prostatic hyperplasia in geriatric patients
• Sleep apnea (may exacerbate condition; patients should be
treated for sleep apnea first [CPAP])
• Edema with or without congestive heart failure
• Patients with polycythemia
• Is not indicated for women, has not been evaluated in
women, and must not be used in women.

Contraindications� Male breast cancer
� Prostate cancer (known or suspected)
� Use in pregnant or breast-feeding women
� Known or suspected sensitivity to ingredients used in T delivery systems
Precautions� Benign prostatic hyperplasia (BPH)
� Lower urinary tract symptoms (LUTS)
� Edema in patients with preexisting cardiac, renal, or hepatic disease
� Gynecomastia
� Precipitation or worsening of sleep apnea
� Azoospermia
� Testicular atrophy
Testosterone-Replacement TherapyContraindications and Precautions
BMD = bone mineral density; DRE = digital rectal exam; PSA = prostate specific antigen;
TRT = testosterone-replacement therapy.
Bhasin S, et al. J Clin Endocrinol Metab. 2006;91(6):1995-2010.

79
Conclusions
• Hypogonadism in adult men is often unrecognized
• Known diseases of aging are associated with an increased
decline in testosterone
• Low testosterone is characterized by changes in the
body fat/lean muscle ratio; bone mineral density; cognition,
memory, and mood; and sexual desire and function
• Before prescribing be sure that it is needed
• Check Levels to be sure that they do not go too high.

What about Women

Women - Symptoms
• Symptoms:
– Decreased sexual desire
– Decreased sexual thoughts & fantasies
– Decreased strength
– Decreased genital response & orgasim
– Decreased lubrication

What about Women
• Can they have low testosterone levels?
• 43% age 18 – 59 suffer from sexual
dysfunction

Low Testosterone Levels
in Women
• Age Total Free
• <50 <25 ng/dl <1.5 pg/ml
• >50 <20 ng/dl <1.0 pg/ml
Guay, A & Davis, S
http://www.bumc.bu.edu/sexualmedicine/publications/testosterone
-insufficiency-in-women-fact-or-fiction

Women and Testosterone
• All women make testosterone
– ¼ from Ovaries
– ¼ from Adrenals
– ½ Peripheralally
• In US no testosterone product is indicated in
women.

Women and Testosterone
• Precursors of testosterone
– DHEA
– DHEA Sulfate
• DHEA has been suggested as treatment for
women
• Over the counter

Endocrine Society Guidelines
• Put together a task force to create Guidelines
• Unable to come up with guidelines
• Too many things were not standardized

Guidelines – British Society for
Sexual Medicine
YES NO
Sexual Distress +
Psychosexual problems
Counseling Counseling
May consider Pharmacology
Sexual distress+
Medical Problems
Treat Medical problem Pharmacology may be
appropriate
Postmenopausal
Psychosexual
Sexual Distress
Counseling
Pharmacology may be
appropriate
Generalized therapy not
recommended
SHBG > 160 Testosterone not appropriate Pharmacology may be
appropriate

Thank You!