Embed Size (px)
Citation preview
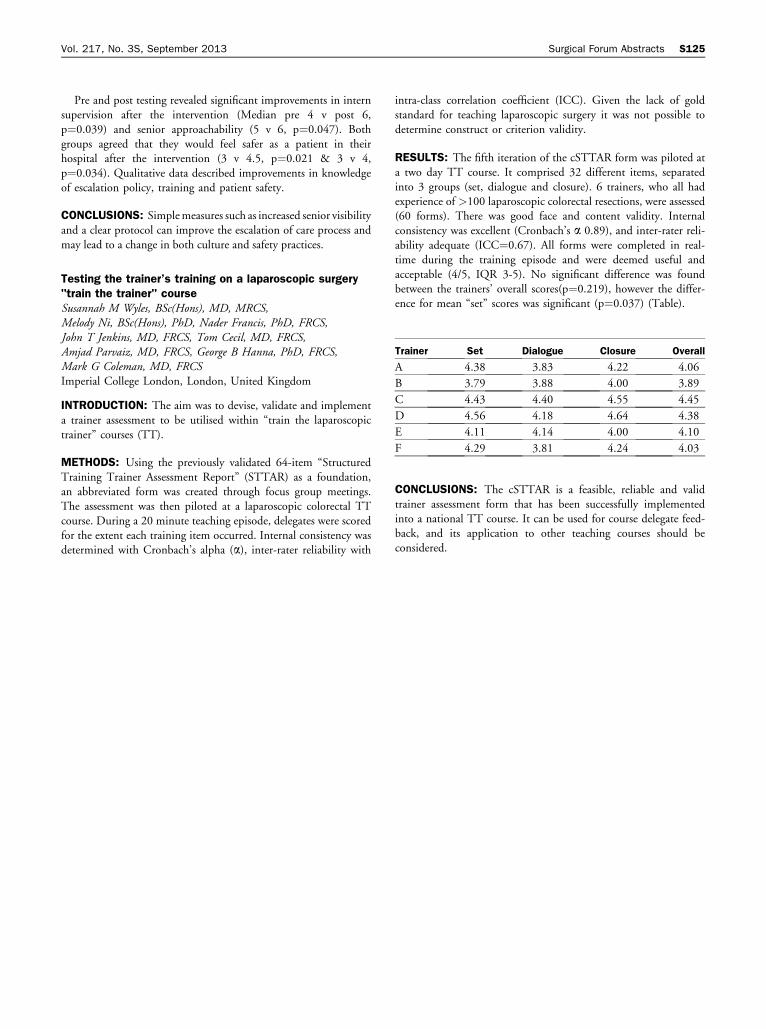
Trainer Set Dialogue Closure Overall
A 4.38 3.83 4.22 4.06
B 3.79 3.88 4.00 3.89
C 4.43 4.40 4.55 4.45
D 4.56 4.18 4.64 4.38
E 4.11 4.14 4.00 4.10
F 4.29 3.81 4.24 4.03
Vol. 217, No. 3S, September 2013 Surgical Forum Abstracts S125
Pre and post testing revealed significant improvements in internsupervision after the intervention (Median pre 4 v post 6,
p¼0.039) and senior approachability (5 v 6, p¼0.047). Bothgroups agreed that they would feel safer as a patient in theirhospital after the intervention (3 v 4.5, p¼0.021 & 3 v 4,
p¼0.034). Qualitative data described improvements in knowledgeof escalation policy, training and patient safety.
CONCLUSIONS: Simplemeasures such as increased senior visibilityand a clear protocol can improve the escalation of care process and
may lead to a change in both culture and safety practices.
Testing the trainer’s training on a laparoscopic surgery"train the trainer" courseSusannah M Wyles, BSc(Hons), MD, MRCS,Melody Ni, BSc(Hons), PhD, Nader Francis, PhD, FRCS,John T Jenkins, MD, FRCS, Tom Cecil, MD, FRCS,Amjad Parvaiz, MD, FRCS, George B Hanna, PhD, FRCS,Mark G Coleman, MD, FRCSImperial College London, London, United Kingdom
INTRODUCTION: The aim was to devise, validate and implementa trainer assessment to be utilised within “train the laparoscopic
trainer” courses (TT).
METHODS: Using the previously validated 64-item “StructuredTraining Trainer Assessment Report” (STTAR) as a foundation,an abbreviated form was created through focus group meetings.The assessment was then piloted at a laparoscopic colorectal TT
course. During a 20 minute teaching episode, delegates were scoredfor the extent each training item occurred. Internal consistency wasdetermined with Cronbach’s alpha (a), inter-rater reliability with
intra-class correlation coefficient (ICC). Given the lack of goldstandard for teaching laparoscopic surgery it was not possible to
determine construct or criterion validity.
RESULTS: The fifth iteration of the cSTTAR form was piloted ata two day TT course. It comprised 32 different items, separated
into 3 groups (set, dialogue and closure). 6 trainers, who all hadexperience of >100 laparoscopic colorectal resections, were assessed(60 forms). There was good face and content validity. Internal
consistency was excellent (Cronbach’s a 0.89), and inter-rater reli-ability adequate (ICC¼0.67). All forms were completed in real-time during the training episode and were deemed useful and
acceptable (4/5, IQR 3-5). No significant difference was foundbetween the trainers’ overall scores(p¼0.219), however the differ-ence for mean “set” scores was significant (p¼0.037) (Table).
CONCLUSIONS: The cSTTAR is a feasible, reliable and validtrainer assessment form that has been successfully implementedinto a national TT course. It can be used for course delegate feed-back, and its application to other teaching courses should be
considered.