Embed Size (px)
Citation preview
Abstract—Functional electrical stimulation is a therapy based procedure where muscles are activated via electrical signals to target stimulation of lost connection between the CNS and motor neurons. During FES application, patients are retaught basic movements and functions through the use of ergometers or simple therapy instructions. Loss of muscular control and peripheral nerve damage are the basic reasons for need of biopotential feedback . Often, in patients with SCI, use of EEG is an effective way to track electrical activity in the brain whilst movements are done. Lack of a neural system to efficiently translate messages to extremities for action can qualify an individual for both FES and BCI interaction. Thus, EEG is often used in conjunction with BCI to get a biopotential feedback for control systems with SCI or paralysis patients. BCI-FES systems that are monitored with help of EEG feedback have proven to be helpful in restoration of motor control, and compared to EMG feedback, and often proves as being more reliable. [2] However, in many FES studies, a phenomenon known as the carryover effect has been recorded to take place. This effect is when patients regain the ability to complete motor tasks after stroke or SCI, thought to be triggered from FES and rehabilitation of muscle memory. However, the period of time where carryover is present and initiates is unknown. This experiment is designed to see if there is a correlation between FES therapy time and duration of carry-over persisting or occurring in a patient. Foot drop patients were grouped into 3 sub groups all with varying time periods of applied therapy, ranging from 6 months to 1 year. The FES system was made up of an EEG-BCI interface connected to a feedback loop to allow stimulation of the peroneal nerve. A capacity score based algorithm on how much improvement within a time frame occurred as a result of carryover was used to detect the phenomenon.
I. INTRODUCTION
Functional electrical stimulation aids to help patients recover movement of lost extremity control from stroke or SCI, especially when administered over a long time period with frequent therapy sessions. Both duration of stimulation and type are large factors in the determination of neural plasticity producing the carryover effect in a patient.
However, the carryover effect has no true trigger, therefore its classification of occurring can vary. We are still unsure of when FES ends and voluntary control takes over. If this range of time was found, then therapeutic stimulation to those with SCI and stroke could be narrowed down to a specific range to allow patients to potentially see and be somewhat guaranteed (based on therapy sessions) some sort of control of lost muscle mass again. These time frames can be tested and applied on different types of trauma to 5/4/16. This work was supported by the UB Biomedical Engineering
Department. Emily Koehler, Biomedical Engineering undergraduate, University at
Buffalo. [email protected]
broaden our understanding of cortical remapping. FES systems and clinical therapy would be able to modify current procedures in rehabilitation to allow for a window of maximal time where carryover can be initiated.
II.BACKGROUND
A. Spinal Cord InjuryThe spinal cord is the site of motor and sensory stimulation passing through the central nervous system and the rest of the human body. According to the NSCSC, there are near 12,500 new SCI injuries per year in the United States, with an average age of 42. [1] Sensory and motor neurons as well as spinal tracts exist within the spinal cord, as axons propagate out of the tract into the body for contact. The spinal cord consists of the cervical spine, thoracic spine, lumbar and sacral areas. Each can be used to classify a type of SCI, depending on where damage occurred. [2]
Loss of muscular control and peripheral nerve damage are the reason for incorporation of biopotential feedback. [6] Lack of a neural system to efficiently translate messages to extremities for action qualifies an individual for both FES and BCI interaction.
B. Foot drop and the Peroneal NerveFoot drop happens often in SCI and stroke patients, where the patient’s foot dips downward and drags as a step is taken. This results from weak dorsiflexors, and also weak or lack of total mobility of the plantar flexors. Spasticity in this area as well is common, resulting in poor control.
The use of FES with foot drop has been shown to increase gait velocity, yet often many tests are done in an unrealistic setting; a small distance with even ground. More challenging surfaces are not usually incorporated into the study mainly for the purpose of achieving basic walking by
themselves, but experiments like these have been done in accordance with endurance and stride time variability.
The peroneal nerve is directly related to foot dorsiflexion, and stimulates the top of the foot to lift upwards and flex. This is the site of stimulation when applying electrodes.
Testing for the carry-over loss time period of SCI patients via FES in conjunction with BCI
(May 2016)Emily Koehler, Undergraduate Biomedical Engineering
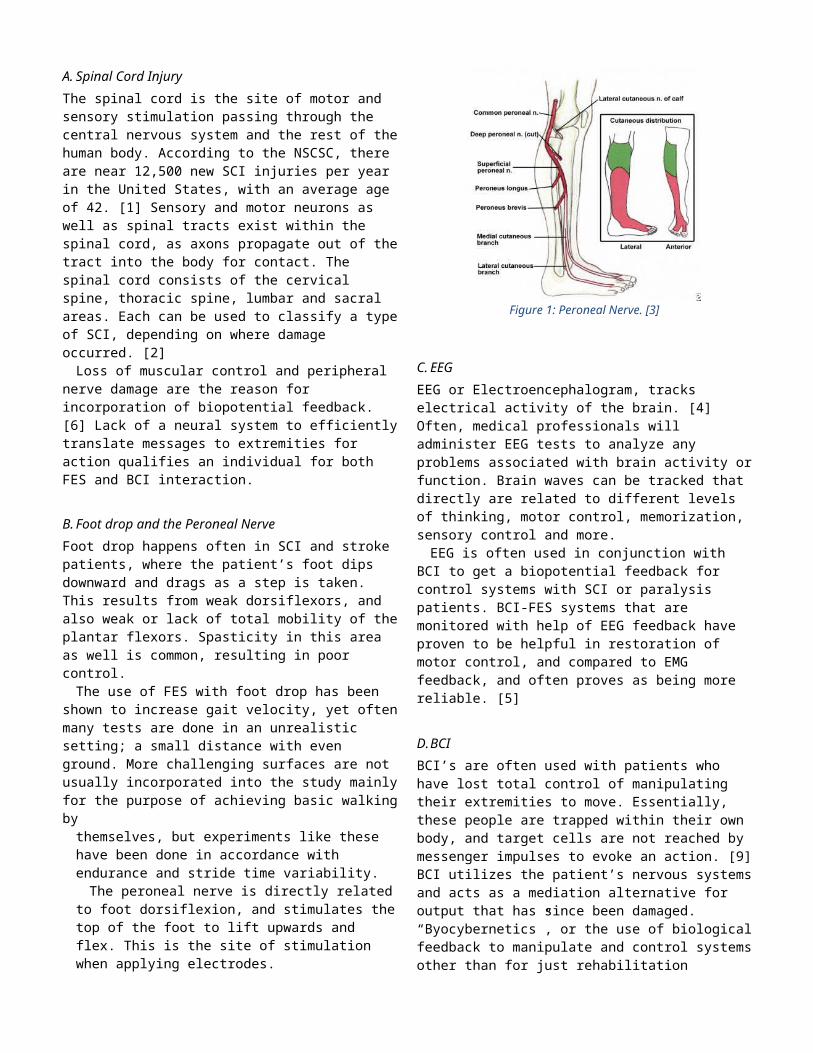
Figure 1: Peroneal Nerve. [3]
C.EEGEEG or Electroencephalogram, tracks electrical activity of the brain. [4] Often, medical professionals will administer EEG tests to analyze any problems associated with brain activity or function. Brain waves can be tracked that directly are related to different levels of thinking, motor control, memorization, sensory control and more.
EEG is often used in conjunction with BCI to get a biopotential feedback for control systems with SCI or paralysis patients. BCI-FES systems that are monitored with help of EEG feedback have proven to be helpful in restoration of motor control, and compared to EMG feedback, and often proves as being more reliable. [5]
D.BCIBCI’s are often used with patients who have lost total control of manipulating their extremities to move. Essentially, these people are trapped within their own body, and target cells are not reached by messenger impulses to evoke an action. [9] BCI utilizes the patient’s nervous systems and acts as a mediation alternative for output that has since been damaged. “Byocybernetics”, or the use of biological feedback to manipulate and control systems other than for just rehabilitation purposes has large applications, but as for now is mainly constrained in research trials. These systems take in the usual commands given by the nervous system for specific actions, send them to the interface where they are translated into physical controls by means of an algorithm. [10] Motor imagery, or the portrayal of movement without such movement through data, assists both the one administering the EEG and the patient in the cognitive process.
E. BCI and FESBCI analyzes all types of neural signals, including predicted and non-predicted signals. These unpredicted signals are not usually in synch, and therefore might suggest some level of cognitive deficiency. As of recent study, BCI-FES systems have been implemented mainly with upper extremities only. For example, a group at the University at California developed
a BCI-FES system to motivate walking in conjunction with EEG signals, specifically foot dorsiflexion. Once the patient became accustomed to the FES, the BCI system was incorporated. Movements were made by the patient to their best degree, then stimulation through the FES was administered to excite the muscle groups to further activate a walking motion. A parastep system was incorporated. Prior to the actual experiment, they also were required to go through a BCI training period. The brain control interface introduced a virtual reality environment, where a patient would try and manipulate movements by being in a false environment while still immobile. Thus, EEG signals were gathered from this part of the training and analyzed to better understand the relationships made between these attempts at motor control. The FES helped to accommodate specific subjects based on time and complexity of the movements they were capable of. Full FES training was performed to the point where the patient would be able to walk a set distance without exterior help from anyone. After they mastered this, the BCI was integrated. [10] Lower extremity control, while important, usually is secondary to motor control of the upper body. Wheelchair accessibility often can replace or restore mobility to patients with lower extremity paralysis, while upper paralysis does not have much of a common replacement. In addition, lower extremities are believed to stimulate more noise and stimuli compared to upper body (walking/stepping as opposed to grasping and flexing of arms) and thus would need more specified EEG algorithms to cancel out this excessive data. [10]
F. Carryover EffectThe “carryover” effect is an unusual situation in
which a patient regains lost muscle memory post trauma (SCI or paralysis). This phenomenon is linked to some sort of stimulation, either deriving from the central nervous system or the peripheral nerves themselves that induce therapeutic connections with past physical mobility. The hypothesis is that FES therapy helps reconnect and retrain the neural-motor pathways that have been damaged but previously been used successfully. Neural plasticity, or the imprinted ability to perform or complete a task from being done repetitively in a previous state, in some way still exists after the damage. FES in some cases has seemed to initiate carry-over, but it also has been seen in cases where FES was not implemented. [10] This proves the fact that carry over is still a sort of mystery, and that its true cause is yet to be discovered.
Post stroke patients number one focus mainly is gait improvement. [11] However, the carry over effect has occurred in other areas besides lower extremity muscles, but is most often tested for in the lower hemisphere. Various mechanisms have been hypothesized to induce the carry-over effect, including central therapeutic benefits and also peripheral mechanism benefits from patients being treated via FES. Peripheral mechanisms, with regards to small nerve endings of bone, skin, muscle and other tissue, are stimulated and translate signals to our brain. These peripheral nerves have been guessed to regenerate to some degree after stroke or serious CNS damage. [12] With the help of FES, improvements in peripheral mechanisms are believed to be
one area for possible reasons where carry-over can be initiated. Ideas like strengthening remaining pathways post trauma, improvement of flexibility and stretch degree of the extremity, and a degradation of spastic movement in the extremity all have been thought of to be reasons good enough for inducing the effect. Yet, after further analysis, each proves to have implications that would prove it to be the best reason possible for the phenomena. Pathways that are still strong and can be voluntary controlled most likely can be improved upon with just simple exercise, not FES. In addition, passive psychotherapeutic stretching would be a good enough alternative to increasing flexibility of lost muscle mass, not as far as going through FES therapy. Lastly, although FES can improve spasticity, not every muscle area that has spasticity also has the carry-over effect. It has been proven that carry over can also occur in muscle groups that don’t inhibit spastic movements post trauma. [13]
Central therapeutic advantages relate to the central nervous system ultimately being improved upon as a result of functional electrical stimulation. Once again, these are just hypotheses. FES via surface electrodes stimulate motor and sensory neurons, and that stimulation of the affected site can in turn elicit cortical remapping that possibly was not done prior to stimulation. In another sense, high frequency sensory stimulation might be capable of connecting and modifying cortical connections [13]
The brain at adulthood is still capable of recovery from damage, and forming new neural pathways, not believed to be true until recently. [14] Cortical remapping occurs when the CNS is destroyed or impacted by an external or internal stimulus that as a result changes the physiology or makeup. This reorganization can vary, and the extent still isn’t fully understood. Post stroke reorganization usually includes the secretion of growth factors, new copying of gene sequences, neurotransmitter receptor modifications, new synapse and axon creation. [15] Imaging techniques analyze these changes and can link things like thermal activity and spatial resolution to changes in performance. Thus, cortical remapping is very relevant after trauma and might be a carryover cause. [13] The ipsilateral pathway takes over and becomes a main neural pathway to aid connections post stroke. [10] Ipsilateral, meaning same side, has precedence when a specific extremity is in rehabilitation. Therefore, it is this pathway that is often looked at and studied when doing carry-over experimental trials.
Other hypotheses also exist, more of the proprioceptive kind, a mix of central and peripheral stimulation as mentioned earlier. FES coupled with predictive and confident movement of the lost site as a closed loop system native to a patient’s own sensory motor organization has been hypothesized to initiate an ability to correct damage from trauma. [10] Basically, the FES helps to stimulate the area, but the patient is aware and understands how the movement needs to be carried out and what it feels like once it is done. These two aspects combined are thought to have a dual effect on carry over coming into play. This dual effect thus triggers muscle memory, or “neural plasticity” and the regaining of the lost movement occurs. [16]
Other not as prevalent hypotheses for carry-over include antidromic firing and its relationship to Hebb synapses. Antidromic firing, occurring from the opposite impulse travelling down the axon after hitting the anterior horn cell after a motor nerve fiber is activated, can occur when patterns of quick electrical impulses are administered to a site. This can show up on an EMG as a smaller but present wave. [16] This discharge before or almost at the same time as presynapse are called Hebb synapses. These are related to the Hebbian theory, or the adjustment of neurons in the brain when exposed to being in a learning or memory state. The presynaptic cell ultimately affects and strengthens the post synaptic. Basically, a common saying being that “cells that fire together, wire together.” [17] Thus, a cell X usually will fire before a cell Y, and even might strengthen the firing of Y. The almost simultaneous firing of X and Y strengthens the learning process and unity of the cells to perform a task. [16] This all leads to a network of uniform muscle memory and rehabilitation learning, which could provide carry-over clues.
Carryover in this experiment will be assessed by an automatic comprehensive method-logarithm based on minimum variables detected away from normalcy, discovered by a research team testing for functional improvement assessment of therapeutic experiments with FES. This process tests for specific parameters when using FES in patients specific to foot drop, that will contribute to a patient possibly acquiring the carryover effect sometime during the therapy. After data acquisition is finished, information will be inserted into a software that computes a raw score. This raw score, called a capacity score, is tested for before experimental trial, during, and after, to compute progress and improvement time segments. Thus, this raw score is presented as a yes or no statement if carry over has occurred or not. [18]
III. PREVIOUS EXPERIMENTS ON CARRY OVER
For most experiments, carryover is observed at the end of an experiment, or hypothesized to have happened during. One foot drop experimental system used the NESS L300 to use active therapy FES to correct foot drop in a closed loop cycle so the patient could have a system the adjust stimulation in relation to their relative output. Like the parameters of the carryover algorithm, status of foot drop progression was analyzed prior, during therapy, and almost a year after to detect stimulation results and to detect carryover. No modality to categorize the detection of carryover was stated.
In a different study, foot drop as a result of stroke was tested against FES and AFO, ankle-foot orthotics. Stated in this experiment, the peroneal nerve was stimulated during the swing phase of gait through a dual channel FES system. The thought was that the coupled repetitive stimulation to the peroneal nerve with the increased amount of stimulation feedback to the central nervous system would elicitcarryover. They found that after FES was turned off, not increase in walking speed on one’s own was present, but during a static voluntary test some form of voluntary control progress was shown that lead them to believe in a small presence of carryover.
The last case presented was focused on and continued over a duration of 9 months. Patients were assessed for improvement two months and then a year later with both FES and non-FES therapy. 31% of available patients were found to not need any assistance and could completely walk on their own at the one-year period. Carryover was based on a baseline between beginning of therapy and a year later both with neuroprosthesis. A clear definition of how exactly carryover was assessed and analyzed was not presented. They suggest a plateau effect for FES use at which the subject can fully perform on their own past the use of the stimulation, as gait velocity increased past the therapy. Usually gait velocity is either thought to stay constant or recess without stimulation help, but with the recordings after a year without neuroprsthesis still being higher than at the end of the study, carryover was thought to have been the reasoning.
IV. EXPERIMENTAL SECTION
A. Materials and MethodsA group of 30 people will be recruited for this experiment, 15 men and 15 women, all first time SCI patients. Patients will be recruited based on similar injury location sites, to keep variables as constant as possible. 3 groups of 5 will be tested at once (1 15 person FES group and 1 without.) The first group will be exposed to FES for 6 months, the next 9, and then the last 1 year.
Exclusion criteria: degree of ankle flex being less than 5 degrees, language or cognitive defects, inability to walk even if assisted, spasticity at ankle, skin or open wounds at electrode sites, medical issues that may interfere with experiment (neurological or muscular), damaged peroneal nerve, not available for test time period, subjects under 18.[25] Inclusion Criteria: determination of clear spinal cord injury and classification, clear foot drop during gait swing, 6 months at least after injury, informed consent is not an issue. Hemiplegic patients only, as a result of spinal hemiplegia. Note that the situation involving how the patient was affected is not relevant in this study.[25]
Control group: Same age and gender average for each impaired patient, same relative average walking speed and foot drop severity. Keeping our subjects as even as possible will result for the best most unbiased results, so all will be analyzed prior to acceptance into the test with relative uniformity of foot drop severity. The control group will have no FES but all of the same therapy techniques and duration times. They will serve as a basis and utilize the same test and carryover assessment at the end. The goal is to find a clear distinction in carryover present in subjects in one of the three therapy groups that may lean towards a threshold time for carryover to be initiated in conjunction with FES.
Subjects will first be assessed on personal parameters. Each group will have a subsequent control group, with a total of 6 groups each of 5 people. The first group will go through therapy for a period of 6 months, the second 9, and the third a full year. Each will be assessed for capacity score parameters prior to the experiment, halfway through their trial, and then 6 months following.
B. Signal AcquisitionThe EEG cap will consist of 64 electrodes, and 2 electrodes will be placed on the peroneal nerve (high calf, low calf.) Impedance values will be kept at 3 k. Current stimulation will be in the range of 80-100 mA.
Being that this experiment is hypothetical, actual electrical stimulation parameters are vague because of varying factors. Tissue potential damage, surface electrode size, and degradation of the electrode must come to mind, especially in the 1-year group. Waveform would be rectangular, and biphasic to allow for least amount of uncomfortable sensation to patient. Being that we are specifically activating the peroneal nerve, short pulses of less than 200 s will be used. Impedance thus should be low and current evenly spread. [20]
C.Prior Testing for ImpairmentPrior to the experiment to begin, each subject will be
analyzed based on gait velocity, endurance velocity, paretic step length, and obvious clear fluidity in movements/spasticity. To ensure patients have needed inclusion criteria based on SCI similarities, a MRC scale index via ankle dorsiflexion will be used. Grade 3 is wanted index; medium resistance to force and muscle control. Muscle strength is further reduced such that the joint can be moved only against gravity with the examiner's resistance completely removed, based on effort scale of patient. [21]
In addition, every patient will go through a calibration process with the EEG to allow those administering the test to see clear differences between foot dorsiflexion and relaxation, as well as gait movement. This way understanding of various EEG signals will be assumed during testing.
These parameters will be incorporated into the comprehensive assessment discussed earlier in carryover to test for capacity score. The following is a proposed experiment to test for threshold time to in regards to carryover in footdrop patients via FES with a EEG-BCI system.
D.Experimental Set UpBCI will allow patients to control FES on their own and
ideally speed up the neural plasticity aspect of this experiment. The FES system used will stimulate the peroneal nerve via
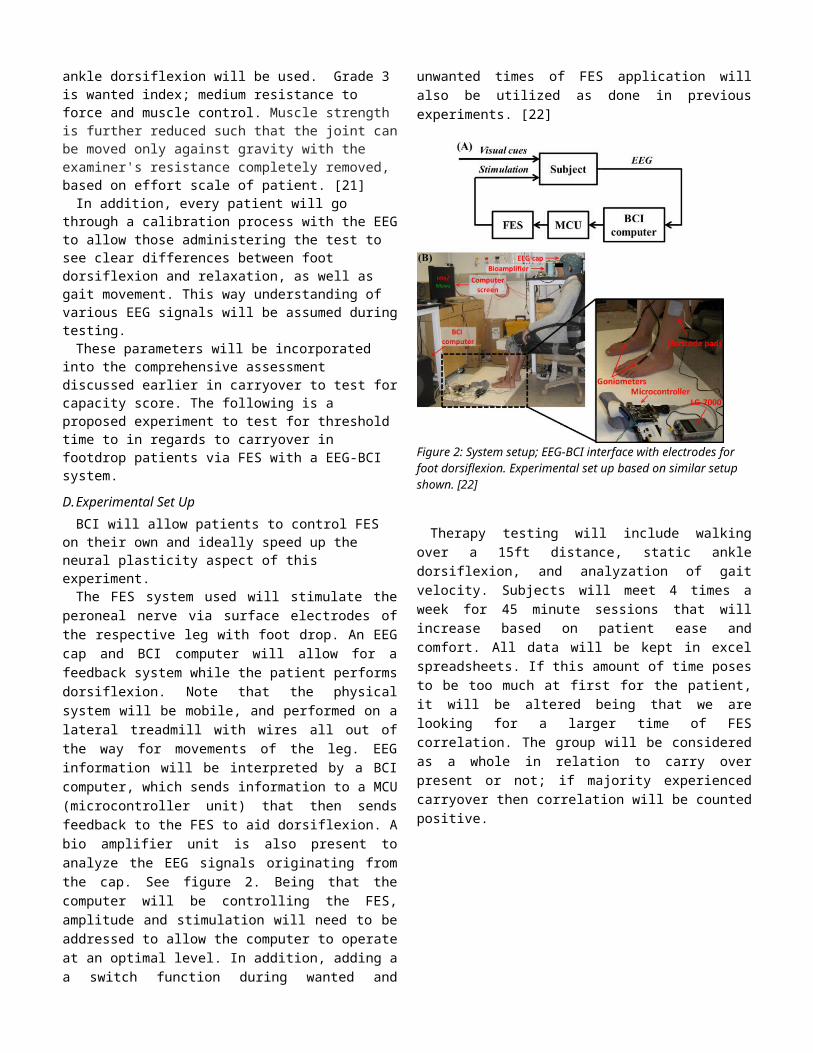
surface electrodes of the respective leg with foot drop. An EEG cap and BCI computer will allow for a feedback system while the patient performs dorsiflexion. Note that the physical system will be mobile, and performed on a lateral treadmill with wires all out of the way for movements of the leg. EEG information will be interpreted by a BCI computer, which sends information to a MCU (microcontroller unit) that then sends feedback to the FES to aid dorsiflexion. A bio amplifier unit is also present to analyze the EEG signals originating from the cap. See figure 2. Being that the computer will be controlling the FES, amplitude and stimulation will need to be addressed to allow the computer to operate at an optimal level. In addition, adding a a switch function during wanted and unwanted times of FES application will also be utilized as done in previous experiments. [22]
Figure 2: System setup; EEG-BCI interface with electrodes for foot dorsiflexion. Experimental set up based on similar setup shown. [22]
Therapy testing will include walking over a 15ft distance, static ankle dorsiflexion, and analyzation of gait velocity. Subjects will meet 4 times a week for 45 minute sessions that will increase based on patient ease and comfort. All data will be kept in excel spreadsheets. If this amount of time poses to be too much at first for the patient, it will be altered being that we are looking for a larger time of FES correlation. The group will be considered as a whole in relation to carry over present or not; if majority experienced carryover then correlation will be counted positive.
V. RESULTS AND DISCUSSION
Figure 4: Mock table for results. The more "Yes" responses to the carryover column after capacity score analyzation means there might be a clue to this group containing threshold time.
A. Proposed ResultsFrom past experiments, the control group most likely will
not benefit as highly from therapy as the FES group did. Assuming this is true will give a positive foundation for our carryover assumptions to focus on.
Ideally, a linear relationship between subject improvement based on the capacity score and therapy time is what we would want to see. A linear improvement however past 1 year would tell us that maybe we haven’t reached a threshold yet that would suggest a FES time period to induce carryover. Capacity scores will be analyzed and give an output of patient’s results. Simple yes or no’s will state for carryover.
However, more positive capacity scores during the middle time therapies may suggest our threshold is around 6-9 months. This is difficult with 5 subjects per group, and as analyzed in other experiments usually subject number drops because of subject availability or factors that can’t be controlled.
Figure 3: Foot dorsiflexion on one's own versus BCI-FES control. Example of EEG data seen in system. [22]
Data like Figure 3 will be used to analyze effort and how the BCI-EEG interaction is working, and is a good example of how data should look after needed calibration and understanding of system setup. [23]
In addition, analyzation of EEG waves will be important if a correlation is found; brainwaves of the central nervous system might hint at cortical remapping of neural pathways needed to correct foot drop.
Increase in gait velocity at the post-rehabilitation checkup from when the experiment was taking place, fluidity of movement, larger angle dorsiflexion and no or little spasticity are ideal outcomes of this experiment,
It is possible that there is no carryover time correlation to FES, and results are inconclusive.
B. Discussion and ConclusionBeing that this is a hypothetical experiment, many of these
parameters would have to be ensured that they won’t play a big role in altering our variables. A majority of the specifics have already been incorporated into FES study, such as successfully BCI-FES integration, foot drop analyzation, but not threshold carryover time. Major areas of concern regarding this experiment’s success revolve around the therapy time. Patients can not all have the same level and type of SCI injury, which provides a basis for error. In addition, motivation of each patient will vary in regards to their training. While one patient might be very dedicated to the process, another in the same or different group might not.
In addition, as we know with EEG slight movements like eye blinks, coughing, swallowing, etc. will show up on an EEG pattern. By having our subjects walk and move as they would normally, we introduce lots of motion artifacts and excess noise that would have to be calibrated out to really see differences in EEG that stand for foot dorsiflexion. Realistically, we might even be able to simplify the system and just stick to an FES system versus threshold time and have stimulation monitored by therapists.
In addition, an apparatus to ensure a moving treadmill with all required features of the system on a moving system as well is needed so that mobility of the subject is not restricted to mobility of the unit.
REFERENCES AND FOOTNOTES
A. References[1]H. Ma, "Spideroak, Whisper Systems, Silent Circle", Technical Services Quarterly, vol. 32, no. 2, pp. 228-229, 2015.
[2]2016. [Online]. Available: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3232636/. [Accessed: 06- May- 2016].
[3]"Diseases & Conditions - Medscape Reference", Emedicine.medscape.com, 2016. [Online]. Available: http://emedicine.medscape.com. [Accessed: 06- May- 2016].
[4]"Electroencephalogram (EEG) | Johns Hopkins Medicine
Health Library", Hopkinsmedicine.org, 2016. [Online]. Available: http://www.hopkinsmedicine.org/healthlibrary/test_procedures/neurological/electroencephalogram_eeg_92,P07655/. [Accessed: 06- May- 2016].
[5]A. Schwartz, "Brain-Controlled Interfaces: Movement Restoration with Neural Prosthetics", Sciencedirect.com, 2016. [Online]. Available: http://www.sciencedirect.com/science/article/pii/S0896627306007264. [Accessed: 06- May- 2016].
[6]S. Fok, R. Schwartz and H. C, "An EEG-based Brain Computer Interface for Rehabilitation and Restoration of Hand Control following Stroke Using Ipsilateral Cortical Physiology", 2016. [Online]. Available: http://ese.wustl.edu/ContentFiles/Research/UndergraduateResearch/CompletedProjects/WebPages/sp11/SamRaphaelChuck/Senior%20Design%20Paper.pdf. [Accessed: 06- May- 2016].
[7]A. Do, P. Wang, C. King, A. Abiri and Z. Nenadic, "Brain-Computer Interface Controlled Functional Electrical Stimulation System for Ankle Movement", Journal of NeuroEngineering and Rehabilitation, vol. 8, no. 1, p. 49, 2011.
[8] Calhoun and G. McMillan, "EEG-based control for human-computer interaction", Proceedings Third Annual Symposium on Human Interaction with Complex Systems., 2016.
[9]"Novel rehabilitation device improves motor skills after stroke", Medicalxpress.com, 2016. [Online]. Available: http://medicalxpress.com/news/2013-12-device-motor-skills.html. [Accessed: 06- May- 2016].
[10]J. SH, "A review of the ipsilateral motor pathway as a recovery mechanism in patients with stroke. - PubMed - NCBI", Ncbi.nlm.nih.gov, 2016. [Online]. Available: http://www.ncbi.nlm.nih.gov/pubmed/19597268. [Accessed: 06- May- 2016].
[11]e. Bauer P, "Functional electrical stimulation-assisted active cycling--therapeutic effects in patients with hemiparesis from 7 days to 6 months after stroke: a... - PubMed - NCBI", Ncbi.nlm.nih.gov, 2016. [Online]. Available: http://www.ncbi.nlm.nih.gov/pubmed/25449195. [Accessed: 06- May- 2016].
[12]N. Donaldson, T. Perkins, R. Fitzwater, D. Wood and F. Middleton, "FES cycling may promote recovery of leg function after incomplete spinal cord injury", Spinal Cord, vol. 38, no. 11, pp. 680-682, 2000.
[13]D. Rushton, "Functional Electrical Stimulation and rehabilitation—an hypothesis", Medical Engineering & Physics, vol. 25, no. 1, pp. 75-78, 2003.
[14]J. Shih and L. Cohen, "Cortical reorganization in the human brain: How the old dog learns depends on the trick", Neurology, vol. 63, no. 10, pp. 1772-1773, 2004.
[15]C. Grefkes and N. Ward, "Cortical Reorganization After Stroke: How Much and How Functional?", The Neuroscientist, vol. 20, no. 1, pp. 56-70, 2013.
[16]P. Wright and M. Granat, "Therapeutic effects of functional electrical stimulation of the upper limb of eight children with cerebral palsy", Dev Med Child Neurol, vol. 42, no. 11, pp. 724-727, 2000.
[17]S. Lowel and W. Singer, "Selection of intrinsic horizontal connections in the visual cortex by correlated neuronal activity", Science, vol. 255, no. 5041, pp. 209-212, 1992.
[18]M. Gandolla, F. Molteni, N. Ward, E. Guanziroli, G. Ferrigno and A. Pedrocchi, "Validation of a Quantitative Single-Subject Based Evaluation for Rehabilitation-Induced Improvement Assessment", Annals of Biomedical Engineering, vol. 43, no. 11, pp. 2686-2698, 2015.
[19]T. Murphy and D. Corbett, "Plasticity during stroke recovery: from synapse to behaviour", Nature Reviews Neuroscience, vol. 10, no. 12, pp. 861-872, 2009.
[20]D. Popovic and T. Sinkjær, Control of movement for the physically disabled. New York: Springer, 2000.
[21]G. MD, "Medical Research Council (MRC) Scale for Muscle Strength", Medicalcriteria.com, 2016. [Online]. Available: http://www.medicalcriteria.com/site/en/criteria/64-neurology/238-neuromrc.html. [Accessed: 06- May- 2016].
[22]A. Do, P. Wang, C. King, A. Abiri and Z. Nenadic, "Brain-Computer Interface Controlled Functional Electrical Stimulation System for Ankle Movement", Journal of NeuroEngineering and Rehabilitation, vol. 8, no. 1, p. 49, 2011.
[23]"The Neural Correlates of Long-Term Carryover following Functional Electrical Stimulation for Stroke : Table 1", Hindawi.com, 2016. [Online]. Available: http://www.hindawi.com/journals/np/2016/4192718/tab1/. [Accessed: 06- May- 2016].
[24]T. Watanabe, S. Endo, K. Murakami, Y. Kumagai and N. Kuge, "A Measurement of Lower Limb Angles Using Wireless Inertial Sensors during FES Assisted Foot Drop Correction with and without Voluntary Effort", IJBBB, pp. 216-220, 2013.[25]Y. Laufer, H. Ring, E. Sprecher and J. Hausdorff, "Gait in Individuals with Chronic Hemiparesis: One-Year Follow-up of the Effects of a Neuroprosthesis That Ameliorates Foot Drop", Journal of Neurologic Physical Therapy, vol. 33, no. 2, pp. 104-110, 2009.
[26]R. Martin, C. Sadowsky, K. Obst, B. Meyer and J.
McDonald, "Functional Electrical Stimulation in Spinal Cord Injury: From Theory to Practice", Topics in Spinal Cord Injury Rehabilitation, vol. 18, no. 1, pp. 28-33, 2012.
[27]"Hemiplegia: Definition, diagnosis and phases", 2016. [Online]. Available: https://www.nscisc.uab.edu/Public/Facts%202015.pdf. [Accessed: 06- May- 2016].
[28]M. KAFRI AND Y. LAUFER, "THERAPEUTIC EFFECTS OF FUNCTIONAL ELECTRICAL STIMULATION ON GAIT IN INDIVIDUALS POST-STROKE", ANNALS OF BIOMEDICAL ENGINEERING, VOL. 43, NO. 2, PP. 451-466, 2014