Embed Size (px)
Citation preview

World J Urol (1995) 13:203-208 World Journal of
Urology © Springer-Verlag 1995
Testicular germ-cell tumors in childhood and adolescence
R. J. Haas and P. Schmidt
Division of Hematology and Oncology, University Children's Hospital, Lindwurmstrasse 4, D-80337 Munich, Germany
Summary. Testicular germ-cell tumors are relatively rare in childhood and adolescence, accounting for only 3.9% of all neoplasms. However, they have become a model for curable cancer. Furthermore, most of them have accurate serum markers [beta-human chorionic gonadotropin and alpha-fetoprotein ], which provide in clinical stage I dis- ease after semicastration a "wait and see" program. MAHO 82, 88, and 92 were cooperative studies on the treatment of testicular germ-cell tumors in childhood and adoles- cence. Between 1982 and 1993, 137 patients were regis- tered. In all, 76 patients suffered from yolk-sac tumors (YST); 30, from differentiated teratomas (TD); 29, from malignant teratomas of either intermediate (MTI), undif- ferentiated (MTU), or trophoblastic type (MTT); and 2, from seminomas. All patients received semicastration. Chemotherapy was given to 53 patients on the basis of disease stage and histology. Standard therapy consisted of four courses of vinblastine, bleomycin and cisplatin. However, if viable tumor was suspected after two courses, delayed laparotomy was performed (seven patients). If there was then complete tumor regression, standard ther- apy was continued (four patients). If there was an incom- plete tumor response, the patients received as salvage ther- apy three courses of etoposide (VP-16), ifosfamide, and cisplatin (three patients). Among the patients with YST, 73 had stage I disease and 3, higher-stage disease; 1 of these died due to tumor progression. In all, 56 patients were followed according to the "wait and see" policy; 9 of these needed a delayed standard chemotherapy. The rate of no evidence of disease (NED) was 98%. Among the patients with TD, 30 had stage I disease. The NED rate was 100%. Among the patients with malignant teratomas (MTI, MTU, and MTT), 13 had stage I disease. The NED rate was 100%. Ten patients had stage II disease and re- ceived chemotherapy. The NED value was 100%. Six pa- tients had stage III disease; three died. Altogether, 26 of 29 patients survived disease-free. In summary, the proba- bility for the disease-free survival of all 137 patients suf- fering from testicular germ-cell tumors is 97% after a me- dian observation period of 60 months.
Germ-cell tumors may develop in the gonads; however, they may be found anywhere in the midline of the body
Correspondence to: R. J. Haas, Fax: +49 (89) 5160-4719
Differentiation of germ ceils
Totipotent germ cell j ~
r i I Multipot q r" Deterrn r germ cell ~ _ u m o r^ | germ cell
d < (zTu) J ------<<~ L
/ '~ Embryonal 1 ['Extraembryonal'~ ~ ~ . < ; ~ ~ ~ ~ ~ bem,noma
\1 immature I Choriocarcinoma / "~btype r (MTT) 13HCG +++ / LT-.-e~,"2~ma AFP-/r~HCG- L Yolk . . . . . . AFP +++ ~
( lu) ~ sac tumor (YS/)
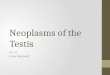
Fig. 1. Histogenetic differentiation of primordial germ cells. Multi- pot, multipotent; Determ, determinated; Diff., differentiated
along the path of migration of the primordial germ-cell population (stem cells), from the wall of the yolk sac to the gonad [5].
Histogenetically, primordial germ cells can differenti- ate into pure germ-cell tumors labeled as seminoma in the testis or dysgerminoma in the ovary. Alternatively, stem cells can develop into undifferentiated embryonic tumors - malignant undifferentiated teratomas (MTU). If further embryonic differentiation occurs, the tumors represent ei- ther immature teratomas of uncertain malignant potential or benign mature teratomas (TD). On the other hand, if primordial germ cells differentiate into tumors manifest- ing extraembryonic features, these tumors are labeled as yolk sac tumors (YST) or choriocarcinomas (MTT; see Fig. 1).
Epidemiology
Cooperative studies on the treatment of testicular germ- cell tumors in childhood and adolescence (MAHO 82, 88, 92) were started in 1982 by the German Society of Pedi- atric Oncology [6]. One of the aims was to determine the incidence of different types of testicular germ-cell tumors in children.

204
80-
60-
r . -
. - 40-
n
20.
73
0
3O
7
o 1 ~ o o o o o I~o..2. 2 1 o i I
YST TD MTI
4 INo t 2..~.~2 o
i
MTU
[ ] Stage I [ ] Stage II A [ ] Stage II B [ ] Stage II C [ ] Stage III A [ ] Stage III B
3 3 2r~-~ 0 0 l O ~ i
MTT
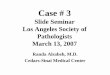
Stage I 73 30 7 4 2
Stage II A 1 0 0 0
Stage II B 0 2 1 0 Stage II C 0 2 2 3
Stage III A 1 1 2 0 Stage III B 1 0 0 3
Fig.2. Distribution according to stage and histology of 135 patients with testic- ular germ-cell tumors (2 patients with stage IA seminoma have been omitted)
Table 1. Distribution by age and histology of 137 children with testicular germ-cell tumors
YST TD MTI MTU MTT Seminoma
< 2 Years 48 26 1 0 0 2-5 Years 23 4 2 2 0 5-10 Years 3 - 1 1 0 > 10 Years 2 - 8 6 8 Total 76 30 12 9 8
YST, Yolk-sac tumor; TD, differentiated tumor (including the im- mature subtype); MTI, intermediate malignant teratoma [embry- onal carcinoma with teratoma (teratocarcinoma)]; MTU, undiffer- entiated malignant teratoma (embryonal carcinoma); MTT, tro- phoblastic malignant teratoma (choriocarcinoma)
tries [9]. The testicular seminoma is very uncommon in childhood.
Etiology
Cryptorchidism is the only proven factor that increases the risk of testicular cancer. In the literature; about 10% of patients with malignant testicular tumors have a history of cryptorchidism. The risk for those with an intraabdominal testis is estimated to be 6 times greater than that for those with only an incompletely descended testis [13]. In our studies, in about 5% of malignant testicular tumors crypt- orchidism was registered with an interval of 1-6 years [7].
Germ-cell tumors were found to represent 3.9% of all malignant tumors in childhood. The data were collected by the German Tumor Register from 1980 up to 1993 [4]. The absolute number of tumors registered during this pe- riod was 712. The incidence of malignant germ-cell tu- mors was calculated to be 0.6 per 100,000 children aged 0-15 years. The age-specific incidence was as follows: < 1 year, 65%; 1-5 years, 17%; 5-10 years, 8%; and 10-15 years, 11%. The male-to-female ratio was 0.8/1.0. The lo- calization of malignant germ-cell tumors was 24% in the testis and 29% in the ovary.
In the United States the reported incidence of malig- nant germ-cell tumors in children is even higher, being 2 per 100,000 children. In the MAHO studies conducted be- tween 1982 and 1992, 137 patients were registered. Fig- ure 2 presents the distribution by stage and histology of 137 patients with testicular germ-cell tumors; 2 patients with seminomas have been omitted. Table 1 shows the distribution by age and histology.
The most common malignant testicular tumor is the yolk-sac tumor which represents about 55% of all testicu- lar tumors. This is similar to the experience in other coun-
Histology
Several attempts at histological classifications resulted in a number of corresponding terms. However, on the basis of the new understanding of histogenesis, only two classi- fications are presently used: the World Health Organisa- tion (WHO) classification [12] and the British Testicular Tumor Panel classification [14]. Table 2 illustrates both corresponding classifications of testicular germ-cell tu- mors. In tumors of more than one histological type, the therapy for the highest malignant element should be cho- sen. Malignancy is defined in the following declining or- der: MTT, MTU, germinoma/seminoma (G), YST, and immature teratoma (T).
Tumor m a r k e r s
Three tumor markers exist: alpha-fetoprotein (ALP), beta- human chorionic gonadotropin (beta-hCG), and human placental alkaline phosphatase (hPLAP). AFP is elevated if at least part of the tumor consists of yolk-sac cells. In

205
Table 2. Comparison of classifications of testicular germ-cell tu- i I l o r s
Table 3. Clinical staging of testicular tumors - Lugano classifica- tion
WHO (1977) British Testicular Tumor Panel (1976)
Seminoma/germinoma YST (endodermal sinus tumor) EC
Seminoma/germinoma YST Malignant teratoma, undifferentiated (MTU)
Teratoma, mature, with malignant Teratoma, differentiated transformation Teratoma, immature
subtype (TD) Chorio Malignant teratoma,
trophoblastic (MTT)
Tumors of more than one histological type:
Embryonal carcinoma with EC + T, EC + YST, EC + T + YST
Chorio and any other types (specify): Chorio + T, Chorio + T + YST, Chorio + EC + T + YST Chorio + T + EC
Seminoma combined (specify): G +T, G + YST, G +EC, G + T + E C
Malignant teratoma, intermediate Malignant teratoma, trophoblastic combined
"Combined tumor" when seminoma is present
Chorio, Choriocarcinoma; EC, embryonal carcinoma; G, germi- noma/seminoma; T, teratoma, differentiated, and teratoma, imma- ture; YST, Yolk-sac tumor
most cases, beta-hCG is elevated when syncytiotro- phoblastic cells are present (choriocarcinoma, MTT).
HPLAP is specific for seminoma; however, it is diffi- cult to determine for technical reasons [9]. Serum AFP and beta-hCG correlate with immune histological stain- ing. Beta-hCG has an elimination half-life (t)_ value of 18-24 h and AFP, a t) value of 5 days. A complete re- sponse to therapy is indicated by a continuous decline of the raised serum levels within 30 days [9]. Normal levels of both tumor markers are up to 15 ng/ml. However, in neonates aged up to 5 months, serum AFP levels are phys- iologically elevated.
In the MAHO studies the tumor markers AFP and beta-hCG were invaluable for monitoring the therapy used; AFP serum levels were increased in all patients suf- fering from YST. Persistence of the disease was indicated in all cases by reelevation of AFP. In seven of eight chil- dren suffering from choriocarcinoma the beta-hCG level was markedly elevated. The effectiveness of chemother- apy could be proven by a continuous decline of the levels.
Embryonal carcinoma (MTU) only rarely produces a tumor marker; only two of nine patients with MTU showed a slight elevation of both tumor markers. Ter- atoma, including the immature subtype (TD), did not pro- duce tumor markers.
In tumors of more than one histological subtype, for instance, in MTI, an elevated serum AFP level indicates the presence of YST cells and reveals that the patient should be treated accordingly. In 5 of 12 cases diagnosed as MTI an elevation in the tumor marker AFP could be detected.
pT 1 Testis/rete testis IA pT2 Beyond the tunica
albuginea or into the epididymis IA pT3 Spermatic cord IB pT4 Scrotum IC
N1 Single, < 2 cm IIA N2 Single, > 2--5 cm; multiple, < 5 cm IIB N3 < 5 cm IIC N4 Bulky disease IID
M Supradiaphragmatic/mediastinal lymphadenopathy IIIA
M Lung metastasis, multiple (< 5), < 2 cm IIIB M Lung metastasis, (> 5), single, > 2 cm IIIC M1 Liver, bone, CNS IV
Clinical presentation and diagnosis
Testicular tumors present a painless swelling in one testis; sometimes a nodular or hard area can be found by physi- cal examination. In more than 80% of patients a stage I tu- mor is detected [8]. Sonography can be helpful for detec- tion of small tumors associated with a hydrocele. Accord- ing to Weissbach et al. [18] intrascrotal masses in children are germ-cell tumors in 71% of cases and nongerminal in 29%; the incidence was reported in 1169 children from their own experience and from the literature [18]. Consid- erations in the differential diagnosis of germ-cell tumors include benign stroma-cell tumors and Leydig-cell tu- mors. There are manifestations of acute lymphoblastic leukemia, rhabdomyosarcoma, torsion, epididymitis, and testicular infarct.
Radical semicastration with high ligation of the cord is the diagnosis and the primary treatment of testicular tu- mors in children. Biopsy is obsolete. However, the rapid section technique can be applied for histology for differ- ential diagnosis. Preoperative determination of the tumor markers AFP and beta-hCG is obligatory. If these markers cannot be obtained prior to surgery, they should be deter- mined at the earliest possible time postsurgery. X-ray of the chest and bone scans may be used for detection of metastasis. However, abdominal and pelvic ultrasound are essential for staging. If abdominal masses are detected, magnetic resonance imaging (MRI) is the best way to vi- sualize the pathological structure. Alternatively, comput- erized tomography (CT) can be used if MRI is not avail- able.
Staging
There are a number of staging classifications for testicular germ-cell tumors, mainly involving USA, WHO, Royal Marsden, and Lugano staging [16]. The German Society of Pediatric Oncology (GPO) uses Lugano staging (Table 3). For stages IA-IC, Lugano staging is based on the find-

206
ings obtained by semicastration, whereas all other stages are determined by clinical staging. If the tumor markers AFP and beta-hCG persist in clinical stage I patients the tumor is of at least stage II.
Treatment
Our treatment protocol for testicular germ-cell tumors (MAHO 82, 88, 92) was started in 1982 [6]. The trial was based on favorable reports obtained in adults [2]. The combination of vinblastine, bleomycin, and cisplatin in the regimen of Einhorn and Donohue [2] had sometimes also been used successfully in children with malignant germ-cell tumors; however, there was a report of in- creased risk for pulmonary fibrosis [11]. The principal aims for treatment in the GPO study were as follows:
1. Reduction of the toxicity of vinblastine, bleomycin, and cisplatin
2. Prevention of mutilation by primary lymphadenectomy as far as possible
3. Determination as to which patients with stage I tumors could safely bypass chemotherapy by the introduction of a "wait and see" program
To reduce the toxicity of chemotherapy in infants and children, the Einhorn protocol was modified as follows [7]: vinblastine was given at half the regular dose, and bleomycin was given by continuous infusion at a reduced dose before treatment with cisplatin was started.
To avoid as far as possible the need for primary lym- phadenectomy with its high risk for loss of ejaculation [17], the following strategies were used. All patients with a stage I YST secreting a significant amount of tumor marker before surgery did not received a primary lym- phadenectomy. However, between 1982 and 1988, pa- tients with stage I malignant teratomas and seminomas were treated by either adjuvant chemotherapy or lym- phadenectomy. Starting in 1988 (MAHO 88), all these pa- tients received only adjuvant chemotherapy [7]. A de- layed exploratory laparotomy was recommended only in cases of suspected viable tumor after two courses of chemotherapy.
Introduction of the "wait and see" program was started in 1982 for all patients under 2 years of age with stage I YST. Between 1982 and 1988, patients older than 2 years received adjuvant chemotherapy. Starting in 1988 (MAHO 88), only semicastration was performed in all pa- tients with stage I YST regardless of their age.
In summary, only the two above-mentioned modifica- tions were used in the revised protocol from 1988 through 1992. It was expected that in about 25% of the YST stage I patients primarily treated by surgery alone, chemotherapy would have to be given at a later time [1, 15, 17].
Surgery
All patients received semicastration to obtain precise his- tology. High ligation of the spermatic cord was attempted. Simple biopsies were avoided.
No patient with stage I YST received a primary lym- phadenectomy. Patients older than 2 years received adju-
vant chemotherapy (17 patients). Beginning in 1988, all patients, regardless of age, received only semicastration without chemotherapy ("wait and see").
Patients with clinical stage I malignant teratoma or seminoma were treated by either adjuvant chemotherapy or lymphadenectomy. Lymphadenectomy was performed in seven patients. All other stages of YST and of malig- nant teratoma received standard chemotherapy (see be- low). However, if there was no complete remission after two courses (as indicated by different methods of imaging or by serum tumor markers), a delayed exploratory la- parotomy was performed; this had to be done in seven cases. If only fibrotic tissue was found (four cases), an- other two courses of standard chemotherapy were given. In cases of viable tumor cells, salvage therapy (see below) was given. If tumor progression was noted, salvage ther- apy was given without laparotomy.
Chemotherapy
The standard chemotherapy (PVB) was carried out as fol- lows. Vinblastine was given i.v. at 3.0 mg/m 2 per day on days 1 and 2. Bleomycin was given at 15.0 mg/m 2 per day on days 1-3 by continuous i.v. infusion. Cisplatin was given at 20.0 mg/m 2 per day on days 4-8 in a 15-min i.v. infusion. Treatment was given every 28 days for a total of four courses.
The salvage therapy (PEI) was carried out as follows. Induction therapy consisted of the following: VP-16 (etoposide) given at 80 mg/m 2 per day on days I-3 in a 30-min i.v. infusion, ifosfamide given i.v. at 1500 mg/m 2 per day on days 1-4 over 30 min, and cisplatin given at 20 mg/m 2 per day on days 2-5 in a 15-min i.v. infusion; treat- ment was given every 28 days for a total of four courses. Maintenance therapy consisted of VP-16 given i.v. at 300 mg/m 2 on day 1 over 2 h; treatment was given every 28 days for a total of three courses.
Results
Outcome
In Table 4 the results of MAHO 82, 88, and 92 are sum- marized. Of 137 patients, 133 are in complete remission after a median observation period of 60 months with a 97% probability of disease-free survival. In all, 19 pa- tients entered the protocol with clinical tumors of more than stage I. Only 29 of 76 children with YST received chemotherapy, including 3 patients with advanced tumors and 17 patients with clinical stage I tumors who received adjuvant chemotherapy. In addition, 9/56 patients man- aged under the "wait and see" program received delayed standard chemotherapy.
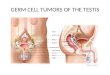
The persistence of tumor was always indicated by ele- vation of the AFP tumor marker. Figure 3 gives an exam- ple of the AFP levels detected in a patient with a clinical stage I YST. As can be seen from the figure, elevation of the tumor marker at 10 months after surgery necessitated delayed chemotherapy.
One patient with stage III disease died of tumor pro- gression while under salvage therapy. The outcome for the

207
10.000
1.000
100
10
1
ng\ml
!!i!i! !!!!i!!!!!!!
0 5 10 15 20 25 30 35
months
Fig. 3. Example of AFP levels measured in a patient with a clinical stage IA YST. The persistence of and even increase in AFP indi- cated persistence of the tumor
Six patients had stage III tumors; two died due to tumor progression and one died during salvage therapy due to candida septicemia. In summary, 26 of 29 patients with malignant teratomas survived relapse-free over a median observation period of 60 months.
Two patients with seminomas of stage IA received a staging lymphadenec tomy confirming the diagnosis. Ad- juvant chemotherapy was not given. These children are in complete remission after 4 and 7 years, respectively.
Taking all MAHO studies together, only seven children obtained salvage therapy in addition to standard chemo- therapy. In only seven cases was a delayed laparotomy necessary after two courses o f standard chemotherapy be- cause imaging indicated persistence of the tumor. How- ever, viable tumor was found in only three cases.
Table 4. Treatment results obtained in 137 children with testicular germ-cell tumors: cooperative MAHO studies of 1982, 1988, and 1992
Diagnosis, n = 137 Mean Chemo- Pro- NED Deaths stage age therapy gress/
(years) relapse
YST St I 73 26 - 73 -
lI 1 1.73 1 - 1 - III 2 2 1 1 1
TD 30 1.31 - - 30 0
Toxicity
The toxicity encountered in 51/137 patients who received standard chemotherapy was tolerable. A reversible severe depression of white blood cells and/or platelets was found in 35% of cases. All seven patients who received salvage therapy suffered from severe myelodepression after each of the four courses o f chemotherapy; one child developed candida septicemia and died. Nephropathy, lung fibrosis, and ototoxicity were not registered.
Discussion
MTI St I 7 . . . . II 4 10.7 8 1 12 0
III 1 . . . .
MTU St I 4 - 1 - - II 3 12.2 8 - 8 -
III 2 - 1 - 1
MTT St I 2 . . . . II 3 15.2 8 1 6 -
III 3 - 2 - 2
Seminoma 2 15.3 2 x LA - 2 0
LA; Lymphadenectomy; NED, no evidence of disease; St, stage
entire group of 76 children with YST is therefore 98.7% disease-free survival after a median observation period o f 60 months. In stage I YST there was no difference between the 17 children treated by adjuvant chemotherapy and the 56 children managed under the "wait and see" program.
As can be seen f rom Table 4, all 30 children with dif- ferentiated teratomas were cured solely by semicastration. In this group, 11/30 patients suffered histologically f rom the so-called immature subtype.
A total o f 29 patients had malignant teratomas. In all, 13 had clinical stage IA tumors, with 5 receiving a staging lymphadenec tomy confirming the diagnosis in all cases; the other 8 patients received adjuvant chemotherapy with- out lymphadenectomy. Ten patients had stage II tumors (five of stage IIC) and received standard chemotherapy.
Efficacy of chemotherapy
At present it is no longer controversial that malignant tes- ticular germ-cell tumors can be effectively cured by chemotherapy. As based on the chemotherapy regimens introduced by E inhom and Donohue [2], the favorable combinations are vinblastine, Neomycin , and cisplatin (PVB) or etoposide, bleomycin, and cisplatin (PEB). Pa- tients with bulky disease or disseminated testicular cancer had an advantage with the PEB regimen in comparison with the PVB regimen. The increase in the therapeutic efficacy of PEB was statistically significant in those patients with advanced disease [19]. However, in lower stages o f the disease, survival data showed no difference.
For salvage therapy, a combinat ion of etoposide, ifos- famide, and cisplatin is preferred [3, 10, 16]. Therapy op- tions that include radiation have been discarded. Interest- ingly, this is also true for the pure seminomatous type of germ-cell tumor in the testis [2]. Chemotherapy has also eliminated histology as a prognostic factor since YST as well as malignant teratomas have been cured [ 1 ].
The trial used in the Cooperat ive German Study for treatment o f testicular germ-cell tumors was a modifica- tion of the original Einhorn protocol. The dose of vinblas- tine was reduced and bleomycin was given as a continu- ous infusion fol lowed by cisplatin. The rationale for this schedule is creatinine clearance. Cisplatin causes a de- cline in creatinine clearance. As bleomycin and cisplatin were not given concurrently, pulmonary fibrosis, as de- scribed in children treated with the original Einhorn regi- men [2], was avoided. The present results suggest that the

208
- - YST, TD: Stage I A --> "Watch and wait"
c O -~ Seminoma, MTT, MTU, MTI, combined:
Stage I A --> 2 x PVB if} ~3 o g: Seminoma, YST, MTT, MTU, MTI, combined:
151~-~Tu'neg: l x P V B '~ Stage I B-II B --> 2 x PVB .2 I'~1 Tu.pos: expl. LAP. --> 3 x PEI
/~1 rr 1~1 Tu.neg: l x P V B
_ _ Stage II C-IV ~ 2 x PVB INI~ ~ Tu.pos: expl. LAP. --> 3 x PEI
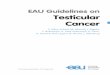
Fig.4. MAHO 94: ongoing protocol of the Cooperative German Working Group for the treatment of malignant testicular germ-cell tumors in children. PVB, Cisplatin/vinblastine/bleomycin; PEB, cis- plafin/etoposide/bleomycin; PEI, cisplatin/etoposide/ifosfamide; expl. LAP, exploratory laparotomy; Tu. neg. CT/ultrasound of the abdomen and tumor marker negative
above-mentioned modified chemotherapy is effective even in advanced-stage malignant testicular tumors. Very few cases require salvage therapy with a combinat ion of eto- poside, ifosfamide, and cisplatin.
Results obtained in differentiated teratoma
It could be shown that the 30 patients registered with ma- ture teratomas of the testis, including 11 cases with the immature subtype, could be cured by semicastration alone. This finding contrasts with the known tendency for recurrence o f mature teratomas at extragonadal sites.
Stage I YST
Patients with stage I YST secreting the tumor marker AFP do not initially need chemotherapy if they are closely fol- lowed. Even in cases of tumor persistence they can be cured by chemotherapy. This could be shown in 56 pa- tients with stage I YST who did not receive orchiectomy ("wait and see" program); all 9 patients who had persis- tent tumor after semicastration could safely be treated by standard chemotherapy. Therefore, an exact pathological staging with primary lymphadenectomy can be omitted. The unfavorable side effect of lymphadenectomy is a loss of antegrade ejaculation in about 60% of patients. The alternatively used modif ied lymphadenec tomy has de- creased this calamity; however, about 20% of patients nonetheless suffer f rom this side effect [17].
Stage I malignant teratoma or seminoma: "wait and see" also in these patients?
Stage I tumors histologically classified as malignant ter- atoma or seminoma usually do not secrete relevant amounts of a tumor marker. Therefore, a "wait and see" program in these patients is rather questionable. As reported in the lit- erature [1, 17] clinical staging alone was insufficient, since about 30% of stage I patients were proven to be in stage II by staging laparatomy.
Our results cannot add new information pertinent to this question because a staging laparatomy was performed in only 7/13 cases; these 7 patients proved to have stage IA tumors. For the moment , all new stage I patients suf- fering f rom malignant teratoma or seminoma will receive adjuvant chemotherapy in our treatment protocol.
In conclusion, the current strategy of the M A H O 94 protocol is given in Fig. 4. The adjuvant chemotherapy is reduced; in agreement with the literature [16], only two cycles containing cisplatin are given. For advanced stages I I C - I V the standard chemotherapy is PEB instead of PVB.
References
1. Dieckmann KP, Kreuser ED (1991) Aktueller Stand der Che- motherapie von Keimzelltumoren. Urologe 30 : 45-51
2. Einhorn LH, Donohue JP (1977) Improved chemotherapy in disseminated testicular cancer. J Urol 117:65-71
3. Einhorn LH, Weathers T, Loehrer P, Nichols C (1992) Second line chemotherapy with vinblastine, ifosfamide and cisplatin after initial chemotherapy with cisplatin, VP 16 and bleomycin in disseminated germ cell tumors (GCT): long term follow up. Proc Am Soc Clin Oncol 11 : 96
4. Haaf HG, Kaatsch P, Michaelis J (1994) Jahresbericht 1993 des Deutschen Kinderkrebsregisters. IMSD, Mainz
5. Haas RJ (1993) Maligne Keimzelltumoren. In: Gutjahr P (ed) Krebs bei Kindern und Jugendlichen. Deutsche Arzte, K61n, S 432M-42
6. Haas RJ, BrSanswig J, G6bel U (1983) Maligne Hodentumoren bei Kindern und Jugendlichen. Klin Paediatr 195:196-201
7. Haas RJ, G6bel U, Harms D (1989) Maligne Hodentumoren im Kindesalter. Klin Paediatr 201:269-274
8. Harms D, J~inig U (1986) Germ cell tumors of childhood. Re- port of 170 cases including 59 pure and partial yolk sac tumors. Virchows Arch [A] 409 : 223-235
9. Hawkins EP (1990) Pathology of germ cell tumors in children. In: Davis S (ed) Critial reviews in oncology/hematology. Boca Raton, Boston, pp 165-179
10. Loehrer PJ, Einhorn LM, Williams SD (1986) VP 16 plus ifos- famide plus cisplatin as salvage therapy in refractory germ cell cancers. J Clin Oncol 4:528-536
11. Mann JR, Pearson D, Barett A (1987) UKCCSG malignant germ cell tumors - treatment results (abstract 57). Proceedings, 19th, meeting of the SIOP, Jerusalem, October 1987
12. Mostofi FK, Sobin LH (1977) Histological typing of testis. Offset publication 16. WHO, Geneva
13. Peckham M (1988) Testicular cancer. Rev Oncol 1:439--453 14. Pugh RCB, Cameron KM (1976) Teratoma. In: Pugh RC (ed)
Pathology of testis. Blackwell Scientific Publications, Oxford, pp 199-244
15. Schmoll HJ (1993) Management of early stages of testicular carcinoma. Recent Results Cancer Res 16:237-255
16. Schmoll HJ (1993) Biology and treatment of testicular cancer. Gardiner-Caldwell Communications, Cheshire
17. Weissbach L, Boedefeld A (1989) Stadium I des Nicht-Semi- noms: Vorteile und Risiken verschiedener Strategien. Aktuel Urol 20:132-139
18. Weissbach L, Altwein JE, Stiens R (1984) Germinal testicular tumors in childhood. Eur Urol 10 : 73-85
19. Williams S, Birch R, Einhorn LM (1987) Treatment of dis- seminated germ cell tumors with cisplatin, bleomycin and either vinblastine or etoposide. N Engl J Med 316: 1435- 1440