Embed Size (px)
Citation preview

312 | JUNE 2013 | VOLUME 10 www.nature.com/nrurol
NEWS & VIEWS
survival in African Americans—to further limit the applicability for AS. That primary care doctors and providers will ignore the AUA and NCCN guidelines that call for a baseline PSA test at age 40 years in all men (regardless of ethnicity) is also a concern. In my opinion, a baseline PSA test is especi-ally important for African American men because they have a tendency to develop prostate cancer at a younger age than white men and might have more to lose if the disease is not detected in an early, curable state. That is, in the PSA era, the ‘racial gap’ was narrowed; if we abandon screening now, we will see more African American men die of prostate cancer.
In 2012, the US Preventive Services Task Force (USPSTF) released guidelines stating that PSA screening did not reduce pros-tate cancer mortality as reported from the currently available randomized trials and suggested that doctors stop performing the serum PSA test to screen for prostate cancer.10 This decision was not supported by many groups and individuals—such as the AUA, NCCN and the Us TOO International Prostate Cancer Education and Support Network—who strongly believe in the value of PSA testing. Unfortunately, this confusion might cause many doctors to stop recom mending PSA testing to their patients, which could further discourage African American men from getting tested.
Since the mid 1990s, the use of PSA testing has become widespread, result-ing in a tremendous stage migration. In other words, during the pre-PSA era about 20–25% of men (both black and white) pre-sented with incurable metastatic disease. Over the past 10 years, the rate of metastatic disease at first presentation has dropped to <5% and more men are diagnosed with early stage disease and are potential candi-dates for AS. If we are now to face a back-lash against PSA screening as a result of the USPSTF recommendation, I am concerned that we might see a return to a time when one-quarter of men present with incurable bony metastatic prostate cancer and have poor prognoses. For African American men, who generally present at a young age, we could shift from seeing men in their mid-40s to late-50s having a mild to
moder ately elevated PSA and early, curable prostate cancers to men presenting in their 50s or 60s with metastatic disease and dismal prognoses. Such a shift means we might be entering an era of fewer eligible men for AS. However, for those men who are eligible, Hu and colleagues’ and other studies suggest that entry criteria for AS might need to be customized for African American men. The bottom line is that we need to be extra vigilant when offering AS to our African American patients.
Duke Cancer Institute, Duke University, Durham, NC 27710, USA. [email protected]
AcknowledgementsThe author gives special thanks to Joan McAlexander for editorial support.
Competing interestsThe author declares no competing interests.
1. Moul, J. W. et al. Prostate-specific antigen values at the time of prostate cancer diagnosis in African-American men. JAMA 274, 1277–1281 (1995).
2. Morgan, T. O. et al. Age-specific reference ranges for prostate-specific antigen in black men. N. Engl. J. Med. 335, 304–310 (1996).
3. Moul, J. W., Douglas, T. H., McCarthy, W. F. & McLeod, D. G. Black race is an adverse prognostic factor for prostate cancer recurrence following radical prostatectomy in an equal access health care setting. J. Urol. 155, 1667–1673 (1996).
4. Powell, I. J. The precise role of ethnicity and family history on aggressive prostate cancer: a review analysis. Arch. Esp. Urol. 64, 711–719 (2011).
5. Dall’Era, M. A. et al. Active surveillance for prostate cancer: a systematic review of the literature. Eur. Urol. 62, 976–983 (2012).
6. Eggener, S. E. et al. A multi-institutional evaluation of active surveillance for low risk prostate cancer. J. Urol. 189 (Suppl. 1), S19–S25 (2013).
7. Ha, Y. S. et al. Increased incidence of pathologically nonorgan confined prostate cancer in African-American men eligible for active surveillance. Urology 81, 831–836 (2013).
8. Iremashvili, V. et al. Comprehensive analysis of post-diagnostic prostate-specific antigen kinetics as predictor of a prostate cancer progression in active surveillance patients. BJU Int. 111, 396–403 (2013).
9. Abern, M. R. et al. Race is associated with discontinuation of active surveillance of low-risk prostate cancer: results from the Duke Prostate Center. Prostate Cancer Prostatic Dis. 16, 85–90 (2013).
10. Moyer, V. A.; US Preventive Services Task Force. Screening for prostate cancer: U. S. Preventive Services Task Force recommendation statement. Ann. Intern. Med. 157, 120–134 (2012).
‘‘…this confusion might cause many doctors to stop recommending PSA testing to their patients…’’
TESTICULAR CANCER
Changing patterns of incidence in testicular germ cell tumoursMausam Singhera and Robert Huddart
Testicular germ cell tumours are the most common malignancy in young adult males. Recent data suggest that the predominant histological subtype appears to be shifting towards seminomas, which is mirrored in an increasing age at presentation. However, as nonseminomatous tumours present earlier, recent declines in its incidence might be more informative of overall trends.Singhera, M. & Huddart, R. Nat. Rev. Urol. 10, 312–314 (2013); published online 23 April 2013; doi:10.1038/nrurol.2013.79
Over the past 40 years, the global rate of incidence of testicular germ cell tumours (TGCTs) has increased annually by 1–6%.1 Whether this trend is continuing is unclear; some studies suggest that the rate of increase is reducing, with a reduction in incidence evident in several countries, including the UK. Ruf et al.2 undertook a retrospective analysis of 2,482 patients diagnosed between 1976 and 2010 who were treated at two insti-tutions in Germany. They allocated patients into five groups based on the time of treat-ment (before 1990, 1990–1994, 1995–1999, 2000–2004 and 2005–2010). The researchers
found an increase in the mean age at diag-nosis (from 28 years to 36 years) and in the proportion of seminomatous tumours diag-nosed (from 30.9% to 56%) between group 1 (before 1990) and group 5 (2005–2010). The authors suggest that, as well as an increasing incidence, a variation in the epidemiology of TGCTs might also be evident.
Although interesting, can these data be corroborated? A problem in using hospital- based data is the potential for bias and, in particular, referral bias. For instance, at the beginning of the period, these institu-tions could have been referred a higher
© 2013 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | UROLOGY VOLUME 10 | JUNE 2013 | 313
NEWS & VIEWS
proportion of younger patients with non-seminomatous TGCTs and, in later years, a more- comprehensive cross-section of patients with TGCTs could have been referred, resulting in increased numbers of patients, increased median age at diag-nosis and an increased proportion of semi-nomatous tumours. However, if the data by Ruf et al.2 could be validated, what are the implications for our understanding of TGCT biology?
The epidemiology of TGCTs is unusual, complex and incompletely understood. As well as the unique age at presentation, evidence suggests a strong familial (with brothers having an eightfold increased risk compared with men without a family history) and racial component, with high incidences in white populations of Northern European countries (8.0–9.0 per 100,000) and low incidences in indigenous Asian and African populations (<1 per 100,000).3 Indeed, some of this risk can be explained by the identification of a number of sequence variants that are associ ated with an increased risk of developing TGCTs.4 Notwithstanding genetic variation, substantial geographi-cal disparity in risk remains; for example, Nordic countries have the highest risk and, within the region, the risk is conspicuously higher in Denmark and Norway than in Sweden and Finland.
The cause of the discrepancy in spatial risk is poorly understood. Increased industrialization in the Western world was thought to increase risk, but the latest data confound this perception; Norway and Israel experienced increases of >100% from 1973–1977 to 1998–2002. By contrast, modest increases in the same time periods were noted in Singaporean, Chinese (8%) and Hong-Kong-based registries (19%). Furthermore, there was a downward trend (24% fewer cases) in men in Mumbai, India.3
Specific triggers that lead to the develop-ment of TGCTs have not been identified. The most definitive association of the disease is with cryptorchidism; however, low birth weight, short gestational age, inguinal hernia and twinning have been implicated.5 Environmental agents are also thought to increase risk by altering the micro environment of the testis, causing hormo nal imbalances. Although little
evidence supports smoking (individual or maternal) as a risk factor, organo chlorines and poly chlorinated biphenyl compounds, such as poly vinyl chloride and phtha-lates, are associated with a higher risk of TGCT d evelopment.6
Set against this background, what are the possible explanations for the rising inci-dence of seminoma and increasing age at presentation? Ruf et al.2 suggested that the increase in the proportion of seminomas could be attributed to different aetiologi-cal factors, but admit that no definitive or congruent evidence supports this notion. However, we propose that these data are compatible with an alternative hypothesis: a birth cohort effect.
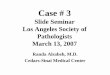
The incidence of seminomas peaks in men aged 30–45 years whereas non-seminomas peak in men aged 20–35 years. If the incidence or risk of developing TGCTs is determined at or near birth and the overall increase in incidence during the 20th century has declined in recent years, we would expect this decline to be initially noted in cases of nonseminomas.7 As the diagnosis of nonseminomatous TGCTs pre-cedes that of seminomas by approximately 10 years, any decline in seminomatous tumour incidence will possibly lag behind (with diagnoses of seminomas continuing to increase for 10 years) and cause the pro-portionate increase in seminoma cases and median age (Figure 1). Our analysis of the UK data reveals that the median age of diag-nosis of TGCTs has not increased drama-tically between 1985 and 1989 (33 years) and 2005 and 2010 (35 years). Specifically, the median age of diagnosis for seminomas was 37 years in 1985–1989 and 38 years in 2005–2010. The corresponding median
age of diagnosis for nonseminomas has remained constant (28 years) for both the time periods.8 Although these data are limited by the considerable proportion of patients coded as ‘other’ in registry data, data from Denmark also demonstrates an earlier decline in incidence for non seminomatous TGCTs (1990) compared with non-seminomatous TGCTs (1995).3 Similarly, in their review of data from a group of European countries, Bray and colleagues reported a decline in non seminomatous TGCT rates, which was reflected by a higher prevalence of seminomatous TGCTs (55–60% compared with 40–45%).9 They also concluded that this finding was in keeping with a birth cohort effect and a background of declining incidence.
Indeed, there are potential confound-ing factors in these analyses that include limitations of registry data (which do not have central review of pathology), incom-plete or incorrect data and discrepancies in histo logical classifications. With respect to the latter, the evolution of International Classification of Diseases for Oncology (ICD-O) codes over the years means that the analyses by Bray et al.1,9 used second-edition classifications that were introduced only part-way through the analysis period. Other biases might be attributed to diag-nostic changes, but the rapid TGCT growth rate and clear clinical signs suggest that any difference in age at diagnosis or histo-logy between time periods are unlikely to be explained by increasing awareness or improved availability of ultrasonography in later decades resulting in earlier diagnosis.
Although the majority of data continue to indicate a common aetiopathogenesis of TGCTs, we cannot rule out that certain
‘‘The epidemiology of TGCTs is unusual, complex and incompletely understood’’
Figure 1 | Diagnosis of testicular cancer in England. By 2025, a decline in seminomatous testicular cancer might be evident.
80 –
70 –
60 –
50 –
40 –
30 –
20 –
10 –
0 –<20 20–29 30–39 40–49
Age at diagnosis (years)
Cas
es (%
)50–59 >60
A recentdecrease indiagnoses
Nonseminomatous 1985–1989Nonseminomatous 2005–2010Seminomatous 1985–1989Seminomatous 2005–2010Seminomatous 2020–2025?
© 2013 Macmillan Publishers Limited. All rights reserved

314 | JUNE 2013 | VOLUME 10 www.nature.com/nrurol
NEWS & VIEWS
factors might influence one particular histo-logical subtype over another.10 Whether any given risk factor is solely responsible for a specific pathology or whether inter-actions with genetic factors are involved is also unclear from the current epidemio-logical data. Evidently, the epidemiology of TGCTs is complex and evolving. As TGCTs are rare, international collabora-tions incorporating genome-wide associa-tion studies with epidemio logical studies are needed to u nderstand these trends and their implications.
Institute of Cancer Research and The Royal Marsden NHS Foundation Trust (M. Singhera), Institute of Cancer Research and The Royal Marsden NHS Foundation Trust (R. Huddart), Downs Road, Sutton, Surrey SM2 5PT, UK. Correspondence to: R. Huddart [email protected]
AcknowledgementsThe authors wish to acknowledge Luke Hounsome at the South West Public Health Observatory, Bristol, UK for the statistical analyses and his help in the preparation of this manuscript.
Competing interestsThe authors declare no competing interests.
1. Bray, F. et al. Trends in testicular cancer incidence and mortality in 22 European countries: continuing increases in incidence and declines in mortality. Int. J. Cancer 118, 3099–3111 (2006).
2. Ruf, C. G. et al. Changes in epidemiologic features of testicular germ cell cancer: age at diagnosis and relative frequency of seminoma are constantly and significantly increasing. Urol. Oncol. http://dx.doi.org/10.1016/ j.urolonc.2012.12.002.
3. Chia, V. M. et al. International trends in the incidence of testicular cancer, 1973–2002. Cancer Epidemiol. Biomarkers Prev. 19, 1151–1159 (2010).
4. Gilbert, D., Rapley, E. & Shipley, J. Testicular germ cell tumours: predisposition genes and the male germ cell niche. Nat. Rev. Cancer 11, 278–288 (2011).
5. Cook, M. B. et al. A systematic review and meta-analysis of perinatal variables in relation to the risk of testicular cancer-experiences of the son. Int. J. Epidemiol. 39, 1605–1618 (2010).
6. Meeks, J. J., Sheinfeld, J. & Eggener, S. E. Environmental toxicology of testicular cancer. Urol. Oncol. 30, 212–215 (2012).
7. McGlynn, K. A. et al. Trends in the incidence of testicular germ cell tumours in the United States. Cancer 97, 63–70 (2003).
8. National Cancer Intelligence Network. Search Results for ‘testicular cancer’ [online], http://www.ncin.org.uk/search/TESTICULAR+CANCER.aspx (2010).
9. Bray, F. et al. Do testicular seminoma and nonseminoma share the same etiology? Evidence from an age-period-cohort analysis of incidence trends in eight European countries. Cancer Epidemiol. Biomarkers Prev. 15, 652–658 (2006).
10. McGlynn, K. A. & Cook, M. B. Etiologic factors in testicular germ-cell tumours. Future Oncol. 5, 1389–1402 (2009).
PROSTATE CANCER
Improvements in risk stratification of prostate cancerGurdarshan S. Sandhu and Gerald L. Andriole
Current biopsy techniques and clinical disease assessment of prostate cancer frequently fail to accurately stratify men according to risk. Recent advances in biopsy techniques, imaging, molecular genetics, and biomarkers could enable physicians to improve risk stratification at the individual level, thereby improving patient management for prostate cancer.Sandhu, G. S. & Andriole, G. L. Nat. Rev. Urol. 10, 314–315 (2013); published online 14 May 2013; doi:10.1038/nrurol.2013.107
Prostate cancer poses a significant world-wide health-care burden, with approxi-mately 1 million men being diagnosed annually and 250,000 deaths every year. Over the past 20 years, a major effort to reduce prostate-cancer-related mortal-ity has involved PSA-based screening coupled with aggressive therapy for most screen-detected cancers. However, recent data from screening trials show that this approach has, at best, only a modest impact on prostate-cancer-related mortality and is associated with substantial overdiagnosis and overtreatment.1,2 Moreover, although radical prostatectomy is an effective treat-ment for clinically detected cancer,3 its effect on screen-detected cancer is much less certain.4 These considerations have led to an increased recognition that active surveil-lance with delayed potentially curative inter-vention is a valid treatment option for many men with low-risk PSA-detected tumours.
A limitation of active surveillance is that up to 50% of men classified as having low-risk disease actually harbour more-aggressive undiagnosed prostate cancers,
which can silently progress despite careful surveillance. This issue regarding disease misclassification has been highlighted by Aizer and colleagues,5 who performed a population-based analysis of 27,969 men with PSA-detected, low-risk prostate cancer (defined as clinical stage T1c, Gleason score ≤6, and PSA ≤10 ng/ml) using the Surveillance, Epidemiology and End Results (SEER) database.
Aizer et al.5 sought to evaluate the effect of older age on prostate-cancer-related mortality in patients with low-risk prostate cancer for whom noncurative management was initially used. The investigators found that both older age (>67 years; adjusted HR 1.05, 95% CI 1.02-1.08) and initial non curative treatment (with either watch-ful waiting or active surveillance; adjusted HR 3.34, 95% CI 1.97-5.67) were associated with an increased risk of prostate-cancer-specific mortality in men. The authors argue that high-grade disease, which is associated with older age, is often missed on conventional prostate biopsy in these men, who are also more likely to have
iSto
ckph
oto/
Thin
ksto
ck
© 2013 Macmillan Publishers Limited. All rights reserved