Embed Size (px)
Citation preview
Test Requisition vs
Test Request A transatlantic look at different approaches to
managing lab test utilization that improves outcomes and reduces costs
Dr Danielle Freedman MD Luton and Dunstable Hospital, Luton, UK
Dr Paul Kurtin MD Mayo Clinic, Rochester, USA
Executive War College, New Orleans, May 2015

Dr Danielle Freedman MD
Consultant Chemical Pathologist Associate Physician in Clinical Endocrinology
Director of Pathology Luton and Dunstable University Hospital
NHS Trust, UK
Nothing to disclose No relevant financial interests
Laboratory Test Requesting in UK
• Factors influencing test ordering by clinicians
• Strategies for modifying clinicians ordering patterns
• Implementing policies to improve laboratory utilisation and thereby improve patient outcome
Question 1
What most determines a clinician’s test ordering? 1. Fear of litigation 2. Cost of test 3. Evidence based guidelines 4. Patient went to Lab Tests Online 5. Watched an episode of ‘House’ last night
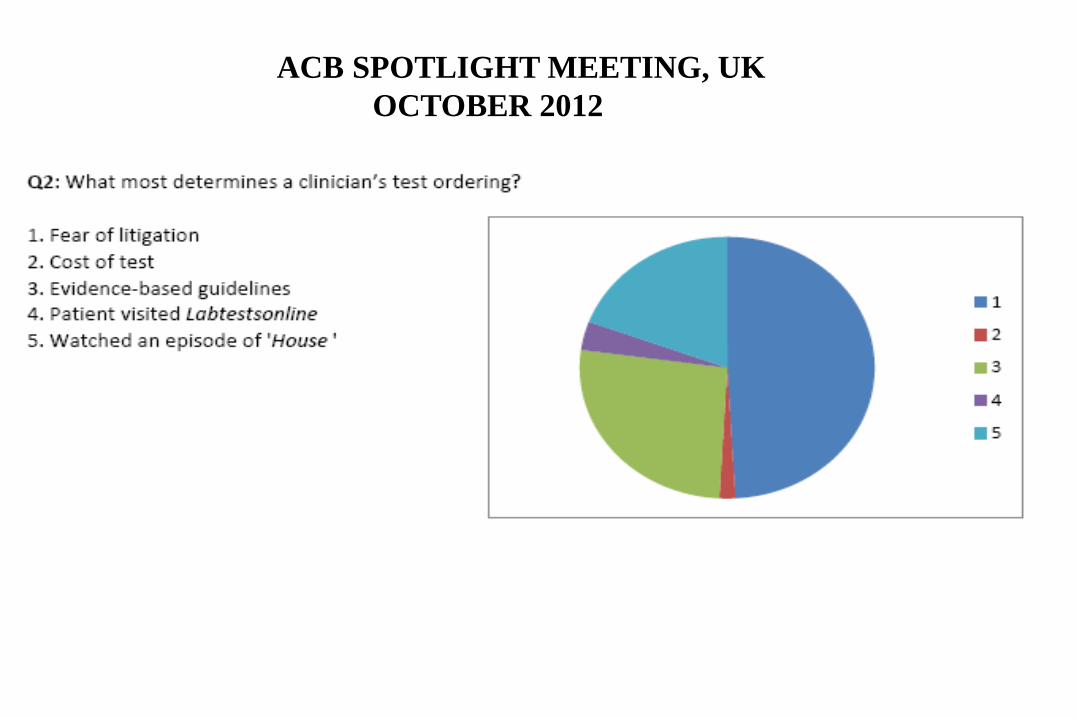
ACB SPOTLIGHT MEETING, UK OCTOBER 2012
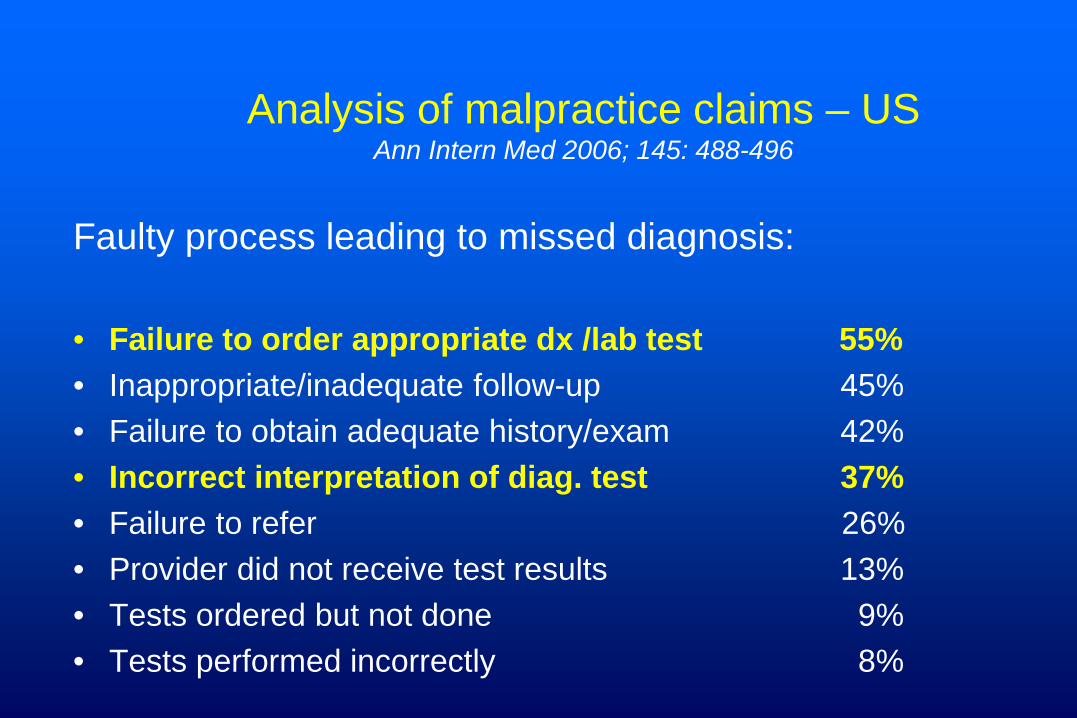
Analysis of malpractice claims – US Ann Intern Med 2006; 145: 488-496
Faulty process leading to missed diagnosis: • Failure to order appropriate dx /lab test 55% • Inappropriate/inadequate follow-up 45% • Failure to obtain adequate history/exam 42% • Incorrect interpretation of diag. test 37% • Failure to refer 26% • Provider did not receive test results 13% • Tests ordered but not done 9% • Tests performed incorrectly 8%
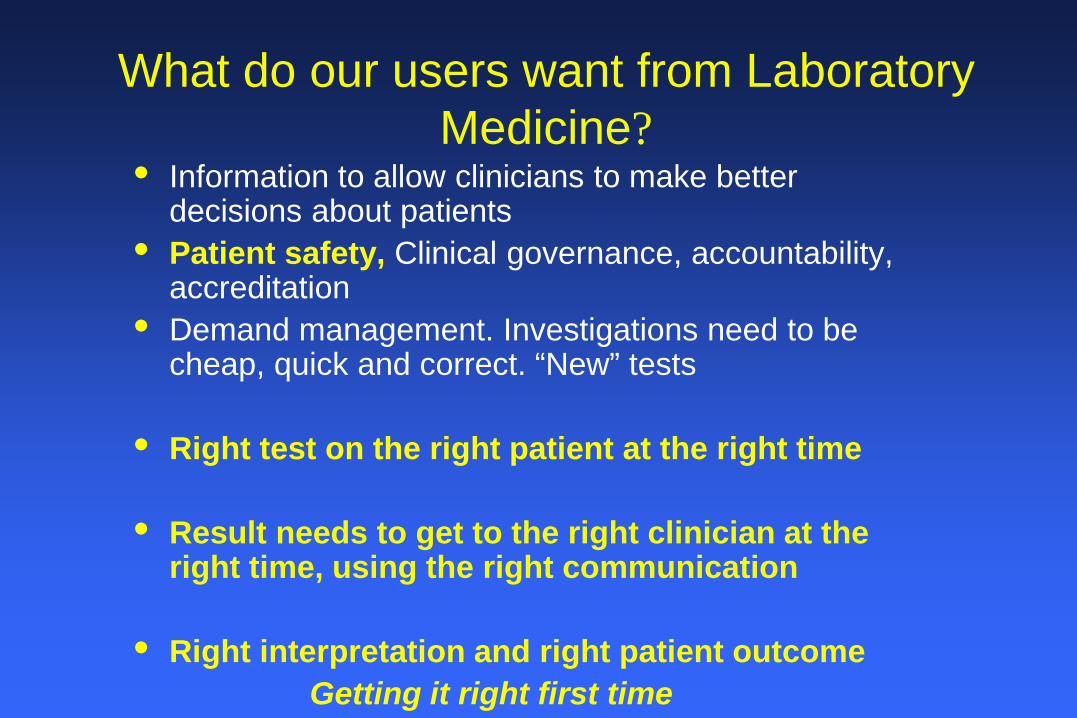
What do our users want from Laboratory Medicine?
• Information to allow clinicians to make better decisions about patients
• Patient safety, Clinical governance, accountability, accreditation
• Demand management. Investigations need to be cheap, quick and correct. “New” tests
• Right test on the right patient at the right time
• Result needs to get to the right clinician at the right time, using the right communication
• Right interpretation and right patient outcome Getting it right first time
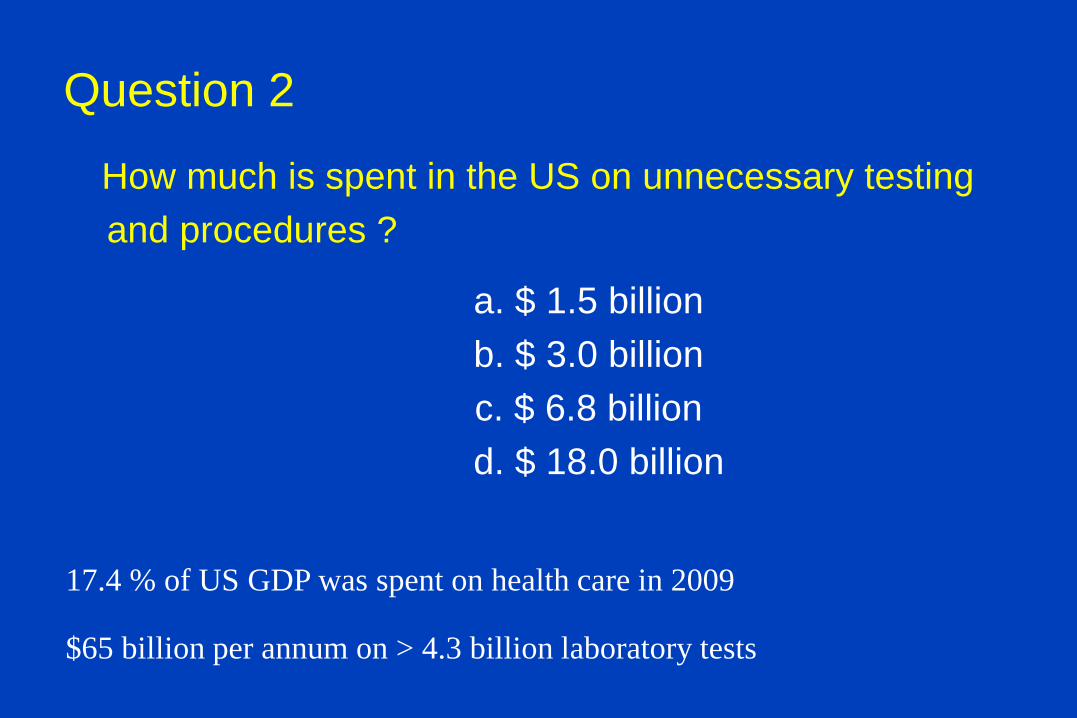
Question 2
How much is spent in the US on unnecessary testing and procedures ?
a. $ 1.5 billion b. $ 3.0 billion c. $ 6.8 billion
d. $ 18.0 billion
17.4 % of US GDP was spent on health care in 2009
$65 billion per annum on > 4.3 billion laboratory tests
Unnecessary testing
• Australia – Vit D requests increased by 4,600 % from 2002/3 to 2011/12 !!
• 73,000 requests pa to 3.5million requests pa
Vasikaran ,Ann
Clin Biochem 2013: 50: 283 - 4
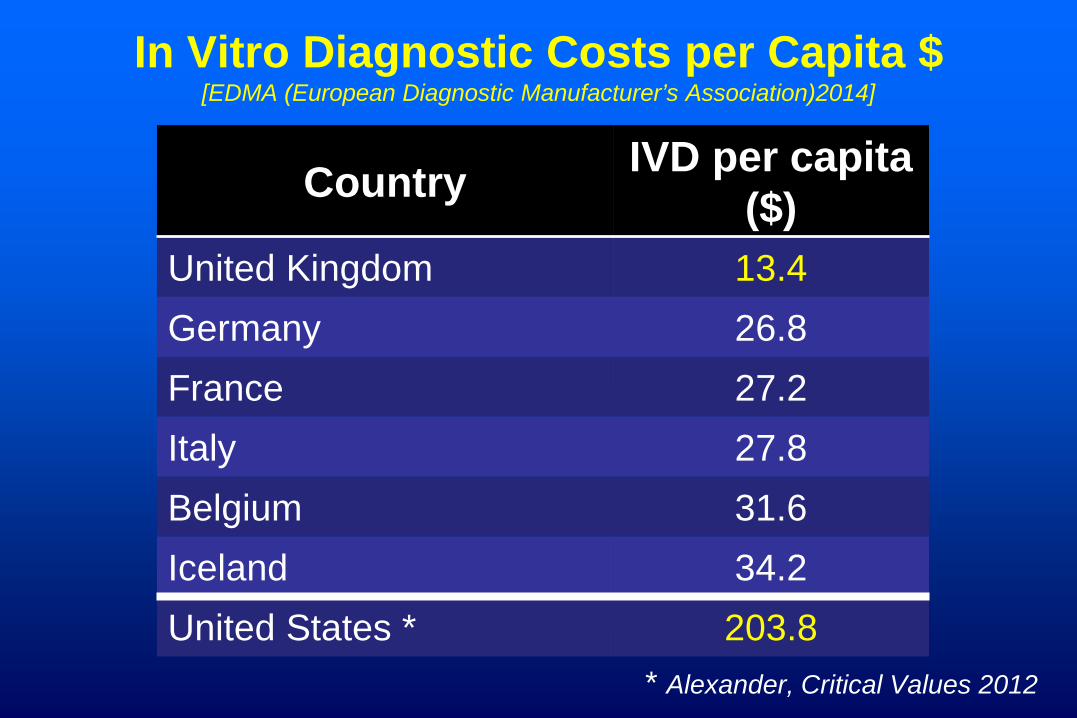
In Vitro Diagnostic Costs per Capita $ [EDMA (European Diagnostic Manufacturer’s Association)2014]
Country IVD per capita ($)
United Kingdom 13.4 Germany 26.8 France 27.2 Italy 27.8 Belgium 31.6 Iceland 34.2 United States * 203.8
* Alexander, Critical Values 2012

Some Causes of Overutilization
• Patient pressure
• Duplicate requesting
• Lack of understanding of the diagnostic value of a test
– “just in case”
• Ordering ‘wrong’ test
• Failure to understand the consequences of overutilization
• Defensive testing
• Perverse financial incentives (more tests = more revenue)
• “Availability creates demand “
Consequences of Overutilization
• Increased resource utilization
• Incorrect diagnosis and treatment
• Incorrect test ordering delays diagnosis
• Increased length of stay
• Patient alarm
• Contribute to blood loss
SYSTEMATIC REVIEW:
In the US, extent of tests not followed up: anything up to 62% of lab tests and 35% of radiology reports
Callen et al,
Journal of General Int. Med (2012); 27 (10), 1334 – 1348.
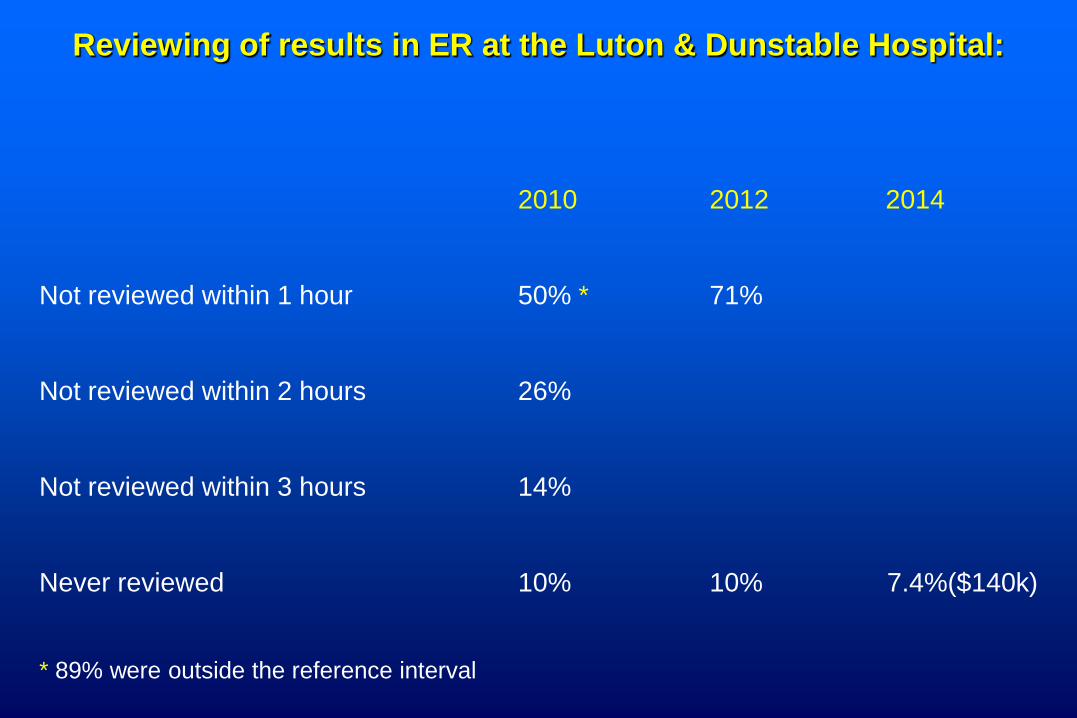
Reviewing of results in ER at the Luton & Dunstable Hospital:
2010 2012 2014
Not reviewed within 1 hour 50% * 71%
Not reviewed within 2 hours 26%
Not reviewed within 3 hours 14%
Never reviewed 10% 10% 7.4%($140k)
* 89% were outside the reference interval
In the UK • Laboratory investigations £2.5 billion / year ( ie $3.6b ) • Approximately 4% of total NHS expenditure • Annual increase in workload 8-10% • 25% of pathology tests unnecessary
– Department of Health Independent Review of Pathology Services 2009
• BUT same amount of under requesting?
• Local audit July 2012 – Inpatients 34% “inappropriate”
Studies outside the UK 4.5 – 95% inappropriate lab use Van Walraven JAMA: 1998 (US) 5.1% Weydert Arch Pathol Lab Med: 2005: 129: 1141-1143 (US) 21% (No reason and low yield) Pal et al JMGIMS: 2009: 14: ii: 40-46
(India) 30% “Consensus” estimate AACC Webinar 26th Oct 2010 30% Repeat testing van Walraven Clin Chem 2003;49:12 (Canada)
Lab-related causes of diagnostic error
• Inappropriate test ordered • Appropriate test not ordered • Appropriate test result not used properly
– Knowledge deficit – wrong interpretation – Misleading result
• Appropriate test result delayed/missed • Appropriate test result wrong – RARE! (Epner & Astion, 2012) Wrong test choice accounts for up to 50 – 60% of
missed / delayed diagnoses ( Plebani, 2010)
Primary Care Physicians Challenges in Ordering Clinical Laboratory Tests and
Interpreting Results Physicians order tests in 31% of patient
encounters 14.7% report uncertainty about ordering 8.3% report uncertainty about interpreting Potentially affects 23 million patients pa Hickner et al JABFM 2014; 27: 268-274
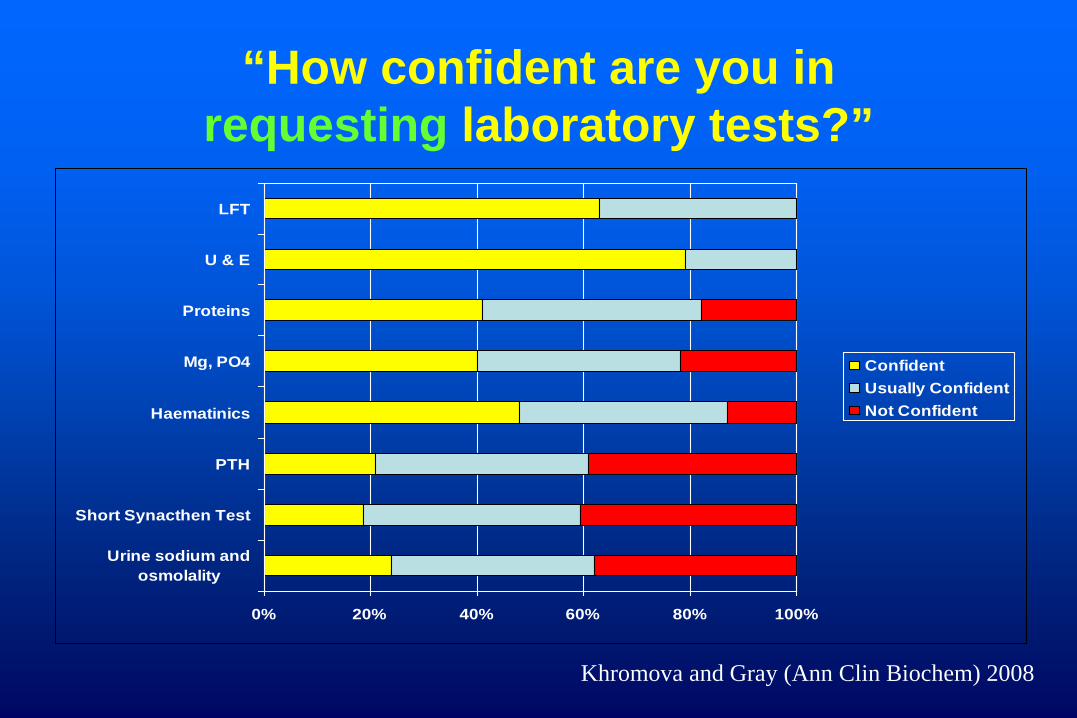
“How confident are you in requesting laboratory tests?”
0% 20% 40% 60% 80% 100%
Urine sodium andosmolality
Short Synacthen Test
PTH
Haematinics
Mg, PO4
Proteins
U & E
LFT
ConfidentUsually ConfidentNot Confident
Khromova and Gray (Ann Clin Biochem) 2008
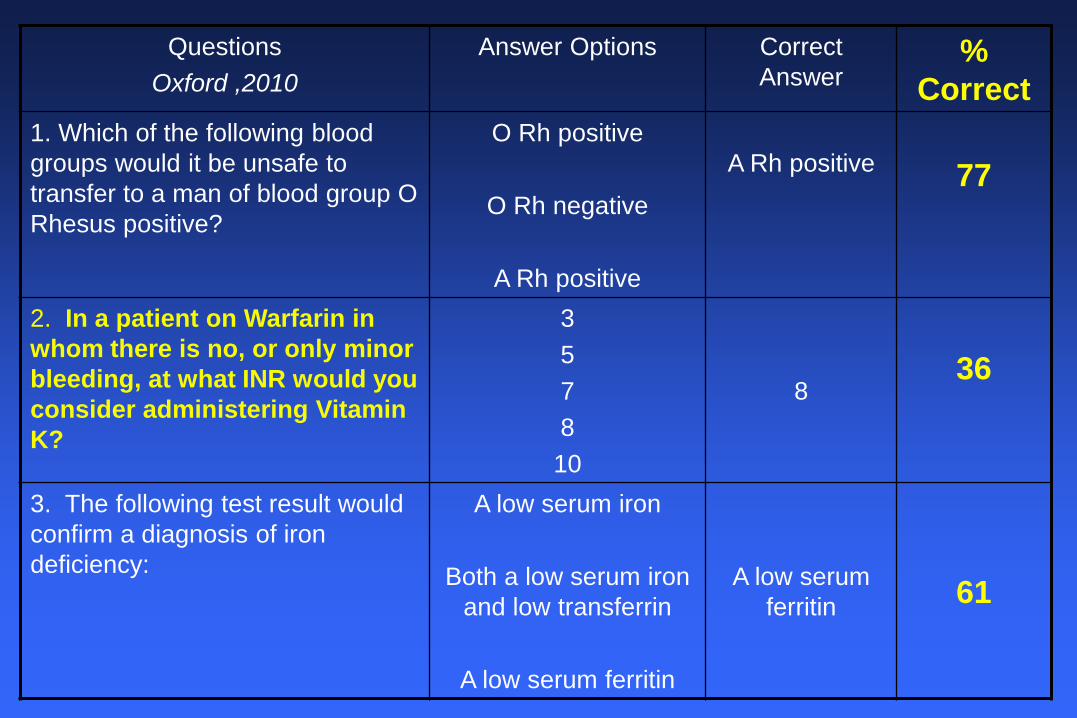
Questions Oxford ,2010
Answer Options Correct Answer
% Correct
1. Which of the following blood groups would it be unsafe to transfer to a man of blood group O Rhesus positive?
O Rh positive
O Rh negative
A Rh positive
A Rh positive
77
2. In a patient on Warfarin in whom there is no, or only minor bleeding, at what INR would you consider administering Vitamin K?
3 5 7 8 10
8
36
3. The following test result would confirm a diagnosis of iron deficiency:
A low serum iron
Both a low serum iron and low transferrin
A low serum ferritin
A low serum ferritin
61
The Problems
• Too many tests
• Different names
• Different units
• Different reference intervals
• Different alert limits
• Inconsistent guidelines
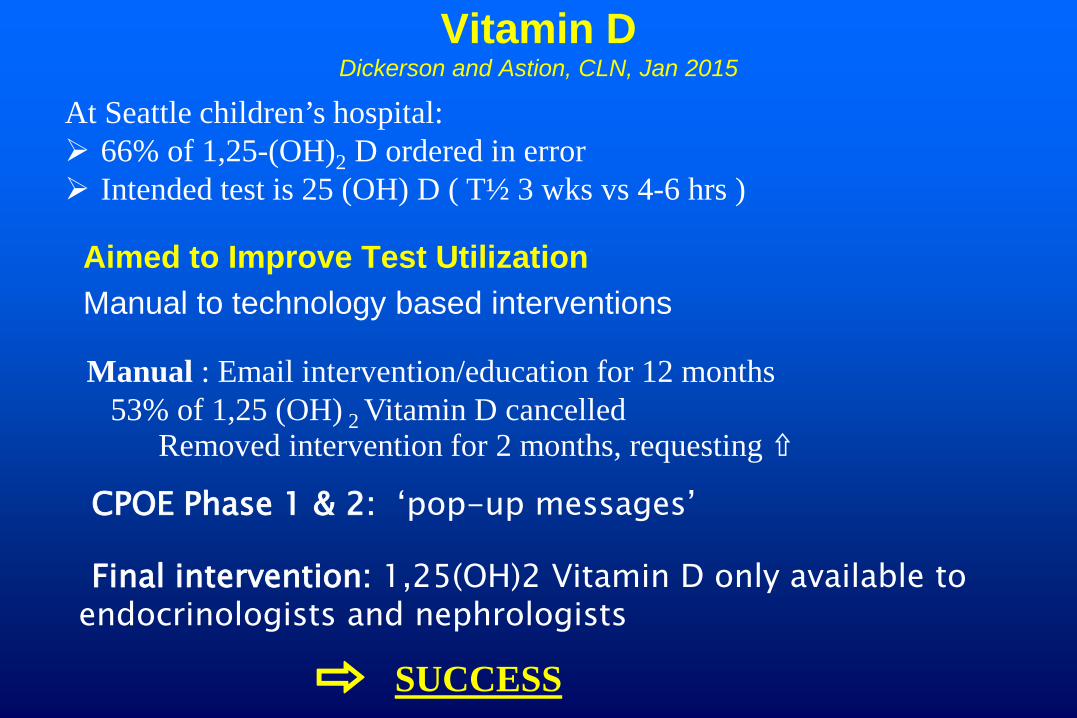
Vitamin D Dickerson and Astion, CLN, Jan 2015
Aimed to Improve Test Utilization Manual to technology based interventions
At Seattle children’s hospital: 66% of 1,25-(OH)2 D ordered in error Intended test is 25 (OH) D ( T½ 3 wks vs 4-6 hrs )
⇨ SUCCESS
Manual : Email intervention/education for 12 months 53% of 1,25 (OH) 2 Vitamin D cancelled
Removed intervention for 2 months, requesting ⇧
Final intervention: 1,25(OH)2 Vitamin D only available to endocrinologists and nephrologists
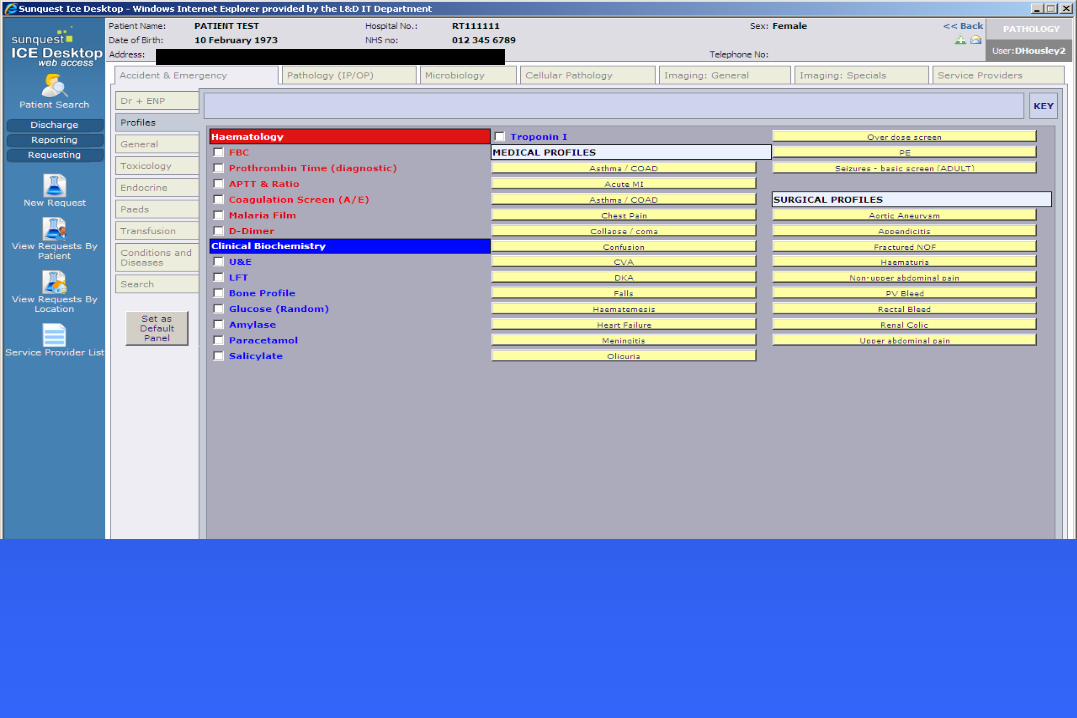
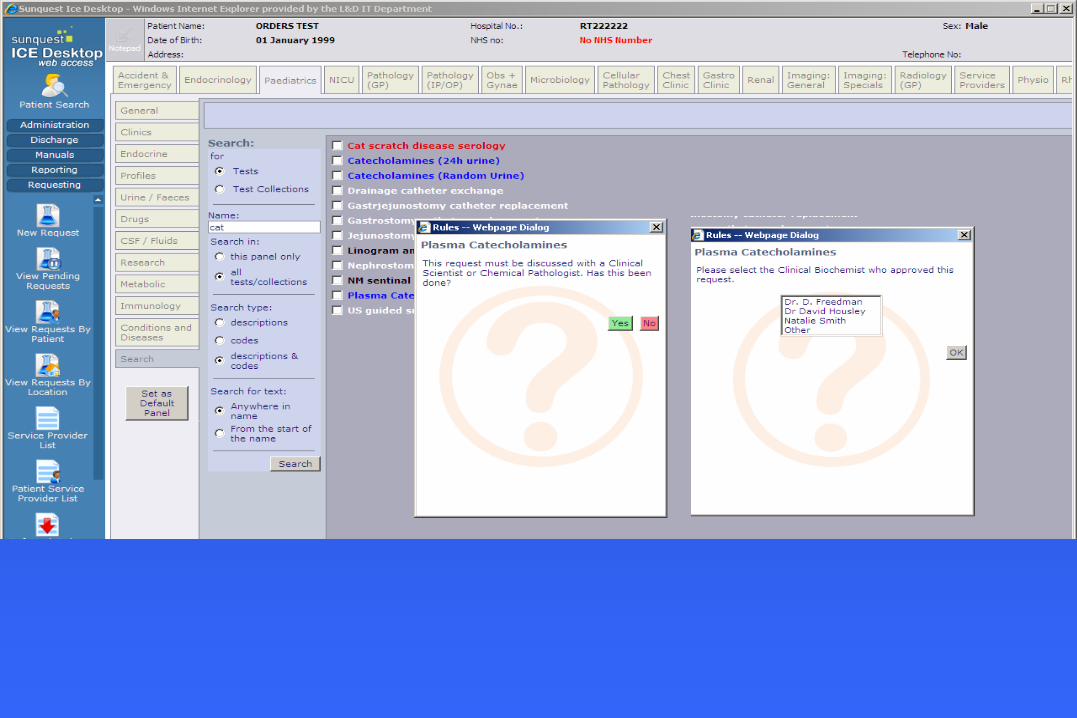
CPOE Phase 1 & 2: ‘pop-up messages’
UK implementing an England-wide model for EHR presented with an initial pathology catalogue derived from a multiplicity of sources:
– Duplications – Inconsistent naming formats – Ambiguity. Unclear what the lab response to a request should
be – Not fit for purpose of applying national codes (SNOMED)
UK
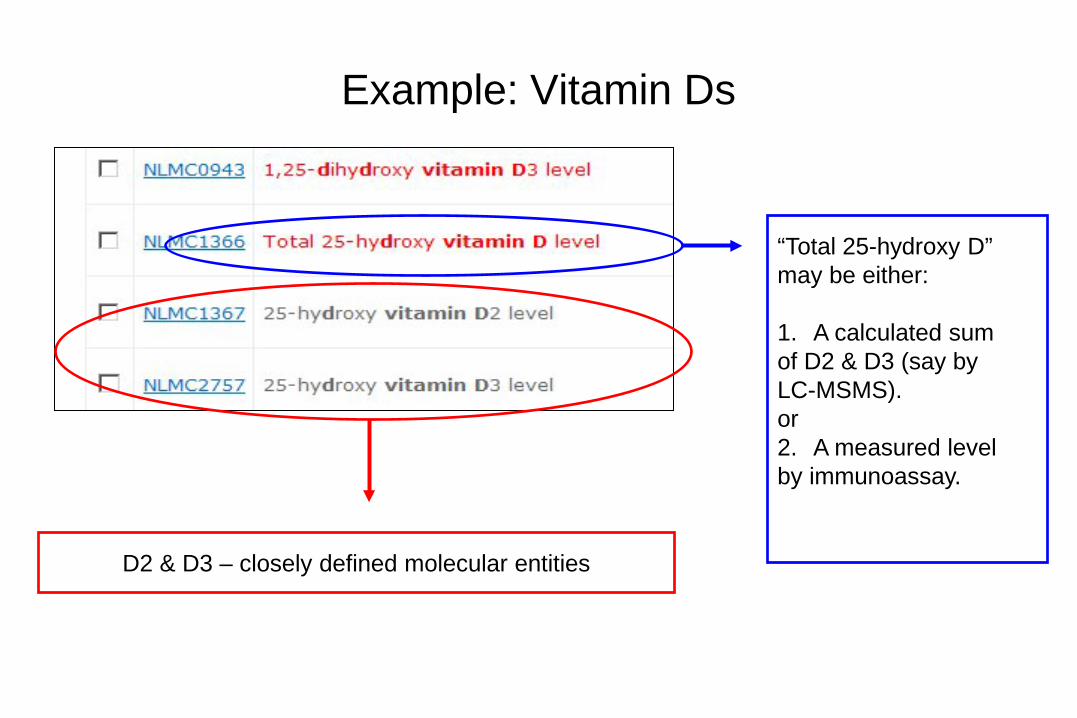
Example: Vitamin Ds
D2 & D3 – closely defined molecular entities
“Total 25-hydroxy D” may be either: 1. A calculated sum of D2 & D3 (say by LC-MSMS). or 2. A measured level by immunoassay.
Strategies for Changing Physician Behaviour in Ordering Lab Tests
• Bandolier Review of 49 articles between 1966 and 1998
• Strategies that don’t work by themselves • Physician consensus building • Test guideline dissemination • Traditional education • Utilisation audits • Inform physicians of lab test charges

Published:
J Clin Path
BMJ
Box 1 Minimum Re-testing Interval Work Streams Renal Liver and Bone Endocrine Lipids and Diabetes Specific Proteins Cardiac Tumour Markers Gastro-Intestinal Occupational/Toxicology Therapeutic Drug Monitoring Pregnancy and Paediatrics
National Minimum Re-testing Interval Project 2013: A final report detailing consensus recommendations for
minimum re-testing intervals for use in Clinical Biochemistry
The Association for Clinical Biochemistry and Laboratory Medicine
To be published Summer 2015: National Minimum Re-testing Intervals: • Clinical Biochemistry [see previous] • Haematology – general, coag, transfusion • Immunology • Microbiology • Virology • Cellular Pathology
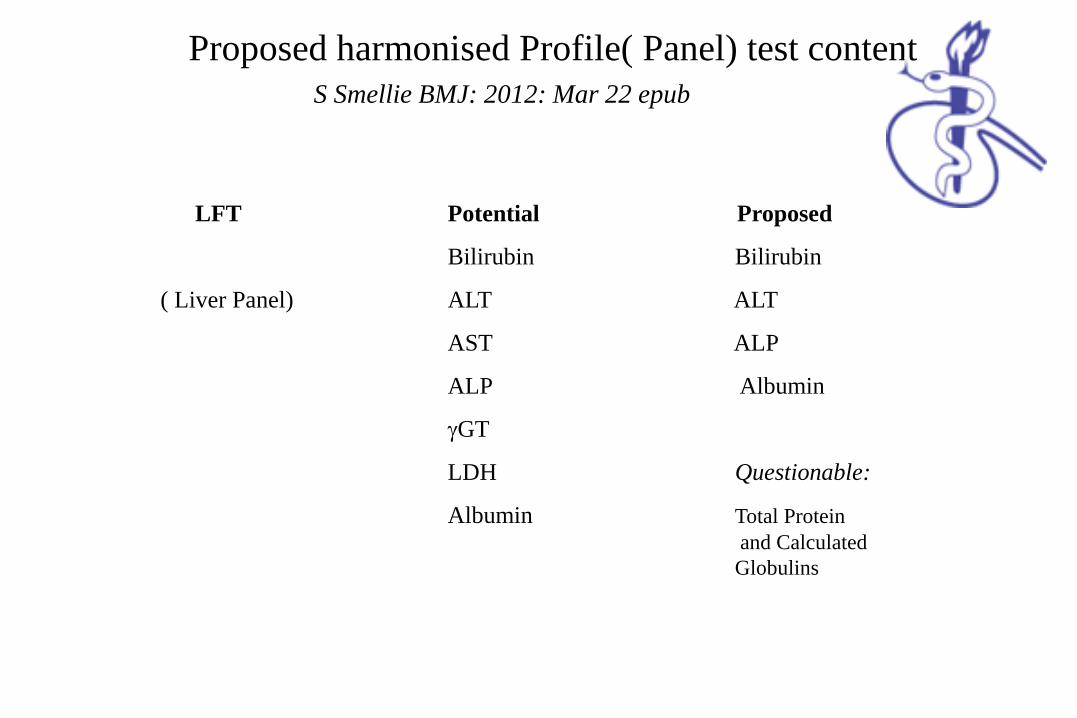
Proposed harmonised Profile( Panel) test content S Smellie BMJ: 2012: Mar 22 epub
Profile Potential content Proposed content
PoiPPotent
LiLFT Potential Proposed
Bilirubin Bilirubin
( Liver Panel) ALT ALT
AST ALP
ALP Albumin
γGT
LDH Questionable:
Albumin Total Protein and Calculated Globulins
UK: “ Do not Do” [NICE April 2014]
US: “Choosing Wisely” [NEJM 2014]
Atrius Health (2014) [ACO]
Guidelines for an annual physical
Displaying cost information
Liver function tests in patients on statins
Vitamin D - education
Incentive : Reimbursement paid in form of capitation, for 70% of patients
$1 Million
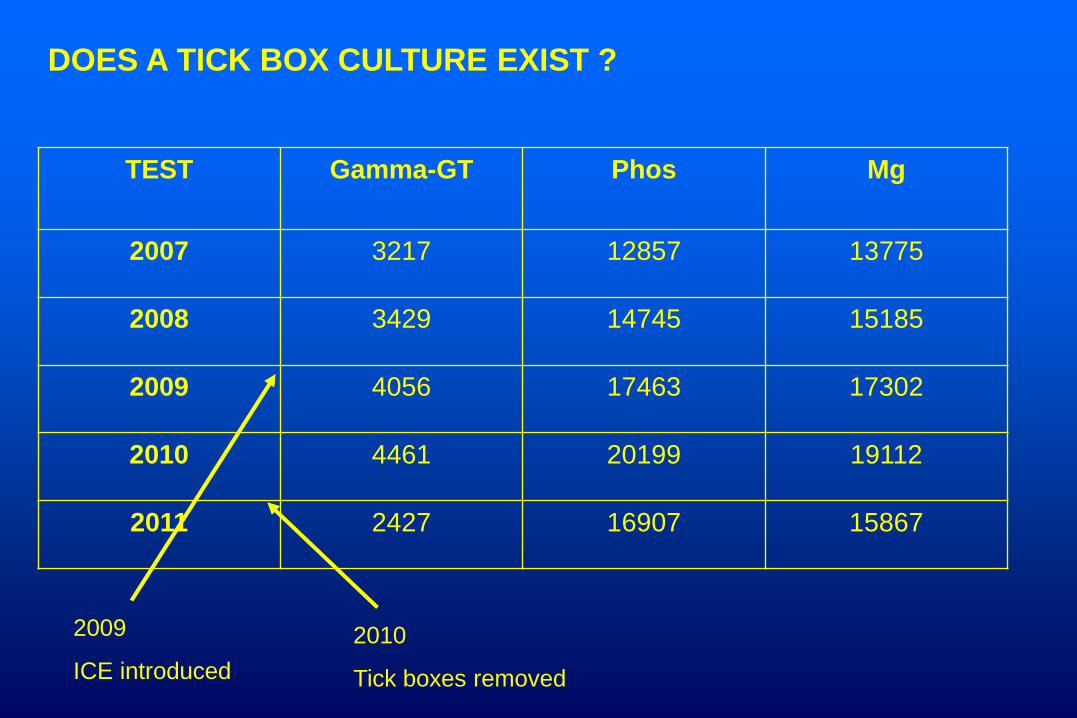
TEST Gamma-GT Phos Mg
2007 3217 12857 13775
2008 3429 14745 15185
2009 4056 17463 17302
2010 4461 20199 19112
2011 2427 16907 15867
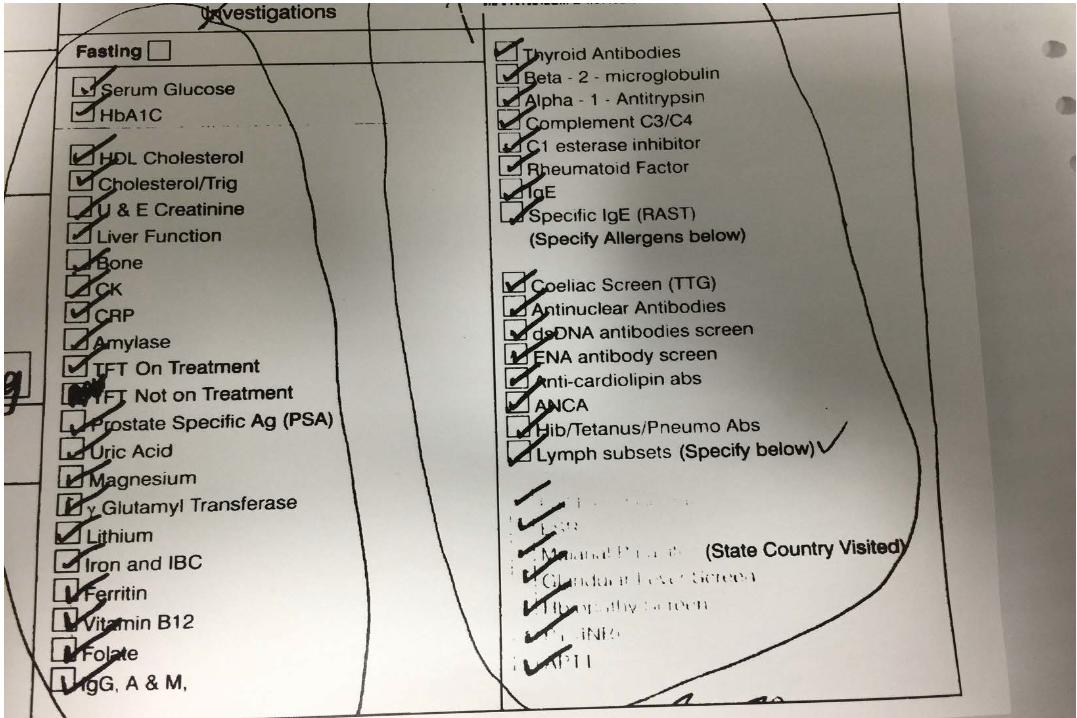
DOES A TICK BOX CULTURE EXIST ?
2009
ICE introduced 2010
Tick boxes removed
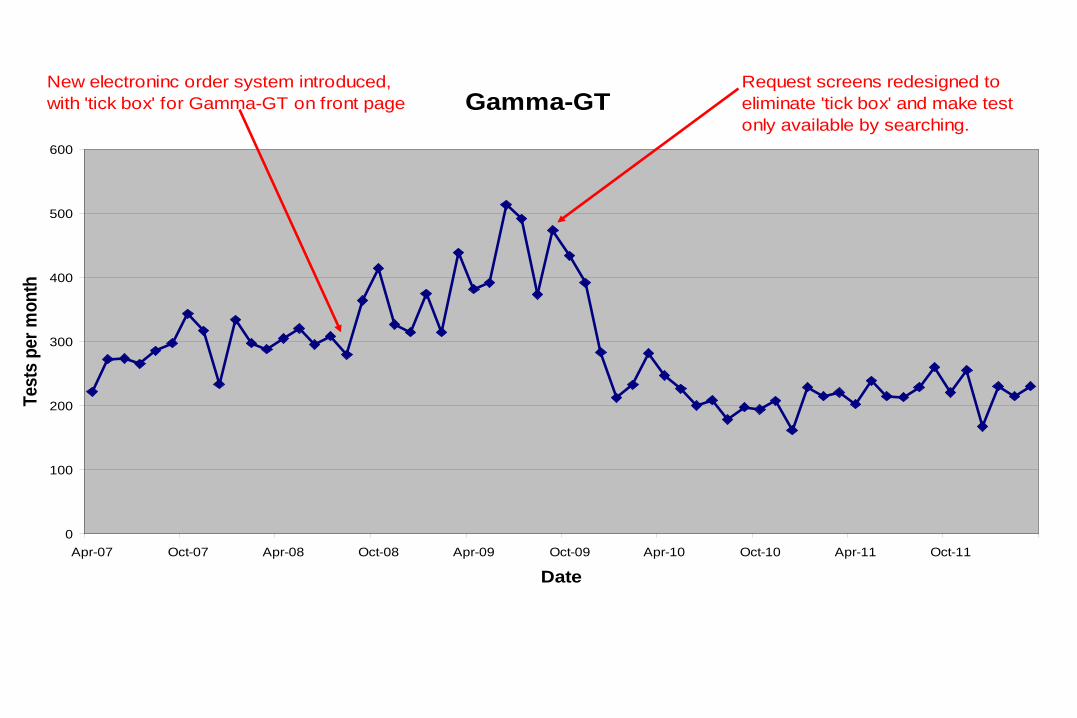
Gamma-GT
0
100
200
300
400
500
600
Apr-07 Oct-07 Apr-08 Oct-08 Apr-09 Oct-09 Apr-10 Oct-10 Apr-11 Oct-11
Date
Test
s pe
r mon
th
New electroninc order system introduced,with 'tick box' for Gamma-GT on front page
Request screens redesigned to eliminate 'tick box' and make testonly available by searching.
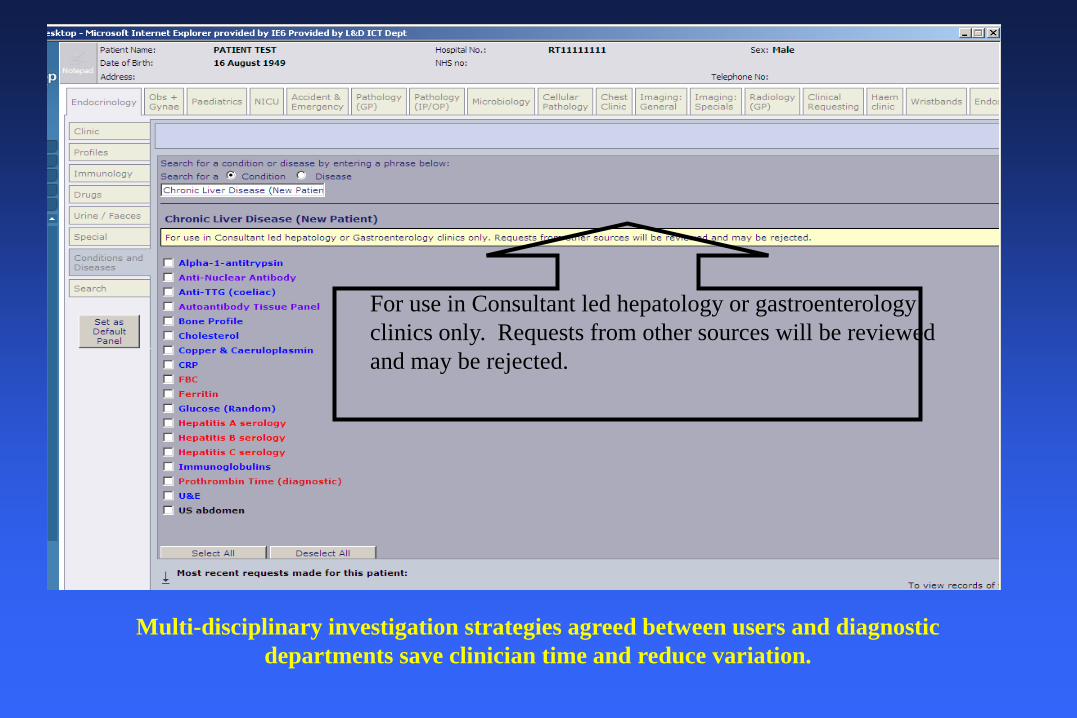
Multi-disciplinary investigation strategies agreed between users and diagnostic departments save clinician time and reduce variation.
For use in Consultant led hepatology or gastroenterology clinics only. Requests from other sources will be reviewed and may be rejected.
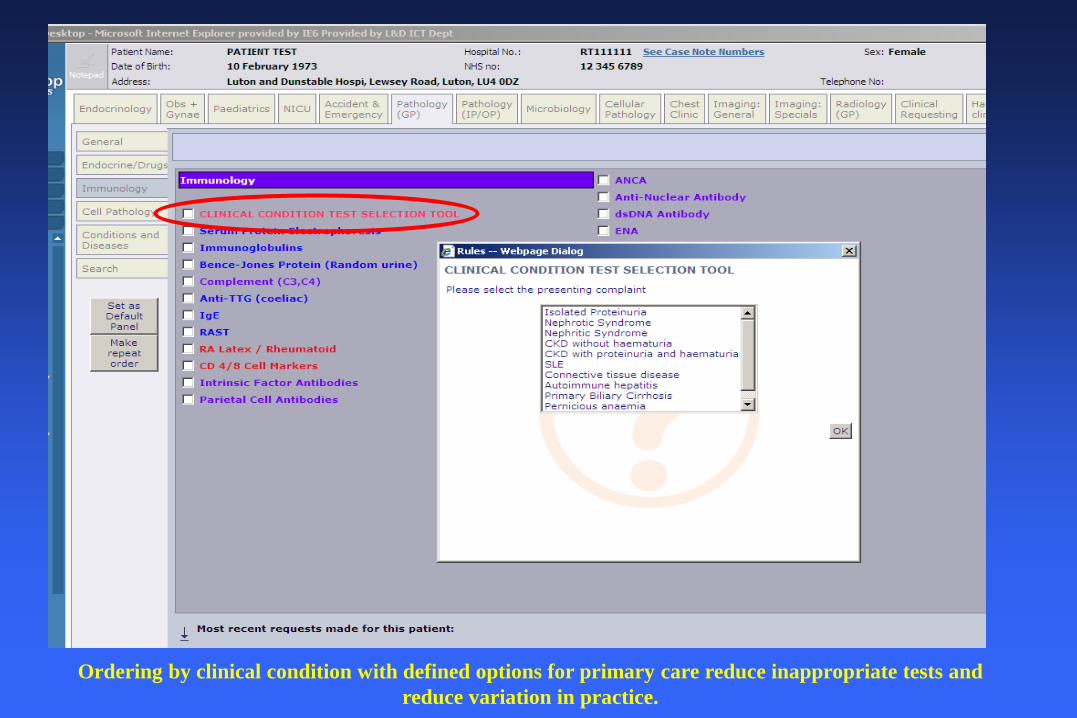
Ordering by clinical condition with defined options for primary care reduce inappropriate tests and reduce variation in practice.
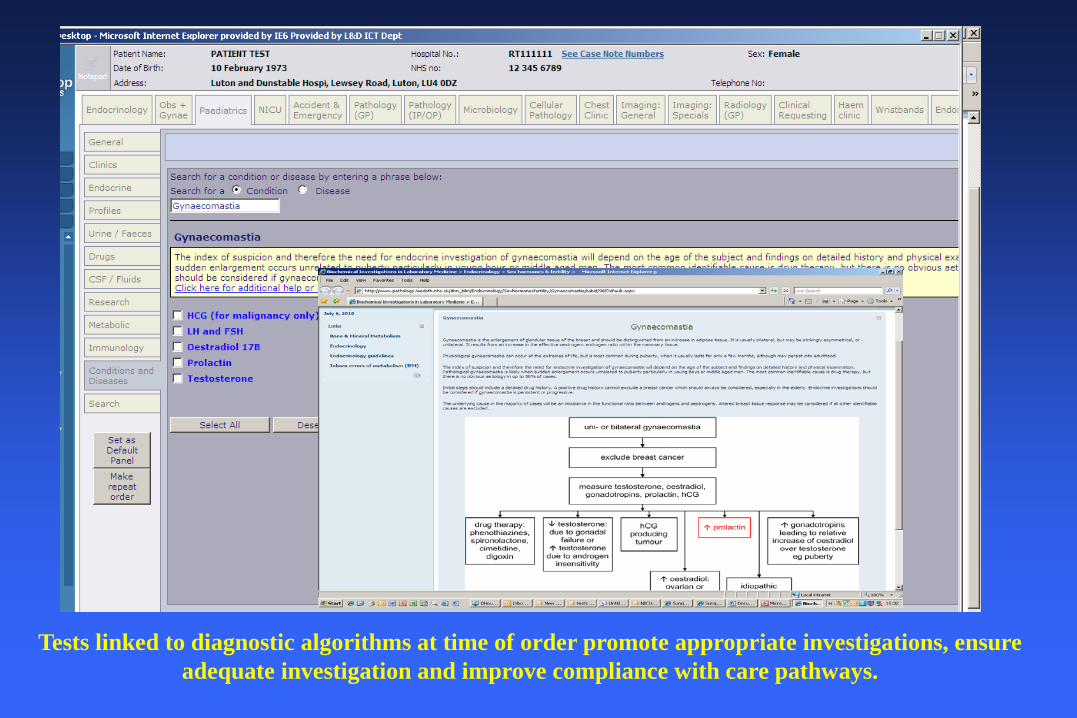
Tests linked to diagnostic algorithms at time of order promote appropriate investigations, ensure adequate investigation and improve compliance with care pathways.
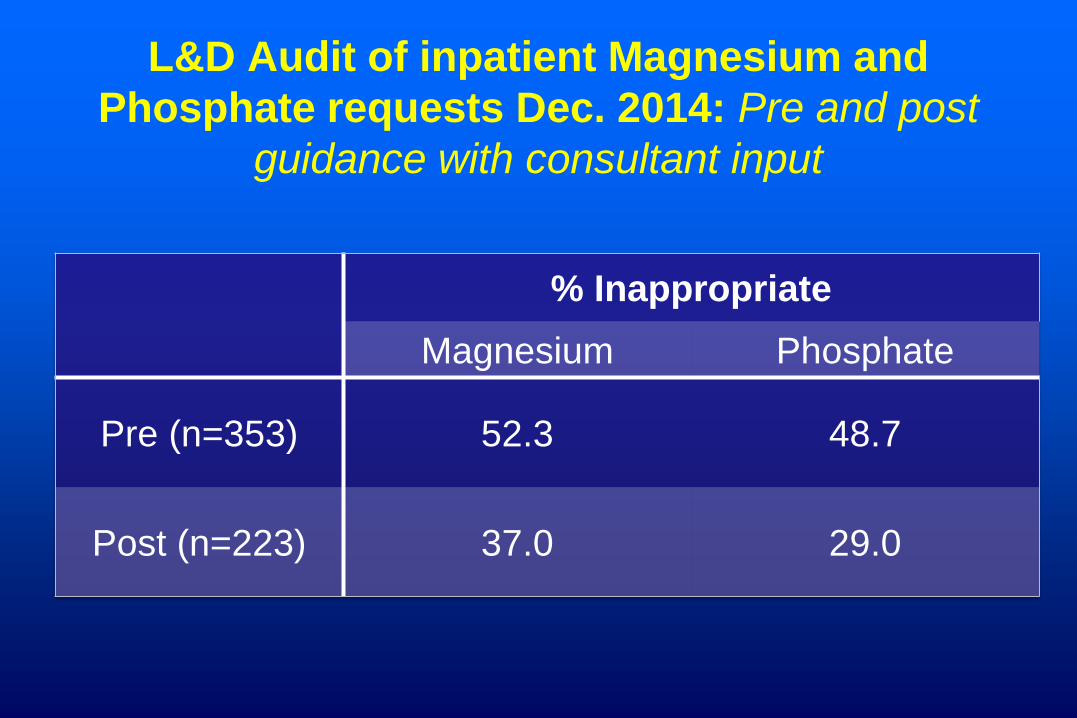
L&D Audit of inpatient Magnesium and Phosphate requests Dec. 2014: Pre and post
guidance with consultant input
% Inappropriate Magnesium Phosphate
Pre (n=353) 52.3 48.7
Post (n=223) 37.0 29.0
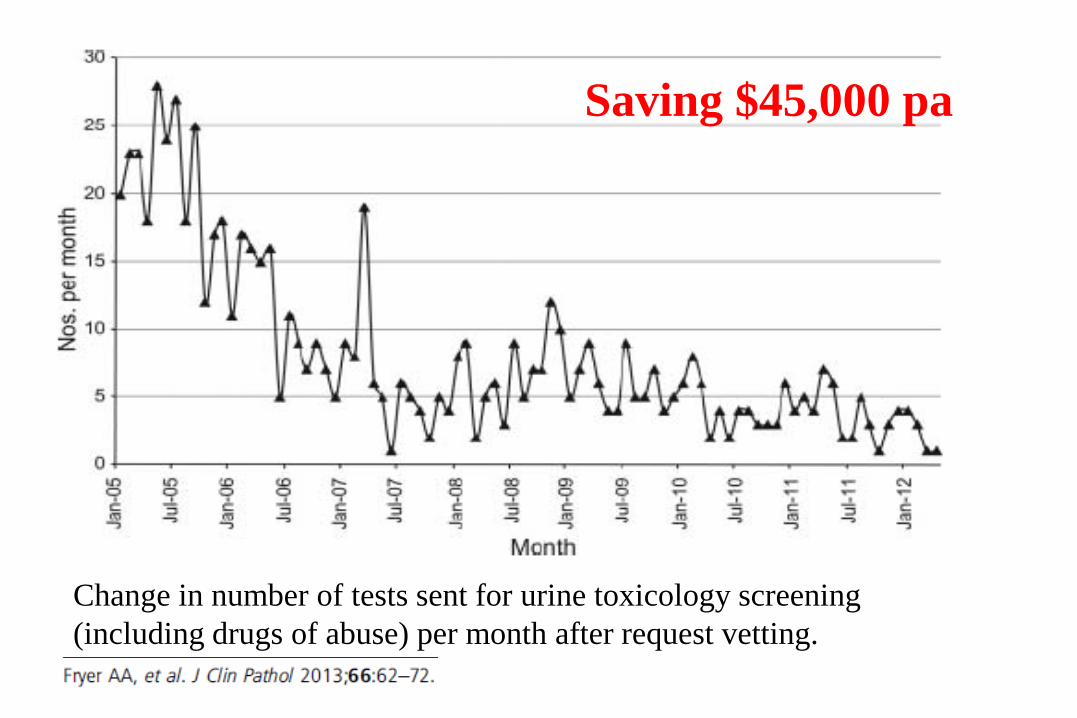
Change in number of tests sent for urine toxicology screening (including drugs of abuse) per month after request vetting.
Saving $45,000 pa

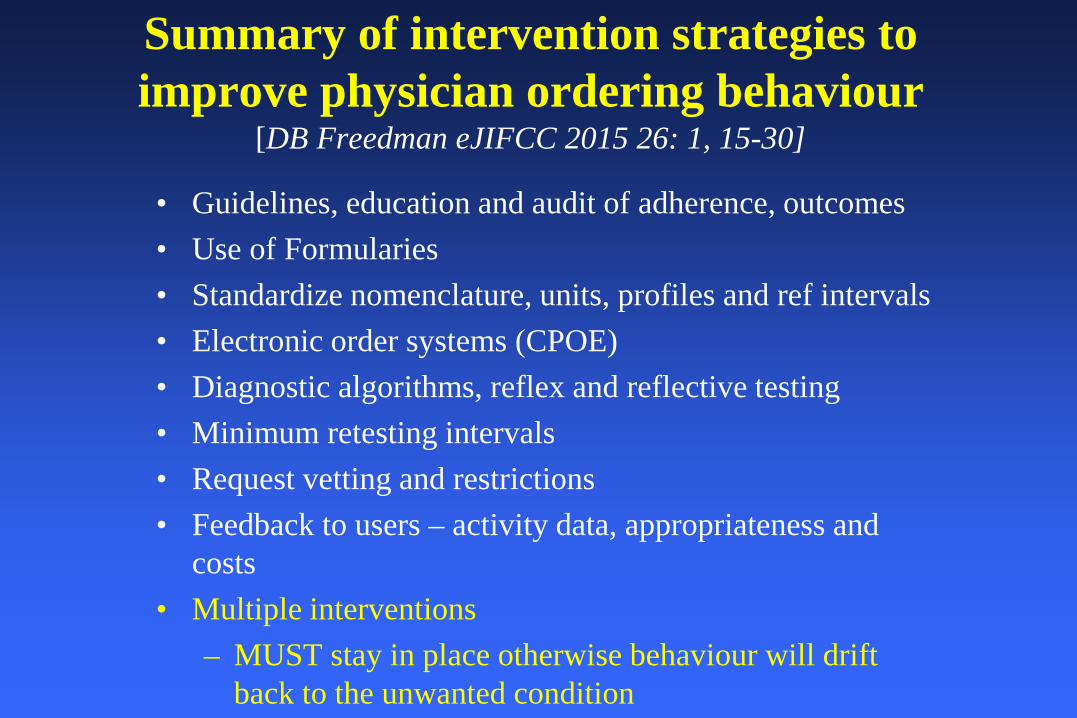
Summary of intervention strategies to improve physician ordering behaviour
[DB Freedman eJIFCC 2015 26: 1, 15-30]
• Guidelines, education and audit of adherence, outcomes • Use of Formularies • Standardize nomenclature, units, profiles and ref intervals • Electronic order systems (CPOE) • Diagnostic algorithms, reflex and reflective testing • Minimum retesting intervals • Request vetting and restrictions • Feedback to users – activity data, appropriateness and
costs • Multiple interventions
– MUST stay in place otherwise behaviour will drift back to the unwanted condition
Zhi et al (2013)
• Overall mean rate of inappropriate overutilization = 20.6% (95% CI 16.2 – 24.9%, n=114)
• Overall mean rate of underutilization = 44.8% (95% CI 33.8-55.8%, n= 18)
IBD and IBS - UK Bloating / distension, abdominal pain, altered bowel
habit – common Clinical exam / history alone not always reliable –
DIAGNOSTIC DILEMMA Coeliac, somatisation, infective, gynae pathology. ? IBD
Patients per year
• Ulcerative Colitis 120,000 • Crohn’s 60,000 • IBS* 9 million
*UK population Approx 60 million IBS incidence 10-20% Average 15%
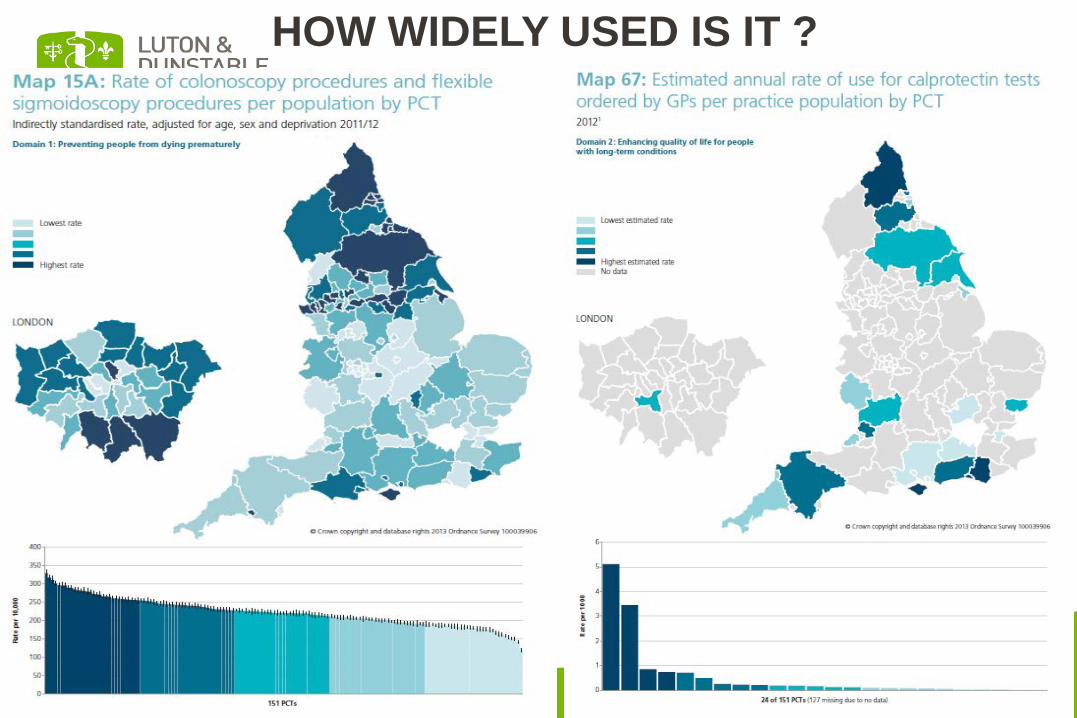
HOW WIDELY USED IS IT ?
CALPROTECTIN CLINICAL USE
• Distinguishes functional (IBS) symptoms from organic symptoms (inflammatory) - >95% sensitivity and specificity
• Normal result excludes IBD and requirement to scope
• Sigmoidoscopy tarriff = $790, Colonoscopy $1040 • Faecal calprotectin testing = $70
• Luton experience (patients referred where diagnosis
of organic versus functional disease uncertain): – In secondary care, – 70% reduction in Endoscopy – Potential saving $68,000 per 100 patients
Reflective “Add on” Tests Case: 65y/o F c/o tingling and cramps
Initially GP requested Bone profile Adjusted Calcium 7.2 mg/dL (9-11)
Subsequently GP requested PTH and Vitamin D PTH Low Vitamin D Normal
Discussion with GP – patient on Omeprazole (PPI) for 3yrs
Magnesium added Magnesium 0.60 mg/dL
(1.8-3.6)
Case: 65y/o F c/o tingling and cramps Hypomagnesaemia
Cardiac dysrhythmia, including ventricular fibrillation
Emergency Admission $2400 plus
Stay on CCU $1200/day

International Health Rankings (Commonwealth Fund, 2014)
AU CH CA DE FR NL NO NZ SE UK US
Overall rank 4 2 10 5 9 5 7 7 3 1 11 Safe care 3 4 10 6 2 7 11 8 5 1 7 $ Per capita 2011 3800 5643 4522 4495 4118 5099 5669 3182 3925 3405 8508
A final thought….
“We need to recognise that the target (of requesting the test and the results) should be the patient. It is the person who actually, in the end, is going to have to change their lives and start adopting new behaviours….”
adapted from Thomas Goetz, 2010 The Decision Tree: taking control of your health in the New Era of personalised medicine.
With grateful thanks to:
Dr David Housley, BSc(Hons), MSc, PhD, FRCPath Luton, UK Rebecca Leyland ,BSc(Hons), MSc,Dip RCPath Luton, UK




























