Embed Size (px)
Citation preview
OMM EXAM 114 September 2010
CARDIOLOGY
TOSTreatment
Home exercise – individualized prescription 1. Common hypertonic muscles
Lengthen to symmetryLevator scapulaeUpper TrapSCMScalenesLatissmusPectoralis minor
Reverse kyphosisThoracic extension exercises
TOSTreatment Common weak/lengthened muscles
Retraining (strengthening) to symmetry Serratus Anterior Middle Trapezius / Rhomboids Lower Trapezius
Dynamic stabilizers
Sympathetic innervation of the heart?
T1-T6
F(x) of sympathetics of the heart? Right side specifically? Left side specifically?
Increase heart rate, increase contractile force, shorten systole
Right side innervates right heart and SA nodePredisposition to supraventricular
tachyarrhythmias (A-fib, SVT) Left side innervates left heart and AV
nodePredisposition to ectopic foci and ventricular
fibrillation Asymmetries in sympathetic tone may
play a role in serious arrhythmias
Level of sympathetic innervation of the heart vessels?
F(x)?
T1-L2 F(x): Vasoconstriction
Parasympathetic innervation of the heart?
Vagus nerve
F(x) of right vagus n? F(x) of left vagus n?
Right Vagus Innervates SA nodeSinus Bradyarrhythmias
Left Vagus Innervates AV nodeAV blocks
Name somatic dysfunctions causing vagal reflexes?
Areas of significant vagal connections Occipitomastoid sutrue, OA, AA, and C2
F(x) of parasypathetics of vessels?
Involved in regulation of peripheral arteriolar vasculature in select areasSubmaxillary Gland Vessels (CN VII), Parotid
gland (CN IX), blush region of the face, tongue (lingual nerve), penis
Definition of Reflex
An involuntary nervous system response to a sensory input. The sum total of any particular involuntary activity
Definition of viscerosomatic reflex
Localized visceral stimuli producing patterns of reflex response in segmentally related somatic structures
Definition of facilitation
The maintenance of a pool of neurons (e.g., premotor neurons, motor neurons or preganglionic sympathetic neurons in one or more segments of the spinal cord) in a state of partial or subthreshold excitation; in this state, less afferent stimulation is required to trigger the discharge of impulses
Definition of viscerosomatic pain
• Nociceptive fibers from the viscera are interpreted as somatic pain and can cause somatic dysfunction
Cause of myocardial infarction?
The result of blockage, partial or complete, of a coronary artery leading to disruption of blood supply to the myocardium causing myocardial ischemiaCommonly caused by arteriosclerotic
plaque
Sx of MI?
Chest pain (crushing), radiation of pain to left arm, jaw, or epigastrum, diaphoresis, heightened sense of anxiety
(Viscerosomatic reflex)
Once patient is stable after an MI, what is your next course of action?
Focus on decreasing myocardial oxygen demand and normalizing autonomic innervationOA release, C2, thoracic inlet, rib raising,
T1-6, lymphatic techniques
What is the main goal for post MI patients?
Lower sympathetic tone
What techniques/areas do you focus on to decreases peripheral vascular resistance and cardiac workload?
Focus on indirect techniques Rib and sternum dysfunction (from CPR,
open heart surgery) Hyoid dysfunction (fascial continuity of
mediastinum
What % of adults are diagnosed with HTN?
85%
What BP is considered to be hypertensive?
Systolic Blood Pressure (SBP) >140 and / or Diastolic BP (DBP) >90 usually on 2 separate occasions
Etiology of HTN?
Multifactorial etiology with genetic predisposition aggravated by environmental, habitual, and physiological factors
What are common functional elements of HTN?
Vascular and cardiac hypersensitivity to sympathetic stimuli
Prolonged sympathetic stimuli to the kidneysCauses functional salt and water retention and
increasing arterial pressure Venoconstriction causing increased cardiac
output with normal peripheral resistanceEventual increase in peripheral resistance to
reduce cardiac output Prolonged HTN causes baroreceptors in the
carotid sinus to reset and maintain the increased arterial pressure
Osteopathic considerations for HTN?
Reduce stress: General OMT, Behavior Modification
Decrease sympathetic tone: Focus on the entire spinal column, Rib raising,
etc. Encourage parasympathetic tone:
OA, cervical OMT, sacral rocking Improve lymphatic drainage:
Open diaphragms, pectoral traction Address Chapman’s reflexes for kidneys and
adrenals “Whatever technique is used, it should be slow-
moving and gentle to augment rest and relaxation, promote autonomic balance and release fascial contractures
Definition of arrhythmia
Disruption of the electrical conduction system of the heart
Etiology of arrhythmia
MI / tissue damage (most common) Congenital (e.g. Septal defects) Unknown
What areas should you focus on when doing OMT on a patient with an arrhythmia?
Focus on T 1-6, Rib dysfunctions, OA, C2, Chapman’s points, and lymphatic movement
Definition of congestive heart failure?
The inability of the heart to maintain adequate circulation of blood in the tissues of the body or to pump out the venous blood returned to it by the venous circulation
Leads to accumulation of fluid throughout the body
Cause of CHF?
• Chronic HTN, congenital abnormalities, valvular defects, loss of heart muscle
Sx of right sided heart failure? Sx of left sided heart failure?
Right sided heart failure: edema of lower extremities
Left sided: pulmonary edemaCough, dyspnea (especially while lying
supine)
Treatment of CHF?
Treatment of underlying cause Interventional medicine may be necessary Focus on the autonomic system and related
structuresOA, C2, Thoracic Inlet, Rib raising, T 1-6
Lymphatic techniquesBalancing diaphragms, lymphatic pumps,
effleurageCAUTION: avoid overloading the heart with
excessive peripheral fluid Chapman’s points Correction of other somatic dysfunctions
To reduce unnecessary work in the use of the extremities and postural muscles
How do you treat Type I (T1-3 RlSr) with ME?
Patient seated, Dr standing opposite side of rotation, Monitoring Apex of curve (T2)
Side bend patient head L until motion felt at T2
Rotate patient head R until motion felt at T2 Patient tries to side bend R and rotate L
against resistance Hold for 3-5 seconds, relax for 1-2 seconds,
further engage barrier and repeat 2-4 more times.
Passive Stretch, then recheck
How do you treat type II (T4 ESrRr) with ME?
• Patient seated, Dr standing same side of rotation, monitoring T4
• Flex patient head until motion felt at T4• Side bend and rotate patient head to the L until
motion felt at T4• Patient tries to extend, rotate R and side bend R
against resistance• Hold for 3-5 seconds, relax for 1-2 seconds,
further engage barrier and repeat 2-4 more times.• Passive Stretch, then recheck
How do you treat T5-T12 with ME?
Type I (T6 – T10 RrSl) Patient seated, R hand behind
head, L hand on R elbow Dr standing opposite side of
rotation (L) and monitors apex (T8) with right hand
Dr’s L arm goes UNDER patient’s L arm, Dr’s L hand rests on patient’s R antecubital fossa
Rotate patient L until motion felt at apex, then side bend patient R until motion felt at apex.
Patient attempts to sit up straight against resistance
Hold for 3-5 seconds, rest for 1-2 seconds, re-engage barrier and repeat 2-4 times
Passive stretch and recheck.
• Type II (T8 FRrSr)– Patient seated, R hand behind
head, L hand on R elbow– Dr standing opposite side of
rotation (L) and monitors lesion (T8) with right hand
– Dr’s L arm goes OVER patient’s L arm, Dr’s L hand rests on patient’s R antecubital fossa
– Extend, rotate and side bend patient L until motion felt at that lesion
– Patient attempts to sit up straight against resistance
– Hold for 3-5 seconds, rest for 1-2 seconds, re-engage barrier and repeat 2-4 times
– Passive stretch and recheck.
Technique for OA/suboccipital release?
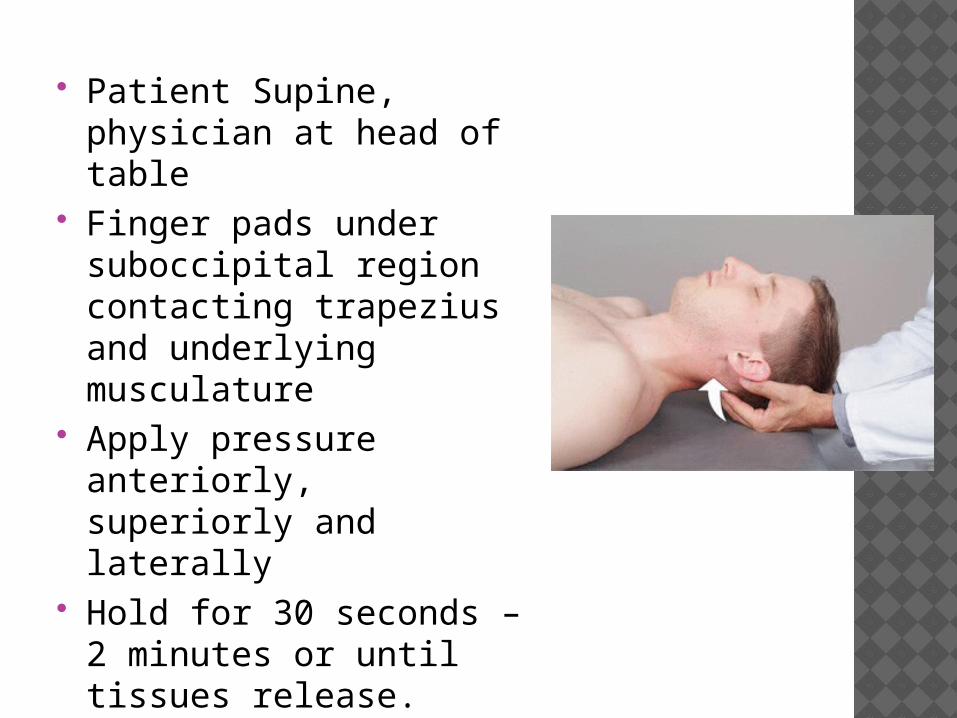
Patient Supine, physician at head of table
Finger pads under suboccipital region contacting trapezius and underlying musculature
Apply pressure anteriorly, superiorly and laterally
Hold for 30 seconds – 2 minutes or until tissues release.
How do you do ME for the AA rotated left?
Patient Supine, physician sits at head of table Flex patient head ( at least 15 – 25 degrees) Rotate head R Patient rotates head L against resistance Hold for 3-5 seconds, rest for 1-2 seconds, re-
engage barrier and repeat 2-4 times Passive stretch and recheck
ME for C2-7 (ex. C3FSrRr) ?
• Patient Supine, physician sits at head of table
• Physician cups patient head, MCP joint of R hand on C3 articular pillar
• Extend neck at C3, rotate and side bend L until motion felt at C3
• Patient flexes head, rotates and sidebends L against resistance
• Hold for 3-5 seconds, rest for 1-2 seconds, re-engage barrier and repeat 2-4 times
• Passive stretch and recheck
Technique for rib raising in the supine position?
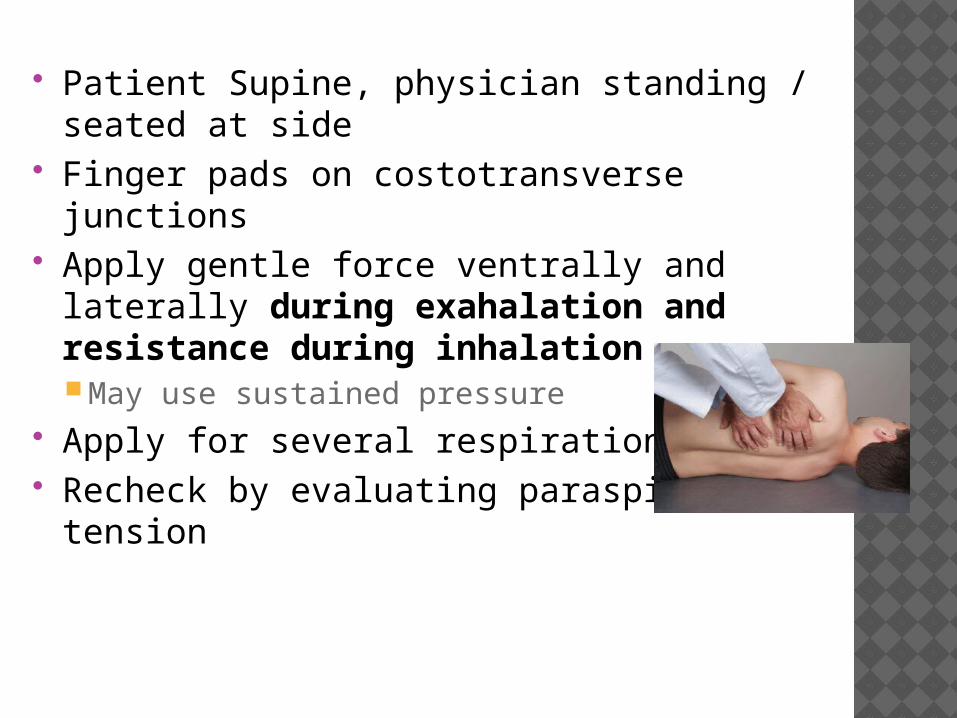
Patient Supine, physician standing / seated at side
Finger pads on costotransverse junctions Apply gentle force ventrally and laterally
during exahalation and resistance during inhalationMay use sustained pressure
Apply for several respirations Recheck by evaluating paraspinal tissue
tension
Technique for rib raising in the seated position?
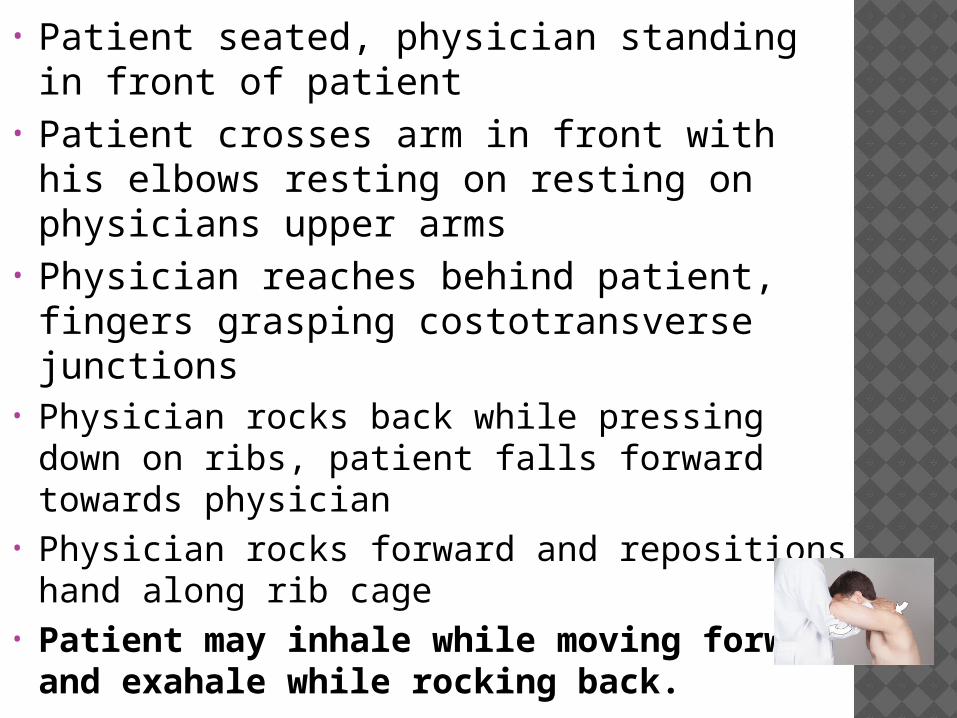
• Patient seated, physician standing in front of patient
• Patient crosses arm in front with his elbows resting on resting on physicians upper arms
• Physician reaches behind patient, fingers grasping costotransverse junctions
• Physician rocks back while pressing down on ribs, patient falls forward towards physician
• Physician rocks forward and repositions hand along rib cage
• Patient may inhale while moving forward and exahale while rocking back.
Technique for myofascial release for T-inlet?
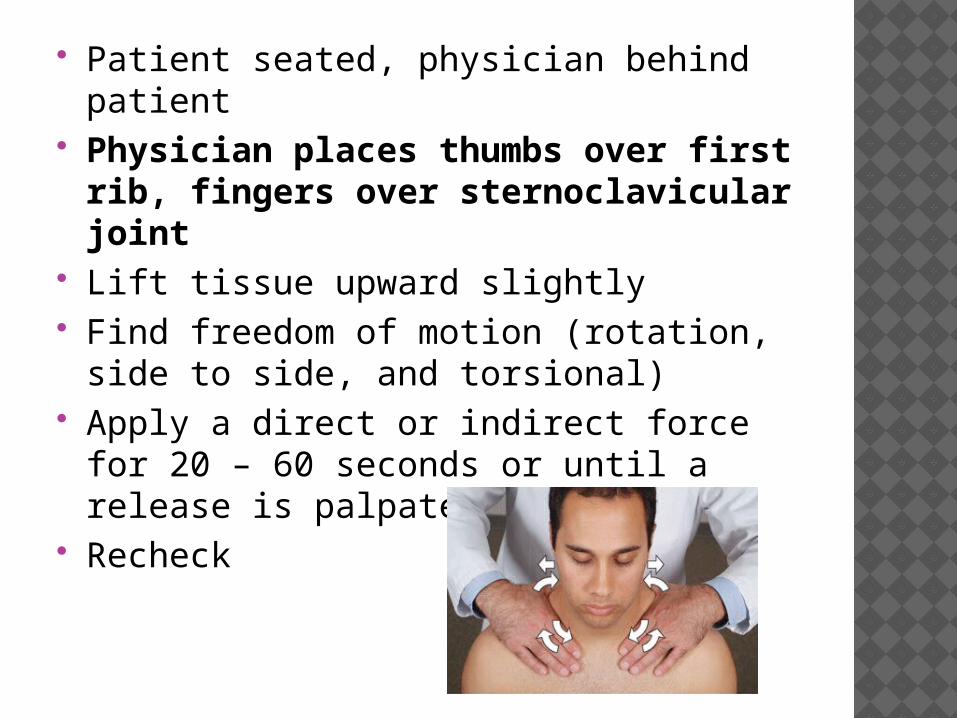
Patient seated, physician behind patient Physician places thumbs over first
rib, fingers over sternoclavicular joint
Lift tissue upward slightly Find freedom of motion (rotation, side to
side, and torsional) Apply a direct or indirect force for 20 – 60
seconds or until a release is palpated Recheck
Technique for myofascial Release for Hyoid, Sternum, and Ribs?
Hyoid / Cricoid Release (Nicholas p. 416)Patient Supine, physician beside patient
stablizes patient head with cephalad hand beneath the head or grasping forhead
Caudad hand gently grasps anterior cervical arches
Apply alternating lateral pressure up and down neck for 30 seconds to 2 minutes or until release is felt
Recheck Hyoid at level of C3 Sternum Ribs
Define Chapman Reflex
A system of reflex points that present as predictable anterior and posterior fascial tissue texture abnormalities (plaque-like changes or stringiness of the involved tissues) assumed to be reflections of visceral dysfunction or pathology.
Originally used by Frank Chapman, DO, and described by Charles Owens, DO
Facts about Chapman’s reflex points
Viscerosomatic reflexes used in the diagnosis and treatment of visceral pathology.
Predictable and consistent findings (T.A.R.T.) on structural exam.
Manifest as “gangliform” contractions or excessive tissue congestion
Described as pea sized areas that are boggy, ropy, shotty and/or thickened
Define spinal facilitation.
1. The maintenance of a pool of neurons (e.g., premotor neurons, motor neurons or preganglionic sympathetic neurons in one or more segments of the spinal cord) in a state of partial or subthreshold excitation; in this state, less afferent stimulation is required to trigger the discharge of impulses.
2. A theory regarding the neurophysiological mechanisms underlying the neuronal activity associated with somatic dysfunction.
3. Facilitation may be due to sustained increase in afferent input, aberrant patterns of afferent input, or changes within the affected neurons themselves or their chemical environment. Once established, facilitation can be sustained by normal central nervous system (CNS) activity
What is the mechanism for chapman’s reflex points?
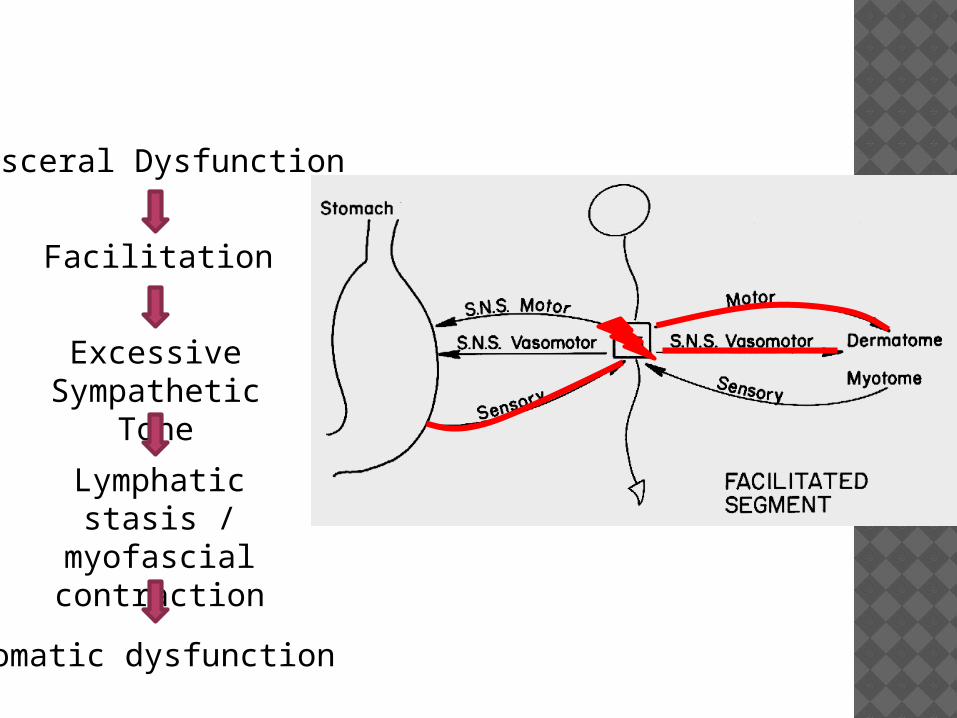
Visceral Dysfunction
Excessive Sympathetic
ToneLymphatic stasis /
myofascial contraction
Somatic dysfunction
Facilitation
Treatment for Chapman’s points?
Treatment: using the finger pad, hold firm but gentle rotary motion for 15 seconds to 2 minutes
Anterior and Posterior points may be treated simultaneously
Chapman’s Reflex points for myocardium?
• Myocardium• Anterior: 2nd intercostal space, bilateral,
parasternal• Posterior: Between spinous process and
transverse process of T2
Chapman’s reflex points for adrenals?
Anterior: 1 inch lateral and 2.5 inches superior from umbilicusKindney: 1 inch lateral and superior from
umbilicusBladder: Periumbilical
Posterior: Between spinous process of T11 and transverse process of T12
LYMPHATICS
Functions of the lymphatic system?
• Filtering of particulate matter prior to venous return
• Development and delivery of components to combat foreign substances
Where is lymph produced? What is it’s function?
• Produced from GI tract and Liver: Fat, proteins, amino acids, clotting factors, etc.
• Produced from peripheral tissues: Filtrate of excess fluid from arterioles and other lymph vessels
• Functions as transport medium of the immune system
Where does the right lymphatic duct drain? What does it drain?
• Drains into R subclavian vein• Drains RUE, R hemicranium, R neck,
heart, lungs and liver
Where does the left lymphatic duct drain? What does it drain?
• Drains everything else into L subclavian vein
• Thoracic duct
Describe flow of lymphatics?
Which muscle is the primary engine and controls the pressure gradient for lymphatics?
Diaphragm• Inhalation• Increased intra-abdominal pressure,
decreased intra-thoracic pressure• Exhlation • Decreased intra-abdominal pressure
Flow into and out of the lymphatic system affected by which four major pressures?
1. Capillary pressure2. Interstitial fluid pressure3. Plasma colloid osmotic pressure4. Interstitial fluid colloid osmotic pressure
What can cause dysfunction in the lymphatic system?
Diaphragms / Skeletal muscle Impaired functionMyofascial restriction
Thoracic cageRestriction of motion
Autonomic toneVasoconstriction
CardiovascularHeart failure, volume overload
What do you want to achieve through OMT on the lymphatic system?
Remove restrictions to flowReduce Sympathetic toneT-inlet releaseRe-dome diaphragmRemove other restricitons
Encourage normal flowLymphatic pumps
Before doing any lymphatic techniques what is the first thing you must do? Why?
Thoracic inlet in order to clear thoracic duct
Technique for thoracic pump (with assist)?
• Patient Supine with head turned to side, physician at head of the table
• Check for gum!• Place thenar eminences inferior to patient
clavicles with fingers over rib cage.• Patient inhales and exhales deeply• Physician exerts pressure during exhalation• May resist inhalation for 3 breaths and release
during 4th breath• Be aware of contraindications!COPD and asthma
Technique for pectoral traction?
• Patient Supine, physician at head of the table• Place finger pads into axillary fold• Lean back slowly, causing hands to move
cephalad into patient’s axilla until barrier is reached
• Patient inhales, physician pulls cephalad and anterior
• Patient exhales while physician resists motion• Repeat for 5 – 7 respirations• Variation: place hands underneath axilla• Contraindications: Subclavian line,
mastectomy, other contraindications to lymphatic treatment
Technique for ischiorectal fossa release?
• Patient Supine with hips and knees flexed• Physician at side of table opposite side of
dysfunction• Place thumb medial to ischial tuberosity of
dysfunctional side• Gentle cephalad pressure until resistance
felt then apply lateral force• May apply respiratory assist• Hold until tissues release
Technique for popliteal fossa release?
• Patient Supine with legs extended• Physician faces head of table, sits at side to
be treated.• Grasp both medial and lateral aspects of
popliteal fossa and palpate fascial restrictions.
• Engage tissue with anterior force while engaging any fascial barriers
• Can be direct or indirect• Hold force until tissue release.
PULMONOLOGY
What are the true ribs and where do they attach?
1-7 Attach directly to sternum via
costochrondral cartilage
What are the false ribs and where do they attach?
7-10 Attach to sternum via costochondral
cartilage of rib 7
What are the typical ribs and what does each contain structurally?
3-10 All contain a head, neck, shaft, tubercle,
and angle
What are the atypical ribs?
1,2,11,12 2 or less articulations
Where does Rib 1 articulate?
Articulation with T1 only; no angle
Where do Ribs 11 and 12 articulate?
Articulation with corresponding vertebrae
No tubercle
What are the pump handle ribs? What plane and axis do they move in?
1-5 Sagittal plane, horizontal axis
What are the bucket handle ribs? What plane and axis do they move in?
6-10 Coronal plane, A-P axis
What are the caliper ribs? What plane and axis do they move in?
11, 12 Transverse plane, vertical axis
What is an inhalation dysfunction and which rib do you treat?
Inhalation dysfunction = elevated rib Exhalation restriction Rib is stuck up and wont go down Key rib = bottom
What is an exhalation dysfunction and which rib do you treat?
Exhalation dysfunction = depressed Inhalation restriction Rib is stuck down and wont come up Key rib = top
What are the major muscles of inspiration?
Diaphragm, external intercostals
What are the accessory muscles of inspiration?
SCM, scalenes
What are the major muscles of exhalation?
Internal intercostal, rectus abdominus, internal and external obliques, transverse abdominus
What are the ribs and related muscles for expiration treatment?
Rib 1 – Anterior and medial scalene Rib 2 – Posterior Scalene Ribs 3 -5 – pectoralis minor Ribs 6-9 – serratus anterior Ribs 10-11 – latissimus dorsi Rib 12 – quadratus lumborum
What is the innervation of the diaphragm?
C3-C5 (phrenic)
What is the sympathetic thorax innervation (levels)?
T1-T6
What is the function of sympathetic innervation in the thorax?
Bronchodilator Vasoconstriction Increases ratio of Goblet cells to ciliated
Cells (thickens secretions)
Stimulation of the sympathetics helps with what disease state?
COPD and asthma
What are the Chapman’s reflex points for the bronchi?
Anterior: 2nd ICS, parasternally Posterior: b/t SP and TP of T2
What are the Chapman’s reflex points for the upper lung?
Anterior: 3rd ICS, parasternally Posterior: b/t SP and tips of TP of T3 and
T4
What are the Chapman’s reflex points for the lower lung?
Anterior: 4th ICS, parasternally Posterior: b/t SP and tips of TP of T4 and
T5
What is the parasympathetic thorax innervation (nerve)?
vagus
What is the function of parasympathetic innervation in the thorax?
Bronchoconstriction, decrease number of goblet cells to thin secretions, vasodilation
Stimulation of the parasympathetics helps with what disease state?
pneumonia
What is the Hering-Breuer reflex?
Hard to differentiate if the alveoli are filled with air or fluid
Causes limited respiratory excursion Reflex to prevent overinflation of the
lungs
Where do the lungs drain?
R lymphatic duct R subclavian vein
What happens when there is a diaphragm dysfunction?
Due to a rib or thoracic dysfunction Diaphragm is flattened and abnormal Lymphatics build up Increases tissue congestion Decreases CO
What kind of dysfunction does coughing lead to?
Exhalation dysfunction Causes rapid contraction of the
intercostals
What are the 3 phases of looking for rib dysfunctions?
1) observationScreen for dysfx
2) scanning Group dx
3) segmentalCheck individual ribs
What levels are associated with the following key landmarks?Sternal notchAngle of louisSpine of scapula Inferior angle of scapula/sternal xiphoid
junction
Sternal notch: T2 Angle of louis: T4, rib 2 Spine of scapula: rib 3 Inferior angle of scapula/sternal xiphoid
junction: rib 7
Where do you palpate the 2nd rib?
Costochondral articulation at the angle of louis
How do you assess ribs 11 and 12?
Patient is PRONE, 2nd finger over 11th rib, 3rd finger over 12th
What are the anterior tender points for Ribs 1, 2, and 3-7
1: sternoclavicular joint 2: midclavicular line 3-7: anterior axillary line
How do you treat an anterior rib 1 or 2?Usually depressed rib
Jones counterstrain Monitor costosternal junction of rib 1 Flex neck, rotate and SB TOWARD TP
How do you treat an anterior rib 3-6?Usually depressed rib
Jones counterstrain OPPOSITE arm goes on doc’s leg Translate away with the body Rotate and SB TOWARDS Patients legs are up on table
How do you treat a posterior rib 2-6?Usually an elevated rib
Jones counterstrain TPs on rib angles SAME arm on doc’s leg Flex pt forward, translate towards Rotate AWAY
What is muscle energy tx for elevated rib 1?
OPPOSITE arm on doc’s leg Place MCP on upper surface of dysfx SB head TOWARD Rotate head AWAY Exert caudad force and forward pressure
in exhalation Resist inhalation
What is muscle energy tx for an inhaled rib 1?
Pt supine Flex cervical spine Thumb on superior surface, b/t SCM Pt inhales while doc resists mvmt
What is muscle energy treatment for inhaled pump handle ribs?
Elevate head and shoulders Bend upper body forward to take
tension off rib Place thenar eminence anterior to
elevated rib Resist inhalation, exaggerate motion in
exhalation
What is muscle energy treatment for inhaled bucket handle ribs?
Side bend patients upper body to take tension off of rib
Place hand on lateral aspect of IC space Resist inhalation Exaggerate exhalation
What is muscle energy treatment for inhaled caliper ribs?
Patient PRONE Place heel of hand posterior and medial
to rib angle Exert a lateral and caudad pressure Grasp ipsilateral ASIS and pull up Have pt pull hip down to table
How do you treat exhalation dysfunctions with ME in ribs 1, 2, 3-5, 5-9, 10-12?
1: hand on forehead, head is 5-10* away Pt pulls head up while doc resists mvmt of
forehead 2: hand on forehead, head is 30* away
Pt pulls head up while doc resists mvmt of forehead
3-5: elbow bent near ear and lifted off table
5-9: arm flexed beside ear; pt lifts elbow towards opposite ASIS
10-12: arm abducted by ear; pt tries to adduct arm
How do you dome the diaphragm in a supine patient?
Indirect technique Thumbs inferior to costal margins Find freedom of motion
Use this position for treatment Resist during inhalation Follow during exhalation
How do you dome the diaphragm in a seated patient?
Physician is behind pt Pt slouches backward Assess ease of motion through rotation
or translation Resist inhalation Follow exhalation away from the barrier
How do you balance a single rib in a seated patient?
Move rib away from restrictive barrier into a direction of freer motion
Find proper position for release and hold Ex: exhaled 5th rib L
Contact entire L 5th rib with both hands (front and back); move rib into position of exhalation
Hold and wait for release
How do you balance multiple ribs in a seated patient?
Ex: exhaled group dysfx, ribs 5-7 LContact left 5th-7th ribs with both handsFocus on 5th ribMove group into position of exhalationHold and wait for release
CLIINCAL APPLICATIONS
What does TART stand for?
Tissue texture abnormalitiesAcute vs. chronic
Asymmetry of positionRestriction of motion (determines
diagnosis)Tenderness
What is the function of a muscle spindle?
Muscle length rate of change of length In parallel
What is the function of the golgi tendon?
Muscle tension Rate of change of muscle tension In series
What activates the nociceptors?
• Prolonged stretch, injury, pressure, thermal and chemical changes, and ischemia
Where are impulses of nociceptors transmitted to?
Higher CNS (appreciation of pain) Spinal interomediolateral system stimulate
preganglionic autonomic neurons Skeletal muscle motor neurons Pain maximal at this segment but poorly
localized
What is the effect of the nociceptors on the injured muscles?
• Sympathetic effect in segmentally targeted organ
• Injured muscle shortens • Overlying muscles contract to guard the
underlying area• Any attempt to stretch the affected muscles
to normal resting length will restress the nociceptors
How does OMM act on the nociceptors to correct dysfunction?
OMM involves neuromuscular techniques to restore normal resting length of muscle and “tricks” to keep the nociceptor from re-activating
What are some of the local neuromuscular consequences of somatic dysfunction?
• Pain nociceptors local inflammatory response initiates cycle
• Autonomic arousal Sympathetic activation
• Muscle spindle over activity motor neuron excitability facilitation increased response to any stimuli
• Reciprocal Inhibition decreased tone (antagonist muscle)
• Restricted motion• Altered proprioception
More specifically, how does somatic dysfunction alter proprioception?Exame of an ankle sprain
Inappropriate CNS interpretation of position Inappropriate body positioning, firing sequence,
load distribution Results in overuse of wrong muscles for the job Increase risk of further injury Eg. ankle sprains altered
proprioception decreased firing of ipsilateral glut max decreased pelvic control with gait and activity increased incidence of low back pain
What are some local consequences of chronic somatic dysfunction?Specifically vascular and lymphatic effects
Vascular constriction hypoxia relative ischemia fibrosis/tissue atrophy cool, ropy/stringy, dry, and minimally tender
Lymphatic constriction tissue congestion relative ischemia and decreased ability to remove by-products of metabolism altered cellular function disease/pathology
What are the systemic consequences of somatic dysfunction? Ie, somatovisceral, viscerosomatic, viscero-
viscero, somato-somatic
Systemic (via interneurons) Somato-visceral
Increased sympathetic tone to corresponding organ
Prolonged sympathetic drive to a visceral organ alters function (toward dysfunction)
Viscero-somatic Increased sympathetic response in
segmentally related muscle/tissue from sympathetically stimulated organ (from noxious stimuli)
Somato-somaticReferred from other somatic region
Viscero-Viscero
Describe neuromuscular compensation in terms of systemic consequences of chronic somatic dysfunction
Neuromuscular compensation from muscles with overlapping function overuse continued compensation adaptive shortening connective tissue reorganized in shortened form postural decompensation and altered proprioception
Name some predisposing and perpetuating factors of somatic dysfunction
Trauma (current or compensations from previous)
Postural stress Habitual/occupational
Gravity Anomalies
Asymmetric facets, leg length discrepancy Transitional areas (OA, C7-T1, T12-L1, L5-S1) Muscle hyperirritability
Muscle imbalance, Stress, Infection, Poor nutrition, Somato-somato or Viscero-somato reflex (organ disease), Cold temp
Repetitive motions overuse Inappropriate training Ligament laxity
How does muscular imbalance lead to somatic dysfunction?
Muscles must have: symmetry of resting length and
resistance to passive stretchsymmetry in concentric and eccentric
contractionssymmetry in muscle firing sequence
If NOT, then muscles are not balanced! (imagine guitar strings..imbalance = out of
tune)
What are some patterns of muscle imbalance?
• Shortening and tightening of muscle groups (usually tonic muscles)
• Usually asymmetric• Weakness of certain muscle groups (usually phasic
muscles) • Usually asymmetric (left vs. right; anterior vs. posterior,
etc.)• Altered afferent input Altered proprioception
Loss of control of integrated function Antagonist/Agonist balance altered Arthrokinetic control altered Reprogramming of setpoint or resting point of joint
control Memory at cord level and/or higher CNS
Reprogramming of movement patterns CNS mediation through lateral reticular system
alters activity of gamma motor neurons altered time activation sequences of muscle action
Prime joint mover inhibition with secondary mover compensation
Relative joint instability/hypermobility
How can you test for muscle imbalance?
LengthTest with passive stretchCompare both sides
Concentric/Eccentric contractionTest by palpating tone and/or resistanceCompare both sides
Firing sequenceFor a given action palpate for sequence
of muscle contractioneg. shoulder abduction deltoid
supraspinatousmid and lower trapcontralateral quadratus lumborum
Describe the VINNDICATES mnemonic for differential diagnoses.
Vascular subclavian artery thrombus or stenosis, venous clot or superior vena
cava syndrome, raynaud’s, or acute coronary syndrome Inflammatory
post-radiation or surgery Neoplastic
breast, lung –pancoast tumor, and head and neck cancers Neurologic peripheral neuropathy, cervical radiculopathy, peripheral nerve
compression such as cubital or carpal tunnel syndrome, brachial neuritis, or reflex sympathetic dystrophy
Drugs Idiopathic Congenital
Anatomic variations Autoimmune
multiple sclerosis, thyroid disease, etc. Traumatic
such as clavicle fracture Endocrine/Metabolic Skeletal/Musculoskeletal
shoulder pathology, somatic dysfunctions, trigger points, postural abnormalities, muscle imbalances
What is Thoracic Outlet Syndrome (TOS)?
Mechanical compression of neural or vascular structures traversing the lower neck into the armAssociated with signs/symptoms of
ischemia or neuropathy
What are the neurological symptoms of TOS?
Parasthesia (C8, T1 dermatome) Muscle weakness and atrophy Difficulty with fine motor tasks Pain in the arm and hand Tingling and numbness in the neck,
shoulder region, arm, hand, and sometimes face
What are the vascular symptoms of TOS?
Less common Bluish discoloration of the hand Feeling of heaviness in the arm or hand Easily fatigued arms and hands Superficial vein distention in the hand
Who are common patients with TOS?
Females > Males 2nd to 8th decade (peaks in 4th) Occupations involving repetitive work
or overhead activities
How do you diagnose TOS? (What are some tests/imaging)
Electrodiagnostic/radiological studies may be normal
No single test is considered diagnostic True neurogenic TOS
Rare (diagnosed by EMG/NCV) True Vascular TOS
Rare (diagnosed by doppler, MRA, angiography) Disputed neurologic TOS
most common (diagnosed by history and physical exam; normal studies)
Magnetic Resonance Angiography- abrupt termination of flow signal in the bilateral subclavian arteries with arm abduction
Describe the anatomy of the three common entrapment spaces for TOS.
Thoracic inlet Three common entrapment sites
Scalene triangle ant/mid scalene, 1st rib Brachial plexus, subclavian artery
Costoclavicular space 1st rib, clavicle, mid scalene post.,
costoclavicular ligament anteriorly Brachial plexus, subclavian artery and vein
Subcoracoid space Overlying ribs under pec minor attachment at
coracoid process
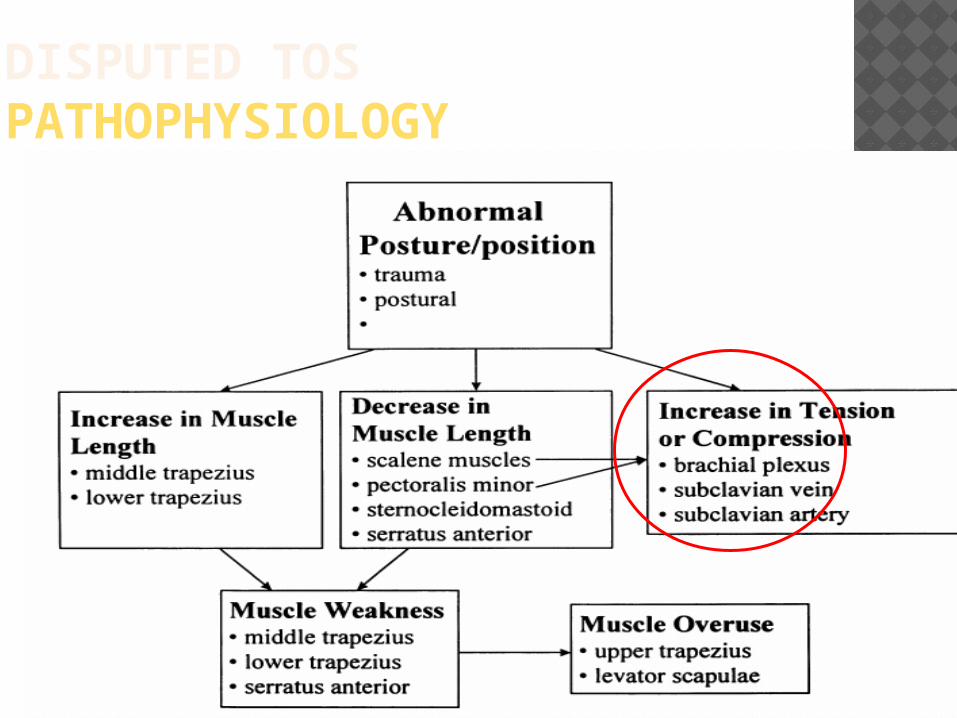
DISPUTED TOSPATHOPHYSIOLOGY
Describe Trigger Points. Are these the same as Jones’ Tenderpoints?
Discrete, focal, hyperirritable spots located in a taut band of skeletal muscle
A type of somatic dysfunction (NOT JONE’S TENDERPOINTS) May not respond to OMT May require lidocaine or saline injection, dry needling, or
spray and stretch technique Muscle range of motion may be limited Muscle may be weak and inhibited
Etiology uncertain, some overlap with other tenderpoints such as Jones Counterstrain, Accupuncture and Chapman Points
Not related to visceral or target organ involvement A point on the body which “Triggers” or refers pain
in a predictable distribution Classified as “Active”,(painful at rest), or “Latent”,
(painful only when palpated)
What are some Trigger Point treatments?
Deep and vigorous massage of each point
Stretch and Spray, (Ethyl Chloride), decrease in temp blocks conduction velocity of C and A Delta reducing afferent input and reducing pain and spasm
Injection with local anesthetics / steroids Stretching and reconditioning muscle
groups
What are some of the reasons for TOS pathophysiology? (next 2 slides)
Progressive postural distortion Adaptive shortening
scalenes, pec minor, SCM, serratus anterior Hypertonicity – increased tone and resistance to passive stretch
Progressive scapular protraction Weakness (mid/lower trap, rhomboid) secondary to
Painful inhibition trigger points, somatic dysfunctions
Stretched resting position Disuse
Scapulothoracic dyskinesis and abnormal scapulohumeral rhythm Compensations:
Overuse of: levator scapulae, upper trap hypertonicity, trigger points Myofascial restrictions
Subscapula, posterior shoulder capsule, scalenes, pec minor
Other contributing/perpetuating factors Anatomic variations Leg length discrepancy Scoliosis (true or functional) Somatic dysfunctions
Mechanical Decreased motion of 1st rib, clavicle, etc.
Neuromuscular Inhibition - type II lower thoracic lower trap Facilitation – type II C3 levator scapulae
Chronic nerve compression perineurium and epineurium - histopathologic
changes ischemia focal demyelination diffuse demyelination axonal injury with Wallerian degeneration
How do you diagnose TOS?
Clinical Tests Provocative Maneuvers
Attempting to induce entrapment Monitor pulse and reproduction of symptoms False positive results
when tested on healthy patients Lower false positive rates when:
positive response was defined as pain for 2 or more maneuvers or
any symptom with 3 or greater maneuvers Adson’s test Costoclavicular/Halstead’s maneuver East’s/Roo’s test Wright’s maneuver
What is Adson’s test?
Neck extended turned toward affected side
Take deep breath and hold Positive is decr or absent pulse Narrows the interscalene space Modified version - turn head to opposite
side For cervical rib
What is the Costoclavicular/Halstead’s maneuver?
Exaggerated military posturescapula retracted and depressed chest protruding Narrows the costoclavicular space Extend and Rotate head awayApply downward traction on arm
What is East/Roo’s test?
Shoulders externally rotated and abducted to 90°; elbows flexed to 90 °
open and close hands repeatedly for up to three minutes
Check for pain, heaviness or weakness
What is Wright’s maneuver?
Tale pulse, note when it diminishes shoulder external rotation abduction beyond 90° Compression below the pectoralis minor
insertion
What is the surgical treatment for TOS?
In disputed neurologic TOS Surgical intervention no benefit over
conservatively treated patients
Surgical intervention reserved for: chronic intractable pain neurologic deficit with evidence of muscular atrophy persistent vascular insufficiency impending vascular catastrophe
Surgery Scalenotomy Scalenectomy Claviculectomy Cervcal rib excision First rib resection
What is the nonsurgical treatment for TOS?
Comprehensive rehabilitation strategy restore normal structure and function
Postural education Ergonomic factors Optimize joint motion
Treat somatic dysfunctions Cervical and thoracic spine SC joint AC joint GH joint Ribcage (esp. 1st rib)
Treat other musculoskeletal contributors Muscle imbalance**
Stretch to symmetry then strengthen to symmetry Myofascial restrictions Lumbar, pelvic, sacral, and lower extremity somatic
dysfunctions Ligament/Tendon laxity (eg. with prolotherapy) Poor core strength and dynamic lumbopelvic stabilization
(unconscious co-contraction of transversus and multifidus) Leg length inequalities Scoliosis Gait abnormalities
What are some common trigger points?
Common trigger points Levator scapulaeUpper TrapAnterior ScaleneSCMLatissmusSupraspinatous InfraspinatousPec minor/majorErecetor spinaeSuboccipital muscles
CLINICAL APPLICATIONS
LAB TECHNIQUES

LEFT 1ST RIB HVLA ELEVATED COMPONENT
Rt hand on temporal area. Left 2nd MCP sup and post to 1st rib. Head slightly flexed, sidebent TOWARD and rotated AWAY. Pt inhales and on exhalation, left hand thrusts downward and sl medial toward contralateral nipple.
1ST RIB HVLA ROTATIONAL COMPONENT Place Right hand post and superior to T1 Hold hand firmly and insert under transverse
process until Rt. MCP joint meets resistance. Sidebend head Rt into palm of Rt hand Have pt inhale and during exhalation…. Rt hand thrusts in a rotational vector toward
Left shoulder. Rotational force is appropriate when Rt
shoulder is raised off table during thrust
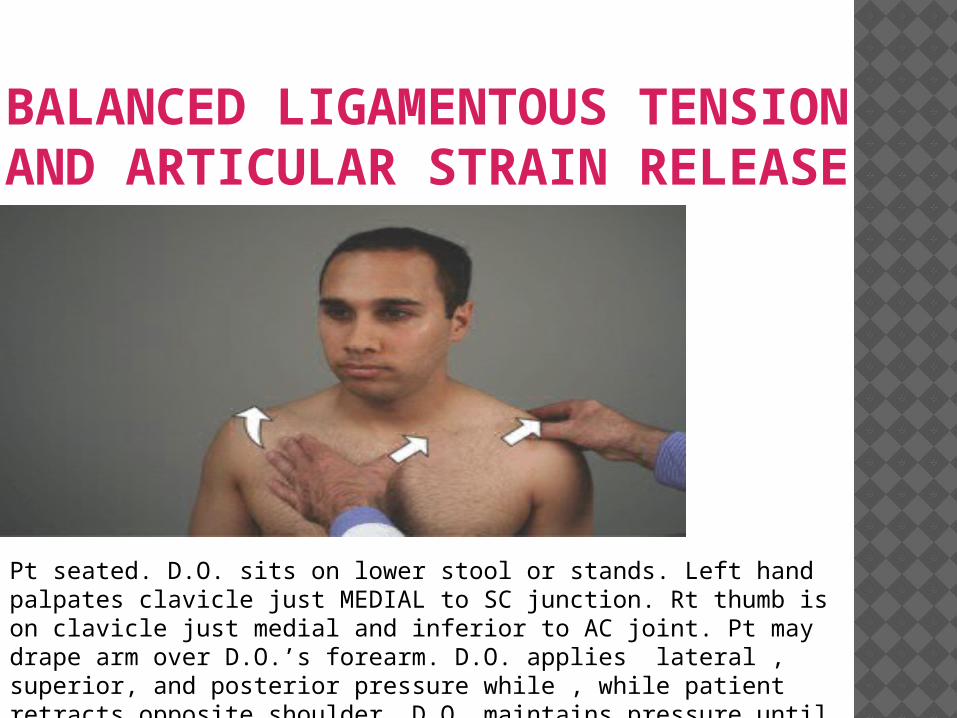
BALANCED LIGAMENTOUS TENSION AND ARTICULAR STRAIN RELEASE
Pt seated. D.O. sits on lower stool or stands. Left hand palpates clavicle just MEDIAL to SC junction. Rt thumb is on clavicle just medial and inferior to AC joint. Pt may drape arm over D.O.’s forearm. D.O. applies lateral , superior, and posterior pressure while , while patient retracts opposite shoulder. D.O. maintains pressure until release is noted. Reassess TART.
MUSCLES THAT NEED TO BE STRETCHED IN TOS Scalenes Pectoralis Minor Sternocleidomastoid Serratus
STERNOCLEIDOMASTOID AND UPPER TRAPEZIUS STRETCH Pt seated Opposite outstretched hand is placed on
head, same side as tight muscle Head is flexed, rotated and sidebent AWAY
until stretch is felt. Hand does NOT pull Pt leans,( sidebends) until stretch is felt Add chin tuck to increase stretch Hold 10-15 sec, repeat 3-5 times
PECTORALIS MINOR STRETCH Pt standing in doorway or facing wall Both hands on wall outstretched at shoulder
height Rotate body away from tight Pec until stretch
is felt Using other hand to stabilize body, lean INTO
wall increasing stretch, keeping spine neutral Hold 10-15 sec, repeat 3-5 times
SCALENE STRETCH Pt seated Opposite hand placed on clavicle Head is side bent and rotated AWAY from
tight scalene, and flexed until chin tucked and stretch is felt
Hold 10-15 sec, repeat 3-5 times
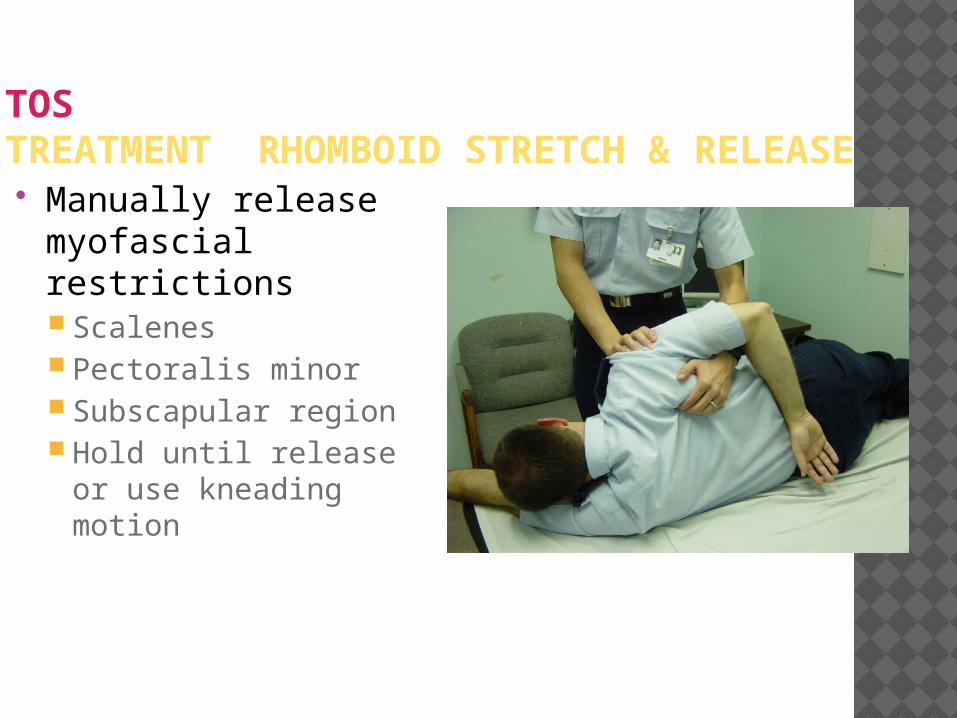
TOSTREATMENT RHOMBOID STRETCH & RELEASE Manually release
myofascial restrictions Scalenes Pectoralis minor Subscapular region Hold until release
or use kneading motion
RHOMBOID AND LOWER TRAPEZIUS STRENGTHENING Pt seated feet flat on floor Pt grasps hands in front of sternum with arms
parallel with floor Pt attempts to pull elbows backwards,
(isometric), Hold 5-7 sec, repeat 5-7 times Raise grasped hands OVER head, pull elbows
to floor,( not touching head), 5-7 sec, repeat 5-7 times
MID AND LOWER TRAPEZIUS STRENGTHING Pt prone, arms flexed and above head Operator palpates lower trapezius Then asks patient to lift hand off of table,
noting when lower trap is activated If possible, then ask patient to lift elbow off of
table, activating lower trap. Hold 5-7 sec, repeat 5-7 times
SERRATUS STRENGTHENING Pt standing Hands against wall shoulder height, spine
neutral Pt touches nose to wall, pulling scapula
midline, hold 5-7 sec. Pt then performs standing push up, with chin
flexed and elbows together to resist scapular elevation.
Can be performed PRONE later
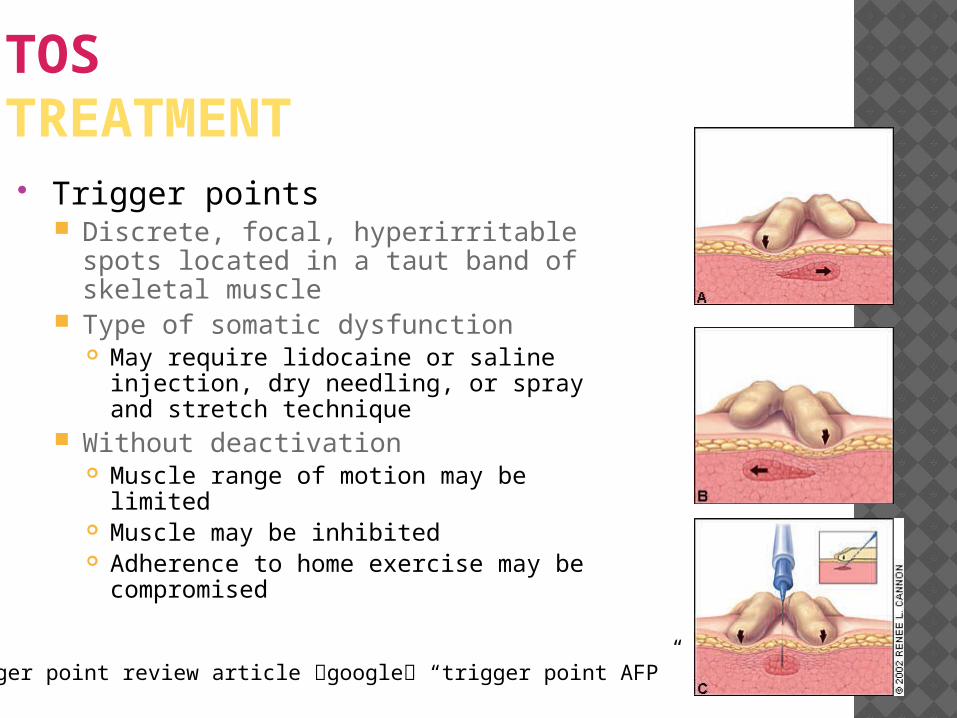
TOSTREATMENT Trigger points
Discrete, focal, hyperirritable spots located in a taut band of skeletal muscle
Type of somatic dysfunction May require lidocaine or saline injection,
dry needling, or spray and stretch technique
Without deactivation Muscle range of motion may be limited Muscle may be inhibited Adherence to home exercise may be
compromised
Trigger point review article google “trigger point AFP”
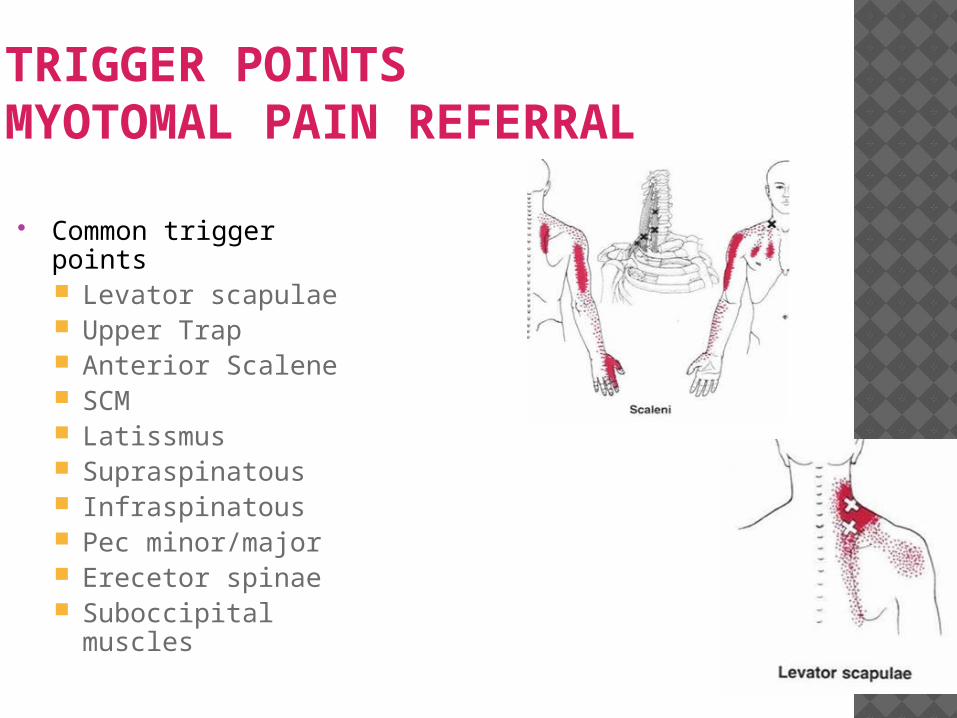
TRIGGER POINTSMYOTOMAL PAIN REFERRAL
Common trigger points Levator scapulae Upper Trap Anterior Scalene SCM Latissmus Supraspinatous Infraspinatous Pec minor/major Erecetor spinae Suboccipital muscles