Embed Size (px)
Citation preview

TERTIARY HYPERPARATHYROIDISM SONIKA PURI

PERSISTENT HYPERPARATHYROIDISM POST RENAL TRANSPLANT • Serum PTH levels decrease 3-6months post RT • One year post transplant resolution of hyperparathyroidism is seen ~50%
patients • Duration of dialysis, parathyroid gland size and development of nodular/
monoclonal hyperplasia are important determinants of persistent hyperparathyroidism ; role of low vitamin D 25oh levels.
• Most studies define PTHPT as serum pth level > ULN ; >2-2.5timew uln; or
>ULN as defined by KDQI guidelines
Torres et al, JASN 2002, Torres et al, NDT 1998

• Long half life of parathyroid cells –cell renewal rate of 5% per year
• protocol biopsies ; 6 weeks/ 3mths and 6mths post tx • 56/213 pts had luminal/ TI calcification • Pre tx variables (graft quality/donor-recip concordance/discordance
similar); similar renal function at time of first biopsy ;>80% DDK • Higher ATG use in pts w/ calcification; • Concurrent findings like rejection/ chronic changes/ CIN toxicity similar • Similar vitamin D replacement; higher phos replacement in pts
w/calcifications

Gwinner et al, AJT 2005

TERTIARY HYPERPARATHRYOIDISM AND BONE DISEASE POST TRANSPLANT
Akaberi et al, Transplantation 2006

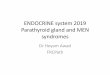
Prevalence of persistent hyperparathyroidism (HPT) up to 4 years after successful renal transplantation.
Evenepoel P et al. Nephrol. Dial. Transplant. 2004;19:1281-1287
Nephrol Dial Transplant Vol. 19 No. 5 © ERA-EDTA 2004; all rights reserved

Prevalence of persistent hyperparathyroidism (HPT) up to 4 years after successful renal transplantation in patients with moderate to severe HPT at the time of transplantation.
Evenepoel P et al. Nephrol. Dial. Transplant. 2004;19:1281-1287
Nephrol Dial Transplant Vol. 19 No. 5 © ERA-EDTA 2004; all rights reserved

Evenepoel et al, NDT 2004

Torres et al, NDT 1998

Persistent hyperparathyroidism after transplant Messa et al, KI 1998



Post Transplant Hypercalcemia • Attributed to high PTH levels 1) Decreased skeletal resistance towards action of PTH 2) Increased production of calcitriol, increased intestinal ca absorption 3) Resolution of hyperphosphatemia
-Incidence 8%-60% in first few months after transplant. -Post transplant hypercalcemia usually resolves after first year of
transplantation, 5-10% cases it can be seen upto 4 yrs post transplant -<5% - vascular calcification/ soft tissue calcification, nephrocalcinosis

Evenepoel et al, Cjasn 2009
-Single centre prospective observational study European study; 201 pts ;2004-2006; 3months post tx -egfr 51 +/- 16 ml/min, stage 3 ckd 70% -42% patients had pth above target -Calcidiol levels >30 ng/ml -27% pts 3mths post tx -Hypercalcemia (Ca-c) 14% pts at 3mths a/w high pth levels/ low phos levels -high FeCa; high FePhos -no significant differnce in Calcidiol l l

Nakai et al

Hypophosphatemia; Role of FGF-23 • Common s/p renal transplant • Attributed to urinary phosphate wasting • Persistent Hyperparathyroidism; however also seen in pts with normal pth
levels, a/w inappropriately low calcitriol levels despite normal allograft function
• Prospective longitudinal study -27 pts (15-m/12-w), Caucasian; 66% first transplants, LR= LUR
• 85% had s.phos <2.5mg/dl, 37% -s.phos <1.5mg/dl
• Multivariate analysis- FGF-23 levels were independently a/w serum phos, urinary phos excretion and calcitriol levels (p <0.01)

Bhan et al, KI 2006

CINACALCET • Calcimimetics are allosteric binders
of CaSR activated
• CaSR in PTH tonically inhibits pth secretion and parathyroid cell proliferation
- Proximal tubular cells – regulates pth medicated phosphate excretion and 1 –alpha hydroxylase activity
- TAL – regulates passive calcium reabosorption via paracellular pathway
(Riccardi, AJRP 2009)
Borchhardt et al, Transplantation2008


PARATHYROIDECTOMY • PTX reported in 0.65-5.6% post renal transplant • No firm guidelines regarding when ptx should be performed post tx,
generally if pth levels remain elevated >1 yr post transplant; or persistent hypercalcemia (other factors excluded)
• Some studies report worsening renal function post ptx , some studies report decline in renal function by ~60% ; fup 6mths-6 yrs, ? Graft failure
• Worse outcomes reported with total parathyroidectomy vs partial with autotransplant.
• Risk of adynamic bone disease
Evenepoel , NDT 2007; Evenepoel , NDT 2004; Lewin et al NDT 2006

Comparison of graft survival between patients requiring parathyroidectomy (n = 90) and a matched cohort of renal allograft recipients (n = 180).
Evenepoel P et al. Nephrol. Dial. Transplant. 2007;22:1730-1737
© The Author [2007]. Published by Oxford University Press on behalf of ERA-EDTA. All rights reserved. For Permissions, please email: [email protected]