Embed Size (px)
Citation preview

1 The Chronicle April 2005
Apr i l 2005 Vo lume 8, Issue 5
This is a story about Timothy Buthimang, a man who has been quietly working for over 50 years in Galiwinku growing fresh fruit and vegetables for the community. Garngulkpuy, his daughter, shared this story with me, as she wants to c e l e b r a t e h e r f a t h e r ’ s achievements and have them recognised outside the community. Ideally, Garngulkpuy would like this story aired on the ABC Australian Story. I hope that happens one day, but in the meantime this short story is a means of celebrating her fathers achievements. Buthimang has been a life long gardener; he was 15 years old when he started working in the community garden at Galiwinku. Over the years he has developed an extensive knowledge of plants and how to care for them. He understands the soil, the weather and what it takes to make things grow in poor conditions. Buthimang believes gardening promotes health; that plants draw valuable nourishment from the soil to feed the community.
Buthimang loves watching and making things grow and his produce has been a valuable source of fresh fruit and vegetables to Galiwinku community for many years. Buthimang’s gardens have produced sweet potatoes, cassava, taro, pumpkin, watermelon, guava, lime, mango, sugar cane and bananas. Buthimang is well known for providing fruit and vegetables at community celebrations, from bananas to sweet potatoes, cassava, taro and pumpkin.
Continued page 2
Timothy Buthimang: a life long gardener and a living legend
THE CHRONICLE
Timothy Buthimang with 2005 Territory Heart Foundation
Kellogg Local Government Award
Women, Asthma Severity & BMI
2
NT Physical Activity Survey 2003
4
Cultural Security/Safety/Respect—what does it mean to you?
5
Nurturing Galiwinku Youth in Northeast Arnhem Land: Yalu Marrngikunharaw
7
Good Food Kitchen New healthy food take-away opens in Maningrida
10
Implementing Aboriginal Health Policy in Australia
11
Mental Problem Story 12-13
Heart Week 1-7 may 14
Childhood Obesity 15
Tackling overweight & obesity 16-17
Educating to improve popula-tion health outcomes in chronic disease
19
9th Annual Chronic Diseases Network Conference
20
INSIDE THIS ISSUE:
Buthimang believes
gardening promotes
health; that plants draw
valuable nourishment
from the soil to feed the
community.

2 The Chronicle April 2005
Women, Asthma Severity and BMI Michelle Menzies—CEO Asthma NT With the spotlight on the growing obesity problem among Australians, it is worthwhile noting a recent report about the association between body mass index (BMI), and asthma severity in women.
The Epidemiological Study on the Genetics and Environment of Asthma in France reviewed 366 adults aged 16 years or older with asthma1.
Results showed that asthma severity increased with BMI, which is the ratio of weight to height, among women but not among men.
Even after adjusting the data for age, smoking status and difficulty breathing due to obesity, the association between BMI and asthma severity in women remained significant.
For the women who experienced menarche at an earlier age, there was a stronger association with asthma severity. The researchers noted that earlier studies have reported a decreased incidence of asthma at menopause as well as variation in visits to emergency departments according to menstrual cycle.
The French study concluded “Findings support the hypothesis of hormonal factors involved in the severity of asthma.”
Last year a Norwegian study found that having a larger waist measurement (the "apple" shape) appears to be a greater risk for developing asthma than just having a high BMI in both males and females2.
References 1. Varraso R, Siroux V, Maccario J, Pin I, Kauffmann F. Asthma severity is associated with body mass index and early menarche in women. Am J Respir Crit Care Med. 2005 Feb 15;171(4):334-9. 2. Kronander UNUN, Falkenberg M, Zetterström O. Prevalence and incidence of asthma related to waist circumference and BMI in a Swedish community sample. Respir Med 2004;98:1109-1116
Continued page 1 These days he is busy helping others get fruit trees, vegetables and other garden flowers growing in their back yard. It was in the early 1970’s that Buthimang started working in the community garden at Galiwinku. In the early 1980’s the garden was producing over a tonne of bananas a week. Bananas were being exported to many nearby Arnhem Land communities. Weekly sales were over $1000. The days of the mission farming finished in 1985, but Buthimang has enjoyed keeping up his work, planting gardens at his outstations and his house and helping others set up their own backyard vegetable patch. He is an adviser to Burwu Ngatha Djama (Yalu Home Gardening project), which supports families with backyard gardening. Steve Djati Yunupingu and Timothy Galalingu manage this project that was initiated through Yalu Marnggithinyaraw (for more information on Yalu see article page 5). Most homelands are now growing their own fruit and vegetable gardens. People are starting to think about ways to grow bush food in their gardens, like munydjuti (green plum- high in vitamin C), Balkpalk (native peanut – high in protein) and ganguri (wild yam – high in fibre). Buthimang no longer drives around selling his produce as he can now take it directly to the store and take away shop. At 67 years of age Buthimang still gets up at 6am to work in his gardens and is busy establishing the Dingu garden and working on the Wanguri Family Food Project that aims to establish a fresh fruit juice business. Many things have come out of this one man’s good work and love of gardening. He has fostered an enthusiasm for gardening amongst the community; drawn nourishment from the land, been independent, and given many families access to a wide range of healthy fresh fruit and vegetables. As told by Garngulkpuy to Justine Glover,
March 2005
THE CHRONICLE
EDITOR & DESK TOP PUBLISHER: Justine Glover, Chronic Diseases & Injury Prevention Officer
DEPARTMENT OF HEALTH & COMMUNITY SERVICES PO BOX 40596
CASUARINA NT 0811 PHONE: (08) 89228280
FAX: (08) 89228310 E-MAIL: [email protected]
Contributions appearing in The Chronicle do not necessarily reflect the views of the editor or DHCS. Contributions are consistent with the aims of the Chronic Diseases Network and are intended to : • Inform and stimulate thought and action; • encourage discussion and comment; • promote communication, co-ordination and collaboration.

3 The Chronicle April 2005
Dear Editor Why do some people make bad lifestyle choices?
This letter responds to Dr Michael Lowe’s article of the same name, published The Chronicle Jan/Feb 2005.
Dr Lowe states that he is using virtue ethics to consider ethical questions of people’s behaviour. At both individual and societal levels, he describes the role of health professionals to discourage what he describes as health vices, such as smoking, and encourage health virtues, such as eating the right amount.
Virtue ethics is an ethical framework that emphasizes the agents who perform actions and make choices (Beauchamp and Childress 1994). In this ethical framework, we recognise ethical behaviour because it is what virtuous people do. A virtue is a disposition to act in keeping with moral principles or ideals. Examples of virtues include respectfulness, justice, truthfulness, forgiveness, generosity and compassion. People with these characteristics are virtuous, and therefore behaviour in keeping with these characteristics is ethical.
Dr Lowe has taken an ethical leap to describe health-promoting behaviour as inherently virtuous, and behaviour that does not promote health as a vice. This alarms me.
I believe that health behaviours such as smoking and overeating are morally neutral. They are neither good nor evil. They just are, and people just do them, without them contributing to virtue or vice.
The depiction of these behaviours as vices has no moral basis, only a health basis. However and worse, the depiction of these behaviours as vices could lead to the interpretation of illness as sin. Regarding illness as sin, or as the result of sinful behaviour is damaging to the relationship between the health-care worker and patient relationship, and the entire health care system.
Illness is not sin, nor is it the result of sin or vice. Health is not necessarily the result of moral behaviour. I do not believe we should use this framework in considering health behaviours.
Virtue ethics is a useful framework in making ethical decisions, particularly those we make as health care professionals. However health behaviour is not an ethical decision and an ethical framework should not contribute to managing others’ health behaviours.
Reference Beauchamp TL, Childress JF. Principles of biomedical ethics 4th edition.
Oxford University Press, New York 1994. Yours truly, Rosalie Schultz Public Health Medical Officer
Dear editor, The letter by Rosalie Schultz
suggests that we should not view unhealthy behaviour in the light of ethics – particularly virtue ethics. Many people would agree with her. For example, one of the key beliefs of Alcoholics Anonymous is that alcohol is an illness, not a moral failure. Yet groups like AA are also deeply concerned with morality, and I do not think they would disagree with the idea that while the disease has nothing to do with morality, many of the behaviours associated with the disease do.
The author says that someone who behaves in unhealthy ways should not be seen in any moral terms, but just as someone who behaves in unhealthy ways. How far should we take this? Should a person who sells cigarettes and alcohol also not be seen in any moral way – or just as someone who sells alcohol and cigarettes. Should a company who makes, distributes and promotes alcohol or cigarettes not be seen in any moral way, or just as another way of making money?
Ethics is all about behaviours! Over the centuries, health behaviours have been the topic of ethical debate just as other forms of behaviour have. Christian, Muslim, Jewish and Hindu ethics all speak about the need to maintain healthy behaviours.
Personally, I do not believe that we should point fingers at others and use arguments based upon virtue ethics against them (although it might be different for companies). Virtue ethics to me is most useful as a way of looking at my own behaviour. The argument in my article is that if we look within, we can see good and bad, and this can help us understand others.
As I think about chronic disease, I have become more and more convinced that ethical issues are central to how we deal with it. These issues have not been very clearly thought about in the literature, but I look forward to discussing and debating them further.
Michael Lowe Community Physician
Letters to the Editor

4 The Chronicle April 2005
Summary of key findings Introduction This survey was a first for the Northern Territory. It was undertaken by the Department of Health and Community Services (DHCS), in partnership with the National Heart Foundation (NT Division). Its primary aim was to measure levels of physical activity undertaken by residents of the Northern Territory aged between 18 and 54 years. The survey also ga t h e r e d i n f o r m a t i o n o n Territorians’ knowledge and attitude in relation to current recommendations for participation in physical activity.
Methods The survey was conducted through telephone interviews in July 2003. From an initial randomly selected eligible sample of 462 households, 349 interviews were completed, giving a response rate of 75.5%. Only 6% of respondents were of Aboriginal and/or Torres Strait Island origin. Records from these respondents were unlikely to be representative of all Indigenous people in the NT and were removed from the final analyses. Survey results therefore apply to 328 non-Indigenous Territorians only.
Levels of physical activity ‘Sufficient’ physical activity was defined as the accumulation of 150 minutes of moderate activity, over at least 5 sessions a week. People who participated in some activity, but either not enough in total or not regularly enough for health benefits were classified as ‘insufficiently’ active. People who reported doing no activity at all were classified as ‘sedentary’.
The key findings of this survey were that 55% of non-Indigenous Territorians aged 18-54 years reported engaging in sufficient
physical activity for health benefits; 35% reported insufficient levels of activity and 10% reported no activity and were classified as sedentary. Gender differences in participation and self-perception of physical activity levels were noticeable. Men were significantly more likely to be sedentary than women (14% compared with 5%). Three-quarters of the sedentary men described themselves as active, compared with 19% of women. Seventy-eight percent of the i nsu f f i c i en t l y ac t i ve m e n considered themselves active, compared with 58% of the women. Groups at greater risk of physical i n a c t i v i t y a l s o i n c l u d e d respondents in the 35-44 years age group, respondents with low levels of education, those with 3 children or more, respondents who were not in the workforce and those who were overweight or obese. Women were more likely to report walking 150 minutes or more per week than men (37% compared with 32%).
Knowledge Most respondents (90%) correctly agreed that 30 minutes of daily moderate physical act ivi ty conferred health benefits. Of concern was the lower level of agreement (75%) with the concept of accumulation of total daily physical activity in bouts of 10 minutes, and the high, and incorrect, level of agreement (69%) with the need to engage in vigorous physical activity for health benefits. Intention to become more active, self-efficacy and barriers to activity Respondents reporting insufficient activity levels were significantly more likely to intend to become more active (70%) than sedentary respondents (45%) or those who
were sufficiently active (49%). Those having received doctor’s advice on exercise were more likely to intend to become more active than those who had not (19% and 11% respectively). More than half of the respondents (57% of the sedentary and 53% of the insufficiently active) lacked confidence to find 30 minutes on 5 or more days of the week, as recommended by the National Physical Activity Guidelines for Australians.1 The main barriers to activity were lack of time (53%), followed by ‘I am active enough’ (21%) and ‘no motivation/can’t be bothered’ (16%).
Physical activity and body mass index (BMI) Overall, 5% of survey respondents were classified as underweight, 43% as of acceptable weight, 35% as overweight and 17% as obese. Physical activity levels were inversely re lated to BMI c a t e g o r i e s . S e d e n t a r y respondents were more likely to be overweight (51%) than respondents reporting insufficient activity (35%) or those reporting sufficient activity (33%). A quarter of the insufficiently active respondents were obese.
Miscellaneous A majority of respondents had access to a shower (68%) and a safe storage area for bicycles (57%) in their workplace. There was no difference in levels of participation in physical activity between respondents who owned a dog and those who did not.
For the full report and list of recommendations
http://www.nt.gov.au/health/publications.shtml
For further information contact
Annie Villeseche 8999 2623 [email protected]
Northern Territory Physical Activity Survey 2003 Non-Indigenous Population Department of Health and Community Services, Darwin, 2004. Villeseche A, Li SQ, Measey ML,

5 The Chronicle April 2005
Cultural Security/Safety/Respect what does it mean to you? There have been many references to the importance of effective cross cultural communication and cultural safety in the Chronicle over the years. Cultural Security/Safety is a very important issue when it comes to safe clinical service delivery. In the Dec 2004 Chronicle, Robyn Wiliams defined Cultural Safety as "an environment which is spiritually, socially and emotionally safe, as well as physically safe for people; where there is no assault, challenge or denial of their identity, of who they are and what they need. It is about shared respect, shared meaning, shared knowledge and experience, of learning together with dignity and truly listening". Cultural security will be emphasised in the forthcoming DHCS 5 year Aboriginal Health Action Plan. The focus will be on behaviours, rather than just attitudes and incorporating Aboriginal culture into the design and delivery of health services. The NT Council on Safety and Quality in Health Care also sees cultural safety as integral to clinical safety. We would like to hear your stories of how your clinical or professional practice in the NT has been affected by cultural safety issues. Do you have a story about how a lack of cultural safety made things go wrong or where having cultural skills and respect enhanced your abilities? Or of effective culturally safe teamwork? Please send your anecdotes to the Chronic Diseases Network by 8th July 2005 Email: [email protected] Fax: 08 8922 8310
Chronic Disease Workshop - Nhulunbuy Joy Pascall, from The Preventable Chronic Diseases Unit in Nhulunbuy has coordinated another highly successful Chronic Diseases workshop over the 14-18 February. There were 18 Participants from Yirrkala, Anugaru, Gove hospital Layna Homelands, Nhulunbuy high school and Women’s health. The program included a range of hands on and interactive sessions. Some of the highlights included bush tucker hunting at the beach with Boyan Yunipingu and a full day with Linda Rennie and Samara learning about diabetes. The group not only hunted for food but also got the opportunity to taste their catch. The program also included sessions on asthma, rheumatic heart disease, brief intervention, nutrition and renal disease.
Each night there was loads of team building with long walks on the beach and gas bagging over dinner at the local bistros. More fun was had when Nick from FACS took the group dragon boating. Congratulations Joy, sounds like you put together a great program that promoted, education, fun and team building. Keep an eye out for future workshops in your region. For further information call Cynthia Croft on 08 8922 8637.

6 The Chronicle April 2005
In December 2004, Galiwinku community hosted a Local Government Awards presentation ceremony for the Territory and National winning projects in the Heart Foundation Kellogg Local Government Awards. The Galiwinku community along with community members from Maparu in the Martharkal homeland put on a fantastic display of traditional dance to welcome the Heart Foundation members and celebrate the success of the local community projects. The event was celebrated in traditional style by the whole of community. Elders and community members alike arrived in full traditional clothing and presented two distinct ceremonial dances reflective of their community groups. The atmosphere was electric. A very proud Jackie Nguluwidi and his family accepted the plaque for winning the National Small Rural and Remote category for successfully opening and running their own food cooperative. The cooperative has had a huge impact on Maparu by, among many things, providing access to a regular, less expensive, healthier food supply. Timothy Buthimang and Timmy Ganalingu in Galiwinku were successful in winning the Territory
award for their exemplar family and community gardens in the category Project with Limited Resources. These men have led by example and had a great influence on other members of the community to work on their home gardens. Graham Opie Chief Executive of the Northern Territory Division of the National Heart Foundation was overwhelmed by the community involvement in the ceremony and the importance that it was given. Mr Opie says “These significant program wins have demonstrated that projects coming from the Northern Territory in remote communities are able to successfully compete on a local and national level. They provide an excellent example of best practice and have assisted in putting remote communities on the map.” Congratulations are offered to both Galiwinku and Maparu. The awards open for 2005 in May. If you have projects you would like to enter please go through your local council for an entry form, visit www.heartfoundation.com.au and look for the Local Government Awards or call the Heart Foundation on 89822703.
Local Government Awards Presentation
Galiwinku Lisa Fox, Heart Foundation NT
The Community Alcohol Action Network (CAAN) aims to reduce alcohol-related harm in the community by addressing the social and cultural forces that encour-age problem drinking. CAAN has been inspired by discussions with individuals from a range of fields who share a common concern about the prevalence of al-cohol misuse in our community. CAAN will raise public awareness of alcohol is-
sues and mobilise the community to take action against inappropriate alcohol use, advertising, promotion, products and supply.
To subscribe to Grog Watch E-Newsletter email [email protected]

7 The Chronicle April 2005
By Ian S McIntosh First published in Cultural Survival Quarterly Issue 26.2 May 31, 2002, reproduced with kind permission of Ian McIntosh
They call themselves yalu, an Aboriginal (Yolngu) word meaning "bird’s nest." But in this case yalu is a metaphor for the learning or nurturing place that six unemployed Yolngu women--Lawurrpa, Garngulkpuy, Bepuka, Yungirrnga, Djalingirr, and Wirriny Wirriny--have created at Galiwin’ku to help community youth grow and "teach them to fly." Representing the Warramiri, B i r r k i l i , W a n g u r r i , a n d Djambarrpiuyngu Mala (clans), they have united in the pursuit of one principle goal: to combat the steady decline in recognition by authorities of Yolngu health, education, and governance priorities, and a corresponding decline in the health and we l l be in g o f comm un i t y members. Self-confidence and interest in Yolngu culture are low, especially among youth.
"Yalu Marrngikunharaw" began when Lawurrpa was contracted by the Aboriginal Tropical Health Unit in Darwin to explore connections between health and education in the community. How could the current malaise affecting youth--substance abuse, drug addiction, teen suicide, television and video-induced apathy--best be a p p r o a c h e d ? O u t s i d e i n t e r v e n t i o n o r i n s i d e intervention? The abandonment of the new and a return to the old ways? Many ideas were generated as a consequence of the research and community consultations, and a holistic plan of action that emphasized cooperation and reconciliation
emerged. Yalu was born. "We Yolngu people are
Australians," says Garngulkpuy. "We know that Western (balanda) education is very important. But so too is Yolngu education--and Y o l n g u k n o w l e d g e a n d understandings in both health and education are not given the priority that they should be by [the] government." Adds Bepuka: "W e believe in two-way education: Aboriginal and non-Aboriginal. But we have been leaning too heavily just on the balanda side. We want to bring the life back to the Yolngu people so we can all live together as equals. There is no desire to do away with balanda education, but rather we want to lift up the Yolngu ways so that people are proud of who they are and where they come from.” And the work begins at home, says Lawurrpa: "To build a strong, healthy community we have to do more than just send our kids off to school. Parents have to teach them--to discipline them--and provide them with a healthy environment. In my father’s day we knew the Law, we understood the need for discipline, and we were healthy. We want the youth to come back to our way--the Yolngu way."
As a result of a successful fundraising campaign, the ladies of Yalu have been able to host a wide range of activities both in t h e G a l i w i n ’ k u s c h o o l (Shepherdson College) and community, as well as in remote outstations. One of the most successful recent undertakings involved the escorting of 10 petrol-sniffing youngsters to the Unbirri island outstation for a two-week retreat where they were s h o w n v a r i o u s h u n t i n g techniques, heard stories from elders about the need for raypirri,
or discipline, and learned about the land’s importance to the Yolngu. On their return to Galiwin’ku, Yalu helped the young men and women find employment with community leaders in gardening and other projects. Throughout Galiwin’ku, Yalu performs a similar role. As Yungirrnga says: "Each Tuesday and Thursday we go to the school to teach the young about Yolngu culture. We take them hunting, show them how to weave, and help connect them with the old people so they can spend time together, just sharing."
Yalu’s philosophy is simple, Garngulkpuy says: "The egg in the nest is trying to hatch and the mother nurtures the young chick so it can learn to fly. Then she hands it over to the men, for the next stage of [its] development. We call ourselves Yalu because it is the women who are leading this cultural revival with the youth at Galiwin’ku. We want them to know their responsibilities both as Aborigines and as Australians. Yalu encouraged the Yolngu to celebrate Australia Day on January 26. We hosted a great party that brought all the people at Galiwin’ku together--black and white--and promoted our message of unity and harmony. We are consumed--all of us--by negative thoughts, always thinking about our problems and how the government mistreats us. But we didn’t want to call it an Invasion Day Remembrance, as some Aborigines do. We should be thinking positively. We want people to respect each other--to show compassion to one another. We say ‘Let’s be strong. Let’s walk together and march on.’"
Copyright Cultural Survival
Nurturing Galiwin'ku Youth in Northeast Arnhem Land: Yalu Marrngikunharaw

8 The Chronicle April 2005
1800 186 026 The Northern Territory Government has introduced NT Health Direct; a new telephone based health service that will increase access to information and advice about health issues. Similar services in other parts of Australia and overseas have demonstrated that they provide an effective health care alternative when a person’s usual health care provider is not available or during times when people are unsure of what they should do. NT Health Direct will give residents of, and tourists to, the Northern Territory fast access to confidential, reliable and consistent health advice. Callers to NT Health Direct will speak directly to a registered nurse for the telephone triage of health symptoms, or assistance and advice on health related issues 24 hours a day, seven days a week. The service will be available free of charge to NT callers. NT Health Direct will redirect callers to appropriate after hours support and care where required, and/or give appropriate care advice where health issues can be
managed by the caller or by the caller’s usual health care provider within normal business hours. In an emergency situation callers are reminded to call the ‘000’ emergency number or if they live in remote areas, their local District Medical Officer. Such calls, should they come to the NT Health Direct service, will be transferred through immediately to the appropriate NT Emergency Service via a dedicated priority access line. NT Health Direct, based in Perth, has a sound understanding of the NT and its health structure through the development, by the Department of Health and Community Services, of a comprehensive service directory and training program for the Northern Territory. Clinical governance and program development is also supported through an NT Liaison Officer and an NT Medical Director. For further information contact Carol Atkinson, NT Liaison Officer, NT Health Direct on 89992759 or Jo Murray, Director, Strategic Policy on 89992534.
NT Stroke Conference Darwin 3rd, 4th June 2005
Alice Springs 6th, 7th June 2005
This conference aims to improve Stroke Care in the NT by … promoting evidence based stroke management
principles improving links between acute and community
stroke care providers promoting shared practice methods across NT
We have secured the attendance of two highly credentialed keynote speakers • Dr David Blacker (Neurologist and Stroke Physician, Sir
Charles Gairdner Hospital, Perth, WA) • Ms Ruth Barker (Physiotherapist, University of Queen-
sland, currently completing PhD in the area of Upper Limb Recovery After Stroke)
For more information contact Aleka Freijah or Denys Spencer
Northern Rehabilitation Network, RDH, PO Box 41326, Casuarina NT 0811
Email – [email protected] Fax – (08) 8922 8900
Australasian Diabetes in Pregnancy Society annual
scientific meeting Darwin 15 and 16th July, 2005
This is an annual meeting of Australasian health professionals. It is a multi-disciplinary forum, where physicians, obstetricians, diabetic educators, nutritionists and others involved in the care of pregnant women with diabetes come together to disseminate information and collaborate in research and the development of guidelines for the management of diabetes in pregnancy. This year's program explores the clinical and scientific advances in the management of diabetes in pregnancy and the effect on the infant and later life. For further information:http://www.asnevents.net.au/adips/

9 The Chronicle April 2005
Media Release Monday, 18 April 2005 A mobile podiatry outreach service aimed at reducing the incidence of foot ulcers and amputation will start in a remote Territory town today. The eight-month project is beginning at Gapuwiyak, about 500km east of Darwin, before continuing on to other Top End communities.
Darwin podiatrists Stephen Bond and his wife Deborah Kalia-Bond recently secured the tender after a 2004 pilot project proved highly successful.
Mr Bond said he was looking forward to working as part of the Department of Health and Community Services team tackling preventable chronic disease, such as diabetes, which can lead to foot ulcerations, infections, amputations and even death, if not properly managed.
Mr Bond said diabetes was a primary cause of the foot problems disabling many Territorians in urban and remote communities. “A large part of our role will be to assist in educating people in the communities regarding diabetes, and how it can affect their entire body and in particular their foot health,” Mr Bond said. “Focusing on foot care is just one way the preventable chronic diseases team is working towards better health outcomes in remote communities.”
Preventable chronic diseases project officer Michel Burgum said diabetes could cause chemical abnormalities that damage the nerves in people’s
feet causing numbness and other problems. “A person with numb feet can hurt their feet without knowing it,” Ms Burgum said.
“This may lead to more serious problems such as ulcers, infection and amputation which can be avoided through better diabetes management including foot care and education.
“Stephen and Deborah are wonderful additions to the marvellous work already being done in the communities but podiatry is certainly a gap that needs to be filled.” Ms Burgum said patients would be assessed and would only receive specialist podiatry treatment if classified as being high-risk of developing more serious foot problems. She said those requiring non-specialist treatment would continue to see Aboriginal Health Workers, nurses and other health staff.
The Commonwealth funded project will be assessed at the end of the year to determine its future. Diabetes currently affects more than 194 million people worldwide and is expected to affect 333 million by 2025. The prevalence of diagnosed diabetes in the Territory is three to four per cent and it is estimated a further three to four per cent remains undiagnosed. These rates are often twice as high in some indigenous communities.
Podiatry Outreach Service
Cardiovascular Disease in the 21st Century: Shaping the Future The National Heart Foundation of Australia is the leading organisation in the fight against cardiovascular disease in Australia. We are proud to announce, for the first time, the Heart Foundation Conference, “Cardiovascular Disease in the 21st Century: Shaping the Future” on 23-24 March 2006. Sydney, NSW, is the host city for the conference. The conference is uniquely positioned to address the key issues surrounding the overall management of cardiovascular disease and set strategies in disease management for the years to come. Stakeholders will include cardiac physicians, cardiac surgeons, cardiac technicians, cardiac nurses, health promotion experts, public health professionals, dietitians, nutritionists, scientists and allied health professionals. An exhibition of the latest products and services will be a key element of the conference. The Conference Chair, Professor Philip Harris and Scientific Chair, Associate Professor Chris Semsarian, invite you to submit your expression of interest in attending this unique event. More information will be made available in the coming weeks. In the meantime, to ensure that you receive all of the conference information as it becomes available, please register your expression of interest online here. Contact Details: Heart Foundation Conference 2006 Secretariat GPO Box 2609, Sydney NSW 2001 Australia Telephone: +61 2 9241 1478 Facsimile: +61 2 9251 3552 E-mail: [email protected]

10 The Chronicle April 2005
Good Food Kitchen New healthy food take-away opens in Maningrida The Bawinanga Aboriginal Corporation’s (BAC)‘Good Food Kitchen’ was opened in November 2004 following original plans for its development around 4 years ago. It is a unique shop offering convenient choices of healthy options with not a single hot chip, meat pie or cola drink in sight. The take-away shop currently serves both hot and cold meals and is open from 8 to 4:30pm. Items for sale include: savoury mince with vegetables and rice, hamburgers made with home-made patties and salad, pasta with tomato based sauce, meat and salad wraps/sandwiches/rolls, fruit and nut platters, fresh seafood platters, fruit, fruit and vegetable juices, milks, diet soft drinks and bottled water. Low fat cooking methods are used for meal preparation; olive oil and spray are used and there is no deep fryer in the kitchen. The staff consists of CDEP workers and privately hired community members. The shop also prepares healthy meals for the meals-on-wheels service 3 times per week. Recently the take-away has extended its service to include a camp run where food is loaded into the truck and driven around the community to provide hot and cold foods for the various camps. This take-away shop provides a great source of healthy meals, snacks and drinks which are all very
reasonably priced. Considering the large proportion of meals sourced outside the home, patrons accessing food for convenience can use the shop to make the healthy option the easy choice. Most people are probably wondering if a healthy food take-away is able to operate profitably. Shop manager Warren reports that products are selling well and he hopes to have reached good profits by around the middle of this year. Warren reports an expansion of some lines such as drinks and is developing more ideas on meals that can be produced cost effectively in bulk and so increase profits. Either way, Warren reports he is determined to continue providing healthy foods in his shop and will persevere to make this a successful business and a service that will be of great benefit to the community.
Anthea Oorloff Public Health Nutritionist/Dietitian
Darwin Rural/Remote
Schoolchildren say goodbye to the pie for a few days per week Media release march 04, 2005 School canteens are being encouraged to leave behind their traditional fare of pies, pasties, soft drinks and lollies as part of a new plan to combat childhood obesity.
The Northern Territory School Canteen Guidelines suggest pastries, fizzy drinks and lollies be sold only once per week to school children and recommends shelves are instead stocked with healthier alternatives such as fruit kebabs, fruit and nut energy packs and frozen bananas on sticks.
The guidelines, which are not mandatory, are being explained in Alice Springs by the Department of Health and Community Services to canteen operators from 12 Central Australian
region schools today.
Co-ordinator for Nutrition and Physical Activity in Central Australia Alison McLay said school canteens played an important role in the health of children.
"Evidence shows that eating habits developed during childhood form the basis of eating habits later in life and that dietary intake and food attitudes of school children are closely linked with school environment," Ms McLay said.
"It is a major concern that around 25 per cent of Australian school children are overweight or obese and three out of 10 do not eat vegetables or consume enough dairy foods.
"With more and more children buying lunch and snacks from school canteens, it is important they are encouraged to choose foods that are low in fat, sugar and salt; and high in nutritional value."

11 The Chronicle April 2005
Implementing Aboriginal Health Policy in Australia: A Case Study of the Northern Territory Preventable Chronic Disease Strategy Jane Lloyd, a PhD Student based at Menzies School of Health Research, is planning to conduct a case study on the implementation of the Northern Territory Preventable Chronic Disease Strategy. There is evidence of an active effort on the part of state and federal governments to reduce gaps in life expectancy and to improve the health of Aboriginal and Torres Strait Islander peoples. Despite some progress in developing health policy, there has been only limited progress in implementing such policies. There appear to be many barriers to the efficient, effective implementation of Aboriginal health policy by responsible agencies, particularly, but not only, the mainstream health sector. Therefore, research is being conducted to identify the multiple factors that influence the implementation of Aboriginal health policy by the health sector. The novelty of this research is its focus on the ‘health’ or capacity of a health care system to design and implement Aboriginal health policy effectively. Influences on the implementation of Aboriginal health policy are being explored through a case study of the implementation of the Northern Territory Preventable Chronic Disease Strategy. The research will include three stages: 1) a literature review; 2) in-depth semi structured interviews; and 3) document analysis. The findings will be triangulated to verify the data from each of the sources, and will enable a richer understanding of the implementation stage in the health policy process. The Northern Territory Preventable Chronic Disease Strategy was chosen because of its integrated approach (across levels in the health sector); duration (has been in operation for a number of years and therefore will allow tracking of the implementation phase overtime and through various phases); and focuses on the priority area of preventable chronic disease. The research seeks to understand how the Northern Territory Preventable Chronic Disease Strategy moved from policy to practice.
For further information please contact Jane Lloyd via email ([email protected]) or telephone 08 8922 8235.
Be a part of Australia’s Biggest Morning Tea
Thursday 26 May 2005 The Cancer Council Northern Territory asks all Territorians to support Australia’s Biggest Morning Tea on Thursday 26 May 2005. Australia’s Biggest Morning Tea is one of The Cancer Council’s foremost fundraising events and is the largest, most successful event of its kind in Australia. More than a million people Australia wide will participate in the event this year and we hope to raise over $7 million. 2005 will be our biggest year yet – Australia’s Biggest Morning Tea is registered with Guinness World Records to break the record for the ‘World’s Largest Simultaneous Tea Party’. The Cancer Council NT is excited about this challenge and is confident that, with the Australian community’s support, we can enter the record books.

12 The Chronicle April 2005
Australian Integrated Mental Health Initiative (AIMHI) NT is a five year project focussed on improving outcomes in Aboriginal Mental Health (for more information see Chronicle 7.6). The project has service delivery and health promotion working parties and an indigenous reference group. This is one of the resources the project completed in its first year, and is one of a number of resources on the website. To give feedback, find out more information, or to order the flip chart contact Erin Dawkins 89227706 or [email protected]. AIMHI NT Chief investigator: Dr Tricia Nagel, Associate investigators: Carolyn Thompson, Robert Mills, Jenni Judd and Pat Bradley'
Mental Problem StoryHi, Its AIMhi back again from the story “That Somebody” with Mental Problem”. I want to talk about another story about mental illness because “That Somebody” might need some help from you mob.
Mental Health
Story Teller Mob
AIMHI
NT
MENTAL PROBLEM STORY
Mental Problem StoryHi, Its AIMhi back again from the story “That Somebody” with Mental Problem”. I want to talk about another story about mental illness because “That Somebody” might need some help from you mob.
see things that are not there
Is sad or crying a lot
That somebody when he/she go silly in the head sometimes he/she will:
Walk around all night.
Get frightened & confused.
Stops hunting, fishing and football.
Sit alone a lot.
Hear voices
Get angry or violent
Won’t eat or sleep
Yeah, that’s like my cousin/sister. After baby one died, she wouldn’t eat and she would sit on her own all the time.
Well, my auntie, she hears voices in her head and she would pick up a knife sometimes and would shout all the time. Us mob we would run away and wait until she stop.
When you know that somebody who’s looking silly in the head, having silly thoughts, not eating or sleeping, awake all night like that… that’s a mental illness. Like sugar diabetes - it needs treatment
What treatment for that bros?
Frightened and confused
Walking around all night
Not eating or sleeping

13 The Chronicle April 2005
Family. Maybe sit and talk with that person, keep him/her company. That person might need to stay somewhere were its quiet for a while - bit of time away from all the humbug.
OR If that person’s problem is cultural he might need help from a healer. Maybe that person might need tablets from the doctor through that mental health mob.
Tablets from them Mental Health Mob
Traditional Healer
Sit and talk/keep him/her company
So that person that’s sick in the head - we should get help for them?
Yes - don’t wait too long -he/she will just get sicker. Go to elders, or clinic. Don’t leave that person alone, he/she might get worse and might need to go to hospital if you leave it too long.
Clinic/Hospital
Mental Health Team
When do you get help?
If you look closely - then you will see that silliness coming on. Things like he/she not sleeping or not eating. Best thing to do is get help and get help early.
Frightened and confused
Not eating or sleeping What makes the sickness come?
Problems like: Husband or wife worries, family worries, money worries, too much gunga, too much grog, cultural worries or stopping tablets that were helping him/her feel good.
Best treatment -keep calm, keep strong family around, keep a close eye, keep taking medicines that help. Don’t stop medicine just because he/she feels better. KEEP MEDICINE GOING TO STAY WELLTreatment to
make it better is family?
Strong family -family can get help from elders, the clinic, mental health mob or the hospital
14 The Chronicle April 2005
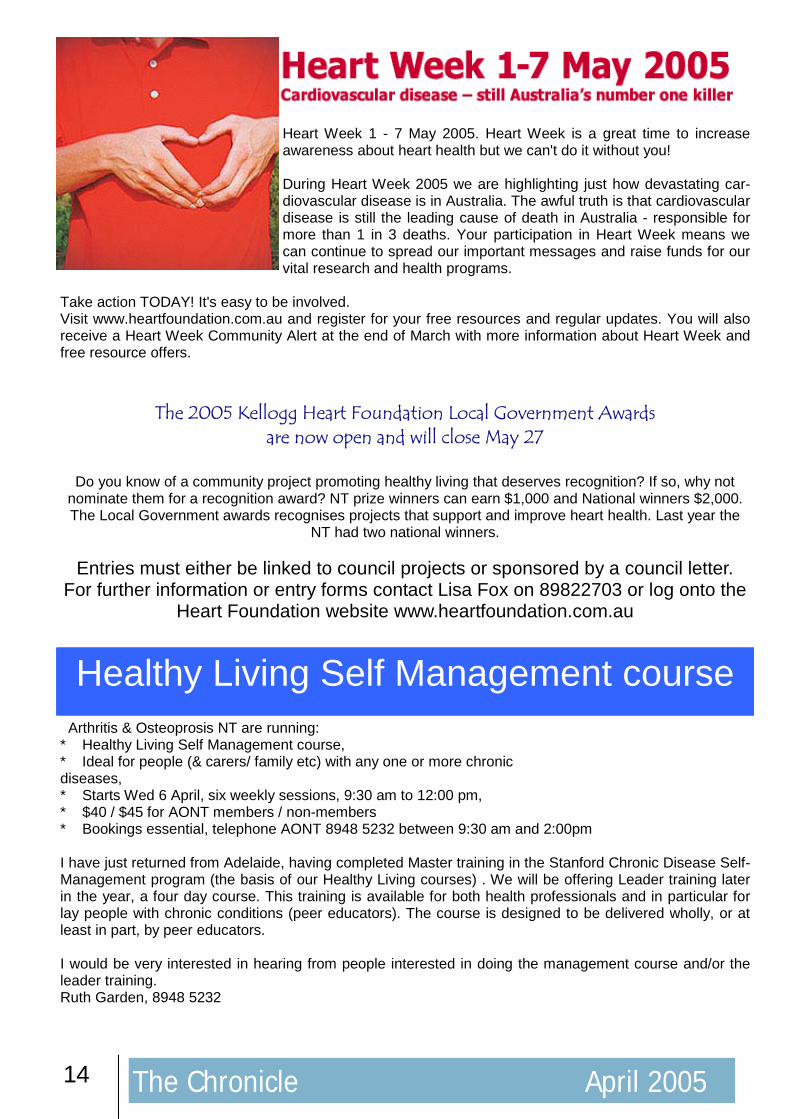
Arthritis & Osteoprosis NT are running: * Healthy Living Self Management course, * Ideal for people (& carers/ family etc) with any one or more chronic diseases, * Starts Wed 6 April, six weekly sessions, 9:30 am to 12:00 pm, * $40 / $45 for AONT members / non-members * Bookings essential, telephone AONT 8948 5232 between 9:30 am and 2:00pm I have just returned from Adelaide, having completed Master training in the Stanford Chronic Disease Self- Management program (the basis of our Healthy Living courses) . We will be offering Leader training later in the year, a four day course. This training is available for both health professionals and in particular for lay people with chronic conditions (peer educators). The course is designed to be delivered wholly, or at least in part, by peer educators. I would be very interested in hearing from people interested in doing the management course and/or the leader training. Ruth Garden, 8948 5232
Heart Week 1 - 7 May 2005. Heart Week is a great time to increase awareness about heart health but we can't do it without you! During Heart Week 2005 we are highlighting just how devastating car-diovascular disease is in Australia. The awful truth is that cardiovascular disease is still the leading cause of death in Australia - responsible for more than 1 in 3 deaths. Your participation in Heart Week means we can continue to spread our important messages and raise funds for our vital research and health programs.
Take action TODAY! It's easy to be involved. Visit www.heartfoundation.com.au and register for your free resources and regular updates. You will also receive a Heart Week Community Alert at the end of March with more information about Heart Week and free resource offers.
The 2005 Kellogg Heart Foundation Local Government Awards are now open and will close May 27
Do you know of a community project promoting healthy living that deserves recognition? If so, why not
nominate them for a recognition award? NT prize winners can earn $1,000 and National winners $2,000. The Local Government awards recognises projects that support and improve heart health. Last year the
NT had two national winners.
Entries must either be linked to council projects or sponsored by a council letter. For further information or entry forms contact Lisa Fox on 89822703 or log onto the
Heart Foundation website www.heartfoundation.com.au
Healthy Living Self Management course
15 The Chronicle April 2005
New research to be published soon by a University of Sydney medical team, shows that childhood obesity is a serious health problem in Australia. Dr Michael Booth from Sydney University's Centre for Overweight and Obesity will be a keynote speaker at the 9th Chronic Diseases Network Conference on 8-9 September 2005. Professor Michael Booth, co-director of the University of Sydney's Centre for Overweight and Obesity, said teenagers were already showing signs of serious illness caused by their weight. Dr Booth and his colleagues are conducting a study of 15-year-olds, and preliminary results show an alarming number of health problems previously only detected in adults. "We've collected blood samples from 500 15-year-olds to look at health markers like cholesterol levels, blood pressure, triglycerides, insulin levels, glucose levels, something called c-reactive protein, which is an indicator of vascular damage, and liver enzymes which give an indication of liver cell damage associated with weight. "We still have to make some adjustments, but overall we've found they are all frighteningly high. "A proportion of 15-year- olds are already showing significant signs of organ damage associated with be-ing overweight." Dr Booth said the increasing level of Type 2 diabetes would result in many children devel-oping potentially deadly diseases by the age of 30 or 40. "For kids with signs of insulin resistance, if they don't improve their health by their 30s they will be suffering all the morbidities that people used to suffer in their 60s, such as amputations, blindness, liver failure, kid-ney failure and heart disease," Dr Booth said. "For others, by the time they reach their 30s and early 40s there will be lines wrapping around the block in front of hospitals of people needing to have liver transplants. I really don't think the magnitude of the prob-lem has settled into the minds of government yet." Dr Booth's results will be presented to the NSW Government later this year. http://www.usyd.edu.au
Source: Child Health News Published: Thursday, 24-Feb-2005 http://www.news-medical.net/print_article.asp?id=7955
Third National Workshop on Strongyloidiasis "We are making progress!"
Fri 10 - Sat 11 June 2005
Rydges Capricorn Resort, Yeppoon, near Rockhampton, Central Queensland
Details, conference registration form, call for abstracts are available from http://www.jcu.edu.au/school/phtm/PHTM/ss/3-ss-workshop.htm. The strongyloidiasis workshop is being held in conjunction with a num-bers of AIMS workshops.
Guest Speakers Prof GA Schad, a prominent researcher on Strongyloides from the USA is an invited speaker. The guest speakers include most of the prominent researchers, clinicians, and field workers on strongyloidiasis in Australia.

16 The Chronicle April 2005

17 The Chronicle April 2005

18 The Chronicle April 2005
GOVERNMENT TO EXTEND FREE VACCINATION PROGRAM
Source Media Release Tony Abbott 07/03/2005
The Commonwealth Government will provide free chickenpox (varicella) vaccine for all babies and for at-risk teenagers and replace oral polio vaccine (OPV) with injectable inactivated polio vaccine (IPV). These two new vaccinations will be funded under the National Immunisation Program and will commence on 1 November 2005. The government has responded to recommendations made in late January 2005 by the Australian Technical Advisory Group on Immunisation (ATAGI) which has been reviewing the latest evidence on the effectiveness of these vaccines. The new vaccines will cost $143.2 million over five years.
Chickenpox vaccine will be offered free to all children turning 18 months of age. In addition, children aged between 10-13 years who have not received chickenpox vaccine or who have not had the disease will be eligible for free vaccine as part of a long-term catch-up program. The replacement of oral with injectable polio vaccine will allow the use of a new six-in-one combination vaccine that provides protection against diphtheria, tetanus, pertussis (whooping cough), hepatitis B, Haemophilus influenzae type b (Hib) and polio. Because hepatitis B and Hib are included in this new combination vaccine, many babies will receive one less injection at 2 and 4 months of age. The government has negotiated internationally competitive prices for these vaccines. In 1996, Commonwealth Government spending on vaccines was $13 million. With the introduction of these new vaccines, National Immunisation Program spending will reach $292 million 2005-06, a 22-fold increase.
Reviews “This excellent report complements and extends World Health Organization efforts to emphasize the importance of health sector reform to combat gender-based violence. […] For Australian readers interested in Australian health care reform, the value of this report lies both in the proposed model and processes used to drive the reform and the excellent resources and bibliography.”
“The flexible, participatory and respectful approach which the authors of this blueprint for health system reform have outlined, and the resources they document of the final pages, are recommended not only for urban-focused policymakers, but will be of particular interest to those involved in and concerned for Aboriginal and Torres Strait Islander family violence and health system reform”. —Australian Health Review, Journal of the Australian Health Care Association. Vol. 28, No. 3
Violence against Women: The Health Sector Responds
Demonstration of an E-mailed Worksite Nutrition Intervention Program G Block, T Block, P Wakimoto, C Block (www.cdc.gov/pcd/issues/2004/jul/04_0016.htm)
A 12-week health-promotion project delivered entirely by e-mail at a corporate worksite increased fruit and vegetable intake and decreased fat intake among employees.
Dietary fat and low fruit and vegetable intake are linked to many chronic diseases. In this study, employ-ees at a worksite were invited to participate in a program, delivered entirely by e-mail, to reduce dietary fat and increase fruit and vegetable intake. Elements of the program included tailoring to the participant’s die-tary lifestyle, baseline assessment and feedback about dietary intake, family participation, and goal set- ting. The program was delivered weekly to participants via e-mail for 12 weeks. Each e-mail included infor-mation on nutrition or on the relationship between diet and health, dietary tips tailored to the individual, and small goals to try for the next week. Approximately one third of employees who were offered the 12-week program signed up for it, and satisfaction was high. Results suggested significant increase in fruit and vegetable consumption and significant decrease in fat intake.

19 The Chronicle April 2005
What is this document? This document is a package of materials that aims to assist health educators to integrate chronic disease education into existing and new programs, using a population health approach. It consists of: • background reading about how this chronic disease package came about • a curriculum framework upon which to develop new or adapt existing educational programs in a population health model • a list of expected core outcomes for all graduate remote and rural primary health care practitioners working in the prevention, early detection and
management of chronic disease • an implementation framework to assist in conducting or managing orientation and professional development, including accredited programs • some suggested teaching and learning approaches • some tools and resources for educators to use.
This document can also be accessed in a pdf file
from www.nt.gov.au/health/publications.shtml To obtain hard copies of this publication, contact
Menzies School of Health Research on ph: (08) 8922 8196 or
email: [email protected]
Written by: Janie Dade Smith, RhED Consulting in conjunction with a steering committee made up of mem-bers from the: Menzies School of Health Re-search James Cook University Aboriginal Medical Services Alliance of the Northern Terri-tory Apunipima Cape York Health Council NT Department of Health and Community Services Queensland Health University of Queensland
The NT Child and Family Health Nurses Association The NT Child and Family Health Nurses Association (NT C&FHNA) was formed in October 2003 to provide networking and professional development opportunities for all Northern Territory nurses who work with children and their families. The membership of NT C&FHNA is steadily growing and can boast representation across a vast geographic area. We have members in Alice Springs, Katherine, Groote Eylandt and Melville Island as well as Darwin urban and rural areas. Paeditric Nurses, Child and Family Health Nurses and Health Promoting School Nurses are represented within the membership. Active participation of all members is made possible by teleconferencing of meetings and educational forums. For further information, interested nurses can contact Marie Land on: (w) 899 92490 (h) 8985 4978 or email [email protected] 2005 is shaping up to be an exciting year for members with planned bi-monthly education forums. There was great attendance at the first forum for the
year. One of our members, Karen Piper RN, RM, Child Health Nurse, MPH, gave an enthusiastic presentation on literature searches and critiquing literature for delivery of evidence based practice. A side product of this presentation was the decision to commence a Journal Club for interested members. The next education forum will be held on Tuesday 26th April and promises to be a very interesting session – Erin Evans, a Health Promoting School Nurse and member of NT C&FHNA, will present an overview of her broad and many roles in her work at Taminmin High School. Last year the NT C&FHNA endorsed a research proposal, ‘The Value of Nurses’ Contribution to Child Protection’, developed by the Chairperson, Marie Land, and was successful in gaining some funding from NAPCAN (National Association for Prevention of child abuse and neglect) to carry out the study. Marie has been granted a full scholarship from Charles Darwin University to conduct this study and present a thesis for a Master of Social and Policy Research. Professor Lesley Barclay is Marie’s supervisor.

20 The Chronicle April 2005
Where: Holiday Inn Esplanade Darwin When: 8 – 9 September 2005
Keynote Speakers Include: • Graham Vimpani
• Sue Sayers, Dorothy Mackerras & Gurmeet Singh • Victor Nossar
• Lesley Barclay • Kate Senior
• Julie Quinlivan • Michael Booth • Paul Torzillo
For Further Information please contact: Gaye Messer at The Best Conference & Events Co.
Ph: 08 8981 1875 Email: [email protected]
Childhood influences on adult chronic disease
“Making the Links “Making the Links -- Improving the Outcomes Improving the Outcomes””
99thth Annual Annual Chronic Diseases Network Chronic Diseases Network
ConferenceConference
There is strong evidence that children’s early life experiences influence their health and wellbeing in later life. We know that the foundations for health are laid down before birth, and continue to be built upon during the critical periods of infancy, childhood and adolescence. The effects of early development last a lifetime. Speakers will explore links between the early years and adult health/wellbeing. The program will in-clude examples of activities that are making a real difference and improving outcomes. The Chronic Diseases Network Conference has a great reputation for imparting practical information to influence policy and practice and provide valuable networking opportunities.