Embed Size (px)
DESCRIPTION
Terminology for representation of Diagnostic Imaging Procedures. Dr Keith Foord Consultant Radiologist, East Sussex Hospitals National Programme for IT in the NHS Wednesday 1 st December 2004. A national system of RIS coding and descriptors ?. - PowerPoint PPT Presentation
Citation preview

Terminology for Terminology for representation of representation of
Diagnostic Imaging Diagnostic Imaging ProceduresProcedures
Dr Keith FoordConsultant Radiologist, East Sussex Hospitals
National Programme for IT in the NHS
Wednesday 1st December 2004

A national system of RIS coding A national system of RIS coding and descriptors ?and descriptors ?
Relates to needs of request/entry systems within ICRS – pre-RIS
Consistency and uniqueness in requesting terminology – pre-RIS and within RIS
Consistency in activity measurement - RIS Consistency in clinical coding of events - RIS But must be as intuitive and easy to use as possible Should have national acceptance For accurate communication of results data between hospitals
– post RIS results reporting, cluster stores and national spine For ‘Payment by results’ – accurate records of same patient
activity – national tariffs

NHS Costings Code BookNHS Costings Code Book

Other sourcesOther sourcesRIS Descriptors and Codings from:GuildfordNorth BristolHastingsEastbourneCalderdaleBart’sNWWM cluster

DescriptorsDescriptors
Descriptors need to be UNIQUE in ICRS
FOOT LEFT not uniqueWhen a user searches all of the examinations available for ‘Foot Left’the search may return:
FOOT LEFT, FOOT LEFT Swab, FOOT LEFT Physiotherapy, FOOT LEFT Dressing,etc., etc.
But XR FOOT LEFT is unique

Radiology Short CodesRadiology Short Codes
Used in RIS as shortcuts
For bookingsFor internal communications within RadiologyTo help group proceduresFor internal management / audit / activity
For common use need a structure, ideallyshort (max. 6 letters/digits) and logical

1 2 3 4 5 6ModalityX – X-rayF – FluoroI – Interventional/FluoroC – CTM – MRIU – U’soundN – Radionuclide ImagingP – PETE- Endoscopy
Post-qualifier
(Extra or sub-descriptor)
4th letter reserved for R, L, B or W
if procedure R or L lateralisable,Both or Whole body,
otherwise can be used for anyletter or number
Three or four letter body part/ function code
Radiological Short Codes

A B C D E
A B C D F
Format for a midline or non lateralising structure, nopost qualifier
Format for a lateralisable or whole body structure, no post qualifier

X S I J S
X H A N R
Eg X-ray SIJ
Eg Right Hand X-ray

M A B D O
N B O N W
Eg MRI Abdomen
Eg Whole body Bone scan

A B C D E G
A B C D F G
Format for a midline or non lateralising structure, with a post qualifier
Format for a lateralisable or whole body structure, with a post qualifier

Extra qualifiers (6Extra qualifiers (6thth letter/number = letter/number = G))
A Ablation B Biopsy (Core or FNA) D Drainage or Aspiration of fluid E Embolisation I Insertion of device J inJection - as an objective of the procedure, not as part of the preliminary to this objective M Mobile - for any modality, but particularly for 'portable' plain films and use of mobile image
intensifiers O tOmography in its wider sense. O may be added to any plain film examination to define planar
tomography - or postcoordinated P Plasty - as in angioPlasty or dacrocystoPlasty - ie balloon dilatation R for Radiotherapy planning S Stent T Use of intraThecal contrast X eXtraction - eg in retrieval of intravascular foreign bodies or removal of temporary IVC filter 1 First part of study 2 Second part of study 3 Third part of study

C P E L V B
I A S F R P
Eg CT guided PELVic Biopsy
Eg Interventional (Fluoroscopic) Right SFA Angioplasty

Pre and Post Co-ordination (1)Pre and Post Co-ordination (1) In order to group procedures many RIS systems lack
the ability to post co-ordinate procedures together under one accession number.
Particular examples are for 'both' plain film exams eg 'both ankles' and in CT where examinations often combine e.g. CT Chest, Abdomen, Pelvis.
Pre co-ordination or grouping of these procedures is therefore required in advance.
Pre co-ordination should not be used in RIS-PACS systems capable of full post co-ordination as with these individual procedure codes will be automatically or manually grouped prior to archiving and reporting

C P E L V B
Eg CT guided PELVic Biopsy
This is pre-coordinated with the wholeprocess described in the code

Examples of other pre co-Examples of other pre co-ordinated studiesordinated studies
CT NECK/THORAX/ABDO/PELVIS CNCAP CNCAP PrecoordinatedCT NECK/THORAX/ABDO/PELVIS WITH CONTRAST CNCPC CNCPC PrecoordinatedCT PELVIS AND ASPIRATION/DRAINAGE CPELVD CPELVD D PrecoordinatedCT PELVIS AND BIOPSY CPELVB CPELVB B PrecoordinatedCT PELVIS WITH/WITHOUT CONTRAST CPEWC CPEWC PrecoordinatedCT THORACIC AND LUMBAR SPINE CTLSP CTLSP PrecoordinatedCT THORACIC AND LUMBAR SPINE WITH CONTRAST CTLSC CTLSC PrecoordinatedCT TRAUMA HEAD AND C SPINE CSKTC CSKTC PrecoordinatedELBOWS BOTH XELBB XELBB PrecoordinatedFEMORA (THIGH) BOTH XTHIB XTHIB PrecoordinatedFOREARMS BOTH XFARB XFARB PrecoordinatedHANDS BOTH XHANB XHANB PrecoordinatedHIPS BOTH XHIPB XHIPB PrecoordinatedHUMERI (UPPER ARMS) BOTH XUPAB XUPAB PrecoordinatedKNEES BOTH XKNEB XKNEB PrecoordinatedLEG LENGTH MEASUREMENT: BOTH XLEMB XLEMB PrecoordinatedMAMMOGRAM BILATERAL XMAMB XMAMB Precoordinated

Pre and Post Co-ordination (2)Pre and Post Co-ordination (2) In modern RIS systems post co-ordination can be applied
to group related procedures together. Some procedure codes such as 'U/S biopsy' by
themselves do not define precisely what has happened although it would define the activity of “Performing a biopsy under ultrasound control and the consumables/activity associated with this.”
Such codes need post co-ordinating with the relevant body part to fully inform activity statistics
Similarly separate CT body part examinations can be post co-ordinated together to enable the multiple examinations to be reported together as one report.
The advantage is a more sophisticated approach to audit, activity measurement and stocktaking

Eg CT guided PELVis Biopsy
C P E L V
C B I O P BPLUSPLUS
Are POST coordinated and describe both processes which arethen reported as one. CT biopsy cost structures do not need to be built into multiple codes
C P E L V B

Eg PET/CT for Chest
C C H E S
P G E N WPLUSPLUS
Are POST coordinated and describe both processes which arethen reported as one.

Codes for post co-ordinationCodes for post co-ordination
ANGIOPLASTY AORTO-FEMORAL IAAFMP IAAFMP P Associate (Postcoordinate with Angio)ANGIOPLASTY CEREBRAL IACEGP IACEGP P Associate (Postcoordinate with Angio)BILIARY DRAINAGE IBILDD IBILDD D Select postcoordinators from biliray listCT 3 D STUDY C3DSY C3DSY Postcoordinate with body part studyCT 4 D STUDY C4DSY C4DSY Postcoordinate with body part studyCT Guided ablation CABLTA CABLTA A Postcoordinate with body part studyCT guided aspiration/drainage CASPD CASPD D Postcoordinate with body part studyCT guided biopsy CBIOPB CBIOPB B Postcoordinate with body part studyCT MIP STUDY CMIPY CMIPY Postcoordinate with body part studyDrainage catheter exchange IEXCHD IEXCHD D Postcoordinate with body part studyEMBOLISATION IEMBOE IEMBOE E Associate (Postcoordinate with Angio)EMBOLISATION CEREBRAL IACEGE IACEGE E Associate (Postcoordinate with Angio)Embolisation of AVM IAVEME IAVEME E Associate (Postcoordinate with Angio)FLUORO ASPIRATION/DRAINAGE FASDRD FASDRD D Postcoordinate with body part studyInternal metallic stent IMETCS IMETCS S Postcoordinate with body part studyPercutaneous ethanol injection IETHAJ IETHAJ J Postcoordinate with body part studySIALOGRAPHY STONE REMOVAL ISIACX ISIACX X Postcoordinate with body part studySIALOPLASTY ISIAOP ISIAOP P Postcoordinate with body part studySPECT (any other additional) NSPECO NSPECO Postcoordinate with body part studyTHROMBOLYSIS: AORTO:FEMORAL IAATTJ IAATTJ J Associate (Postcoordinate with Angio)U/S ARTERIAL UARTE UARTE Postcoordinate with body part studyU/S BIOPSY/FNA BIOPSY UBIOPB UBIOPB B Postcoordinate with body part studyU/S DOPPLER UDOPP UDOPP Postcoordinate with body part studyU/S EXTREMITY UEXTR UEXTR Postcoordinate with body part studyU/S GUIDED CORE or FNA BIOPSY UBIOPB UBIOPB B Postcoordinate with body part studyU/S GUIDED INJECTION USINJJ USINJJ J Postcoordinate with body part studyVENOUS SAMPLING FVSAM FVSAM Postcoordinate with body part study

Alphabetical list of all proceduresAlphabetical list of all proceduresby DESCRIPTOR or CODE by DESCRIPTOR or CODE
(1037 codes)(1037 codes)
Descriptors Codes

Sub-Descriptors / CodesSub-Descriptors / Codes REQUESTING Layer
(1st order) Right Oblique QR Left Oblique QL Right Lateral LR Left Lateral LL Weight Bearing WB Standing ST Axial AX AP20o 20 Judet’s JU Stryker’s SY Etc…
IN RADIOLOGY Layer (2nd order)
Supine SU Prone PR Decubitus DE Complex Oblique QC Angled Oblique
22,30,45 Frog laterals FR May need to combine with
1st order list eg DELR

Total diagnostic Total diagnostic examinations/interventionsexaminations/interventions
Pre-coordinated full list
1037
Post-coordinators only
46
Post-coordinated examinations
924
‘Both’ and
multi-CTs
67
Endoscopy
11
X-Ray
144
CT
166
MRI
149
IR Fluoro
157
US
131
PET
4
Diag Fluoro
190
Diag RNI
107

NPfIT and Descriptors/CodesNPfIT and Descriptors/Codes
Southern Cluster – IDX – GE PACS- ? Cerner RISCerner RIS London Cluster-IDX- Philips PACS-? Sectra RIS NE & EEM Clusters- iSOFT-? Agfa PACS-? RIS NWWM Cluster- iSOFT- ComMedica PACSComMedica PACS –Kodak
RIS Has RCR endorsement SNOMED CT can be integrated-matched (Dr David
Nag)

SNOMED CTSNOMED CT
Carecast provides support for clinical coding using the SNOMED CT nomenclature for diagnosis and procedure codes.
SNOMED CT codes will be applied to the patients record through manual selection by users, as well as an integrated bi-product of clinical processes (i.e. orders, assessments).
SNOMED CT clinical coding is supported for inpatient and outpatient encounters.

SNOMED CTSNOMED CT
At the end of an episode / encounter of care, SNOMED CT codes are recorded in Carecast via the Discharge Summary / Encounter diagnosis and procedure codes. The SNOMED codes recorded in Carecast are sent to the 3M clinical encoder where clinical coding is completed in SNOMED CT, ICD10, Read, and OPCS4.
Codes will be transferred back to Carecast and will update, not replace, the patient diagnosis and procedure codes. A full audit trail is available.

SNOMED CTSNOMED CTWithin Carecast P1R2, users will have the ability to manually record SNOMED CT codes within the following areas:§ Discharge Summary / Encounter § Problems / Provisional Diagnoses
Within Carecast P1R2, SNOMED CT codes will be recorded against the patients record, as a bi-product of clinical processes, in the following clinical areas: § Assessments§ Findings / Flowsheets
§ Orders§ Results

OrdersOrders and and ResultsResultsin Radiologyin Radiology
SNOMED CT Order codes can be derived from Order/Entry systems, but will be MUCH MORE ACCURATE if derived from the accepted and if required modified final RIS procedure entry with SNOMED CT matching.
SNOMED CT Results codes from Radiology are a dilemma. A provisional radiological diagnosis which may be a list of differential diagnoses could be entered by a reporter (ie manually). Unlikely to happen !
The use of DICOM structured reporting may give the possibility of automatically constructing radiological diagnosis codes from the structured report

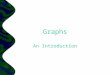
Incorporated into the report are captured images of key findings (which can be exploded to full screen presentation), structured diagnosis information, recorded audio, the ability to sort findings by anatomy or priority, to view prior findings associated with the corresponding patient and hyperlinks to related information.
DICOM SR – is an ‘envelope’, but within this useful structure is available.
User decides how much structure to use and controls with templates the type of content, if it is mandatory or optional and modes of expression
Structured reporting

Link Features to Description
New nodulesuperimposedwith rightfourth rib
Free air
10% Pneumothorax
Cavitation
Structured reporting

David Clunie
Development Director, Imaging Products
ComView Corporation – Paper at SPIE, 2001
Structured reporting

David Clunie
Development Director, Imaging Products
ComView Corporation – Paper at SPIE, 2001
Structured reporting