Embed Size (px)
Citation preview
L. Berrino
Dipartimento di Medicina SperimentaleSez. di Farmacologia “L. Donatelli”
Facoltà di Medicina e Chirurgia
Terapia empirica antibioticain urgenza:
è sempre valida?
Per instaurare un’appropriataPer instaurare un’appropriataantibioticoantibiotico--terapia empirica bisognaterapia empirica bisogna
tener conto di:tener conto di: I più probabili patogeni che causanoI più probabili patogeni che causano
specifiche infezioni gravispecifiche infezioni gravi
La distribuzione locale dei patogeni e dellaLa distribuzione locale dei patogeni e dellaloro antibioticoloro antibiotico--resistenzaresistenza
Gli specifici fattori di rischio dei pazientiGli specifici fattori di rischio dei pazienti
Terapia antibiotica empirica:Terapia antibiotica empirica:durata del trattamentodurata del trattamento
La durata è condizionataLa durata è condizionata dal patogeno in causadal patogeno in causa dalla rapidità di risposta al trattamentodalla rapidità di risposta al trattamento
inizialeiniziale dalla presenza didalla presenza di comorbiditàcomorbidità dalla presenza di complicanzedalla presenza di complicanze Sospensione dopo almeno 72 h diSospensione dopo almeno 72 h di
sfebbramentosfebbramento
What is misuse of antibiotics?What is misuse of antibiotics?
Misuse of antibiotics can include any of the followingMisuse of antibiotics can include any of the following1818::
When antibiotics are prescribed unnecessarily;When antibiotics are prescribed unnecessarily; When antibiotic administration is delayed in critically illWhen antibiotic administration is delayed in critically ill
patients;patients; When broadWhen broad--spectrum antibiotics are used toospectrum antibiotics are used too
generously, or when narrowgenerously, or when narrow--spectrum antibiotics are usedspectrum antibiotics are usedincorrectly;incorrectly;
When the dose of antibiotics is lower or higher thanWhen the dose of antibiotics is lower or higher thanappropriate for the specific patient;appropriate for the specific patient;
When the duration of antibiotic treatment is too short orWhen the duration of antibiotic treatment is too short ortoo long;too long;
When antibiotic treatment is not streamlined according toWhen antibiotic treatment is not streamlined according tomicrobiological culture data results.microbiological culture data results.
18. Gyssens IC et al. 1992, 30: 724-7.
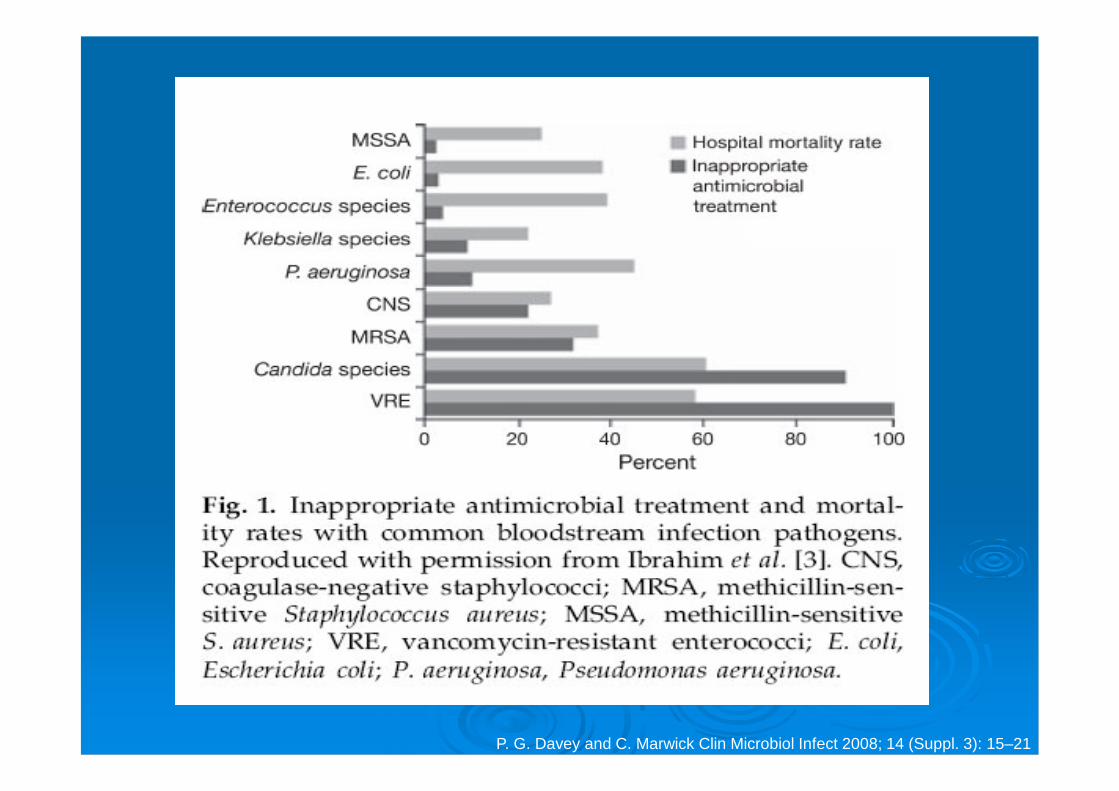
P. G. Davey and C. Marwick Clin Microbiol Infect 2008; 14 (Suppl. 3): 15–21
…the timing of antimicrobial treatment is important. Treating only afterthe microbiological test results are obtained ensures that the correctantimicrobial is chosen, but this strategy increases the risk of a worseoutcome due to delayed treatment.
Changing to the right antibiotic once the culture results come back is notas beneficial as getting the antibiotic right from the start, possiblybecause of physiological deterioration of the patient or because ofbacterial dissemination or abscesses, which are difficult to treat withantibiotics.
To avoid delays in therapy, which can have significantconsequences for treatment outcomes in serious infections,clinicians regularly make decisions on empirical therapyimmediately on presentation, without the benefit of laboratoryresults, thereby making educated guesses as to the causativepathogens and their resistance phenotypes.
Segreti J. 2009; 15: 5–10
The likelihood of patients receiving inadequate empirical therapyincreases with the increasing prevalence of infections caused byantimicrobial-resistant bacteria. Local epidemiology and resistancerates should therefore be taken into consideration.
Several studies have demonstrated that the administration ofinadequate empirical antimicrobial therapy and, furthermore,inappropriate empirical therapy, significantly increase the rate ofmortality in infections such as bloodstream infections, MRSA sterilesite infections, nosocomial pneumonia, and ventilator-associatedpneumonia. In addition, delaying therapy for S. aureus bacteraemiahas been shown to increase the risk of mortality and the overalllength of hospitalization; early administration of appropriate therapyin S. aureus infections is key to reducing these risks.
The Empirical DilemmaThe Empirical DilemmaWhat is the impact of choosing inappropriate therapy?
Segreti J. 2009; 15: 5–10
Ashkenazi S. Eur J Pediatr (1996) 155 : 545-550
Among the risk factors identified, one factor, inappropriateempiric antibiotic treatment, depends on us, thephysicians. Inappropriate therapy affected survivalsignificantly and independently of other factors, increasingthe risk of mortality by 2.4-fold (95% confidence interval,1.1-5.4). Others have also reported the detrimentalconsequences of inappropriate antibiotic therapy ofchildhood bacteraemia in terms of mortaliy andcomplications.
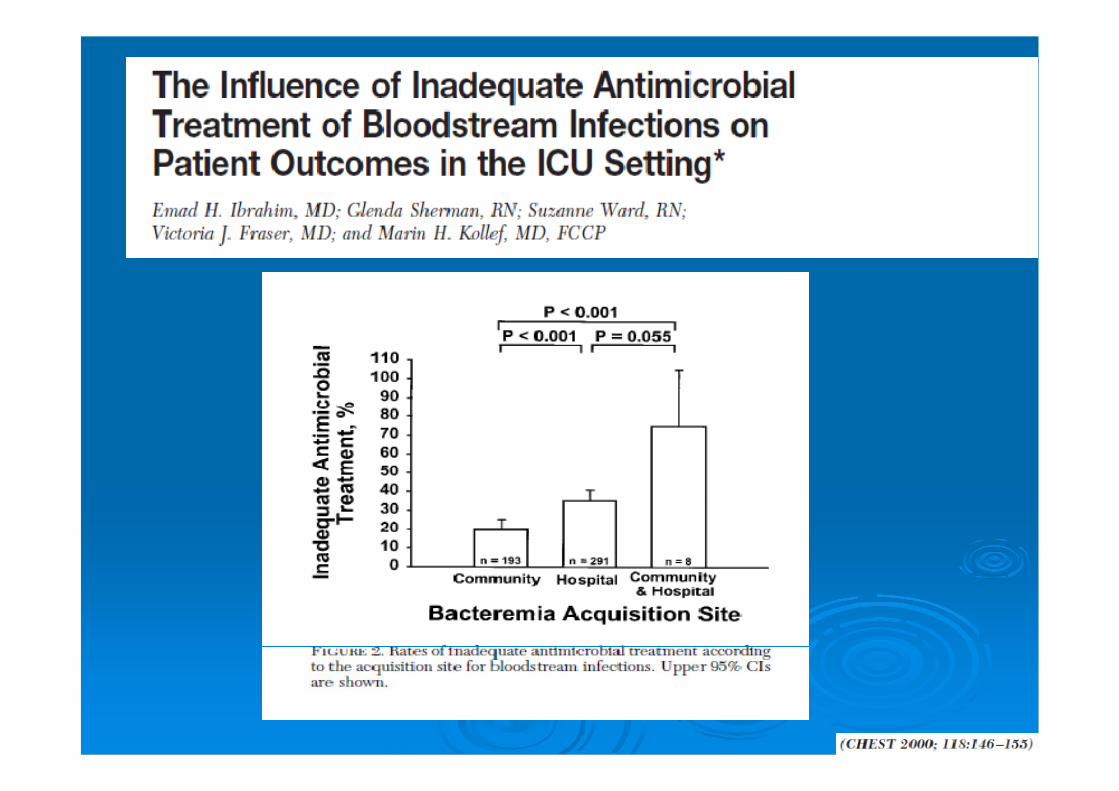
In a prospective cohort study of 492 critically ill patients admitted to
the intensive care unit (ICU) with a bloodstream infection, inadequate
antimicrobial treatment proved to be the most important risk-factor for
in-hospital mortality.
The mortality rate for patients who initially received inappropriate
antimicrobial treatment (61.9%) was significantly greater than the rate
for patients who received antimicrobial treatment that matched the
pathogen from the start (28.4%; p < 0.001).
P. G. Davey and C. Marwick Clin Microbiol Infect 2008; 14 (Suppl. 3): 15–21
IMPACT OF INAPPROPRIATEIMPACT OF INAPPROPRIATETREATMENTTREATMENT
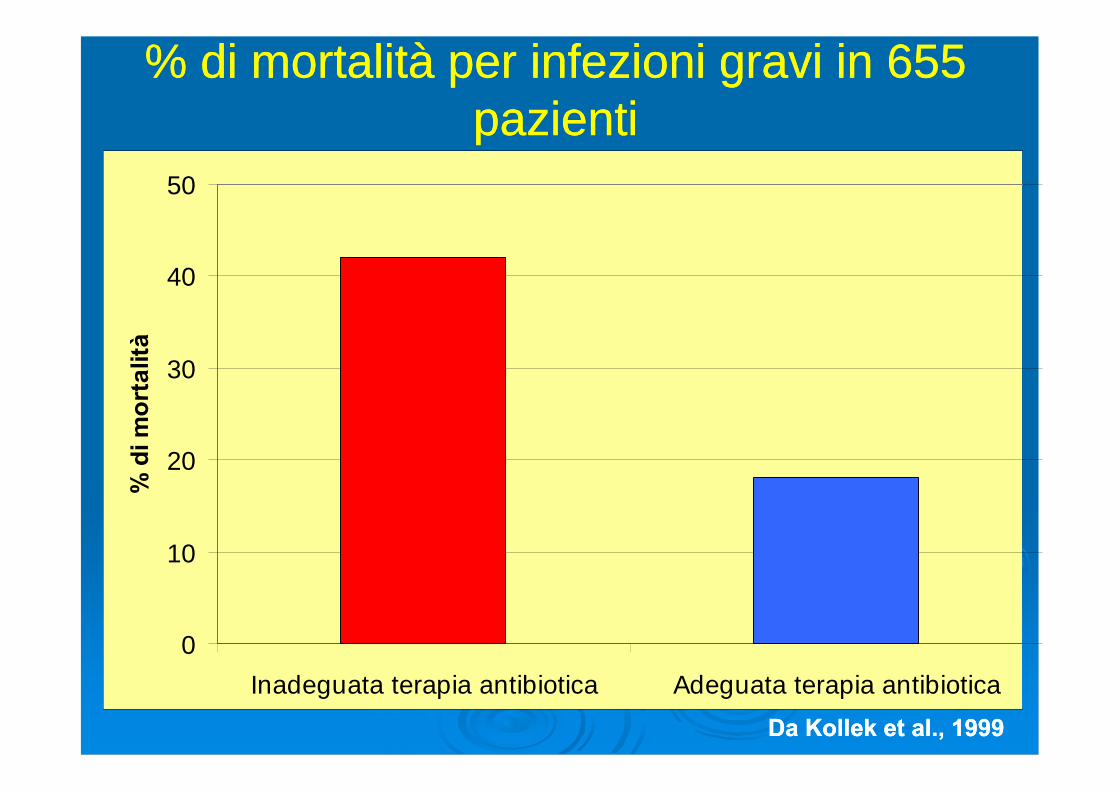
% di mortalità per infezioni gravi in 655% di mortalità per infezioni gravi in 655pazientipazienti
0
10
20
30
40
50
Inadeguata terapia antibiotica Adeguata terapia antibiotica
%d
imo
rtal
ità
Da Kollek et al., 1999Da Kollek et al., 1999
A total of 106 community-onset P. aeruginosa bacteraemia cases inthe ER were included (mean age, 57.61±14.44 years old; M:F,58:48).
Malignancy (n=83, 78.3%) was the most common underlyingdisorder.
The overall 30-day mortality rate was 26.4% (28/106).
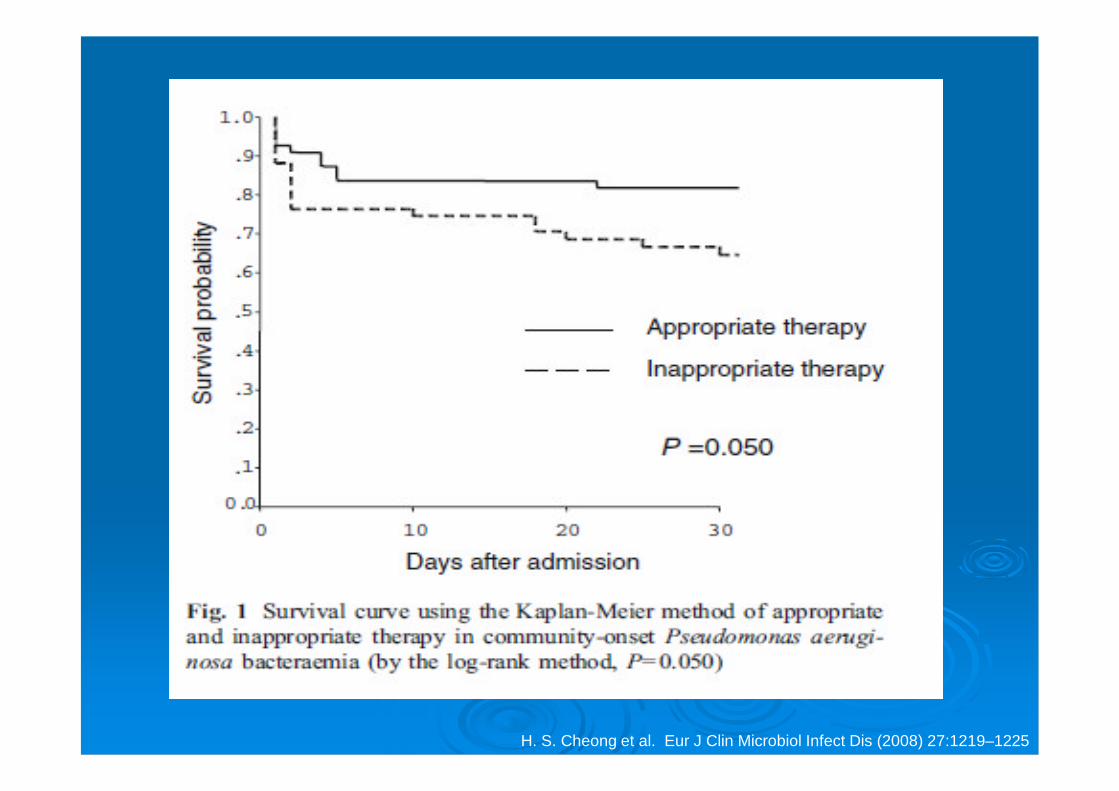
H. S. Cheong et al. Eur J Clin Microbiol Infect Dis (2008) 27:1219–1225
P. G. Davey and C. Marwick Clin Microbiol Infect 2008; 14 (Suppl. 3): 15–21
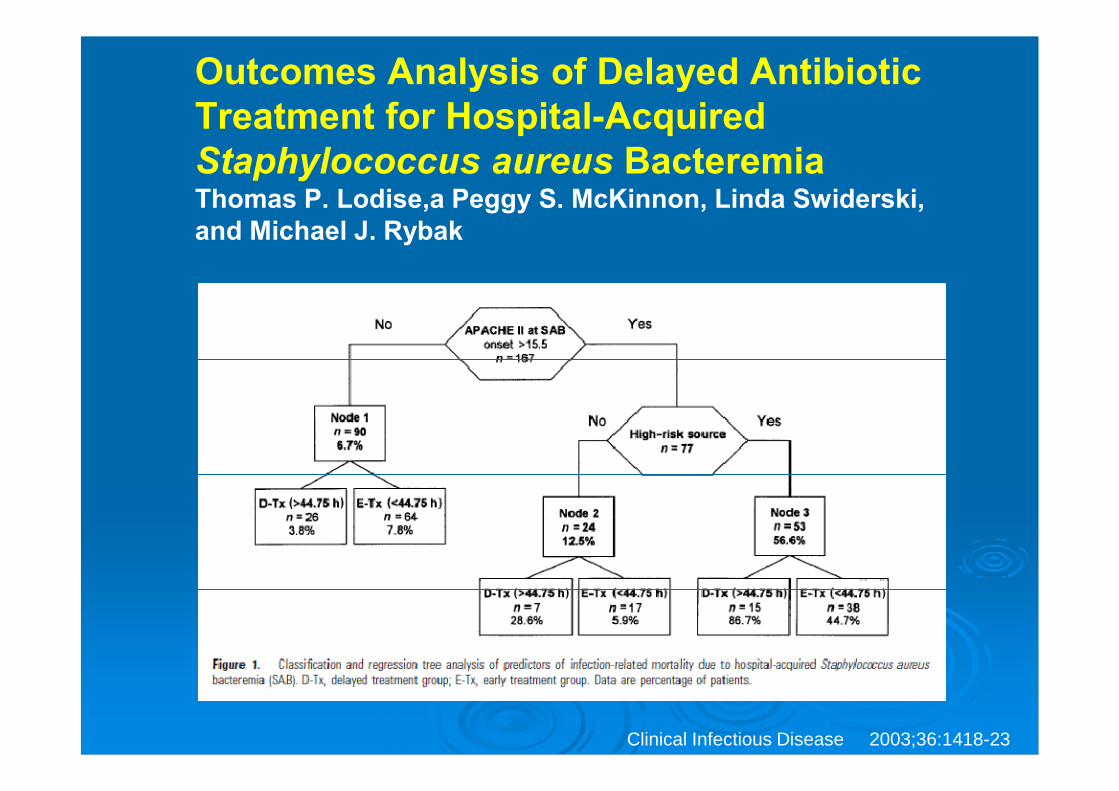
Outcomes Analysis of Delayed AntibioticTreatment for Hospital-AcquiredStaphylococcus aureus BacteremiaThomas P. Lodise,a Peggy S. McKinnon, Linda Swiderski,and Michael J. Rybak
Clinical Infectious Disease 2003;36:1418-23
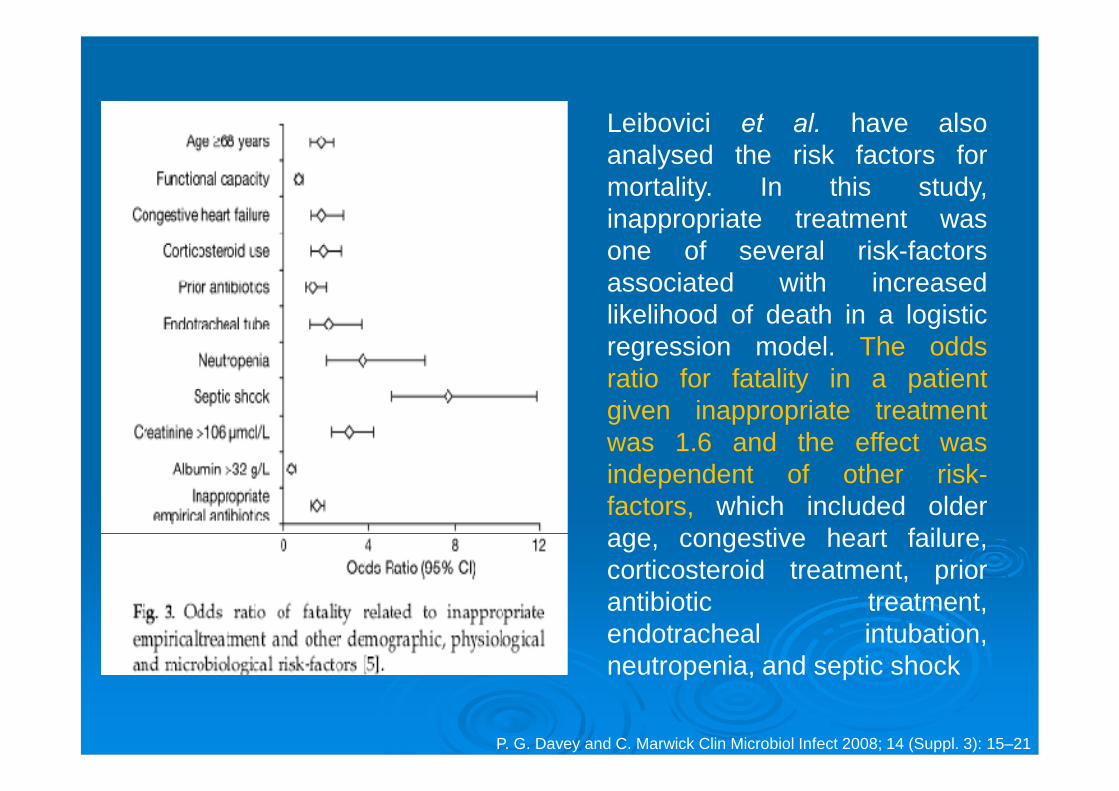
Leibovici et al. have alsoanalysed the risk factors formortality. In this study,inappropriate treatment wasone of several risk-factorsassociated with increasedlikelihood of death in a logisticregression model. The oddsratio for fatality in a patientgiven inappropriate treatmentwas 1.6 and the effect wasindependent of other risk-factors, which included olderage, congestive heart failure,corticosteroid treatment, priorantibiotic treatment,endotracheal intubation,neutropenia, and septic shock
P. G. Davey and C. Marwick Clin Microbiol Infect 2008; 14 (Suppl. 3): 15–21
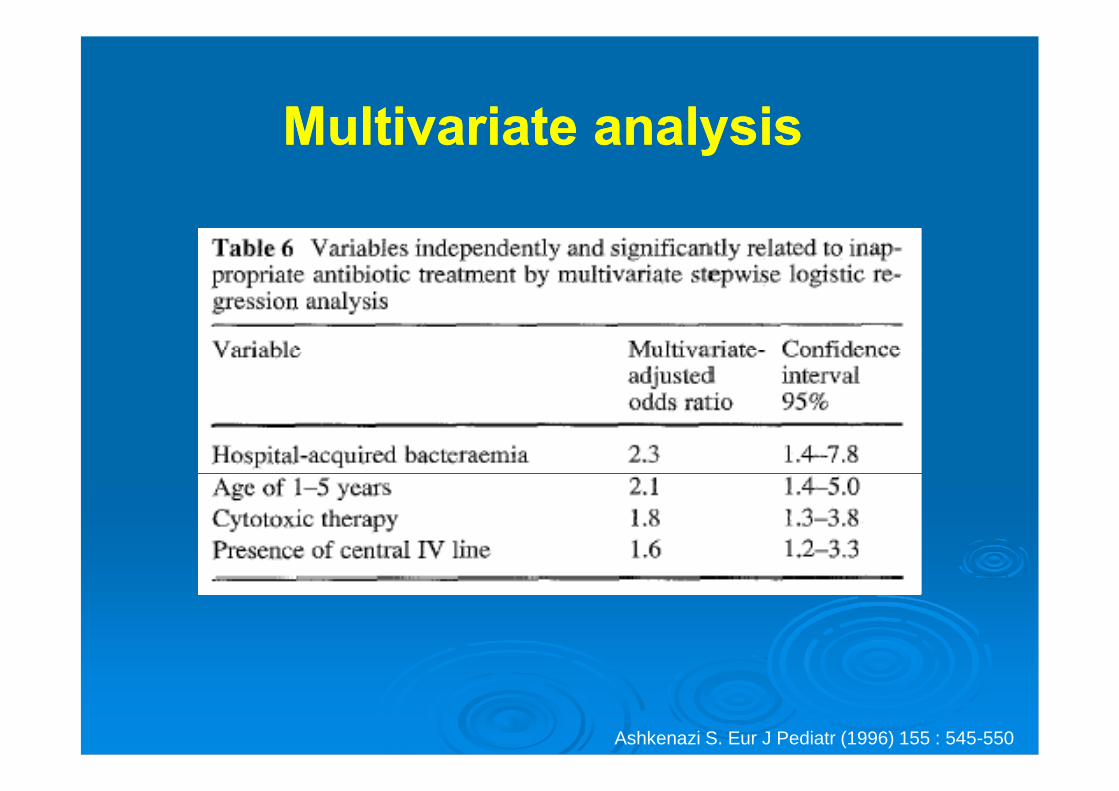
Multivariate analysisMultivariate analysis
Ashkenazi S. Eur J Pediatr (1996) 155 : 545-550
InIn--patients are at high risk of antibioticpatients are at high risk of antibiotic--resistant infectionsresistant infections
Misuse of antibiotics in hospitals is one of the main factors thatdrive development of antibiotic resistance.7-9
Patients in hospitals have a high probability of receiving anantibiotic10 and 50% of all antibiotic use in hospitals can beinappropriate.11-12
In a 2009 prevalence survey of antibiotic use in Irish hospitals: 34% of patients were receiving antibiotics on the day of the
survey 42% of antibiotic use did not follow evidence-based guidelines
7. Singh N et al. 2000, 117:1496-9.8. Lesch CA et al. 2001, 41:149-54.9. Lepper PM et al. 2002, 46:2920-5.10. Ansari F et al. 2009,49:1496-504.11. Davey P et al. 2005:CD003543.12. Willemsen I et al. 2007, 51:864-7.
Misuse of antibiotics drives antibioticMisuse of antibiotics drives antibioticresistanceresistance
Studies prove that misuse of antibiotics may cause patients tobecome colonised or infected with antibiotic-resistant bacteria,such as; Meticillin-resistant Staphylococcus aureus (MRSA) Vancomycin-resistant enterococci (VRE) Highly-resistant Gram-negative bacilli 13-14
• E.g. E. coli, Klebsiella sp., Pseudomonas sp. Misuse of antibiotics is also associated with an increased
incidence of Clostridium difficile infections.15-17
13. Safdar N et al. 2002, 136: 834-44.14. Tacconelli E et al. 2009, 53: 4264-9.15. Davey P et al. 2005, 15: CD003543.16. Carling P et al. 2003, 24: 699-706.17. Fowler S et al. 2007 59: 990-5.
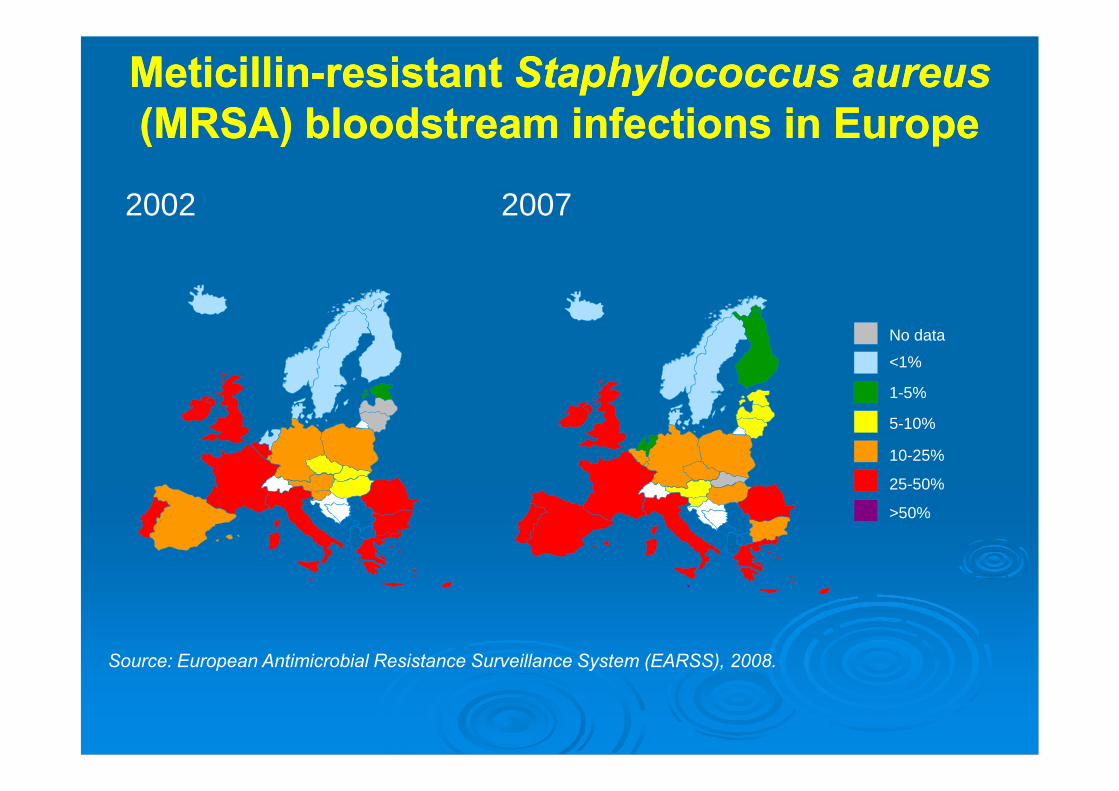
2002 2007
MeticillinMeticillin--resistantresistant Staphylococcus aureusStaphylococcus aureus(MRSA) bloodstream infections in Europe(MRSA) bloodstream infections in Europe
No data
<1%
1-5%
5-10%
10-25%
25-50%
>50%
Source: European Antimicrobial Resistance Surveillance System (EARSS), 2008.
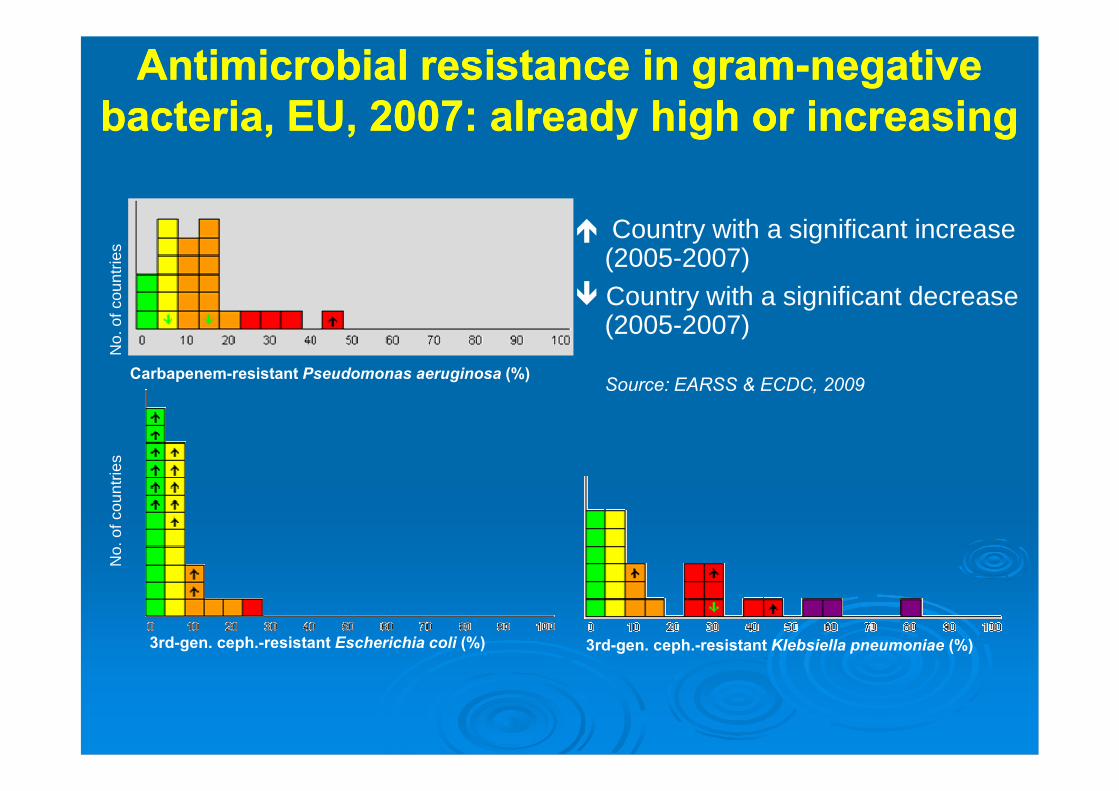
Antimicrobial resistance in gramAntimicrobial resistance in gram--negativenegativebacteria, EU, 2007: already high or increasingbacteria, EU, 2007: already high or increasing
Country with a significant increase(2005-2007)
Country with a significant decrease(2005-2007)
Carbapenem-resistant Pseudomonas aeruginosa (%)
3rd-gen. ceph.-resistant Klebsiella pneumoniae (%)3rd-gen. ceph.-resistant Escherichia coli (%)
Source: EARSS & ECDC, 2009
No.
ofco
untr
ies
No.
ofco
untr
ies
How prudent use of antibiotics canHow prudent use of antibiotics canbe promoted in hospitalsbe promoted in hospitals
–– the “how”the “how”
23
Lack of empirical coverage for microbiological agents insepsis is not uncommon. Institutional efforts are neededto improve the empirical use of antimicrobials for sepsisin the Emergency Department.
ConclusionsConclusions
De Miguel-Yanes JM et al. 2009, 2: 11-17
Multifaceted strategies can address and decreaseMultifaceted strategies can address and decreaseantibiotic resistance in hospitalsantibiotic resistance in hospitals
Antibiotic prescribing practices anddecreasing antibiotic resistancecan be addressed throughmultifaceted strategies including:29-31
Use of ongoing education Use of evidence-based
hospital antibiotic guidelinesand policies
Restrictive measures andconsultations frommicrobiologists, infectiousdisease physicians andpharmacists
29. Davey P et al. 2005: CD003543.30. Carling Pet al. 2003, 24: 699-706.31. Byl B et al. 1999, 29: 60-6.

Grazie per l’attenzione !
Why inappropriate use ofWhy inappropriate use ofantibiotics contributes toantibiotics contributes to
antibiotic resistanceantibiotic resistance–– the “why”the “why”
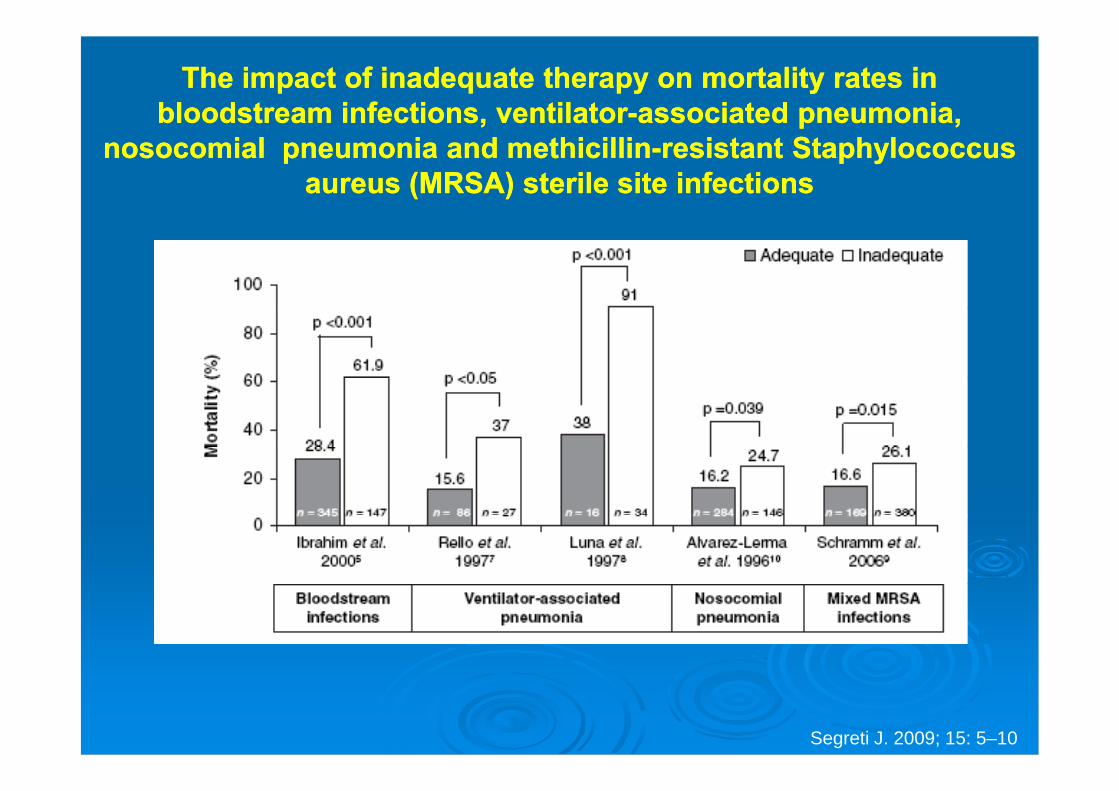
The impact of inadequate therapy on mortality rates inThe impact of inadequate therapy on mortality rates inbloodstream infections, ventilatorbloodstream infections, ventilator--associated pneumonia,associated pneumonia,
nosocomial pneumonia and methicillinnosocomial pneumonia and methicillin--resistant Staphylococcusresistant Staphylococcusaureus (MRSA) sterile site infectionsaureus (MRSA) sterile site infections
Segreti J. 2009; 15: 5–10
Emergenze acute infettivologiche nellaEmergenze acute infettivologiche nellapratica clinicapratica clinica
Le malattie infettive sono frequente causa di urgenzaLe malattie infettive sono frequente causa di urgenzanella pratica clinica.nella pratica clinica.
Alcune patologie di natura infettiva sono a rischioAlcune patologie di natura infettiva sono a rischioper la vita: per esempio la infezione meningococcica,per la vita: per esempio la infezione meningococcica,le infezioni batteriche in pazienti asplenici, lo shockle infezioni batteriche in pazienti asplenici, lo shocksetticosettico--tossico.tossico.
Queste condizioni di grave emergenza richiedonoQueste condizioni di grave emergenza richiedono
una terapia antibiotica empirica immediatauna terapia antibiotica empirica immediata..Ther Umsch 2005, 62, 351Ther Umsch 2005, 62, 351--77
Emergenze infettivologiche nel pazienteEmergenze infettivologiche nel pazienteoncologicooncologico
Terapia antibiotica empirica immediataTerapia antibiotica empirica immediata
Devono essere considerate emergenze infettivologiche leseguenti patologie: Meningiti Infezioni addominali Sepsi Polmonite
I pazienti con queste infezioni devono essere sottoposti aterapia a empirica immediata ed intensiva.
La scelta degli antibiotici sarà “ragionata”, perché terràconto del microrganismo più probabilmente implicato
The initiation of monotherapy with a third- or fourth-generationcephalosporin, or with a carbapenem antibiotic, is now established medicalpractice for the neutropenic patient who becomes febrile.
Empirical antimicrobial therapy, initiated with monotherapy and thenmodified based on the patient’s risk status, has become the standard ofcare and is associated with a survival rate of 95%.
For the moment, empirical monotherapy remains a standard of care for thecancer patient with fever and neutropenia.
Pizzo PA et al. 2009, 63 (Suppl. 1): i16–i17
Sepsis in the ED can safely be treated empirically with a
broad-spectrum beta-lactam antibiotic alone.
For most patients, the empiric addition of an aminoglycoside
will not significantly improve outcome but will increase the
risk of nephrotoxicity.
Local and regional ED early goal-directed therapy guidelines
should be revised to indicate this.
















![[ ] Park_2003_An empirica .doc](https://img.pdfslide.us/doc/110x75/55851a0ed8b42ae4748b463d/-park2003an-empirica-doc.jpg)
![[En] More Yo-yos pendulums ... Empirica STAR Report](https://img.pdfslide.us/doc/110x75/5591f9ee1a28abff658b45c9/enmore-yo-yos-pendulums-empirica-star-report.jpg)
![Corrientes Empirica y Racionalista [Autoguardado] (1)](https://img.pdfslide.us/doc/110x75/55cf8dfe550346703b8d7186/corrientes-empirica-y-racionalista-autoguardado-1.jpg)








![Nl Forecasting Report Empirica v3[1]](https://img.pdfslide.us/doc/110x75/577d35801a28ab3a6b909ca2/nl-forecasting-report-empirica-v31.jpg)
