Embed Size (px)
Citation preview

Tenecteplase for Treatment of Acute Ischemic Stroke
•Background on TNK
•Published studies of TNK in Stroke
•Ongoing studies of TNK in Stroke
•AHA/ASA Guidelines relative to TNK
•Mission and New Hanover experience
•Impact of the COVID pandemic on thrombolytic treatment of stroke
Alteplase
Tenecteplase
Andrew W. Asimos, MD
Medical Director, Carolinas Stroke Network
Atrium Health
Professor, Department of Emergency Medicine
Carolinas Medical Center
Charlotte, NC

Tenecteplase
•Third-generation, genetically modified version of rt-PA•Longer half life - given as a single bolus
•Greater fibrin specificity - theoretical advantage of reduced risk of hemorrhage
•Greater resistance to its endogenous inhibitor
•Workflow advantages, with potential time and money savings•Especially for interfacility transfer for thrombectomy
•Not FDA approved for use in stroke•Does not currently have a high LOR for acute stroke thrombolysis in the most recent AHA/ASA guideline

Two Published Meta-analyses of Tenecteplase versus Alteplasefor Management of Acute Ischemic Stroke

Tenecteplase versus Alteplase for Management of Acute Ischemic Stroke:Characteristics of the Included Randomized Clinical Trials
Kheiri, B. et al. J Thromb Thrombolysis 2018;46:440–450. https://doi.org/10.1007/s11239-018-1721-3

Tenecteplase versus Alteplase for Management of Acute Ischemic Stroke:Meta-analysis of Randomized Clinical Trials
Kheiri, B. et al. J Thromb Thrombolysis 2018;46:440–450. https://doi.org/10.1007/s11239-018-1721-3

Forest Plots of the Efficacy Outcomes: TNK vs Alteplase
Kheiri, B. et al. J Thromb Thrombolysis 2018;46:440–450. https://doi.org/10.1007/s11239-018-1721-3

Forest Plots of the Safety Outcomes: TNK vs Alteplase
Kheiri, B. et al. J Thromb Thrombolysis 2018;46:440–450. https://doi.org/10.1007/s11239-018-1721-3

Tenecteplase vs Alteplase
•Compared with alteplase, higher rates of recanalization and early neurological improvement with TNK
•TNK is not associated with significant differences in safety compared with alteplase
•TNK 0.25 mg/kg is associated with better imaging-based outcomes and higher levels of function than alteplase, with no increased risk of intracerebral bleeding or mortality
Kheiri, B. et al. J Thromb Thrombolysis 2018;46:440–450. https://doi.org/10.1007/s11239-018-1721-3

Campbell BCV et al. JAMA Published online February 20, 2020. doi:10.1001/jama.2020.1511

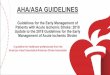
Distribution of 90-day mRS in pooled analysis of the EXTEND-IA TNK trials
Campbell BCV et al. JAMA Supplementary Online Content Published online February 20, 2020.
doi:10.1001/jama.2020.1511

TWIST ATTEST-2 TASTE-2 TIMELESS TEMPO-2 NORTEST-2 TASTEa
Countries Europe UK Australia US, Canada Multinational Norway Australia
Target Enroll # 500 1,870 1,124 456 1,124 1.342 80
% Target enrolled(as of 8/1/20)
100% ~49% ~42% ~38% ~37% ~1% ?
Time window ≤4.5 hrFrom
wake-up
≤4.5 hr ≤4.5 hr 4.5 - 24 hr ≤12 hr,NIHSS <6,
ASPECTS >7
≤4.5 hr from LKWor awakening,
NIHSS >5
≤4.5 hr,Tx in MSU
Imaging UECT UECT CTP/MRI CTP/MRI CTA/MRA/CTP/MRP
UECT,FLAIR-DWI
UECT
TNK dose(s) 0.25 vsstandard tx
0.25 vs tPA 0.25 vs tPA 0.25 vs placebo
0.25 vs antiplatelet*
0.40 vs tPA 0.25 vs tPA
LVO Not required ICA, M1, M2 MCA, ACA,PCA, VB
Allowed Not required
Endovascular Tx Prohibited Allowed Prohibited Allowed
Outcome mRS at 3 mo mRS at 3 mo mRS at 3 mo mRS at 3 mo mRS at 3 mo mRS at 3 mo CTP lesion vol
Ongoing Trials of TNK in Acute Ischemic Stroke
* Planned thrombolysis with IV tPA excluded