Upload
ari-ganesh
View
148
Download
6
Embed Size (px)
Citation preview
CONTINUING
MEDICAL EDUCATION
Toxic epidermal necrolysisFrederick A. Pereira, MD,a,b Adarsh Vijay Mudgil, MD,a and David M. Rosmarin, MDc New York, New YorkToxic epidermal necrolysis (TEN) is an unpredictable, life-threatening drug reaction associated with a 30% mortality. Massive keratinocyte apoptosis is the hallmark of TEN. Cytotoxic T lymphocytes appear to be the main effector cells and there is experimental evidence for involvement of both the Fas-Fas ligand and perforin/granzyme pathways. Optimal treatment for these patients remains to be claried. Discontinuation of the offending drug and prompt referral to a burn unit are generally agreed upon steps. Beyond that, however, considerable controversy exists. Evidence both pro and con exists for the use of IVIG, systemic corticosteroid, and other measures. There is also evidence suggesting that combination therapies may be of value. All the clinical data, however, is anecdotal or based on observational or retrospective studies. Denitive answers are not yet available. Given the rarity of TEN and the large number of patients required for a study to be statistically meaningful, placebo controlled trials are logistically difcult to accomplish. The absence of an animal model further hampers research into this condition. This article reviews recent data concerning clinical presentation, pathogenesis and treatment of TEN. (J Am Acad Dermatol 2007;56:181-200.) Learning objectives: At the conclusion of this learning activity, participants should have acquired a more comprehensive knowledge of our current understanding of the classication, clinical presentation, etiology, pathophysiology, prognosis, and treatment of TEN.
INTRODUCTIONThe majority of adverse cutaneous reactions to medications are benign and transient. A rare few, however, are serious and potentially life-threatening. The most important of these are StevenseJohnson syndrome/toxic epidermal necrolysis (SJS/TEN) and drug hypersensitivity syndrome (DHS), also known as drug rash with eosinophilia and systemic symptoms (DRESS). This review will focus on SJS/TEN, but occasional reference will be made to DHS.
CLINICAL ASPECTS OF SJS/TENTEN is heralded by the abrupt onset of fever; systemic toxicity; a generalized, dusky, erythematous rash; bullae; separation of large sheets of
From the Departments of Dermatology, Mount Sinai School of Medicinea and New York Medical College,b and the Department of Medicine,c College of Physicians and Surgeons, Columbia University. Dr Rosmarin is currently affiliated with the Department of Dermatology, Boston University School of Medicine and the Department of Dermatology, Tufts University School of Medicine, New England Medical Center, Boston, Massachusetts. Funding sources: None. Conflicts of interest: None identified. Reprint requests: Frederick A. Pereira, MD, 51-14 Kissena Blvd, Flushing, NY 11355-4163. E-mail: [email protected]. 0190-9622/$32.00 2007 by the American Academy of Dermatology, Inc. doi:10.1016/j.jaad.2006.04.048
epidermis from the dermis; purulent conjunctivitis; and mucositis of the mouth and genital area. Mucositis generally precedes skin lesions by a few days.1 The skin is painful to touch, and any shearing force will cause the involved epidermis to slide off the dermis. Progression of skin lesions is variable. In one out of seven patients, massive necrolysis involving the entire skin surface can occur within 24 hours; but in most, lesions erupt over a period of two to fifteen days. In severe cases, necrolysis has been observed to occur in areas of reepithelialization.2 Even in extensive disease, the hairy portion of the scalp is generally not affected.3 Anemia and lymphopenia are common, but the presence of neutropenia portends a poor prognosis (Figs 1 to 4).4 Inammation of internal mucosal surfaces, such as the gastrointestinal and respiratory tracts, commonly occurs in TEN.5 Internal involvement may be caused by the release of massive amounts of proinflammatory cytokines into the systemic circulation.6 Involvement of respiratory mucosa is insidious, and serious pulmonary disease can be seen with a normal chest radiograph. Clinical clues include dyspnea, tachypnea, and hypoxemia.7 The patient with TEN is a very ill individual suffering from acute skin failure. The condition can be associated with major metabolic abnormalities, sepsis, multiorgan failure, pulmonary embolism and gastrointestinal hemorrhage.2,8 The overall mortality rate of TEN is approximately 30%.9 181
182 Pereira, Mudgil, and Rosmarin
J AM ACAD DERMATOLFEBRUARY 2007
Abbreviations used: acute generalized exanthematous pustulosis AGVHD: acute graft-versus-host disease CLA: cutaneous lymphocyte antigen CTL: cytotoxic T lymphocyte CYP: cytochrome P DHS: drug hypersensitivity syndrome DIF: direct immunofluorescence DR: death receptor DRESS: drug rash with eosinophilia and systemic symptoms EGTA: ethylene glycol bis (2-aminoethylether)N,N,N,9 N9 -tetraacetic acid EM: erythema multiforme FADD: Fas-associated death domain protein FasL: Fas-Fas ligand HLA: human leukocyte antigen IL: interleukin IVIG: intravenous immune globulin KAR: killer activating receptor KIR: killer inhibitory receptor MP: metalloproteinase PBMC: peripheral blood mononuclear cell PCR: polymerase chain reaction PNP: paraneoplastic pemphigus rhsFasL: recombinant human sFasL sIL-2R: soluble IL-2 receptor SJS: StevenseJohnson syndrome sFasL: soluble FasL SSSS: staphylococcal scalded skin syndrome TEN: toxic epidermal necrolysis TNF: tumor necrosis factor TRAIL: TNF-related apoptosis-inducing ligand UVB: ultraviolet B AGEP:
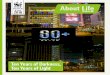
Fig 1. Patient with advanced HIV disease developed TEN approximately 4 weeks after the institution of phenytoin therapy for the prevention of seizures. Extensive, painful erosions are present on the trunk and extremities. The patient died from overwhelming sepsis a few days after the onset of skin lesions.
In the absence of infection or active disease, healing of the skin occurs in a few days. In areas of pressure or in macerated intertriginous areas, healing may take up to two weeks. The healing of mucosal surfaces is especially slow, and lesions of the glans penis may persist for up to two months.2 Skin sequelae include vaginal, urethral, and anal strictures; loss of nails; scarring; and pigmentation abnormalities. Hypopigmentation is more common than hyperpigmentation. Hyperpigmentation secondary to TEN has been successfully treated with pulsed light treatments.10 Vulvovaginal involvement can result in stenosis and dyspareunia.11-13 Vulvar adenosis, the abnormal presence of mucinous and/or tuboendometrial epithelium in the labia minora, has been reported to follow both SJS and TEN.14-17 This condition tends to occur in young women, and it can present several years after the episode of disease. The clinical presentation is that of tender, erosive, hemorrhagic lesions. In men, phimosis is a common complication.2 The most serious sequelae relate to the eye. In all cases of SJS/TEN, early ophthalmologic consultation is advised. Synechiae, corneal ulcers, xerophthalmia, symblepharon, Meibomian gland dysfunction,
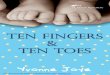
Fig 2. Photo of a 72-year-old male patient who developed TEN in 1970. Allopurinol was the causative drug. Note the typical dusky erythema. The white material on the scrotum is silver sulfadiazine cream. His treatment, which would not meet todays standard of care, consisted of prednisone 80 mg/day, massive doses of multiple antibiotics, and measures to relieve pain. He was not admitted to a burn unit. The patient died of sepsis and multiorgan failure.
panopthalmitis, and blindness are all potential complications.18 In the original paper by Stevens and Johnson, one of the two children reported was left permanently blind.19 The most common ocular sequelae are photophobia, dryness, and a foreign body sensation.2 Some patients experience decreased salivary flow after a bout of TEN, and lip biopsies have shown lymphocytic infiltration around minor salivary glands.2,20 Over the long term, survivors of TEN function well in activities of daily living; however, the cutaneous and ophthalmologic sequelae impair quality of life.21 SJS and TEN belong to a spectrum of reactive disorders: SJS lies at one end and TEN at the other. Several classication systems exist, but the most widely accepted, formulated by Bastuji-Garin et al,22 divides the spectrum into five categories: (1) Bullous erythema multiforme (EM): epidermal detachment involving\10% of the body surface,
J AM ACAD DERMATOLVOLUME 56, NUMBER 2
Pereira, Mudgil, and Rosmarin 183
Fig 4. Same patient shown in Figs 2 and 3. A large erosion is present on the elbow. At the periphery of the erosion, the epidermis is parchment-like, peeling, and necrotic. Areas of friction and trauma are common sites of erosion in TEN.
Fig 3. Same patient shown in Fig 2. Note the dusky erythema, crusting, and extensive erosions on the neck and face. Hair thinning was secondary to chemotherapy, not TEN. Silver sulfadiazine cream is also present.
(2)
(3)
(4)
(5)
coupled with localized typical targets or raised atypical targets SJS: epidermal detachment of \ 10% of the body surface in association with widespread erythematous or purpuric macules or flat atypical targets SJS/TEN overlap: epidermal detachment of 10% to 30% of the body surface plus widespread purpuric macules or flat atypical targets TEN with spots: epidermal detachment of [ 30% of the body surface coupled with widespread purpuric macules or flat atypical targets TEN without spots: large sheets of epidermal detachment involving [ 10% of the body surface without purpuric macules or target lesions
EM, as originally described by von Hebra in 1862 (category 1 of the BastujieGarin classication) is now considered a different disease than SJS/TEN.23 EM is characterized by the appearance of typical or raised atypical target lesions, distributed acrally. Mucositis generally involves only the oral mucosa, though rarely two sites can be affected. EM occurs predominantly in young, healthy people, particularly males, and the condition is characterized by mild clinical course and frequent recurrences. Polymerase chain reaction (PCR) assays will reveal the DNA of herpes simplex virus in lesional skin of a majority of patients with EM, and skin lesions are positive for interferon gamma.24,25
SJS/TEN by contrast is a more severe disease. Patients are febrile and prostrated by illness. It is usually caused by medications. The distribution of skin lesions is predominantly central with involvement of at least two mucosal sites. Lesions consist of widespread, at atypical targets or purpuric macules, and tumor necrosis factor (TNF)ea can be detected in skin lesions. SJS occurs predominantly in children and adolescents, whereas TEN occurs in all ages, from premature infants to the frail elderly.26 The incidence of TEN and drug reactions generally is 2.7 times higher in the elderly than in younger populations, and mortality from TEN is twice as high in elderly patients (51%) than in younger patients (25%).27 SJS/TEN is rare. The incidence among Europeans of both SJS and TEN is approximately two patients per million people per year.28 However, a recent South Indian study of 404 patients with adverse cutaneous drug reactions showed a much higher incidence (19.5%).29 The incidence of TEN and drug reactions generally is higher in HIV-infected patients, particularly those with advanced disease. In the year 2000, a mathematical tool called SCORTEN was developed to assess severity of illness and predict mortality.30 SCORTEN should be computed within the first 24 hours after admission and again on day three.31 The score is the sum of seven easily measured clinical variables: (1) age over 40 years; (2) heart rate [ 120 beats per minute; (3) the presence of cancer or hematologic malignancy; (4) epidermal detachment involving body surface area [10% on day one; (5) blood urea nitrogen[28 mg/dL (10 mmol/L); (6) glucose [ 252 mg/dL (14 mmol/L); and (7) bicarbonate \ 20 mEq/L. One point is given for each variable, and the mortality increases sharply with each additional point (Table I). SCORTEN has proven to be remarkably accurate in predicting mortality. Other clinical parameters that
184 Pereira, Mudgil, and Rosmarin
J AM ACAD DERMATOLFEBRUARY 2007
Table I. SCORTEN level and predicted mortalitySCORTEN Mortality
0-1 2 3 4 5 or greater
3.2% 12.1% 35.3% 58.3% 90.0%
are reported to be predictive of mortality include thrombocytopenia, leukopenia, delay in hospital admission, and treatment with antibiotics or corticosteroids prior to admission.32,33 SJS/TEN virtually always represents an idiosyncratic reaction to medication, but there are exceptions. The condition has followed vaccinations, such as measles, mumps, and rubella, and exposure to industrial chemicals and fumigants.34-37 Infection with Mycoplasma pneumoniae is a known cause of SJS, and a few cases of TEN have been reported to complicate infection with this agent.38-41 For all practical purposes, though, drugs are the main cause.42 More than 220 medications have been implicated, but the major offenders are sulfonamide antibiotics, particularly trimethoprim/sulfamethoxazole; aromatic anticonvulsants such as phenytoin, phenobarbital, and carbamazapine; beta-lactam antibiotics; nevirapine; abacavir; nonsteroidal antiinflammatory drugs, particularly the oxicams; allopurinol; lamotrigine; tetracyclines; and quinolones, especially ciprofloxacin.43-46 In Asian populations, carbamazapine, phenytoin, and allopurinol are particularly common causes.47 TEN has followed topical intranasal application of mupirocin.48 It has also occurred in patients who have ingested natural medications and traditional Chinese herbal medications.49-51 Pseudoephedrine, a common ingredient in over-the-counter cold remedies and decongestants, can cause TEN.52 The period of greatest risk for developing SJS/TEN is in the first two months of treatment.4 Two case of TEN have been reported in which the bullae and erosions occurred in sun-exposed areas.53,54 These patients presented with typical features of fever, mucositis, and erosions, but the erosions were limited to light-exposed skin. Subsequent photopatch tests were negative. It was hypothesized that ultraviolet B (UVB) radiation induced the secretion of TNF-a and interleukin (IL)-1 by keratinocytes, which in turn enhanced the expression of adhesion molecules, such as intercellular adhesion molecule-1. Activated cytotoxic T lymphocytes (CTLs) then localized to the UVBexposed areas triggering apoptosis of keratinocytes. Thus, UVB did not precipitate TEN per se, but rather
it accelerated the pathogenetic mechanisms responsible for the disorder. If someone experiences TEN to one class of medication, such as sulfonamide antibiotics, that patient is not at higher risk for developing TEN to medications of a different chemical class, such as tetracyclines. However, cross reactivity resulting in TEN can occur within different classes of beta-lactam antibiotics, such as penicillins and cephalosporins.55 A reaction to sulfonamide antibiotics does not mean sensitivity to sulfonamide nonantibiotic drugs, such as thiazide diuretics, sufonylureas, furosemide, or cyclooxygenase-2 inhibitors. All of these medications have a sulfonamide moiety, but only sulfonamide antibiotics have an arylamine group at the N4 position. The arylamine is oxidized to a hydroxylamine by hepatic cytochrome P-450 enzymes, and further oxidation of the hydroxylamine will result in the highly reactive nitroso product.56 The aromatic anticonvulsants carbamazepine, phenytoin, and phenobarbital are major causes of TEN, and the three cross react with one another. The risk of TEN is highest in the rst 8 weeks of antiepileptic therapy, and it is ten times higher in patients who have been previously treated with anti-epileptic medication.57 In new users of antiepileptic medications, Mockenhaupt et al58 determined that more than 90% of SJS/TEN cases occurred in the first 63 days of therapy, and the overall risk of a serious cutaneous adverse reaction was estimated to be in the range of 1 to 10 per 10,000 new users.58 Patients undergoing radiation therapy for brain tumors appear to be particularly susceptible to SJS/TEN when given phenytoin.59-61
HISTOPATHOLOGY AND DIFFERENTIAL DIAGNOSISThe diagnosis of TEN is conrmed by histopathologic analysis of lesional tissue. Early lesions demonstrate scattered necrotic keratinocytes in the epidermis (Fig 5). Late stage lesions reveal confluent full-thickness epidermal necrosis, which eventuates in the formation of subepidermal bullae.62 Classically, the dermal inltrate of TEN has been described as sparse. Recently, however, Quinn et al63 demonstrated a range of dermal mononuclear cell infiltration from sparse to dense. Furthermore, the density of the infiltrate correlates with severity of disease.63 In a study of 37 patients, an extensive mononuclear cell infiltrate was associated with a 71% death rate, a moderate infiltrate was associated with a 53% death rate, and a sparse infiltrate was associated with a 27% death rate. Quantification of dermal mononuclear cell infiltration is almost as accurate in predicting outcome as SCORTEN.63 This
J AM ACAD DERMATOLVOLUME 56, NUMBER 2
Pereira, Mudgil, and Rosmarin 185
study also underscores the fact that TEN is a T celle mediated disorder.6 To expedite diagnosis, two biopsy specimens should be taken from patients with suspected TEN: one for routine, formalin-xed hematoxylin and eosin processing, and the other for immediate frozen section. Epidermis must be present to make the diagnosis, as epidermal necrosis is the pathognomonic nding in this entity.64 Although the clinical presentation and patient history usually make the diagnosis of TEN obvious, other conditions should be considered in the differential diagnosis, particularly in the early stages of disease when the full-blown picture may not be fully apparent. It is important that a skin biopsy be performed early on, because specic and effective treatments are available for the other disorders that can clinically resemble TEN.65 These simulators of TEN include: staphylococcal scalded skin syndrome (SSSS); linear IgA dermatosis; paraneoplastic pemphigus (PNP); acute graft-versus-host disease (AGVHD); drug-induced pemphigoid and pemphigus; and acute generalized exanthematous pustulosis (AGEP). See Table II. Although SSSS is predominantly a pediatric disease involving infants and children younger than 5 years of age, it also occurs in adults, particularly those who are immunosuppressed or on dialysis.66 SSSS is caused by epidermolytic toxins produced by toxin-producing strains of Staphylococcus aureus. The toxins cause superficial intraepidermal blistering at the level of the epidermal granular layer.67 Patients present with fever, erythema, and painful skin, followed by the development of blistering, typically accentuated in areas of friction and around body orifices. SSSS follows local or systemic staphylococcal infection, but preceding infection is not always detected.68,69 Unlike TEN, the exfoliation in SSSS is generally not clinically dangerous as the blistering occurs in a superficial plane and healing is rapid. Importantly, there is no mucosal involvement in SSSS, whereas in TEN mucositis is a prominent feature. Histologically, SSSS shows a superficial blister through the granular layer, without necrosis or inflammation.70 Drug-induced linear IgA bullous dermatosis can produce an extensive bullous eruption that can closely resemble SJS/TEN.71 The disease appears suddenly with the appearance of EM-like lesions, pruritic urticarial plaques, and tense bullae on the trunk and limbs. Mucosal lesions are rare in druginduced disease.72 Vancomycin is the most commonly implicated drug; however, numerous other drugs can cause this eruption. Vancomycin itself has been reported to induce TEN.73 Direct
Fig 5. Epidermis shows conuent necrosis and separation from the dermis. Within the dermis there is a sparse inltrate consisting mainly of lymphocytes. Note the reepithelialization occurring as the necrotic keratinocytes are shed. (Hematoxylin-eosin stain; original magnication: 320.)
immunofluorescence (DIF) will show linear deposition of IgA at the basement membrane zone. Upon discontinuation of the causative drug, lesions will resolve in the absence of specific therapy.74 PNP, rst described in 1990 in a classic article by Anhalt et al,75 presents with severe and intractable oral mucosistis coupled with a generalized, polymorphous blistering eruption in association with an occult or overt malignancy, particularly lymphoma and Castlemans disease (angiofollicular lymph node hyperplasia).75,76 Conjunctivitis is common, and respiratory and gastrointestinal mucosal surfaces can be involved. Several clinical and histologic features differentiate PNP from TEN. TEN has an abrupt onset and rapid course, whereas PNP is insidious in onset, chronic in course, and notoriously resistant to all forms of treatment. The lesions in PNP may be polymorphous, even in the same patient. For example, lichenoid lesions may be present alongside bullous lesions.77 The lesions of TEN are monomorphous. Acantholysis, a cardinal feature of PNP, is not seen in TEN; and DIF is positive in PNP, but negative in TEN. AGVHD shares many of the same clinical, pathologic, and immunologic features as TEN.78 Additionally, bone marrow-transplant patients frequently receive medications known to incite TEN, and high-dose, chemotherapy-induced neutropenia can cause oral mucositis. AGVHD generally occurs about four weeks after stem cell transplantation. Patients describe a sensation of skin pain or itching, followed by a morbilliform rash.79 In severe cases, the eruption becomes generalized with widespread areas of epidermal necrosis and denudation. The early exanthem of AGVHD has a folliculocentric distribution, and folliculotropic inammation
186 Pereira, Mudgil, and Rosmarin
J AM ACAD DERMATOLFEBRUARY 2007
Table II. Differential diagnosis of TENBullous disease Fever Mucositis Morphology IF Onset Miscellaneous features
Drug-induced pemphigoid Staphylococcal scalded skin syndrome Drug-induced pemphigus Drug-triggered pemphigus
No Yes
Rare Absent
Tense bullae (sometimes 1 Acute hemorrhagic) Erythema, skin tenderness, e Acute periorificial crusting Erosions, crusts, patchy erythema (resembles pemphigus foliaceous) Mucosal erosions, flaccid bullae
No
Usually absent Present
No
Paraneoplastic pemphigus Acute graft-versushost disease Acute generalized exanthematous pustulosis Drug-induced linear IgA bullous dermatosis
No
Yes Yes
No
Polymorphous skin Present lesions, flaccid bullae (usually severe) Present Morbilliform rash, bullae and erosions Rare Superficial pustules (resembles pustular psoriasis) Rare Tense, subepidermal bullae (resembles pemphigoid)
Diuretics a common cause, especially spironolactone; often pruritic Affects children under 5, adults on dialysis, and those on immunosuppressive therapy 6 Gradual Commonly caused by penicillamine and other thiol drugs; resolves after inciting agent is discontinued 1 Gradual Caused by non-thiol drugs; persists after discontinuation of drug; may require long-term immunosuppressive therapy 1 Gradual Resistant to treatment; associated with malignancy, especially lymphoma e Acute Closely resembles TEN Self-limiting on discontinuation of drug Vancomycin most commonly implicated drug; pruritus often present
e Acute
1 Acute
is also seen pathologically.80 Additionally, TEN usually begins on the trunk and spreads distally, whereas AGVHD frequently begins acrally and spreads proximally. Though subtle, these features may help differentiate the two. Drug-associated pemphigus is rare, but the condition may be more common than realized. A distinction must be made between drug-induced pemphigus and idiopathic pemphigus vulgaris triggered by a drug in genetically predisposed individuals. Drugs containing sulfhydryl (thiol) groups, such as penicillamine, are the most common causes of drug-induced pemphigus. These drugs appear to interact directly with epidermis.81 In vitro, penicillamine can induce acantholysis in the absence of antibody, and in vivo, this biochemical mechanism may be operative.82 DIF may or may not be positive. The clinical picture of penicillamine-induced pemphigus resembles that of pemphigus foliaceus, and discontinuation of drug will usually result in clearing of the eruption. Non-thiol drugs, such as rifampin, can cause a disease indistinguishable from idiopathic pemphigus vulgaris (drug-triggered pemphigus). These drugs may impair the function of suppressor T-cells, resulting in the proliferation of forbidden B-cell clones and production of autoantibodies.83 DIF is positive. Discontinuation of the drug usually does
not cause resolution of disease, and long-term immunosuppressive therapy is needed. In contradistinction to TEN, pemphigus caused by drugs is a chronic illness. Mucosal lesions may or may not be present depending upon the clinical variant of pemphigus caused by the drug. A number of medications are known to induce bullous pemphigoid, but the most common are diuretics, particularly furosemide and spironolactone.84 Drugs should be especially suspect if pemphigoid occurs in young patients.85 Drug-induced pemphigoid is characterized by the sudden appearance of hive-like erythema and large, tense bullae. Unlike TEN, mucosal lesions are generally absent, the patient is afebrile, and direct immunofluorescence is positive, showing IgG and/or C3 in the basememt membrane zone. AGEP also bears similarities to TEN. AGEP is usually seen as a reaction pattern to antimicrobials.86 Patients with AGEP are febrile. The typical clinical course is characterized by the development of generalized erythema with subsequent sterile pustule formation, often with accentuation in flexural areas. In early stages, this condition resembles pustular psoriasis; as the disorder progresses, widespread erosions mimicking TEN can develop.87 Mucositis is very rare in AGEP.88 Most cases resolve spontaneously upon discontinuation of drug.
J AM ACAD DERMATOLVOLUME 56, NUMBER 2
Pereira, Mudgil, and Rosmarin 187
GENETIC FACTORS AND PREDICTION OF RISKDrug reactions in general and SJS/TEN in particular have a genetic component. In a study of 44 patients surviving TEN, a small, but statistically signicant increase in the human leukocyte antigen (HLA)-B12 phenotype was observed.89 Among Han Chinese, a strong association exists between HLA-B*1502 and carbamazapine-induced SJS/TEN.90 HLA-B*1502 was present in 100% of patients experiencing SJS, but in only 3% of carbamazapinetolerant patients, and in 8.6% of the population at large. Similarly, the HLA-B*5801 allele was present in 100% of 51 Han Chinese patients experiencing severe cutaneous reactions to allopurinol, but it was present in only 15% of 135 tolerant patients.91 Two studies have shown an association between HLAB*5701 and hypersensitivity reactions to abacavir.92,93 The combination of HLA-B*5701, HLA-DR7, and HLA-DQ3 is 100% predictive of a hypersensitivity reaction to abacavir. At the present time, HLA testing is prohibitively expensive for routine screening.94 Unfortunately, there is currently no reliable, safe, and easily available test that can predict life-threatening drug reactions such as TEN or DHS. A DNA microarray analyzing polymorphisms in genes coding for CYP2D6, which metabolizes antidepressants, antipsychotics, and beta-blockers, has recently been developed. Future renement of this technology to include other genes may allow physicians to identify those at risk. Patch testing has been attempted, but the results are unreliable, particularly with respect to TEN.95 The lymphocyte cytotoxicity assay is an in vitro test designed to measure activity of detoxification enzymes. This assay is not readily available for general clinical use, and it remains basically a research tool.96 Provocation tests using small doses of a given drug are potentially dangerous and should be undertaken only by experienced personnel equipped to handle emergencies.97 Inquiry into family history remains the easiest and most important step a clinician can take in assessing risk. If a rst-degree relative has experienced a serious drug reaction to a particular medication, that patient is also at risk. Likewise, family members of SJS/TEN patients should be counseled to avoid an implicated drug.
IMMUNOPATHOGENESISPatients who have had TEN or DHS can develop a second case within hours should they be inadvertently reexposed to the offending drug. This rapid anamnestic response is consistent with an immunologic mechanism. TEN is considered a T cellemediated disorder. There is little evidence
implicating the B cell arm of the immune system in the pathogenesis of TEN. Cytotoxic antibodies, immune complexes, complement activation, and deposits of immune reactants in skin are rarely found. The occasional C3 and IgG, sometimes seen on DIF at the dermal-epidermal junction and around small blood vessels, is considered a nonspecic nding, probably related to exudation.98 A number of studies analyzing live immune cells from blister uid of TEN patients have found T lymphocytes to be the predominant cell type. In early stages of disease, there are mainly CD81 lymphocytes in blister fluid and epidermis, and CD41 lymphocytes in the dermis.99 The finding of CD81 lymphocytes is unusual because in most allergic reactions involving the epidermis, CD41 lymphocytes are the predominant cell type.100 Monocytes are also present in the epidermis of TEN patients, and in later stages of the disease there is a relative decrease in lymphocytes and increase in monocytes. Additional evidence supporting the role of cytotoxic T lymphocytes in the pathogenesis of TEN is the observation that high levels of soluble IL-2 receptor (sIL-2R) are present in blister uid and serum of TEN patients. sIL-2R is a marker for activated T cells, and levels mirror disease activity.101 In addition, it has also been shown that the numbers of activated T lymphocytes expressing the skin homing receptor, cutaneous lymphocyte antigen (CLA), are elevated in the peripheral blood of TEN patients. The elevation correlates with disease activity and returns to normal upon resolution of the condition.102 Further characterization of the CD81 T cells in the epidermis of TEN patients shows that a majority of these also show markers of NK cells, namely killer inhibitory receptor and killer activating receptor (KIR/KAR).103 CD56 (neural cell adhesion molecule [NCAM]), a marker for NK cells and highly cytotoxic CD81 cells, has also been identified on a high percentage of CD81 lymphocytes in blister fluid.104 These findings all support the hypothesis that cytotoxic T lymphocytes are major effector cells in early lesions of TEN. However, they may not be the only immune cells involved in the pathogenesis. Whereas examination of blister uid cells shows mainly lymphocytes, immunohistochemical staining of skin biopsies from TEN patients shows a different picture, namely a predominance of cells of the monocyte-macrophage lineage, a paucity of CD4 and CD8 cells, and high levels of TNF-a.98 In one such study involving 23 TEN patients, Paquet et al105 showed that MAC 3871 macrophages were the most numerous cells in the epidermis, and factor XIIIa1 dendritic cells were abundant in the dermis. MAC
188 Pereira, Mudgil, and Rosmarin
J AM ACAD DERMATOLFEBRUARY 2007
387 is a monoclonal antibody that recognizes a cytoplasmic antigen expressed by monocytes and macrophages.106 Factor XIIIa1 dendritic cells, otherwise known as dermal dendrocytes, are capable of phagocytosis and antigen presentation. Factor XIIIa1 dendritic cells are increased in a variety of skin disorders, such as psoriasis and atopic dermatitis, and they may also be involved with tissue repair.107,108 The authors suggest that TEN is not a disease involving T cells alone. Macrophages play a significant role, and TNF-a is a major cytokine.98 Cytotoxic T lymphocytes kill other cells by inducing apoptosis, a type of cell death by which the cell dies from within. During apoptosis, there is degradation of chromatin, blebbing of the cell membrane, shrinkage, and death of the cell. Cell remnants are phagocytized by nearby macrophages. Apoptosis is an immunologically silent process that does not trigger an inammatory response. It also occurs very rapidly. When cytotoxic T lymphocytes come into contact with target cells, the biochemical reactions leading to cell death, namely activation of a cascade of intracellular enzymes called caspases, are set into motion quickly. In vitro, it has been shown that target cell death occurs within minutes.109 Once apoptosis is triggered, it cannot be reversed. Cytotoxic T lymphocytes can induce the caspase cascade either through the perforin/granzyme or the Fas-Fas ligand (FasL) pathway.* Unlike apoptosis, necrosis is a type of cell death that spills cellular contents, including pathogens, into the surrounding tissue. This spillage elicits an inammatory reaction. Necrosis can be brought about by a variety of causes, such as physical trauma, ischemia, and infection. There is general agreement that keratinocyte cell death in TEN is the result of apoptosis, not necrosis.110 Electron microscopy of involved epidermis shows characteristic morphologic changes of apoptosis, and DNA fragmentation analysis shows that DNA is broken up into regular 200 base-pair subunits, a very specific feature of apoptosis. Finally, special staining techniques have identified apoptotic cells throughout all layers of the epidermis in TEN.
*In 1984, Dr Shin Yonehara and associates discovered a monoclonal antibody that attached to a cell surface receptor on human amnion-derived FL cells. This binding caused death of the cells. The antibody was produced using murine spleen cells immunized with human diploid fibroblast FS-7 cells. Dr Yonehara designated the cell surface antigen as Fas antigen. Fas is an abbreviation of: FS-7(F ) and FL(F )-associated (a) cell surface (s) antigen. After Fas Ligand was cloned, Fas antigen came to be known simply as Fas. Synonyms for this molecule include CD95, Apo-1, APT-1, and most recently, TNFRSF 6.
Both Fas-FasL and perforin/granzyme appear to be instrumental in triggering apoptosis in TEN. Viard et al111 have produced experimental and clinical evidence suggesting that the massive keratinocyte apoptosis of TEN is mediated through activation of the death receptor (DR), Fas. DRs are transmembrane proteins that are members of the TNF superfamily.112 At least eight different DRs have been identified, but the first discovered and the most thoroughly studied is Fas.113 In brief, upon recognition of FasL, Fas undergoes conformational changes in its cytoplasmic death domain. This causes recruitment of an adaptor protein called Fas-associated death domain protein (FADD). The adaptor protein is a molecule that attaches to both the Fas death domain and to procaspase 8. Its function is to bring together multiple copies of procaspase 8. These multiple copies then autoactivate to form caspase 8, the active enzyme, which in turn triggers the entire caspase cascade. Caspases are a group of proteases, each one of which cleaves a key protein within the cell. Caspases dismantle the cell in an orderly fashion. Caspases also activate nucleases, which can degrade intracellular viral DNA in addition to cellular DNA109 (Fig 6). Under normal conditions, Fas is present on the surface of keratinocytes. FasL, FADD, and caspases are present intracellularly. Should it be necessary for an epidermal cell to self-destruct, for example a keratinocyte damaged by UV radiation, intermediate laments are thought to transport FasL rapidly to the cell surface.114,115 Viard et al111 demonstrated that skin of TEN patients has FasL on the cell surface of keratinocytes, but FasL is not present on the keratinocytes of patients with maculopapular drug reactions or normals. Frozen sections of skin taken from TEN patients will induce apoptosis in Fas-sensitive Jurkat cells (a T-cell lymphoblastic leukemia cell line), and this effect can be blocked by FasL-blocking monoclonal antibody, or by Fas-Fc, a competitive inhibitor of keratinocyte cell surface Fas. In patients with TEN, high levels of soluble FasL (sFasL) are also found in the serum, whereas sFasL is not found in the serum of patients with maculopapular drug reactions or in normal controls.111 At the cell surface of numerous tissues, FasL expression is downregulated by metalloproteinases (MPs), which cleave the TNF-homologous portion of membrane-bound FasL. The product is shed as sFasL. Increased MP activity results in increased sFasL in serum.116,117 The increased serum levels of sFasL observed in TEN patients may be caused by the action of MPs at the keratinocyte cell surface.114 Consistent with this idea is a clinical observation
J AM ACAD DERMATOLVOLUME 56, NUMBER 2
Pereira, Mudgil, and Rosmarin 189
Fig 6. Schematic diagram of apoptosis induced by Fas ligand.
made by Chang et al.118 Serum levels of sFasL from a 42-year-old male with antibiotic-induced TEN were measured daily. A marked rise in sFasL levels occurred approximately 24 to 48 hours after the onset of major skin damage.118 This observation suggests that sFasL does not cause keratinocyte apoptosis, but rather that it is a byproduct of FasL expressed by keratinocytes. Not all investigators have been able to duplicate Viards model. In a study of 22 patients with SJS/TEN, Abe et al119 showed a consistent elevation of sFasL in serum. Addition of this serum to cultured keratinocytes induced apoptosis, and the effect could be blocked by addition of anti-FasL monoclonal antibody. Significantly, peripheral blood mononuclear cells (PBMCs) of TEN patients produced high levels of sFasL upon stimulation with the causal drug. In this study, DIF of skin biopsies from three of the 22 patients failed to show FasL on the surface of keratinocytes. The overall conclusion was that sFasL is produced by PBMCs, not epidermal cells, and the sFasL binds to Fas expressed on keratinocytes to cause apoptosis. The study disputes the source of FasL, but not the central role of the Fas-FasL pathway in the pathogenesis of TEN. The study also suggests that elevated sFasL in serum may serve as a serologic marker for TEN. Other DRs, most notably TNF-R1 and TNF-related apoptosis-inducing ligand (TRAIL), may also play a role in the pathogenesis of TEN.120 TNF-a, which is elevated in blister fluid, skin, mononuclear cells, and serum of TEN patients, can activate TNF-R1, which in turn can activate FADD and downstream caspases. However, TNF-R1 also activates NF-kB, which has an
antiapoptotic effect.120 NF-kB is probably the privileged pathway because TNF-induced apoptosis occurs only when cellular protein synthesis is blocked.112 It is not entirely clear whether TNF-a has predominantly proapoptotic or antiapoptotic effects in TEN. Therefore, anti-TNF therapies should be used with caution.120 Other studies challenge the role of Fas-FasL in the pathogenesis of TEN and place emphasis on perforin/granzyme. Perforin and granzyme are proteins stored within lytic granules of CTLs. Upon recognition of a target cell, the CTL releases perforin, which creates 16-nm channels in the target cell membrane. Granzyme B, a protease, passes through these channels to activate the caspase cascade (Fig 7). Nassif et al104 showed that in the presence of a causal drug, such as sulfamethoxazole, blister fluid mononuclear cells of TEN patients are cytotoxic, whereas PBMCs are not. This cytotoxicity is not blocked by anti-Fas monoclonal antibody, but it is blocked by ethylene glycol bis (2-aminoethylether)N,N,N,9 N9 -tetraacetic acid (EGTA) and concanamycin, both of which inhibit perforin/granzyme-induced apoptosis. In contradistinction to the findings of Viard et al, these findings implicate perforin/granzyme as the main cytotoxic pathway in TEN.104,121 In a later study of blister-uid cytokines involving 13 TEN patients, Nassif et al122 found elevated levels of IFN gamma, sTNF-a, and sFasL. Analysis of cytokine gene expression of blister fluid cells showed that the sFasL and sTNF-a found in blister fluid is produced by keratinocytes, not by mononuclear cells. The levels of sFasL, however, are very
190 Pereira, Mudgil, and Rosmarin
J AM ACAD DERMATOLFEBRUARY 2007
Fig 7. Apoptosis induced by perforin/granzyme B.
low. Cultured keratinocytes did not undergo apoptosis when incubated with cell-free supernatants of blister fluid because of this low concentration of sFasL. The investigators concluded that apoptosis in TEN is not mediated through the Fas-FasL pathway, and they proposed the following hypothesis: drugspecific CD8 cells secrete IFN-gamma, which activates keratinocytes to produce TNF-a, FasL, and small amounts of IL-10. TNF-a upregulates expression of MHC 1 molecules, which increase exposure of keratinocytes to CTLs and subsequent perforin/ granzyme mediated apoptosis. The production of FasL and IL-10 by keratinocytes is an epiphenomenon, not a primary pathogenic event. The authors speculated that these molecules may actually serve a protective role inasmuch as sFasL can induce apoptosis of CTLs and IL-10 downregulates inflammatory reactions.122 Finally, a study by Posadas et al123 supports the involvement of both cytokine pathways in the pathogenesis of TEN. The investigators studied cytokine expression in PBMCs and in blister fluid mononuclear cells of patients with delayed reactions to drugs. These reactions were divided into four categories: benign maculopapular rashes, desquamative exanthema, SJS, and TEN. The investigators showed a direct correlation between levels of disease severity and levels of perforin and granzyme B. Perforin and granzyme B were expressed at all degrees of disease severity; however, PBMCs of patients with maculopapular drug reactions expressed far less than patients with SJS or TEN. In
addition to perforin/granzyme B, FasL was detected in PBMCs and blister fluid mononuclear cells of patients with SJS and TEN. This particular study suggests a central role for perforin/granzyme; however, it also suggests that Fas-FasL is involved in the more severe reactions.123 In summary, laboratory evidence suggests that Fas-FasL is not the only pathway leading to keratinocyte apoptosis in TEN, but that perforin/granzyme also plays a role. Immunohistochemical ndings also suggest that in addition to cytotoxic T lymphocytes, monocytes, macrophages and TNF-a are intimately involved in the pathogenesis. Other biochemical derangements have been detected in TEN. Increased gelatinase A and B activity, expression of calprotectin (an antimicrobial protein not found in normal skin), and increased nitric oxide (which can induce apoptosis of keratinocytes) are all additional features.124-126 Precisely what role, if any, these abnormalities play in pathogenesis remains to be elucidated.
T CELL ACTIVATIONDrugs can activate T cells (1) by acting as haptens, (2) by acting as prohaptens, or (3) by direct pharmacologic interaction among the drug, MHC molecule, and T cell receptor. Most drugs are chemically inert; however, a few can react directly with tissue proteins to act as haptens. Notable examples include penicillin G, which covalently binds to lysine groups within endogenous proteins, cephalosporins, captopril, and certain cancer chemotherapeutic agents.127
J AM ACAD DERMATOLVOLUME 56, NUMBER 2
Pereira, Mudgil, and Rosmarin 191
The majority of drugs are prohaptens. The chemically inert parent drug does not itself act as a hapten, but following metabolism, a chemically reactive intermediate does. Drug metabolism is a biochemical process by which lipid soluble chemicals are converted to hydrophilic, water soluble compounds that are easily excreted by the body. The process occurs in two phases. Phase one is an oxidation reaction (loss of electrons) mediated through the cytochrome P (CYP) 450 enzyme system. Chemically reactive intermediates having an afnity for electrons (electrophilic) are formed. CYP450 refers to a superfamily of at least 57 related enzymes that degrade a variety of substrates including drugs and environmental toxins.128,129 These enzymes are found predominantly in the liver, but also in the lungs, intestines, and skin. CYP450emediated oxidative reactions add or expose binding sites for phase two reactions. In phase two reactions, the chemically reactive intermediates form a covalent linkage with polar conjugates such as glutathione, acetate, sulfate, or glucuronic acid. The linkage detoxifies the metabolite and simultaneously makes it water soluble and easily excreted. Under abnormal conditions, these reactive and sometimes toxic intermediates (e.g., epoxide, quinone, or nitroso products) can act as haptens and covalently bond to electron-donating, nucleophilic endogenous proteins to form complete antigens.130,131 SMX, for example, can become immunogenic after conversion to SMX-hydroxylamine by CYP450, and then by enzyme-independent oxidation to SMX-nitroso, the chemically reactive species that haptenates with cysteine residues in proteins. TEN, DRESS, and drug reactions generally occur with greater frequency in situations where there is a build up of chemically reactive metabolites, for example, in patients with renal or hepatic insufciency. Administration of allopurinol to patients with asymptomatic hyperuricemia and renal insufciency (a common clinical scenario) can result in accumulation of the chemically reactive intermediate oxypurinol. Oxypurinol can cause allopurinol hypersensitivity syndrome, which includes TEN as a skin manifestation.132,133 HIV patients, who have reduced levels of the cellular detoxifying chemicals glutathione and cysteine, are at risk for developing TEN to sulfonamides because of accumulation of the chemically reactive nitroso product.56 The incidence of all drug reactions in the HIV-infected population is higher than in the general population.134,135 When large initial doses of a drug such as lamotrigine overwhelm enzymatic detoxifying capacity, SJS/TEN or DHS can result.136 Coadministration of certain drugs can predispose to adverse drug reactions by
competition for the same enzyme binding site, or by upregulation or downregulation of detoxifying enzymes. For example, reactions to carbamazapine and lamotrigine are more common when given in combination with valproic acid. The addition of valproic acid overloads detoxifying capacity.137-142 Patients who are slow metabolizers because of polymorphisms of genes coding for drug metabolizing enzymes are at risk for adverse drug reactions. Large differences exist among individuals in their ability to metabolize medications. Each of the 57 CYP450 genes has variants with functional differences. For example, more than 78 CYP450-2D6 alleles have been characterized, the phenotypic expression of which results in enzymes having anywhere from poor to ultrarapid activity.129 The clinical result is an enormous difference among individuals in their ability to metabolize a drug, varying from supernormal to virtually absent.143 Polymorphisms in gene families other than CYP450 can also affect drug kinetics and toxicity, for example N-acetyltransferase. Persons with the slow acetylator phenotype are less efcient than rapid acetylators in metabolizing drugs with a primary aromatic amine or hydrazine group, such as sulfonamide antibiotics, isoniazid, hydralazine, and dapsone. Patients with SJS/TEN have a low N-acetylating capacity in comparison to normal controls. Low N-acetylating capacity may predispose to serious cutaneous adverse reactions.144 Glutathione S-transferase refers to another group of detoxification enzymes. Polymorphisms GST M1 and GST T1 are regularly associated with adverse cutaneous drug reactions.145 Polymorphisms in positions 308 and 238 of the promoter region of the TNF-a gene have been shown to be associated with carbamazapine hypersensitivity.146 Chemical reactivity and hapten formation may not be the only factors rendering a drug immunogenic. It has been demonstrated that T cell clones from patients with SMX hypersensitivity will recognize not only SMX-nitroso, but also SMX in its parent, unchanged form.147 SMX alone is chemically inert and nonreactive. This has lead to the idea that the chemical structure of a drug may be just as important as its chemical reactivity in the pathogenesis of adverse drug reactions. Normally, antigenic peptides are covalently linked and very tightly bound to the MHC molecule. Some drugs, though, have the capacity to bind to an MHC molecule and T cell receptor in the same way they would bind pharmacologically to a cellular receptor. This type of binding is labile and probably mediated by hydrogen bonds and Van der Waals forces. Pichler et al148 have shown that if a drug binds in this fashion to an MHC
192 Pereira, Mudgil, and Rosmarin
J AM ACAD DERMATOLFEBRUARY 2007
molecule and to a T cell receptor that will interact with the drug, that drug has the capacity to activate the T cell.148 This pharmacologic interaction with an immunological receptor has been termed the p-i concept.149,150 Pharmacologic interaction requires two surface molecules, an MHC molecule and a T cell receptor, to bind pharmacologically with the chemically inert drug. Because an MHC molecule is needed, only T-cell phenomena, such as maculopapular rash, SJS/TEN, and DRESS, can be accounted for by this mechanism. The p-i concept may also explain why certain medications such as carbamazepine are almost never associated with B-cell mediated reactions, such as urticaria or leukocytoclastic vasculitis. Some drugs that t the p-i model include carbamazapine, lamotrigine, sulfamethoxazole, and celecoxib.148 The most important implication of the p-i concept is that drug metabolism does not have to be abnormal in order for adverse cutaneous drug reactions to occur.
TEN patients require debridement of necrotic epidermis and coverage of denuded areas with either articial membranes, such as Biobrane (Bertek Pharmaceuticals, UDL Laboratories, Rockford, Ill), or with biologic dressings, such as porcine xenograft or human skin allograft. Coverage with banked allograft skin enhances healing, and it reduces pain, scarring, and infection. Treatment of the eyes consists of round-the-clock lubrication and lysis of adhesions with a sterile glass rod. Amniotic membrane transplantation appears to be a promising approach in reducing long-term ocular sequelae.41,159 Amniotic membrane has also been used for skin coverage in TEN.160 In a report by Spies et al161 of 15 children treated in a burn unit, without any adjuvant treatment, such as intravenous immune globulin (IVIG) or cyclosporine, the mortality was 7%. Similarly, Sheridan et al162 reported a series of 10 children with TEN treated in a burn unit with supportive care alone. Mortality was zero.
PRIMARY TREATMENTThe rst and most important element of treatment consists of discontinuation of the offending drug. The faster the causative drug is eliminated, the better the prognosis. Unfortunately, this appears to be less true if the drug has a long half-life.151 Second, the patient should be admitted to a burn unit where intensive supportive care and specialized treatment can be given by personnel experienced in handling extensive cutaneous injuries.152-154 The rapidity with which a patient is admitted to a burn unit is directly proportional to survival.155-157 Scrupulous attention must be paid to the eyes, respiratory tract, fluid and electrolyte balance, nutrition, infection, and pain relief. Frequent cultures of skin, urine, blood, and intravascular cannulas are recommended. The major causes of sepsis in TEN patients are Staphylococcus aureus and Pseudomonas aeruginosa. The Staphylococcus species cultured from blood is generally the same as that cultured from skin.2 When antibiotics are used empirically or prophylactically in the setting of TEN, there can be emergence of resistant organisms and increased mortality.158 Outcomes have never been shown to be better when antibiotics are used in this fashion. Antibiotic therapy is best initiated only when signs of sepsis occur. These signs include change in mental status, shivering, hypothermia, decreased urine output, and overall deterioration in clinical condition.2 Massive exudation of fluid from denuded skin may necessitate higher than usual doses of antibiotics because of their loss through skin.2
ADJUVANT TREATMENTSA number of interventions have been tried in TEN to stop disease progression, but no specic treatment has unequivocally proven to be effective. The cornerstone of SJS/TEN treatment remains supportive care in a burn unit. Adjuvant treatments are complementary. Plasmapheresis Plasmapheresis is a procedure in which whole blood is withdrawn and plasma separated from the cellular constituents. The patients plasma is then discarded, and the cellular constituents plus albumin or banked plasma are reinfused back into the patient. The purpose of plasmapheresis is to remove a pathogenic, nondialyzable plasma factor, such as a drug, poison, metabolite, antibody, immune complex, or disease-inducing cytokine. Plasmapheresis has been used in TEN with some measure of success. The procedure is quite safe, and in the treatment of TEN, anywhere from one to eight plasma exchanges are performed. In one series, plasmapheresis was combined with IVIG.163 Overall, the results have been good, and one investigator noted dramatic improvement in his patients.164 Survivals varied from 77% to 100%.164-166 One report, however, involving eight patients, showed no difference in survival in patients undergoing plasmapheresis compared to two similar groups treated with supportive care alone.167 In this small series, however, the overall survival was 87.5%, and the one death occurred in a patient with severe ischemic heart disease.
J AM ACAD DERMATOLVOLUME 56, NUMBER 2
Pereira, Mudgil, and Rosmarin 193
Cyclophosphamide and cyclosporine Although there are reports attesting to the value of cyclophosphamide, this medication is currently not used in the treatment of TEN. 157,168,169 Cyclosporine has been used successfully in doses of 3 mg/kg/day. In one series of eleven patients, there was zero mortality.170 Several individual case reports have described good outcomes in patients treated with cyclosporine.171-173 In one TEN patient with pancytopenia, cyclosporine was successfully combined with granulocyte colony-stimulating factor.174 In addition to its potent immunosuppressive effects, cyclosporine may also have anti-apoptotic effects inasmuch as it inhibits downregulation of NF-kB.120,171 Corticosteroids The role of corticosteroids in the treatment of SJS/TEN has always been controversial. A few reports show benet.175,176 However, the preponderance of opinion holds that corticosteroids are best avoided. Corticosteroids given 48 hours or more prior to admission are associated with an increase in the incidence of infection, length of stay, and mortality.33 If a patient is taking corticosteroids for another condition, the corticosteroids will not stop TEN from occurring, and they have no effect in stopping TEN progression once the reaction is initiated.177,178 However, this negative appraisal may change. The poor outcomes may be the result of inadequate doses. Some evidence is emerging that suggests benet from high-dose, pulse corticosteroids in early stages of TEN.179 Twelve patients with SJS/TEN were treated with dexamethasone pulse therapy, 1.5 mg/kg/day, intravenously for three consecutive days. Disease progression was arrested on average in three days and healing occurred within three weeks. The predicted SCORTEN mortality was four deaths, but only one died. This particular patient had advanced cancer, but at the time of death his skin lesions were almost completely healed.180 In a study involving the largest cohort of SJS/TEN patients yet assembled, treatment outcomes were studied in 281 patients with SJS/TEN treated in French and German hospitals. The overall mortality was 22%. Adjusting for variables such as age, extent of disease, and co-morbid conditions, the investigators concluded that pulse corticosteroids significantly reduced the risk of death. They also concluded that IVIG is of no value and may in fact be associated with excess mortality.181 TNF-a inhibitors Thalidomide is an inhibitor of TNF-a. A prospective trial comparing thalidomide to placebo in TEN
was suspended because of excess mortality in patients given thalidomide. It was thought that thalidomide paradoxically elevated TNF-a levels.182 Thalidomide itself has also been reported to cause TEN.183 Rapid and dramatic improvement was observed in a 56-year-old female with TEN treated with a single infusion of infliximab.184 Pentoxifylline is also an inhibitor of TNF-a, and a few TEN patients have been reported to benefit from this drug.185 Although some anti-TNF therapies seem promising, they should be used cautiously because TNF-a may have anti-apoptotic effects through the TNF-R1e NF-kB pathway.120 Intravenous immune globulin IVIG is derived from a plasma pool of several thousand donors, and it consists mainly of IgG. IVIG contains a wide variety of antibodies, including autoantibodies against normal proteins such as Fas.186 IVIG interferes with Fas-FasL interactions. Human keratinocytes are sensitive to recombinant human sFasL (rhsFasL). In vitro, IVIG completely blocks rhsFasL-mediated apoptosis of keratinocytes. IVIG contains anti-Fas IgG, which attaches to Fas receptors. This attachment blocks binding of rhsFasL to the receptors. Depletion of anti-Fas IgG from IVIG will remove its ability to stop Fas-FasL mediated cell death.111,187 In vitro evidence provides a rational basis for treatment, and there have been numerous anecdotal case reports showing benefit from IVIG in both SJS and TEN.188-195 There have also been studies involving larger groups of patients. In a multicenter, retrospective study involving 14 European and American university-based dermatology centers, 48 consecutive patients with TEN were treated with IVIG and standard supportive care between 1997 and 2000.196 The survival rate was 88%. The recommended dose of IVIG was 1 g/kg/day for 3 days.196 In a similar study of 16 TEN patients treated with IVIG (1 g/kg/day), only one patient died whereas the predicted SCORTEN mortality was 5.8 deaths. The one fatality occurred in a dialysis patient with multiple co-morbid conditions, but at the time of death, her skin lesions were resolved.197 One-hundred percent survival was observed in a prospective study of 12 TEN patients from Kuwait treated with IVIG.198 In a report of nine TEN patients treated with IVIG and pulse methylprednisolone, eight survived. Although the methylprednisolone is a confounding factor, it was nonetheless concluded that IVIG is a safe and valid therapy for TEN.199 Reviewing 28 published reports from the pediatric literature, plus 7 cases of their own, Metry et al200 concluded that IVIG is a useful and safe therapy for
194 Pereira, Mudgil, and Rosmarin
J AM ACAD DERMATOLFEBRUARY 2007
children with SJS/TEN. Rapid and consistent recovery ensued in every patient following use of IVIG, and there were no deaths.200 Tristani-Firouzi et al192 evaluated the outcome of 8 pediatric TEN patients treated with IVIG. Survival was 100%. Similarly, in still another retrospective study of twelve pediatric patients with SJS treated with IVIG in doses of 0.6 g/kg/day, survival was 100% and objective response was observed within 2 days.201 In one case study, IVIG was used successfully to prevent SJS from occurring in a woman who had experienced multiple episodes following use of intravenous contrast dye.202 Interestingly, human IVIG was used with good results in the treatment of SJS in a dog.203 Initial optimism over IVIG has been tempered by at least six reports showing minimal or no benet from IVIG, including the European observational study of 281 patients. In a retrospective study by Brown et al,204 24 patients treated with IVIG were compared to 21 patients not treated with IVIG. The dose of IVIG was 0.4 g/kg/day, and the two groups were essentially identical. There was no therapeutic advantage in using IVIG at any level of SCORTEN severity between the two groups. In fact, the overall mortality was 41.7% for those treated with IVIG and 28.6% for those not treated. The importance of this study lies in the fact that all patients were treated in one institution using a uniform treatment protocol and the same medical team. The authors concluded that IVIG should not be given to TEN patients outside of a clinical trial. In a similar study, 16 TEN patients admitted to a burn unit and treated with IVIG were compared to a similar retrospective group of 16 not treated with IVIG. There was no signicant difference in mortality, length of stay, incidence of sepsis, or incidence of the systemic inammatory response syndrome.205 In a prospective open trial from a single institution, 35 patients with TEN were treated with IVIG in doses of 1 g/kg/day. The predicted SCORTEN mortality was 8.2 deaths (21%), but the actual deaths were 11 (32%). In addition, the death rate of those treated with IVIG was higher than the 20% historical death rate for TEN in that institution. The authors concluded that IVIG cannot be recommended as a treatment of SJS and TEN without further studies. IVIG was found to be of minimal value in 7 children with SJS when compared to 5 children with SJS treated with corticosteroids or supportive care alone.206 Finally, in a comparison of 10 treated patients with 18 historical controls, IVIG did not reduce the severity of the ocular complications of TEN.207 It is difcult to reconcile the studies showing negative results with the large number of reports showing benet, but one inference is that Fas-FasL
is not the only pathway to apoptosis.208 Other pathogenetic mechanisms, most notably perforin/ granzyme, must be involved. Although there are batch-to-batch variations in IVIG activity, interbatch variation has never been a cause of therapeutic failure in diseases where IVIG consistently works. In the study by Brown, the 0.4 g/kg/day dose was slightly lower than the usual recommended dose, and in all five studies, the numbers of patients were small. Nonetheless, a strong argument emerges disputing the consistent value of IVIG in TEN. A prospective, controlled study is realistically unlikely given the rarity of the disease and the large numbers of patients needed for such a study to have statistical power. The absence of an animal model also greatly hampers research into the molecular pathogenesis and treatment of the disorder. Although carefully planned, single-institution studies have shown no benet from IVIG, the wealth of clinical experience supporting its therapeutic value cannot be dismissed. Many practicing physicians feel that the clinical and laboratory evidence is sufciently compelling to justify its use. In comparison to treatments whose value has been questioned, such as prednisone and cyclophosphamide, IVIG has minimal toxicities; and considering the gravity of the condition being dealt with, the risk/benet ratio is quite favorable.209 IVIG may also help combat infection, and it might favorably affect fluid balance in these patients, many of whom are hypovolemic.210
CONCLUSIONAs more medications are developed and prescribed, life-threatening drug reactions will become an increasingly important problem. The most crucial interventions in TEN are discontinuation of the offending drug and intensive supportive care in a burn unit. However, the real key to prevention of death and long-term morbidity depends upon stopping disease progression during the acute phase.211 Unfortunately, no rm conclusions or recommendations concerning specic therapies can be derived from the welter of conicting data and opinions surrounding this condition. Use of adjunctive therapies remains a matter of clinical judgment. Given that apoptosis is a rapid and irreversible biologic process once triggered, early and aggressive intervention with the chosen modality is essential. Timing is critical, and it has been suggested that therapy should be initiated within the rst four days of disease onset.212 Combination treatments attacking different components of the pathogenetic pathways appear particularly promising, for example pulse
J AM ACAD DERMATOLVOLUME 56, NUMBER 2
Pereira, Mudgil, and Rosmarin 195
corticosteroids (broad based immunosuppression) and plasmapheresis (physical removal of drug, metabolites, and cytokines). Neutropenia worsens prognosis because risk of infection is signicantly increased. There have been several case reports describing addition of granulocyte colony-stimulating factor to treatment regimens.213-216 It appears that granulocyte colony-stimulating factor is beneficial, and it too may also have a place in combination therapy of TEN. As the eld of pharmacogenetics develops, there may come a time when patients who are genetically predisposed to serious cutaneous adverse reactions can be identied. This will allow for individualized therapies and prevention of unnecessary suffering.REFERENCES 1. Revuz J, Roujeau JC, Guillaume JC, Penso D, Touraine R. Treatment of toxic epidermal necrolysis. Creteils experience. Arch Dermatol 1987;123:1156-8. 2. Revuz J, Penso D, Roujeau JC, Guillaume JC, Payne CR, Wechsler J, et al. Toxic epidermal necrolysis. Clinical findings and prognosis factors in 87 patients. Arch Dermatol 1987; 123:1160-5. 3. Roujeau JC. Drug-induced toxic epidermal necrolysis. II. Current aspects. Clin Dermatol 1993;11:493-500. 4. Wolkenstein PE, Roujeau JC, Revuz J. Drug-induced toxic epidermal necrolysis. Clin Dermatol 1998;16:399-408. 5. Sugimoto Y, Mizutani H, Sato T, Kawamura N, Ohkouchi K, Shimizu M. Toxic epidermal necrolysis with severe gastrointestinal mucosal cell death: a patient who excreted long tubes of dead intestinal epithelium. J Dermatol 1998;25: 533-8. 6. Faye O, Wechsler J, Roujeau JC. Cell-mediated immunologic mechanism and severity of TEN. Arch Dermatol 2005;141: 775-6. 7. Lebargy F, Wolkenstein P, Gisselbrecht M, Lange F, FleuryFeith J, Delclaux C, et al. Pulmonary complications in toxic epidermal necrolysis: a prospective clinical study. Intensive Care Med 1997;23:1237-44. 8. Wolkenstein P, Revuz J. Toxic epidermal necrolysis. Dermatol Clin 2000;18:485-95. 9. Ghislain PD, Roujeau JC. Treatment of severe drug reactions: Stevens-Johnson syndrome, toxic epidermal necrolysis and hypersensitivity syndrome. Dermatol Online J 2002;8:5. 10. Paquet P, Pierard GE. Intense pulsed light treatment of persistent facial hypermelanosis following drug-induced toxic epidermal necrolysis. Dermatol Surg 2004;30(12 Pt 2): 1522-5. 11. Meneux E, Paniel BJ, Pouget F, Revuz J, Roujeau JC, Wolkenstein P. Vulvovaginal sequelae in toxic epidermal necrolysis. J Reprod Med 1997;42:153-6. 12. Meneux E, Wolkenstein P, Haddad B, Roujeau JC, Revuz J, Paniel BJ. Vulvovaginal involvement in toxic epidermal necrolysis: a retrospective study of 40 cases. Obstet Gynecol 1998;91:283-7. 13. Sheridan RL, Schulz JT, Ryan CM, Schnitzer JJ, Lawlor D, Driscoll DN, et al. Long-term consequences of toxic epidermal necrolysis in children. Pediatrics 2002;109:74-8. 14. Bonafe JL, Thibaut I, Hoff J. Introital adenosis associated with the Stevens-Johnson syndrome. Clin Exp Dermatol 1990;15: 356-7.
15. Noel JC, Buxant F, Fayt I, Bebusschere G, Parent D. Vulval adenosis associated with toxic epidermal necrolysis. Br J Dermatol 2005;153:457-8. 16. Marquette GP, Su B, Woodruff JD. Introital adenosis associated with Stevens-Johnson syndrome. Obstet Gynecol 1985; 66:143-5. 17. Wilson EE, Malinak LR. Vulvovaginal sequelae of StevensJohnson syndrome and their management. Obstet Gynecol 1988;71(3 Pt 2):478-80. 18. Di Pascuale MA, Espana EM, Liu DT, Kawakita T, Li W, Gao YY, et al. Correlation of corneal complications with eyelid cicatricial pathologies in patients with StevensJohnson syndrome and toxic epidermal necrolysis syndrome. Ophthalmology 2005;112:904-12. 19. Stevens AM, Johnson FC. A new eruptive fever associated with stomatitis and ophthalmia. American Journal of Diseases of Children 1922;24:526-33. 20. Roujeau JC, Phlippoteau C, Koso M, Wechsler J, Andre C, Binaghi M, et al. Sjogren-like syndrome after drug-induced toxic epidermal necrolysis. Lancet 1985;1:609-11. 21. Haber J, Hopman W, Gomez M, Cartotto R. Late outcomes in adult survivors of toxic epidermal necrolysis after treatment in a burn center. J Burn Care Rehabil 2005;26:33-41. 22. Bastuji-Garin S, Rzany B, Stern RS, Shear NH, Naldi L, Roujeau JC. Clinical classification of cases of toxic epidermal necrolysis, Stevens-Johnson syndrome, and erythema multiforme. Arch Dermatol 1993;129:92-6. 23. Assier H, Bastujigarin S, Revuz J, Roujeau JC. Erythema multiforme with mucous-membrane involvement and Stevens-Johnson Syndrome are clinically different disorders with distinct causes. Arch Dermatol 1995;131:539-43. 24. Auquier-Dunant A, Mockenhaupt M, Naldi L, Correia O, Schroder W, Roujeau JC. Correlations between clinical patterns and causes of erythema multiforme majus, StevensJohnson syndrome, and toxic epidermal necrolysis: results of an international prospective study. Arch Dermatol 2002; 138:1019-24. 25. Kokuba H, Aurelian L, Burnett J. Herpes simplex virus associated erythema multiforme (HAEM) is mechanistically distinct from drug-induced erythema multiforme: interferongamma is expressed in HAEM lesions and tumor necrosis factor-alpha in drug-induced erythema multiforme lesions. J Invest Dermatol 1999;113:808-15. 26. Lohmeier K, Megahed M, Schulte KW, Stannigel H, Mayatepek E, Schroten H. Toxic epidermal necrolysis in a premature infant of 27 weeks gestational age. Br J Dermatol 2005; 152:150-1. 27. Bastuji-Garin S, Zahedi M, Guillaume JC, Roujeau JC. Toxic epidermal necrolysis (Lyell syndrome) in 77 elderly patients. Age Ageing 1993;22:450-6. 28. Rzany B, Mockenhaupt M, Baur S, Schroder W, Stocker U, Mueller J, et al. Epidemiology of erythema exsudativum multiforme majus, Stevens-Johnson syndrome, and toxic epidermal necrolysis in Germany (1990-1992): Structure and results of a population-based registry. J Clin Epidemiol 1996;49:769-73. 29. Sushma M, Noel MV, Ritika MC, James J, Guido S. Cutaneous adverse drug reactions: a 9-year study from a South Indian Hospital. Pharmacoepidemiol Drug Saf 2005;14:567-70. 30. Bastuji-Garin S, Fouchard N, Bertocchi M, Roujeau JC, Revuz J, Wolkenstein P. SCORTEN: A severity-of-illness score for toxic epidermal necrolysis. J Invest Dermatol 2000;115:149-53. 31. Guegan S, Bastuji-Garin S, Poszepczynska-Guigne E, Roujeau JC, Revuz J. Performance of the SCORTEN during the first five days of hospitalization to predict the prognosis of epidermal necrolysis. J Invest Dermatol 2006;126:272-6.
196 Pereira, Mudgil, and Rosmarin
J AM ACAD DERMATOLFEBRUARY 2007
32. Westly ED, Wechsler HL. Toxic epidermal necrolysis: granulocytic leukopenia as a prognostic indicator. Arch Dermatol 1984;120:721-6. 33. Engelhardt SL, Schurr MJ, Helgerson RB. Toxic epidermal necrolysis: an analysis of referral patterns and steroid usage. J Burn Care Rehabil 1997;18:520-4. 34. Dobrosavljevic D, Milinkovic MV, Nikolic MM. Toxic epidermal necrolysis following morbilli-parotitis-rubella vaccination. J Eur Acad Dermatol Venereol 1999;13:59-61. 35. Radimer GF, Davis JH, Ackerman AB. Fumigant-induced toxic epidermal necrolysis. Arch Dermatol 1974;110:103-4. 36. Ball R, Ball LK, Wise RP, Braun MM, Beeler JA, Salive ME. Stevens-Johnson syndrome and toxic epidermal necrolysis after vaccination: reports to the vaccine adverse event reporting system. Pediatr Infect Dis J 2001;20:219-23. 37. House RA, Jakubovic H, Wong L, Holness DL. Work-related toxic epidermal necrolysis? J Occup Med 1992;34:135-9. 38. Lam NS, Yang YH, Wang LC, Lin YT, Chiang BL. Clinical characteristics of childhood erythema multiforme, StevensJohnson syndrome and toxic epidermal necrolysis in Taiwanese children. J Microbiol Immunol Infect 2004;37:366-70. 39. Stevens D, Swift PG, Johnston PG, Kearney PJ, Corner BD, Burman D. Mycoplasma pneumoniae infections in children. Arch Dis Child 1978;53:38-42. 40. Fournier S, Bastuji-Garin S, Mentec H, Revuz J, Roujeau JC. Toxic epidermal necrolysis associated with Mycoplasma pneumoniae infection. Eur J Clin Microbiol Infect Dis 1995; 14:558-9. 41. John T, Foulks GN, John ME, Cheng K, Hu D. Amniotic membrane in the surgical management of acute toxic epidermal necrolysis. Ophthalmology 2002;109:351-60. 42. Guillaume JC, Roujeau JC, Revuz J, Penso D, Touraine R. The culprit drugs in 87 cases of toxic epidermal necrolysis (Lyells syndrome). Arch Dermatol 1987;123:1166-70. 43. Roujeau JC, Kelly JP, Naldi L, Rzany B, Stern RS, Anderson T, et al. Medication use and the risk of Stevens-Johnson syndrome or toxic epidermal necrolysis. N Engl J Med 1995;333:1600-7. 44. Caumes E, Bossi P, Katlama C, Bricaire F. [Antiretroviralinduced toxiderma in HIV-infected patients.] Presse Med 2003;32:1325-33. 45. Leone R, Venegoni M, Motola D, Moretti U, Piazzetta V, Cocci A, et al. Adverse drug reactions related to the use of fluoroquinolone antimicrobials: an analysis of spontaneous reports and fluoroquinolone consumption data from three Italian regions. Drug Saf 2003;26:109-20. 46. Litt JZ. Litts Drug Eruption Reference Manual. 10th ed. New York: Taylor & Francis, Parthenon Books; 2004. 47. Lin MS, Dai YS, Pwu RF, Chen YH, Chang NC. Risk estimates for drugs suspected of being associated with StevensJohnson syndrome and toxic epidermal necrolysis: a casecontrol study. Intern Med J 2005;35:188-90. 48. Praz SM, de Torrente A, Zender H, Schmied E, Schleppy CA, Genne D. Toxic epidermal necrolysis after topical intranasal application of mupirocin. Infect Control Hosp Epidemiol 2003;24:459-60. 49. Fogh K. [Toxic epidermal necrolysis following intake of vitamins and natural medication.] Ugeskr Laeger 1995;157: 3631-3. 50. Mochitomi Y, Inoue A, Kawabata H, Ishida S, Kanzaki T. Stevens-Johnson syndrome caused by a health drink (Eberu) containing ophiopogonis tuber. J Dermatol 1998;25:662-5. 51. Lim YL, Thirumoorthy T. Serious cutaneous adverse reactions to traditional Chinese medicines. Singapore Med J 2005;46:714-7. 52. Nagge JJ, Knowles SR, Juurlink DN, Shear NH. Pseudoephedrine-induced toxic epidermal necrolysis. Arch Dermatol 2005;141:907-8.
53. Redondo P, Vicente J, Espana A, Subira ML, De Felipe I, Quintanilla E. Photo-induced toxic epidermal necrolysis caused by clobazam. Br J Dermatol 1996;135:999-1002. 54. Mansur AT, Aydingoz IA. A case of toxic epidermal necrolysis with lesions mostly on sun-exposed skin. Photodermatol Photoimmunol Photomed 2005;21:100-2. 55. Paquet P, Jacob E, Damas P, Pierard GE. Recurrent fatal druginduced toxic epidermal necrolysis (Lyells syndrome) after putative beta-lactam cross-reactivity: Case report and scrutiny of antibiotic imputability. Crit Care Med 2002; 30:2580-3. 56. Slatore CG, Tilles SA. Sulfonamide hypersensitivity. Immunol Allergy Clin North Am 2004;24:477-90. 57. Rzany B, Correia O, Kelly JP, Naldi L, Auquier A, Stern R. Risk of Stevens-Johnson syndrome and toxic epidermal necrolysis during first weeks of antiepileptic therapy: a case-control study. Study Group of the International Case Control Study on Severe Cutaneous Adverse Reactions. Lancet 1999; 353:2190-4. 58. Mockenhaupt M, Messenheimer J, Tennis P, Schlingmann J. Risk of Stevens-Johnson syndrome and toxic epidermal necrolysis in new users of antiepileptics. Neurology 2005;64: 1134-8. 59. Micali G, Linthicum K, Han N, West DP. Increased risk of erythema multiforme major with combination anticonvulsant and radiation therapies. Pharmacotherapy 1999;19:223-7. 60. Gomez-Criado MS, Ayani I, Leon-Colombo T, Ramos ML, Reneses MJ. [Stevens-Johnson syndrome, toxic epidermal necrolysis and phenytoin. Factors linked to a higher risk.] Rev Neurol 2004;38:1056-60. 61. Aguiar D, Pazo R, Duran I, Terrasa J, Arrivi A, Manzano H, et al. Toxic epidermal necrolysis in patients receiving anticonvulsants and cranial irradiation: a risk to consider. J Neurooncol 2004;66:345-50. 62. Becker DS. Toxic epidermal necrolysis. Lancet 1998;351: 1417-20. 63. Quinn AM, Brown K, Bonish BK, Curry J, Gordon KB, Sinacore J, et al. Uncovering histologic criteria with prognostic significance in toxic epidermal necrolysis. Arch Dermatol 2005; 141:683-7. 64. Amon RB, Dimond RL. Toxic epidermal necrolysis. Rapid differentiation between staphylococcal- and drug-induced disease. Arch Dermatol 1975;111:1433-7. 65. Neff P, Meuli-Simmen C, Kempf W, Gaspert T, Meyer VE, Kunzi W. Lyell syndrome revisited: analysis of 18 cases of severe bullous skin disease in a burns unit. Br J Plast Surg 2005;58: 73-80. 66. Mockenhaupt M, Idzko M, Grosber M, Schopf E, Norgauer J. Epidemiology of staphylococcal scalded skin syndrome in Germany. J Invest Dermatol 2005;124:700-3. 67. Yamasaki O, Yamaguchi T, Sugai M, Chapuis-Cellier C, Arnaud F, Vandenesch F, et al. Clinical manifestations of staphylococcal scalded-skin syndrome depend on serotypes of exfoliative toxins. J Clin Microbiol 2005;43:1890-3. 68. Ladhani S. Recent developments in staphylococcal scalded skin syndrome. Clin Microbiol Infect 2001;7:301-7. 69. Ladhani S, Robbie S, Garratt RC, Chapple DS, Joannou CL, Evans RW. Development and evaluation of detection systems for staphylococcal exfoliative toxin A responsible for scaldedskin syndrome. J Clin Microbiol 2001;39:2050-4. 70. Gentilhomme E, Faure M, Piemont Y, Binder P, Thivolet J. Action of staphylococcal exfoliative toxins on epidermal cell cultures and organotypic skin. J Dermatol 1990;17: 526-32. 71. Tonev S, Vasileva S, Kadurina M. Depot sulfonamid associated linear IgA bullous dermatosis with erythema
J AM ACAD DERMATOLVOLUME 56, NUMBER 2
Pereira, Mudgil, and Rosmarin 197
72. 73.
74. 75.
76. 77.
78.
79.
80.
81. 82.
83. 84.
85. 86.
87.
88.
89.
90.
91.
92.
93.
multiforme-like clinical features. J Eur Acad Dermatol Venereol 1998;11:165-8. Collier PM, Wojnarowska F. Drug-induced linear immunoglobulin A disease. Clin Dermatol 1993;11:529-33. Craycraft ME, Arunakul VL, Humeniuk JM. Probable vancomycin-associated toxic epidermal necrolysis. Pharmacotherapy 2005;25:308-12. Camilleri M, Pace JL. Drug-induced linear immunoglobulin-A bullous dermatosis. Clin Dermatol 1998;16:389-91. Anhalt GJ, Kim SC, Stanley JR, Korman NJ, Jabs DA, Kory M, et al. Paraneoplastic pemphigus. An autoimmune mucocutaneous disease associated with neoplasia. N Engl J Med 1990;323:1729-35. Wade MS, Black MM. Paraneoplastic pemphigus: a brief update. Australas J Dermatol 2005;46:1-8, quiz 9-10. Marzano AV, Grammatica A, Cozzani E, Terracina M, Berti E. Paraneoplastic pemphigus. A report of two cases associated with chronic B-cell lymphocytic leukaemia. Br J Dermatol 2001;145:127-31. Correia O, Delgado L, Barbosa IL, Campilho F, FlemingTorrinha J. Increased interleukin 10, tumor necrosis factor alpha, and interleukin 6 levels in blister fluid of toxic epidermal necrolysis. J Am Acad Dermatol 2002;47:58-62. Vargas-Diez E, Garcia-Diez A, Marin A, Fernandez-Herrera J. Life-threatening graft-vs-host disease. Clin Dermatol 2005;23: 285-300. Friedman KJ, LeBoit PE, Farmer ER. Acute follicular graft-vshost reaction. A distinct clinicopathologic presentation. Arch Dermatol 1988;124:688-91. Brenner S, Bialy-Golan A, Ruocco V. Drug-induced pemphigus. Clin Dermatol 1998;16:393-7. Ruocco V, De Angelis E, Lombardi ML. Drug-induced pemphigus. II. Pathomechanisms and experimental investigations. Clin Dermatol 1993;11:507-13. Mutasim DF, Pelc NJ, Anhalt GJ. Drug-induced pemphigus. Dermatol Clin 1993;11:463-71. Bastuji-Garin S, Joly P, Picard-Dahan C, Bernard P, Vaillant L, Pauwels C, et al. Drugs associated with bullous pemphigoid. A case-control study. Arch Dermatol 1996;132:272-6. Fellner MJ. Drug-induced bullous pemphigoid. Clin Dermatol 1993;11:515-20. Beylot C, Bioulac P, Doutre MS. [Acute generalized exanthematic pustuloses (four cases) (authors transl).] Ann Dermatol Venereol 1980;107:37-48. Cohen AD, Cagnano E, Halevy S. Acute generalized exanthematous pustulosis mimicking toxic epidermal necrolysis. Int J Dermatol 2001;40:458-61. Lin JH, Sheu HM, Lee JY. Acute generalized exanthematous pustulosis with erythema multiforme-like lesions. Eur J Dermatol 2002;12:475-8. Roujeau JC, Huynh TN, Bracq C, Guillaume JC, Revuz J, Touraine R. Genetic susceptibility to toxic epidermal necrolysis. Arch Dermatol 1987;123:1171-3. Chung WH, Hung SI, Hong HS, Hsih MS, Yang LC, Ho HC, et al. Medical genetics: a marker for Stevens-Johnson syndrome. Nature 2004;428:486. Hung SI, Chung WH, Liou LB, Chu CC, Lin M, Huang HP, et al. HLA-B*5801 allele as a genetic marker for severe cutaneous adverse reactions caused by allopurinol. Proc Natl Acad Sci U S A 2005;102:4134-9. Mallal S, Nolan D, Witt C, Masel G, Martin AM, Moore C, et al. Association between presence of HLA-B*5701, HLADR7, and HLA-DQ3 and hypersensitivity to HIV-1 reversetranscriptase inhibitor abacavir. Lancet 2002;359:727-32. Hetherington S, Hughes AR, Mosteller M, Shortino D, Baker KL, Spreen W, et al. Genetic variations in HLA-B region and
94.
95. 96.
97. 98.
99.
100.
101.
102.
103.
104.
105.
106.
107.
108.
109.
110.
111.
hypersensitivity reactions to abacavir. Lancet 2002;359: 1121-2. Telenti A, Aubert V, Spertini F. Individualising HIV treatmentpharmacogenetics and immunogenetics. Lancet 2002;359:722-3. Revuz J. New advances in severe adverse drug reactions. Dermatol Clin 2001;19:697-709. Neuman MG, Malkiewicz IM, Shear NH. A novel lymphocyte toxicity assay to assess drug hypersensitivity syndromes. Clin Biochem 2000;33:517-24. Gruchalla RS, Pirmohamed M. Clinical practice. Antibiotic allergy. N Engl J Med 2006;354:601-9. Paquet P, Nikkels A, Arrese JE, Vanderkelen A, Pierard GE. Macrophages and tumor necrosis factor alpha in toxic epidermal necrolysis. Arch Dermatol 1994;130:605-8. Correia O, Delgado L, Ramos JP, Resende C, Torrinha JA. Cutaneous T-cell recruitment in toxic epidermal necrolysis. Further evidence of CD81 lymphocyte involvement. Arch Dermatol 1993;129:466-8. Friedmann PS, Strickland I, Pirmohamed M, Park BK. Investigation of mechanisms in toxic epidermal necrolysis induced by carbamazepine. Arch Dermatol 1994;130:598-604. Correia O, Delgado L, Roujeau JC, Le Cleach L, FlemingTorrinha JA. Soluble interleukin 2 receptor and interleukin 1alpha in toxic epidermal necrolysis: a comparative analysis of serum and blister fluid samples. Arch Dermatol 2002; 138:29-32. Leyva L, Torres MJ, Posadas S, Blanca M, Besso G, OValle F, et al. Anticonvulsant-induced toxic epidermal necrolysis: monitoring the immunologic response. J Allergy Clin Immunol 2000;105(1 Pt 1):157-65. Le Cleach L, Delaire S, Boumsell L, Bagot M, Bourgault-Villada I, Bensussan A, et al. Blister fluid T lymphocytes during toxic epidermal necrolysis are functional cytotoxic cells which express human natural killer (NK) inhibitory receptors. Clin Exp Immunol 2000;119:225-30. Nassif A, Bensussan A, Dorothee G, Mami-Chouaib F, Bachot N, Bagot M, et al. Drug specific cytotoxic T-cells in the skin lesions of a patient with toxic epidermal necrolysis. J Invest Dermatol 2002;118:728-33. Paquet P, Paquet F, Al Saleh W, Reper P, Vanderkelen A, Pierard GE. Immunoregulatory effector cells in drug-induced toxic epidermal necrolysis. Am J Dermatopathol 2000;22: 413-7. Kirkham N, Peacock SJ, Jones DB. Monoclonal antibody MAC 387 recognizes a myelomonocytic antigen shared by epithelial cells in inflammatory skin diseases. Br J Dermatol 1990; 122:61-9. Monteiro MR, Murphy EE, Galaria NA, Whitaker-Menezes D, Murphy GF. Cytological alterations in dermal dendrocytes in vitro: evidence for transformation to a non-dendritic phenotype. Br J Dermatol 2000;143:84-90. Paquet P, Quatresooz P, Pierard GE. Factor-XIIIa-positive dendrocytes in drug-induced toxic epidermal necrolysis (Lyells syndrome): paradoxical activation in skin and rarefaction in lymph nodes. Dermatology 2003;206:374-8. Janeway CA, Travers P, Walport M, Shlomchik M. Immunobiology: the immune system in health and disease. 5th ed. New York: Garland Publishing; 2001. Paul C, Wolkenstein P, Adle H, Wechsler J, Garchon HJ, Revuz J, et al. Apoptosis as a mechanism of keratinocyte death in toxic epidermal necrolysis. Br J Dermatol 1996;134:710-4. Viard I, Wehrli P, Bullani R, Schneider P, Holler N, Salomon D, et al. Inhibition of toxic epidermal necrolysis by blockade of CD95 with human intravenous immunoglobulin. Science 1998;282:490-3.
198 Pereira, Mudgil, and Rosmarin
J AM ACAD DERMATOLFEBRUARY 2007
112. Wehrli P, Viard I, Bullani R, Tschopp J, French LE. Death receptors in cutaneous biology and disease. J Invest Dermatol 2000;115:141-8. 113. French LE, Tschopp J. Protein-based therapeutic approaches targeting death receptors. Cell Death Differ 2003;10:117-23. 114. Viard-Leveugle I, Bullani RR, Meda P, Micheau O, Limat A, Saurat JH, et al. Intracellular localization of keratinocyte Fas ligand explains lack of cytolytic activity under physiological conditions. J Biol Chem 2003;278:16183-8. 115. Filipowicz E, Adegboyega P, Sanchez RL, Gatalica Z. Expression of CD95 (Fas) in sun-exposed human skin and cutaneous carcinomas. Cancer 2002;94:814-9. 116. Tanaka M, Itai T, Adachi M, Nagata S. Downregulation of Fas ligand by shedding. Nat Med 1998;4:31-6. 117. Knox PG, Milner AE, Green NK, Eliopoulos AG, Young LS. Inhibition of metalloproteinase cleavage enhances the cytotoxicity of Fas ligand. J Immunol 2003;170:677-85. 118. Chang HY, Cooper ZA, Swetter SM, Marinkovich MP. Kinetics and specificity of fas ligand induction in toxic epidermal necrolysis. Arch Dermatol 2004;140:242-4. 119. Abe R, Shimizu T, Shibaki A, Nakamura H, Watanabe H, Shimizu H. Toxic epidermal necrolysis and Stevens-Johnson syndrome are induced by soluble Fas ligand. Am J Pathol 2003;162:1515-20. 120. Chave TA, Mortimer NJ, Sladden MJ, Hall AP, Hutchinson PE. Toxic epidermal necrolysis: current evidence, practical management and future directions. Br J Dermatol 2005;153: 241-53. 121. Nassif A, Bensussan A, Boumsell L, Deniaud A, Moslehi H, Wolkenstein P, et al. Toxic epidermal necrolysis: effector cells are drug-specific cytotoxic T cells. J Allergy Clin Immunol 2004;114:1209-15. 122. Nassif A, Moslehi H, Le Gouvello S, Bagot M, Lyonnet L, Michel L, et al. Evaluation of the potential role of cytokines in toxic epidermal necrolysis. J Invest Dermatol 2004; 123:850-5. 123. Posadas SJ, Padial A, Torres MJ, Mayorga C, Leyva L, Sanchez E, et al. Delayed reactions to drugs show levels of perforin, granzyme B, and Fas-L to be related to disease severity. J Allergy Clin Immunol 2002;109:155-61. 124. Gaultier F, Ejeil AL, Igondjo-Tchen S, Dohan D, Dridi SM, Maman L, et al. Possible involvement of gelatinase A (MMP2) and gelatinase B (MMP9) in toxic epidermal necrolysis or Stevens-Johnson syndrome. Arch Dermatol Res 2004;296: 220-5. 125. Paquet P, Pierard GE. Keratinocyte injury in drug-induced toxic epidermal necrolysis: simultaneous but distinct topographic expression of CD95R and calprotectin. Int J Mol Med 2002;10:145-7. 126. Lerner LH, Qureshi AA, Reddy BV, Lerner EA. Nitric oxide synthase in toxic epidermal necrolysis and Stevens-Johnson syndrome. J Invest Dermatol 2000;114:196-9. 127. Friedmann PS, Lee MS, Friedmann AC, Barnetson RSC. Mechanisms in cutaneous drug hypersensitivity reactions. Clin Exp Allergy 2003;33:861-72. 128. Hardman JG, Limbird LE. Goodman and Gilmans: The Pharmacological basis of therapeutics. 9th ed. New York: McGraw-Hill; 1996. 129. Wilkinson GR. Drug metabolism and variability among patients in drug response. N Engl J Med 2005;352:2211-21. 130. Knowles SR, Uetrecht J, Shear NH. Idiosyncratic drug reactions: the reactive metabolite syndromes. Lancet 2000;356: 1587-91. 131. Knowles SR, Shapiro LE, Shear NH. Reactive metabolites and adverse drug reactions: clinical considerations. Clin Rev Allergy Immunol 2003;24:229-38.
132. Kumar A, Edward N, White MI, Johnston PW, Catto GR. Allopurinol, erythema multiforme, and renal insufficiency. BMJ 1996;312:173-4. 133. Hande KR, Noone RM, Stone WJ. Severe allopurinol toxicity. Description and guidelines for prevention in patients with renal insufficiency. Am J Med 1984;76:47-56. 134. Temesgen Z, Beri G. HIV and drug allergy. Immunol Allergy Clin North Am 2004;24:521-31. 135. Smith KJ, Skelton HG, Yeager J, Ledsky R, Ng TH, Wagner KF. Increased drug reactions in HIV-1-positive patients: a possible explanation based on patterns of immune dysregulation seen in HIV-1 disease. The Military Medical Consortium for the Advancement of Retroviral Research (MMCARR). Clin Exp Dermatol 1997;22:118-23. 136. Mylonakis E, Vittorio CC, Hollik DA, Rounds S. Lamotr