Embed Size (px)
Citation preview

228
TEMPORAL LOBE EPILEPSYBy NEIL GORDON, M.D., M.R.C.P., M.R.C.P.E.
Senior Registrar to the Department of Neurology, St. Mary's Hospital, London, W.2
'Loss of consciousness is not essential for thediagnosis of epilepsy.'--John Hughlings Jackson.IntroductionThe purpose of this paper is to show that,
however varied and complex seizures arising in thetemporal lobes may be, there are many featuresin the clinical picture which are sufficientlycharacteristic to suggest the correct diagnosis.This diagnosis has become of increasing import-ance from the point of view of management andtreatment; partly because temporal lobe epilepsymay be the presenting symptom of some under-lying lesion such as a tumour, and partly becausemedical treatment presents particular problemsof its own. However, it is the bizarre form whichthese attacks may take that often leads to diffi-culties in diagnosis.The attacks often take unusual forms owing to
the complex functions of the temporal cortex andnot to any fundamental difference from othertypes of focal epilepsy. The term psychomotorepilepsy is frequently used to describe seizuresof this kind, but epilepsy arising in other parts ofthe cortex or even from the diencephalon, mayalso be classified under this heading. This will beespecially so if the fits are associated with automat-ism and therefore the term cannot be consideredsufficiently specific. The same criticism maybe applied to such terms as 'epileptic equivalents,''psychic variants,' and 'ictal automatism.'
In many patients with this type of epilepsy theelectro-encephalogram will show at one time oranother that the attacks are associated withelectrical discharges from one or other temporallobe and in some a definite lesion will be demon-strated in this part of the cortex. As in othertypes of focal epilepsy the discharge may remainconfined to a small area or spread widely. In theformer case the nature of the attack will tend tobear some relation to the normal function of thearea of the cortex involved and in the latter, ifthe spread is not too rapid, there may be an' aura'
preceding a generalized convulsion which gives asimilar clue to the site of the origin of thedisturbance.
In any focal epileptic fit there may be bothpositive and negative aspects contributing to thefinal form of the attack. Part of the patient'sexperiences or actions may bear a relationship tothe normal functions of the area of the cortexinvolved and constitute the positive aspects, andpart may be the result of the limited integrationof the rest of the brain which may be termed thenegative aspects. For example, in a focal fitarising in the motor cortex there may be clonicmovements involving the thumb and, at the sametime, the patient will be unable to use that thumbvoluntarily for as long as the fit lasts; because anypart of the cortex occupied by an epileptic dis-charge will be temporarily out of action as far asnormal function is concerned. In fits arisingin the temporal lobe the same factors applyalthough in a more complex form. The positivefeatures may manifest themselves as unpleasantsmells, visual or auditory hallucinations and vertigowhilst the negative aspects of these fits are oftendramatically demonstrated in the automatismwhich may constitute such a large part of them.Automatism is presumably common in this type ofepilepsy because the temporal cortex, althoughconcerned with many of the more complexfunctions of the brain, is not essential to theperformance of simple and stereotyped actions.
In a series recorded by Lennox in 195I, 63 percent. of patients with temporal lobe epilepsy gavea history of grand mal as well of focal fits andpatients such as these may be able to recall that theaura of the major attacks is similar to the minorseizures from which they also suffer. Thesewarnings may consist of positive features such asolfactory hallucinations or, more rarely, of onlynegative ones. In the latter case a period ofautomatism will precede the onset of a generalizedconvulsion, although this fact may only be elicitedif it is possible to interview a witness.
copyright. on July 26, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.33.379.228 on 1 May 1957. D
ownloaded from

May 1957 GORDON: Temporal Lobe Epilepsy 229
Clinical PictureThe varied clinical manifestations of these
seizures are difficult to classify but for the purposesof description they fall roughly into three mainclasses: motor, sensory and psychic. No moredefinite classification has been attempted as it isnot intended to cover all the possible manifesta-tions of seizures arising in the temporal lobes, butonly to stress their variability and those particularfeatures on which a clinical diagnosis of this typeof epilepsy may be made. For instance, abdominalwarnings are not considered as they have littlelocalizing value. Examples have also been con-fined to those of which the author has had personalexperience.The motor features may be exceedingly brief and
consist of only a generalized tonic contraction of themuscles,' as opposed to the clonic contractionssometimes associated with the minor epilepticattacks apparently arising in deep mid-linestructures. Other patients give a history ofsuddenly falling unconscious without warning.
In other attacks the motor manifestations maybe prolonged and consist of co-ordinated and evenskilled movements, and these do not differ fromthose seen in automatism occurring in any othertype of epilepsy. During these episodes thepatients may perform a few confused movementswhich are not even purposive, or they may carryout co-ordinated movements although in such away that even the inexpert eye can recognize thatsomething is wrong. However, they may act inwhat appears to be a normal manner to all buttheir closest friends. In the latter type of attackthey may drive a car or continue to perform somedetailed aspect of their work with little loss oftheir usual skill. The patients often becomeaggressive if they are restrained during theseattacks. The reason that they are unable to recallwhat has happened during these periods is nodoubt related to the fact that parts of the temporalcortex are not being used for normal integrativefunctions and the temporal lobes appear to beessential for the laying down of memory patterns.The sensory type' of seizure arising in the
temporal lobe is characterized by a distortion of anormal sensation of one kind or another. Thepatient may complain of a strange smell or tastewhich is usually unpleasant. If the aura isfollowed by smacking of the lips or sucking thiswill occur during the period of amnesia as it is amanifestation of automatism and informationabout it will have to be obtained from witnesses.Illusions of perception occur and objects looked atmay suddenly become smaller or larger or mayalter in shape. Visual hallucinations are notuncommon and are often associated with a feelingof familiarity or of impending disaster. They
may take the form of people's faces or of scenesand occasionally the patient may apparently bewatching himself perform some action, a so-calledheautoscopic hallucination. Auditory hallucina-tions also occur in this type of seizure and varyfrom discordant sounds to voices or snatches ofmusic. The voices may be impersonal or recog-nized as those of friends or relatives and the musicnormally consists of a familiar tune. Sounds mayalso appear to be softer or louder than normal.Occasionally these attacks commence with intensevertigo which may at first be thought to belabyrinthine in origin, although usually in thesepatients the vertigo is of very brief durationespecially if it is associated with unconsciousness.Finally proprioceptive sensations are sometimesdistorted and patients may complain that a part oftheir body feels abnormal in size or shape.The psychic aspects of these fits are equally
varied. The patient may be aware of compulsivethoughts or interference with his thoughts duringthem. Different emotional feelings occur andthese may constitute the whole episode (Williams,1956). Perhaps most commonly the patientcomplains of attacks of fear which come on for noparticular reason and stop and start with un-explained suddenness. As with other sensationsand feelings produced by the epileptic disturbancesunderlying these attacks it is in some way ab-normal and the patients are frequently at a loss forwords to describe exactly what they do feel. Thismay be due to the fact that the experience thepatient is trying to put into words is a mixture ofsensations arising from an abnormal stimulus andnot one encountered in normal life. The feelingof fear may be so intense as to cause the patient torun away in panic although afterwards he may haveno recollection of what happened. The dejai vuphenomenon has already been mentioned and thisfeeling of familiarity is sometimes the featurewhich impresses the patient most during hisattacks and in fact may be their only manifestation.Conversely there may be a vivid sensation ofstrangeness and this may apply to objects, scenesor parts of the patient's own body. When theenvironment is affected it may seem to the patientthat he is asleep and dreaming.The fact that the temporal lobe of the dominant
hemisphere is intimately concerned with speechfunction makes it inevitable that epileptic dis-charges in this lobe will cause transient attacks ofdysphasia, because, as has already been stressed,such a discharge in any part of the cortex willprevent it being used normally. Transientdysphasia may occur in association with some ofthe other varieties of temporal lobe epilepsy or onits own. It has been considered separately as itmay also be the manifestation of fits arising in other
copyright. on July 26, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.33.379.228 on 1 May 1957. D
ownloaded from

230 POSTGRADUATE MEDICAL JOURNAL May 1957
parts of the cortex. The patients complain that intheir seizures they cannot understand what is said tothem or cannot utter the words they wish to andwitnesses state that if a patient is talking when afit occurs his speech becomes confused and some-times unintelligible.
Before leaving the clinical aspects of this subjectit should be mentioned that patients suffering fromtemporal lobe epilepsy are particularly liable todisorders of emotion and behaviour. Theybecome depressed, tense and anxious, and some-times these symptoms are worst when the fits areoccuring less frequently than usual. It is notuncommon for a patient to state that on his presenttreatment the incidence of his attacks has beengreatly reduced but that he does not feel so well inhimself, and that should one occur he then feelsbetter again for a while. These patients may alsobe difficult to handle and have various defects ofadaptation in their everyday lives.' They oftenfail to take the treatment prescribed, develop agrudge against society, do not hold jobs for long ata time and tend to have a quarrelsome nature.If their attacks continue for many years thepatients may begin to present a clinical picturewhich is virtually indistinguishable from paranoidschizophrenia.' This first of all occurs in episodesbut may become more and more protracted, so thatits occurrence is always of grave prognostic import.As this condition develops the fits sometimesbecome less frequent or even stop altogether.
It is evident that in a certain number of patientsdisorders of behaviour may be due to a morecontinuous epileptic discharge from the temporallobes, particularly if these disorders are episodic,starting and stopping with unexplained sudden-ness. It is well established that focal epileptic fitscan continue without interruption for prolongedperiods, a condition referred to as focal status, andtemporal lobe seizures are no different in thisrespect from any other type of focal fit. Forexample the patient's complaint may be of a con-tinuous feeling of familiarity which lasts for hourson end and affects whatever he may be doing sothat it all seems to have happened before. Onepatient was watching a football match during sucha prolonged episode and was convinced that hecould foretell what was going to happen next, andthought that when he passed this information onto the crowd they became annoyed because he wasspoiling the game for them. Any of the otherpositive aspects of temporal lobe fits might occurin this way and modify the patient's behaviour.Automatism may also be prolonged due to thetemporal lobe being out of action because it isoccupied by a continuous epileptic discharge orbecause it takes time to recover its normal functionafter such a discharge has stopped. The most
satisfactory proof that such episodes are due to-focal status in one temporal lobe is the findingduring' them of abnormalities in the electro-encephalogram confined'to that area.
DiscussionIt will be seen that temporal lobe epilepsy can
be of almost infinite variety as motor, sensoryand psychic phenomena may occur alone or in anykind of combination. The patient may becompletely amnesic for some attacks and often forlong periods, while other patients can describetheirs in the minutest detail. The description ofthe attacks will often suggest that their origin iswithin the temporal lobes but this is not invariablyso. For example the patient may have no memoryof what happens during a fit so that his complaintis of a brief loss of consciousness and these'pseudo-lapses' of temporal lobe origin may bedifficult to distinguish from petit mal attacksarising from the diencephalon. Fits in which thepatient falls limply to the ground without warningor has a brief generalized tonic contraction or inwhich he experiences some peculiar sensation hecannot put into words are also apt to causeconfusion.The special problems that arise in the manage-
ment of temporal lobe seizures make it particularlyimportant to establish this diagnosis, an importancewhich is increased by the frequency with whichthis type of epilepsy occurs. For instance in alarge series of epileptic patients studied byLennox (1951) over 20o per cent. had fits arisingin the temporal lobe. In the first place it mayhave to be established that the patient is reallysuffering from focal epilepsy and this may presentdifficulties if a generalized convulsion has neveroccurred and especially if the attacks arecharacterized by automatism.When the history is more than usually bizarre
the patient is sometimes thought to be sufferingfrom hysteria or some type of psychosis. The pasthistory is of obvious importance as it may revealhysterical traits or other phychotic symptoms,or on close questioning of the patient and hisrelatives a history of fits in years gone by may beelicited. The nature of the attacks themselves,the fact that they always run to the same patternsand the normal personality of the patient betweenthe attacks would all help to confirm the diagnosisof epilepsy. -The development of a schizophrenic-like condition in long-standing temporal lobeepilepsy has already been mentioned and this maybe particularly confusing if the patient is firstseen at this late stage of his illness.
Sometimes hypoglycaemia, which may be dueto a functioning islet-cell tumour, gives, rise toperiods of confused behaviour of which the patient
copyright. on July 26, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.33.379.228 on 1 May 1957. D
ownloaded from

May 1957 GORDON: Temporal Lobe Epilepsy 23I
'1 V-#
I/ 79
----------/ --8~~-·-(~- ------\ ' ,>6 'ePJ---/d /2 t'C~
/\/8 /- Xh~1~rVr\J~-\kJY* Z t =-8SO1v = /Cm.
SPeed Jcm\sec.
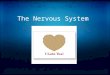
FIG. I.-Spiking activity occurring from the left anterior temporal region during light sleep.
has little or no recollection. Epileptic fits, evenof a focal nature, may also be precipitated by alowered blood sugar. However, for practicalpurposes, there will be none of the positive featuresof temporal lobe epilepsy, the hypoglycaemicattacks will tend to be prolonged and associatedwith sweating, and there may be a definite relation-ship between their onset and fasting or the takingof a meal some three hours previously.
If it is concluded that the patient is sufferingfrom epilepsy, the site of origin of the fits has stillto be decided upon. The distinction between the' pseudo-lapses ' of temporal lobe origin and petitmal has already been mentioned. Petit mal statusis another condition which can cause prolongedperiods of confusion associated with automaticbehaviour. However, it is almost confined tochildren among whom temporal lobe attacks arerelatively rare. Automatism occasionally occursin epileptic fits arising in other parts of the cortex,especially the frontal lobes, but this is such a rareoccurrence that it seldom adds to the difficultiesof diagnosis. It must also be stressed thatpatients with temporal lobe epilepsy may presentwith only grand mal, although a history may beobtained later from a witness of some episodespreceding the generalized convulsions that wouldsuggest the attacks had a focal origin in thetemporal lobes. It is well known that the patient'smemory of the aura of these attacks may quicklyfade and if they can be questioned within an houror so of a fit they may be able to recall details ofconsiderable diagnostic import.There are other small points in the clinical
history which may help in diagnosis. As will bementioned later the value of sleep as a method ofactivation in the electro-encephalographic studyof temporal lobe seizures is well established, the
focal abnormalities often appearing only duringthe stage of drowsiness (Gibbs and Gibbs, I947).These observations may be linked to the clinicalfact that patients with epilepsy of this kindfrequently suffer from their most severe attacksduring the night. One sometimes obtains ahistory that for a number of years a patient hassuffered from brief attacks during the day whichmay not have been recognized as epileptic andthen major convulsions start to occur duringsleep and this leads to the patient seeking medicaladvice.Temporal lobe epilepsy tends to be commoner
among adults but may occur at any age. As withother types offocal epilepsy it will often be sympto-matic of some underlying disease, so that if forinstance 'minor' epileptic. attacks occur aftercerebral trauma, one should always suspect thepossibility oftemporal lobe epilepsy even in a veryyoung child. Occasionallymore than one memberof a family may suffer from this type of epilepsy,when even the exact pattern of the fit may berepeated in two or more relatives. Genetic factorsmay play a part but birth injuries in siblings arenot uncommon if the mother's pelvis is deformedin any way.
In the majority of cases the diagnosis of thesefits will be made on the clinical history but whenfor one reason or another this is inadequate, specialinvestigations are often of value. This is parti-cularly true of the electro-encephalogram, whichmay be of mQre help in this kind of epilepsy thanin most others. The specific seizure discharge isthe occurrence of well marked focal abnormalitiesin the temporal regions. These may consist ofirregular slow waves or of random spikes andsharp waves. However, the record taken whenthe patient is awake is frequently normal or it may
copyright. on July 26, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.33.379.228 on 1 May 1957. D
ownloaded from

232 POSTGRADUATE MEDICAL JOURNAL May 1957
only show a non-specific dysrhythmia, and then itwill be necessary to try the effect of variousmethods of activation. The injection of sub-stances like bemegride (megimide) may bring outfocal abnormalities but the procedure of mostvalue is to take an electro-encephalogram while thepatient is going to sleep and during a period ofdeep sleep (Gibbs and Gibbs, 1947). Spikes andother focal abnormalities may then appear, mostfrequently as the patient becomes drowsy, butsometimes only when he is in a deep sleep (Fig. I).The origins of many of the epileptic dischargesfrom the temporal cortex are a considerabledistance from the scalp, for example the dischargeswhich occur in the hippocampus and accompanyolfactory hallucinations. There is no doubt thatthe electro-encephalograms from such cases forma large percentage of the routine recordings whichare either normal or show generalized and non-specific abnormalities. In patients who may haveepileptogenic foci on the under surface of thetemporal lobes positive focal findings may beobtained if sphenoidal electrodes are used. Theseare placed below the foramen ovale; a needle,insulated except at its tip, being inserted just infront of the ear below the zygomatic arch(Pampiglione and Kerridge, 1956). A record isthen taken with the patient awake and asleep.When the diagnosis of temporal lobe epilepsy
has been established the implications are the sameas for any other type of focal epilepsy. Eachindividual case must be judged on its merits butmore often than not further investigations will beindicated in order to try and exclude the presenceof an underlying lesion which might be amenableto surgery. These will include X-ray of theskull, air studies and arteriography.
In a large number of patients suffering fromepilepsy of every kind no definite actiology for theseizures is discovered and temporal lobe epilepsyis no exception to this. A history of cerebraltrauma is not infrequently obtained from patientswith this type of epilepsy, the interval between theaccident and the onset of the fits varying withinwide limits. The hippocampal gyrus appears tobe particularly liable to be affected in closed headinjuries. This may be due to generalized cerebraloedema causing herniation of the hippocampusthrough the tentorial opening with resultingdamage to this area of the brain through inter-ference with its blood supply. A similarmechanism possibly operates in birth injuries,and it has been suggested that the lesion causedby the vascular insufficiency may ripen into anepileptogenic focus in later life (Earle et al., I953).Some patients give a history of generalized
convulsions for many years and then, in latemiddle age, begin to experience minor attacks of
the kind described in this paper. A possibleexplanation of this course of events is that theanoxia associated with the major convulsionscauses damage to parts of the temporal cortexparticularly sensitive to oxygen lack and soproduces a new discharging focus.
Air encephalography may reveal evidence ofcerebral atrophy or of an expanding lesion such asa glioma or meningioma in the temporal regions.Arteriography may also show abnormalities com-patible with the presence of a tumour in theseareas or it may reveal an aneurysm or angiomawhich is interfering with the function of thetemporal cortex. However, such pathologicalconditions have no particular predilection for thetemporal lobes and therefore will not be consideredfurther.Temporal lobe epilepsy is notoriously difficult
to treat, but the introduction of some of the newerdrugs has undoubtedly improved the situation.When, after any necessary investigations havebeen carried out, it is decided that medicaltreatment should be started a choice will have tobe made between the various drugs available. Inthe first place it is worth while trying the effect ofphenobarbitone or one of the closely relatedcompounds, as a certain number of patients mayrespond satisfactorily. If they do not, phenytoinsodium, either alone or combined with pheno-barbitone, should be given, gradually increasingthe dose of both drugs to the limit of tolerance.Then, after a reasonable trial, it may be decidedthat further alterations are indicated. The controlof the fits can sometimes be improved by graduallysubstituting primidone for the phenobarbitone orMethoin for the phenytoin sodium. Methoin ismore liable to cause toxic reactions than the otherdrugs so far mentioned. Skin rashes, particularly ofa morbilliform kind, may occur, and deaths havebeen recorded from more generalized allergic re-actions and from aplasia of the bone marrow (Jones,I95I). It is therefore necessary to keep patientsunder close observation while on this drug, theaverage dose of which is 6 g. a day for an adult.Finally, if the attacks have not responded to any ofthese methods of treatment it is worth-while tryingthe effect of phenacetylurea. This may be usedalone or in combination with any of the other anti-convulsants which may have already been found tobe of some help. It also has dangerous side-effectsand deaths have occurred from hepatitis andaplastic anaemia (Liversedge et al., I952),(Simpson et al., 1950). Therefore, as with anyother potentially dangerous drug, the patientsshould be warned to, report any illness, butespecially any gastro-intestinal upset, and to stopthe tablets if they are unable to see a doctorimmediately. Routine blood counts may show
copyright. on July 26, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.33.379.228 on 1 May 1957. D
ownloaded from

May 1957 GORDON: Temporal Lobe Epilepsy 233
A new monograph entitledPULMONARY COMPLICATIONS|OF ABDOMINAL SURGERYby ANTHONY R. ANSCOMBE,M.S. (Lond.), F.R.C.S. (Eng.)Senior Lecturer in Surgery andHonorary Consultant, St. George's HospitalSurgeons, anaesthetists and physicians, who have care of patients after operation, cannot fail to bestimulated by the problem of post-operative pulmonary complications as described in this book. These all-too-frequent complications are shown to be due to the effect of the abdominal operation on the mechanicalfunction of the lungs: an effect which may be so severe as to cause the death of some patients inthe immediate post-operative period. A simple method of estimating pulmonary function is described, x + 121 pp.and much evidence produced to show that such an estimation is essential in patients before an abdominal 37 illustrationsoperation. (1957) 20s. net
An indispensable guideMEDICAL ETHICSedited by MAURICE DAVIDSOND.M. (Oxon.), F.R.C.P. (Lond.)Consulting Physician, Brompton HospitalThe contributors to this volume are distinguished members of the medical and other learned professions,whose reputation in the world of scholarship and learning must command general respect. Each chapter x + 165 pp.deals with those fundamentals of conduct which rest upon the collective philosophy and wisdom of the 1 illustrationages, about which much has been said and written and ofwhich the profession was never in greater need than (1957) 20s. netat the present day. Ready shortly
Lloyd-Luke (Medical Books) Ltd., 49, Newman Street, W.I
that the activity of the bone marrow is becomingdepressed and examination of the urine forurobilinogen may give warning of the onset ofhepatitis. These tests, however, are of secondaryimportance and the greatest safeguard is for thepatient to see a doctor as soon as he feels ill.It is best to start with a small dose such as half agram twice a day and gradually increase this overa period of several weeks. An average dose of2 to 3 g. a day is adequate for most adults.
If due precautions are taken, a trial of phen-acetylurea is certainly justifiable when frequentfits are still occurring in spite of intensive treatmentwith other drugs. Some patients obtain a strikingdegree of relief from it, their attacks ceasing orbecoming infrequent; and often both the patientand his relatives remark how the personality hasgreatly improved since taking it. Unfortunatelythis is not always so and sometimes the phen-acetylurea has to be stopped owing to the patientdeveloping a psychosis. This is usually due tothe toxic effect of the drug, but may be occasionallyrelated to the liability of some patients to developsuch states- when their attacks do become in-frequent. When medical treatment has failed to
control the fits and the electro-encephalogramreveals well-defined focal abnormalities in theanterior part of one temporal lobe the question ofsurgical excision of the epileptogenic focus shouldbe considered, even if other investigations haveshown no definite evidence of a focal pathology.
SummaryA review is given of some of the clinical mani-
festations of temporal lobe epilepsy. Specialaspects of this condition are then discussed,including diagnosis, aetiology and treatment.
BIBLIOGRAPHYEARLE, K. M., BALDWIN, M., and PENFIELD, W. (1953),A,rch. Neurol. Psychiat. (Chicago), 69, 27.GIBBS, E. L., and GIBBS, F. A. (I947), Proc. Ass. Res. nerv. ment.
Dis., 26, 366.JACKSON, H. (I93I), 'Selected Writings of John Hughlings
Jackson,' Hodder and Stoughton, London.JONES, D. P. (I95I), Brit. med. .7., i, 64.LENNOX, W. G. (xI95), Neurology, i, 5.LIVERSEDGE, L. A., YATES, P. O., and LAMPERT, H. (1952),
Lancet, i, 242.PAMPIGLIONE, G., and KERRIDGE, J. (x956), 7. Neurol.
Neurosurg. Psychiat., 19, II7.SIMPSON, T. W., WILSON, F. B. J., and ZIMMERMAN, S. L.
(I95o), Ann. intern. Med., 32, x224.WILLIAMS, D. (x956), Brain, 79, 29.
copyright. on July 26, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.33.379.228 on 1 May 1957. D
ownloaded from