Embed Size (px)
Citation preview

This article was downloaded by: [University of Auckland Library]On: 08 October 2014, At: 17:31Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office:Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Aging & Mental HealthPublication details, including instructions for authors and subscriptioninformation:http://www.tandfonline.com/loi/camh20
Televisits: Sustaining long distance familyrelationships among institutionalized eldersthrough technologyM. A. Mickus a & C. C. Luz aa Department of Psychiatry , Michigan State University , East Lansing,Michigan, USAPublished online: 09 Jun 2010.
To cite this article: M. A. Mickus & C. C. Luz (2002) Televisits: Sustaining long distance familyrelationships among institutionalized elders through technology, Aging & Mental Health, 6:4, 387-396, DOI:10.1080/1360786021000007009
To link to this article: http://dx.doi.org/10.1080/1360786021000007009
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”)contained in the publications on our platform. However, Taylor & Francis, our agents, and ourlicensors make no representations or warranties whatsoever as to the accuracy, completeness, orsuitability for any purpose of the Content. Any opinions and views expressed in this publication arethe opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis.The accuracy of the Content should not be relied upon and should be independently verified withprimary sources of information. Taylor and Francis shall not be liable for any losses, actions,claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arising out ofthe use of the Content.
This article may be used for research, teaching, and private study purposes. Any substantialor systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, ordistribution in any form to anyone is expressly forbidden. Terms & Conditions of access and usecan be found at http://www.tandfonline.com/page/terms-and-conditions

Introduction
Social relationships and support bear tremendousin� uence on personal health and well-beingthroughout the entire life course. Although slightvariations across racial, ethnic, and cultural groupsexist, most people continue to value and bene� t fromreciprocal interactions with family and friends in laterlife (Atchley, 1997; Levitt, 2000; Sherman et al.,2000; Troll, 1999). Not only are psychosocial needsmet by such relationships but also are needs for phys-ical care and many instrumental activities of dailyliving. The majority of care of the elderly in theUnited States is provided through informal socialnetworks and kin, primarily women (Abel, 1991;Stone et al., 1987;Ward, 1993) even at great personalcosts (Hooyman & Kiyak, 1996; Ward, 1993; Wood,1994). This is true despite changing demographicsthat include increased life expectancy and morewomen than ever in the work force (Hooyman &Gonyea, 1999; Moen et al., 1994).
Just as positive social relationships and environ-ments can promote health and life satisfaction (Glasset al., 1999; Minkler et al., 2000; Seeman, 2000), alack of such social relationships and support mayhave grave consequences. Research indicates thatthere is an association between social isolation and
increased mortality as well as morbidity, particularlydepression (Dalgard & Lund, 1998; Frasure-Smith et al., 2000; House et al., 1990; Hybels et al., 2001;Krishnan et al., 1998; Seeman, 2000). Moreover,older people with no or few kin are more likely toenter a nursing home (Russell et al., 1997; Pearlman& Crown, 1992) where isolation is compounded(Diamond, 1992; Henderson & Vesperi, 1995) andrates of depression are high. The research of Weyereret al., (1995) indicated that the lack of social supportvia relatives and friends was a signi� cant predictor ofdepression eight months after admission to a nursinghome.
For many family members as well, nursing homeplacement and related depression creates emotionaldistress. It may engender feelings of anxiety, failure,guilt and loss of control (Drysdale et al., 1993;Kellet, 1999; Rodgers, 1997). Most individualsutilize a nursing home only as a last resort, when allinformal and community care resources have beenexhausted. The moral dilemmas following nursinghome placement may be compounded by limitedabilities of residents and family members to visit ona regular basis. Many family members are elderlythemselves and have physical dif� culty engaging inregular visits to a nursing home. Others live in locations that are geographically distant from the
1111111
Aging & Mental Health 2002; 6(4): 387–396
ORIGINAL ARTICLE
Televisits: sustaining long distance family relationships amonginstitutionalized elders through technology
M. A. MICKUS & C. C. LUZ
Department of Psychiatry, Michigan State University, East Lansing, Michigan, USA
AbstractThe role of social support in the health of older persons is well documented. This support is particularly important forisolated nursing home residents.The purpose of this study was to test the feasibility of using low-cost videophones to enhancecommunication between nursing home residents and their families. Ten pairs of residents and family members receivedvideophones and engaged in regular televisits for six months. All participants completed brief survey instruments prior toand after the study period to determine the effects of the televisits on the frequency and quality of contacts. A post-studysurvey assessed ease and satisfaction with using videophones. Findings include identi� cation of technical and design prob-lems, possible solutions, factors affecting actual use of equipment, and conditions under which bene� ts of use may beoptimal. Categories for estimating potential actual users are suggested. Importantly, the study demonstrates that videophonescan be used successfully by a wide range of frail nursing home residents and can enhance social interactions, regardless ofdistance. Affordable videophone technology offers the potential for reduced isolation among institutionalized elders andothers with distance and mobility barriers.
Correspondence to: Maureen A. Mickus, Department of Psychiatry, Michigan State University, East Lansing, Michigan,48824, USA.
Received for publication 1st October 2001. Accepted 11th March 2002.
ISSN 1360-7863 print/ISSN 1364-6915 online/02/04387–10 © Taylor & Francis LtdDOI: 10.1080/1360786021000007009
Dow
nloa
ded
by [
Uni
vers
ity o
f A
uckl
and
Lib
rary
] at
17:
31 0
8 O
ctob
er 2
014

nursing home.Yet most individuals wish to maintaintheir social relationships and doing so may serve as a buffer to the impact of losses in later life (Kammer,1994; Park & Vandenberg, 1994; Penninx et al., 2000;Pruchno & Kleban, 1993; Thompson et al., 1993).It is thus important to explore new and effectivemethods for supporting positive relationships be-tween nursing home residents and their families andfriends.
Teleconferencing is rapidly becoming an effectivemedium for the delivery of information in the healthcare arena, especially in psychiatry and home care(Galliene et al., 1993; Jones, 1999; Redford &Whitten, 1997; Rothchild, 1999; Zaylor, 1999). Themajority of these interactions are between patientsand providers or between providers for purposes ofdiagnosis, treatment, and follow-up care. It is notknown if, and how, individuals might use such tech-nology for social support. This pilot study, known as‘Televisits’, used teleconferencing to link nursinghome residents and their families for increased socialinteraction. It is the � rst known study to use videotechnology with a nursing home population for socialrather than strictly clinical use. The study is alsounique in that it involved frail residents manipulatingthe equipment themselves. Televisits was based onthe central idea that telephone contact between resi-dents and their families would be more rewarding ifenhanced with visual images of each other.The basicresearch questions addressed were:
� Are nursing home residents capable of using suchequipment themselves?
� Do televisits increase or enhance social interac-tions, particularly between residents and familymembers who are geographically distant?
� What is the level of satisfaction with using avideophone among residents and familymembers?
Satisfaction levels are important to ascertain becauseeven if a resident is capable of using the equipment,actual usage is not likely if satisfaction is low. Thenumber of therapeutic possibilities available topeople may dramatically increase by demonstratingthe extent to which nursing home residents, or anyisolated persons, can independently and willingly usecommunication technology.
Methods
The subjects for this study were drawn from threeskilled nursing facilities in the mid-Michigan area.Selection criteria speci� ed that the resident presentwith no or mild cognitive impairment as indicated by the Mini-Mental Status Examination (MMSE)(Folstein et al., 1975).The research team anticipatedthat residents with moderate impairment might becapable of videophone use. Additional criteriaincluded having an active telephone line, and
identifying a family member willing to participate inthe study. Particular consideration was given to residents who had a clinical diagnosis of depressionin the medical charts and to pairs separated by physical distance or other barriers to regular in-person visits. Both resident and family member hadto be willing to engage in televisits during otherwiseregular phone contacts for six months and to sign an informed consent to participate in the study.Fifty-eight residents were identi� ed by facility socialservice staff as being potential subjects and contactedin person by a member of the research team. Theresearcher explained the purpose of the study anddemonstrated use of the equipment. During thedemonstration, one unit was used and consequentlythe resident could only see their own image. Still,the researcher was able to show how to install and use the equipment and to convey how a familymember’s image would appear during video trans-mission.
Forty-eight residents were eliminated because theydid not meet all criteria. Of these, 10 residents did nothave an active phone line and six did not have a diag-nosis of depression. The remainder either were notwilling to participate in the study or did not have afamily member that was willing to participate. Theprimary reasons given for not wanting to take partincluded not feeling up to it, having too much tohandle already, and thinking it was not necessary.Several residents did not want to ask family membersto participate as ‘they are too busy and can’t be both-ered’. None of the residents declined participationbecause of being intimidated by the technology.Ultimately, 10 pairs of residents and family memberswere selected to receive the videophone equipment.They all signed a consent form to participate and theresearcher administered the Geriatric DepressionScale (Yesavage et al., 1983) to each resident. Despitea clinical diagnosis of depression, none of the 10 resi-dents screened positive for depression or expressedsymptoms of depression. Consequently, depressionoutcomes related to the intervention could not beexamined.
Once the sample was selected, a member of theresearch team installed and programmed a video-phone in the room of all participating residents andrepeated instructions and demonstrations on usageprior to the � rst video contacts. Considerable atten-tion was given to assisting subjects with operating thevideophones. The units were mailed to familymembers with instructions. Two of the familymembers stated they could install the units them-selves and did so without dif� culty. Eight familymembers requested assistance with installation andprogramming prior to the � rst video contact, whichthe researcher provided. If the family member waslocal, the researcher made a home visit. Long-distance family members were provided with detailedinstructions and technical assistance via telephone.All of the participants required some assistance with
388 M. A. Mickus & C. C. LuzD
ownl
oade
d by
[U
nive
rsity
of
Auc
klan
d L
ibra
ry]
at 1
7:31
08
Oct
ober
201
4

the � rst video transmission which the researcherprovided either by being present at the nursing homeat the time of the � rst video call or by providing step-by-step instructions to the family member bytelephone. In addition, the researcher posted simpleinstructions on the residents’ videophones as re-minders of proper procedures as well as a contactnumber for the research team. The researcher thenreiterated that a study requirement was regular video-phone contacts. Furthermore, family members wereencouraged to use the equipment for regular residentcare conferences. The researcher remained readilyavailable for technical consultation and trouble-shooting throughout the duration of the study.
Given the high workloads of nursing home aides, it was the research team’s intent to minimizestaff involvement in the project. Moreover, thisapproach supported a study aim, which was toexplore how feasible it is for nursing home residentsto use the videophones with minimal assistance.However, the facility charge nurses were noti� ed ofwhich residents were using the equipment and theresearcher’s contact number, both of which wereentered into resident records. In most cases, theresearcher informally showed staff members theequipment and generally how the videophonesworked so that they could provide occasional assis-tance as needed.
The videophones used consisted of a telephonewith a small screen attached that allowed both partiesto see one another in real-time once the videoconnection was activated. The video connectionsoperated through what is referred to as POTS (plainold telephone systems). In other words, subjectsmerely needed to plug into a regular, active phoneline in which case the videophone connection cost nomore than a regular telephone call. The only majorexpense was the one-time cost of purchasing thevideophones. Each unit cost approximately $500.00and two units are required for communication.Relative to other forms of communication tech-nology, this analogue equipment was low-cost, easyto install and program, and utilized neither high-speed digital lines or a personal computer, all ofwhich makes the technology highly accessible to awider range of people.
At approximately one month, the researchercontacted all residents and family members tocon� rm that they were still using the videophonesand to determine if they had any concerns or ques-tions. The researcher contacted all subjects again atfour months to remind them that the study wouldsoon be coming to a close.At this point the researcherasked how well the units were working and addressedtechnical concerns. Participants were able to dropout of the study at any time for any reason.
All subjects completed a brief survey instrumentprior to and immediately following the study periodto determine the frequency and quality of contacts.The surveys were mailed to family members to
complete and administered to residents by a memberof the research team. This pre/post-test instrumentconsisted primarily of Likert-scale questions such as‘How frequently do you visit in person with your rela-tive?’ followed by response choices ranging from lessthan one time per month to two or more times perweek.
An additional post-test survey assessed ease andsatisfaction with using the videophones. Thisincluded a combination of Likert scales and open-ended questions. For example, subjects were asked,‘How would you rate your overall satisfaction withthe videophone?’ and given four response choicesfrom very satis� ed to very dissatis� ed. Theseresponses were collapsed into two categories foranalysis. Subjects were also asked questions such as,‘Did you have any of the following dif� culties in usingthe videophone?’ followed by a list of choices. Finally,open-ended questions were asked such as ‘What didyou like most, and least, about using the video-phone?’ This qualitative feedback improves ourunderstanding of the meaning and value of video-phone use for the subjects and how decisions relatedto use are in� uenced.
Capability of videophone use was de� ned in termsof whether or not pairs of participants continuedusing the equipment for the duration of the study.Pairs were determined incapable if they stoppedprematurely due to severe physical, cognitive, ortolerance limitations that rendered the use of theequipment too dif� cult even with signi� cant support.Again, it is important to recognize the role of satis-faction in whether or not a pair continued to use theequipment. An examination of the impact of capa-bility coupled with level of satisfaction provides amore accurate estimate of actual potential users.Therefore, the range of reasons for discontinuing useand how qualitative differences among them may beinterpreted related to their varied outcomes isaddressed in the discussion section.
Sample description
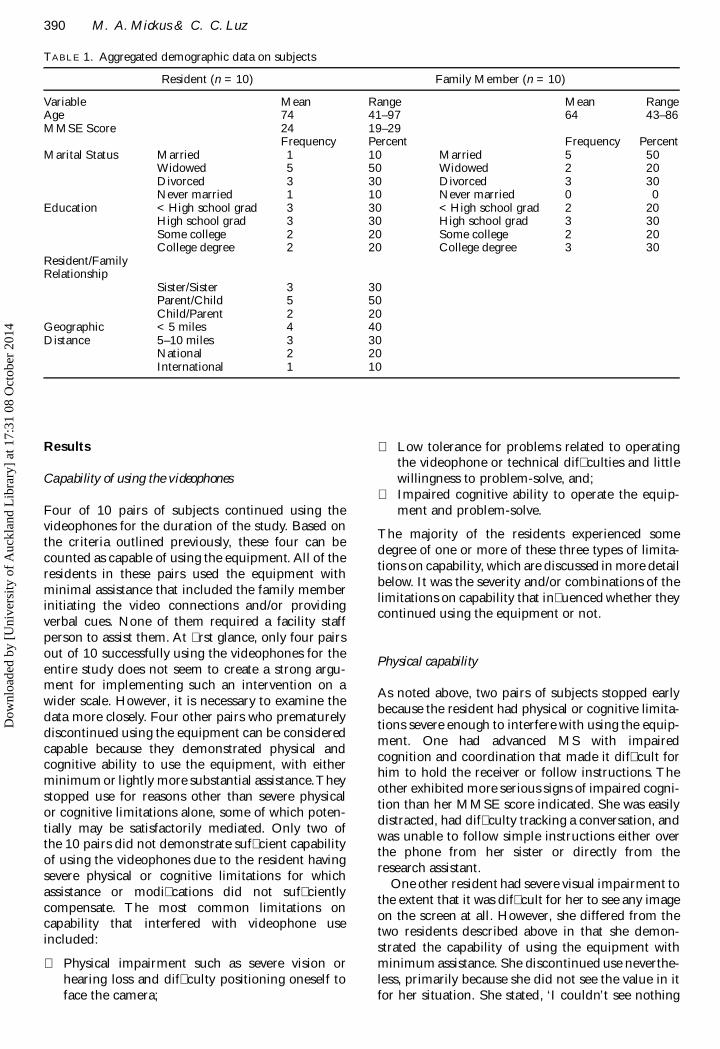
The demographic pro� les of residents and familymembers are illustrated in Table 1. Both groups werecomposed of eight women and two men. All of thestudy participants were of Caucasian descent.Gender and race composites were re� ective of thetotal nursing home population in this area. The twoyoungest residents, ages 41 and 44, both had multiplesclerosis (MS) and were paired with their mothers.One of these mothers lived nearby yet had healthproblems of her own that made regular visits to thenursing home dif� cult. Two other family members,who lived within 10 miles of the nursing home, rarelyvisited because of health and transportation prob-lems. In other words, regardless of distance, morethan half of the pairs had limitations on their abilityto visit in person with one another.
1111111
Televisits with institutionalized elders 389D
ownl
oade
d by
[U
nive
rsity
of
Auc
klan
d L
ibra
ry]
at 1
7:31
08
Oct
ober
201
4
Results
Capability of using the videophones
Four of 10 pairs of subjects continued using thevideophones for the duration of the study. Based onthe criteria outlined previously, these four can becounted as capable of using the equipment. All of theresidents in these pairs used the equipment withminimal assistance that included the family memberinitiating the video connections and/or providingverbal cues. None of them required a facility staffperson to assist them. At � rst glance, only four pairsout of 10 successfully using the videophones for theentire study does not seem to create a strong argu-ment for implementing such an intervention on awider scale. However, it is necessary to examine thedata more closely. Four other pairs who prematurelydiscontinued using the equipment can be consideredcapable because they demonstrated physical andcognitive ability to use the equipment, with eitherminimum or lightly more substantial assistance.Theystopped use for reasons other than severe physical or cognitive limitations alone, some of which poten-tially may be satisfactorily mediated. Only two of the 10 pairs did not demonstrate suf� cient capabilityof using the videophones due to the resident havingsevere physical or cognitive limitations for whichassistance or modi� cations did not suf� cientlycompensate. The most common limitations on capability that interfered with videophone useincluded:
� Physical impairment such as severe vision orhearing loss and dif� culty positioning oneself toface the camera;
� Low tolerance for problems related to operatingthe videophone or technical dif� culties and littlewillingness to problem-solve, and;
� Impaired cognitive ability to operate the equip-ment and problem-solve.
The majority of the residents experienced somedegree of one or more of these three types of limita-tions on capability, which are discussed in more detailbelow. It was the severity and/or combinations of thelimitations on capability that in� uenced whether theycontinued using the equipment or not.
Physical capability
As noted above, two pairs of subjects stopped earlybecause the resident had physical or cognitive limita-tions severe enough to interfere with using the equip-ment. One had advanced MS with impairedcognition and coordination that made it dif� cult forhim to hold the receiver or follow instructions. Theother exhibited more serious signs of impaired cogni-tion than her MMSE score indicated. She was easilydistracted, had dif� culty tracking a conversation, andwas unable to follow simple instructions either overthe phone from her sister or directly from theresearch assistant.
One other resident had severe visual impairment tothe extent that it was dif� cult for her to see any imageon the screen at all. However, she differed from thetwo residents described above in that she demon-strated the capability of using the equipment withminimum assistance. She discontinued use neverthe-less, primarily because she did not see the value in itfor her situation. She stated, ‘I couldn’t see nothing
390 M. A. Mickus & C. C. Luz
TABLE 1. Aggregated demographic data on subjects
Resident (n = 10) Family Member (n = 10)
Variable Mean Range Mean RangeAge 74 41–97 64 43–86MMSE Score 24 19–29
Frequency Percent Frequency PercentMarital Status Married 1 10 Married 5 50
Widowed 5 50 Widowed 2 20Divorced 3 30 Divorced 3 30Never married 1 10 Never married 0 0
Education < High school grad 3 30 < High school grad 2 20High school grad 3 30 High school grad 3 30Some college 2 20 Some college 2 20College degree 2 20 College degree 3 30
Resident/FamilyRelationship
Sister/Sister 3 30Parent/Child 5 50Child/Parent 2 20
Geographic < 5 miles 4 40Distance 5–10 miles 3 30
National 2 20International 1 10
Dow
nloa
ded
by [
Uni
vers
ity o
f A
uckl
and
Lib
rary
] at
17:
31 0
8 O
ctob
er 2
014

on it. It didn’t do me no good.’ She understandablyrated her overall satisfaction as low but she also wenton to say, ‘It would probably be good for lots ofpeople, just not me.’ The severity of her vision lossin� uenced her use. The low value she placed on usemay also have been in� uenced by the fact that shereceived regular face-to-face visits from her son anddaughter-in-law. Had her family been unable to visit,she may have placed more valued on the videophonecontacts.
More mild limitations were compensated for withdesign modi� cations so that use could continue. Forexample, one resident with visual impairment bene-� ted from placing large, bright, raised numbers onthe keypad. Another resident with mildly impairedhearing changed to a phone with volume control andthen proceeded to enjoy televisits with her sister.
Tolerance
Some participants demonstrated an unwillingness toexperiment with various modi� cations such as these.They exhibited a low tolerance for technical problemsor dif� culty with operating the equipment and dis-continued using the equipment rather than try to solvethe problems. All of the pairs experienced at least onetechnical problem including an inability to establish avideo connection, interrupted video connections, sta-tic on the line, no image on the screen, and freezing ofthe image. Most often, the dif� culty could be resolvedwith minimal assistance. However, participants variedin their willingness to try different problem-solvingoptions.They were considered to have low tolerance ifthey had trouble operating the videophones or experi-enced technical problems and consequently quit try-ing after limited, if any, attempts at resolving theproblems. Statements such as the following ones wereindicators of low tolerance. ‘B. was frustrated. I wouldjust say I can’t see you and she’d push some buttonsand she’d be gone . . . I told her to call you but shewouldn’t do it’. Meanwhile, B. said, ‘A. didn’t like it.’These sisters may have enjoyed bene� ts of using thevideophone had their tolerance been higher since A.said she liked to see her sister’s face when the unitworked and B. said, ‘I don’t get to see my sister muchand this was like going to see her.’
Matching of tolerance levels within each pair ofparticipants is depicted in Table 2. This illustratesthat all the pairs in which at least one of the partici-pants demonstrated low tolerance stopped using theequipment prematurely.
It is interesting to note that among all four pairsthat used the equipment for the duration of the study,all participants demonstrated a high tolerance forproblems and a willingness to try various problem-solving strategies. They continued use even whenmore substantial problems occurred, exhibiting littlefrustration and at times appearing to enjoy the chal-lenge. In one other pair, both of the participants
demonstrated high tolerance as well. They stoppedearly nevertheless because the resident’s physicallimitations proved to be too severe to successfullyoperate the equipment. However, they did so onlyafter repeated attempts to resolve the operating andtechnical problems that they were having.These � nd-ings indicate that tolerance may be a powerful vari-able when determining potential use.
Cognitive ability
Lastly, the cognitive ability to actually operate theequipment and problem-solve had signi� cant in� u-ence on success and satisfaction. Three categories ofcognitive ability were constructed based on similari-ties among statements and behavior of participants.These relate to how they operated the equipment, theproblems they experienced, and how they respondedto problems.The � rst group (Independent) consistedof � ve of the twenty participants (25%) who wereconsidered to be able to operate and problem-solveindependently. They contacted the research consul-tant only after trying different strategies on their ownto resolve problems. Quite often their strategiesworked and additional assistance was not required.
The majority of the participants (65%) composedthe second group (Help). They were able to operatethe equipment and/or problem-solve with instructionor assistance from either their partner or someoneelse such as another family member, a nurse, or theresearcher. For example, one participant, who wasthe oldest participant (age 97) and had the lowestMMSE score indicating mild dementia, was able toengage in meaningful televisits with her sister whoprovided minimal instruction over the phone duringthe televisits. Her sister (age 86) always initiated thevideo connection. They continued to use the video-phones for the duration of the study and both ratedtheir satisfaction as high.The third group (Dif� culty)consisted of the two remaining participants who haddif� culty operating the equipment even with assis-tance.
Again, what appears to be most important is thematch of abilities within each pair. Five types ofability matches were present in this sample (See Table3). As Table 3 illustrates, none of the pairs thatincluded a participant from the group with dif� cul-ties used the videophone for the duration of the study.Three of the four pairs in which both participantsneeded assistance (Help-Help) stopped early. Theother pair did not. The main difference between thethree who stopped early and the one that did not is intheir tolerance levels for operating and technicalproblems. All of the participants in the pairs thatstopped early demonstrated low tolerance.While tol-erance and cognitive ability matches within pairsappear to be important individual predictors of suc-cessful use, the interaction of these constructs is alsoinformative. Six patterns of interactive relationships
1111111
Televisits with institutionalized elders 391D
ownl
oade
d by
[U
nive
rsity
of
Auc
klan
d L
ibra
ry]
at 1
7:31
08
Oct
ober
201
4
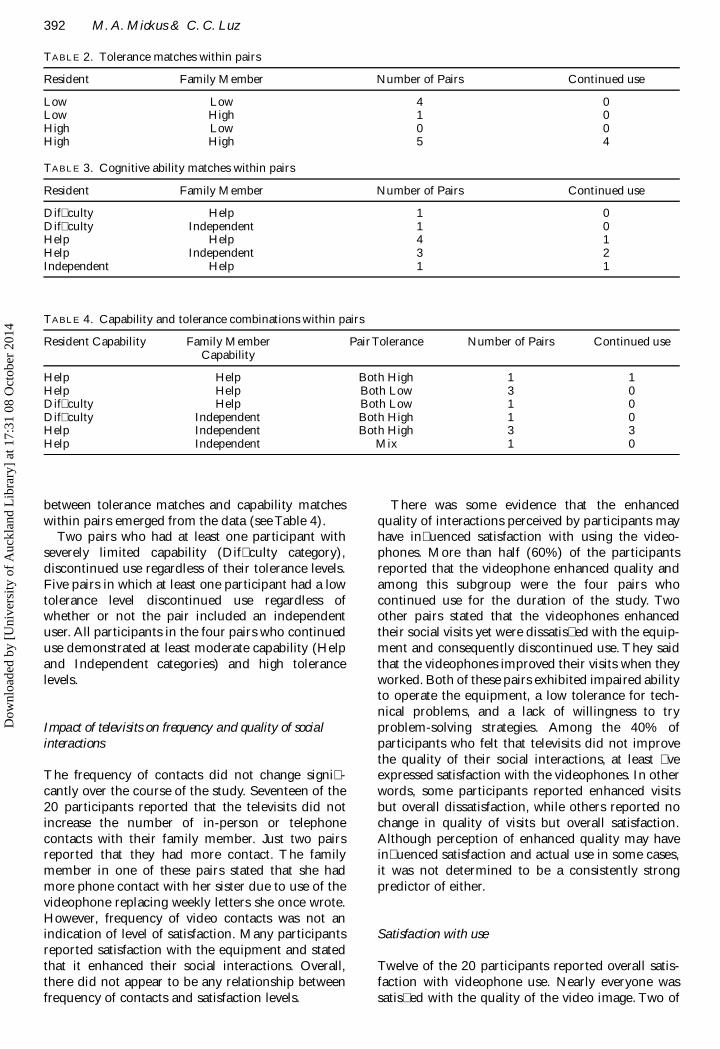
between tolerance matches and capability matcheswithin pairs emerged from the data (see Table 4).
Two pairs who had at least one participant withseverely limited capability (Dif� culty category),discontinued use regardless of their tolerance levels.Five pairs in which at least one participant had a lowtolerance level discontinued use regardless ofwhether or not the pair included an independentuser. All participants in the four pairs who continueduse demonstrated at least moderate capability (Helpand Independent categories) and high tolerancelevels.
Impact of televisits on frequency and quality of socialinteractions
The frequency of contacts did not change signi� -cantly over the course of the study. Seventeen of the20 participants reported that the televisits did notincrease the number of in-person or telephonecontacts with their family member. Just two pairsreported that they had more contact. The familymember in one of these pairs stated that she hadmore phone contact with her sister due to use of thevideophone replacing weekly letters she once wrote.However, frequency of video contacts was not anindication of level of satisfaction. Many participantsreported satisfaction with the equipment and statedthat it enhanced their social interactions. Overall,there did not appear to be any relationship betweenfrequency of contacts and satisfaction levels.
There was some evidence that the enhancedquality of interactions perceived by participants mayhave in� uenced satisfaction with using the video-phones. More than half (60%) of the participantsreported that the videophone enhanced quality andamong this subgroup were the four pairs whocontinued use for the duration of the study. Twoother pairs stated that the videophones enhancedtheir social visits yet were dissatis� ed with the equip-ment and consequently discontinued use. They saidthat the videophones improved their visits when theyworked. Both of these pairs exhibited impaired abilityto operate the equipment, a low tolerance for tech-nical problems, and a lack of willingness to tryproblem-solving strategies. Among the 40% ofparticipants who felt that televisits did not improvethe quality of their social interactions, at least � veexpressed satisfaction with the videophones. In otherwords, some participants reported enhanced visitsbut overall dissatisfaction, while others reported nochange in quality of visits but overall satisfaction.Although perception of enhanced quality may havein� uenced satisfaction and actual use in some cases,it was not determined to be a consistently strongpredictor of either.
Satisfaction with use
Twelve of the 20 participants reported overall satis-faction with videophone use. Nearly everyone wassatis� ed with the quality of the video image. Two of
392 M. A. Mickus & C. C. Luz
TABLE 2. Tolerance matches within pairs
Resident Family Member Number of Pairs Continued use
Low Low 4 0Low High 1 0High Low 0 0High High 5 4
TABLE 3. Cognitive ability matches within pairs
Resident Family Member Number of Pairs Continued use
Dif� culty Help 1 0Dif� culty Independent 1 0Help Help 4 1Help Independent 3 2Independent Help 1 1
TABLE 4. Capability and tolerance combinations within pairs
Resident Capability Family Member Pair Tolerance Number of Pairs Continued useCapability
Help Help Both High 1 1Help Help Both Low 3 0Dif� culty Help Both Low 1 0Dif� culty Independent Both High 1 0Help Independent Both High 3 3Help Independent Mix 1 0
Dow
nloa
ded
by [
Uni
vers
ity o
f A
uckl
and
Lib
rary
] at
17:
31 0
8 O
ctob
er 2
014

the participants who were dissatis� ed overall anddiscontinued using the equipment early were never-theless satis� ed with the image quality when itworked. The fact that it did not always work wasdisappointing and the primary reason for their dissat-isfaction overall. Likewise, almost all of the partici-pants were satis� ed with the audio quality includingthose who reported overall dissatisfaction. Only oneresident was dissatis� ed overall as a result of dissat-isfaction with the audio quality. She had impairedhearing, limited ability to operate the equipment anda low tolerance for technical problems. Satisfactionwith the video image and/or audio quality was notdetermined to be closely associated with actual use.Overall satisfaction may be a better predictor ofactual use. All of the residents who expressed overalldissatisfaction discontinued use prematurely.
Discussion
At month one, all of the pairs were still using theequipment. The majority had experienced problemssuch as inability to see the video image or keypad dueto vision impairment, line static and freezing of theimage. Shortly after, two pairs decided not tocontinue, one related to poor vision and the other toadvancing MS. The remaining pairs were informedthat technical help would continue to be available butif they did not contact the research team for assis-tance, it would henceforth be assumed that they werecontinuing to use the equipment and not experi-encing dif� culties that they could not handle them-selves. Again, this was consistent with the aim ofdetermining how feasible it was for nursing homeresidents to use the videophones with minimal assis-tance. Yet, the contact at four months revealed thatfour more pairs had discontinued use over the pastthree months. Two residents stated that it wasbecause their family member was too busy andvisited in-person on a regular basis anyway. Twostated it was because of frustration with using theequipment, one related to the resident being unableto follow cues.
With one exception, family members had chosennot to participate in the residents’ quarterly care con-ferences despite having expressed interest in doing so.Those who provided a reason for not participatingsuggested that their decisions were related to timelimitations or other family representation at the meet-ings. The one daughter who arranged a video pres-ence was the primary responsible party for theresident despite the fact that she resided in Europeand local family members existed. Her role and thegeographic distance may have rendered the videoimage more valuable. The daughter later reported avery rewarding experience. The care team temporar-ily moved the resident’s videophone into the confer-ence room for the care plan meeting. The daughterinitiated the videophone contact, from Europe, at an
appointed time. She stated that being able to see thestaff members made a positive difference. This pairremained in the study for the remainder of the studydespite occasional problems establishing a video con-nection. The resident made the comment that whatshe liked best about the equipment was ‘being able tosee her. With her living so far away, it was a realbonanza, a blessing, all kinds of positive things.’
These examples illustrate how the value placed onthe video image by participants may in� uence use.One family member expressed annoyance at theimage occasionally freezing up and thought it wasdif� cult for her father to position himself comfortablyin front of the lens but they stayed in the study never-theless because, in her words, ‘The videophone wasa nice uplift to my dad and me. Dad always had amore enthusiastic voice when we could talk togetherand see each other. It helped my dad through thewinter months tremendously.’ The resident said, ‘Itwas great just being able to see my daughter’s face.’This pair also was separated by geographic distanceand the daughter was unable to travel due to healthproblems of her own.
Physical, cognitive, and tolerance limitations, tech-nical problems, frequency of interactions, enhancedsocial interactions, nor satisfaction with image andaudio quality rarely stood alone as reliable predictorsof actual use. It was necessary instead to examinecombinations of factors within pairs.The most potentfactors were physical and or cognitive capability, tol-erance levels, and the value placed on the video image.By examining the relationships between these factors,patterns of relationships and their related outcomesemerged. Although all possible patterns were not rep-resented by the study sample, several tentative con-clusions can be drawn and serve as the basis for futureresearch.These can be summarized as follows:
� Estimates of potential for actual videophone useneed to take into consideration matches withinpairs related to capability, tolerance levels, andvalue placed on the video image.
� Although not explored in depth in this research,� ndings suggest that if even one member of a pairdoes not value the video image, continued use isquestionable.
� The value placed on video images may be relatedto the availability of face-to-face contacts. All ofthe pairs who continued use lived at distances thatmade on-site visits dif� cult and rare.
� Individuals with severe physical or cognitive limi-tations, who have dif� culty operating the equip-ment, even with substantial assistance, may not beviable candidates for videophone use regardless oftolerance levels or value placed on video image.
� Individuals with low tolerance for technical oroperating problems and limited willingness toproblem-solve may not be viable candidates foruse unless such problems are ameliorated prior toimplementation.
1111111
Televisits with institutionalized elders 393D
ownl
oade
d by
[U
nive
rsity
of
Auc
klan
d L
ibra
ry]
at 1
7:31
08
Oct
ober
201
4

� If anticipated problems with equipment use couldbe minimized prior to implementation, even indi-viduals with low tolerance levels may be candi-dates for use. Had this been the case in this study,three additional pairs may have continued use fora total of seven pairs or 70% of the sample.
Potential for actual use
Future utilization of videophone equipment for socialinteraction between nursing home residents and theirfamily members should consider potential for actualuse. Based on the above � ndings, the following fourcategories of potential are suggested:
� High potential in which both participants in a pairare capable of using the equipment with assis-tance and have high tolerance for technical andoperating dif� culties.
� Contingent potential in which both participants ina pair are capable of using the equipment withassistance and who may be willing to use theequipment if certain changes are made to resolvetechnical or unit design problems.
� Low potential in which both participants in a pairare capable but at least one is unwilling to use theequipment even if changes are made. Forexample, a participant may place insuf� cientvalue on videophone use.
� No potential in which, regardless of satisfaction orwillingness, at least one participant is incapable ofusing the equipment due to the type and severityof physical or cognitive limitations that exist.
In summary, the televisits study suggests that video-phones can be used successfully by select nursinghome residents to enhance social interactions,regardless of distance. This includes individuals whohave mild dementia and a full range of medicalconditions and physical limitations. Equallyimportant is the fact that not all of the participantsexperienced success or satisfaction. They demon-strated for example that videophone use might notbene� t people with a certain severity of vision loss ora low tolerance for frustration with new activities.Discerning the differences in the characteristics ofthese two types of experiences helps explain whomight bene� t from the use of communication tech-nology and the conditions under which bene� ts canbe optimized.
Video contact can enhance the quality of interac-tions over audio contact alone, evidenced by positivecomments made by participants such as, ‘We need to� nd a way to keep using this equipment.’ and, ‘It hasreally helped my mother but I didn’t realize howmuch it would help me too’. Several cases in partic-ular clearly illustrated the extent to which the video-phone improved the value of social interactionsincluding one in which two elderly sisters separatedby geographic distance visually saw each other for the
� rst time in several years.When they � rst establisheda video connection, the sister said, ‘Thank you God,thank you whoever made this possible. It is sowonderful to see my sister’s face. I never thought I’dsee her again’.The story of these sisters is a dramaticexample of how effective and rewarding use ofcommunication technology can be for nursing homeresidents and that age is not a predictor of success.Given the decrease of social networks in late life,enhancing the quality of remaining relationships is animportant � nding from this study.
Videophone use may also improve communicationfor people with speech impairments due to the addedvisual image. One participant who had MS wasunable to speak clearly, and found the visual imageallowed family to observe her lips moving and bodylanguage.
The speed of the transmission, size of screen, andthe clarity of the image were all acceptable to partic-ipants. Most family members were able to install andprogram the equipment with minimal assistance. Useof the equipment cost no more than the cost of aregular audio phone call (and the initial investment)and it is anticipated that the cost of this technologywill decrease in the future.
There were several limitations with the studyincluding the small sample size and the lack of acontrol group. In addition, the equipment was testedwhile the study was in progress. Participants deterredby technical and design problems may have bene� tedfrom videophone use had these problems beenresolved prior to data collection. Finally, it is possiblethat residents who were depressed were not consid-ered as potential subjects because they did not havea written diagnosis as such. Future studies in whichdepression is a primary variable will use differentmeasures of depression for subject recruitmentincluding staff observation and chart notations ofdepressive symptoms. However, this exploratoryresearch is breaking new ground with regard tomedically compromised, isolated individuals usingtechnology themselves, without the assistance ofmedical workers, to improve their own quality of life.
Future research
The preliminary � ndings from this pilot studysupport the need to further explore videophone useon a larger scale with other populations with atten-tion toward variables such as cost. Relative to otherforms of technology, the videophones are inexpen-sive. Nevertheless, costs may be prohibitive for indi-viduals, or for facilities considering purchasing theequipment in quantity. Options for minimizing costsuch as a facility purchasing one unit and placing itin a central but private location for resident use. Inaddition to cost, feasibility of videophone use for careplan conferences or by individuals with more severedementia and related behavioral concerns also
394 M. A. Mickus & C. C. LuzD
ownl
oade
d by
[U
nive
rsity
of
Auc
klan
d L
ibra
ry]
at 1
7:31
08
Oct
ober
201
4
warrants attention. Videophone contact with familymembers may be useful for decreasing symptoms ofanxiety or agitation. Studies such as these wouldnecessitate greater involvement and training ofnursing home staff.
References
ABEL, E.K. (1991). Who cares for the elderly? Public policyand the experiences of adult daughters. Philadelphia:Temple University Press.
ATCHLEY, R. (1997). Social forces and aging (8th ed.).Belmont, CA: Wadsworth Publishing Company.
DALGARD, O.S. & LUND, H.L. (1998). Psychosocial riskfactors and mortality: a prospective study with specialfocus on social support, social participation, and locus ofcontrol in Norway. Journal of Epidemiological CommunityHealth, 52 (8), 476–481.
DIAMOND, T. (1992). Making gray gold: narratives ofnursing home care. Chicago, IL: University of ChicagoPress.
DRYSDALE, A.E., NELSON, C.F. & WINEMAN, N.M.(1993). Families need help too: group treatment forfamilies of nursing home residents. Clinical NurseSpecialist, 7 (3), 130–134.
FOLSTEIN, M.F., FOLSTEIN, S.E. & MCHUGH, P.R.(1975). ‘Mini-mental state’. A practical method forgrading the cognitive state of patients for the clinician.Journal of Psychiatric Research, 12 (3), 189–198.
FRASURE-SMITH, N., LESPERANCE, F., GRAVEL, G.,MASSON, A., JUNEAU, M., TALAJIC, M. & BOURASSA,M.G. (2000). Social support, depression, and mortalityduring the � rst year after myocardial infarction.Circulation, 101 (16), 1919–1924.
GALLIENE, R.L., MOORE, S.M. & BRENNAN, P.F. (1993).Alzheimer’s caregivers: psychosocial support viacomputer networks. Journal of Gerontological Nursing, 19(12), 15–22.
GLASS, T.A., MENDES DE LEON, C., MAROTTOLI, R.A.& BERKM AN, L.F. (1999). Population based study ofsocial and productive activities as predictors of survivalamong elderly Americans. British Medical Journal, 319(7208), 478–483.
HENDERSON, J.N. & VESPERI, M.D. (Eds.) (1995). Theculture of long-term care: nursing home ethnography.Westport, Connecticut: Bergin & Garvey.
HOOYMAN, N.R. & GONYEA, J.G. (1999). A feministmodel of family care: practice and policy directions.Journal of Women and Aging, 11 (2–3), 149–169.
HOOYMAN, N.R. & KIYAK, H.A. (1996). Social geron-tology: a multidisciplinary perspective (4th ed.) (pp.282–283). Boston: Allyn and Bacon.
HOUSE, J.S., LANDIS, K.R. & UMBERSON, D. (1990).Social relationships and health. In P. CONRAD & R.KERN (Eds.), The sociology of health and illness (3rd ed.)(pp. 85–94). New York: St. Martin’s Press.
HYBELS, C.F., BLAZER, D.G. & PIEPER, C.F. (2001).Toward a threshold for sub-threshold depression: ananalysis of correlates of depression by severity of symp-toms using data from an elderly community sample. TheGerontologist, 41 (3), 357–365.
JONES, B.N. (1999). Telemedicine in geriatric psychiatry.Psychiatric Annals, 29 (7), 416–420.
KAMMER, C.H. (1994). Stress and coping of familymembers responsible for nursing home placement.Research in Nursing and Health, 17 (2), 89–98.
KELLET, U.M. (1999). Transition in care: family carers’experience of nursing home placement. Journal ofAdvanced Nursing, 29 (6), 1474–1481.
KRISHNAN, K.R., GEORGE, L.K., PIEPER, C.F., JIANG,W., ARIAS, R., LOOK, A. & O’CONNOR, C. (1998).Depression and social support in elderly patients withcardiac disease. American Heart Journal, 136 (3),491–495.
LEVITT, M.J. (2000). Social relations across the life span:in search of uni� ed models. International Journal of Agingand Human Development, 51 (1), 71–84.
MINKLER, M., SCHAUFFER, H. & CLEMENTS-NOLLE,K. (2000). Health promotion for older Americans in the21st century. American Journal of Health Promotion, 14(6), 371–379.
MOEN, P., ROBISON, J. & FIELDS, V. (1994). Women’swork and caregiving roles: a life course approach. TheJournal of Gerontology, 49 (4), S176–S186.
PARK, D. & VANDENBERG, B. (1994). The in� uence ofseparation orientation on life satisfaction in the elderly.International Journal of Aging and Human Development,39(2), 177–187.
PEARLMAN, D.N. & CROWN, W.H. (1992). Alternativesources of social support and their impacts on institu-tional risk. The Gerontologist, 32 (4), 527–535.
PENNINX, B.W., GURALNIK, J.M., BANDEEN-ROCHE,K., KASPER, J.D., SIMONSICK, E.M., FERRUCCI, L. &FRIED, L.P. (2000). The protective effect of emotionalvitality on adverse health outcomes in disabled olderwomen. Journal of American Geriatric Society, 48 (11),1525–1526.
PRUCHNO, R. & KLEBAN, M.H. (1993). Caring for aninstitutionalized parent: the role of coping strategies.Psychology and Aging, 8 (1), 18–25.
REDFORD, L.J. & WHITTEN, P. (1997). Ensuring access tocare in rural areas: the role of communication tech-nology. Generations, Fall, 19–23.
RODGERS, B.L. (1997). Family members’ experiences withthe nursing home placement of an older adult. AppliedNursing Research, 10 (2), 57–63.
ROTHCHILD, E. (1999). Telepsychiatry: why do it?Psychiatric Annals, 29 (7), 394–401.
RUSSELL, D.W., CUTRONA, C.E., DE LA MORA, A. &WALLACE, R.B. (1997). Loneliness and nursing homeadmission among rural older adults. Psychology andAging, 12 (4), 574–589.
ROVNER, B.W., GERMAN, P.S., BRANT, L.J., CLARK, R.,BURTON, L. & FOLSTEIN, M.F. (1991). Depression andmortality in nursing homes. Journal of American MedicalAssociation, 265, 993–996.
SEEMAN, T.E. (2000). Health promoting effects of friendsand family on health outcomes in older adults. AmericanJournal of Health Promotion, 14 (6), 362–370.
SHERMAN, A.M., DE VRIES, B. & LANSFORD, J.E. (2000).Friendship in childhood and adulthood: lessons acrossthe life span. International Journal of Aging and HumanDevelopment, 51 (1), 31–51.
STONE, R., CAFFERATA, G.L. & SANGL, J. (1987).Caregivers of the frail elderly: a national pro� le. TheGerontologist, 27 (5), 616–626.
THOMPSON, E.H. JR., FUTTERMAN, A.M.,GALLAGHER-THOMPSON, D., ROSE, J.M. & LOVETT,S.B. (1993). Social support and caregiving burden infamily caregivers of frail elders. Journal of Gerontology, 48(5), S245–S254.
TROLL, L.E. (1999). Questions for future studies: socialrelationships in old age. International Journal of Aging andHuman Development, 48 (4), 347–351.
WARD, D. (1993). Women and the work of caring. SecondOpinion, 19 (2), 11–26.
WEYERER, S., HAFNER, H., MANN, A.H., AMES, D. &GRAHAM, N. (1995). Prevalence and course of depres-sion among elderly residential home admissions inMannheim and Camden, London. InternationalPsychogeriatrics, 7 (4), 479–493.
1111111
Televisits with institutionalized elders 395D
ownl
oade
d by
[U
nive
rsity
of
Auc
klan
d L
ibra
ry]
at 1
7:31
08
Oct
ober
201
4

WOOD, J.T. (1994). Who cares? Women, care, and culture.Carbondale: Southern Illinois University Press.
YESAVAGE, J.A., BRINK, T.L., ROSE, T.L., LUM, O.,HUANG, V., ADEY, M. & LEIRER, O. (1983).Development and validation of a geriatric depression
screening scale: a preliminary report. Journal ofPsychiatric Research 17, 37–49.
ZAYLOR, C.L. (1999). An adult telepsychiatry clinic’sgrowing pains: how to treat more than 200 patients inseven locations. Psychiatric Annals, 29 (7), 402–408.
396 M. A. Mickus & C. C. LuzD
ownl
oade
d by
[U
nive
rsity
of
Auc
klan
d L
ibra
ry]
at 1
7:31
08
Oct
ober
201
4