Embed Size (px)
Citation preview

Telemonitoring
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011
Simonetta Scalvini
No conflict of interest
Telemedicine Service, IRCCS Salvatore Maugeri Foundation Lumezzane (BS)-Italy

Definitions
• Structured telephone support:“if the monitoring and/or self-care management is delivered
using simple telephone technology (data may have been
collected and stored by a computer)”
• Telemonitoring:“if there was digital/broadband/satellite/wireless
or bluetooth trasmission of physiologic and other non-invasive data”
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

1. Case Definition
2. Patient’s evaluation
3. Therapeutic objectives
6. Patient’s education
7. Appropriate use of the services
4. Development of a care plan
5. Monitoring
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

In situ monitoring of health in older adults: technologies and issues.JAGS 58:1579-1586, 2010.
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

Personal Tele-health System
NE
TW
OR
K (
PO
TS
, GS
M, B
B)
Glucose
Meter
Pedometer
Blood-
pressure
Medication
Tracking
Fitness
Equipment
Weight
Scale
Thermometer
Pulse
Oximeter
Spirometer
Cholesterol
Monitor
Home
sensing &
control
Bed / Chair
Sensors
Implant
Monitors
Baby
Monitors
PERS
CONNECTIVITY
ETHERNET
SENSORSAGGREGATIONCOMPUTATION SERVICES
Diet or
Fitness
Service
Disease
Management
Service
Personal
Health
Record
Service
Implant
Monitoring
Service
Healthcare
Provider
ServicePC
Cell Phone
AggregatorConsumer
Electronics
Personal
Health
System
GRID
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

Personal Health Record
a complete and accurate summary of the health and medical history of an individual by gathering data from many sources and making this information accessible online to anyone who has the necessary electronic credentials to view the information.
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

Videoconference
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

Point- multi point videoconference

GPs
Patients
Service Centre
Hospitals
Telemonitoring
Nurse

S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011


Telemonitoring
(scheduled call for collection of clinical data and biological signals, i.e. blood pressure)
Teleassistance
(unscheduled calls for evaluation of symptoms and/or signals)
Teleconsulting
(each calls requiring a second opinion by a specialist)
CLINICAL HEALTH RECORD
BLOOD PRESSURE
Telematic support

What the nurse do: Comprehensive assessment, proactive clinical intervention, marshalling of resources, assessment of the quality of care; enable people with multiple conditions, affecting all areas of daily living, to remain in control.
Implementsclinical guidelines of the
specific disease
Consultation withspecialist supervisions
if necessary
Formulatesdecisions aboutcare of patients
Organisationaland management
of care
Patient
Specialist
GP
Ask for diagnosticexaminations according
with specialist
Knowledge of symptomsperception

Blood Pressure Telemonitoring
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

Blood Pressure Telemonitoring
2
3
Patient
Device and mobile phone for the transmission of the blood pressure
Nurse or specialist’s counselling
Service Center

Blood Pressure Telemonitoring
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

Role of home blood pressure telemonitoring in hypertension management: an update.
Blood Pressure Monitoring 2010, 15:285-295.

Blood Pressure Monitoring 2010, 15:285-295.
Role of home blood pressure telemonitoring in hypertension management: an update.

Blood Pressure Monitoring 2010, 15:285-295.
Role of home blood pressure telemonitoring in hypertension management: an update.

Telemonitoring of Diabetes


J Diabetes Sci Technol 2009, 3(6):1501-1506.
Enhanced 911/Global Position System Wizard: a telemedicine application for the prevention of severe hypoglycemia-monitor, alert, and locate.

J Diabetes Sci Technol 2009, 3(6):1501-1506.
Enhanced 911/Global Position System Wizard: a telemedicine application for the prevention of severe hypoglycemia-monitor, alert, and locate.

Circ Cardiovasc Qual Outcomes 2011, 4:235-242.
Secondary prevention risk intervention via telemedicine and tailored patient education (SPRITE). A randomized trial to improve postmyocardial infarction management.

Circ Cardiovasc Qual Outcomes 2011, 4:235-242.
Secondary prevention risk intervention via telemedicine and tailored patient education (SPRITE). A randomized trial to improve postmyocardial infarction management.

The Home care
EFG
I
L
A
spiro
holter
sat02
F
II
L
M
A
spiro
holter
sat02holter
BC
D
F
K
T
NN

Virtual Hospital
Patient/Family/GP
\
CALL CENTER
\
CALL CENTER
\
LABORATORIES
\
IMAGES
\
IMAGES
\
IMAGES
\
GYM
\
GYM
\
GYM
\
LABORATORIES
\
LABORATORIES
\
LABORATORIES
\
GP
\
GP
\
GP\
DOCTORS
\\
DOCTORS
\
NURSE
\
NURSE
\
NURSE
\
ECG/pSAT
\
ECG/pSAT
\
ECG/SAT
\WEBCAM TREND\WEBCAM TREND\
WEBCAM
TREND\
PHONE
\
PHONE
\
PHONE
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

Home-based exercise rehabilitation with
telemedicine
following cardiac surgery S Scalvini et al. JTT 2009;15:297-301

The purpose of our pilot study was to evaluate programmes of primary prevention in patients with multiple risk factors for cardiovascular diseases by using TMS to achieve the following objectives: control of hypertension, changes in lifestyle, and adherence to physical training.
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

Methods
1
Nurse-tutor
Service Center
2° opinion
consultation
4
Patients in Tele-training: 3-5 times/week
Devices, ECG and BP telemonitoringS. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

Blood pressure monitoring
Twenty-four-hour ambulatory blood pressure (BP) monitoring was
performed at T0 and T6 using a validated Mobil O Graph Ambulatory
BP monitor (IEM, Stolberg, DE). In case of clinically significant
changes during the 24-h BP monitoring, antihypertensive treatment
was adjusted accordingly.
Home self-measurement with an oscillometric device was also
performed (Omron M6 Comfort; Omron, Kyoto, Japan) at least three
times a week.
Home self-measurement with BP-Tel (Aerotel) device for 1 week at T0
and T6. The system includes:
(i) a home BP measuring device that uses the oscillometric system;
(ii) a built-in proprietary communicator which automatically transmits
data from home to the service centre via telephone; and
(iii) a computer programme at the service centre for receiving and
storing measurements in a database and preparing reports.
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

• Physiotherapist go at patient’shome monthly
• During the visit thephysiotherapist evaluates thecorrect execution of physicaltraining
• Increases the work load
• Personalises the exercise incase of physical limitations,(osteoarthritis, fractures,etc.)
Home visits by physiotherapist
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

Physical activity programme
Patients had to undergo a minimum of three sessions a week of bicycle exercise training or fast walking for at least 30 min and calisthenic exercises.
Physical programme had three basic activities: (i) 5–10-min warming, (ii) 20-min active exercise, and (iii) 5–10-min cool-down phase. A baseline 1-lead electrocardiogram followed by the trans-telephonic delivering of all tracks recorded had to be performed.
Physiotherapists organized home visits and/or telephone contacts aimed at increasing workload and evaluating the proper execution of calisthenic exercises.
At both T0 and T6, all patients performed one maximal effort test and the metabolic Holter monitoring using the Body Monitoring Multi-Sensor Armband
(BMSA) (SenseWear) worn at the triceps of the right arm for at least 72 h. The activation of the BMSA was completed using the InnerView Research software version 2 (BodyMedia) measuring energy expenditure and duration and quantification of physical activity.
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

SenseWear® Armband
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

Teletraining
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

Questionnaires
Quality of life (WHO QoL-short)13 at both T0 and T6;
Pisa Stress (PSQ-form A), which assesses presence and
type of stress-related behavioural responses,14 at
both T0 and T6;
Diary of daily eating habits (only at T0) needed to arrange
an individual programme of nutrition education;
Questionnaire of satisfaction only at T6: a 10-item
questionnaire which focused on patients’ satisfaction,
acceptance of the technology used, and efficiency of
personnel.
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

Tele-psychology online
Patients
Nurse
Service Centre
Psychologist
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

Scheduled one domiciliary
visit at the beginning of
prevention programme and,
however in case of need.
Evaluates vitals signs
Sanitary education reinforce
Help patient to fill in
questionnaires (nutritional
habits and stress)
Home visits by nurse
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

General characteristics of the patient population (1)
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

General characteristics of the patient population (2)
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

• 1706 contacts, 63±33 calls/patient were performed. Each call required a
mean-time of 12.8 ± 1.4 min each
• Each patient performed 61±32 scheduled and 2.2±2.5 unscheduled calls
• During the call 39±23 BP measurements and 50±26 ECG-transmission were
referred per patient.
Calls and consequences
REASONS FOR CALLING ACTION TAKEN
Scheduled controls
Palpitations 16 Therapy modification 28
13
Educational reinforcement
9Dyspnoea 1
Hypertensive Attack
8 137
General weakness 4
General malaise
General communications 123
New scheduled contacts 1508
Telephone consultations 22
Further examinations
1547
• 281 contacts with specialists, 218 contacts with hypertension or cardiologist
specialist
• 140 home visits of physiotherapists (5.0±1.0/patient)
• 52 psychological contacts (7±3/patient performed only in six patients)

Physical Activity Programme at Home
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

Body Monitoring Multi-Sensor Armband at T0 and T6
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

Systolic blood pressure
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

Diastolic blood pressure
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

Telemonitoring in
chronic heart failure

Structured telephone support or telemonitoring programmes for patients with chronic heart failure (Review)
All-cause hospitalization (full-peer reviewed pubblication only)
Telemonitoring vs usual care
Clark RA et al. 2010

Structured telephone support or telemonitoring programmes for patients with chronic heart failure(Review)
CHF-related hospitalization (full-peer reviewed pubblication only)
Telemonitoring vs usual care
Clark RA et al. 2010

Clark RA et al. 2010
Structured telephone support or telemonitoring programmes for patients with chronic heart failure(Review)
All-cause mortality (full-peer reviewed pubblication only)
Telemonitoring vs usual care

Structured telephone support or telemonitoring programmes for patients with chronic heart
failure(Review)
Implication for pratice
Clark RA et al. 2010

Structured telephone support or telemonitoring programmes for patients with
chronic heart failure(Review)
Implications for research (1)
Clark RA et al. 2010

230 CHF patients followed for 365 days usingtelephonic follow-up and ECG monitoring
230 patients in the control group
average age 57±10 y; FE 27±6%; VO2 13.3ml/kg/min
In the “Telemedicine Group” we observed a reduction in:
- hospitalizations (~ 44%)
- destabilizations (~ 50%)
- costs (~ 24%)
Multicenter randomised trial on home based
telemanagement to prevent hospital readmission of
patients with chronic heart failure
Giordano et al. IJC 2009;131:192-199

Home Based Telemanagement
programme
Total358
Cardiovascular Death19
Non Cardiovascular Death2
Drop out9
No events6 months re-evaluation
238
Cardiovascular Hospitalizations112
Non CardiovascularHospitalizations
46
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

HOME BASED TELEMANAGEMENT
Patients’ baseline characteristics
Years of enrollement Total
(n=358)
2000-2003
(n=210)
2004-2007
(n=148)
P
Female (%) 18.7 16 22.3 ns
Age (y) 63±12 60±11 68±13 <0.001
NYHA Class 2.6±0.5 2.5±0.5 2.7±0.5 <0.01
NHYA III (%) 60.6 50.4 75.6 <0.0001
LVEF (%) 30.1±9.6 28.7±7.6 31.9±11.7 ns
Onset of symptoms <6 m
(%)24.3 17.6 33.7 <0.0007
CAD Ethiology (%) 55.3 57.6 52.3 ns
COPD (%) 12.9 9.5 17.6 <0.03
CRI (%) 15.9 12.8 20.3 =0.07
Diabetes (%) 19.3 21.9 15.6 ns
-Blockers agents (%) 84.4 89.9 76.3 <0.01
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

HOME BASED TELEMANAGEMENT
Clinical Events
Years of enrollement Total 2000-
2003
2004-
2007
p
(n=358) (n=210) (n=148)
Acute HF Instabilization w/o hospitalization
rate (%)
9.8 11.4 7.4 ns
Cardiovascular (including HF) readmission
rate (%)
31.2 29.0 34.5 ns
Acute HF readmission rate (%) 19.6 16.7 23.6 ns
Non cardiovascular readmission rate (%) 12.9 9.5 17.6 <0.03
All-cause readmission rate (%) 38.3 33.8 44.6 <0.05
Cardiovascular mortality rate (%) 5.3 5.7 4.7 ns
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

HOME BASED TELEMANAGEMENT
Six-month re-evaluation
TOTAL (n=238)
Pre Post p
NHYA Class 2.5±0.5 2.0±0.7 <0.0001
LVEF % 30±7.8 33.1±10.6 <0.0001
6 min-WT (mt) 427.6±109 442.8±107 NS
MLHFQ 30.2±18.1 25.2±21.1 <0.01
Hb (mg/dl) 13.0±1.9 13.6±1.8 <0.0006
βBlockers (mg/day) 34.7±21.4 40.3±21 <0.001
βBlockers 88.2 89.9 NS
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

Extracardiac
diseasesMultiple risk
factors
Multidistrectual
Vascular disease
Multiple cardiac
disease
Oldest Old
“homeostenosis”
Primary or secondary
prevention
Multidisciplinary management
S. Scalvini, EuroPRevent 2011, Geneve 14 April 2011

Our understanding the future
Projects
Remb. Operations
R&D
Projects
Remb.
Operations
R&D
Projects
Remb.
Operations
R&D
now
2/3 yy 3/5 yy
Cash flows from Projects still finance a large amount of
operating activities.Probably, it will take 5 years to reverse this structure. Mostly, it depends on
the speed of expansion of reimbursment, in terms of
number of services and number of types of services.

0
40,000
80,000
120,000
160,000
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
€0
00
s
present value of cumulative costs present value of cumulative benefits
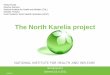
Telecardiology in Italy: Benefits from a telemedicine network connecting chronic patients, General Practitioners and Health
Provider Organisations
The economic impact of extending telecardiology across the whole Lombardy Region,steadily over about six years up to 2012, is material. Much of the investment needed ininformation and communication technology, electrocardiogram equipment and serviceinfrastructure has already been set in place by Health Telematic Network. The total netbenefits are considerable, with an estimated annual benefit cost ratio of more than 3.3:1 by2012

A different future, new ability,
new organizations, new
methods to prevent ….
….. In some reality a
present !!!