Embed Size (px)
DESCRIPTION
Telemetry/EKG/Pacers. MCC NURSING DIANA BLUM MSN. A dysrhythmia is a disturbance of the rhythm of the heart caused by a problem in the conduction system. Categorized by site of origin: atrial , AV nodal, ventricular - PowerPoint PPT Presentation
Citation preview

Telemetry/EKG/Pacers
MCC NURSING DIANA BLUM MSN

A dysrhythmia is a disturbance of the rhythm of the heart caused by a problem in the conduction system.
Categorized by site of origin: atrial , AV nodal, ventricular
Blocks are interruptions in impulse conduction: 1st, 2nd type 1&2, 3rd or complete heart block
2



5

P wave
6
Measures: 0.12-0.20

Measures: 0.06-0.12
QRS WAVE
7

QT Wave
8
Measures approx 0.34-0.43 secs

Calculating Heart Rate Quick Estimate: The 6-second Method - count the # of QRS complexes in a 6 sec. length of strip & multiply by 10 (the second mark is = to 5 large boxes) This can be used is rhythm is reg or unreg.


11
TO MAP= TO DETERMINE IF REGULAR OR IRREGULAR
Each small box measures 0.041 big box (5 small boxes) is equal to a HR of 3002 big boxes is hr of 1503 big boxes is hr of 1004 big boxes is hr of 755 big boxes is hr of 606 big boxes is hr of 507 big boxes is hr of 438 big boxes is hr of 38

Large box estimate of heart rate works with regular rhythms

Count small boxes between two R waves. Divide into1500 Gives BPM

Atrial arrythmias Normal sinus rhythm Sinus tachycardia Sinus bradycardia Premature atrial contraction (PAC) Supraventricular tachycardia Atrial flutter Atrial fibrillation
14

Ventricular arrythmias Junctional rhythm AV blocks Premature junctional rhythm Premature ventricular contraction (PVC) Ventricular Tachycardia (V-tach) Ventricular Fibrillation (V-Fib) Torsade de Pointes (TdP) Pulseless electrical activity (PEA) Asystole
15

ARTIFACT

NSR
17

18
SINUS ARRHYTHMIA
Hr= 60-100 bpm On strip it looks regular but does not map
out PR interval= 0.12-0.20

19
JUNCTIONAL ESCAPE RHYTHM
HR 40-60 bpm<60 bpm is acceleratedRhythm is regularPwaves not always present

Junctional Rhythm
20

SB
21

ST
22

Supraventricular Tachycardia
23

SVT converted with Adenosinegiven rapid IV Push stimulates vagal response. S/E: flushing,bronchospasm,AVblock
24

AV Blocks First degree block Second degree block Type I (Wenchebach) Second degree block Type II (Mobitz II) Third degree block Bundle branch block
25

26
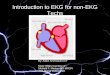
FIRST DEGREE HEART BLOCK
Rate is usually WNLRhythm is regularPwaves are normal in size and shape The PR interval is prolonged (>0.20 sec) but constant

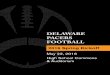
27SECOND DEGREE HEART BLOCK TYPE 1
Pwaves are normal in size and shape; Some pwaves are not followed by QRSPR interval: lengthens with each cycle until it appears without QRS Complex
then the cycle starts overQRS is usually narrow

http://www.youtube.com/watch?v=GVxJJ2DBPiQ&feature=related

29SECOND DEGREE HEART BLOCK TYPE 2
Ventricular rate is usually slowRhythm is irregularPwaves are normal in size and shape (more pwaves than QRS)PR interval is within normal limitsQRS is usually wide

303RD DEGREE HEART BLOCK OF COMPLETE HEART BLOCK
Ventricular rate is regular but there is no correlation between pwaves and QRSPwaves are normal in size and shapeNo true PR interval

Atrial Fibrillation31
Erratic wavy basePr is not measurableQRS 0.10 sec or less usuallyhttp://www.youtube.com/watch?v=VKxQgjj2yVU&feature=related

Afib causes : Chocolate large amounts: contains
theobromine, a mild cardiac stimulant. - sleep apnea - athletes more prone (enlarged heart) - tall athletes (esp basketball players) - aging heart - men more than women - sleeping on left side or stomach etc.
32

A-fib treatment: ASA not as effective as Coumadin in
preventing strokes. ASA less likely to cause abnorm
bleeding **since hemorrhagic stroke increases
with age & is also increased by taking Coumadin, some Drs. may switch older pts from Coumadin to ASA.
33

A Fib electrical cardioversion: High risk of forming clots & causing
stroke Anticoagulants taken before treatment
and 3-4 weeks post treatment If life-threatening, may need Heparin IV
before cardioversion
Best time: recent A fib
34

35
ATRIAL FLUTTER
Atrial rate of 250-450 bpm ventricular rate variesAtrial rhythm is regular ventricular rate is irregularNo identifiable p wavesP wave is not measurableQrs: 0.10 or less usually

Atrial fib/flutter
36

37
PACED BEAT
Pacer spike should fall before the P wave unless a dualChamber pacemaker; if it does not there could be a problem

PAC
38

39PREMATURE VENTRICULAR CONDUCTION (PVC)
Extra beat Types
uniform=go the same directionmultifocal= go in different directionR on T=when the pvc fall on the preceding twavecouplet= 2 pvcs togetherbigeminy= pvc every other beattrigeminy=pvc every third beat

PVCs (unifocal)
40

PVCs (multifocal)
41

Ventricular tachycardia
42
Monomorphic: beats are same size and shapePolymorphic: different size and shape

43
TORSADES DE POINTE
This is a polymorphic VTUsually electrical imbalance in nature r/t NA+ or K+

44


Ventricular Fibrillation
46
Rate can not be determined because of no identifiable wavesRapid chaotic rhythm with no patternNo p wavesNo PR intervalNo QRS

Vtach/Vfib Both can be life threatening VT= V HR 100-250 bpm Causes: AMI, CAD, hypokalemia, dig
toxic S/S: palpitations, dizzy, angina, <LOC Treatment: assess for pulse, if none,
defib VF=Rate undeterminable Cause: same Treatment: CPR
47

Asystole
48

Asystole and PEA CPR
Oxygen Epinephrine 1 mg IV/IO (repeat 3-5 minutes) May give Vasopressin 40U IV/IO to replace 1st or 2nd dose of epinephrine Consider Atropine 1 mg IV/IO Repeat every 3 to 5
min (up to 3 doses)
49

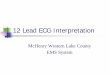
ST elevation

5 Steps to 12 Lead Interpretation1. Assess regularity and speed2. Look for signs of infarction3. Present in >1 lead, but not all?4. Assess associated conditions5. Correlate with clinical condition

Normal EKG

MI

Polymorphic VT

VFIB

57

58

59

60

http://nursebob.com/
http://www.usfca.edu/fac_staff/ritter/ekg.htm
http://ems-safety.com/12-lead-ekg.htm

Rhythms for Cardioversion A-fib A-flutter Supraventricular tachycardia
62

Post cardioversion care: 1. generally the care for a patient tells
cardioversion is the same as for the fibrillation. 2. If it is a elective procedure, digoxin is usually
withheld for 48 hours prior to cardioversion to prevent dysrhythmias after the procedure.
3. Airway patency should be maintained and the patient state of consciousness should be evaluated.

Indications for pacemaker Temporary: -symptomatic bradycardia (not
controlled by meds) - ant MI - drug overdose (dig, beta blocker) Permanent: - 2nd degree Mobitz Type II - 3rd degree Block - symptomatic bradycardia, arrhythmias - suppress tachyarrythmias
64

Position of the letterDesignation1st letterChamber being paced (A=atrium, V=ventricle, 0=none)
2nd letterChamber being sensed (A=atrium, V=ventricle, 0=none)
3rd letterPacing Mode (O=none, I=inhibited, T=triggered, D=dual)
4th letterRate Response (R=rate response is on)

Chambers that can be paced:AtriumVentricleDual (both atrium and ventricle)ICD (Implantable Cardioverter
Defibrillator)
66

AP VP AP VP
V-AAV V-AAV
Dual Paced
Atrial Pace, Ventricular Pace (AP/VP)

ICD - prevents sudden cardiac death due to V-tach or V-fib. Pt can feel the shock -defib felt like “kick in the chest” that lasts 1 second - cardiovert feels like “thump in
chest - pt doesn’t feel pacing
68

Operative failures with pacers: Pneumothorax Pericarditis Infection Hematoma Lead dislodgement (seen on X-ray) Venous thrombosis (rare but would see unilateral edema to arm on same
side as pacer)
69

Pt Education: 1. carry ID card (Xray code seen in standard chest Xray) 2. not allowed to drive for 1 month 3. no metal detectors or no longer than nec. 4. MRI interrupts pacing-can’t get one for some time if
new 5. No power generators (welding) 6. microwave questionable 7. radiotherapy (may damage circuits) The pacer may need to be surgically moved if in path of radiation field. 8. TENS (transcutaneous electrical stimulation) interferes may need reprogramming 9. Cell phone use in opposite ear of pacer and store away from side of pacer
70

EP with Ablation
An electrophysiology study is simply a study of the electrical function of your heart.

Bundle Branch Blocks: Diagnosed with 12 lead EKG: most common cause: acute MI
Right bundle branch block: - impulse travels through left ventricle
first, then activates right ventricle (gives am “M” shaped complex
Left bundle branch block: --impulse first depolarizes right side
of heart then the left ventricle (gives deep, wide “V” shaped complex
72

73

Hyperkalcemia
74

Intro to ACLS

Primary Survey Airway: Open airway, look, listen, and
feel for breathing Breathing: If not breathing slowly give
2 rescue breaths. If breaths go in continue to next step.
Circulation: Check the carotid artery (Adult) for a pulse. If no pulse begin CPR.
Defibrillation: Search for and Shock V-Fib/Pulseless V-Tach

Adult ACLS Secondary Survey ABCDs (abbreviated)
Airway: Intubate if not breathing. Assess bilateral breath sounds for proper tube placement.
Breathing: Provide positive pressure ventilations with 100% O2.
Circulation: If no pulse continue CPR, obtain IV access, give proper medications.
Differential Diagnosis: Attempt to identify treatable causes for the problem.
.


stress Common responses can include:
Feeling a sense of loss, sadness, frustration, helplessness, or emotional numbness
Experiencing troubling memories from that day Having nightmares or difficulty falling or
staying asleep Having no desire for food or a loss of appetite Having difficulty concentrating Feeling nervous or on edge

Teaching to cope Reach out and talk. Express yourself. Watch and listen. Stay active. Stay in touch with family. Take care of yourself.

ANY QUESTIONS?Let’s Practice