Embed Size (px)
Citation preview

©2017 MFMER | 3671080-1
TELEMEDICINE FOR NEWBORN
RESUSCITATION
Jennifer Fang, MD, MS
Division of Neonatal Medicine
MAYO CLINIC

©2017 MFMER | 3671080-2
DISCLOSURES• In the past 12 months, I have had the following financial
relationships with the manufacturer(s) of any commercial product(s) and/or provider(s) of commercial service(s) discussed in this CME activity:
– Unrelated licensed intellectual property with InTouch Health
• I do not intend to discuss an unapproved/investigative use of a commercial product/device in my presentation

©2017 MFMER | 3671080-3
1
OBJECTIVES
Recognize system-level challenges to optimal newborn resuscitation
Identify how telemedicine may improve access to subspecialty care and enhance the regional practice
Describe the impact telemedicine has on the quality of newborn resuscitations in the community setting
2
3

©2017 MFMER | 3671080-4
IDENTIFYING A CLINICAL NEED
REGIONALIZATION of perinatal
care has IMPROVED OUTCOMES
for mothers and newborns
Neonates born at hospitals with
LOWER LEVELS OF NEWBORN
CARE are at INCREASED RISK
OF MORTALITY and morbidities

©2017 MFMER | 3671080-5
THE CHALLENGE
FREQUENCY OF HIGH-RISK NEWBORN RESUSCITATION – once every 2-3 years
DELIVERY VOLUME – 200-500 deliveries/year
RESOURCES AVAILABLE – RN and FM or Pediatrician in clinic or at home
TECHNICAL SKILLS REQUIRED – Advanced airway management, central line placement, chest compressions, meds
ACHIEVE COMPETENCY – Residency training, decreased ICU exposure, competition for procedures
MAINTENANCE OF COMPETENCY – Complete NRP, frequent practice/simulation
MEDICAL TRANSPORT – Geography or weather can delay arrival of transport team
INCIDENCE OF HIGH-RISK RESUSCITATION – 1:1,000

Does the system allow for an outcome disparity based on birth location?
CULTURE OF SAFETY
MASTERY OF NRP
BRIEFING AND DEBRIEFING
SIMULATION
TELEMEDICINE
Can we close this quality gap using TELEMEDICINE?

©2017 MFMER | 3671080-7
1
SIMULATION STUDY
Fang et al, Resusc 2014
46Study participants
(pediatric residents)
ASSIGNED
TO
Bedside providerled resuscitation
Bedside provider + telemedicine support
+2

©2017 MFMER | 3671080-8
SCENARIO
“You have been called to the vaginal delivery of a full-term infant due to fetal bradycardia”
At delivery apneic and bradycardic with heart rate of 70 bpm
Scenario concluded once effective ventilation established MR. SOP(A) or successfully intubated patient

©2017 MFMER | 3671080-9
• TELEMEDICINEreduced the time to effective ventilation by 35% (4.2 vs 2.7 minutes)
• 100% of participants in the telemedicine group performed all five corrective steps
• All participants in the control group placed an ET tube to effectively ventilate the baby
Control group(n=23)
Intervention group (n=23)
P
Time to effective ventilation in seconds, mean (range)
251 (125-479) 162 (98-233) <0.001
Stimulates the infant, n (%) 18 (78) 22 (96) 0.19
Positive pressure ventilation, n (%) 23 (100) 23 (100) NA
Number of first five corrective steps used, n (%)
0 5 (22) 0 <0.001
1 4 (17) 0
2 6 (26) 0
3 3 (13) 0
4 5 (22) 0
5 0 23 (100)
Use of the first five corrective steps, n (%)
M – Adjusts mask Position 11 (48) 23 (100) <0.001
R – Repositions the head 16 (70) 23 (100) 0.009
S – Suctions mouth and nose 11 (48) 23 (100) <0.001
O – Opens mouth or lifts jaw 4 (17) 23 (100) <0.001
P – Increases positive inspiratory pressure
3 (13) 23 (100) <0.001
Endotracheal intubation, n (%) 23 (100) 0 <0.001

©2017 MFMER | 3671080-10
CONCLUSION
Telemedicine significantly REDUCED THE TIME
to establish effective ventilation and IMPROVED
ADHERENCE to the NRP algorithm
This may be a means for regional providers to
support local providers during neonatal emergencies

©2017 MFMER | 3671080-11
TELENEONATOLOGY
• Pilot began in MARCH OF 2013
• Program development and
expansion in partnership with CENTER FOR
CONNECTED CARE
• OVER 200 CONSULTS
provided to date

©2017 MFMER | 3671080-12
SETTING – THE HUB
26 BED Level IV regional NICU
Staffed by 8 NEONATOLOGISTS
2500 deliveries per year
400 admissions per year
50% are out-born

©2017 MFMER | 3671080-13
SETTING – THE SPOKES
©2012 MFMER | 3288990-13
10 MAYO CLINIC
HEALTH SYSTEM sites
Staffed by PEDIATRICIANS and/or
FAMILY MEDICINE PHYSICIANS
7 – Level I nurseries
2 – Level II nurseries
1 – Level III nursery
5500 deliveries per year

146
1500
200
2400
102
1012
943
424393
310
69237
BEFORE TELENEONATOLOGY
43% of newborns at MAYO MIDWEST HOSPITALS
had immediate access to a Neonatologist
AS OF OCTOBER 2016
100% of newborns in the MAYO CLINIC MIDWEST REGION
have immediate access to a Neonatologist
©2017 MFMER | 3671080-15
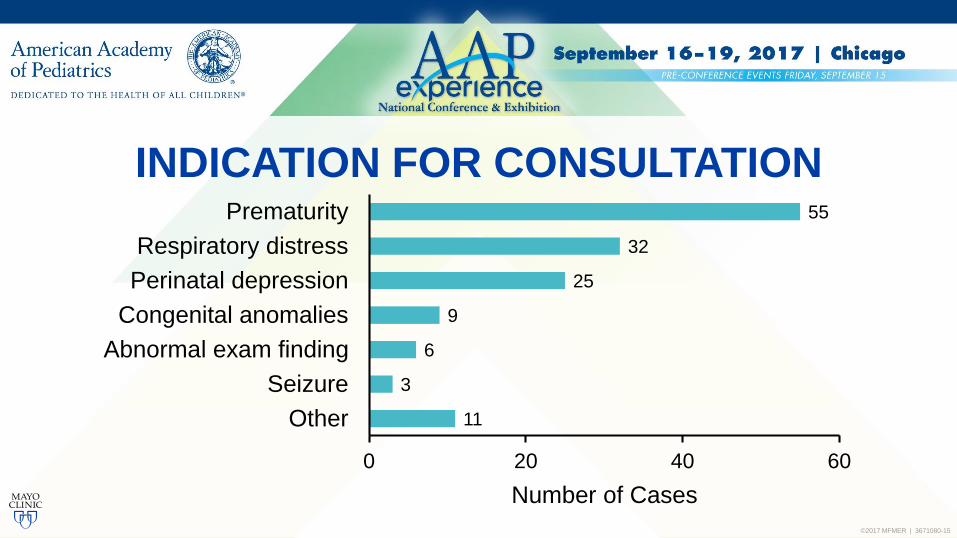
INDICATION FOR CONSULTATION
11
3
6
9
25
32
55
0 20 40 60
Other
Seizure
Abnormal exam finding
Congenital anomalies
Perinatal depression
Respiratory distress
Prematurity
Number of Cases

©2017 MFMER | 3671080-16
PATIENT DISPOSITION
Transferred to the NICU
Remained in the MCHS
Transferred to the ISCN
Transferred to a different NICU
Died
33%

©2017 MFMER | 3671080-17
95%
98%
96%
96%
PROVIDER SATISFACTION
Fang et al, Mayo Clin Proc 2016
Of local providers agree that the consulting neonatologist
worked collaboratively with their team
Of providers agree that the teleneonatology consult
improved patient safety and/or quality of care
Would use teleneonatology again and would recommend
its use to their colleagues
Agreed that there is a need for teleneonatology
at their hospital

©2017 MFMER | 3671080-18
DOES TELEMEDICINE IMPROVE THE QUALITY
OF NEWBORN RESUSCITATION?

©2017 MFMER | 3671080-19
Outborn neonates admitted to the Mayo Clinic NICUP
TELENEONATOLOGY OUTCOMES STUDY
Synchronous video telemedicine consult with a neonatologistI
Outborn matched controls cared for by the local teamC
Overall quality of the resuscitationO

©2017 MFMER | 3671080-20
RETROSPECTIVE COHORT STUDY
• INTERVENTION – telemedicine consult during
resuscitation or initial stabilization
• CONTROL – cared for by the local team
– Preterm, matched by gestational age
– Term, matched by admission diagnosis
– Also matched to gender and level of newborn care
EXCLUSION CRITERIA – presence of the transport team

©2017 MFMER | 3671080-21
• Abstracted data from the electronic health record
• Patient characteristics
• Resuscitation metrics
• Mortality and major morbidities
Gestational age, birth weight, gender, mode of delivery, pregnancy and intrapartum complications
Apgar scores, need for intubation, chest compressions, epinephrine, time/value of temperature, glucose, blood gas

©2017 MFMER | 3671080-22
Blinded to the intervention, two neonatologists reviewed the patient characteristics and resuscitation metrics
Assigned a “resuscitation quality rating” using a 1 to 10 descriptive rating scale
▪ Significant deviation from the standard of care
▪ Resuscitation metrics never measured or significantly abnormal1
▪ Excellent resuscitation with no room for improvement
▪ All resuscitation metrics are measured and within normal limits10

©2017 MFMER | 3671080-23
RESULTS

©2017 MFMER | 3671080-24
Patient Characteristic Intervention Group (n=47) Controls (n=45)
Gestational Age, Mean (SD) 34.7 (5.5) 35.1 (4.8)
Gestational age category
Less than 29 weeks 9 (19%) 7 (16%)
29 0/7 to 33 6/7 weeks 9 (19%) 9 (20%)
34 0/7 to 36 6/7 weeks 10 (21%) 6 (13%)
37 0/7 weeks or greater 19 (40%) 23 (51%)
Birth weight (grams)
Mean (SD) 2491 (1150) 2531 (997)
Range (460-4833) (590-4270)
Gender
Female 19 (40%) 24 (53%)
Male 28 (60%) 21 (47%)

©2017 MFMER | 3671080-25
Patient Characteristic Intervention Group (n=47) Controls (n=45)
Level of newborn care at referral hospital
Level I nursery 18 (38%) 19 (42%)
Level II nursery 29 (62%) 26 (58%)
Exposure to any antenatal steroids
Yes 3 (6%) 8 (18%)
No 24 (51%) 13 (29%)
Not indicated (e.g. GA >/= 37 0/7 weeks) 19 (40%) 23 (51%)
Indeterminate 1 (2%) 1 (2%)
Mode of delivery
Vaginal 22 (47%) 17 (38%)
Emergency C-section 19 (40%) 13 (29%)
C-section 5 (11%) 13 (29%)
Assisted vaginal delivery (vacuum or forceps) 1 (2%) 2 (4%)

©2017 MFMER | 3671080-26
Patient Characteristic Intervention Group (n=47) Controls (n=45)
Pregnancy and intrapartum complications
Preterm labor 23 (49%) 15 (33%)
Meconium stained amniotic fluid 13 (28%) 12 (27%)
Persistent or deep decelerations in fetal heart rate 8 (17%) 15 (33%)
Preterm premature rupture of membranes 8 (17%) 7 (16%)
Twin gestation 6 (13%) 6 (13%)
Placental abruption 9 (19%) 2 (4%)
Congenital anomaly 4 (9%) 4 (9%)
Umbilical cord accident 2 (4%) 1 (2%)

©2017 MFMER | 3671080-27
Median (IQR) rating for the telemedicine group was 7(3,8) compared to 4 (3, 5) for the control group (median difference 1, P=0.002)
55%
30%
0%
20%
40%
60%
80%
100%
Telemedicine (n=47) Control (n=47)
P=0.02
Newborns with a Quality Rating 5
The quality of resuscitation was SIGNIFICANTLY IMPROVED for newborns who received a telemedicine consult

©2017 MFMER | 3671080-28
57%
26%
0%
20%
40%
60%
80%
100%
Telemedicine (n=35) Control (n=35)
P=0.01
Newborns with a Quality Rating 5
Median time from birth to telemedicine consult was 12.1 MINUTES (IQR 5.0, 25.1)
For the 35 matched pairs that had a consult within 1 hour of birth – Median rating for the telemedicine group was 8compared to 4 for the control group (median difference 2, P=0.003)
©2017 MFMER | 3671080-29
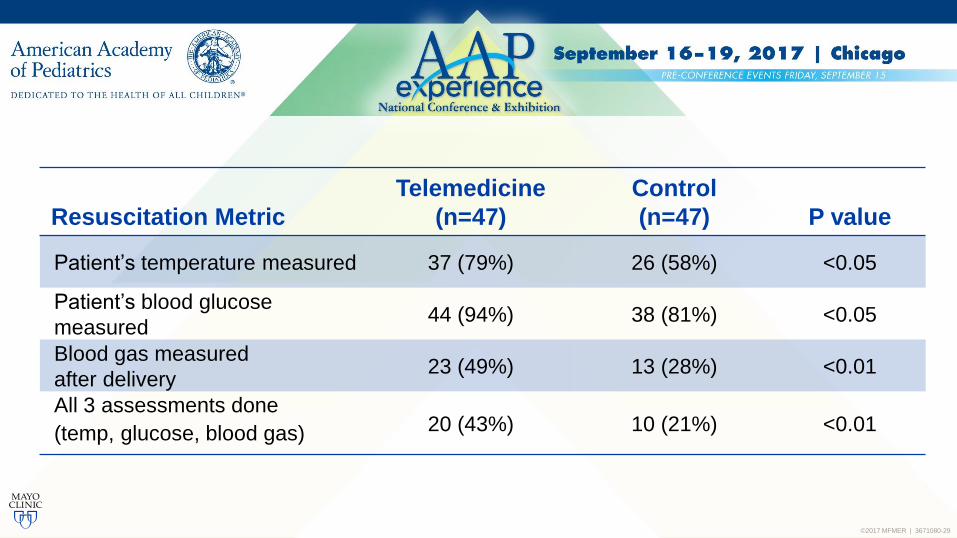
Resuscitation Metric
Telemedicine
(n=47)
Control
(n=47) P value
Patient’s temperature measured 37 (79%) 26 (58%) <0.05
Patient’s blood glucose
measured44 (94%) 38 (81%) <0.05
Blood gas measured
after delivery23 (49%) 13 (28%) <0.01
All 3 assessments done
(temp, glucose, blood gas) 20 (43%) 10 (21%) <0.01

©2017 MFMER | 3671080-30
P=0.058
Patient Outcome
Intervention
(n=47)
Control
(n=45)
Death before discharge 3 (6%) 7 (16%)
Death or morbidity before discharge 11 (23%) 12 (27%)
Length of NICU stay (in days) 25.0 (34%) 19.6 (25%)
Chronic lung disease 4 (9%) 3 (7%)
Necrotizing enterocolitis 0 (0%) 2 (4%)
Severe retinopathy of prematurity 0 (0%) 1 (2%)
Periventricular-intraventricular
hemorrhage8 (17%) 4 (9%)
Severe periventricular-
intraventricular hemorrhage5 (11%) 2 (4%)

©2017 MFMER | 3671080-31
RIGHT TIME
CONCLUSION• System-level challenges create an outcome
disparity for newborns based on birth location
• Teleneonatology consults may IMPROVE THE QUALITY of high-risk newborn resuscitations that occur in community hospitals
• Teleneonatology programs can enhance the healthcare delivery system for newborns
RIGHT PLACERIGHT CARE

©2017 MFMER | 3671080-32
ACKNOWLEDGEMENTSDIVISION OF NEONATAL MEDICINE
CENTER FOR CONNECTED CARE

©2017 MFMER | 3671080-33
SIMULATED TELENEONATOLOGY CONSULT

©2017 MFMER | 3671080-34
QUESTIONS AND DISCUSSION

©2017 MFMER | 3671080-35
REFERENCESFor more information on this subject, see the following publications• Lorch SA, Baiocchi M, Ahlberg CE, Small DS. The differential impact of delivery hospital on the
outcomes of premature infants. Pediatrics. 2012;130(2):270-278
• Brantley MD, Davis NL, Goodman DA, Callaghan WM, Barfield WD. Perinatal regionalization: a geospatial view of perinatal critical care, United States, 2010-2013. Am J Obstet Gynecol. 2016
• Fang JL, Carey WA, Lang TR, Lohse CM, Colby CE. Real-time video communication improves provider performance in a simulated neonatal resuscitation. Resuscitation. 2014 Nov; 85(11):1518-22. Epub 2014 Aug 15. PMID: 25132477
• Colby CE, Fang JL, Carey WA. Remote video neonatal consultation: a system to improve neonatal quality, safety and efficiency. Resuscitation. 2014 Feb; 85(2):e29-30. Epub 2013 Nov 19
• Scheans P. Telemedicine for neonatal resuscitation. Neonatal Netw. 2014;33(5):283-287
• Fang JL, Collura CA, Johnson RV, Asay GF, Carey WA, Derleth DP, Lang TR, Kreofsky BL, Colby CE. Emergency Video Telemedicine Consultation for Newborn Resuscitations: The Mayo Clinic Experience. Mayo Clin Proc 2016 Dec; 91 (12):1735-1743 Epub 2016 Nov 22 PMID: 27887680

©2017 MFMER | 3671080-36
INDEX CASEphone call
from a
COMMUNITY
PEDIATRICIAN
Mother with no
prenatal care
presents with
placental abruption
LOCAL PEDIATRICIAN is concerned baby
may be peri-viable and is questioning whether
they should resuscitate the baby

©2017 MFMER | 3671080-37
INDEX CASE
CONNECTED
via a video call
Neonate was
more mature
(est. 28 weeks)
and bigger (1 kg)
GUIDED RESUSCITATION – Mask PPV,
placed UVC, checked CBC, blood gas, glucose,
Managed acidosis and hypoglycemia
Admitted and
subsequently
discharged
from the
NICU without
morbidities