Embed Size (px)
Citation preview

#teachproject
#teachproject
Good Morning!
Welcome to DAY 3
1
#teachproject
Were you able to complete the Values Check #2 exercise last
night?
a. Yesb. Noc. I meant to, but was busy
doing other things.
2
#teachproject
Values Exercise # 2Choose the answer closest to yours : “Women smoke because _______”?
a. They think it’s feminine
b. They want to control their weight
c. They love to smoke
d. It helps their stress levels
e. Other
4
#teachproject
Values Exercise # 2Choose the answer closest to yours :
“Tobacco manufacturers are _______”?
a. Too powerful
b. Gazillionaires
c. Killing millions of people every year
d. Coercing children and youth to smoke through their advertising campaigns
e. Other
6
#teachproject
Specific Populations and Tobacco
Use
7
#teachproject
Learning Objectives
• Increased salient factors in different populations.
• Enhanced skills at applying effective cessation.
8
#teachproject
Introduction (1): Defining Special Populations
• Defined as having 1 or more of:– T: Lack of prospective, longitudinal treatment trials.
– A: Less access to treatments, and/or
– D: Disproportionate tobacco-related health disparities, and/or
– V: Increased vulnerability to addiction, and/or
– P: >10% higher smoking prevalence than the general population of smokers, and/or
Adapted from: Borrelli B. (2010). Journal of Consulting and Clinical Psychology, 78(1), 1–12
#teachproject
Introduction (2)
• Historically neglected• Multiple barriers exist • Complex associations, yet:
– Robust, – Reproducible, – Clinically significant
Els & Kunyk (2008). Smoking Cessation Rounds, 2(2).

#teachproject
• Mental health issues• Medical issues• Addictions• Gambling disorders• People who are
homeless or under-housed
• Older Adults
• LGBTTTIQQ persons• Youth• Pregnant women• Incarcerated
individuals• Military recruits• Ethno-cultural groups• Aboriginal Persons
Why Focus on Specific Populations?
11
#teachproject
• People with MI/A• Homeless persons• Older Adults• LGBTTTIQQ persons
• Youth• Pregnancy• Incarcerated persons• Indigenous Peoples
Brief Focus on Selected Populations (1)
#teachproject
In which type of disorder would we see the highest rate of smoking prevalence?
a. Anxiety disorder
b. Major depression
c. Bi-polar disorder
d. Schizophrenia
e. Personality disorders
13
#teachproject
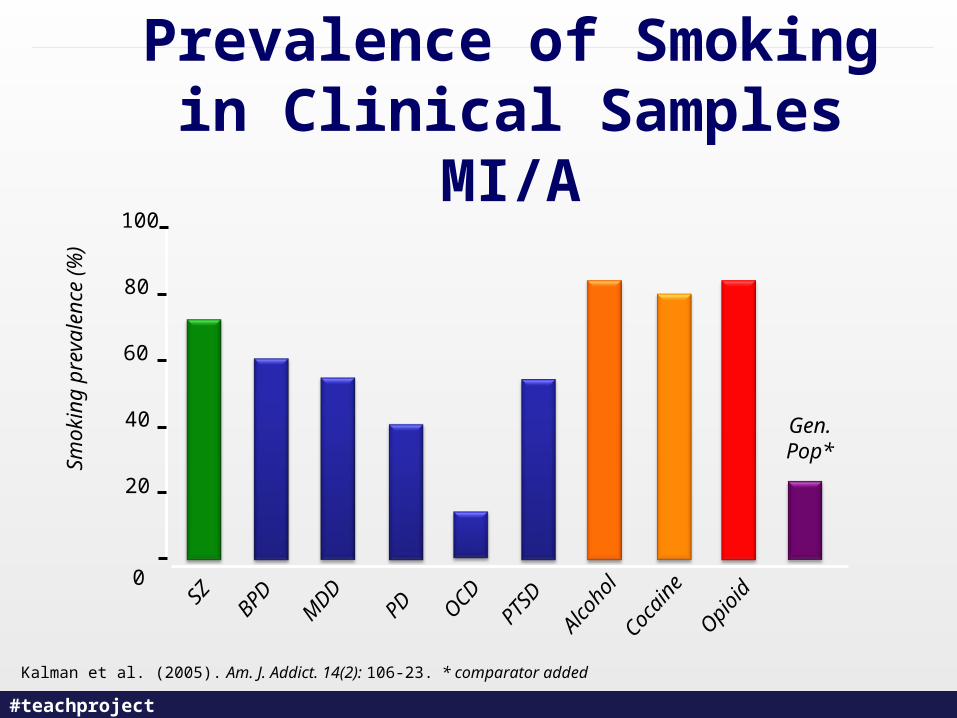
• Mental illnesses associated with higher rates:• Schizophrenia• Major mood disorders
– Depression– Mania / Bipolar illness
• Alcohol use• Other substance-related disorders• Anxiety disorders• Personality disorders
Lasser et al. (2000). JAMA, 284(20): 2606-10. Kalman et al. (2005) Am J Addict 14(2): 106-23.
14
Tobacco and Mental Illness (1)
#teachproject
• High prevalence and high consumption.
• Unique topography and variables.
• Increased morbidity and mortality.
• Treatment guidelines available
McClave et al.(2010). Am J Public Health, 100: 2464-72.
Tobacco and Mental Illness (2)
#teachproject
Kalman et al. (2005). Am. J. Addict. 14(2): 106-23. * comparator added
Prevalence of Smoking in Clinical Samples MI/A
Sm
okin
g pr
eval
ence
(%
)
SZ
BPD
MDD
PD OCD
PTSD
Alcoho
lCoc
aine
Opi
oid
100
80
60
40
20
0
Gen.Pop*
#teachproject
I have, or my organization has, cessation services available for specific
populations:
a. We are structured to be accessible to a range of populations.
b. We are accessible to a few specific populations on an as-needed basis.
c. I am not sure what is available.d. Limited cessation services are available
for specific populations.e. No services available
17
#teachproject
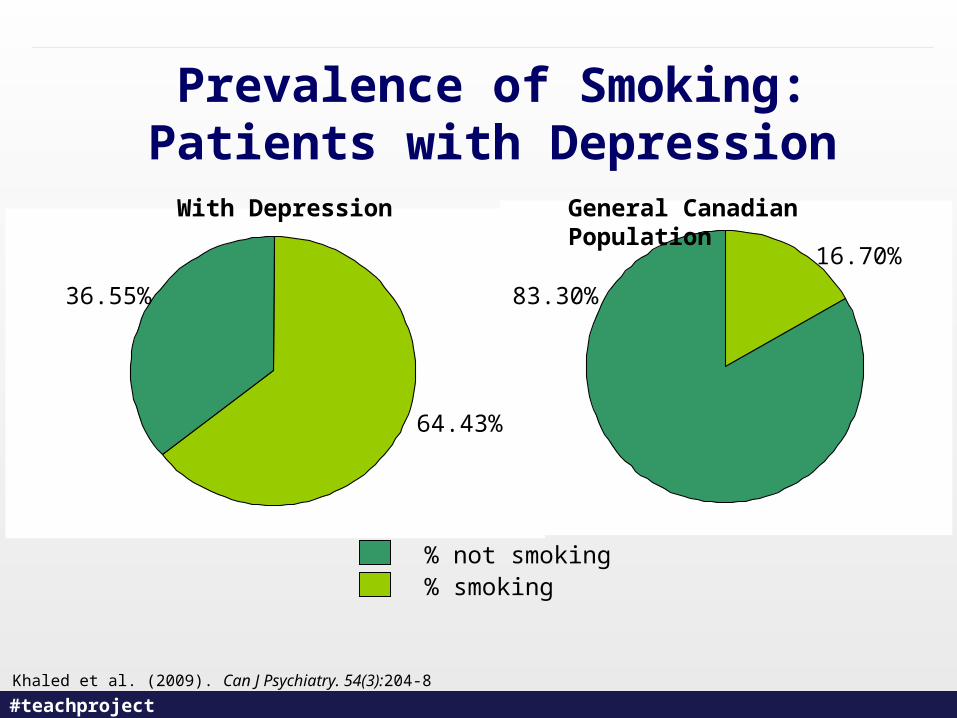
Prevalence of Smoking: Patients with Depression
18
% not smoking% smoking
With Depression General Canadian Population
36.55%
64.43%
83.30%
16.70%
Khaled et al. (2009). Can J Psychiatry. 54(3):204-8
#teachproject
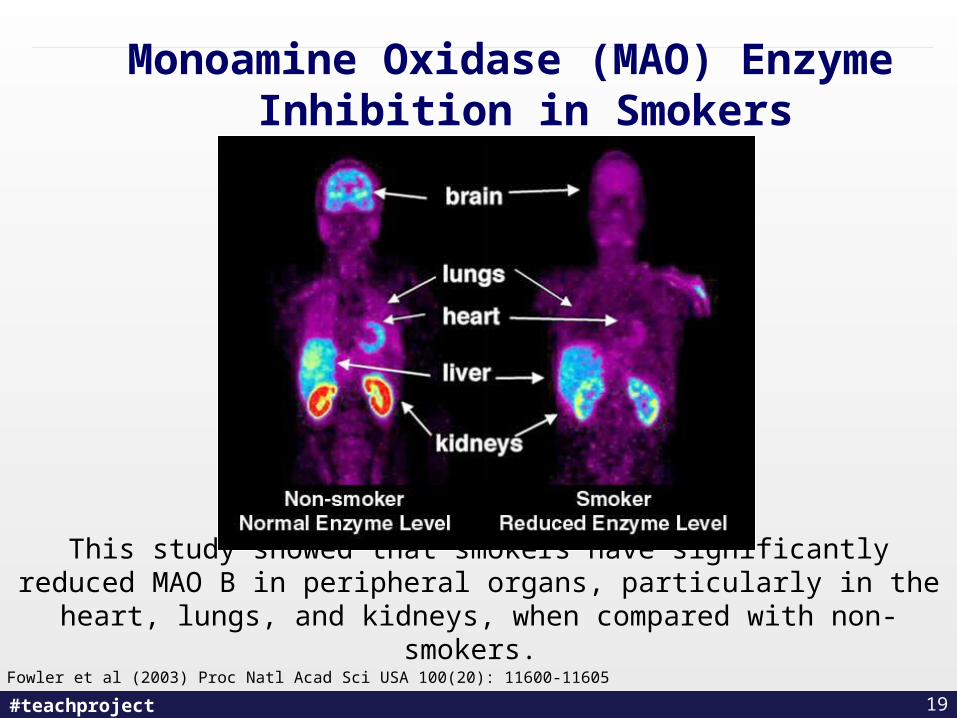
Fowler et al (2003) Proc Natl Acad Sci USA 100(20): 11600-11605
Monoamine Oxidase (MAO) Enzyme Inhibition in Smokers
This study showed that smokers have significantly reduced MAO B in peripheral organs, particularly in the heart, lungs, and kidneys, when
compared with non-smokers.
19
#teachproject
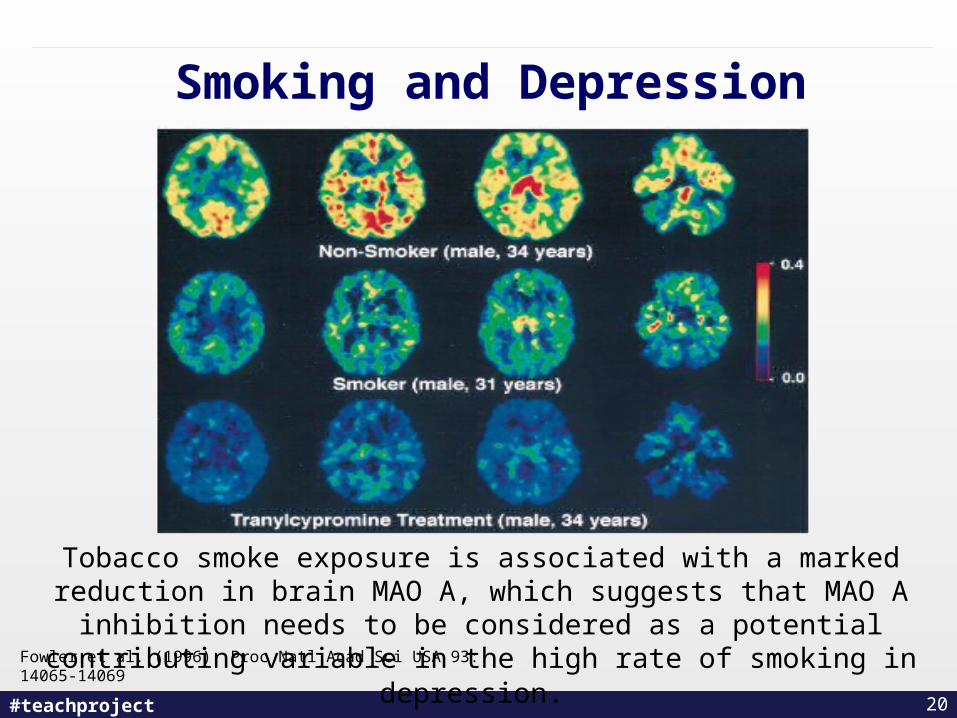
Smoking and Depression
Fowler et al. (1996). Proc Natl Acad Sci USA 93: 14065-14069
Tobacco smoke exposure is associated with a marked reduction in brain MAO A, which suggests that MAO A inhibition needs to be considered as a
potential contributing variable in the high rate of smoking in depression.
20
#teachproject
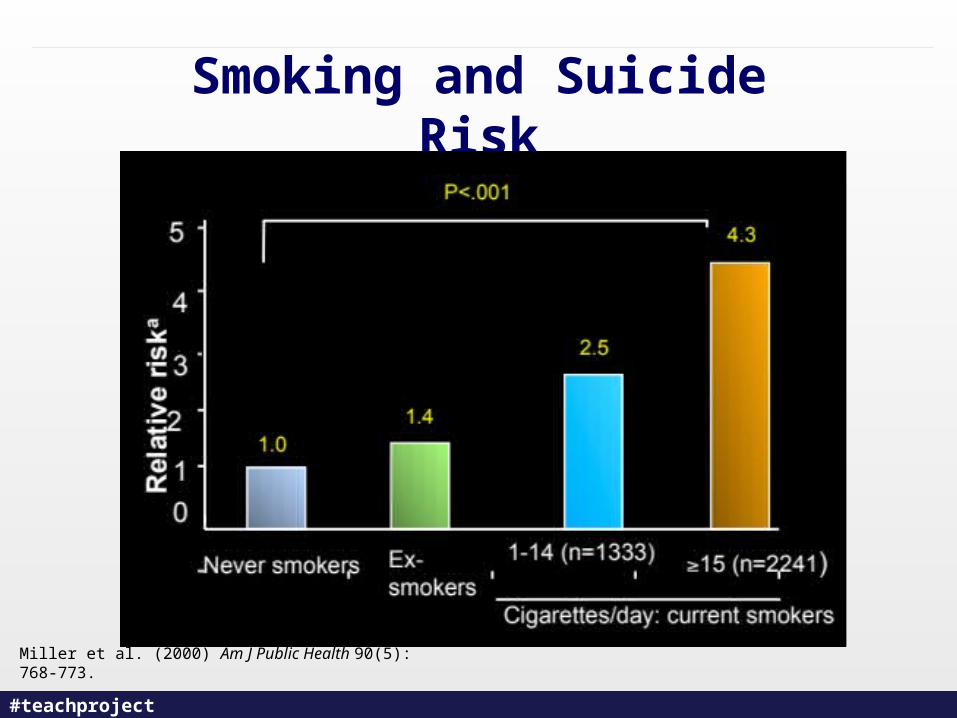
Smoking and Suicide Risk
Miller et al. (2000) Am J Public Health 90(5): 768-773.
#teachproject
Smoking and Mood Disorders
– Etiological explanations vary:1. MAO
2. Nicotine withdrawal
3. Caffeine
4. Pre-existing psychopathology
– Suicide risk– Treatment
Mackay J. et al., (2006). The Tobacco Atlas 2nd ed.Tonstad S & Els C. (2010). Clinical Medical Insights Therapeutics, 2: 681-695.
#teachproject
Treatment Implications
• NRT1
• Bupropion2
• Atypical antipsychotics1
• Varenicline3
1) George, Ziedonis, et al. (2000). Am J Psychiatry, 157 (11): 1835-42. 2) George, Vessicchio, et al. (2002). Biological Psychiatry, 52(1): 53 – 61.3) Smith, Lindenmayer, Davis, et al. (2009). Schizophrenia Research, 110: 149-155.
23
#teachproject
Safety Considerations
• History of Depression: • High prevalence of depressed mood when quitting• Need aggressive monitoring and treatment• Vigilance for up to 6 months after quitting• Beck Depression Inventory, consultation with
psychiatrist• Depression is a predictor of relapse
24
Wilhelm, Wedgwood et al. (2005). Drug and Alcohol Review, 25, 97 – 107.
#teachproject
Anxiety
• Rates of smoking 2x greater then general population
• Range 19.2 – 56%• Panic Disorder 40% • PTSD 63%
• Nicotine is anxiogenic• Lower anxiety within 2 weeks of quitting
25Kalman et al. (2005). Am. J. Addict. 14(2): 106-23. * comparator added
#teachproject
Gambling
1. Ontario Tobacco Research Unit (2010). Monitoring and Evaluation Series, Vol. 14/15(2).2. Glantz & Wilson-Loots (2003). Tob Control, 12(4): 411-3.
• Strong association• 45% tobacco prevalence in Ontario among problem gamblers1
• Limited empirical evidence• Systemic approaches, e.g. bans, have little impact on
monetary profits2
#teachproject
Smoking and Schizophrenia
– Impact on MSE– Impact on Medication– Cessation interventions
Ferron, Alterman, et al. (2009). Mental Health and Substance Use, 2(1), 64-79
#teachproject
Smoking and Schizophrenia
• Prevalence rates of 72.5% (up to 90%)
• More likely to smoke and less likely to quit
• Biological variables
• Quitting smoking may impact on symptoms of schizophrenia:
• Positive symptoms
• Negative symptoms
• Cognitive symptoms
Baker, Lubman, et al. (2010) Primary Psychiatry, 17(1):49-54. 28
#teachproject
Psychotropic Drug Interactions
Impacted:
• Clozapine
• Olanzapine
• Haloperidol
• Chlorpromazine
• Caffeine
Not Impacted:
• Risperidone
• Ziprasidone
• Aripiprazole
• Quetiapine
• Bupropion
DeLeon (2004). Psychopharmacology, 55(5): 491-493.
Desai, Seabolt, et al. (2001). CNS Drugs, 15(6): 469-494.
29
#teachproject
Psychotropic Drug Interaction Example: Clozapine
• Smoking cessation leads to increased clozapine plasma levels of up to 50%, which could lead to adverse events and toxicity1
• Increase could persist to up to 4 weeks• Plasma levels should be monitored frequently2 • Dose may require lowering of 30-40% of original dose3
• Warning signs that medication dose needs adjusting3 Worsening psychiatric symptoms– Excessive fatigue or sleepiness– Extrapyrimidal effects (i.e. tremor, slurred speech, dystonia)– Seizures
1) Cormac, Brown, et al. (2010). Acta Psychiatr Scand 2010: 121: 393–3972) DeLeon (2004). Psychopharmacology, 55(5): 491-493. 3) Lowe & Ackman (2010). Ann Pharmacother. 44(4):727-32
30
#teachproject
When is the “best” time for a person with substance use problems to quit
smoking?
a. Before they enter addiction treatment
b. Concurrently with their other treatment
c. After they have been treated
31
#teachproject
Concurrent Treatment of Tobacco and Other Substances
• 25% of clients in addiction treatment want to quit all substances1
• Relapse rates lower if all substances are addressed concurrently2
• Need to address therapists’ misconceptions of concurrent substance use treatment – Concurrent tobacco dependence treatment does not
jeopardize alcohol and non-nicotine drug outcomes3
1. Schroeder & Morris (2010) Annual Review of Public Health, 31: 297-314. 2. Kohn, Tsoh et al. (2003). Drug and Alcohol Dependence, 69(1): 61-71. 3. Kalman, Kim, et al. (2010 ). Clinical Psychology Review, 30: 12-24.
32
#teachproject
“A court could have sufficient basis to find that the failure to adequately treat the main cause of preventable disease and death qualifies as a violation of the legal duty that healthcare practitioners owe to patients habituated to tobacco use and dependence…”
Concurrent Treatment: A Standard-of-Care and a Duty-of-Practice
33
Torrijos & Glantz (2006). Tob Control 2006;15:447-451
#teachproject
Alcohol and Tobacco
• Strong correlation
• Dose-dependent
• Mortality rates increased
• Possible gateway hypothesis?
Selby & Els (2004). Alcohol & Drug Problems: A Practical Guide for Counsellors (pp. 709–731).
34
#teachproject
Smoking and Substance-Related Disorders
– Significant co-occurrence epidemiologically
– Increased mortality
– Biological and Sociological interface
– Optimal sequencing of treatment
– Treatment
Kalman et al. (2005). Am. J. Addict. 14(2): 106-23.
#teachproject
Summary Statement #1
Health care providers should screen persons with mental illness and/or addictions for tobacco use.
GRADE: 1A
Slide Source: CAN-ADAPTT http://www.can-adaptt.net/ http://www.can-adaptt.net/
#teachproject
Summary Statement #2
Health care providers should offer counseling and pharmacotherapy treatment to persons who smoke and who have a mental illness and/or addiction to other substances.
GRADE: 1A
Slide Source: CAN-ADAPTT http://www.can-adaptt.net/ http://www.can-adaptt.net/
#teachproject
Summary Statement #3
While reducing smoking or abstaining (quitting), health care providers should monitor the patient’s/client’s psychiatric condition(s).
Medication dosage should be monitored and adjusted as necessary.
GRADE: 1A
Slide Source: CAN-ADAPTT http://www.can-adaptt.net/ http://www.can-adaptt.net/
#teachproject
Clinical Considerations cont’d
• Offer pharmacotherapy/counselling
It should be noted that no (cessation) pharmacotherapy has been contraindicated in persons with mental illness unless medically contraindicated.
Recognize that involuntary abstinence from tobacco requires management with an agonist at sufficient doses.
The withdrawal/anxiety experienced by persons abstaining from smoking should be recognized and addressed; especially in acute care facilities.
Slide Source: CAN-ADAPTT http://www.can-adaptt.net/ http://www.can-adaptt.net/
#teachproject
Clinical Considerations cont’d
• Offer pharmacotherapy/counselling
• It should be noted that no (cessation) pharmacotherapy has been contraindicated in persons with mental illness unless medically contraindicated.
• Recognize that involuntary abstinence from tobacco requires management with an agonist at sufficient doses.
• The withdrawal/anxiety experienced by persons abstaining from smoking should be recognized and addressed; especially in acute care facilities.
Slide Source: CAN-ADAPTT http://www.can-adaptt.net/ http://www.can-adaptt.net/
#teachproject
Clinical Considerations cont’d
Monitor
• Consider that persons with mental illness and/or addiction(s) who smoke might need higher doses of NRT or combination therapies and for a longer duration.
• Assess for interactions with medications used for co- morbid conditions.
• Caffeine should be considered a compound to be monitored.
Slide Source: CAN-ADAPTT http://www.can-adaptt.net/ http://www.can-adaptt.net/
#teachproject
Clinical Considerations cont’d
• Monitor
Consider that persons with mental illness and/or addiction(s) who smoke might need higher doses of NRT or combination therapies and for a longer duration.
Assess for interactions with medications used for co- morbid conditions.
Caffeine should be considered a compound to be monitored.
#teachproject
• People with MI/A• Homeless persons• Older Adults• LGBTTTIQQ persons
• Youth• Pregnancy• Incarcerated persons• Ethno-cultural groups
Brief Focus on Selected Populations (2)
#teachproject
People who are homeless or underhoused
1. Tsai, J., & Rosenheck, R.A. (2012). Psychiatric Services in Advance. 2. Apollonio & Malone (2005). Tob Control;14: 409-415
• Difficult research population• 70-80 % tobacco prevalence1 • Master Settlement Agreement revealed
industry marketing2 • No peer-reviewed smoking cessation
programs • Interest likely exists in quitting
44
#teachproject
• People with MI/A• Homeless persons• Older Adults• LGBTTTIQQ persons
• Youth• Pregnancy• Incarcerated persons• Ethno-cultural groups
Brief Focus on Selected Populations (3)
#teachproject
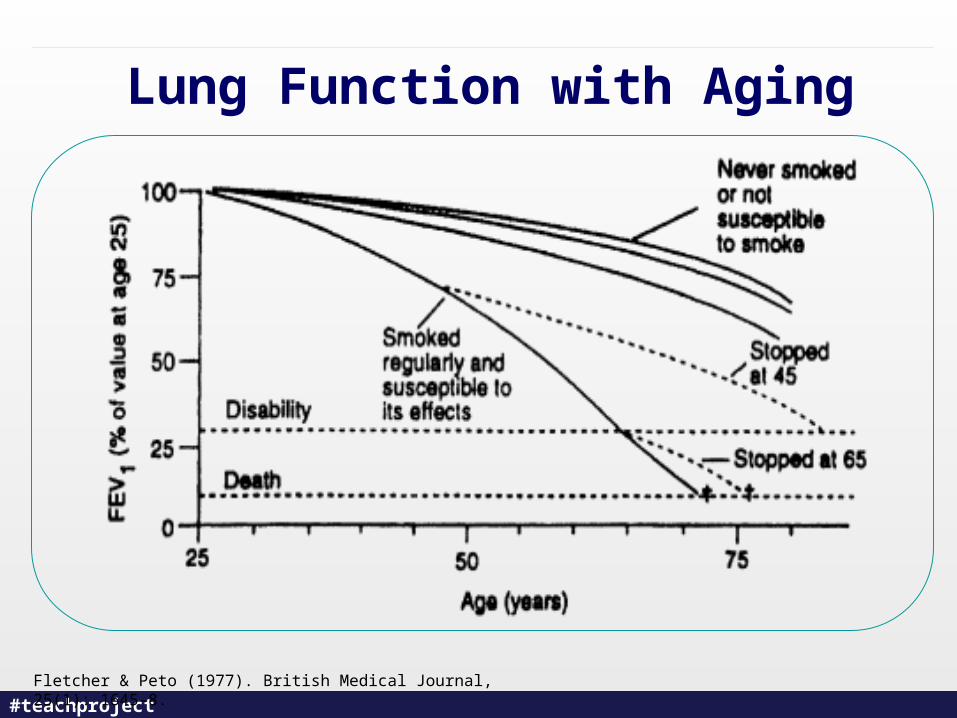
Lung Function with Aging
Fletcher & Peto (1977). British Medical Journal, 25(1): 1645-8.
#teachproject
Smoking in Elderly Persons
• Prevalence 10%
• Obstacles to smoking cessation
• Interventions
Tuppo, E.E. (2008). Smoking and the Older Person. Clinical Geriatrics
#teachproject
• People with MI/A• Homeless persons• Older Adults• LGBTTTIQQ persons
• Youth• Pregnancy• Incarcerated persons• Ethno-cultural groups
Brief Focus on Selected Populations (4)
#teachproject
LGBTTTIQ* Population
Greenwood et al (2005). Am J Public Health, 95(1): 145-51.
• Limited studies & almost no Canadian data
• Demographics vary & methodological flaws
• Reasons for high smoking rates?
• Treatment on small scale with limited evidence
* L = Lesbian; G = Gay; B = Bisexual; T= Transsexual; T = Transgendered; T = Two-Spirited;
I = Intersex; Q = Queer/Questioning
49
#teachproject
Statistics in LGBTTTIQ Community
• Some US studies estimate 48% of LGBTTTIQ population smoke
• Association between smoking and bacterial pneumonia, hairy leukoplakia, oral candidiasis and AIDS-related dementia
Forsythe, (2010). Healthy People: Lesbian, Gay, Bisexual and Transgender Health. Chapter on Tobacco Use.
50
#teachproject
• People with MI/A• Homeless persons• Older Adults• LGBTTTIQQ persons
• Youth• Pregnancy• Incarcerated persons• Ethno-cultural groups
Brief Focus on Selected Populations (5)
#teachproject
Youth & Smoking: There is no significant difference between the number of teenage males and teenage females
who smoke
a. True
b. False – Significantly more teenage females smoke
c. False – Significantly more teenage males smoke
52
#teachproject
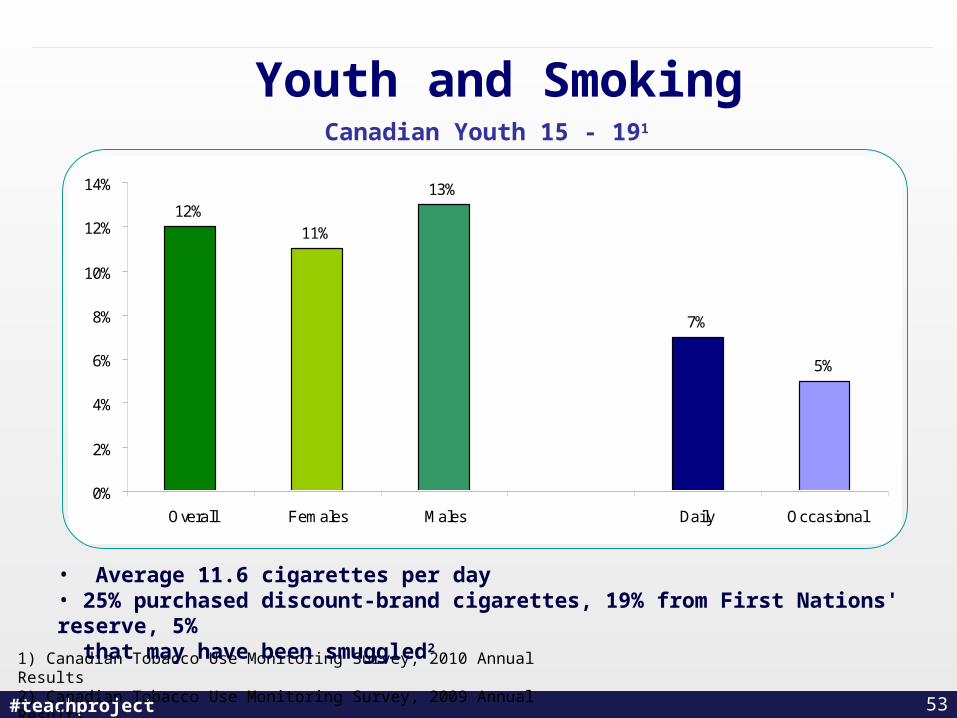
Youth and Smoking
1) Canadian Tobacco Use Monitoring Survey, 2010 Annual Results2) Canadian Tobacco Use Monitoring Survey, 2009 Annual Results
53
• Average 11.6 cigarettes per day• 25% purchased discount-brand cigarettes, 19% from First Nations' reserve, 5% that may have been smuggled2
12%11%
13%
7%
5%
0%
2%
4%
6%
8%
10%
12%
14%
Overall Females Males Daily Occasional
Canadian Youth 15 - 191
#teachproject
Young Adult Male Smoking: 20-24 Years of Age
• 24% are Current Smokers has consumed 100 cigarettes in his/her life and has smoked within
the last 30 days
• 16.4% are Daily Smokers has consumed 100 cigarettes in his/her life and has smoked daily
for the last 30 days
• 8.5% are Former Smokers Someone who has not smoked in the last 30 days
• 67.5% are Non Smokers Someone who has never smoked 100 cigarettes or more in his life
Canadian Tobacco Use Monitoring Survey, 2010 Annual Results 54
#teachproject
Other Associations in Youth
1. De Von Figueroa-Moseley, Landrine, Klonoff. (2004). Addictive Behaviors, 29: 245-251 2. Dube, Felitti, et al. (2003). Pediatrics, 111(3): 564-723. Potter, Peterson, et al. (2004). Nicotine & Tobacco Research, 6(3): 397-425. 4. Cornelius, Sallorum, et al. (2001). Annals of the New York Academy of Sciences, 932: 78-90.5. Mäkikyrö, Hakko, Timonen, et al. (2004). Journal of Adolescent Health, 34(3): 250-2536. Milberger, Biederman, Faraone, et al. (1997). Journal of the American Academy of Child and Adolescent Psychiatry, 36(1): 37-44.
• Sexual and physical abuse/trauma1,2
• Other psychiatric disorders–Eating disorders4
–Depressive disorders7
–Suicide attempts5
–Substance abuse5
–ADHD6
• Impoverished and dysfunctional households3
55
#teachproject
• People with MI/A• Homeless persons• Older Adults• LGBTTTIQQ persons
• Youth• Pregnancy• Incarcerated persons• Ethno-cultural groups
Brief Focus on Selected Populations (6)
#teachproject
Women and PregnancyWhy do women smoke?
• Controlling weight / fear of weight gain• Addiction• Concurrent mental health problems• Coping with emotions, stress• “Fitting in”• Fashion, style and marketing
Risks decrease with quitting: • Vaginal bleeding, premature delivery, abruptio placenta
and placenta previa• Spontaneous abortion• Perinatal mortality• Better chance of having a healthier birth weight• Easier time with breastfeeding
57
#teachproject
Evidence-Based Interventions• Maximum quit rate about 20% despite best
intervention
• Self-help materials tend to have good quit rates
• Telephone quit lines are a cost-effective way to reach smokers with some efficacy
• Counselling doubled abstinence rates
• Seven quit-line counselling sessions
• Brief treatment often no different than intensive counselling
• Consider NRT if behavioural interventions do not work
Lumley, Chamerlain, et al. (2009). Interventions for promoting smoking cessation during pregnancy. Cochrane Database of Systematic Reviews
58
#teachproject
• People with MI/A• Homeless persons• Older Adults• LGBTTTIQQ persons
• Youth• Pregnancy• Incarcerated persons• Ethno-cultural groups
Brief Focus on Selected Populations (7)
#teachproject
Incarcerated Individuals
1. Cropsley et al. (2008). American Journal of Public Health, 98, 1894–19012. Donahue (2009). Journal of Offender Rehabilitation, 48: 7, 589 — 6043. Diamond et al. (2009). Adm Policy Ment Health, 29: 21–40
• Extremely high smoking prevalence:– Up to 91%2
– Nearly 50% report other substance abuse and mental health issues3 – 75-100% relapse rate upon release3
• Limited treatment or programs available– 1 RCT to date; outcome indicates a combination of CBT +
pharmacotherapy is effective (quit rate of 14% at 6-month follow-up)1
• Smoking bans will contribute to a healthier environment, better air quality; but should be coupled with cessation interventions for sustained quit– Forced abstinence through bans leads to short-term cessation only
60
#teachproject
• People with MI/A• Homeless persons• Older Adults• LGBTTTIQQ persons
• Youth• Pregnancy• Incarcerated persons• Ethno-cultural groups
Brief Focus on Selected Populations (7)
#teachproject
Are you aware of the differences between non-traditional and traditional tobacco
use in First Nations?
a. Yes, I am sensitive to this in my practice.
b. Yes but I don’t know how to approach it with my Aboriginal clients.
c. No, this is something I need more information about.
62
#teachproject
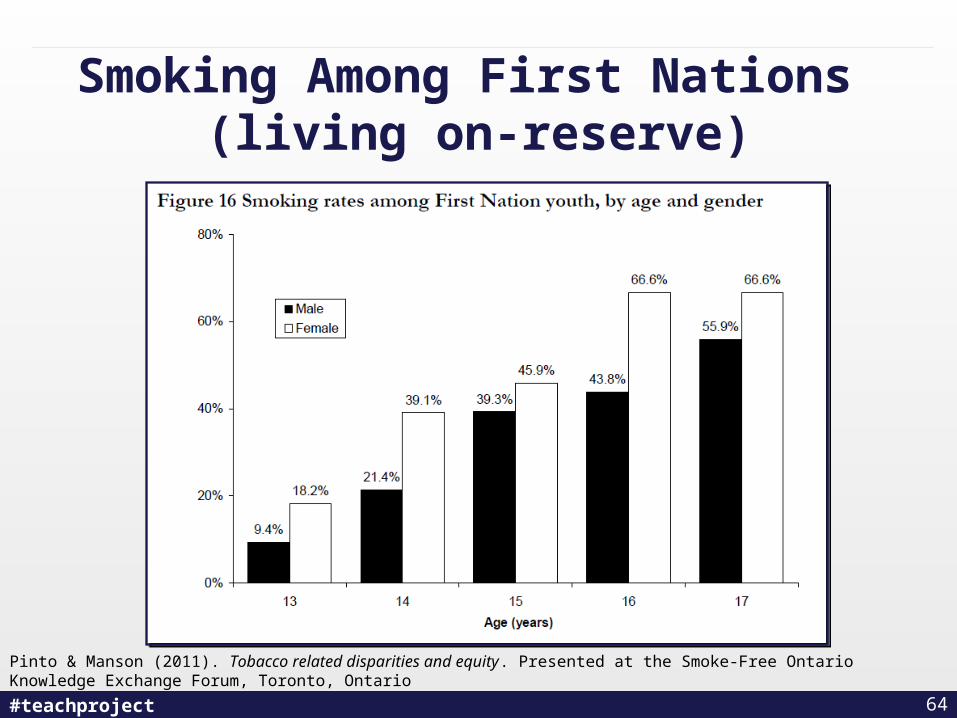
Indigenous Populations
• What is traditional use of tobacco?
• Smoking rates higher
• Lower age groups overrepresented
*Although the tobacco plant is sacred among some First Nations, it is not revered by all groups or by the Inuit
Health Canada, 2004. Baseline Study Among First Nations On-reserve and Inuit in the North. http://www.hc-sc.gc.ca/fniah-spnia/substan/tobac-tabac/index-eng.php
63
#teachproject
Pinto & Manson (2011). Tobacco related disparities and equity. Presented at the Smoke-Free Ontario Knowledge Exchange Forum, Toronto, Ontario
Smoking Among First Nations (living on-reserve)
64
#teachproject
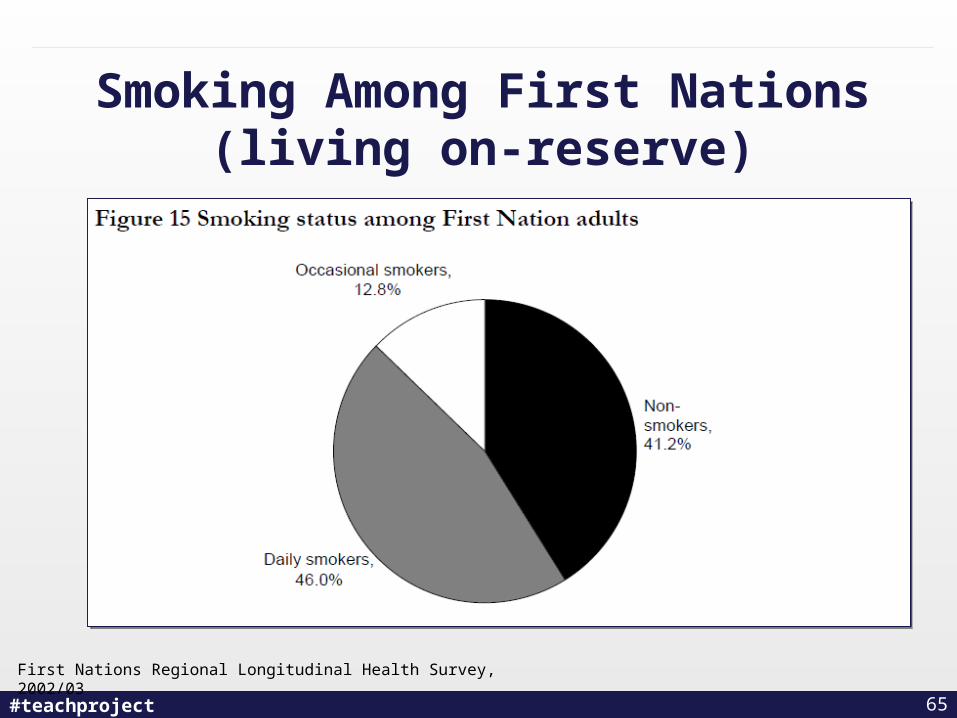
Smoking Among First Nations (living on-reserve)
First Nations Regional Longitudinal Health Survey, 2002/03
65
#teachproject
Small Group Discussion
• At your tables, please share your experiences providing cessation services to specific populations…..
• What are some key considerations?
• What questions to do you have?
66
#teachproject
Factors to Consider
• Diversity among Indigenous Populations • Access to healthcare resources• Traditional approaches to healing/recovery• Geographical location• Intergenerational trauma • Economic incentives from tobacco
sales/production in some communities
67
#teachproject
Focus on Special Populations: Implications for Tobacco Control
• High prevalence & high risk• Smoking impacts disproportionately • Rates overrepresented in subgroups• Mentally ill youth at greater risk of uptake• Often not addressed by mainstream tobacco
control approaches
68
#teachproject
Contingency Management
• Incentive based programming • Despite demonstrated efficacy in addictions limited use
in smoking cessation• Barriers include people’s attitude towards incentives in
treatment.
69
Ledgerwood (2008). Current Drug Abuse Reviews 1(3): 340-9
#teachproject
Suggestions for Tobacco Control
• Identify high-risk youth• Identify hard-to-reach populations• Offer counselling/medications in criminal justice
settings• Parity of coverage
70
#teachproject
Conclusions
• Evidence emerging• Supporting cessation is crucial for health
promotion• Needed:
– More comprehensive and tailored supports – Further research– Advocacy
71
#teachproject
Case Discussion• Kevin is a 45-year-old male who is living with schizophrenia
who reports regular smoking since age 14. • He is on clozapine, which he takes regularly as prescribed,
and was referred to the tobacco clinic by his community support worker.
• His support worker noticed that even though Kevin smokes contraband cigarettes, the financial impact of his smoking affects his overall quality of life and ability to “make ends meet” between receiving government disability cheques.
• Kevin states that he smokes approximately 76 cigarettes per day, and says that he has been wanting to quit for a long time.
• His CO levels are 25 ppm. In his assessment, Kevin states, “I heard you people can make quitting easy – that’s what I need.
• This is it! I am walking out of here a non-smoker.”
72
#teachproject
Discussion Questions
1. In addition to the financial impact and # of cigarettes per day, what other areas would you want to assess (and address) with respect to Kevin’s tobacco use?
2. What do you think of Kevin’s decision to quit immediately? How would you respond?
3. If you were recommending a nicotine patch, what level would you recommend he start with?
4. What psychosocial intervention(s) might be helpful in this case?
73
#teachproject
Break Time: 15 Minutes
74
#teachproject
Tobacco Industry Denormalization
Michael Perley: Director,
Ontario Campaign for Action on Tobacco
Based on research and presentations from the Non-Smokers’ Rights Association
75
#teachproject
Learning Objective
Contextualize tobacco use within a broader tobacco control policy framework
76
#teachproject
What is Tobacco Industry Denormalization (TID)?
• Telling the public the truth about the tobacco industry’s role in the perpetuation of the tobacco epidemic in appropriate language
• Show the public why the tobacco industry falls outside the boundaries of normal business behaviour
• Reverse the industry’s decades-long effort to normalize itself
77
#teachproject
What Tobacco Industry Denormalization Is Not
• Messages or programs that do not refer to the tobacco industry and its role in the epidemic, such as those referring to “smoking” or “smokers” as their main subjects
78
#teachproject
From this list, select one statement with which you agree the most strongly.
a. Cigarettes are too dangerous to be sold at all;
b. The tobacco industry rarely/never tells the truth about health effects of smoking;
c. The tobacco industry is mostly/completely responsible for health problems smokers have because of their smoking;
d. The Ontario government should sue tobacco companies for health care costs caused by tobacco products;
e. The tobacco industry should be fined by government for money earned from tobacco sales to minors.
79
#teachproject
Tobacco Industry Behaviour
1950s-60s• First linkage of tobacco-lung cancer in medical
literature; industry PR firm suggests counter-attack against scientists to reduce public worry
• The TIRC plan: spend massively to block scientists and public health officials from warning people of potential health hazards
• Industry researchers find numerous carcinogens in tobacco smoke: research hidden
80
#teachproject 81
#teachproject
Tobacco Industry Behaviour (2)
• In 1962, the Chairman of British American Tobacco asked:“If we make safer brands, how to justify continuing the sale of other brands? It would be admitting that some of (our) products already on the market might be harmful.” (A McCormick, British American Tobacco, 1962)
1970s
• “Safer” cigarettes designed and tested, but companies could no longer afford to offer safer cigarettes to smokers
82
#teachproject 83
#teachproject
Tobacco Industry Behaviour (3)
• The 1977 Bath Summit (BAT, PM, ITL, RBH, RJR): agreed to deny known health effects of tobacco and conceal known toxicity of tar, nicotine and other chemicals in tobacco
1980s• Company scientific labs shut down, medical findings
hidden or destroyed
84
#teachproject
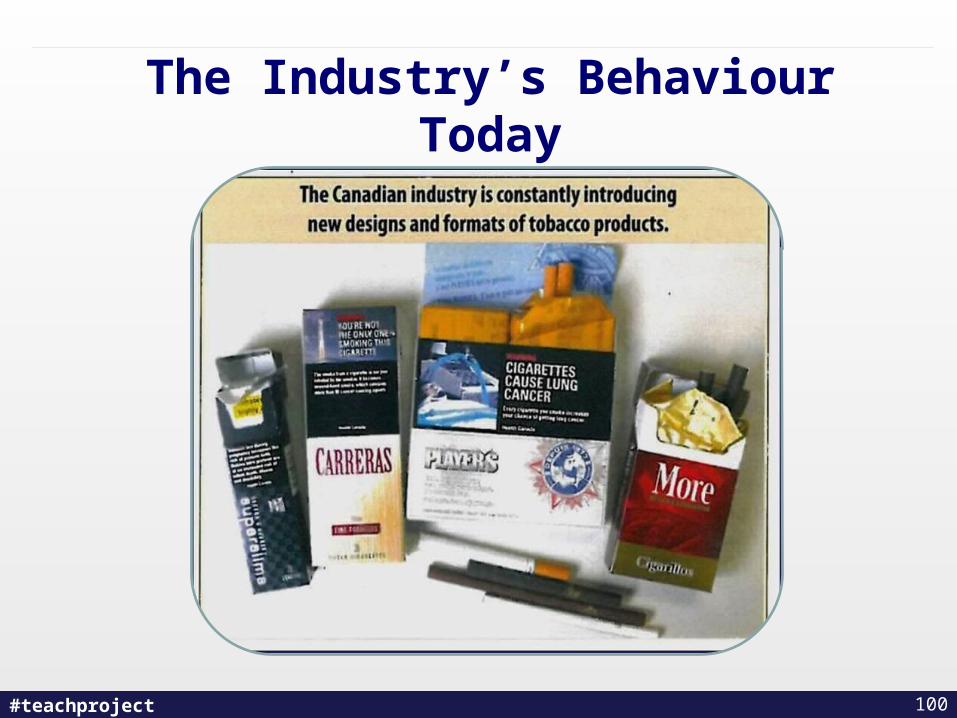
The Industry’s Behaviour Today
“Cigarette makers destroyed research on health risks, court hears”
- The Montreal Gazette, 2 April 2012
“A former tobacco executive has admitted he helped to destroy research documents in the 1990s, when he was Vice-President of Legal Affairs at Imperial Tobacco and a member of the firm’s management committee.”
“This all happened 20-some-odd years ago, and I have no memory of it”
- Roger Ackman
85
#teachproject
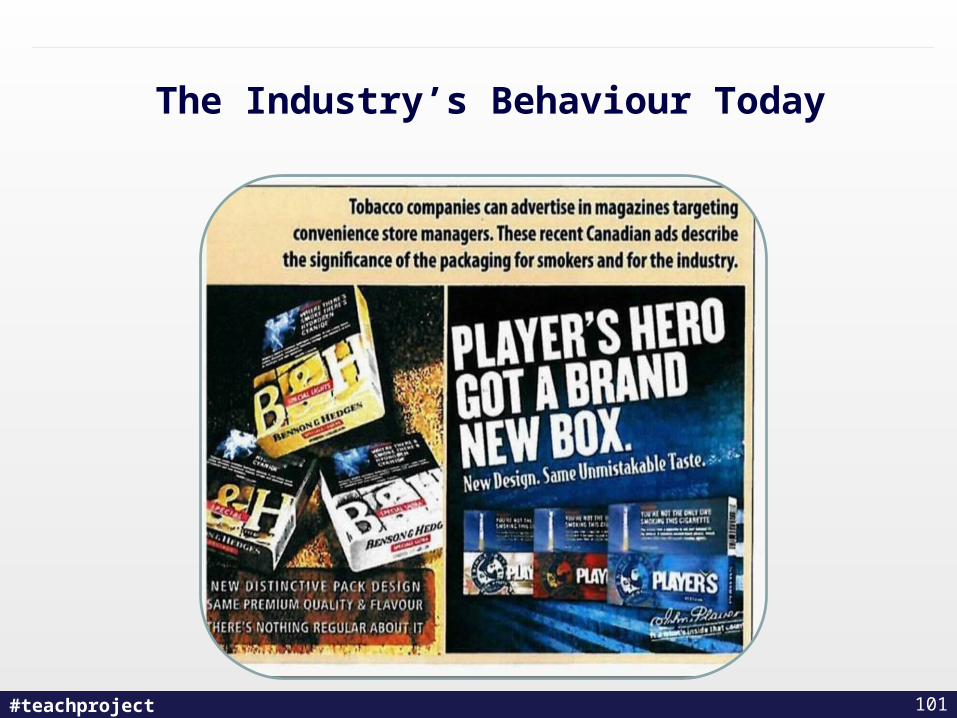
The Industry’s Behaviour Today (2)
“Documents show Imperial sought to discredit scientific evidence against tobacco, trial hears”
- The Montreal Gazette, 15 March 2012
“When Alcan Aluminum Ltd became one of the first companies to institute a workplace ban on smoking in 1980, Imperial Tobacco launched a campaign to convince the manufacturer to reverse its ban, according to evidence before the Quebec class action lawsuit against Canada’s three largest tobacco companies.”
86
#teachproject
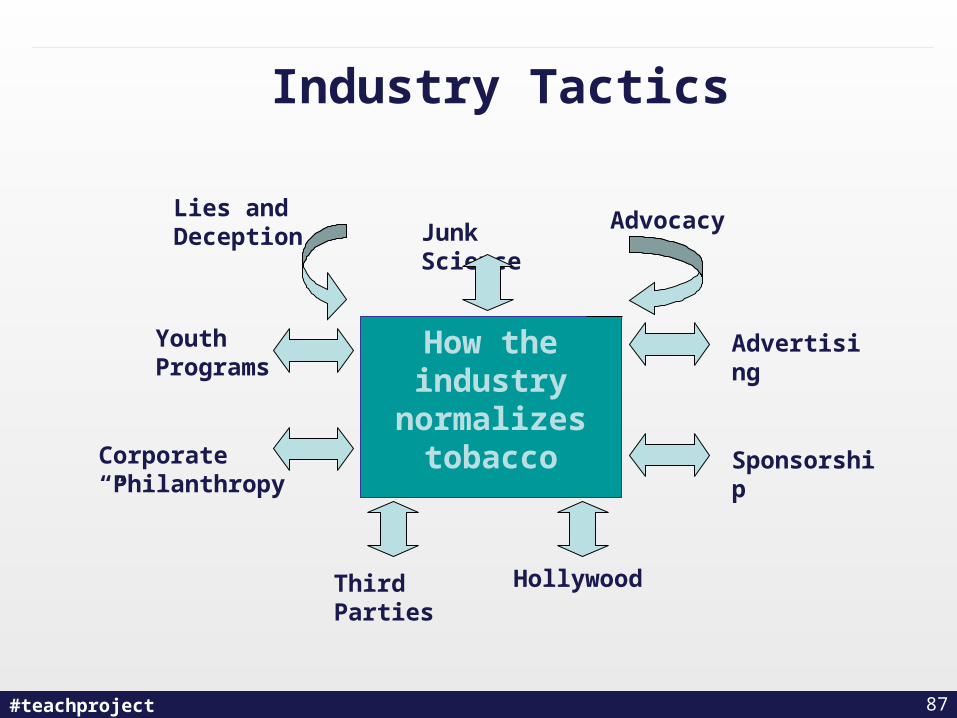
Industry Tactics
How the industry
normalizes tobacco Sponsorship
Youth Programs
Corporate “Philanthropy”
Third Parties
Lies and Deception
Advertising
Advocacy
Hollywood
Junk Science
87
#teachproject
What the Industry Really Thinks
“In order to make further inroads into the younger segment, we must continue to project an image that is consistent with the needs and values of today’s younger smokers.”
(RJR, 1989)
“Although the key 15-19 age group is a must for RBH there are other bigger volume groups that we cannot ignore.”
(RBH, 1997)
88
#teachproject
What the Industry Really Does
“The 1988 tracking study is the second of a planned series of research studies into the lifestyles and value systems of young men and women in the 13-24 age range.”
(ITL, 1988)
89
#teachproject
Operation ID:The Tobacco Industry’s
Youth-Friendly Face
90
#teachproject
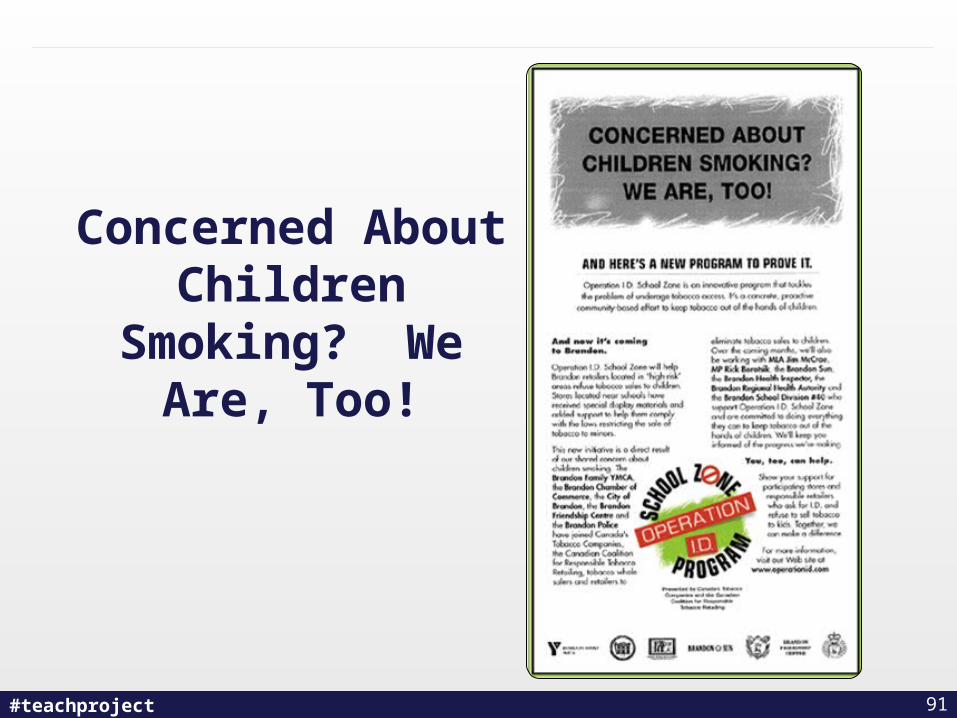
Concerned About Children Smoking?
We Are, Too!
91
#teachproject
Three on Three Hockey
92
#teachproject
Lanny McDonald
93
#teachproject
Guy Carbonneau
94
#teachproject
In 2002, the Ontario Medical Association drew the following conclusions about
Operation ID:• “Tobacco industry documents make clear that their
youth access programs have little or nothing to do with reducing youth smoking”.
• “The failure of these programs is inevitable because they are voluntary”.
• “Youth access and educational programs target the wrong outcome, access, rather than consumption”.
Perley, M., (2002). More Smoke and Mirrors: Tobacco Industry-Sponsored Youth Prevention Programs in the Context of
Comprehensive Tobacco Control Programs in Canada. Ontario Medical Association.
95

#teachproject
Key Industry Tactics/Messages
A risky – but legal – product
• “We don’t market to children”• Light and mild• Questionable research (attacks on the risks of second-
hand smoke)• Cigarette smuggling uncontrollable• Rights and freedoms: the “nanny state”• Economic fallout• Front groups (mychoice.ca [now defunded by ITL],
FAAC, hospitality)
96

#teachproject
Industry Tactics:Advertising and Promotion
• Power walls (banned in most provinces, including Ontario)
• Point-of-sale signage and displays (as above)
• Branding
• Movies
• Grey areas (bar promotions)
97

#teachproject
Industry Sponsored Tobacco Promotions
http://www.tobaccofreekids.org/ adgallery/display.php3?ID=204
98
#teachproject
Benson and Hedges Cigarette Girls for a 2003 promotion aimed at Young Adults
99
#teachproject
The Industry’s Behaviour Today
100
#teachproject
The Industry’s Behaviour Today
101
#teachproject
The Industry’s Behaviour Today
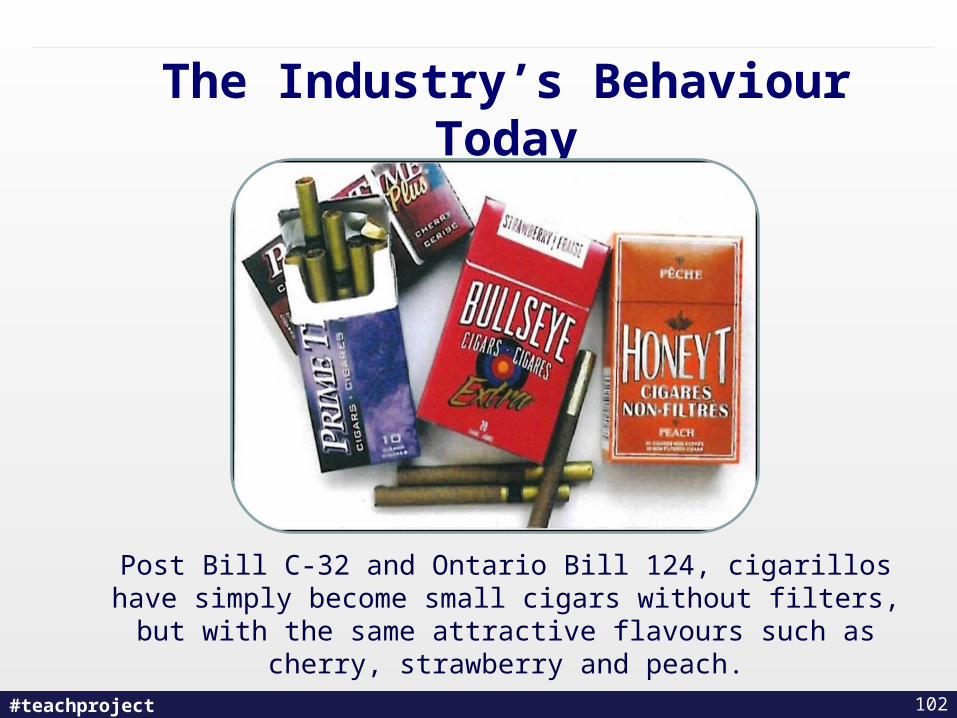
Post Bill C-32 and Ontario Bill 124, cigarillos have simply become small cigars without filters, but with the same
attractive flavours such as cherry, strawberry and peach.
102

#teachproject 103
#teachproject
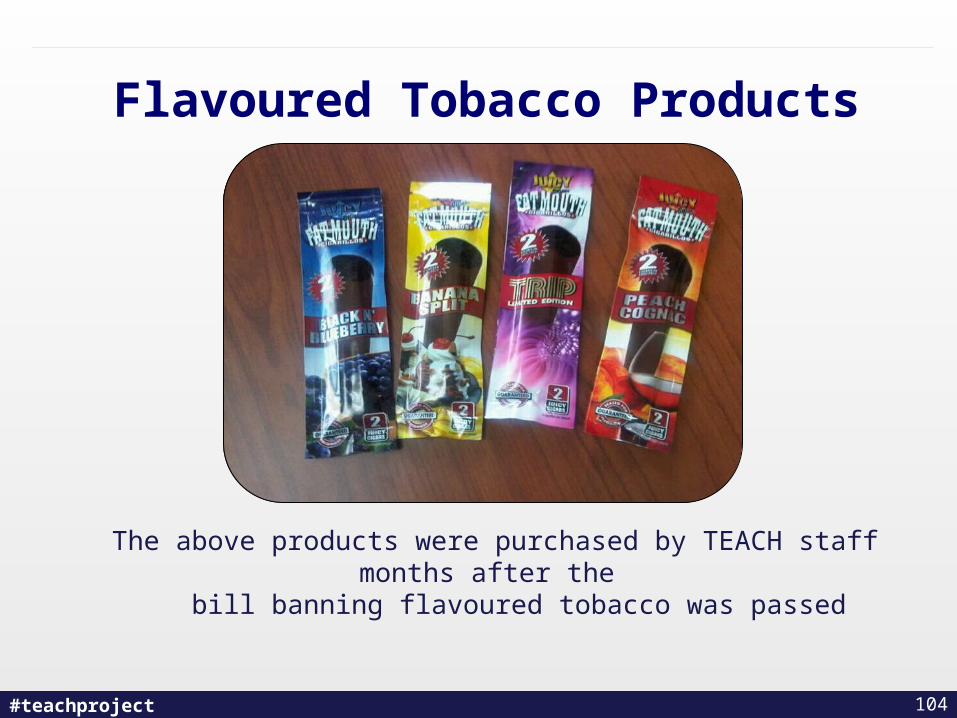
Flavoured Tobacco Products
104
The above products were purchased by TEACH staff months after the bill banning flavoured tobacco was passed
#teachproject
An Ontario Response to Flavoured Products
• NDP MPP France Gélinas introduces a Private Member’s Bill to ban all flavoured products, and new tobacco products such as sticks, strips and orbs now being tested in the U.S., across Ontario (April 17, 2012)
105
#teachproject
Tobacco Industry Denormalization Strategies
Objective: Expose the Industry
• Combat myths about tobacco products
• Draw attention to nature, extent, impact of tobacco industry advertising/promotional activities
• Draw attention to role of other organizations in supporting promotion and sale of tobacco
106

#teachproject
Tobacco Industry Denormalization Strategies (2)
• Paid media (CA, Mass., other US states)
• Earned media (NSRA exposure of St. Michael’s University acceptance of ITL corporate ethics funding; CCS/NSRA protest chief tobacco lobbyist’s presence on WCH board; U of Sask. SU rejects $250,000 grant from ITL)
• Research/lobbying/advocacy
107
#teachproject
Unsweetened Truth
108
#teachproject
Do You Have What it Takes…?
109
#teachproject
Smokenders
110
#teachproject
Smoking Dog
111
#teachproject
Demon Awards
112
#teachproject
Contraband
113
#teachproject
Contraband
What does this word mean to you?
With a partner, discuss this for a few minutes.
114
#teachproject
Are some cigarettes more harmful than others?
A. No- all have the same level of danger to health, no matter where the cigarettes are manufactured
B. Yes- unregulated cigarettes are more harmful
C. Maybe- I need some more information to make a decision
115
#teachproject
The 1990s Smuggling Crisis
• Tobacco industry-driven: tax-free main-brand industry products exported to bonded warehouses in New York State, smuggled back into Ontario/Quebec
• Result: Federal and several provincial governments cut tobacco taxes by 50% in 1994
• Impact: Up to 40,000 excess deaths as a result of increased youth smoking (Health Canada draft)
116
#teachproject
Smuggling/Contraband Today
• The product: 200-cigarette “baggies” manufactured on 4-5 U.S./Ontario/Quebec reserves (contrast: 190+ reserves in Ontario alone)
• Involvement of non-FN organized crime elements: contraband tobacco trade funds smuggling of drugs/guns/people
117
#teachproject
Smuggling/Contraband Today (2)
• A problem for all communities: $8-10/baggie cigarettes vs. $50-70+ discount/main brands help lead to 1) FN community smoking rate of 59%; 2) flattening/reversal of non-FN prevalence declines
• Sources: on-reserve smoke shacks (some southern Ontario/ Quebec reserves), off-reserve non-FN supply chains
118

#teachproject 119

#teachproject 120

#teachproject 121
#teachproject
Solutions
• Nation-to-nation negotiations/trade and other economic agreements
• Off-reserve enforcement esp. re: organized crime
122
#teachproject
Ontario’s Bill 186
• Tobacco leaf management system
• Fine cut tobacco marking system
• New fine structure
• Seizure “in plain view”
• Arrangements and agreements with First Nations
123
#teachproject
The 2012 Ontario Budget
• Promises to double enforcement efforts – annual enforcement costs to increase by $34 million by 2014-15.
• Numerous measures promised including increased fine, POA Part 1 tickets, vehicle impoundment, other best practices.
124
#teachproject
Questions?
125
#teachproject
Lunch!30 Minutes
126
#teachproject
Ask the Expert! Q & A Session
Dr. Peter SelbyDr. Charl ElsDr. Marilyn HerieAlexandra Andric
127

#teachproject
Break Time: 15 Minutes
128
#teachproject 129
Harm Reduction
#teachproject
Learning Objective
Apply harm reduction strategies with clients who are not ready to quit smoking
130
#teachproject
What is your perspective on harm reduction and tobacco use?
a. There is no such thing – all tobacco use is harmful
b. I can see that might be necessary with some populations
c. I believe in using a harm reduction approach
d. I’m not sure - I need more information
131
#teachproject
Discussion
What is one thing you want to take away about harm
reduction?
132
#teachproject
“ Don’t give up the ship in a storm because you cannot hold back the winds. You must not deliver strange and out of the way speeches to people with whom they will carry no weight because they are firmly persuaded the other way.
Instead, by an indirect approach, you must strive and struggle as best you can to handle everything tactfully – and thus what you cannot turn to good, you must at least
make as little bad as you can.”
St. Thomas More 1478-1535, Utopia, CWM, v. 4, pp. 99, 101
133
#teachproject
Do you drive a car with anti-lock brakes?
a. Yes
b. No
c. Do bikes count?
134
#teachproject
Which type of vehicle allows you to stop faster?
a. Cars with anti-lock brakes
b. Cars without anti-lock brakes
c. No difference
135
#teachproject
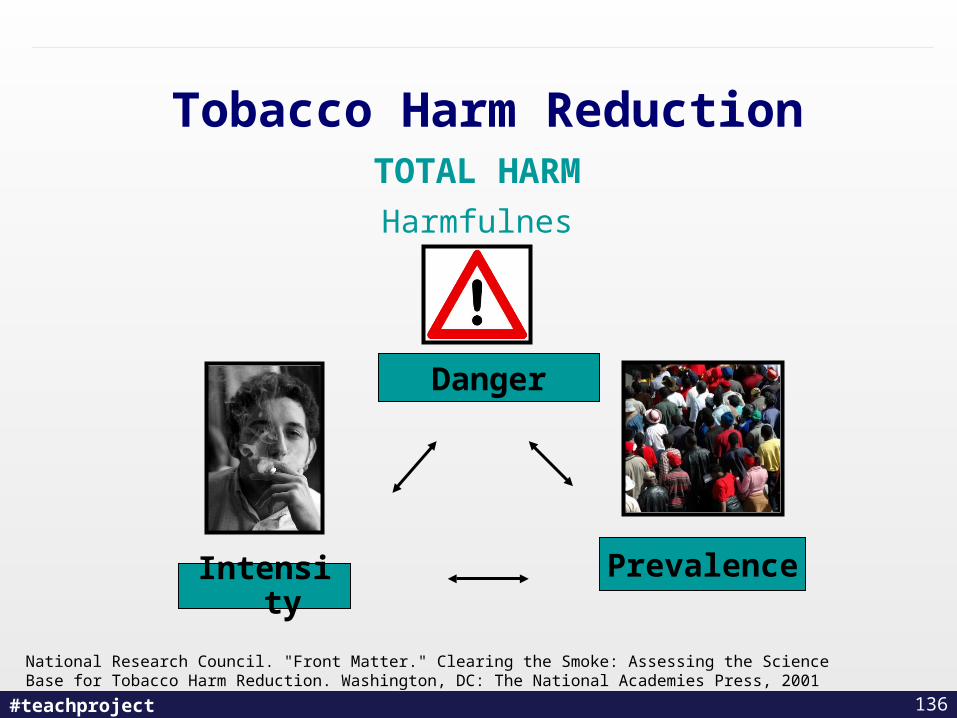
Tobacco Harm Reduction
National Research Council. "Front Matter." Clearing the Smoke: Assessing the Science Base for Tobacco Harm Reduction. Washington, DC: The National Academies Press, 2001
TOTAL HARM
Harmfulness
Danger
IntensityPrevalence
136
#teachproject
Issue: The Precautionary Principle – Can science of nicotine help?
• The precautionary principle:– "When an activity raises threats of harm to human health
or the environment, precautionary measures should be taken even if some cause and effect relationships are not fully established scientifically. In this context the proponent of an activity, rather than the public, should bear the burden of proof."
• A key issue in advocating a tobacco control harm reduction strategy involving the use of less harmful forms of nicotine delivery, is the evidence of safety of nicotine per se.
Kurland (2002). The Heart of the Precautionary Principle in Democracy. Public Health Reports, December.
137

#teachproject
Most Harmful – least regulated
Some Harm – some regulation
Least Harmful – most regulated
138
#teachproject
A Controversial Topic?
• Tobacco control has always taken a harm reduction perspective
– Smoke free policies, taxation, etc.
• There is support for harm reduction – CAMH, OMA
• What do we mean by harm reduction?
139
#teachproject
General View on Harm Reduction
• Aims to reduce the adverse health, social, and economic consequences of drug use without requiring abstinence
• Abstinence is healthiest choice• Focuses on the most immediate and achievable
changes• Public health alternative to the moral/criminal and
disease models of drug use• Non-judgmental, non-coercive
140
#teachproject
General Principles of Harm Reduction
• End users should have a voice in the creation of programs and policies designed to serve them (client-centered care)
• Values patient autonomy and provider patience
• Culturally sensitive
• Although abstinence from tobacco is recommended, many smokers are unable or not ready to quit
141
#teachproject
Benefits of Harm Reduction Approach (1)
• Engages
• Increases confidence
• Changes behavioural patterns
Daily use Abstinence
Continuum
Reduction
142
#teachproject
• Appears deeply rooted in some communities (i.e.: those with mental health issues, aboriginal)
• Creates a market incentive for ever-better products to replace cigarettes
• “Quit or die” is irresponsible, unethical and unrealistic
• Millions are highly addicted and have low cessation rates
143
#teachproject
Cautions against Harm Reduction
• Distraction from quitting – Need more resources devoted to quitting
• Premature admission of defeat • Extra harm to people that would have otherwise
quit completely• Potential for young people to start with products
they believe it to be safe• Ex-smokers may use products as an option
causing relapse
144
#teachproject
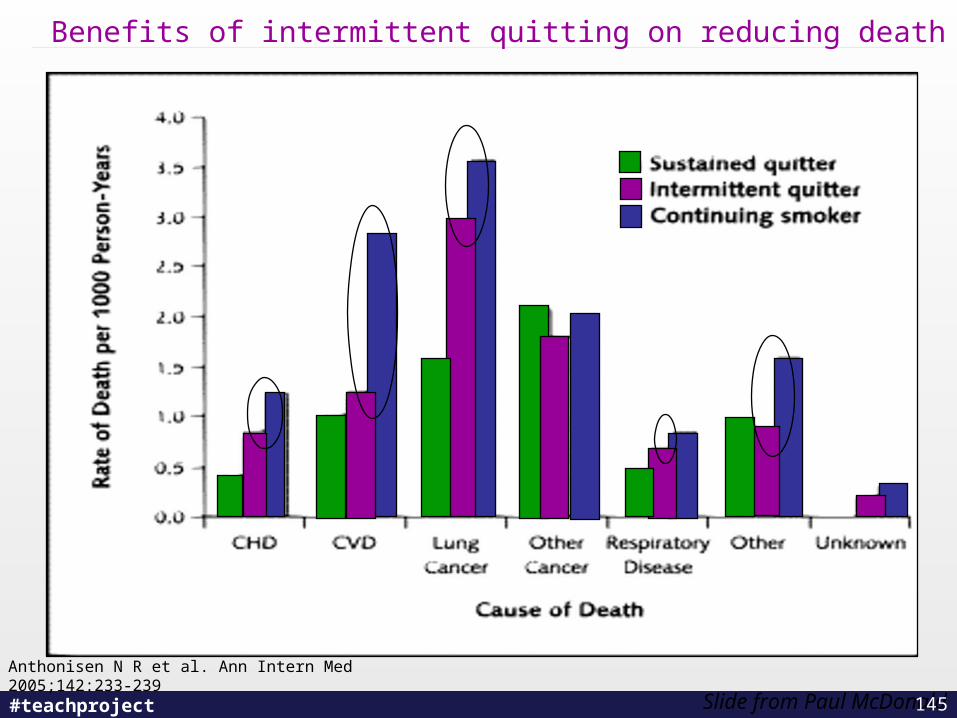
Benefits of intermittent quitting on reducing death
Slide from Paul McDonald145
Anthonisen N R et al. Ann Intern Med 2005;142:233-239
#teachproject
Effective Harm Reduction Strategies
• Product regulation – warnings on packages, making cigarettes taste bad, anti-counterfeiting
• Changing nature of products containing nicotine– Low nitrosamine cigarettes only cut out 1 carcinogen
• Taxation - increasing the amount of taxes on cigarettes decreases consumption especially with 18-24 year olds
• Limiting access / visibility – retail displays being removed. “Out of sight out of mind”
• NRT, bupropion and other approved cessation medications
• Eliminating provincial sales tax in Ontario on nicotine replacement products``
146
#teachproject
NRT and Reduction
• Cleaner, safer delivery system of nicotine• Separates addictive behaviour from harm • Prevents use of tobacco products to help with
withdrawal• Increases familiarity with cessation products• Combined with other treatment (behavioral,
emotional triggers) • New literature = start NRT two weeks before
quit date
147
Nicotine Assisted Reduction to Stop (NARS), Action on Smoking Health (2005).
#teachproject
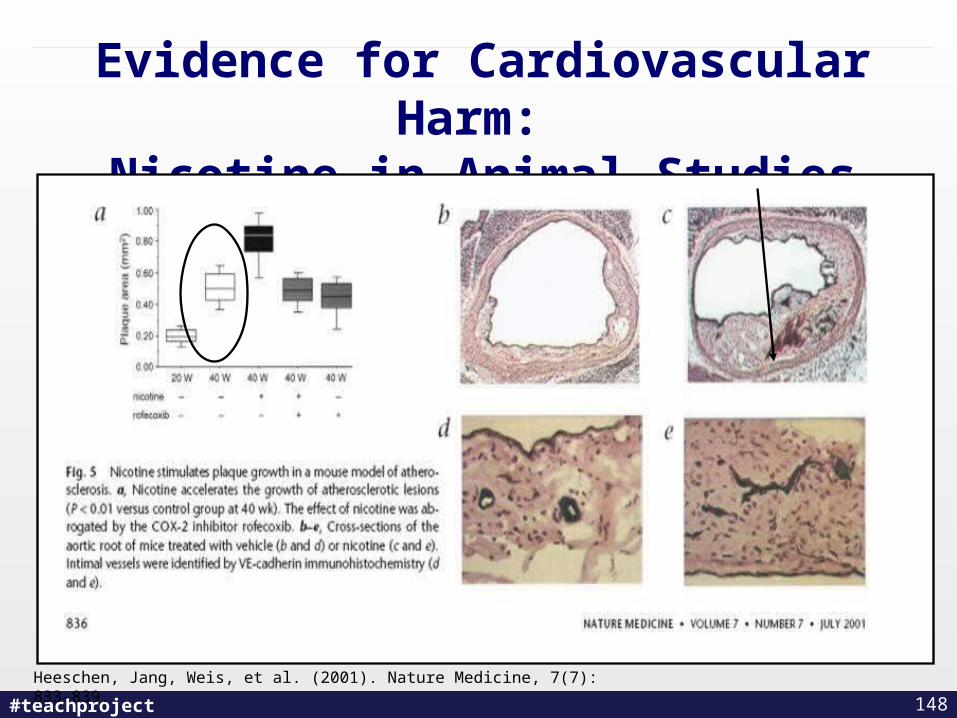
Evidence for Cardiovascular Harm: Nicotine in Animal Studies
148
Heeschen, Jang, Weis, et al. (2001). Nature Medicine, 7(7): 833-839.
#teachproject
Evidence for Cardiovascular Harm – Humans
• Blood pressure: older studies, higher resting BP, newer studies, no effect.
• Heart rate: mild increase but not significant
• Waist-hip: nil/variable
• BMI: variable
• Max workload capacity: no difference
• Insulin resistance higher risk both in long term NRT users. Variable in smokeless users.
Asplund (2003). Progress in Cardiovascular Diseases, 45: 383-394.
149
#teachproject
Conclusion
• Nicotine may have increased cardiovascular effects that are associated with increased morbidity and mortality mainly in smokers.
• However, compared to smoked tobacco, other forms have less risk and at times are similar to that of non-smokers.
• In Sweden, many males switch to smokeless as a means to quit smoking.
• NRT appears to be safe. However long-term use only examined in the Lung Health Study (1996).
150
#teachproject
Evidence of Harm in Pregnancy
• Nicotine is a neuroteratogen • However, CO and Thiocyanates also play
a role• Smoking is associated with cleft lip, low
birth weight, SIDS• Downstream psychiatric symptoms in
children• However, most pregnant women continue
to smoke while pregnant even with the best available intervention.
• Fetocentric versus woman-centred approach
151
Slotkin, Seider, et al., (2005). Neuropsychopharmacology, 30(1): 129-44.
#teachproject
NRT in pregnancy
• Try behavioural interventions first
• When cannot quit, try intermittent forms of NRT starting with lowest dose
• If using patch, remove at bedtime
• Continue behavioural support
Benowitz, Dempsey (2004). Nicotine and Tobacco Research, 6(Suppl 2): S189-S202.
152
#teachproject
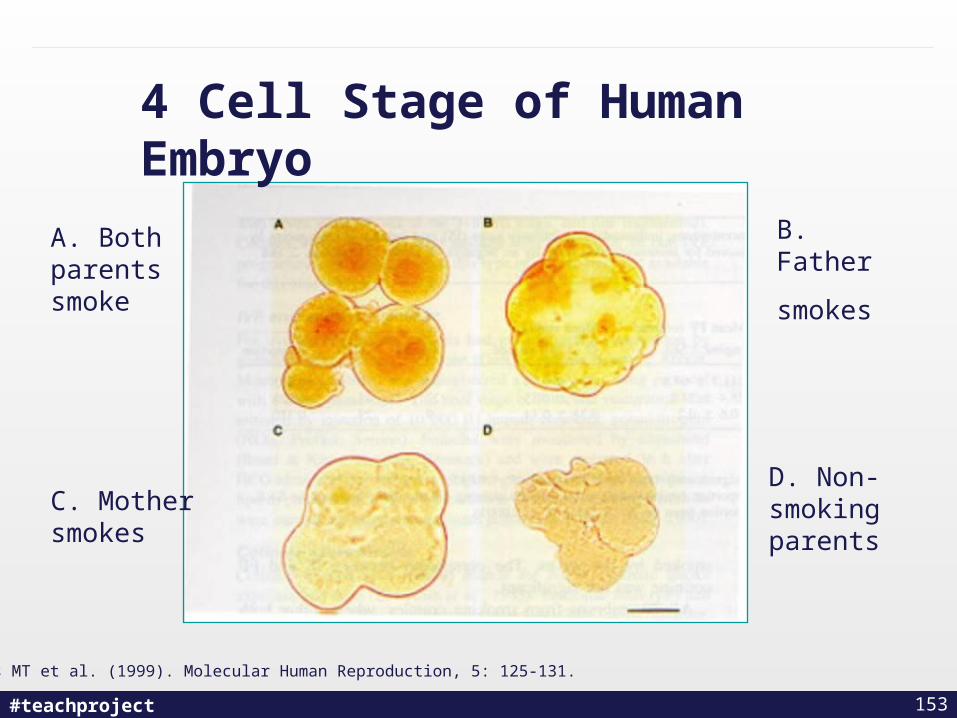
Zenzes MT et al. (1999). Molecular Human Reproduction, 5: 125-131.
A. Both parents smoke
C. Mother smokes
B. Father
smokes
D. Non-smoking parents
4 Cell Stage of Human Embryo
153
#teachproject
Cigarettes and Reproduction
• Women who smoke undergo menopause 1 to 4 years earlier than non-smokers.
• Zenzes et al have shown that smoking causes benzo(a)pyrene diol epoxide DNA (BPDE-DNA) adduct formation in human sperm
• Similar proportions of BPDE-DNA adducts in embryos where both parents smoke, compared to where only the father smoked, suggested that contribution of DNA adducts is mainly from sperm
154
Zenzes MT et al. (1999). Molecular Human Reproduction, 5: 125-131.
#teachproject
Implications
• Understanding the role of nicotine in the harm caused by smoking is important if smokers are to be encouraged to use less harmful nicotine delivery devices and will help to identify where a cautious approach might be necessary as well as gaps for further research.
155
#teachproject
When does a person’s risk of developing lung cancer become high? ( > 10 times the risk of a non-smoker)
a. Up to 10 cigarettes per day
b. Between 10-19 cigarettes per day
c. 20 cigarettes per day
d. Between 21-31 cigarettes per day
e. More than 31 cigarettes per day
156
#teachproject
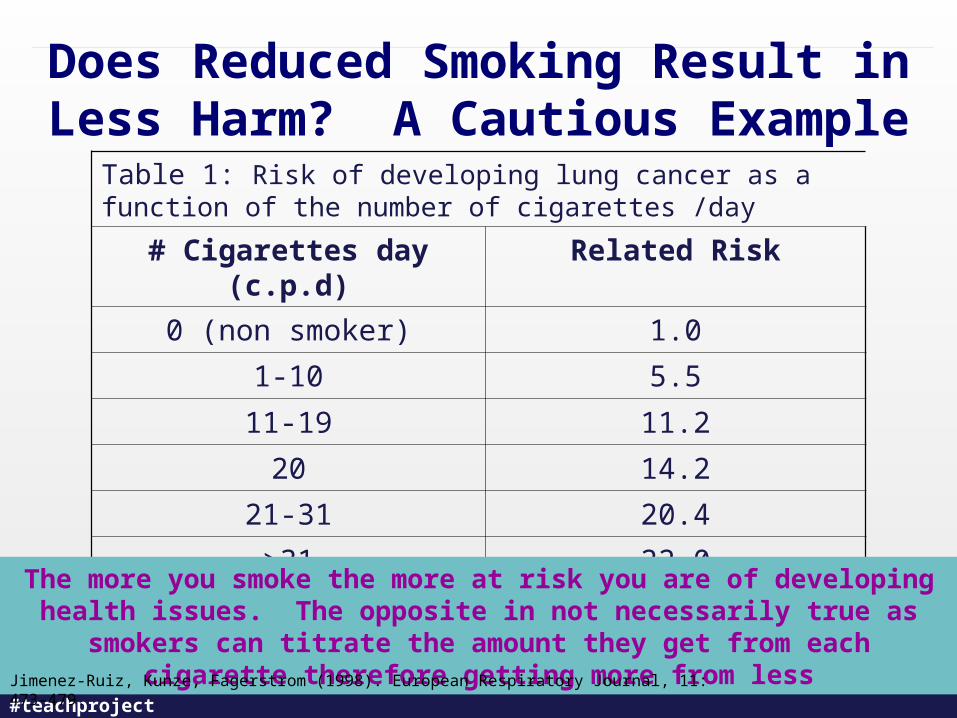
Does Reduced Smoking Result in Less Harm? A Cautious Example
Table 1: Risk of developing lung cancer as a function of the number of cigarettes /day
# Cigarettes day (c.p.d) Related Risk
0 (non smoker) 1.0
1-10 5.5
11-19 11.2
20 14.2
21-31 20.4
>31 22.0
The more you smoke the more at risk you are of developing health issues. The opposite in not necessarily true as smokers can titrate the amount
they get from each cigarette therefore getting more from lessJimenez-Ruiz, Kunze, Fagerstrom (1998). European Respiratory Journal, 11: 473-479.
#teachproject
What about……….
Tobacco or tobacco blends that are chewed or sucked on. A person who uses eight to 10 dips or
chews a day receives the same amount of nicotine as a heavy smoker who smokes 30 to 40
cigarettes a day
One can contains 4 x the nicotine in a pack of cigarettes
World Health Organization International Agency for Research on Cancer (2007). IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, Volume 89.
158
#teachproject
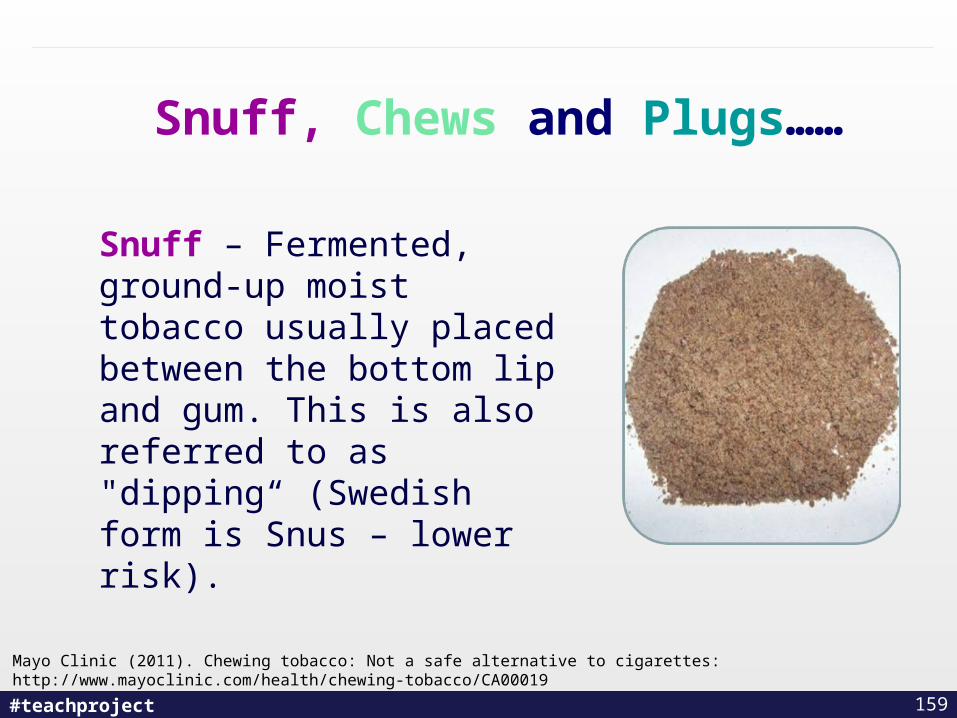
Snuff, Chews and Plugs……
Snuff – Fermented, ground-up moist tobacco usually placed between the bottom lip and gum. This is also referred to as "dipping“ (Swedish form is Snus – lower risk).
159
Mayo Clinic (2011). Chewing tobacco: Not a safe alternative to cigarettes: http://www.mayoclinic.com/health/chewing-tobacco/CA00019
#teachproject
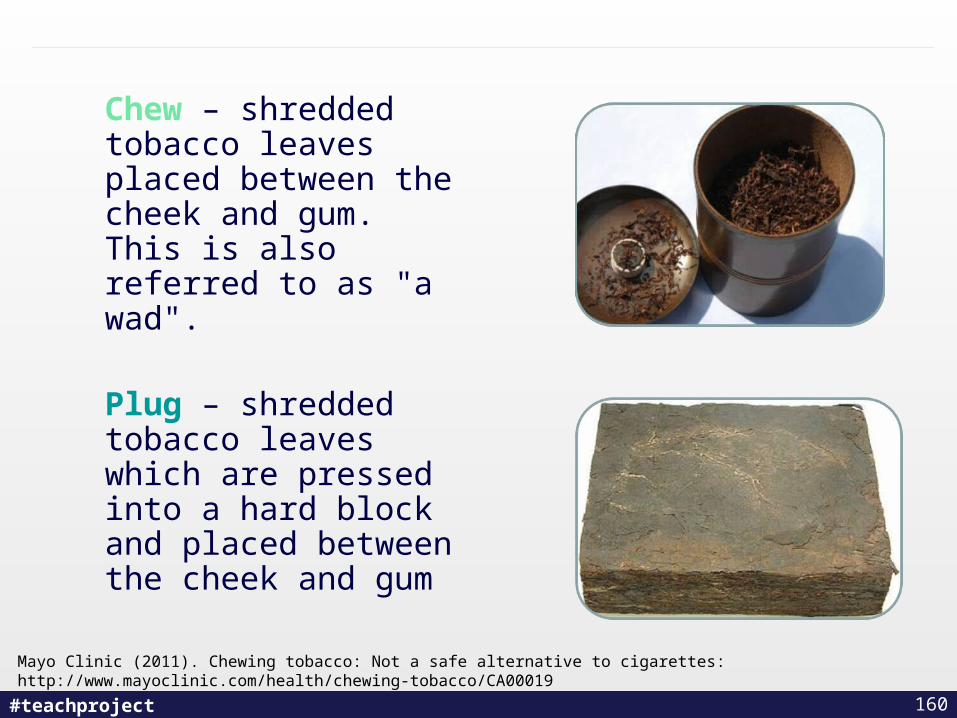
Chew – shredded tobacco leaves placed between the cheek and gum. This is also referred to as "a wad".
Plug – shredded tobacco leaves which are pressed into a hard block and placed between the cheek and gum
160
Mayo Clinic (2011). Chewing tobacco: Not a safe alternative to cigarettes: http://www.mayoclinic.com/health/chewing-tobacco/CA00019
#teachproject
Ingredients in Smokeless Tobacco
• Nicotine: poisonous and highly addictive drug
• Carcinogens: many cancer-producing chemicals have been identified in smokeless (spit) tobacco.
• Sweeteners: tobacco has an unpleasant taste, some brands of smokeless tobacco are heavily sweetened with sugars, which promote tooth decay.
• Abrasives: scratch the soft tissues in the mouth, allowing the nicotine and other chemicals to get directly into the blood system.
• Salt: Flavouring salts found to contribute to abnormal blood pressure and kidney disease.
• Other Chemicals: Hundreds of other chemicals can be found in tobacco which contribute to many health problems.
161
National Institute of Dental and Craniofacial Research (2010). Smokeless Tobacco: A Guide for Quitting http://www.nidcr.nih.gov/OralHealth/Topics/SpitTobacco/SpitTobaccoAGuideforQuitting.htm
#teachproject
Health Risks of Smokeless Tobacco (1)
• Mouth Cancer – cancer of the cheeks, gums, lips and tongue. Smokeless (spit) tobacco users have a 50% higher chance of getting oral cancer than non-users.
• Throat Cancer – cancer of the voice box and cancer of the esophagus.
• Heart disease – heart attacks, strokes and high blood pressure.
http://www.health.gov.sk.ca/rr_smokeless_tobacco.html
162
#teachproject
Health Risks of Smokeless Tobacco (2)
• Dental diseases – stained teeth, tooth decay, receding gums, gum disease, bad breath and black hairy tongue.
• Stomach problems – ulcers, stomach upset, increased bowel activity and stomach cancer.
• Loss of taste and smell – causes loss of appetite which results in poor nutrition and poor health.
• Physical changes – fatigue, muscle weakness, dizziness and decreased physical performance, dermatologic changes
http://www.health.gov.sk.ca/rr_smokeless_tobacco.html
163
#teachproject
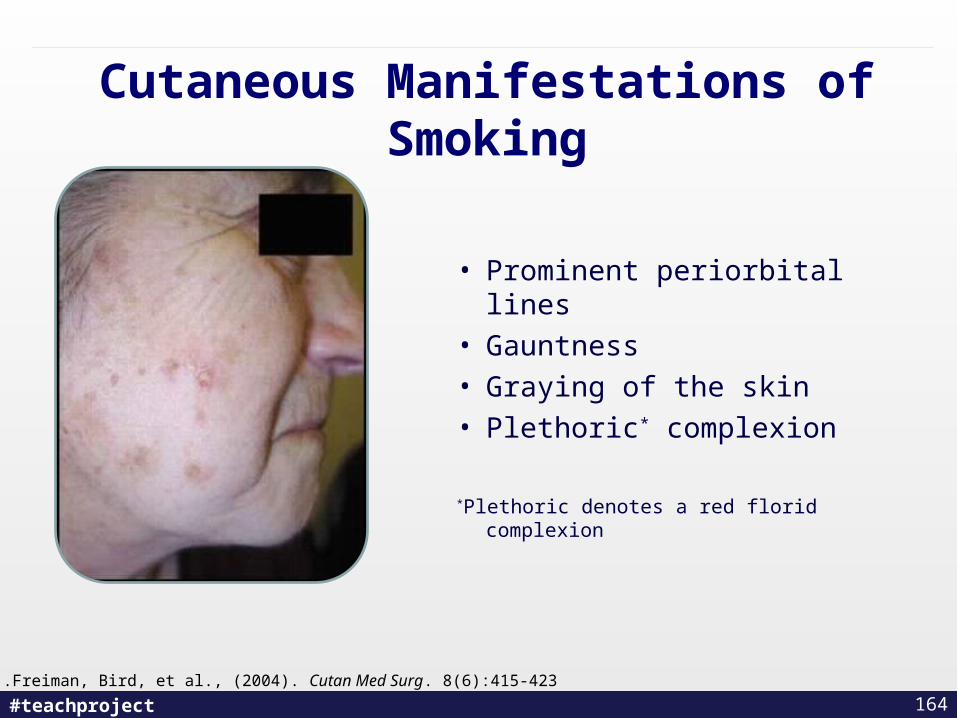
Cutaneous Manifestations of Smoking
• Prominent periorbital lines
• Gauntness
• Graying of the skin
• Plethoric* complexion
*Plethoric denotes a red florid complexion
.Freiman, Bird, et al., (2004). Cutan Med Surg. 8(6):415-423
164
#teachproject
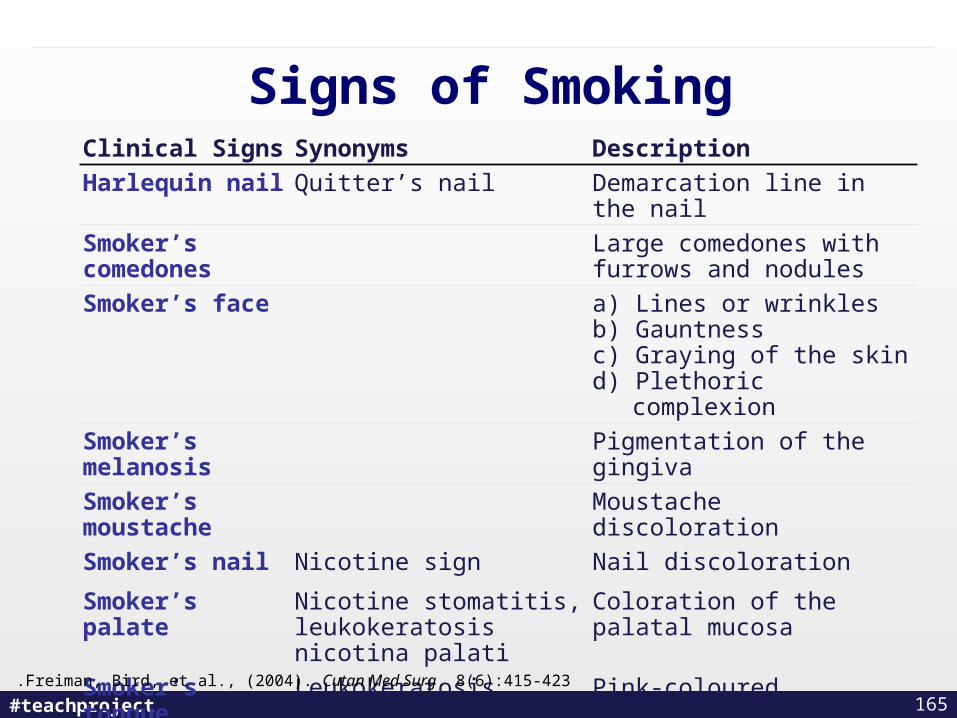
Signs of SmokingClinical Signs Synonyms Description
Harlequin nail Quitter’s nail Demarcation line in the nail
Smoker’s comedones Large comedones with furrows and nodules
Smoker’s face a) Lines or wrinklesb) Gauntnessc) Graying of the skind) Plethoric complexion
Smoker’s melanosis Pigmentation of the gingiva
Smoker’s moustache Moustache discoloration
Smoker’s nail Nicotine sign Nail discoloration
Smoker’s palate Nicotine stomatitis, leukokeratosis nicotina palati
Coloration of the palatal mucosa
Smoker’s tongue Leukokeratosis nicotina glossi Pink-coloured depressions
Snuff dipper’s lesion Smokeless tobacco keratosis, tobacco pouch keratosis
White lesion in the oral cavity where smokeless tobacco is held
165.Freiman, Bird, et al., (2004). Cutan Med Surg. 8(6):415-423
#teachproject
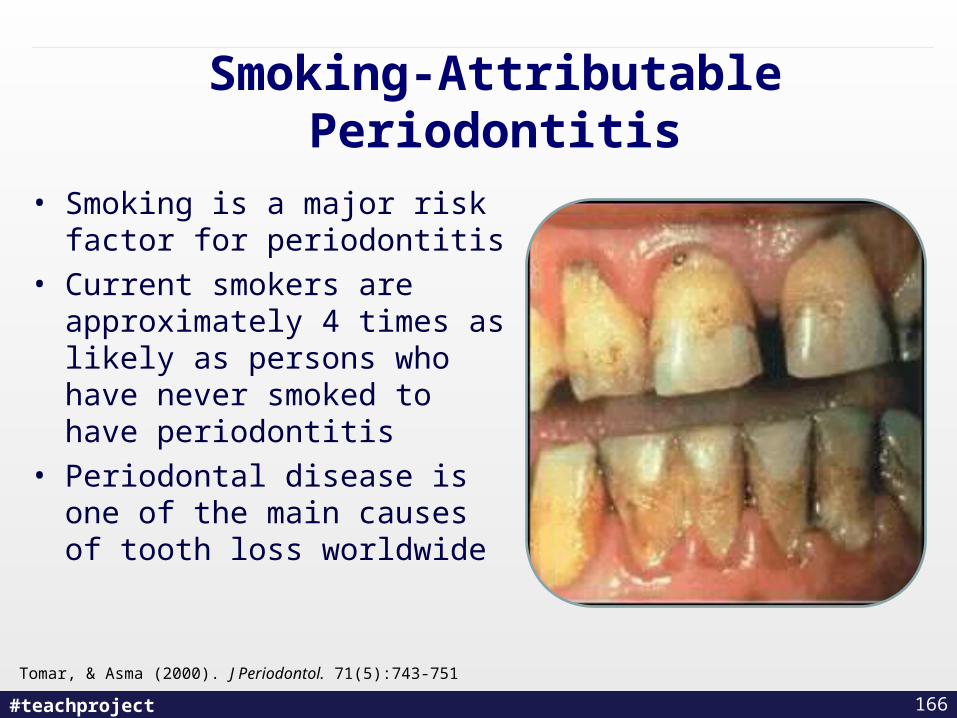
Smoking-Attributable Periodontitis
• Smoking is a major risk factor for periodontitis
• Current smokers are approximately 4 times as likely as persons who have never smoked to have periodontitis
• Periodontal disease is one of the main causes of tooth loss worldwide
Tomar, & Asma (2000). J Periodontol. 71(5):743-751
166

#teachproject
Gum Recession
167
#teachproject
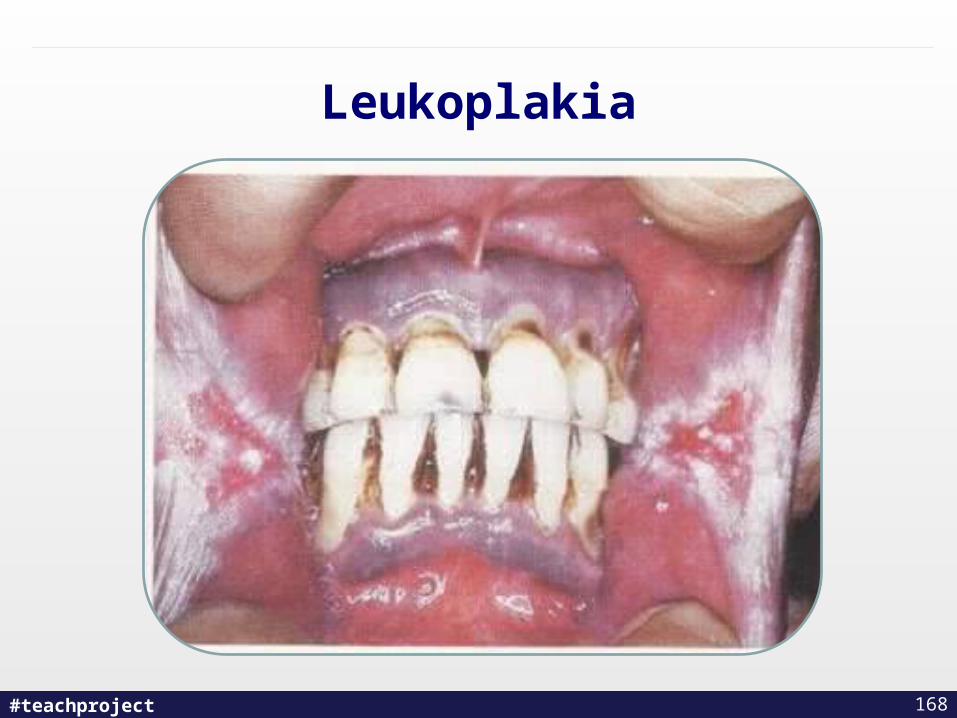
Leukoplakia
168

#teachproject
Nicotine StomatitisBrown Hairy Tongue
Davis (2005). J Contemp Dent Pract.,6:158-166
169
#teachproject
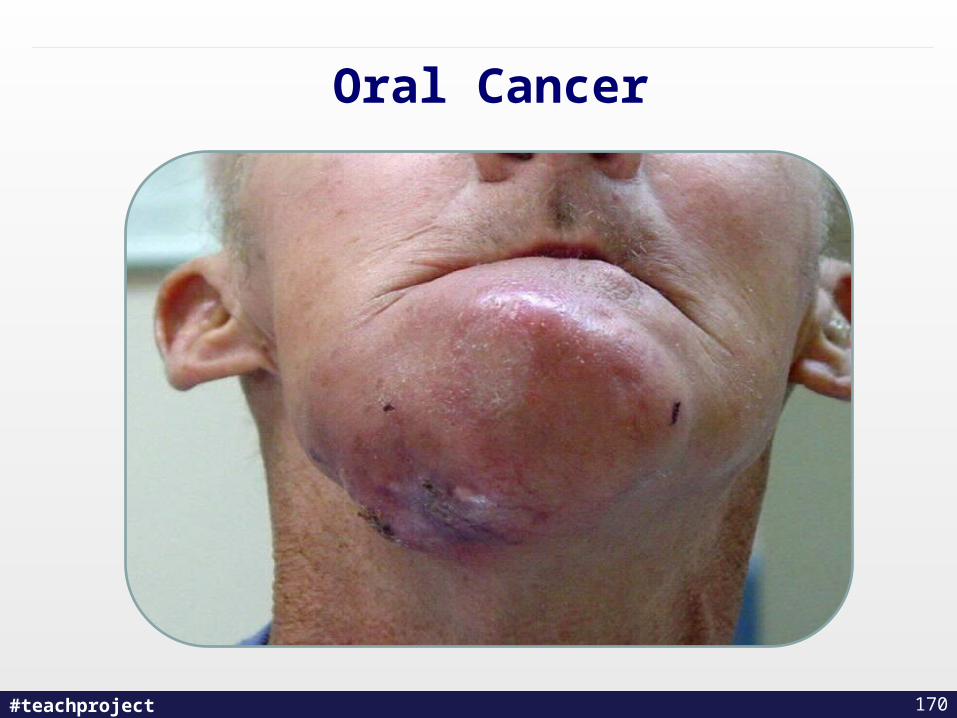
Oral Cancer
170
#teachproject
Smokeless Tobacco Prevention Websites
• http://mylastdip.com/ - Web-based intervention that is designed to help young chewing tobacco users quit.
• http://www.chewfree.com/ - Website created to help people quit their use of chewing tobacco or snuff.
171
#teachproject
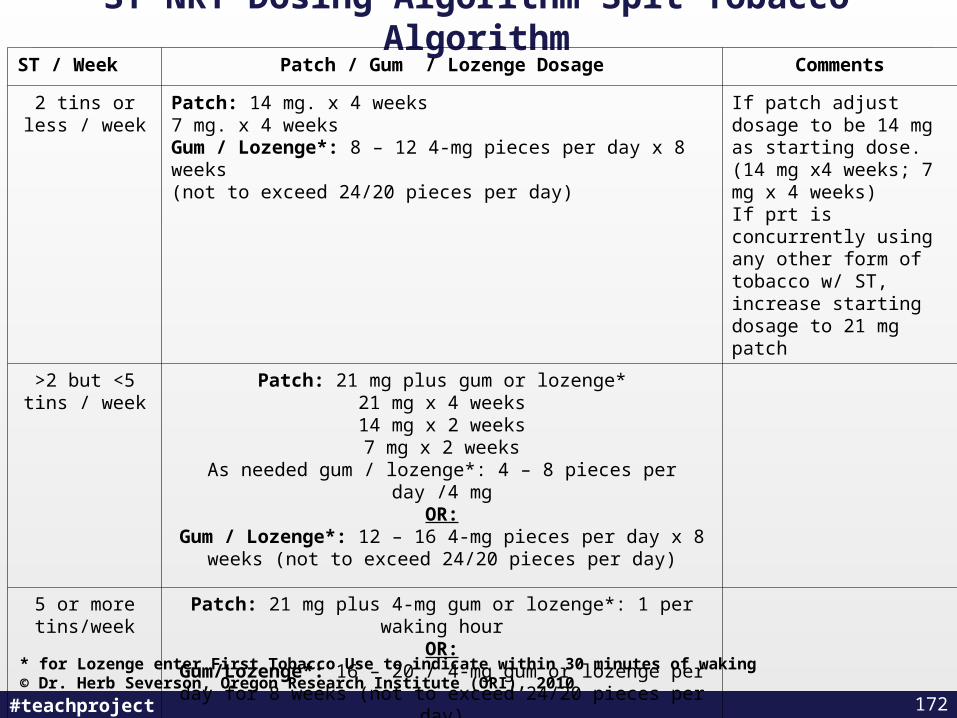
ST NRT Dosing Algorithm Spit Tobacco AlgorithmST / Week Patch / Gum / Lozenge Dosage Comments
2 tins or less / week
Patch: 14 mg. x 4 weeks7 mg. x 4 weeksGum / Lozenge*: 8 – 12 4-mg pieces per day x 8 weeks(not to exceed 24/20 pieces per day)
If patch adjust dosage to be 14 mg as starting dose. (14 mg x4 weeks; 7 mg x 4 weeks)If prt is concurrently using any other form of tobacco w/ ST, increase starting dosage to 21 mg patch
>2 but <5 tins / week
Patch: 21 mg plus gum or lozenge*21 mg x 4 weeks14 mg x 2 weeks7 mg x 2 weeks
As needed gum / lozenge*: 4 – 8 pieces per day /4 mgOR:
Gum / Lozenge*: 12 – 16 4-mg pieces per day x 8 weeks (not to exceed 24/20 pieces per day)
5 or more tins/week
Patch: 21 mg plus 4-mg gum or lozenge*: 1 per waking hourOR:
Gum/Lozenge*: 16 – 20 / 4-mg gum or lozenge per day for 8 weeks (not to exceed 24/20 pieces per day)
* for Lozenge enter First Tobacco Use to indicate within 30 minutes of waking© Dr. Herb Severson, Oregon Research Institute (ORI), 2010
172
#teachproject
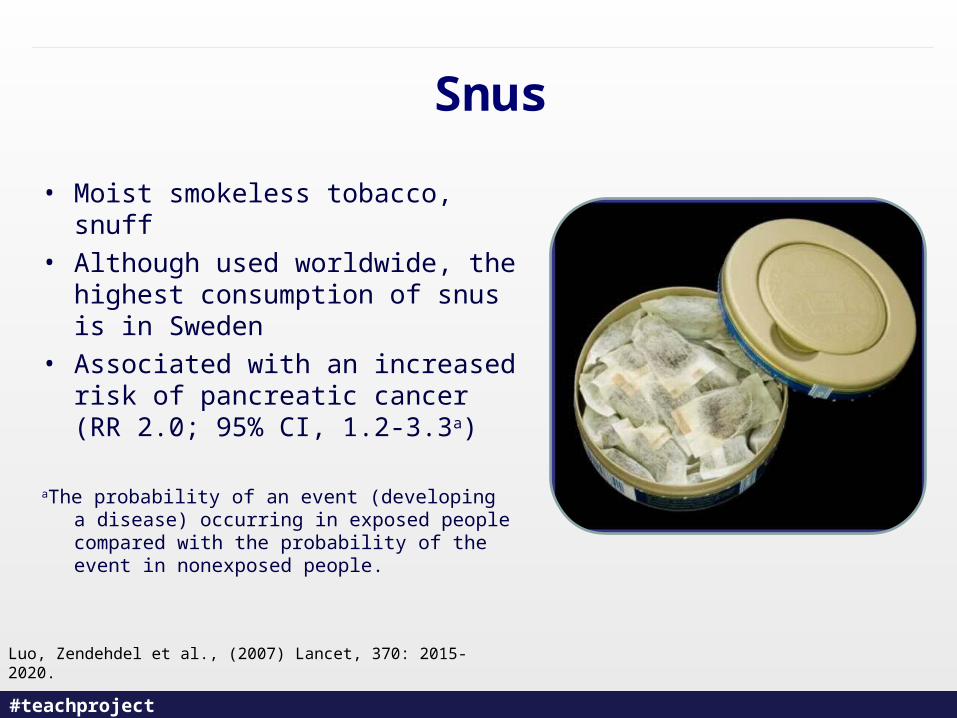
Snus
• Moist smokeless tobacco, snuff
• Although used worldwide, the highest consumption of snus is in Sweden
• Associated with an increased risk of pancreatic cancer (RR 2.0; 95% CI, 1.2-3.3a)
aThe probability of an event (developing a disease) occurring in exposed people compared with the probability of the event in nonexposed people.
Luo, Zendehdel et al., (2007) Lancet, 370: 2015-2020.
#teachproject
Snus
• Different from other chew
tobacco – it is sterilized, decreasing the number of nitrosamines (cancer-causing agents)
• Reduced risk of lung cancer• No emphysema• 2x risk of pancreatic cancer
(down from 3x risk with smoking)
174
#teachproject
Snus Study
• International researchers followed 279,897 male Swedish construction workers from 1978 to 1992. About 26 percent were snus users, 37 percent were smokers and the rest never used tobacco.
• For smokers, the incidence rate of pancreatic cancer was 13 cases per 100,000 versus 8.8 cases per 100,000 for snus users.
• Among those who did not use tobacco, the rate was 3.9 cases per 100,000.
175
Luo, Zendehdel et al., (2007) Lancet, 370: 2015-2020.
#teachproject
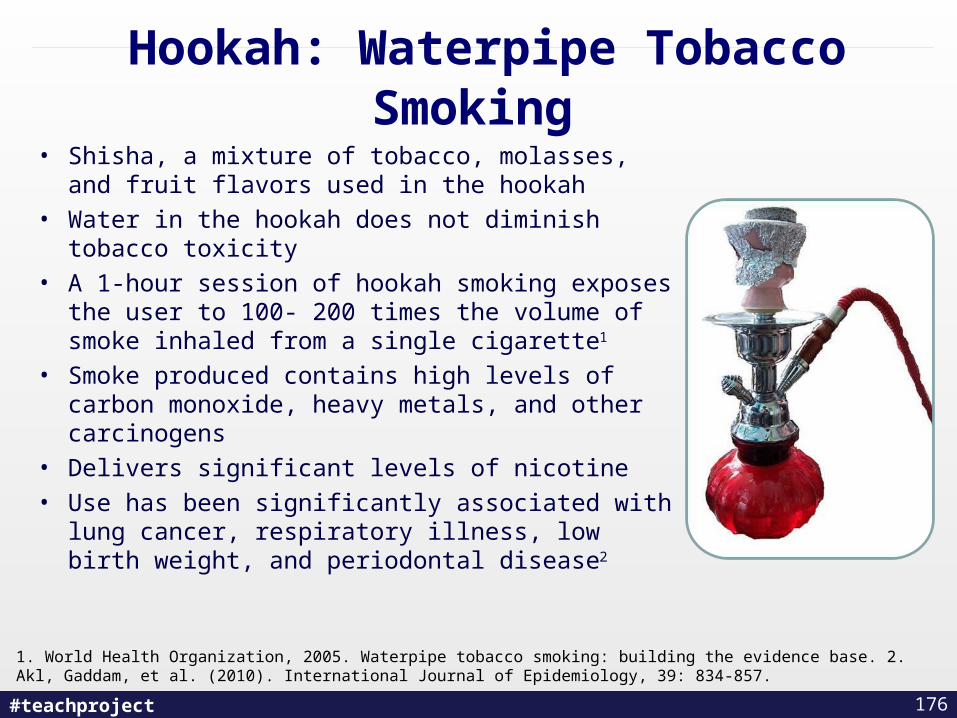
Hookah: Waterpipe Tobacco Smoking • Shisha, a mixture of tobacco, molasses, and fruit
flavors used in the hookah
• Water in the hookah does not diminish tobacco toxicity
• A 1-hour session of hookah smoking exposes the user to 100- 200 times the volume of smoke inhaled from a single cigarette1
• Smoke produced contains high levels of carbon monoxide, heavy metals, and other carcinogens
• Delivers significant levels of nicotine
• Use has been significantly associated with lung cancer, respiratory illness, low birth weight, and periodontal disease2
1. World Health Organization, 2005. Waterpipe tobacco smoking: building the evidence base. 2. Akl, Gaddam, et al. (2010). International Journal of Epidemiology, 39: 834-857.
176
#teachproject 177
#teachproject 178
#teachproject
• As dependence-forming as cigarettes
• Users develop cravings and nicotine withdrawal when abstaining
• Does not produce second-hand-smoke BUT people who dip or chew spread their germs when they spit. This increases the risk of passing an infection to others.
Smokeless Tobacco as Harm Reduction? (1)
179
Benowitz (2011). Clinical Pharmacology & Therapeutics 90, 491-493 American Cancer Society
(2011). Quitting Smokeless Tobacco.
#teachproject
Smokeless Tobacco as Harm Reduction? (2)
• Most smokeless tobacco users are regular users before age 18
• Almost all users are male
• High co-use of cigarettes (est. 10-20%)
• 38% of users develop oral lesions within 3 years
180
Benowitz (2011). Clinical Pharmacology & Therapeutics 90, 491-493 American Cancer Society
(2011). Quitting Smokeless Tobacco.
#teachproject
Smokeless Tobacco Cessation
• Nicotine lozenge appears to be the most preferred cessation aid
• Varenicline and behavioural interventions can assist cessation
• Presence of lesions is an opportunity to motivate behaviour change
• 2 week rule: If lesions do not heal within 2 weeks, recommend a biopsy
181
Ebbert, Montori et al. (2011). Interventions for smokeless tobacco use cessation. Cochrane Database of Systematic Reviews (2).

#teachproject
New Smokeless Cessation Aid- Mint Snuff
•Non tobacco product, edible and made with real mint
•Safe to swallow/eat
•Available in 4 flavours
•Mint Snuff Pouches are miniature teabags filled with Mint and Mint Oil Crystals.
•1-800-EAT-MINT
www.mintsnuff.com
182
#teachproject
Bottom Line on Harm Reduction
Using fewer tobacco products may have little to no effect on reducing morbidity and mortality
BUT
Reducing consumption may increase likelihood of future cessation
183
#teachproject
What is your perspective on harm reduction and tobacco use?
a. There is no such thing – all tobacco use is harmful
b. I can see it that might be necessary with some populations
c. I believe in using a harm reduction approach
d. I’m not sure - I need more information
184
#teachproject 185
Evaluation and Wrap
Up
#teachproject
Learning Objective
Access additional clinical tools and resources to use in clinical practice and continuing professional development
186
#teachproject
TEACH Community of Practice & Listserv
As a graduate of this course, you are eligible to join the TEACH Community of Practice Listserv! Our TEACH COP Listserv is configured so that you need to self-register, which quick and easy to do.
To “subscribe” to the Listserv, please send an email to: [email protected]
and write: “subscribe teach” in the subject line of your e-mail.
You will then receive a message confirming your subscription to the List, as well as instructions on how to post or unsubscribe.
187
#teachproject
1. Please complete the Evaluation Form before you leave.
2. Log on to the TEACH Website to make sure you’ve completed Learning Assessments # 1 & #2 (you must complete both in order to receive the CAMH Letter of Completion and U of T Certificate).
3. Online follow-up survey in three and six months – TEACH will send you a reminder !
Course Evaluation: 3 Things to Remember
188
#teachproject
Are you interested in becoming a
Tobacco Cessation Practice Leader?
An Opportunity to…. Possible Roles…..• Develop your skills - Clinical Consultation• Network - Conference Speaker• Attend TEACH courses - In –Service Trainer• Achieve credit units - Media Interviews
- Resource Link
Questions? Email: [email protected]
189
#teachproject
How would you rate this course?
a. Excellent
b. Very good
c. Good
d. Fair
e. Poor
190

#teachproject
Quick Break
See you in 10 minutes!
191
#teachproject 192
TEACH Exam
#teachproject
Please remember to leave your i-clicker on your table, Thanks.
193

#teachproject
#teachproject
194