Embed Size (px)
Citation preview

An Innovative Curriculum Teaching the Integration of Communication and
Clinical Reasoning Skills to Medical Students
Donna M. Windish, M.D.
MPH Capstone Project
April 28, 2004
Co-curriculum Developers: Eboni G. Price, M.D., Sarah L. Clever, M.D., M.S.
MPH Capstone Advisor: Eric B. Bass, M.D., M.P.H.
ABSTRACT
Context: Medical students rarely are taught how to integrate communication and clinical reasoning
skills during patient-physician interactions.
Objectives: For medical students to be able to demonstrate: (1) the connection between
communication and clinical reasoning by integrating biomedical and psychosocial aspects of patient
care, (2) strategies to engage in patient-centered communication, and (3) strategies for clinical
reasoning during patient encounters.
Design: Randomized trial of a curricular intervention in communication and clinical reasoning
implemented in 2003.
Setting: Johns Hopkins University School of Medicine.
Participants: Sixty of 121 second-year medical students participated in the curriculum with the
remaining 61 students serving as controls.
Intervention: A 6-week, 18-hour course taught the integration of specific communication and clinical
reasoning techniques in a small group setting using role-play, reflection and feedback in a structured
iterative reflective process.
Main Outcome Measures: Students interviewed standardized patients who assessed their
communication skills in: establishing rapport, data gathering and patient education and counseling.
For clinical reasoning, students generated problem lists and differential diagnoses for each case. Mean
scores were calculated for each communication skill area, problems listed and differential diagnoses
generated. Integration of communication and clinical reasoning was measured by students’ listing
psychosocial history items on their problem lists.
Results: Students in the curriculum were rated more favorably in their ability to establish rapport by
the standardized patients (p=0.08). Participants listed on average one more patient problem on their
Windish 2004 1
problem lists compared to controls (mean 8.4 versus 7.5; p=0.05). Sixty-four percent of students in the
curriculum versus 44% of controls listed one or more psychosocial history items in their problem lists
(p=0.03). Groups did not differ significantly in other communication skill ratings or in the mean
number of differential diagnoses generated. Ninety-five percent of curricular participants found
importance in integrating communication and clinical reasoning skills.
Conclusions: Teaching medical students communication and clinical reasoning skills concomitantly
improved their ability to integrate the biomedical and psychosocial aspects of patient care. Similar
educational initiatives in all stages of training could lead to improved patient-physician interactions
and medical care.
Windish 2004 2
To provide good medical care, physicians must understand each patient as a whole including
his or her biological, psychological, social and cultural background. This requires adequate knowledge
of epidemiology and pathophysiology, effective communication, and good clinical judgment to
generate and modify diagnostic hypotheses as information is gathered during a clinical encounter (i.e.,
clinical reasoning skills). Communication and clinical reasoning skills must be mastered during
medical training, as required by the Association of American Medical Colleges,1 the Liaison
Committee on Medical Education,2 and the Accreditation Council for Graduate Medical Education3.
Successful use of these skills has been linked to important outcomes, including improved diagnostic
and clinical proficiency,4,5 increased patient and physician satisfaction,6-8 reduced emotional distress,2
decreased frequency of medical errors,9 and improved efficiency in medical care10. Since clinicians
use communication and clinical reasoning skills together, instruction in these areas should occur in an
integrated fashion to help the learner understand how each element informs the other. Although
communication skills training may improve a student’s diagnostic efficiency,4 we found no published
examples of curricula that help medical students learn to integrate these skills.
To overcome potential educational deficiencies, we developed a curriculum entitled AIME (An
Integrated Medical Encounter) to teach the integration of communication and clinical reasoning skills
to second-year medical students. The specific objectives of the curriculum were for students to be able
to demonstrate: (1) the connection between communication and clinical reasoning skills by integrating
biomedical and psychosocial aspects of patient care, (2) strategies to engage in patient-centered
communication, and (3) strategies for clinical reasoning during patient encounters. This paper
describes the development of the curriculum and the results of a randomized trial to determine the
effectiveness of teaching these skills together.
Windish 2004 3
METHODS
Background
We used a six-step approach to curriculum development as described by Kern and colleagues.11
Briefly, from our literature review, we found five models that serve as the basis for teaching patient-
physician communication.12-16 Of these, the Three Function Model of the Medical Interview12 (that
emphasizes establishing rapport, gathering data, and educating and counseling patients) provides the
best framework to discuss elements of communication and clinical reasoning. To teach clinical
reasoning, we found teaching methods that focus on a case-based approach to learning with an
emphasis on generating differential diagnoses.17-19
Institutional Needs Assessment
To determine how communication and clinical reasoning skills were taught at the Johns
Hopkins University School of Medicine, we conducted a needs assessment in 2002-3. We
administered questionnaires and conducted in-person interviews with the instructors of the first year
Introduction to Clinical Medicine course (emphasizing components of the medical interview through
observation of a practicing physician), the second year Clinical Skills course (teaching history-taking
and physical examination), and the Physician and Society course (emphasizing medical ethics in the
patient-physician relationship). We also surveyed and interviewed clerkship directors in six required
clerkships (Ambulatory Medicine, Inpatient Medicine, Neurology, Pediatrics, Psychiatry, and
Surgery). We asked faculty to rate student preparedness for the clerkship years in seven
communication skills and four areas of clinical reasoning using ratings of “less prepared”, “at the level
they should be”, or “more prepared”. During the in-person interviews, we reviewed individual course
syllabi and discussed the types of formal teaching provided in these areas.
Windish 2004 4
We also surveyed 96 third- and fourth-year students. We asked them to indicate which medical
school courses provided formal training in communication and clinical reasoning and to self-rate their
proficiency in each skill using responses of “no exposure”, “familiar with concept”, “can perform skill
somewhat”, “can perform skill well”, or “can teach skill to other students”.
In the preclinical years, we found that the Introduction to Clinical Medicine course introduces
the Bayer Institute of Health Care Communication model: engagement, enlistment, empathy and
education.20 Since the course is designed to be an observational experience of a community
physician’s interaction with patients, opportunities to perform interviews and practice these skills vary
based on preceptor assignment. The second-year Clinical Skills course assigns four students to a
facilitator and allows student pairs to practice interviewing hospitalized patients one afternoon each
week. This course emphasizes obtaining the biomedical components of the medical history (i.e.,
history of present illness, past medical history, social history, and family history) with no specific
training or feedback in communication skills. In the Physician and Society course, no formal
instruction is provided in communication skills; however, student groups have opportunities to practice
interviewing standardized patients in sensitive areas including domestic violence and delivering bad
news.
For clinical reasoning, students may be introduced to differential diagnoses in their Clinical
Skills group through informal discussions of the medical history gathered during patient interviews;
however, they do not receive formal training in clinical reasoning in any preclinical course. Thus, in
the preclinical years, specific instruction and reinforcement of communication and clinical reasoning
skills was limited.
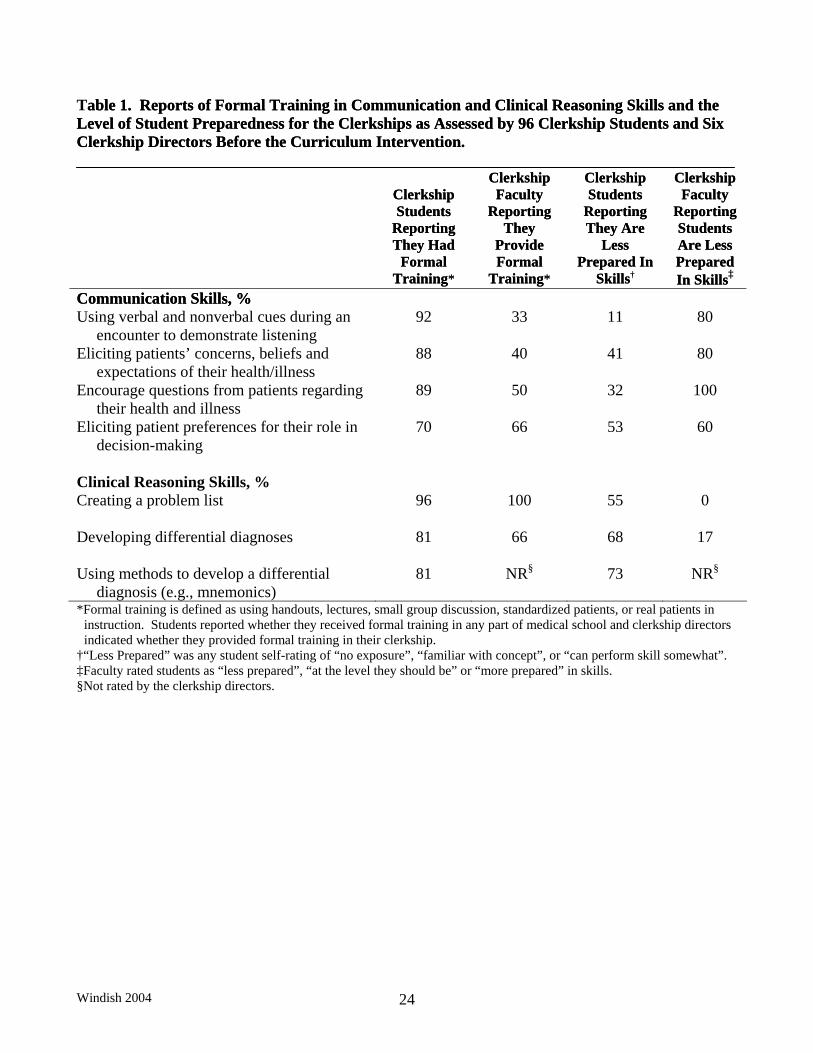
Many of the clerkship directors indicated that they provide some formal training in
communication and clinical reasoning during their clerkship (Table 1). Nevertheless, most used non-
Windish 2004 5
experiential learning techniques (e.g., handouts and small group discussion). The majority of faculty
felt that students were less prepared than necessary in most communication and clinical reasoning
skills, which is consistent with the results of a national survey of clerkship directors.21 Clerkship
students also perceived their preparation in these areas as less than optimal, although most students
acknowledged receiving some formal training (Table 1). Given the results of our needs assessment, it
was clear that additional communication and clinical reasoning skills instruction was needed.
Curriculum
Overview of Teaching and Learning Strategies
Our intervention targeted second-year medical students and was taught concurrently with the
courses on Pathophysiology and Clinical Skills. We used self-reflection, small group discussion,
videotaped encounters, role-play, standardized patients, and feedback to teach different aspects of the
doctor-patient encounter. The role-play cases were linked to medical information being taught
concurrently in the Pathophysiology course. Most cases contained a communication barrier (e.g.,
patient reluctance to discuss illicit drug use) to allow students to work through specific communication
challenges.
To help students learn communication skills, we developed a Communication Skills
Observation Guide that was modeled after the Calgary Cambridge Observation Guide (Figure 1).22
The guide contains questions corresponding to the Three Function Model of interviewing.12 We asked
students to use the guide during role-plays to observe for and comment on the use of open and close-
ended inquiry, detection of verbal and nonverbal cues, elicitation of patients’ concerns about their
health and elicitation of a patient’s psychosocial history.
Our clinical reasoning instruction focused on developing a patient-specific problem list and
differential diagnosis. We emphasized understanding the patient as a whole: including all elements of
Windish 2004 6
the patient’s medical history; understanding a patient’s preferences for medical care; and
understanding how a patient’s psychosocial history and medical concerns can influence the plan of
care. Using this information, students applied knowledge of epidemiology and pathophysiology to
generate clinical hypotheses. To help students through the diagnostic thinking process, we presented a
structured approach to developing a differential diagnosis. This included thinking broadly about
disease processes using the mnemonic VINDICATE (vascular, infectious, neoplastic, drug related,
inflammatory, collagen vascular, traumatic, endocrine/metabolic) and by reviewing potential diagnoses
in each organ system to avoid premature closure in hypothesis generation.
Curriculum Structure
The curriculum was taught over the course of six weeks in small groups of six students with
one or two faculty facilitators. It consisted of weekly three-hour sessions designed to introduce
techniques in communication and clinical reasoning in a step-wise fashion. The learning objectives
and educational methods for each session are listed in Table 2. In brief, the first session introduced
communication skills based on the Three Function Model of medical interviewing. The second session
introduced clinical reasoning through the creation of problem lists and formulation of differential
diagnoses. The third session addressed components of a psychosocial history, cultural competence,
and patient education and counseling. Session four integrated communication skills and clinical
reasoning through a small group exercise with a standardized patient. Session five introduced the role
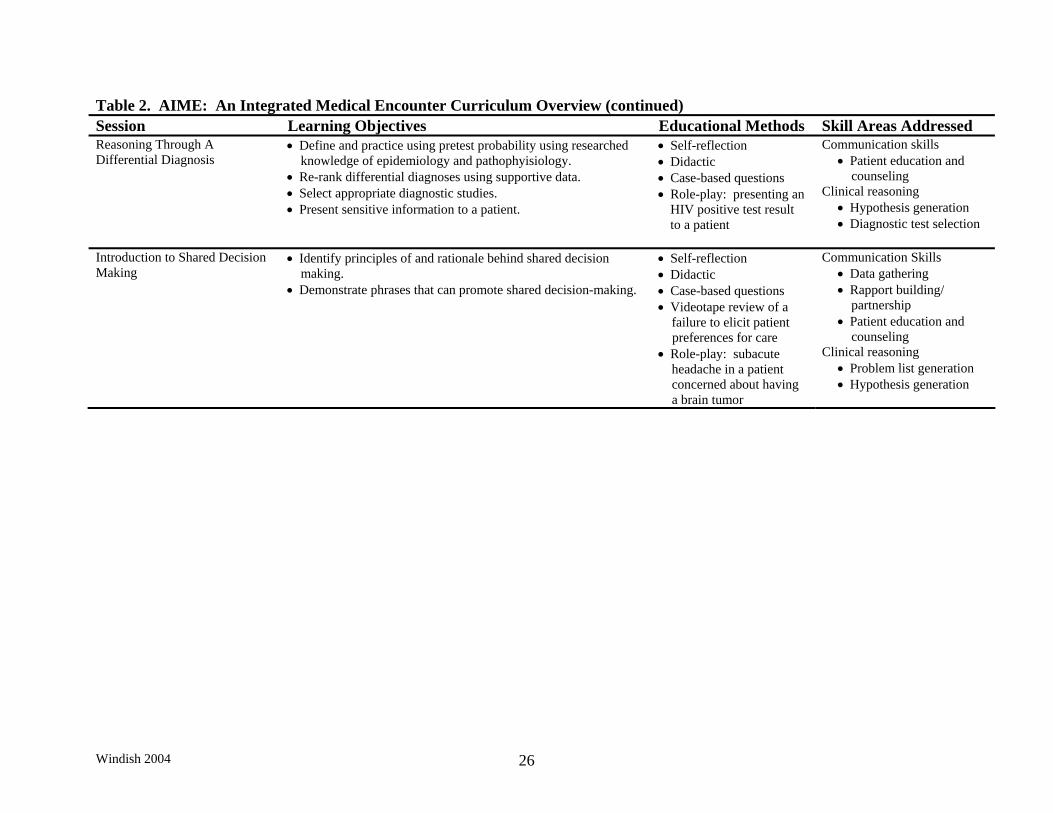
of epidemiology, pathophysiology and pre-test probability in diagnostic decision-making. Finally,
session six presented the principles of and the rationale behind shared decision making.
Each session began with a reflection on the communication and clinical reasoning skills
students used during their interviews with hospitalized patients over the previous week. The facilitator
Windish 2004 7
then offered a brief didactic on the topic of the day. After discussion of the skill area, a brief video clip
presented highlights of certain communication and clinical reasoning components of a medical
encounter. The remainder of the session (between 60-90 minutes) was devoted to a patient-physician
role-play.
The role-play was a structured experience using time-outs to highlight the cognitive processes
at work during a medical interview. One student played the patient and another student played the
clinician. The remaining students were assigned to observe different communication skills using the
Communication Skills Observation Guide. Time-outs occurred during the interview to allow reflection
on communication skills and to brainstorm clinical hypotheses. The time-outs could be called by
anyone in the group and focused on the communication or clinical reasoning challenge that the
interviewing student was facing.
During a time-out, the discussion used a six-step iterative reflective process with feedback by
self-reflection, peers, faculty and patients to examine communication skills (Figure 2). The discussion
also highlighted how the communication challenges affected the quality of the medical information
obtained. The information gathered in that segment of the interview was listed in a problem list and
differential diagnoses were generated using VINDICATE and an organ system approach. Finally,
students discussed the medical information they obtained, the hypotheses they wished to test, and how
best to approach the patient to gather more information. The role-play resumed with a different
student continuing the interview. This six-step approach emphasized how communication affects
clinical reasoning and how diagnostic hypotheses direct further interviewing.
Implementation
In the 2003-4 academic year, there were 121 students in the second-year class. Sixty were
randomly assigned to the AIME curriculum, and the remaining 61 students participated in AIME later
Windish 2004 8
in the year to ensure that all students received equal instruction. The Johns Hopkins Institutional
Review Board approved the study protocol.
We recruited faculty to teach who were not currently facilitating in other areas of the
curriculum. To ensure uniform instruction, we held a two-hour faculty development session one week
before starting AIME that allowed faculty to participate in an experiential session of role-playing using
the iterative reflective process. We also met with faculty on a weekly basis to review the goals for
each session.
Curriculum Evaluation Methods
Baseline Assessment of Students’ Knowledge and Skills
We introduced the curriculum to the second-year class in a lecture one week before the start of
AIME. At this point in their training, students had only had one opportunity to practice interviewing a
patient. Students completed background questions regarding their age, gender, college major, previous
interviewing experience, and prior medical training. Students also rated their proficiency in specific
communication and clinical reasoning skills on a 5-point scale, where 0 = no exposure, 1 = familiar
with concept, 2 = can perform skill somewhat, 3 = can perform skill well, 4 = can teach to other
students.
To assess baseline knowledge and skills, students observed a video clip of a medical encounter
involving a patient with alcoholic pancreatitis. The roles of the patient and the physician were scripted
to display positive and negative communication behaviors. After viewing the tape, students answered
questions about communication behaviors displayed by the physician, created a problem list and
generated possible diagnoses with supporting and refuting reasons for their top three choices. Finally,
students completed the Diagnostic Thinking Inventory which is a self-reported questionnaire designed
Windish 2004 9
to assess an individual’s clinical reasoning in two areas: the degree of flexibility in thinking and the
degree of knowledge structure in memory.23 The inventory contains 41 questions rated on a six-point
scale, with higher scores indicating a greater degree of diagnostic thinking ability, and has a reliability
of 0.83 (Cronbach α).
Assessment of Student Performance
One week after completing the curriculum, all students underwent a two-station standardized
patient interaction to measure their communication and clinical reasoning skills. The cases represented
disease processes previously covered in Pathophysiology (hyperthyroidism and rheumatoid arthritis).
For each patient, students had fifteen minutes to complete a medical history and to perform a focused
physical exam. To measure communication skills, the standardized patient completed a 30-item
interpersonal checklist that rated behaviors on a 5-point Likert scale, where 1 = poor, 2 = adequate, 3 =
good, 4 = very good, 5 = excellent. We combined select questions into three subscales relating to the
elements of the Three Function Model, including five questions on data gathering (subscale reliability
by Cronbach α was 0.85), eleven questions on establishing rapport (Cronbach α 0.95), and five
questions concerning patient education and counseling (Cronbach α 0.86) (see Table 3). The
standardized patients also completed a case-specific history item checklist to determine what areas of
the medical history were elicited.
To measure clinical reasoning skills, students generated a problem list and differential
diagnosis giving supporting and refuting features for their top three choices. At the end of the session,
students completed the Diagnostic Thinking Inventory. To check the accuracy of each clinical
presentation, fifteen internal medicine physicians independently reviewed a written version of the
Windish 2004 10
history and physical exam for both scenarios and all supported hyperthyroidism and rheumatoid
arthritis as the leading hypotheses.
Assessment of the Curriculum
Students and faculty evaluated each of the six sessions and provided a final assessment at the
end of AIME through questionnaires and informal discussions. Questions asked respondents to rate
the effectiveness of the teaching methods to achieve the curricular objectives (4-point scale: 1 = very
effective, 2 = somewhat effective, 3 = somewhat ineffective, 4 = very ineffective) and to assess the
importance of teaching the targeted skills together (4-point scale: 1 = strongly agree, 2 = agree, 3 =
disagree, 4 = strongly disagree). Open-ended questions asked for feedback regarding the most and
least useful parts of the curriculum and suggestions for change.
Statistical Analyses
We compared baseline characteristics of students using Student’s t-tests for continuous
variables and chi-square analyses for categorical variables. We assessed differences in baseline self-
rated proficiency in communication and clinical reasoning skills using the Wilcoxon rank-sum test.
We used chi-square analyses to compare students’ baseline ability to document communication
observations from the videotaped encounter. In the standardized patient encounters, we used four
measures to assess communication skills, including a mean total interpersonal score for both cases, and
three mean subscores reflecting elements of data gathering, establishing rapport, and patient education
and counseling. We compared each of these scores using Student’s t-tests.
We examined different aspects of clinical reasoning ability at baseline with the video
assessment and after the course with the standardized patient exercise. These included the mean
Windish 2004 11
number of patient problems listed for both cases, the mean number of differential diagnoses generated
for both cases, the mean number of supporting and refuting factors for each case’s correct diagnosis,
and the Diagnostic Thinking Inventory scores. We evaluated differences in the mean number of
patient problems listed, the mean number of differential diagnoses listed, and Diagnostic Thinking
Inventory scores using Student’s t-tests. We used the Wilcoxon rank-sum test to assess differences in
the mean number of supporting and refuting factors. We were particularly interested in the students’
ability to list psychosocial history items (including a patient’s concerns about their illness) as a
measure of their ability to link the psychosocial aspects of communication skills with the biomedical
aspects of clinical reasoning. We assessed the difference in the number of students listing one or more
psychosocial history items on their problem lists using a chi-square analysis.
For our analyses, we had 80% power to detect a difference of 0.22 in each of the four
communication scale ratings (setting alpha at 0.05). We also had 80% power to detect a 1.2 difference
in the mean total number of patient problems listed. All analyses were performed using Stata
Statistical Software: Release 8.0 (Stata Corporation, College Station, Texas, 2002).
RESULTS
Baseline Student Characteristics, Knowledge and Skills
All 121 students randomized remained in their assigned group and 120 successfully completed
the standardized patient exercise. At baseline, we found no differences in age, gender, college major
or previous interviewing experience, but found a significant difference in previous medical training
(see Table 3). With respect to self-rated proficiency in communication and clinical reasoning skills,
AIME students were more likely to report familiarity with methods to develop a differential diagnosis
Windish 2004 12
before the curriculum (p=0.01). They did not differ from the non-AIME students in any other area of
self-evaluation.
For the baseline video assessment, we found no difference in the students’ ability to report on
specific communication skills in data gathering and rapport building (Table 4). For clinical reasoning,
58% of students in each group listed pancreatitis as their top diagnosis. The groups had the same mean
number of patient problems, differential diagnoses, and supporting and refuting factors for the
diagnosis of pancreatitis (Table 4). The groups did not differ in their clinical reasoning ability as
assessed by the Diagnostic Thinking Inventory.
Student Performance at the End of the Curricular Intervention
For the standardized patient exercise, interpersonal score ratings were similar for AIME and
non-AIME students (Table 5). In addition, each group obtained similar numbers of history items from
the patients during the interviews (mean of 64.2% vs. 63.1%). Although communication skills did not
differ significantly between groups, we observed a trend in the AIME students having an increased
ability to establish and maintain rapport during a medical interview (p=0.08).
For clinical reasoning, both groups listed a mean of 4 differential diagnoses. In the
hyperthyroid case, 79% of AIME students listed the correct diagnosis as their top choice compared to
69% of non-AIME students (p=0.21). For the rheumatoid arthritis case, 92% of AIME students and
95% of non-AIME students listed rheumatoid arthritis as their top diagnosis (p=0.44). On average,
each group generated two supporting factors and less than one refuting factor for the correct diagnosis
(p=0.40).
Differences were seen in the students’ ability to generate a problem list. AIME students had on
average one more problem listed for each patient (mean 8.4 versus 7.5; p=0.05). In addition, their
Windish 2004 13
problem lists were more likely to contain elements of the history of present illness (mean 5.7 versus
4.8; p=0.01) and the psychosocial history (64% of AIME students listing one or more items vs. 44% of
non-AIME students; p=0.03). We saw no difference between the groups in their Diagnostic Thinking
Inventory scores.
Participant and Faculty Evaluation of the Curriculum
At the end of AIME, 56 of 60 students provided feedback on the curriculum. Eighty-four
percent reported that the curriculum was somewhat to very effective in teaching techniques to establish
rapport, to elicit patient preferences and to develop problem lists and differential diagnoses. Ninety-
five percent of students found it beneficial to learn communication and clinical reasoning skills in an
integrative fashion. Students rated self-reflection and observation as a highly effective learning
strategy (98% of respondents). Seventy-five percent of students used approaches to the medical
encounter taught in AIME during other patient interactions. Of those who had not used the
approaches, 72% stated they did not have an opportunity to practice but hoped to use these skills in the
future. Role-playing was felt to be the most useful part of the curriculum by 68% of students.
Faculty felt strongly that role-play with time-outs allowed for meaningful discussion of
communication and clinical reasoning [median of 1 (interquartile range (IQR) 1-2) with 1=strongly
agree and 4=strongly disagree] and indicated that it was valuable to teach these skills together [median
of 1 (IQR 1-2)]. Since teaching during role-play was a new technique for most facilitators, many felt
that having additional instruction in this area would be beneficial. Half of the facilitators noted being
more engaged in shared decision-making styles of communication with their own patients as a result of
teaching in the curriculum.
Windish 2004 14
CONCLUSIONS
We designed AIME to teach the integration of communication and clinical reasoning skills.
We found that students who participated in the curriculum were better at integrating these skills during
a medical encounter than those students who did not have the intervention. In particular, students were
more likely to list elements of a patient’s psychosocial history on their problem lists, including a
patient’s concerns about their illness. This suggests that AIME helped students understand the
connection between biomedical and psychosocial aspects of patient care.
We saw statistically significant differences in AIME students’ ability to integrate biomedical
and psychosocial aspects of patient information during the standardized patient exercise. In
communication skills, we saw a trend toward significance in AIME students’ ability to establish
rapport with patients, which was an emphasis of our communication skills training. In clinical
reasoning, AIME students listed more patient problems on their problem lists including more elements
of the biomedical and psychosocial history. We did not see a difference between groups with respect
to the number of diagnoses generated or in the Diagnostic Thinking Inventory scores. This most likely
reflected the limited opportunities students had to practice generating hypotheses and to subsequently
reflect on their thinking during patient encounters outside of AIME.
In medical practice, good communication and clinical reasoning skills are important clinical
competencies. However, research shows many physician inadequacies in these skills including
incomplete solicitation of patient concerns24 and inconsistent exploration of psychosocial issues25.
These practices can lead to inappropriate prioritization of problems, impaired clinical reasoning and
poor therapeutic alliances with the potential for medical error and harm to patients. Providing medical
students with the framework to integrate biomedical and psychosocial aspects of patient care early in
their training may prevent these errors from occurring later in practice.
Windish 2004 15
A report summarizing the efforts to integrate basic sciences, clinical sciences and
biopsychosocial medicine in the Robert Wood Johnson Foundation’s Program in Medical Education
found that despite attempts at curriculum reform, “Basic science dominates; at best, biopsychosocial
issues are treated as separate but equal—and often as separate and not equal.”26 This may lead
students to perceive the psychosocial aspects of medicine as less important. We feel that by teaching
the connection between communication skills and clinical reasoning through reflective learning in a
patient-centered manner, students will understand the important relation between the biomedical and
psychosocial aspects of patient care and value this approach to problem solving. This was supported
by our formative curricular assessment that showed that both students and faculty appreciated the
connection between the two skills and found importance in learning them together.
Our work has several limitations. First, only two standardized patient interactions were used to
evaluate differences between groups. Literature suggests that multiple stations of an objective
structured clinical exam are needed to truly assess differences.27 Due to a limited number of cases, we
may not have been able to detect all of the differences that may have existed between the two groups.
In the future, we plan to use a more structured assessment to measure students’ acquisition of skills.
Second, the structure of the standard Clinical Skills curriculum limits opportunities to interview
patients on an individual basis until late in the second year. This restricted the students’ ability to
practice techniques learned in AIME and may have limited our ability to show a difference in certain
skills. We hope to incorporate AIME longitudinally into the Clinical Skills curriculum this upcoming
year. With more practice, both communication and clinical reasoning scores might improve. Third,
despite randomization, students assigned to the AIME curriculum reported more prior medical training
and familiarity with techniques to generate differential diagnoses. We doubt that this played a role in
the higher clinical reasoning scores we saw in the final assessment, because the baseline assessment of
Windish 2004 16
these skills did not differ between groups. Finally, since we intended to explore various domains of
communication and clinical reasoning, we used multiple measures to determine differences in
performance. Although we did not adjust our tests of statistical significance for multiple comparisons,
the significant differences and the non-significant trends were consistently in the direction of
improvement in skill acquisition with the curricular intervention.
We believe that teaching students communication and clinical reasoning skills in a patient-
centered manner using reflection and feedback promotes understanding the patient as a whole, allows
individual thinking, and encourages collaborative learning among peers, skills that are important to
future success in medical practice. With this innovative curriculum, we have shown that these closely
related, yet often separately taught, skills can be integrated and are valued when learned together. The
results of this study should help other educators develop curricula aimed at teaching the integration of
these important clinical competencies. Future educational initiatives in all stages of training could lead
to improved patient-physician interactions and positively impact satisfaction and health outcomes.
Windish 2004 17
REFERENCES
1. Association of American Medical Colleges (AAMC). Learning objectives for
medical student education—guidelines for medical schools: report I of the medical
school objectives project. January 1998; Available from: http://www.aamc.org/meded/msop/.
Accessed March 28, 2003.
2. Liaison Committee on Medical Education (LCME). Functions and structures of a medical school:
standards for accreditation of medical education programs leading to the M.D. degree. July 2003;
Available from: http://www.lcme.org/. Accessed July 16, 2003.
3. Accreditation Council for Graduate Medical Education (ACGME). Outcome project: enhancing
residency education through outcomes assessment. Available from: http//www.acgme.org/Outcome/.
Accessed March 28, 2003.
4. Evans RJ, Stanley RO, Mestrovic R, Rose L. Effects of communication skills training on students’
diagnostic efficiency. Med Educ. 1991;25(6):517-26.
5. Roter D, Hall JA, Kern DE, Barker LR, Cole KA, Roca RP. Improving physicians’ interviewing
skills and reducing patients’ emotional distress: A randomized clinical trial. Arch Intern Med.
1995 Sept 25;155(17):1877-84.
6. Little P, Everitt H, Williamson I, Warner G, Moore M, Gould C, Ferrier K, Payne S. Observational
study of effect of patient centredness and positive approach on outcomes of general practice
consultations. BMJ. 2001 Oct 20;323(7318):908-11.
7. Roter DL, Hall JA, Katz NR. Relations between physicians' behaviors and analogue patients'
satisfaction, recall, and impressions. Med Care. 1987 May;25(5):437-51.
8. Mead N, Bower P. Patient-centred consultations and outcomes in primary care: a review of the
literature. Patient Educ Couns. 2002 Sep;48(1):51-61.
Windish 2004 18
9. Kempainen RR, Migeon MB, Wolf FM. Understanding our mistakes: a primer on errors in clinical
reasoning. Med Teach. 2003;25(2):177-81.
10. Weise J, Saint S, Tierney, Jr. LM. Using clinical reasoning to improve skills in oral case
presentation. Seminars in Medical Practice. 2002 Sep;5(3):29-36.
11. Kern DE, Thomas PA, Howard DM, Bass EB. Curriculum development for medical education: a
six-step approach. Baltimore: The Johns Hopkins University Press, 1998.
12. Bird J, Cohen-Cole SA. The three function model of the medical interview. Adv Psychosom Med.
1990;20:65-88.
13. Keller V, Carroll J. A new model for physician-patient communication. Patient Educ Couns.
1994;23:131-40.
14. Kurtz S, Silverman J. The Calgary-Cambridge Referenced Observation Guides: an aid to defining
the curriculum and organizing the teaching in communication training programs. Med Educ.
1996;30:83-9.
15. Makoul G. “The SEGUE Framework for teaching and assessing communication skills.” Patient
Educ Couns. 2001;(45):23-34.
16. Stewart M, Brown JB, Weston WW, McWhinney IR, McWilliam CL, Freeman TR. Patient-
centered medicine: transforming the clinical method (patient-centered case series). Thousand
Oaks: Sage, 1995.
17. Thomas RE. Teaching medicine with cases: student and teacher opinion. Med Educ.
1992;26:200-7.
18. Rogers JC, Swee DE, Ullian JA. Teaching medical decision making and students’ clinical
problem solving skills. Med Teach. 1991;13(2):157-63.
Windish 2004 19
19. Menahem S, Paget N. Role play for the clinical tutor: towards problem-based learning. Med
Teach. 1990;12(1):57-61.
20. Bayer Institute for Healthcare Communication. Available from: http://www.bayerinstitute.com.
Accessed March 22, 2004.
21. Windish DM, Paulman PM, Goroll AH, Bass EB. Do clerkship directors think medical students
are prepared for the clerkship years? Acad Med. 2004;79:56-61.
22. Kurtz SM, Silverman JD, Draper J. Teaching and learning communication skills in medicine.
Oxford: Radcliffe Medical Press, 1998.
23. Bordage G, Grant J, Marsden P. Quantitative assessment of diagnostic ability. Med Educ. 1990;
24(5):413-25.
24. Marvel MK, Epstein RM, Flowers K, Beckman HB. Soliciting patient’s agenda: have we
improved? JAMA. 1999 Jan 20;281(3):283-7.
25. Levinson W, Roter D. Physicians’ psychosocial beliefs correlate with their patient communication
skills. J General Intern Med. 1995 Jul;10(7):375-9.
26. Schmidt H. Integrating the teaching of basic sciences, clinical sciences, and biopsychosocial
issues. Acad Med. 1998 Sep;73(9 Suppl):S24-31.
27. Norcini J, Boulet J. Methodological issues in the use of standardized patients for assessment.
Teach Learn Med. 2003 Fall;15(4):293-7.
Windish 2004 20
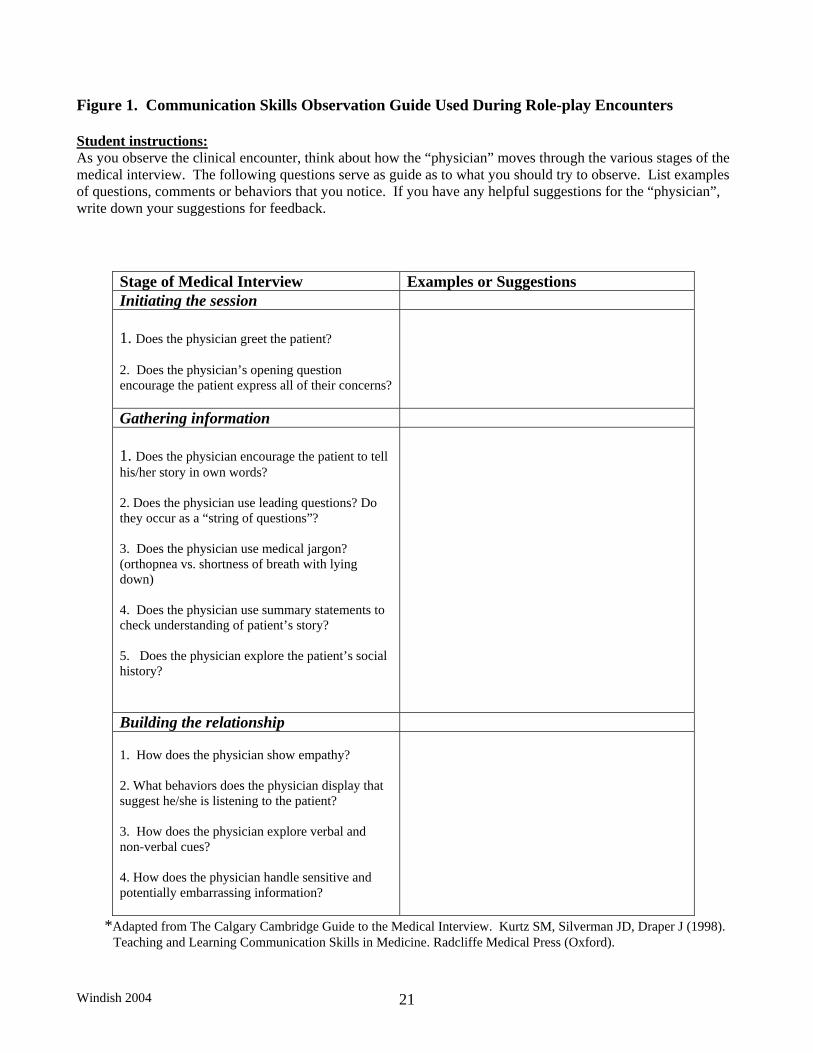
Figure 1. Communication Skills Observation Guide Used During Role-play Encounters
Student instructions: As you observe the clinical encounter, think about how the “physician” moves through the various stages of the medical interview. The following questions serve as guide as to what you should try to observe. List examples of questions, comments or behaviors that you notice. If you have any helpful suggestions for the “physician”, write down your suggestions for feedback.
Stage of Medical Interview Examples or Suggestions Initiating the session 1. Does the physician greet the patient? 2. Does the physician’s opening question encourage the patient express all of their concerns?
Gathering information 1. Does the physician encourage the patient to tell his/her story in own words? 2. Does the physician use leading questions? Do they occur as a “string of questions”? 3. Does the physician use medical jargon? (orthopnea vs. shortness of breath with lying down) 4. Does the physician use summary statements to check understanding of patient’s story? 5. Does the physician explore the patient’s social history?
Building the relationship 1. How does the physician show empathy? 2. What behaviors does the physician display that suggest he/she is listening to the patient? 3. How does the physician explore verbal and non-verbal cues? 4. How does the physician handle sensitive and potentially embarrassing information?
*Adapted from The Calgary Cambridge Guide to the Medical Interview. Kurtz SM, Silverman JD, Draper J (1998). Teaching and Learning Communication Skills in Medicine. Radcliffe Medical Press (Oxford).
Windish 2004 21
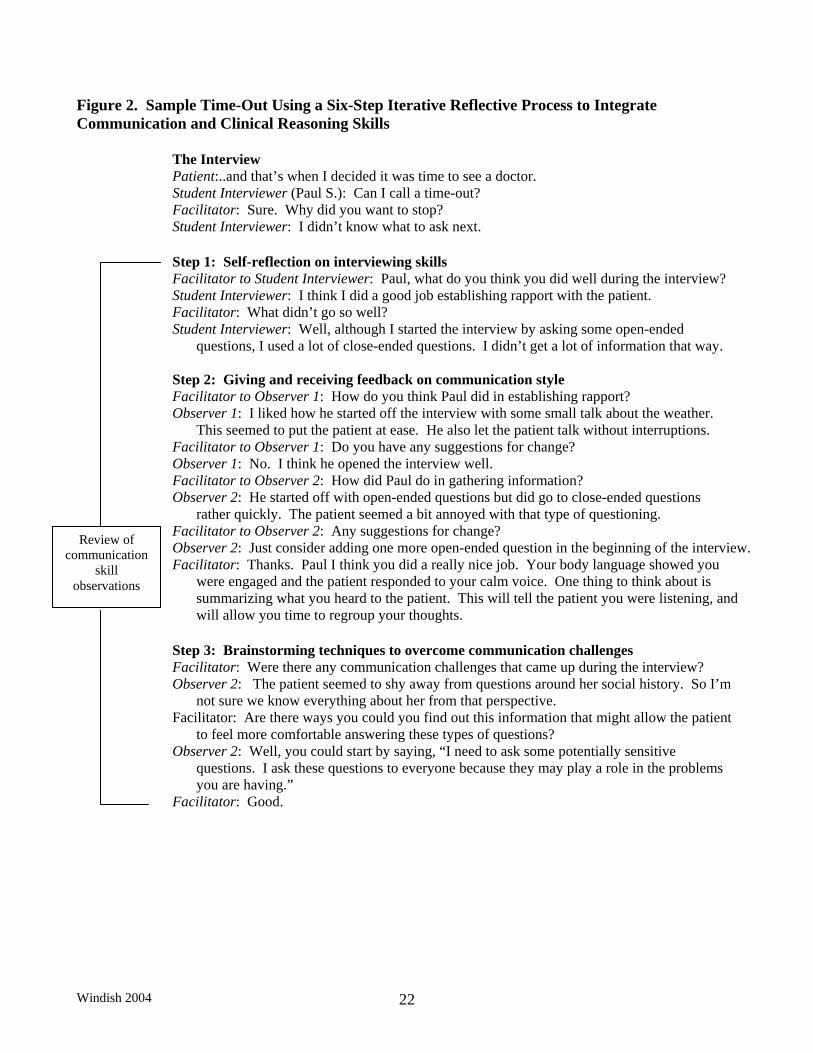
Figure 2. Sample Time-Out Using a Six-Step Iterative Reflective Process to Integrate Communication and Clinical Reasoning Skills The Interview Patient:..and that’s when I decided it was time to see a doctor.
Student Interviewer (Paul S.): Can I call a time-out? Facilitator: Sure. Why did you want to stop? Student Interviewer: I didn’t know what to ask next. Step 1: Self-reflection on interviewing skills Facilitator to Student Interviewer: Paul, what do you think you did well during the interview? Student Interviewer: I think I did a good job establishing rapport with the patient.
Review of communication
skill observations
Facilitator: What didn’t go so well? Student Interviewer: Well, although I started the interview by asking some open-ended
questions, I used a lot of close-ended questions. I didn’t get a lot of information that way.
Step 2: Giving and receiving feedback on communication style Facilitator to Observer 1: How do you think Paul did in establishing rapport? Observer 1: I liked how he started off the interview with some small talk about the weather.
This seemed to put the patient at ease. He also let the patient talk without interruptions. Facilitator to Observer 1: Do you have any suggestions for change? Observer 1: No. I think he opened the interview well. Facilitator to Observer 2: How did Paul do in gathering information? Observer 2: He started off with open-ended questions but did go to close-ended questions
rather quickly. The patient seemed a bit annoyed with that type of questioning. Facilitator to Observer 2: Any suggestions for change? Observer 2: Just consider adding one more open-ended question in the beginning of the interview. Facilitator: Thanks. Paul I think you did a really nice job. Your body language showed you
were engaged and the patient responded to your calm voice. One thing to think about is summarizing what you heard to the patient. This will tell the patient you were listening, and will allow you time to regroup your thoughts.
Step 3: Brainstorming techniques to overcome communication challenges Facilitator: Were there any communication challenges that came up during the interview? Observer 2: The patient seemed to shy away from questions around her social history. So I’m
not sure we know everything about her from that perspective. Facilitator: Are there ways you could you find out this information that might allow the patient
to feel more comfortable answering these types of questions? Observer 2: Well, you could start by saying, “I need to ask some potentially sensitive
questions. I ask these questions to everyone because they may play a role in the problems you are having.”
Facilitator: Good.
Windish 2004 22
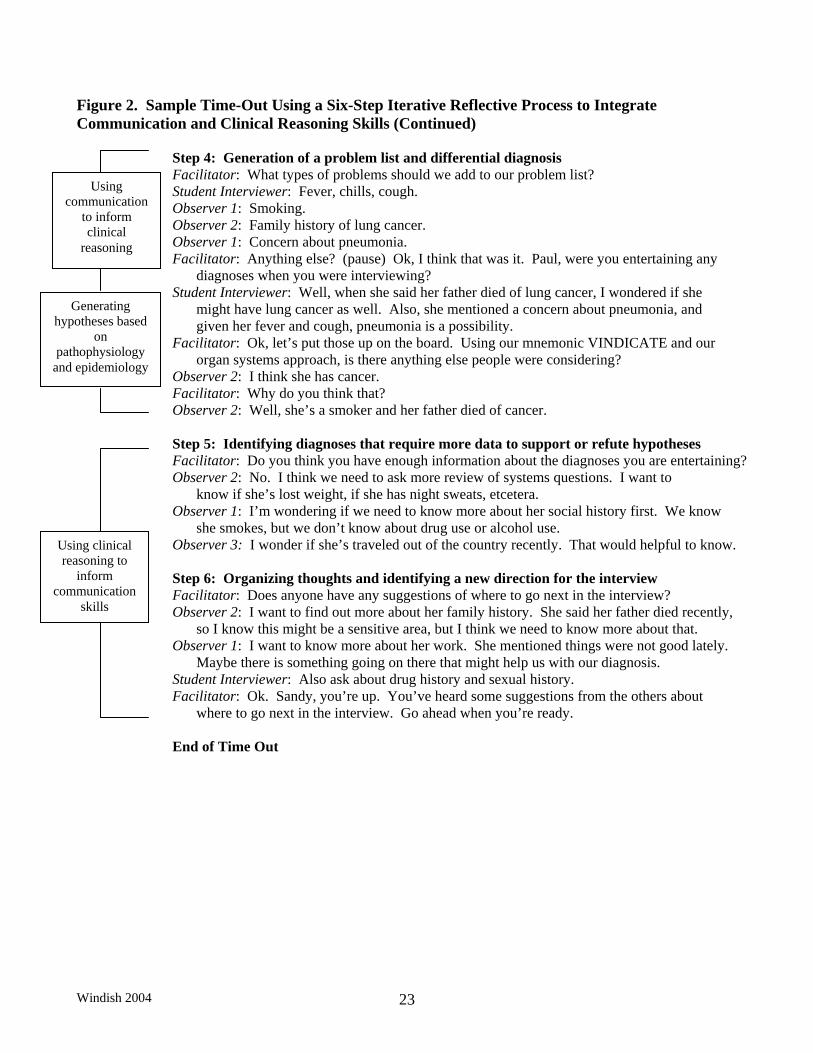
Figure 2. Sample Time-Out Using a Six-Step Iterative Reflective Process to Integrate Communication and Clinical Reasoning Skills (Continued)
Step 4: Generation of a problem list and differential diagnosis
Using communication
to inform clinical
reasoning
Generating hypotheses based
on pathophysiology
and epidemiology
Using clinical reasoning to
inform communication
skills
Facilitator: What types of problems should we add to our problem list? Student Interviewer: Fever, chills, cough. Observer 1: Smoking. Observer 2: Family history of lung cancer. Observer 1: Concern about pneumonia. Facilitator: Anything else? (pause) Ok, I think that was it. Paul, were you entertaining any
diagnoses when you were interviewing? Student Interviewer: Well, when she said her father died of lung cancer, I wondered if she
might have lung cancer as well. Also, she mentioned a concern about pneumonia, and given her fever and cough, pneumonia is a possibility.
Facilitator: Ok, let’s put those up on the board. Using our mnemonic VINDICATE and our organ systems approach, is there anything else people were considering?
Observer 2: I think she has cancer. Facilitator: Why do you think that? Observer 2: Well, she’s a smoker and her father died of cancer.
Step 5: Identifying diagnoses that require more data to support or refute hypotheses Facilitator: Do you think you have enough information about the diagnoses you are entertaining? Observer 2: No. I think we need to ask more review of systems questions. I want to
know if she’s lost weight, if she has night sweats, etcetera. Observer 1: I’m wondering if we need to know more about her social history first. We know
she smokes, but we don’t know about drug use or alcohol use. Observer 3: I wonder if she’s traveled out of the country recently. That would helpful to know.
Step 6: Organizing thoughts and identifying a new direction for the interview Facilitator: Does anyone have any suggestions of where to go next in the interview? Observer 2: I want to find out more about her family history. She said her father died recently,
so I know this might be a sensitive area, but I think we need to know more about that. Observer 1: I want to know more about her work. She mentioned things were not good lately.
Maybe there is something going on there that might help us with our diagnosis. Student Interviewer: Also ask about drug history and sexual history. Facilitator: Ok. Sandy, you’re up. You’ve heard some suggestions from the others about
where to go next in the interview. Go ahead when you’re ready.
End of Time Out
Windish 2004 23
Windish 2004 24
Table 1. Reports of Formal Training in Communication and Clinical Reasoning Skills and the Level of Student Preparedness for the Clerkships as Assessed by 96 Clerkship Students and Six Clerkship Directors Before the Curriculum Intervention.
able 1. Reports of Formal Training in Communication and Clinical Reasoning Skills and the Level of Student Preparedness for the Clerkships as Assessed by 96 Clerkship Students and Six Clerkship Directors Before the Curriculum Intervention.
Clerkship Clerkship Students
Reporting They Had
Formal Training*
Students Reporting They Had
Formal Training*
Clerkship Clerkship Faculty
Reporting They
Provide Formal
Training*
Faculty Reporting
They Provide Formal
Training*
Clerkship Clerkship Students
Reporting They Are
Less Prepared In
Skills†
Students Reporting They Are
Less Prepared In
Skills†
Clerkship Clerkship Faculty
Reporting Students Are Less Prepared In Skills‡
Faculty Reporting Students Are Less Prepared In Skills‡
Communication Skills, % Communication Skills, % Using verbal and nonverbal cues during an encounter to demonstrate listening
92 33 11 80
Eliciting patients’ concerns, beliefs and expectations of their health/illness
88 40 41 80
Encourage questions from patients regarding their health and illness
89 50 32 100
Eliciting patient preferences for their role in decision-making
70 66 53 60
Clinical Reasoning Skills, %
Creating a problem list 96 100 55 0
Developing differential diagnoses 81 66 68 17
Using methods to develop a differential diagnosis (e.g., mnemonics)
81 NR§ 73 NR§
*Formal training is defined as using handouts, lectures, small group discussion, standardized patients, or real patients in instruction. Students reported whether they received formal training in any part of medical school and clerkship directors indicated whether they provided formal training in their clerkship. †“Less Prepared” was any student self-rating of “no exposure”, “familiar with concept”, or “can perform skill somewhat”. ‡Faculty rated students as “less prepared”, “at the level they should be” or “more prepared” in skills. §Not rated by the clerkship directors.
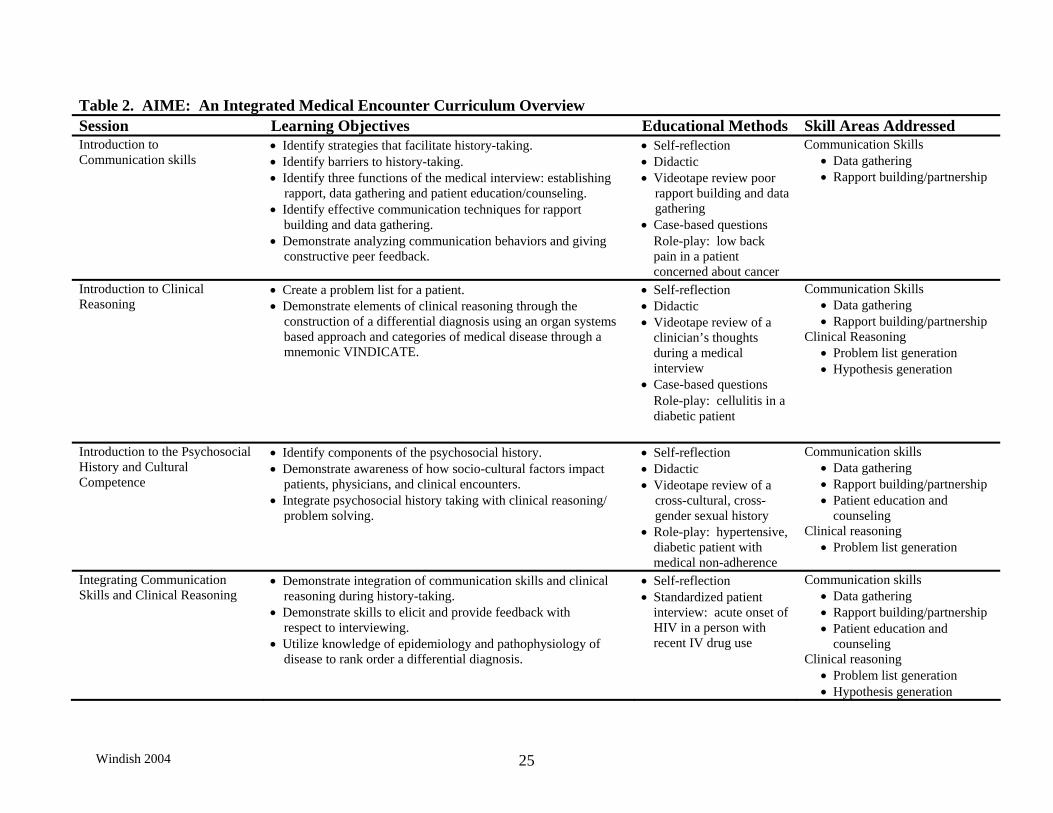
Table 2. AIME: An Integrated Medical Encounter Curriculum Overview Session Learning Objectives Educational Methods Skill Areas Addressed
Introduction to Communication skills
• Identify strategies that facilitate history-taking. • Identify barriers to history-taking. • Identify three functions of the medical interview: establishing rapport, data gathering and patient education/counseling. • Identify effective communication techniques for rapport building and data gathering. • Demonstrate analyzing communication behaviors and giving constructive peer feedback.
• Self-reflection • Didactic • Videotape review poor rapport building and data gathering • Case-based questions
Role-play: low back pain in a patient concerned about cancer
Communication Skills • Data gathering • Rapport building/partnership
Introduction to Clinical Reasoning
• Create a problem list for a patient. • Demonstrate elements of clinical reasoning through the construction of a differential diagnosis using an organ systems based approach and categories of medical disease through a mnemonic VINDICATE.
• Self-reflection • Didactic • Videotape review of a
clinician’s thoughts during a medical interview
• Case-based questions Role-play: cellulitis in a diabetic patient
Communication Skills • Data gathering • Rapport building/partnership
Clinical Reasoning • Problem list generation • Hypothesis generation
Introduction to the Psychosocial History and Cultural Competence
• Identify components of the psychosocial history. • Demonstrate awareness of how socio-cultural factors impact patients, physicians, and clinical encounters. • Integrate psychosocial history taking with clinical reasoning/ problem solving.
• Self-reflection • Didactic • Videotape review of a cross-cultural, cross- gender sexual history • Role-play: hypertensive,
diabetic patient with medical non-adherence
Communication skills • Data gathering • Rapport building/partnership • Patient education and
counseling Clinical reasoning
• Problem list generation
Integrating Communication Skills and Clinical Reasoning
• Demonstrate integration of communication skills and clinical reasoning during history-taking. • Demonstrate skills to elicit and provide feedback with respect to interviewing. • Utilize knowledge of epidemiology and pathophysiology of disease to rank order a differential diagnosis.
• Self-reflection • Standardized patient
interview: acute onset of HIV in a person with recent IV drug use
Communication skills • Data gathering • Rapport building/partnership • Patient education and
counseling Clinical reasoning
• Problem list generation • Hypothesis generation
Windish 2004 25
Windish 2004 26
Table 2. AIME: An Integrated Medical Encounter Curriculum Overview (continued) Session Learning Objectives Educational Methods Skill Areas Addressed
Reasoning Through A Differential Diagnosis
• Define and practice using pretest probability using researched knowledge of epidemiology and pathophyisiology. • Re-rank differential diagnoses using supportive data. • Select appropriate diagnostic studies. • Present sensitive information to a patient.
• Self-reflection • Didactic • Case-based questions • Role-play: presenting an
HIV positive test result to a patient
Communication skills • Patient education and counseling
Clinical reasoning • Hypothesis generation • Diagnostic test selection
Introduction to Shared Decision Making
• Identify principles of and rationale behind shared decision making. • Demonstrate phrases that can promote shared decision-making.
• Self-reflection • Didactic • Case-based questions • Videotape review of a failure to elicit patient preferences for care • Role-play: subacute headache in a patient concerned about having a brain tumor
Communication Skills • Data gathering • Rapport building/ partnership • Patient education and counseling
Clinical reasoning • Problem list generation • Hypothesis generation
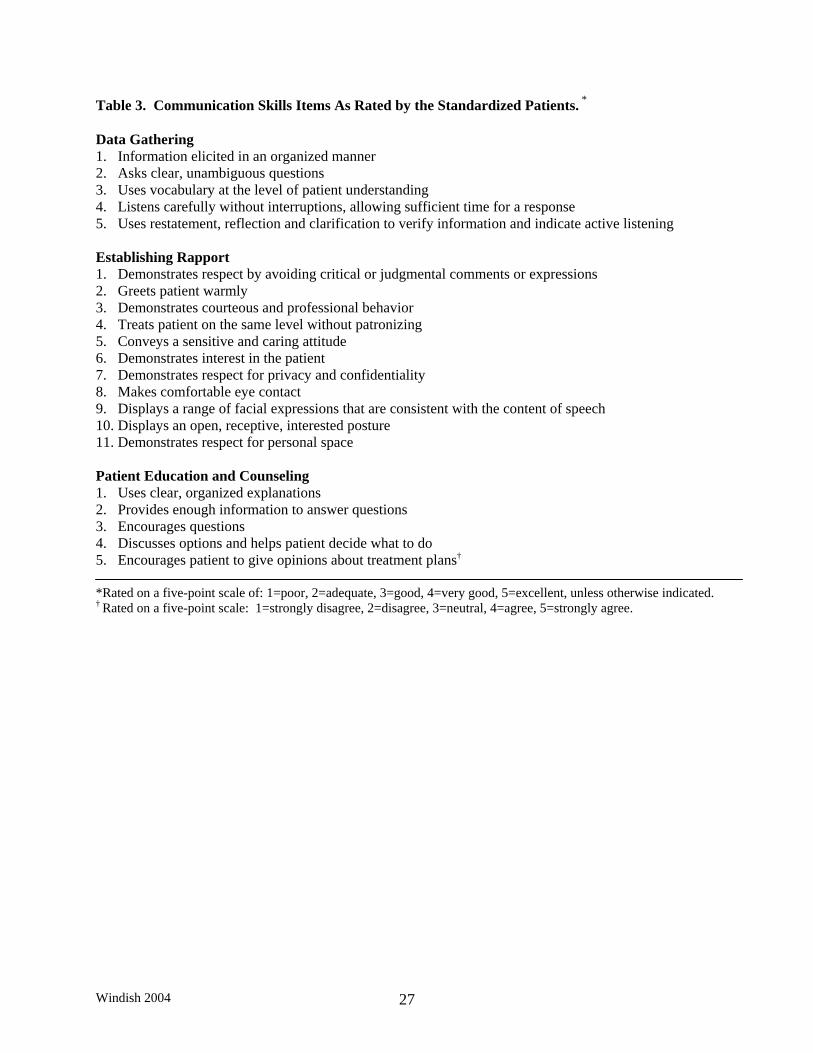
Table 3. Communication Skills Items As Rated by the Standardized Patients. * Data Gathering 1. Information elicited in an organized manner 2. Asks clear, unambiguous questions 3. Uses vocabulary at the level of patient understanding 4. Listens carefully without interruptions, allowing sufficient time for a response 5. Uses restatement, reflection and clarification to verify information and indicate active listening
Establishing Rapport 1. Demonstrates respect by avoiding critical or judgmental comments or expressions 2. Greets patient warmly 3. Demonstrates courteous and professional behavior 4. Treats patient on the same level without patronizing 5. Conveys a sensitive and caring attitude 6. Demonstrates interest in the patient 7. Demonstrates respect for privacy and confidentiality 8. Makes comfortable eye contact 9. Displays a range of facial expressions that are consistent with the content of speech 10. Displays an open, receptive, interested posture 11. Demonstrates respect for personal space Patient Education and Counseling 1. Uses clear, organized explanations 2. Provides enough information to answer questions 3. Encourages questions 4. Discusses options and helps patient decide what to do 5. Encourages patient to give opinions about treatment plans† *Rated on a five-point scale of: 1=poor, 2=adequate, 3=good, 4=very good, 5=excellent, unless otherwise indicated. † Rated on a five-point scale: 1=strongly disagree, 2=disagree, 3=neutral, 4=agree, 5=strongly agree.
Windish 2004 27
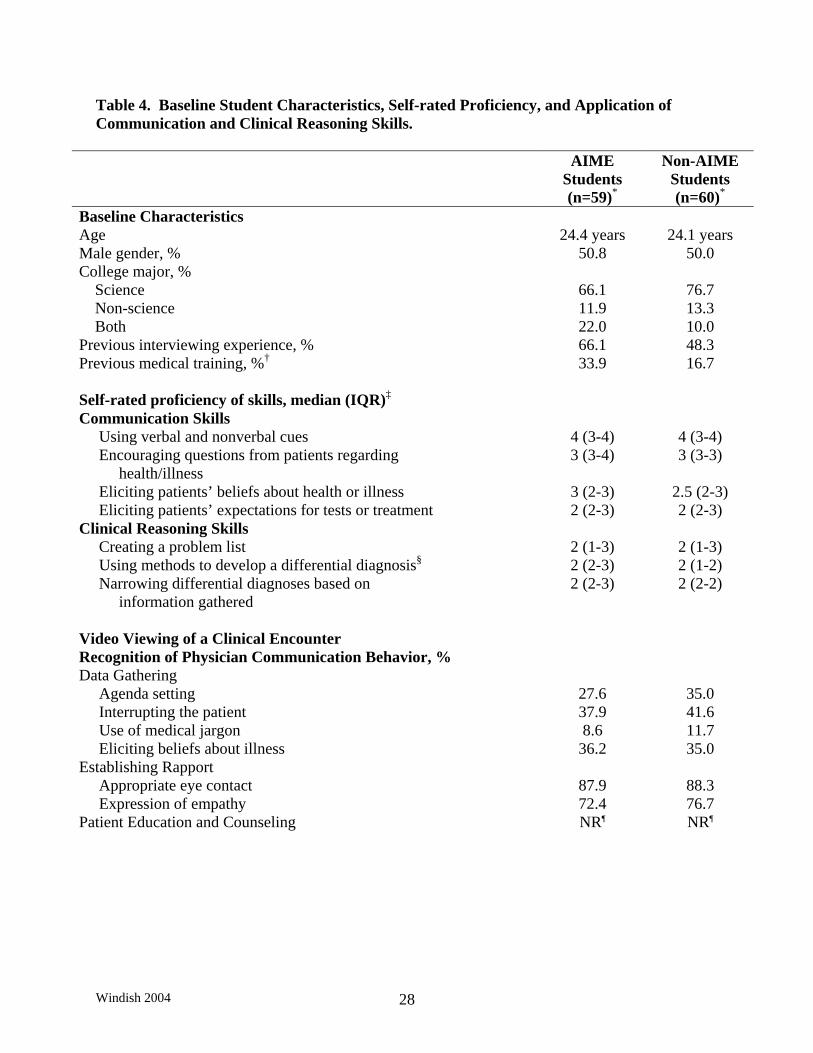
Table 4. Baseline Student Characteristics, Self-rated Proficiency, and Application of Communication and Clinical Reasoning Skills.
AIME Students (n=59)*
Non-AIME Students (n=60)*
Baseline Characteristics Age 24.4 years 24.1 years Male gender, % 50.8 50.0 College major, % Science 66.1 76.7 Non-science 11.9 13.3 Both 22.0 10.0 Previous interviewing experience, % 66.1 48.3 Previous medical training, %† 33.9 16.7 Self-rated proficiency of skills, median (IQR)‡ Communication Skills Using verbal and nonverbal cues 4 (3-4) 4 (3-4) Encouraging questions from patients regarding health/illness
3 (3-4) 3 (3-3)
Eliciting patients’ beliefs about health or illness 3 (2-3) 2.5 (2-3) Eliciting patients’ expectations for tests or treatment 2 (2-3) 2 (2-3) Clinical Reasoning Skills Creating a problem list 2 (1-3) 2 (1-3) Using methods to develop a differential diagnosis§ 2 (2-3) 2 (1-2) Narrowing differential diagnoses based on information gathered
2 (2-3) 2 (2-2)
Video Viewing of a Clinical Encounter Recognition of Physician Communication Behavior, % Data Gathering Agenda setting 27.6 35.0 Interrupting the patient 37.9 41.6 Use of medical jargon 8.6 11.7 Eliciting beliefs about illness 36.2 35.0 Establishing Rapport Appropriate eye contact 87.9 88.3 Expression of empathy 72.4 76.7 Patient Education and Counseling NR¶ NR¶
Windish 2004 28
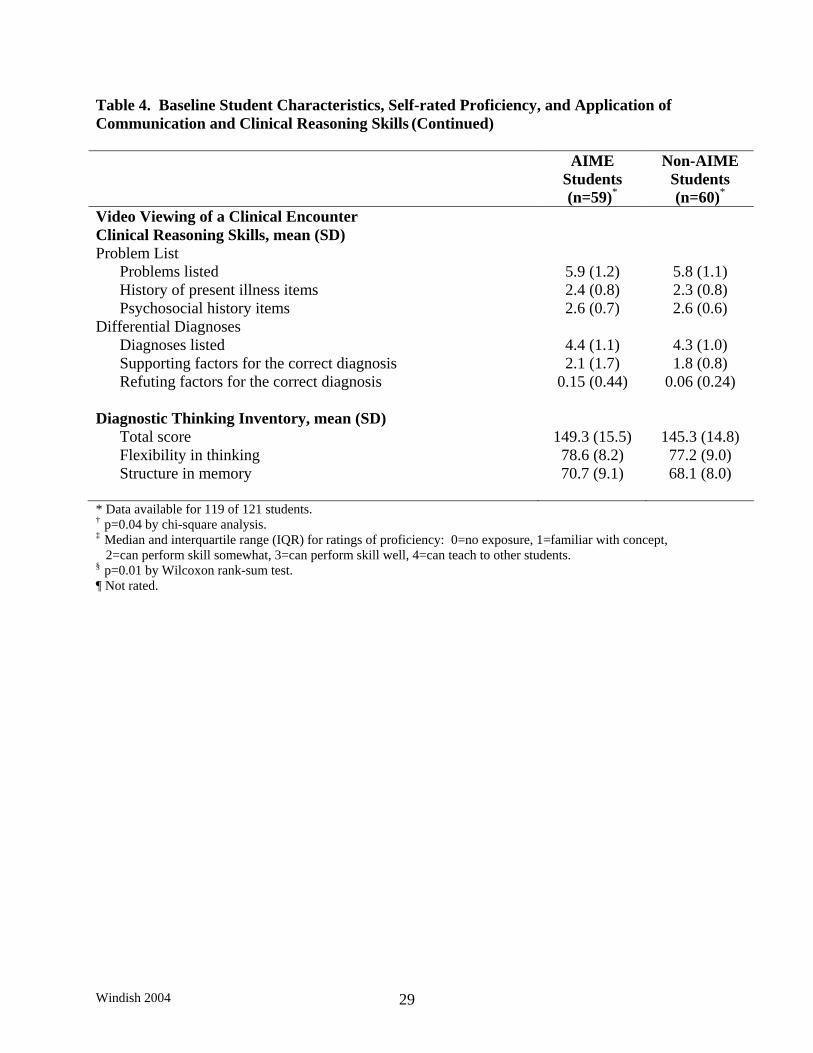
Table 4. Baseline Student Characteristics, Self-rated Proficiency, and Application of Communication and Clinical Reasoning Skills (Continued) AIME
Students (n=59)*
Non-AIME Students (n=60)*
Video Viewing of a Clinical Encounter Clinical Reasoning Skills, mean (SD) Problem List Problems listed 5.9 (1.2) 5.8 (1.1) History of present illness items 2.4 (0.8) 2.3 (0.8) Psychosocial history items 2.6 (0.7) 2.6 (0.6) Differential Diagnoses Diagnoses listed 4.4 (1.1) 4.3 (1.0) Supporting factors for the correct diagnosis 2.1 (1.7) 1.8 (0.8) Refuting factors for the correct diagnosis 0.15 (0.44) 0.06 (0.24) Diagnostic Thinking Inventory, mean (SD) Total score 149.3 (15.5) 145.3 (14.8) Flexibility in thinking 78.6 (8.2) 77.2 (9.0) Structure in memory 70.7 (9.1) 68.1 (8.0) * Data available for 119 of 121 students. † p=0.04 by chi-square analysis. ‡ Median and interquartile range (IQR) for ratings of proficiency: 0=no exposure, 1=familiar with concept, 2=can perform skill somewhat, 3=can perform skill well, 4=can teach to other students. § p=0.01 by Wilcoxon rank-sum test. ¶ Not rated.
Windish 2004 29
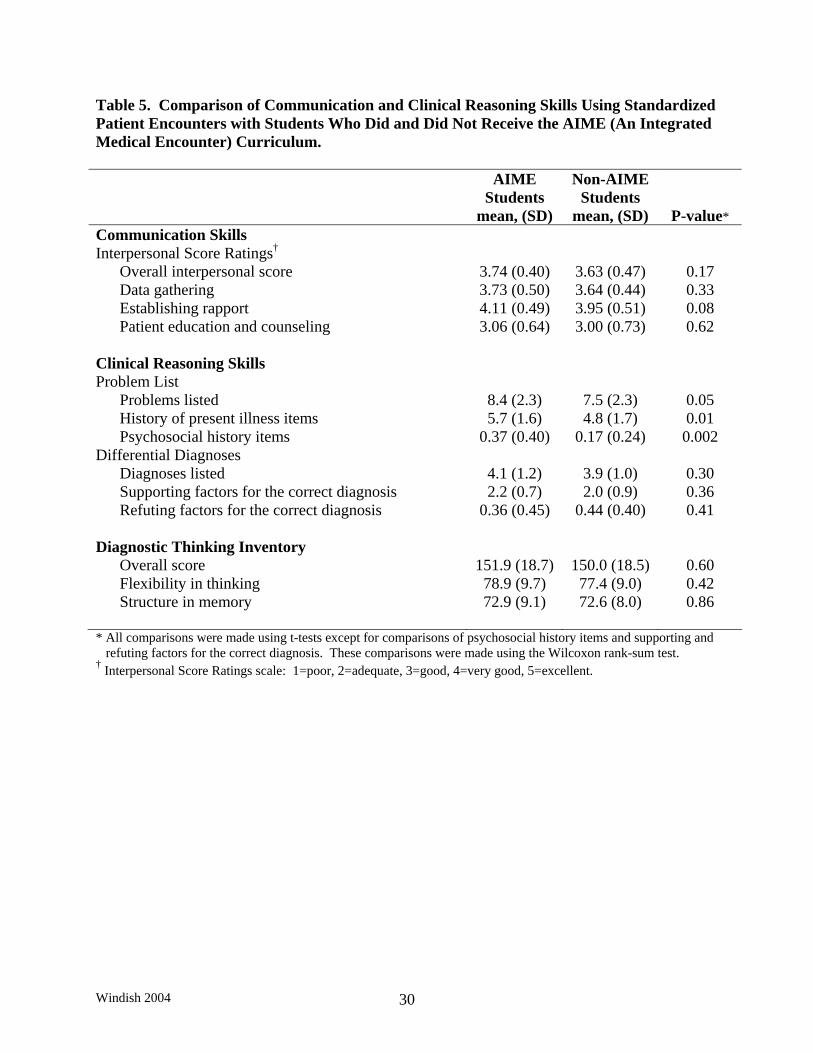
Table 5. Comparison of Communication and Clinical Reasoning Skills Using Standardized Patient Encounters with Students Who Did and Did Not Receive the AIME (An Integrated Medical Encounter) Curriculum. AIME
Students mean, (SD)
Non-AIME Students
mean, (SD)
P-value* Communication Skills Interpersonal Score Ratings† Overall interpersonal score 3.74 (0.40) 3.63 (0.47) 0.17 Data gathering 3.73 (0.50) 3.64 (0.44) 0.33 Establishing rapport 4.11 (0.49) 3.95 (0.51) 0.08 Patient education and counseling 3.06 (0.64) 3.00 (0.73) 0.62 Clinical Reasoning Skills Problem List Problems listed 8.4 (2.3) 7.5 (2.3) 0.05 History of present illness items 5.7 (1.6) 4.8 (1.7) 0.01 Psychosocial history items 0.37 (0.40) 0.17 (0.24) 0.002 Differential Diagnoses Diagnoses listed 4.1 (1.2) 3.9 (1.0) 0.30 Supporting factors for the correct diagnosis 2.2 (0.7) 2.0 (0.9) 0.36 Refuting factors for the correct diagnosis 0.36 (0.45) 0.44 (0.40) 0.41 Diagnostic Thinking Inventory Overall score 151.9 (18.7) 150.0 (18.5) 0.60 Flexibility in thinking 78.9 (9.7) 77.4 (9.0) 0.42 Structure in memory 72.9 (9.1) 72.6 (8.0) 0.86 * All comparisons were made using t-tests except for comparisons of psychosocial history items and supporting and refuting factors for the correct diagnosis. These comparisons were made using the Wilcoxon rank-sum test. † Interpersonal Score Ratings scale: 1=poor, 2=adequate, 3=good, 4=very good, 5=excellent.
Windish 2004 30





























