Embed Size (px)
Citation preview
The University of Sydney ‐ Commercial in Confidence Page 1 of 36
Teaching Resources

The University of Sydney ‐ Commercial in Confidence Page 2 of 36
Contents
What is the Competency Based Curriculum ................................................................................. 3
Background .................................................................................................................................... 3
Competency Based Teaching ........................................................................................................ 5
Assessment .................................................................................................................................... 5
Attributes of Competency Based Teaching ................................................................................... 6
Importance for the Student .......................................................................................................... 7
The University of Sydney ‐ Commercial in Confidence Page 3 of 36
The Competency Based Curriculum D IDC BASED PRACTICE
What is a Competency Based Curriculum?
Following a systematic review of the literature on competency‐based education (CBE) Frank et al
(2010) came up with what they describe as a 21st century definition of CBE for medical education, a
definition highly transferable to any health professional discipline, including Midwifery:
Competency‐based education (CBE) is an approach to preparing physicians / (midwives) for
practice that is fundamentally oriented to graduate outcome abilities and organized around
competencies derived from an analysis of societal and patient needs. It deemphasizes time‐
based training and promotes greater accountability, flexibility, and learner centredness
(2010, 636).
Put simply, a CBE has as its goal student demonstration of learning and skill development through
assessment of successful performance. This contrasts with older style curricula which focus on the
teachers’ delivery of a syllabus with learning tested in a terminal examination. Outcome AND process
are both emphasised in a CB education or curriculum design, or as Harden et al suggest education for
capability (Harden, Crosby & Davis, 1999).
Background
The Competency Based Curriculum (CBC) has been the subject of wide interest since the 1950s but it
had a major push forward in 1978 when the World Health Organisation (WHO) released its paper
“Competency‐based Curriculum Development in Medical Education: an introduction” (WHO, 1978).
The focus of the CBE/CBC on graduate outcomes was a great challenge to the tradition curriculum
used in health professional education which had focused on knowledge acquisition rather than
practice ability. The move to competency based education, since the 1990s in particular, has been a
response to the realisation that the education of health professionals is an issue of public
accountability; a need to assure the public that graduates would not only have knowledge that could
be repeated in tests but had the skills that are fundamental public expectations of a health care
practitioner, i.e. safe and effective care. This required assessment of both the “knowing skills” and
the “doing” skills. Ideally this included an assessment of these skills in combination within the
complexity of the health care setting.
Most countries which have health professional regulatory authorities now require competency based
curricula for both programme accreditation and health professional registration, including the USA,
UK, Australia and New Zealand. As part of the accreditation of the programmes the authorities
expect to see evidence of the use of Objective Structured Clinical Assessments/Examination
(OSCA/OSCE) or their equivalent, and evidence of within‐training clinical experience and assessment.
The move to CBE/CBC has not been without controversy. Some criticised competency based
education as too reductionist and too mechanistic. They thought it focused on small independent
partial skills rather than accurately representing the complex decision‐making needed in practice.
This specific part‐task form of competency may be used in lower level technical education but is NOT
what is meant by the term “competency” when used in association with professional education. In
an attempt to distinguish between the two ways in which the word is used, the professional
competency is sometimes referred to as a “meta‐competency”. This “meta‐competency” refers to “a
The University of Sydney ‐ Commercial in Confidence Page 4 of 36
general ability to learn and apply competencies effectively in many different aspects of a person’s
activities” (Leung, 2002, 694), or the capability to perform complex work in multiple contexts, as is a
necessary skill for the graduate of any health professional programme.
The definition cited at the beginning of the chapter by Frank et al. suggests several core elements of
CBE: competency, societal and patient needs, a different notion of time‐based training,
accountability, flexibility, and learner centredness. Of these elements the International
Confederation of Midwives (ICM) suggests the learner centredness is the most important.
The learner must be engaged and active in all aspects of acquiring the knowledge, skills and
professional behaviors needed to demonstrate practice in a specific discipline. In other words,
competency‐based education uses teaching and learning strategies that facilitate the
development and demonstration of competency….Other common elements include the need
to have a clear, evidence‐based definition of the learning outcomes to be demonstrated for
performance of the professional role (i.e., the specific competencies) (ICM, 2012, 5).
In our 4 year midwifery curriculum the outcomes competencies that guide all elements of curriculum
design are those determined by the Ministry of Health in VietNam “No342/QD‐BYT Decision on
approval of Essential Competencies of Viet Nam Midwives” (MoH, 2014) (see appendix 1 or
abridged version). These competencies are taken directly from the ICM competencies with one small
addition indicated within the Appendix. These competencies are based in the answers to the two
questions: “What is a midwife expected to know?” and “What does a midwife do?” The competencies
are evidence‐based (ICM, 2010, 1).
“The basic essential elements consist of functional analysis of the occupational roles
(‘competencies’) into outcomes, and assessment of trainees’ progress in these outcomes on
the basis of demonstrated performance…. Assessments are based on a set of clearly defined
outcomes so that all parties concerned, including assessors and trainees, can make
reasonably objective judgements about whether or not each trainee has achieved them”
(Leung,2002,693).
The benefits of taking the outcome expectations from professional and public expectations of
professional behaviour (functional analysis) and testing them progressively and objectively to ensure
the graduate are able to practice as the public expects addresses the issue of public accountability. It
provides a transparent standard and also gives the educational institution flexibility on how to help
the students achieve these outcomes.
Another of the characteristics of CBE definition is that of a different notion of a “time‐based
curriculum”. This difference is summarised as the difference between a traditional curriculum which
had content delivered sequentially over a specified number of years with a terminal examination at
the end of that period; and a curriculum in which time relates much more specifically to the student’s
learning and how much time it takes for a student to demonstrate his or her learning. ICM suggests
the CB curriculum pays:
attention to the learning needs and patterns of adults, providing the time needed for the
learner to acquire and repeatedly perform or demonstrate the expected competencies
The University of Sydney ‐ Commercial in Confidence Page 5 of 36
(knowledge, skills, professional behaviours) and creating a supportive/enabling environment
for learning. All health professions have a societal mandate to provide needed services to the
public and therefore need to include social accountability in the educational process
(relevance, cost‐effectiveness, equity, and quality). Competency‐based education can be
pursued through various approaches to curricular design. Whatever the design, however, all
curricula need to be evidence‐based and outcome focused and all teaching strategies need to
be matched to their learning domain (psychomotor, cognitive and affective) (ICM, 2012, 5‐6).
Competency Based Teaching
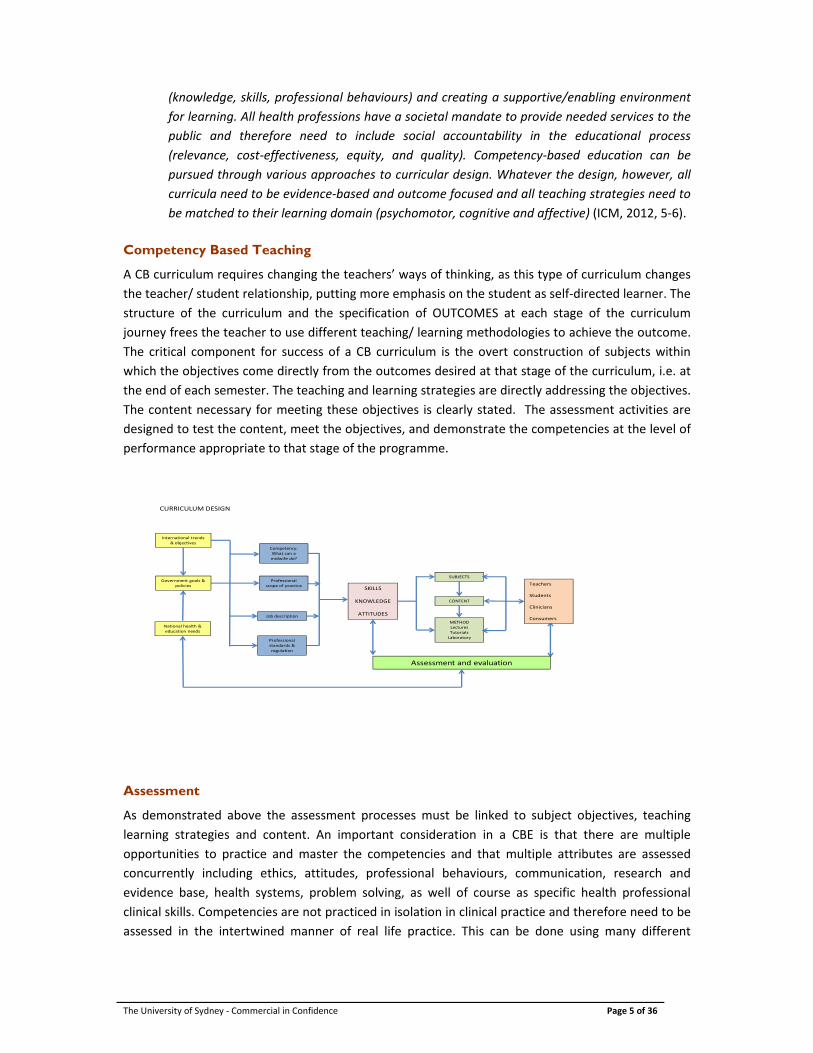
A CB curriculum requires changing the teachers’ ways of thinking, as this type of curriculum changes
the teacher/ student relationship, putting more emphasis on the student as self‐directed learner. The
structure of the curriculum and the specification of OUTCOMES at each stage of the curriculum
journey frees the teacher to use different teaching/ learning methodologies to achieve the outcome.
The critical component for success of a CB curriculum is the overt construction of subjects within
which the objectives come directly from the outcomes desired at that stage of the curriculum, i.e. at
the end of each semester. The teaching and learning strategies are directly addressing the objectives.
The content necessary for meeting these objectives is clearly stated. The assessment activities are
designed to test the content, meet the objectives, and demonstrate the competencies at the level of
performance appropriate to that stage of the programme.
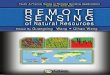
METHODLecturesTutorialsLaboratory
International trends & objectives
Government goals & policies
National health & education needs
Competency:What can a midwife do?
Professional scope of practice
Job description
Professional standards & regulation
SKILLS
KNOWLEDGE
ATTITUDES
SUBJECTS
CONTENT
Teachers
Students
Clinicians
Consumers
Assessment and evaluation
CURRICULUM DESIGN
Assessment
As demonstrated above the assessment processes must be linked to subject objectives, teaching
learning strategies and content. An important consideration in a CBE is that there are multiple
opportunities to practice and master the competencies and that multiple attributes are assessed
concurrently including ethics, attitudes, professional behaviours, communication, research and
evidence base, health systems, problem solving, as well of course as specific health professional
clinical skills. Competencies are not practiced in isolation in clinical practice and therefore need to be
assessed in the intertwined manner of real life practice. This can be done using many different
The University of Sydney ‐ Commercial in Confidence Page 6 of 36
assessment strategies such as the use of simulated patients. Such assessment is always to a standard
which must be known and transparent.
Competency based curricula do not usually have examinations at the end of the programme which
purports to test everything across the curriculum. The learning is assessed throughout a semester
and a grade given at the end of each semester. This learning is then the scaffold on which the next
semester’s learning rests. The learning spirals throughout the programme becoming more complex
and akin to practice as expected of a graduate.
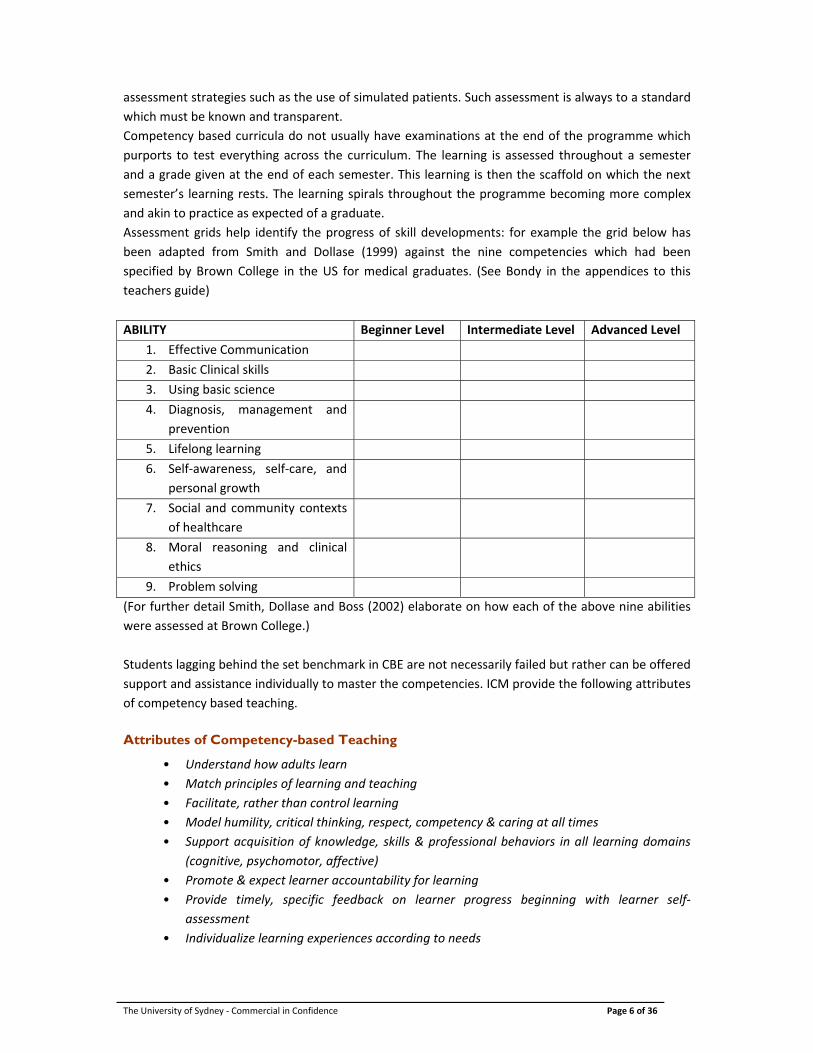
Assessment grids help identify the progress of skill developments: for example the grid below has
been adapted from Smith and Dollase (1999) against the nine competencies which had been
specified by Brown College in the US for medical graduates. (See Bondy in the appendices to this
teachers guide)
ABILITY Beginner Level Intermediate Level Advanced Level
1. Effective Communication
2. Basic Clinical skills
3. Using basic science
4. Diagnosis, management and
prevention
5. Lifelong learning
6. Self‐awareness, self‐care, and
personal growth
7. Social and community contexts
of healthcare
8. Moral reasoning and clinical
ethics
9. Problem solving
(For further detail Smith, Dollase and Boss (2002) elaborate on how each of the above nine abilities
were assessed at Brown College.)
Students lagging behind the set benchmark in CBE are not necessarily failed but rather can be offered
support and assistance individually to master the competencies. ICM provide the following attributes
of competency based teaching.
Attributes of Competency-based Teaching
• Understand how adults learn
• Match principles of learning and teaching
• Facilitate, rather than control learning
• Model humility, critical thinking, respect, competency & caring at all times
• Support acquisition of knowledge, skills & professional behaviors in all learning domains
(cognitive, psychomotor, affective)
• Promote & expect learner accountability for learning
• Provide timely, specific feedback on learner progress beginning with learner self‐
assessment
• Individualize learning experiences according to needs
The University of Sydney ‐ Commercial in Confidence Page 7 of 36
• Expect increasing complexity of performance as the learner progresses throughout the
programme (ICM, 2012, 6)
The CBC can appear much more simple to achieve than is the case in practice. There are critical
elements to ensuring that students can perform in the real world situation that may not have been
thought about in the tradition curriculum where knowledge is imparted and then the student
graduates prior to moving into practice. The CBC requires integration of theory and practice in a very
structured and coordinated way. It requires the planning and execution of a clinical programme for
each student and across multiple settings. This mandates a different imbedded relationship with
health care providers and the supervision and clinical teaching of students by professionals who are
committed to the curriculum and knowledgeable about it. These clinical teachers must also be skilled
in assessing students in practice against the competency standards.
“practice‐based learning requires direct supervision and multiple opportunities for the
learners to demonstrate their competency in practice over a period of time. Often midwifery
programmes will have a set minimum number of practical experiences mandated by the
regulatory authority in the country in order to graduate/complete the educational offering.
Completing this minimum number of experiences is not, however, a guarantee of competent
practice. Adults learn at different rates and in different ways, so 20 attended births may be
sufficient for one learner to demonstrate a safe beginning level of performance of this skill
while another will require 50 births to meet the same learning outcome. This is the primary
reason why competency‐based education must include direct observation of competency
demonstration over time. There is also value in observing learner’s provision of midwifery
care in a variety of settings and types of clients to move the learner’s critical thinking and
reasons skills beyond a single approach to midwifery care (ICM, 2012, 10‐11).
The expected outcome competencies and their breakdown by learning components are provided for
this curriculum in the Midwifery Clinical Practice Record Book and the skills to be assessed are
specified within the subject outlines of the “Four Year Bachelor Level Programme in Midwifery”
curriculum document.
Importance for the Student
The relationship of the student to both the learning and the teacher is therefore also different in CBE.
The students MUST be active participants in their own learning and act as adults. They are not able to
be passive observers, but must be able to perform, as well as observe, reflect, think critically and
act. This is learning by mastery and sequential building through the curriculum over time. This is a
long way away from the old medical education adage of “see one; do one; teach one”. ICM suggests
the following as defining attributes of such a CBE.
Defining Attributes of Competency‐Based Learning
Understand how one learns best (style)
Understand exactly what is expected outcome(s) of learning
Take responsibility for one’s learning
Motivated to learn – goal oriented
Ethical person and practitioner
Critical thinker
The University of Sydney ‐ Commercial in Confidence Page 8 of 36
Self‐assess learning & performance
Commitment to ongoing learning (ICM, 2012, 8‐9).
The University of Sydney ‐ Commercial in Confidence Page 9 of 36
The Competency Based Curriculum
The University of Sydney ‐ Commercial in Confidence Page 10 of 36
Contents
Purpose ........................................................................................................................................ 10
Link with the Curriculum ............................................................................................................. 10
Design of Chapters ...................................................................................................................... 10
How was the curriculum developed ............................................................................................ 11
How to Integrate Curriculum Themes in Teaching...................................................................... 13
Teaching and Learning Strategies ............................................................................................... 14
Motivation to Learn ..................................................................................................................... 16
Key Assumptions About Learning ................................................................................................ 16
Principles of Adult Learning ........................................................................................................ 17
Traditional Methods of Teaching and Active teaching Methods ................................................ 18
Engaging the Student .................................................................................................................. 19
Blooms Taxonomy ....................................................................................................................... 20
Learning Outcome Statements ................................................................................................... 22
Questions in the Classroom ......................................................................................................... 22
Lesson Plan .................................................................................................................................. 25
Cinical Experience ........................................................................................................................ 27
Feedback ..................................................................................................................................... 28
Teaching Resources ..................................................................................................................... 28
Conclusion ................................................................................................................................... 32
Reflective Activites ...................................................................................................................... 32
References ................................................................................................................................... 34
Appendix A .................................................................................................................................. 35

The University of Sydney ‐ Commercial in Confidence Page 11 of 36
Purpose
The purpose of this chapter is to provide the teacher with a guide to the use of the textbook, to
provide guidance in the development and use of teaching materials, to review assessment of student
learning and to suggest ways of supporting students in their learning. This chapter is included in the
textbook for both teachers and students to read to emphasise the relationship between teaching and
learning.
Like all textbooks, this one has some limitations. Like all textbooks, the material in it will become
outdated in a few years. This is one of the reasons that that the use of current evidence is
encouraged. Another limitation is that it is written for a variety of settings, and midwives must learn
to apply the principles of good practice in any setting that they work in.
It is designed for use in the three‐year and four year curricula for the training of midwives in the
Vietnamese context. For this reason, the textbook must be used in conjunction with the national
guidelines. It does cite evidence from international research, and this may in some instances appear
to conflict with local guidelines. The teacher has a significant role in assisting the student to
understand why this may appear to be so, and to reduce their confusion at the same time as
ensuring they develop an enquiring and critical approach to their learning.
Link with curriculum
The curriculum themes are embedded through the text. In much the same way as the pattern in a
woven cloth reveals its pattern as the weaver intertwines the threads, the students’ understanding
and awareness of themes will be developed with the skill of the teacher. The five themes of the
curriculum: primary health care, evidence based practice, communication, cultural awareness and
respect and woman centred care are all addressed in the text. The teacher’s role is to ensure that the
student sees the links between these themes and the subject matter as well as developing the
knowledge, skills and attributes essential for the safe practice of midwifery.
Design of the chapters
Each chapter is presented in a similar format to help the reader move from simple understanding to
more complex analysis. Headings guide the reader throughout. The questions and points for
reflection at the end of each chapter are not meant to be assessment of learning, but are designed to
encourage the student to evaluate their engagement with the material. Students should be
discouraged from viewing the questions as ‘sample examination’ questions for this reason.
The references listed are not by any means exhaustive. Both the teacher and the student should seek
the most recent evidence from the international literature, and use sources available on the internet
wisely.
A limitation of the txt is that while written to meet current international midwifery standards, it will
not capture the nuances of Vietnamese culture and context because it has not been written by
Vietnamese experts. It is imperative for the cultural safety of women and students that the
academics who will use the book and teach the subjects are able to add this dimension.
The University of Sydney ‐ Commercial in Confidence Page 12 of 36
An important feature of the text is that it must be used in conjunction with the local guidelines. This
means that the teacher must always be aware of the most recent changes to directives and policies
and bring these to the attention of the student.
The four‐year midwifery curriculum will provide a number of challenges to teachers and students.
This chapter will provide some ways in which teachers might be able to develop their own skills in
order to teach this curriculum more effectively.
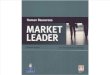
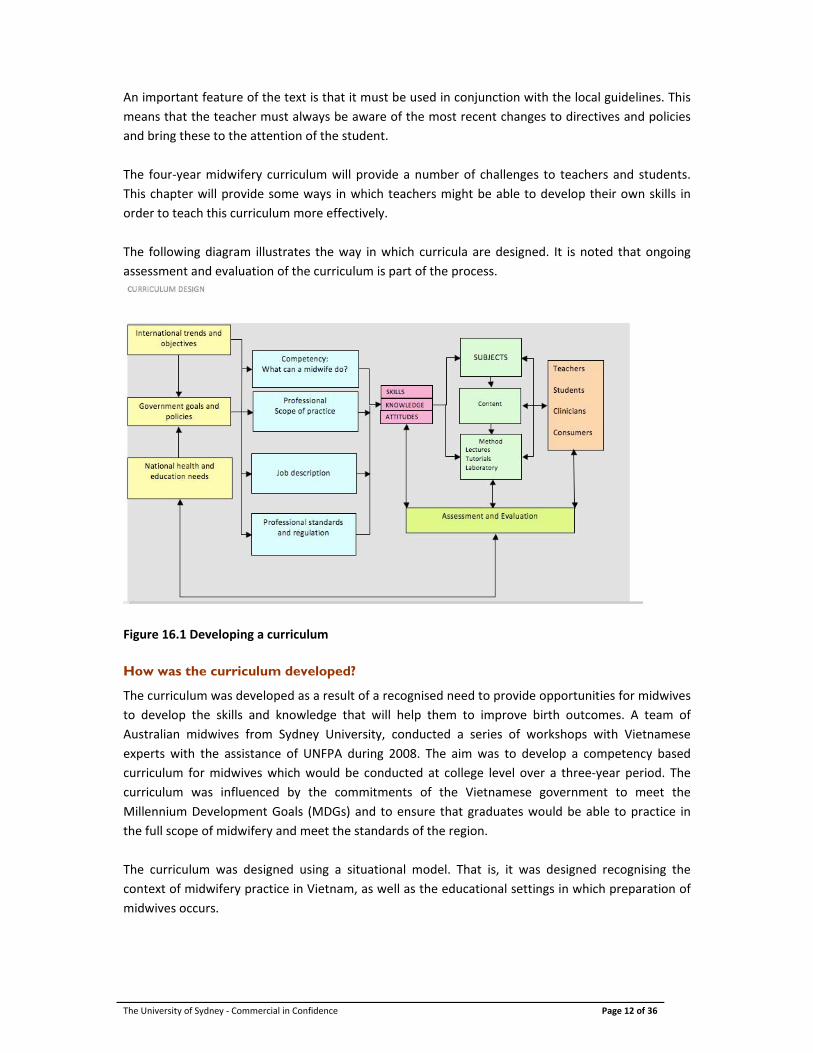
The following diagram illustrates the way in which curricula are designed. It is noted that ongoing
assessment and evaluation of the curriculum is part of the process.
Figure 16.1 Developing a curriculum
How was the curriculum developed?
The curriculum was developed as a result of a recognised need to provide opportunities for midwives
to develop the skills and knowledge that will help them to improve birth outcomes. A team of
Australian midwives from Sydney University, conducted a series of workshops with Vietnamese
experts with the assistance of UNFPA during 2008. The aim was to develop a competency based
curriculum for midwives which would be conducted at college level over a three‐year period. The
curriculum was influenced by the commitments of the Vietnamese government to meet the
Millennium Development Goals (MDGs) and to ensure that graduates would be able to practice in
the full scope of midwifery and meet the standards of the region.
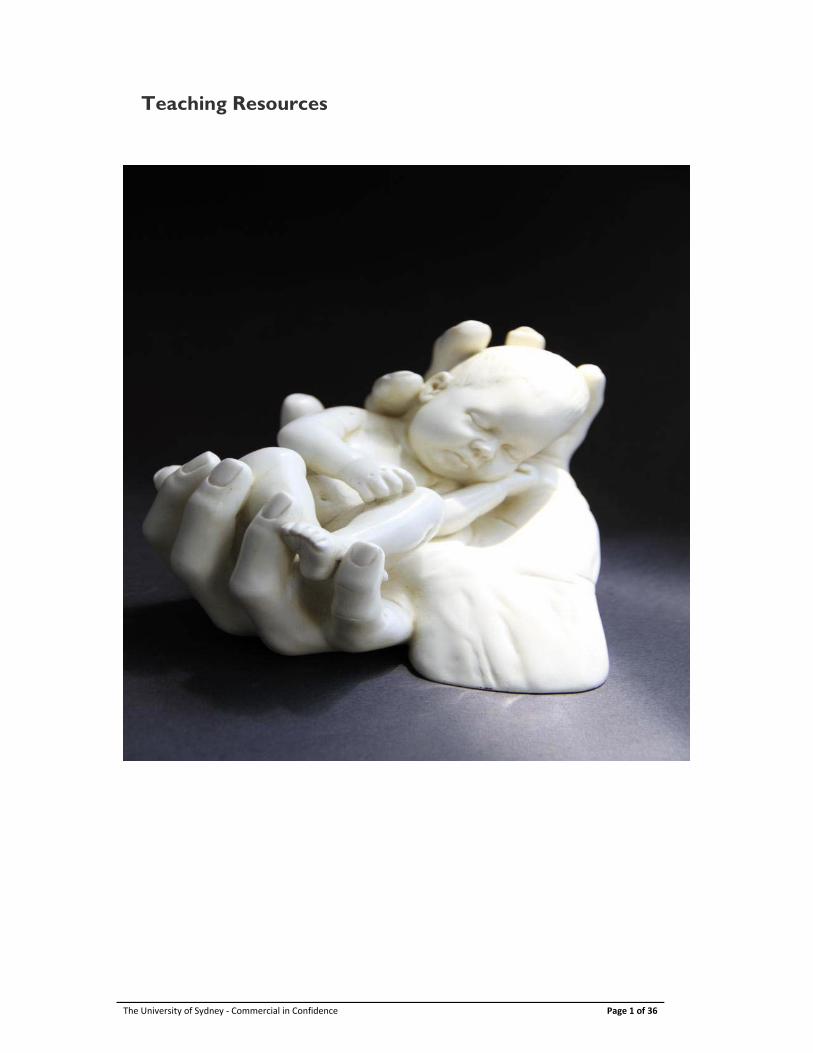
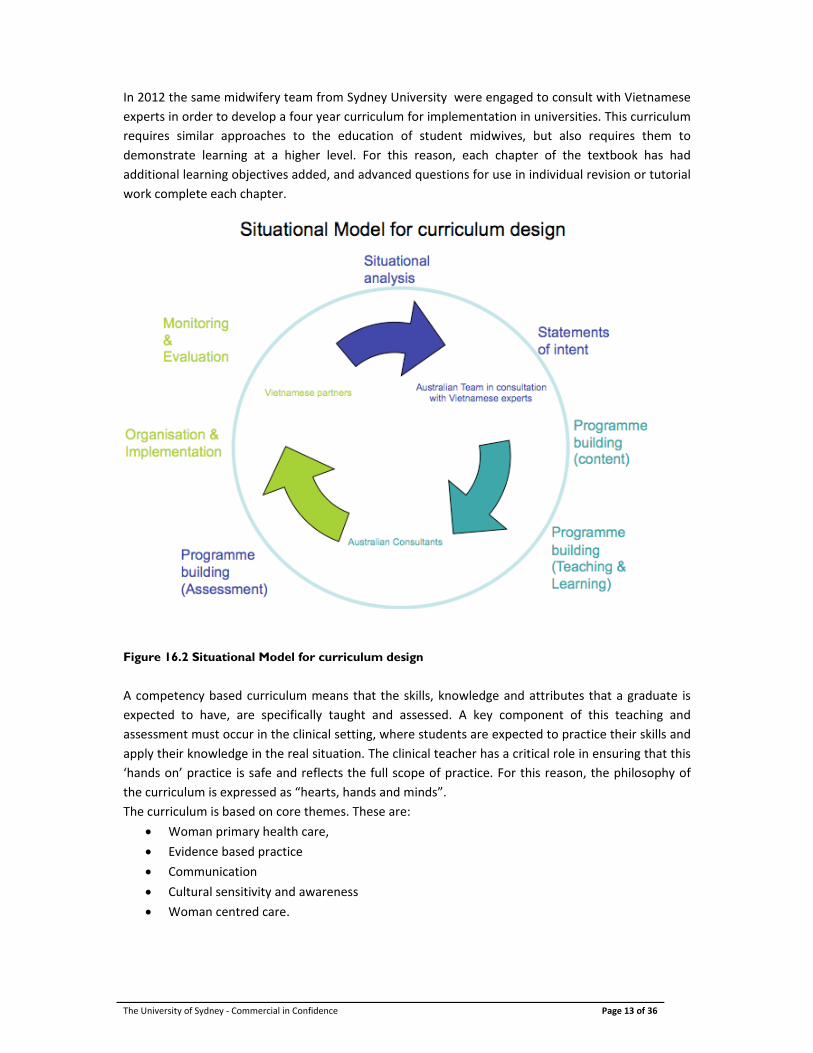
The curriculum was designed using a situational model. That is, it was designed recognising the
context of midwifery practice in Vietnam, as well as the educational settings in which preparation of
midwives occurs.
The University of Sydney ‐ Commercial in Confidence Page 13 of 36
In 2012 the same midwifery team from Sydney University were engaged to consult with Vietnamese
experts in order to develop a four year curriculum for implementation in universities. This curriculum
requires similar approaches to the education of student midwives, but also requires them to
demonstrate learning at a higher level. For this reason, each chapter of the textbook has had
additional learning objectives added, and advanced questions for use in individual revision or tutorial
work complete each chapter.
Figure 16.2 Situational Model for curriculum design
A competency based curriculum means that the skills, knowledge and attributes that a graduate is
expected to have, are specifically taught and assessed. A key component of this teaching and
assessment must occur in the clinical setting, where students are expected to practice their skills and
apply their knowledge in the real situation. The clinical teacher has a critical role in ensuring that this
‘hands on’ practice is safe and reflects the full scope of practice. For this reason, the philosophy of
the curriculum is expressed as “hearts, hands and minds”.
The curriculum is based on core themes. These are:
Woman primary health care,
Evidence based practice
Communication
Cultural sensitivity and awareness
Woman centred care.
The University of Sydney ‐ Commercial in Confidence Page 14 of 36
These were developed during the workshops and reflect the purpose of the new curriculum – to
develop midwives who can provide the best and safest care to women and their babies in Vietnam.
Curriculum Implementation
Teachers will need to work with their colleagues to implement the curriculum which involves
determining who will teach which subjects, as well as the teaching methods to be employed and the
lesson plans for each session.
In subjects where teaching is provided by lecturers with specific expertise outside midwifery practice,
it is essential that they are briefed as to where the emphasis should be placed for safe midwifery
practice.
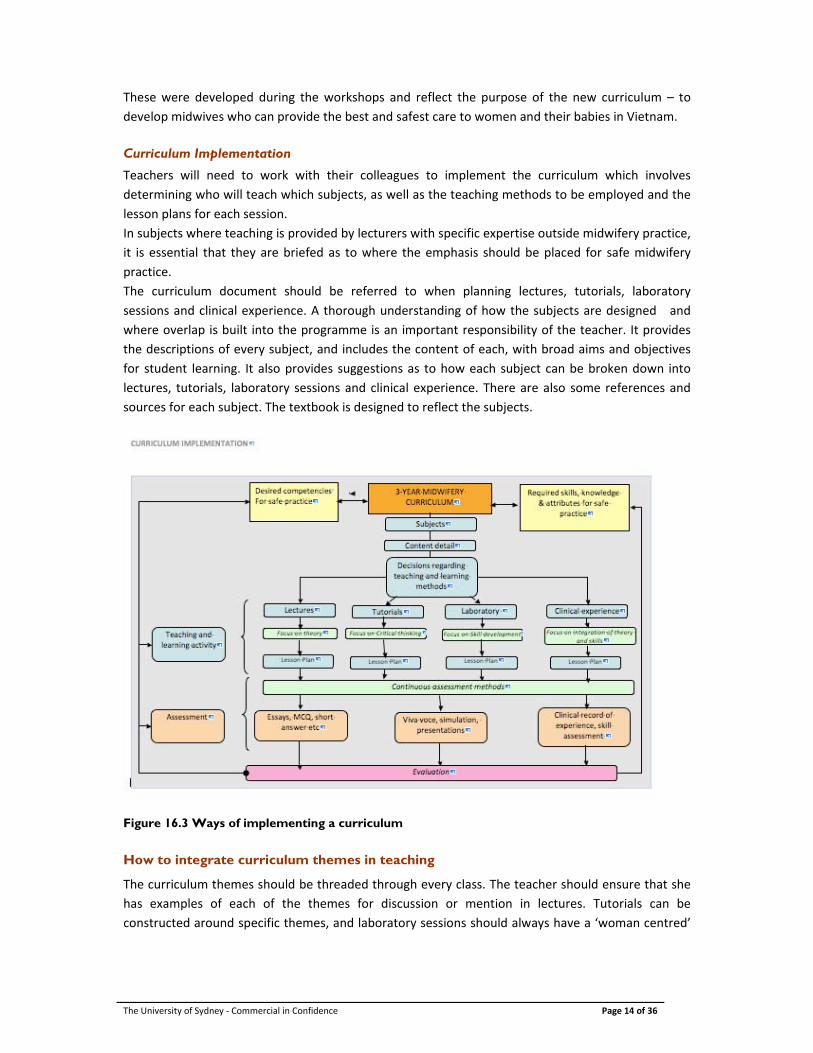
The curriculum document should be referred to when planning lectures, tutorials, laboratory
sessions and clinical experience. A thorough understanding of how the subjects are designed and
where overlap is built into the programme is an important responsibility of the teacher. It provides
the descriptions of every subject, and includes the content of each, with broad aims and objectives
for student learning. It also provides suggestions as to how each subject can be broken down into
lectures, tutorials, laboratory sessions and clinical experience. There are also some references and
sources for each subject. The textbook is designed to reflect the subjects.
Figure 16.3 Ways of implementing a curriculum
How to integrate curriculum themes in teaching
The curriculum themes should be threaded through every class. The teacher should ensure that she
has examples of each of the themes for discussion or mention in lectures. Tutorials can be
constructed around specific themes, and laboratory sessions should always have a ‘woman centred’
The University of Sydney ‐ Commercial in Confidence Page 15 of 36
focus. The teacher can also ask questions in the classroom, and marking criteria should include
recognition of the themes whenever possible.
It is important to make the themes as explicit as possible because they shape midwifery practice.
Teaching and learning strategies
Learning styles
Most adults have a preferred learning style and this influences the way in which they engage with
new information. One model for describing learning styles relates to the individual’s visual, auditory
and kinetic learning preferences. (VAK).
Visual learners are most comfortable when they see things being demonstrated or can read about it
or see pictures of it. They relate to information they get through their sense of sight. In the
classroom, this student may be the one reading the textbook while the teacher is explaining
something, or drawing and writing copious notes. Often they enjoy films, extra readings and
observing someone demonstrating a skill.
Auditory learners prefer to learn through hearing about things, having concepts explained and being
able to ask questions. They use their sense of hearing to gain understanding. This kind of learner will
enjoy lectures, listening to recordings and having the opportunity to ask questions.
Kinetic learners have to do and experience things in order to learn. They are sometimes restless in
class, and will enjoy laboratory sessions and clinical practice sessions. Touch and activity are very
important to these learners.
In reality most of us learn through a combination of styles. The implication for this as teachers is that
all teaching and learning activities should be designed to appeal to all of the preferred learning styles.
Lectures that are a recitation of written notes are not stimulating to anyone. The use of visual media
is critical, but also each class needs some kind of activity built into it in order to make it interesting.
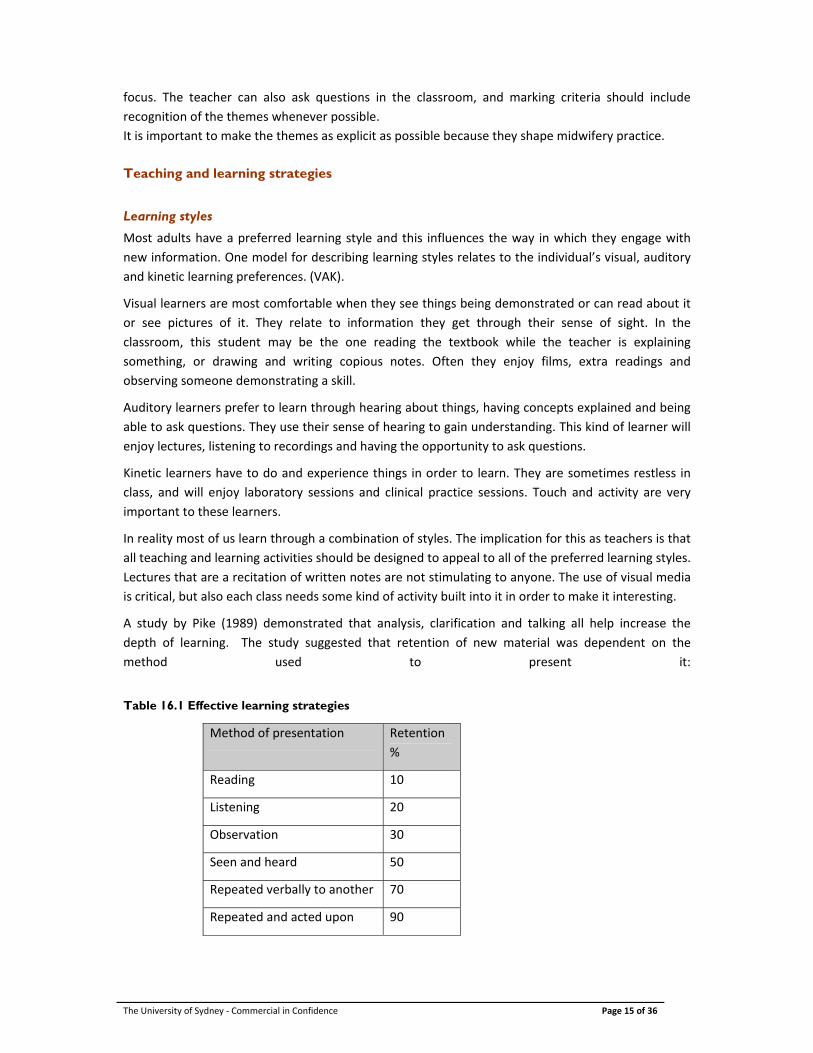
A study by Pike (1989) demonstrated that analysis, clarification and talking all help increase the
depth of learning. The study suggested that retention of new material was dependent on the
method used to present it:
Table 16.1 Effective learning strategies
Method of presentation Retention
%
Reading 10
Listening 20
Observation 30
Seen and heard 50
Repeated verbally to another 70
Repeated and acted upon 90
The University of Sydney ‐ Commercial in Confidence Page 16 of 36
This study supports the idea that the more actively engaged the learner is – especially though
discussing and practicing (saying and doing) the material – the more effective their learning will be.
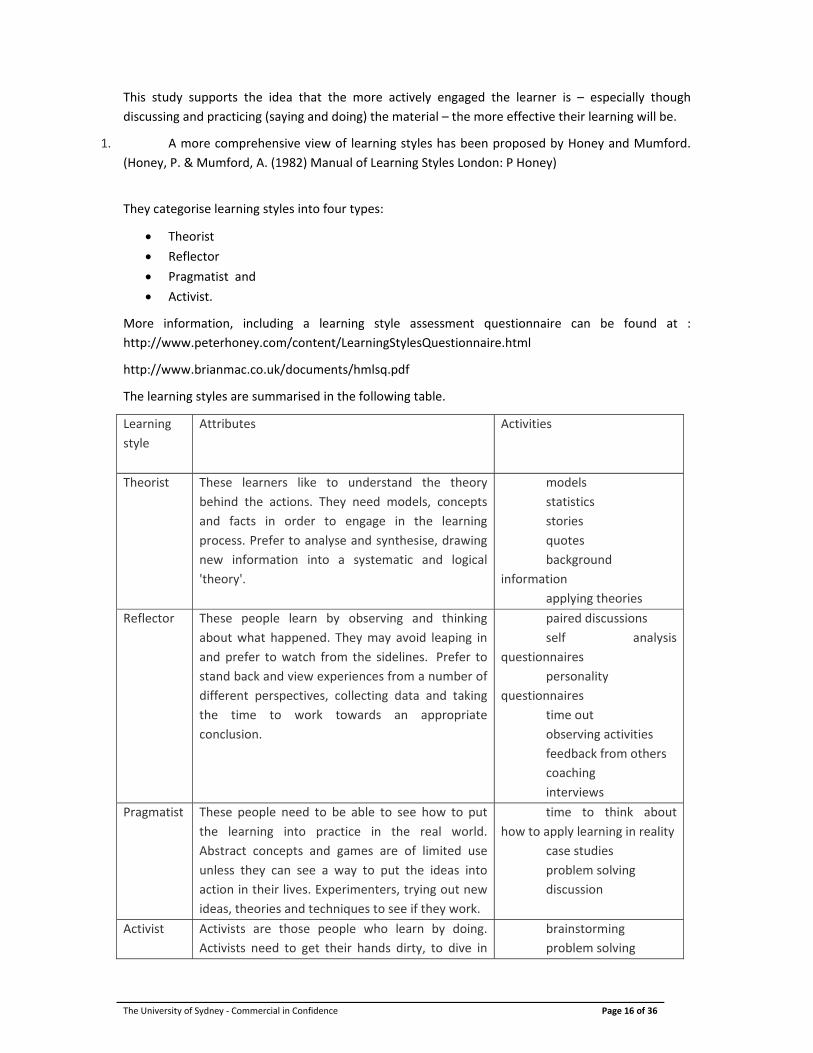
1. A more comprehensive view of learning styles has been proposed by Honey and Mumford.
(Honey, P. & Mumford, A. (1982) Manual of Learning Styles London: P Honey)
They categorise learning styles into four types:
Theorist
Reflector
Pragmatist and
Activist.
More information, including a learning style assessment questionnaire can be found at :
http://www.peterhoney.com/content/LearningStylesQuestionnaire.html
http://www.brianmac.co.uk/documents/hmlsq.pdf
The learning styles are summarised in the following table.
Learning
style
Attributes Activities
Theorist These learners like to understand the theory
behind the actions. They need models, concepts
and facts in order to engage in the learning
process. Prefer to analyse and synthesise, drawing
new information into a systematic and logical
'theory'.
models
statistics
stories
quotes
background
information
applying theories
Reflector These people learn by observing and thinking
about what happened. They may avoid leaping in
and prefer to watch from the sidelines. Prefer to
stand back and view experiences from a number of
different perspectives, collecting data and taking
the time to work towards an appropriate
conclusion.
paired discussions
self analysis
questionnaires
personality
questionnaires
time out
observing activities
feedback from others
coaching
interviews
Pragmatist These people need to be able to see how to put
the learning into practice in the real world.
Abstract concepts and games are of limited use
unless they can see a way to put the ideas into
action in their lives. Experimenters, trying out new
ideas, theories and techniques to see if they work.
time to think about
how to apply learning in reality
case studies
problem solving
discussion
Activist Activists are those people who learn by doing.
Activists need to get their hands dirty, to dive in
brainstorming
problem solving
The University of Sydney ‐ Commercial in Confidence Page 17 of 36
with both feet first. Have an open‐minded
approach to learning, involving themselves fully
and without bias in new experiences.
group discussion
puzzles
competitions
role‐play
Source
http://www2.le.ac.uk/departments/gradschool/training/eresources/teaching/theories/honey‐
mumford
Motivation to learn
The motivation of individuals to learn depends on them. They can be either externally or internally
motivated. External motivation occurs when some outside agent – the threat of punishment or
promise of reward, drives them to learn. Internal motivation occurs when the individual has their
own internal driver – they want to learn. The teacher can use an examination as an external
motivator, as the student will know failure is a likely consequence if they do not learn the material. It
is the fear of failure that motivates the student to study. Internal motivation is evident when the
student is engaged in the learning because he wants to understand and use the knowledge for
reasons other than just passing the test.
In order for teachers to encourage internal motivation, a number of strategies are useful. The
student will be more likely to be motivated if they see the relevance of material being taught. The
teacher can do this though the use of examples. Case studies are very useful as are clinical pictures
and stories from practice.
One of the most important things a teacher can do to motivate students is to be clear about the
expected learning outcomes of a subject, use a variety of teaching methods and encourage students
to be active learners in a safe learning environment. A safe learning environment refers to more than
physical safety, which of course is important. A safe learning environment is one in which the student
feels that their learning is important, that they are respected in terms of their learning needs, that
they can set their own goals and that they can ask questions without being embarrassed or made to
feel foolish. The role of the teacher in providing such a learning environment is very important. If the
teacher is unwilling to answer questions, is unable to admit they do not know the answer
themselves, or ignores some students while favouring others, students will not be actively engaged in
learningl. It should be remembered that the risk of embarrassment is not one many adults are willing
to take. If the teacher asks questions and seeks questions from students, if she is open in admitting
when she does not know the answer, if all students are included in discussions and communication is
open, students are more likely to engage in the lessons and learn more actively.
There are many theories of learning, A useful website is http://www.learning‐theories.com/
Key assumptions about learning
Everyone has the potential to learn – age and intellectual capacity influence this
Stress and confusion are natural responses to new situations, and high levels of these
interfere with learning.
Adults retain different amounts according to the method used to learn
Formal teaching forms only one part of learning – experience forms the greater part
There is no learning without motivation – this can be internal or external.
The University of Sydney ‐ Commercial in Confidence Page 18 of 36
Feedback helps shape learning and the closer the feedback is (in time) to the experience,
the more effective it will be
Learning occurs at both superficial and deep levels
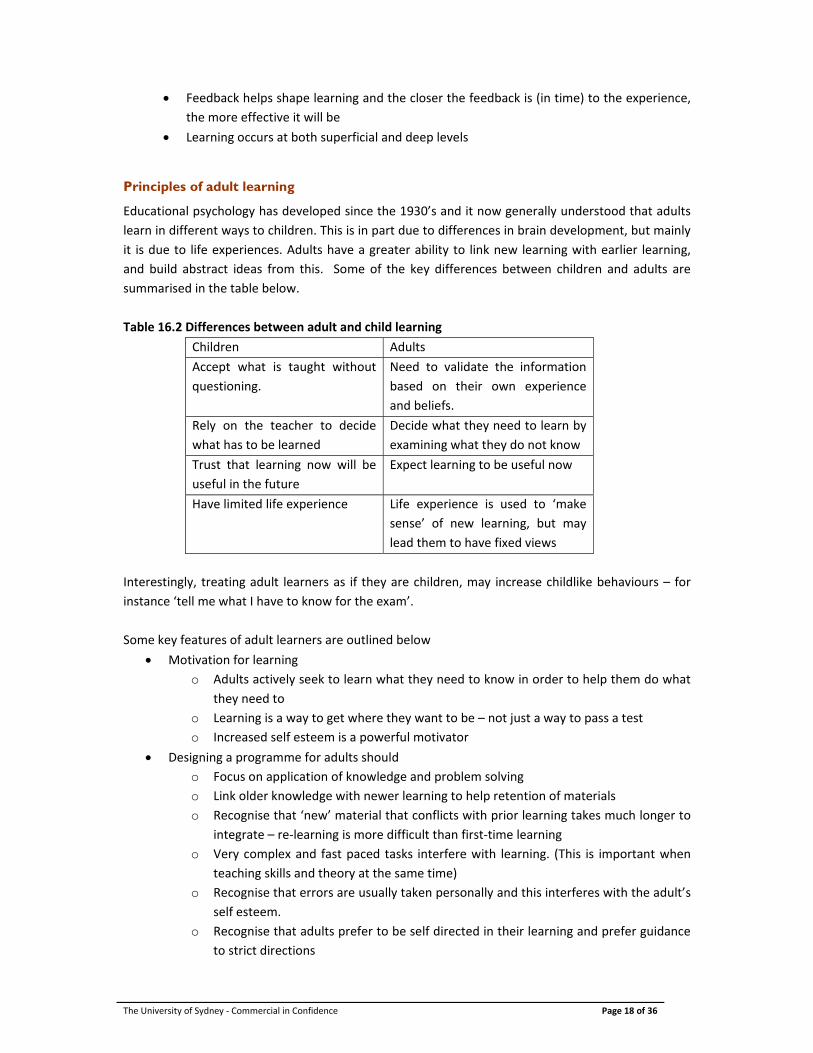
Principles of adult learning
Educational psychology has developed since the 1930’s and it now generally understood that adults
learn in different ways to children. This is in part due to differences in brain development, but mainly
it is due to life experiences. Adults have a greater ability to link new learning with earlier learning,
and build abstract ideas from this. Some of the key differences between children and adults are
summarised in the table below.
Table 16.2 Differences between adult and child learning
Children Adults
Accept what is taught without
questioning.
Need to validate the information
based on their own experience
and beliefs.
Rely on the teacher to decide
what has to be learned
Decide what they need to learn by
examining what they do not know
Trust that learning now will be
useful in the future
Expect learning to be useful now
Have limited life experience Life experience is used to ‘make
sense’ of new learning, but may
lead them to have fixed views
Interestingly, treating adult learners as if they are children, may increase childlike behaviours – for
instance ‘tell me what I have to know for the exam’.
Some key features of adult learners are outlined below
Motivation for learning
o Adults actively seek to learn what they need to know in order to help them do what
they need to
o Learning is a way to get where they want to be – not just a way to pass a test
o Increased self esteem is a powerful motivator
Designing a programme for adults should
o Focus on application of knowledge and problem solving
o Link older knowledge with newer learning to help retention of materials
o Recognise that ‘new’ material that conflicts with prior learning takes much longer to
integrate – re‐learning is more difficult than first‐time learning
o Very complex and fast paced tasks interfere with learning. (This is important when
teaching skills and theory at the same time)
o Recognise that errors are usually taken personally and this interferes with the adult’s
self esteem.
o Recognise that adults prefer to be self directed in their learning and prefer guidance
to strict directions

The University of Sydney ‐ Commercial in Confidence Page 19 of 36
Classrooms for adults
o Embarrassment is a risk most adults will not take
o Physical comfort is important
o Shared experience is a rich source of learning – teachers must facilitate this
o New knowledge must be linked to previously learnt material
o Practice (repetition) is important, especially when there is feedback given
o Adults have differing learning styles and preferences – the teacher should design
sessions to cater for these
o Active learning occurs where there is opportunity for reflection, analysis and
discussion
Things to remember when teaching adults
Recognise the experience that each learner brings to the situation
Adults have beliefs and values and established opinions – these should be appreciated
Adults learn differently to children
Adults need frequent breaks
Adults have pride and avoid embarrassment
Adults need to be self directing
Adults tend to be problem oriented
Adults are social beings – they like to spend time together,
Traditional methods of teaching and active teaching methods
Traditional methods of teaching see the teacher as the controller of the classroom and all that goes
on it. The teacher is seen as the holder of all knowledge, and his task is to fill the student with that
knowledge. The lecture is the traditional teaching method, where the teacher speaks, perhaps with
the use of PowerPoint presentations or diagrams, and the student listens and takes notes. This one‐
way traffic of information is not the most effective way for adults to learn, given that we know that
as little as 20% of this information will be retained. The use of the traditional approach requires a
high degree of compliance from students, and classrooms are often silent apart from the voice of the
lecturer.
The lecture does have a useful place though. It can provide a framework or outline of the key ideas,
and can use examples to make the subject matter relevant and interesting. It is also a convenient
way of addressing large numbers of students at the same time and ensuring that all have the same
information. It is relatively time and resource efficient, and large amounts of information can be
presented.
Active teaching methods engage the learner in a different way. They encourage the learner to
examine and analyse ideas, find their own examples to support them and to discuss these with their
peers and teachers. Reflection on experience is a key component of active learning.
Active learning occurs when the learner tries to build links between what they already know and
what is new material. This is done through exploring the material to see what is the same or similar
to previous learning. Knowledge that is similar is rapidly absorbed because it builds on previous
learning. Material that does not obviously overlap with existing knowledge takes longer to absorb,
but may engage the learner at a deeper level as they try to resolve what they thought they knew
with the new information.
The University of Sydney ‐ Commercial in Confidence Page 20 of 36
For this reason, the teacher needs to make obvious any links when presenting new material, but also
must recognise that not all students learn uniformly. It is also important for the teacher to be aware
that it is difficult for large groups to learn from each other, and that small group work allows
students to test our ideas and build more active links with previous learning.
The most effective active learning occurs when the student asks questions of himself and others that
allows for clarification and application. Such active learning is more likely to result in deep, rather
than superficial learning, meaning that the student will not rely just on recall of facts, but will be able
to apply knowledge to a variety of different situations.
Superficial learning is concerned with recall and possibly rearrangement of facts. It relates only to
knowledge – and is often motivated by the need to be able to recall information for examinations. It
relies heavily on memorisation. Deeper learning relates to the ability to apply knowledge, analyse
facts and think critically. For deep learning to occur, the learner must understand concepts and
principles and be able to apply them. It is significant not just in that the student can problem solve,
but also because the learning has greater permanence. Most students will begin their learning in a
subject by memorisation and repetition, but effective teachers will encourage them towards deeper
level learning. Active teaching methods aim to do this.
Active teaching methods include the use of case studies, problem solving, small group discussion and
questioning techniques. As a result, classrooms where active teaching occurs are noisier and the
transfer of knowledge is a two‐way process.
Teachers who have used the traditional method will need to develop a new set of skills if they are to
have ‘active’ classrooms. These are mainly to develop ways in which the students can interact with
the teacher, each other and the material. The learners become more active – through discussions,
through classroom activities and through problem solving. Teachers need to put more emphasis on
the student engaging in the material being presented, and less on formal power relationships. This
may involve looking at the way they teach with a critical eye, and seeking the experience of their
colleagues to help them develop the skills required. They also need to be prepared to answer the
students questions and to encourage their students to ask challenging questions.
Engaging the student
As adult learners students need to see the relevance of what they are learning. Ways of encouraging
this are to:
Use case studies to illustrate the importance of the theory being taught
Present a series of clinical problems relevant to practice
Use structured role play
Ask probing questions that help the students explore different aspects of the topic
Provide demonstrations
Provide hands on simulated or real practice
Develop a classroom relationship with students in which they feel safe to offer an opinion or
attempt to answer questions when they are not confident that they have the correct answer.
The teacher needs to be careful to avoid making the student feel embarrassed if they are
incorrect.
Small group work is an important tool in engaging students

The University of Sydney ‐ Commercial in Confidence Page 21 of 36
Blooms Taxonomy
Bloom’s work helps to illustrate that knowledge has a number of levels. These are hierarchical,
ranging from simple recall to synthesis of new ideas.
Benjamin Bloom developed a method for categorising the level of abstraction in educational settings.
It is useful because it helps to write objectives and questions at various levels – from simple recall of
information to integration of ideas. At the lower levels, students rely on recall of facts, and at the
higher levels, students are able to use what they have learnt to solve problems. Ideally we want
students to develop problem‐solving skills and to be able to use their knowledge in a variety of
settings. The taxonomy helps to provide a framework to write objectives and questions that guide
and test the student at a variety of levels. Questions written to test the higher orders of learning
should help to identify the students who are most able to use what they have learnt in a meaningful
way.
Domains
There are three domains of learning. These are:
Cognitive ‐ what is known
Affective ‐ what is felt and or thought
Psychomotor ‐ what the learner can physically do
Within each domain there is a hierarchy, that is an ordering from simple to complex.
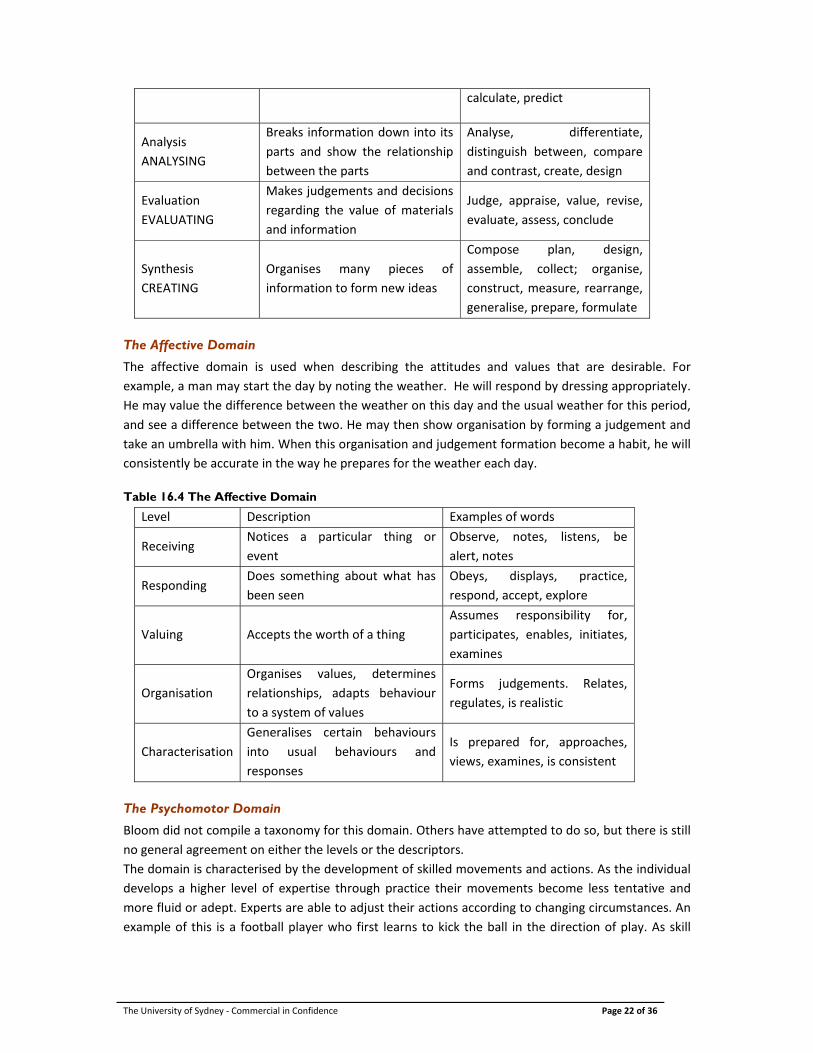
Cognitive domain
There are 6 levels in this domain. In the table below, the level is accompanied by examples of the
words that may be used when writing objectives or questions. These are arranged from lower order
to higher order. Each level builds on the previous level. An example of development in the cognitive
domain is the learning of a second language. At knowledge level, the learner can make a list of words
in the new language. At comprehension the learner may be able to recognise two different words for
flowers (orchid and blossom) as both belonging to a category of flower. At application level they can
apply their knowledge to have a simple conversation, or translate a written passage. At analysis level,
they would be able to critique a written passage. At synthesis they would be able to express complex
ideas in the language. At evaluation level they would be able to evaluate by judging someone else’s
skill in the language. In the 1990’s, Bloom’s taxonomy was revised by Anderson, and the top two tiers
have been swapped. Now the highest level is called creating and the level immediately below is
evaluating.
Table 16.3 The six levels of cognitive domain in Blooms taxonomy
Level Description Examples of words
Knowledge
REMEMBERING
Recall of specific information or
facts
List, repeat, tell, review,
define, collect
Comprehension
UNDERSTANDING
Can recall AND use the recalled
information in a different way,
understanding of subject, can
predict consequences
Discuss, describe, recognise,
identify, locate, explain
Application
APPLYING
Uses abstract information and
applies to a concrete situation
Apply, interpret, use, illustrate,
examine, solve, demonstrate,
The University of Sydney ‐ Commercial in Confidence Page 22 of 36
calculate, predict
Analysis
ANALYSING
Breaks information down into its
parts and show the relationship
between the parts
Analyse, differentiate,
distinguish between, compare
and contrast, create, design
Evaluation
EVALUATING
Makes judgements and decisions
regarding the value of materials
and information
Judge, appraise, value, revise,
evaluate, assess, conclude
Synthesis
CREATING
Organises many pieces of
information to form new ideas
Compose plan, design,
assemble, collect; organise,
construct, measure, rearrange,
generalise, prepare, formulate
The Affective Domain
The affective domain is used when describing the attitudes and values that are desirable. For
example, a man may start the day by noting the weather. He will respond by dressing appropriately.
He may value the difference between the weather on this day and the usual weather for this period,
and see a difference between the two. He may then show organisation by forming a judgement and
take an umbrella with him. When this organisation and judgement formation become a habit, he will
consistently be accurate in the way he prepares for the weather each day. Table 16.4 The Affective Domain
Level Description Examples of words
Receiving Notices a particular thing or
event
Observe, notes, listens, be
alert, notes
Responding Does something about what has
been seen
Obeys, displays, practice,
respond, accept, explore
Valuing Accepts the worth of a thing
Assumes responsibility for,
participates, enables, initiates,
examines
Organisation
Organises values, determines
relationships, adapts behaviour
to a system of values
Forms judgements. Relates,
regulates, is realistic
Characterisation
Generalises certain behaviours
into usual behaviours and
responses
Is prepared for, approaches,
views, examines, is consistent
The Psychomotor Domain
Bloom did not compile a taxonomy for this domain. Others have attempted to do so, but there is still
no general agreement on either the levels or the descriptors.
The domain is characterised by the development of skilled movements and actions. As the individual
develops a higher level of expertise through practice their movements become less tentative and
more fluid or adept. Experts are able to adjust their actions according to changing circumstances. An
example of this is a football player who first learns to kick the ball in the direction of play. As skill
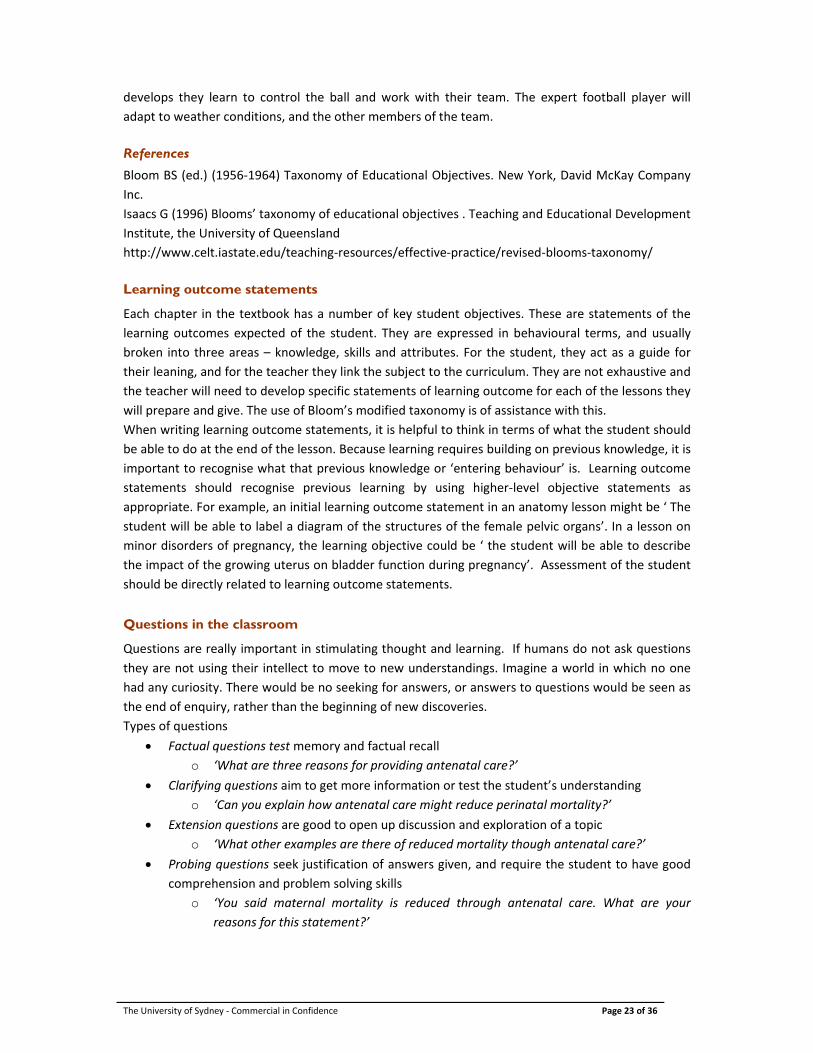
The University of Sydney ‐ Commercial in Confidence Page 23 of 36
develops they learn to control the ball and work with their team. The expert football player will
adapt to weather conditions, and the other members of the team.
References
Bloom BS (ed.) (1956‐1964) Taxonomy of Educational Objectives. New York, David McKay Company
Inc.
Isaacs G (1996) Blooms’ taxonomy of educational objectives . Teaching and Educational Development
Institute, the University of Queensland
http://www.celt.iastate.edu/teaching‐resources/effective‐practice/revised‐blooms‐taxonomy/
Learning outcome statements
Each chapter in the textbook has a number of key student objectives. These are statements of the
learning outcomes expected of the student. They are expressed in behavioural terms, and usually
broken into three areas – knowledge, skills and attributes. For the student, they act as a guide for
their leaning, and for the teacher they link the subject to the curriculum. They are not exhaustive and
the teacher will need to develop specific statements of learning outcome for each of the lessons they
will prepare and give. The use of Bloom’s modified taxonomy is of assistance with this.
When writing learning outcome statements, it is helpful to think in terms of what the student should
be able to do at the end of the lesson. Because learning requires building on previous knowledge, it is
important to recognise what that previous knowledge or ‘entering behaviour’ is. Learning outcome
statements should recognise previous learning by using higher‐level objective statements as
appropriate. For example, an initial learning outcome statement in an anatomy lesson might be ‘ The
student will be able to label a diagram of the structures of the female pelvic organs’. In a lesson on
minor disorders of pregnancy, the learning objective could be ‘ the student will be able to describe
the impact of the growing uterus on bladder function during pregnancy’. Assessment of the student
should be directly related to learning outcome statements.
Questions in the classroom
Questions are really important in stimulating thought and learning. If humans do not ask questions
they are not using their intellect to move to new understandings. Imagine a world in which no one
had any curiosity. There would be no seeking for answers, or answers to questions would be seen as
the end of enquiry, rather than the beginning of new discoveries.
Types of questions
Factual questions test memory and factual recall
o ‘What are three reasons for providing antenatal care?’
Clarifying questions aim to get more information or test the student’s understanding
o ‘Can you explain how antenatal care might reduce perinatal mortality?’
Extension questions are good to open up discussion and exploration of a topic
o ‘What other examples are there of reduced mortality though antenatal care?’
Probing questions seek justification of answers given, and require the student to have good
comprehension and problem solving skills
o ‘You said maternal mortality is reduced through antenatal care. What are your
reasons for this statement?’
The University of Sydney ‐ Commercial in Confidence Page 24 of 36
Hypothetical or ‘what if’ questions require the student to extend their reasoning beyond the
immediate question
o ‘What if you encountered a woman who refuse to have antenatal care. How would
you explain the benefits?’
Redirected questions can be used to extend the discussion to other students
o ‘Huyen has said that she would tell the woman the risks she is facing. What would
you do Nga?
Reflective questions require the student to review their thoughts, actions and emotions in a
given situation. Generally they are used in one‐to‐one sessions or in small, well‐established
groups where the student feels ‘safe’.
o ‘So how did you feel then?’ What were your thoughts at the time?’ what will you do
differently next time as a result of this experience?’
Tips for asking good questions:
Ask questions at different levels of the Blooms Hierarchy
Prepare the questions before hand
Ask specific questions – if they are too general a precise response cannot be expected
Vary the way you direct questions in a classroom – some should be to the class in general,
and others can be targeted to individual students. Avoid always asking the same students.
Wait in silence after asking a question. This allows the student to frame an answer, or for
others in the room to be ready. A rough guide is 15 seconds.
Practice with your colleagues. This can be very helpful in focussing questions.
Dealing with answers
Acknowledge attempts at answering with positive feedback
Avoid embarrassing the student or making them feel stupid
If answers are incorrect, rephrase the question – it is often because the student did not
understand what was being asked
If the answers given are still wrong, ask more questions to redirect the student. You may also
ask another student to help them
If a student asks a question the teacher does not know the answer to, there is no shame in
this. Open the question to the class – someone may know the answer, but most importantly,
discuss ways in which the answer can be found, and report back to the next class.
Learning in small groups
A small group can be defined as three to ten people working together with common aims. Small
group work is an important active teaching and learning strategy. Small group work enhances
student interaction and collaboration and learning. Many of the adult learning principles are
addressed through small group work. Small group work is useful when a team can be expected to
complete more complex and demanding tasks than individuals alone, such as projects, complex
clinical scenarios, and problem solving.
The most common forms of small group work are in the tutorial and laboratory sessions. However it
is possible to use small group discussion as part of a lecture, when students can work in groups of
three to meet short‐term goals.

The University of Sydney ‐ Commercial in Confidence Page 25 of 36
For small groups to function well, the members must be comfortable with each other and be
prepared to work as a team. They must also have common goals – these can be set or evolve
naturally, but usually include meeting the target, sharing the workload, committing to the timeframe
and so on. Leadership of the group is important, and training of tutors may be required. The leader –
usually a tutor ‐ is responsible for ensuring that the group stays on target, that all members are
involved and that time frames and schedules are met. They need to ensure that the group members
are respectful of each other and that they assess the functioning of the group. Any assessment
associated with work being done by the group should include the input of the tutor.
Finally, the use of groups should be accompanied by clearly defined goals and supportive educational
materials. These should form part of the course materials and lesson plans.
A useful resource for group work is
http://www.jcu.edu.au/wiledpack/modules/feedback/JCU_090547.html
Developing lesson plans
Lesson plans are used to ensure that the content of a session is defined, delivered in accordance with
the curriculum and the subject, and that the teaching‐ learning activities are appropriate to the
resources available and to the students. Another important aspect of the lesson plan is that it allows
the teacher to design assessment that meets the learning outcomes and also allows assessment of
her own classroom performance.
The University of Sydney ‐ Commercial in Confidence Page 26 of 36
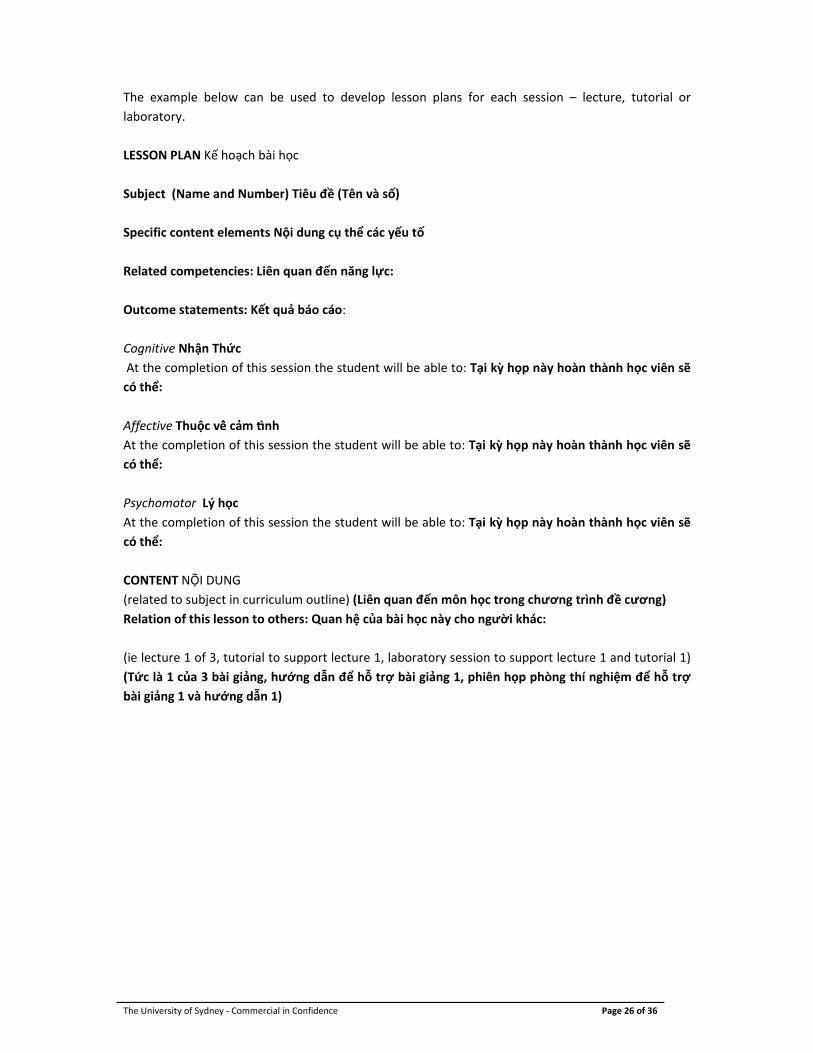
The example below can be used to develop lesson plans for each session – lecture, tutorial or
laboratory.
LESSON PLAN Kế hoạch bài học
Subject (Name and Number) Tiêu đề (Tên và số)
Specific content elements Nội dung cụ thể các yếu tố
Related competencies: Liên quan đến năng lực:
Outcome statements: Kết quả báo cáo:
Cognitive Nhận Thức
At the completion of this session the student will be able to: Tại kỳ họp này hoàn thành học viên sẽ
có thể:
Affective Thuộc vê cảm nh
At the completion of this session the student will be able to: Tại kỳ họp này hoàn thành học viên sẽ
có thể:
Psychomotor Lý học
At the completion of this session the student will be able to: Tại kỳ họp này hoàn thành học viên sẽ
có thể:
CONTENT NỘI DUNG
(related to subject in curriculum outline) (Liên quan đến môn học trong chương trình đề cương)
Relation of this lesson to others: Quan hệ của bài học này cho người khác:
(ie lecture 1 of 3, tutorial to support lecture 1, laboratory session to support lecture 1 and tutorial 1)
(Tức là 1 của 3 bài giảng, hướng dẫn để hỗ trợ bài giảng 1, phiên họp phòng thí nghiệm để hỗ trợ
bài giảng 1 và hướng dẫn 1)
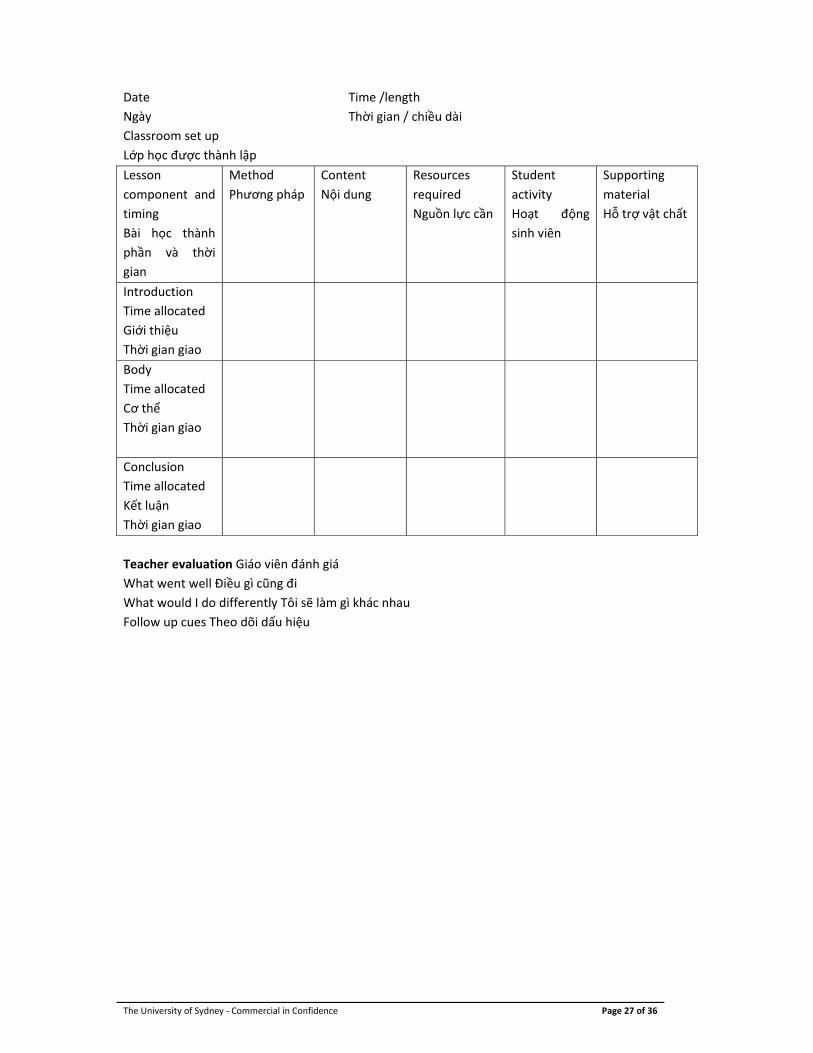
The University of Sydney ‐ Commercial in Confidence Page 27 of 36
Date Time /length
Ngày Thời gian / chiều dài
Classroom set up
Lớp học được thành lập
Lesson
component and
timing
Bài học thành
phần và thời
gian
Method
Phương pháp
Content
Nội dung
Resources
required
Nguồn lực cần
Student
activity
Hoạt động
sinh viên
Supporting
material
Hỗ trợ vật chất
Introduction
Time allocated
Giới thiệu
Thời gian giao
Body
Time allocated
Cơ thể
Thời gian giao
Conclusion
Time allocated
Kết luận
Thời gian giao
Teacher evaluation Giáo viên đánh giá
What went well Điều gì cũng đi
What would I do differently Tôi sẽ làm gì khác nhau
Follow up cues Theo dõi dấu hiệu
The University of Sydney ‐ Commercial in Confidence Page 28 of 36
Clinical Experience
Clinical experience is a vital part of any curriculum that prepares health professionals for the work
they will do after graduation. This is especially so in a competency based curriculum.
For this reason, teachers must plan clinical experience carefully, and prepare students for their time
in the clinical area. While a lesson plan is not usually developed for clinical placement, the following
points must be observed. The safety of the woman and her baby is the most important consideration
in any placement, and this is ensured by adequate preparation and planning for clinical placements.
o Appropriate selection of experience for the learning outcomes must be a priority. Midwifery
skills are learnt in midwifery settings.
o The clinicians must be prepared for the students. Colleges must have strong relationships
with the clinical facilities. Negotiating placements, providing the clinicians with educational
preparation and support and formal agreements between colleges and hospitals, facilitates
this.
o Clinicians must have some familiarity with the curriculum in order to help the students’
learning as well as their skill development.
o Clear statements of the expectation of the clinical placement must be made available to the
people who will be supervising the students and the students themselves. This will enhance
the confidence of the supervisor.
o The responsibility for assessment of the student in the clinical setting must be clear and the
result of negotiation. Clinical assessment procedures must be uniform and fair.
o Clinicians must understand the need for the record of clinical experience and appreciate how
it is used to enhance learning as well as record experiences.
o Clinical experience should involve actual hands on experiences, which are guided and
supported by the clinical teacher.
o Poor performance in the clinical setting must be treated in the same way as academic
underperformance. Clinicians must be able to speak to the nominated academic
representative responsible for monitoring performance at any time. In this way the safety of
the woman and her baby is given the highest priority.
o Students must only provide care under the supervision of a qualified midwife or obstetrician.
o Finally, the woman who is provided care by a student should be confident that the student is
adequately skilled and supervised. She should be assured that the care she receives is safe
and effective.
Tips for clinical teaching:
Be clear about what you want to do
Plan your actions ‐ what are you trying to achieve with the patient?
o What are you trying to achieve with the student?
o How does this fit in with protocols and set procedures?
Explain yourself ‐ give reasons
o Remember that beginning practitioners are "rule" driven. If they follow the "rules" it will
work for them. Advanced practitioners tend to take short cuts and are more idiosyncratic
about the way they approach things. This can be extremely difficult for the student to
understand.
o Giving reasons for what you do often helps you to examine your own practice. Most of us
teach the way that we were taught.
The University of Sydney ‐ Commercial in Confidence Page 29 of 36
o Some research has demonstrated that most clinical preceptors get the student to watch
what they do for a while before the student is expected to do it. When the student does do
it, they may have missed critical elements or links because they did not "see" you do it. By
explaining each component you give emphasis to it and appeal to different learning styles.
Remember to discuss the encounter afterwards
o Give the student a chance to ask questions without feeling embarrassed for not knowing the
answers.
o Practice clear communication with the student
o Encourage reflection
o Draw links with theory where possible
o Make comparisons with other cases
Encourage the student
Feedback
Feedback is a term that is applied to the process where someone is told how well or otherwise they
have performed in a situation. The purpose of giving feed back is to motivate the learner and to
enhance learning. There are two main forms of feedback, formative and summative.
Formative feedback represents information communicated to the learner that is intended to modify
the learner’s thinking or behaviour for the purpose of improving learning. Formative feedback helps
students to identify their strengths and weaknesses and target areas that need work.
Formative feedback is provided in order to develop the practice of an individual. The following is a
useful examination of the literature surrounding formative feedback.
http://www.ets.org/Media/Research/pdf/RR‐07‐11.pdf
Summative feedback is generally given as a final assessment of knowledge or competency. Examples
include final examinations and assessments of clinical competency.
Characteristics of effective feedback
Effective feedback should be
Unambiguous ‐the learner should be clear about what they did or did not do. The standards
against which the student is expected to perform should be clear.
Timely – it should be given as close as possible to the event
Respectful and constructive ‐ the student needs to feel that they are heard, but the teacher
needs to also give clear direction
More information can be found at this website
http://www.jcu.edu.au/wiledpack/modules/feedback/JCU_090547.html
Teaching resources
Teaching materials
Traditionally, teaching materials consist of lecture notes and handouts, textbooks, charts and
diagrams and models. More recently, the use of PowerPoint presentations and internet resources
have changed the way lectures are prepared and presented.
The single most important aid to teaching is the preparation. Regardless of the methods chosen to
deliver material, a lecturer who is well prepared and organised will earn the respect of their
students. When planning lessons, the nature of the classroom setup, the teaching approach, the

The University of Sydney ‐ Commercial in Confidence Page 30 of 36
equipment to be used and the questions to be asked should be prepared in advance. Research of the
material to be taught should be thorough and be arranged from simple to more complex ideas.
When using PowerPoint, care should always be taken to ensure that the content is not overlooked in
favour of a visually pleasing presentation. Classroom notes should be concise and relate directly to
learning objectives. All materials should be prepared with a view to appealing to different learning
styles.
The classroom
Traditional classroom
The typical classroom for lectures is set up with tables and seating in rows. The teacher is at the
front. This asserts the teacher as dominant and students as passive. It limits the amount of
interaction in the classroom.
Figure 16.4 Traditional classroom
Fishbone
This involves placing tables and seating into diagonal rows. The teacher is still dominant, but the
students can see each other, so this allows for more interaction.
Figure 16.5 Fishbone arrangement
Café style
Tables and chairs are grouped to form small squares or rectangles, allowing all seated at that table to
see each other. This is ideal for interaction between 6‐8 students.
Figure 16.6 Café style
Ballroom

The University of Sydney ‐ Commercial in Confidence Page 31 of 36
Larger tables seating 10 or 12 are arranged around a space in the centre of the room. This allows for
interaction between students and the teacher is free to move around the room, but can become the
focus by placing themselves at the centre.
Figure 16.7 Ballroom
Circles
Tables are arranged in a circle, with the teacher forming part of the circle. This is a good set up for
class discussion. The closed rectangle is a similar structure, but is less conducive to eye contact
between class members.
Figure 16.8 Circles
U shape
This is a common set up for seminars and conferences, where there is a need for many people to
speak.
Figure 16.9 U shape
Equipment
There are guidelines for classroom spaces for Vietnam which describe minimum requirements. It is
useful for the teacher to decide the classroom set up they would like to use and to prepare the room
with necessary equipment before the class. Teaching resources are often expensive and may be
limited, so teachers need to develop skills in being resourceful. Inexpensive teaching aids can be as
effective as sophisticated models.
Teaching aids may be very simple or extremely life‐like. Fidelity is the term used to describe how life‐
like a model is. For example, the skill of introducing a catheter into a woman’s bladder requires fine
motor skills. These can be practiced by introducing a catheter into a small hole drilled into a piece of
board, or by using an expensive training model. The piece of board is low fidelity but is just as
The University of Sydney ‐ Commercial in Confidence Page 32 of 36
effective at teaching the student the hand‐eye coordination required as the higher fidelity expensive
plastic mannequin.
Training models can also be part‐task or full‐task trainers. Part task refers to equipment that
represents only a part of the skill or the body. A cannulation arm is a part task trainer because it does
not include the interaction that is required between the midwife and the patient. It can be made
closer to a full task trainer, by having another student pretend that the arm is theirs, and interacting
with the student.
Teachers should use their imaginations to develop innovative ways of teaching content for the simple
reason that learning that occurs with the student’s active engagement is more likely to be effectively
retained, and most importantly, applied in a variety of situations. This is because students will build
on what they already know, assisting them to move towards deeper understanding, analysis and
synthesis.
Assessing learning
There are a number of reasons to assess students. These include motivation to learn, diagnosis of
strengths and weaknesses, creating an opportunity to provide feedback, to pass or fail a student, to
grade students, to improve teaching or assess the teacher and to monitor educational standards over
time.
Whatever the reason, assessment must always relate to the learning outcomes expected of the
student. Assessment should also be pitched at a number of different levels, from knowledge to
synthesis.
The traditional method of assessing how much students have learnt is the examination. This may be
either written or oral. In the past twenty to thirty years, there has been an international trend away
from using written exams as the only form of assessment. Progressive assessment and continuous
assessment are being used more often as they ensure that students learn continuously and
progressively. Learning for exams only relies more on short to medium term memory than long‐term
memory, and retention is poor. Students can pass exams, but not have the knowledge for application
to practice. Continuous assessment has been shown to lead to higher overall marks than the
traditional end of year examination alone. It allows students opportunities to learn according to their
individual learning style preference. It also allows the teacher to provide formative feedback. This
means that learning and behaviour can be shaped progressively, and standards reinforced over time.
Progressive assessment means that assignments, group work and workbooks can contribute to the
final mark. The final exam can be used as part of an assessment total, or to grade students after they
have passed all of the elements of assessment in a course.
For instance, a course may be assessed using the following strategies:
Assignment (3000 word essay on a set topic) 30%
Tutorial presentation and written summary 25%
Workbook 10%
Examination 35%
Or, if the examination is to be used to grade students, all course work must be passed at 50%
Assignment 1 (2000 word essay) 30%
Assignment 2 (2000 word essay) 30%
Tutorial presentation plus report 30%
Tutorial contributions 10%
Grading examination
The University of Sydney ‐ Commercial in Confidence Page 33 of 36
0‐55% = Pass
56‐69% = Credit
70 ‐84% = Distinction
85‐100% = High Distinction
The format of assessment should be varied, so that levels of knowledge are assessed and the
students’ ability to interpret data, apply knowledge and to problem solve is tested. For final written
examinations, there should generally be a means by which the student’s ability to analyse and
synthesis (the higher levels of Blooms’ taxonomy) are assessed.
Skill development is often assessed by checklists which can be used either in the simulated
(laboratory) or real clinical setting. These two can be used formatively and summatively. Formatively
refers to the student being given detailed feedback after a performance. The assessor describes the
strengths as well as the areas for improvement, and encourages the student to reflect on
performance. Summative assessment is used to pass or fail a student, and feedback, while still given,
is in the form of final assessment.
The importance of feedback is that it allows behaviours to be shaped, and provides the student with
direction.
The assessment of students in the clinical setting is as important as assessment in examinations or
through assignments. The student will be assessed through the skills assessment tests that are of two
types – formative and summative. These tests are more than checklists because they incorporate the
affective as well as the psychomotor domains.
The students’ record books should be reviewed regularly to ensure that they are recording their
clinical experiences, and also to ensure that they are demonstrating development of skills and
knowledge through the nature of their documentation. Feedback must be given on this aspect of the
students’ work.
A useful resources is :
http://sydney.edu.au/education_social_work/learning_teaching/staff/evaluation/index.shtml
Conclusion
This chapter has outlined some of the elements which must be considered in order to ensure that
teaching and learning activities are designed to maximise the student’s professional development.
The relationship between what is learnt in the classroom and the ability of the midwife to provide
safe and effective care is the end result of the education she receives. As a learner, the student has a
responsibility to complete the learning tasks set, but also to develop an active approach to their own
learning, so that they can maximise the opportunities that are provided by their teachers and their
clinical learning environment.
Reflective activities
Think about a lesson you have recently given. How did the students respond to it? What did you have
to research or learn in order to give it? How did you measure the effectiveness of the session?
What would it be like to be in your class? Would you be excited and interested?
How did you learn to teach? Are your methods the same as those who taught you?

The University of Sydney ‐ Commercial in Confidence Page 34 of 36
Ask a colleague to sit in on one of your classes. Get them to record what they felt was the core
information of the lesson. How well does this match with your intended learning outcomes?
Imagine you need to learn a new skill. What are the key elements? What previous knowledge is
required? How will you be most comfortable learning this skill? What things might help you learn it?
The University of Sydney ‐ Commercial in Confidence Page 35 of 36
References:
Ben‐David, M. (1999). AMEE Guide No 14: outcome‐based education. Part 3 –Assessment in
outcome‐based education. Medical Teacher. 21(1) 23‐25.
Frank, J., Mungroo, R., Ahmed, Y., Wang, M., DeRossi, S. & Horsley, T. (2010). Toward a definition of
competency‐based education in medicine: a systematic review of published definitions. Medical
Teacher 32: 631‐637.
Harden, R., Crosby, J. & Davis, M. (1999) AMEE Guide No 14: outcome‐based education. Part 1 – An
introduction to outcome‐based education. Medical Teacher. 21(1): 7‐14.
Harden, R., Crosby, J., Davis, M. & Friedman, M. (1999) AMEE Guide No 14: outcome‐based
education. Part 5 – From competency to meta‐competency: a model for the specification of learning
outcomes. Medical Teacher. 21(6) 546‐552.
ICM (2010) ICM Essential Competencies for Basic Midwifery Practice (2010 amended 2013).
http://www.internationalmidwives.org/what‐we‐do/education‐coredocuments/essential‐
competencies‐basic‐midwifery‐practice/
ICM (2012) International Confederation of Midwives’ Model Curriculum Outlines for Professional
Midwifery Education. ICM Resource Packet #4: Teaching and learning in a competency‐based
curriculum. http://www.internationalmidwives.org/what‐we‐do/education‐coredocuments/model‐
curriculum‐outlines‐for‐professional‐midwifery‐education/packet‐1‐2‐3‐4.html
Leung, W. (2002). Competency based medical training review. British Medical Journal 325, 693‐695.
Ministry of Health (2014) Essential Competencies for Midwifery Practice in VietNam. Decision No
342/QD‐BYT. Hanoi, MoH.
Smith, S. & Dollase, R. (1999) AMEE Guide No 14: outcome‐based education. Part 2 – Planning,
implementation and evaluating a competency‐based curriculum. Medical Teacher. 21(1) 15‐22.
Smith, S., Dollase, R. & Boss, J. (2002) Assessing students’ performance in a competency‐based
curriculum. Academic Medicine. 78 (1), 97‐107.
WHO (1978) Competency‐based Curriculum Development in Medical Education: an introduction.
Geneva: WHO.
The University of Sydney ‐ Commercial in Confidence Page 36 of 36
Appendix A:
Essential Competencies for Midwifery Practice in VietNam (abridged version):
Each competency is expanded to encompass the knowledge, skills and professional practice components which make up each competency.
1. Midwives should have the requisite knowledge and skills from obstetrics, neonatology, the
social sciences, public health and ethics that form the basis of high quality, culturally
relevant, appropriate care for women, newborns, and childbearing families.
2. Midwives provide high quality, culturally sensitive health education and services to all in the community in order to promote healthy family life, planned pregnancies and positive parenting.
3. Midwives provide high quality antenatal care to maximize health during pregnancy and that
includes early detection and treatment or referral of selected complications.
4. Midwives provide high quality, culturally sensitive care during labour, conduct a clean and safe birth and handle selected emergency situations to maximize the health of women and their newborns.
5. Midwives provide comprehensive, high quality, culturally sensitive postpartum care for women.
6. Midwives provide high quality, comprehensive care for the essentially healthy infant from birth to two months of age.
7. Midwives provide a range of individualised, culturally sensitive abortion‐related care services
for women requiring or experiencing pregnancy termination or loss that are congruent with applicable laws and regulations and in accord with national protocols. (and guidelines in reproductive health care services).
From: Ministry of Health (2014) Essential Competencies for Midwifery Practice in VietNam. Decision No 342/QD‐BYT. Hanoi, MoH, pp7‐20. These are the International Confederation of Midwives Competencies – with the small addition shown in italics in Competency 7. ICM Essential Competencies for Basic Midwifery Practice (2010 amended 2013).
![Agriculture Resources on the Internet 2018whitepapers.virtualprivatelibrary.net/Agriculture Resources.pdf · [Updated: November 9, 2017] Agriculture Resources 2018 White Paper Link](https://img.pdfslide.us/doc/110x75/5a78a73f7f8b9a7b698e2b15/agriculture-resources-on-the-internet-resourcespdfupdated-november-9-2017-agriculture.jpg)