Embed Size (px)
Citation preview

MENTAL HANDICAP VOL. 18 DECEMBER 1990
Teaching people how to manage their own “special” diets:
Angela Cole
Anyone can develop health problems which result in the need to follow a particular type of diet in order to stay well. If this happens, having the opportunity to learn how to manage their health through their diet can mean the difference between a life style that is relatively independent from the medical profession and one that is not. People who have mental handicaps may require increased assistance to learn dietary control of their health, and there may be risks involved. This article examines some of the issues that arose in relation to such a situation in practice, and draws out some of the lessons that were learned.
Anyone may need to follow a “special” diet at some time during their life because of a temporary or permanent health problem. Some examples which come readily to mind are diets associated with ulcers and hernias, heart and circulatory conditions, and bowel disorders. Poor management of the diet can have unwelcome, oRen ainful consequences; in some cases,
where dietary education is crucial if people are to manage their own diets successfully and maintain control over their health, thereby being able to lead lives which are relatively free from dependence upon the medical professions.
For people with mental handicaps who need a “special” diet because of health problems there are factors which complicate the process of teaching dietary self-management. The importance of taking these into account was reinforced for me through my contact with a woman who had diabetes and I will, therefore, use that experience to illustrate my arguments. The points made, however, apply to teaching people with mental handicaps about managing their diet whatever their medical condition.
Controlling health throu h diet is often com licated
“fine-tuning” is often required to adjust sugar levels in the body. For most ople, awareness and vigilance over food and drink i n s e become almost second nature over time. This, however, is a learned response which people who have mental handicaps may need extra help to develop. That help must be offered in the most a propriate ways in order that learning can occur, for
it can also be life-t K reatening. Diabetes is one instance
and difficult to understand. B or example, with iiabetes
a P 1 people “are capable of personal growth, given the
right conditions for doing SO’’ (Mental Handicap in Wales Applied Research Unit, 1985). Without the “ri ht conditions”, people who have mental handicaps
therefore, remain depen ent upon others. In this society, dependent adults often suffer loss of
status and, are not valued. The “right conditions” should, therefore, involve the use of “means which are valued in our society in order to develop and support personal behaviour, experiences and characteristics, which are, likewise, valued” (O’Brien and Tyne, 1981). Thus, dietary education which achieves its goal can help people with mental handicaps to increase their status and value by taking control over an aspect of their own lives - health care - like others who have special dietary needs.
x” wil 5 be denied the op rtunity to learn and will,
Diabetes, independence, and risk The philosophy of normalisation (Wolfensberger,
1972) and the current policy of care in the community (DHSS, 1981) have seen many people with mental handicaps achieve increased independence in their lives through moves into ordinary housing. For most, advice and guidance is available from a network of su porters, the intensity of this depending upon
independence may be limited if the dietary education process fails to meet their learning needs.
In the past, when it was the norm that people with mental handicaps were “cared for” by others, manage- ment of health problems was not an issue. It was sim ly taken out of their hands from the outset, in the beEef that they were unable to cope with their own medical care, or learn how to do so, without danger to themselves.
This protective and paternalistic consideration of risk is present in arguments which advocate continual support and “care” for people who have mental handicaps and diabetes, purely on the basis that they are having, or may have, problems managing their diet. This is a negative approach which fails to take into account two important factors.
0 People who have mental handicaps may not have been adequately taught how to manage their own diabetic diets. This may well be a
in B ividual need. For any who have diabetes, however,
ANGELA COLE is a Senior Lecturer in the Department of Health, Nursing, and Social Work at Anglia Higher Education College, Victoria Road South, Chelmsford, Essex, CM1 1LL.
0 1990 BlMH Publications

MENTAL HANDICAP VOL. 18 DECEMBER 1990
failure of the dietary education process to find appropriate educational techniques, rather than a “failure” of the individual.
0 Learning new skills involves risks for every one of us, not only for ople with mental handicaps.
risk that an accident may result in injury or death. However, many of us take this risk because, in law, it is minimised by the requirement that a qualified driver be present. Without taking the risk, we would not learn a new skill - how to drive - and enjoy the benefits it brings.
Opportunities for developing new skills must be presented to people with mental handicaps in ways which both minimise any risks involved and meet their learnin needs. Such opportunities must be provided
Take learning to r rive as an example: there is a
before c f eclarations of “inability” are made.
Current problems: an example The problems of teaching dietary self-management to
people with mental handicaps was highlighted for me in my contact with Jane. When her father died she had experienced difficulty in coping alone and was moved to a hostel to receive the support she was felt to need. However, this “support” amounted to “care”, and Jane lost the opportunity to undertake many of the tasks she had previously taken pride in attempting. Having been used to a more significant role within the household it was, perhaps, not surprising that when, some years later, she met and formed a close bond with Bob, they both talked eagerly of finding a home together.
Both Bob and Jane were assessed and considered to have the necessary skills to achieve such independence,
iven initial intensive support and “training”, followed f y ongoing help of a less intensive nature. They, there- fore, moved into a local authority flat and received eight weeks’ intensive daily training in household mana ement skills. This was followed b twice weekly
social worker, and daily visits from a district nurse who administered Jane’s insulin injection. Jane also received guidance and support from the local day centre, which she attended three times per week, and regular outpatient appointments at the local hospital to monitor her diabetes. In addition, she was seen by a dietician.
Despite this very high level of support and guidance, it soon became evident that Jane was experiencing difficulty in managing her diet. Her daily urine tests showed constant swings and she was having problems with her feet at very regular intervals. In every other area of their lives the couple were managing reasonably well and, above all, were happy in their new home. It was clear, though, that neither Jane nor Bob (who had suffered an accidental head injury) could fully understand Jane’s dietary needs. They did understand that Jane’s health was affected by her diet, but did not know what they were doing “wrong”.
Consultation with the dietician revealed that Jane had been given a basic diet sheet, largely in picture form, showing foods with the same “exchange” value. However, the sheet was not easy for Jane to understand because of the choices presented within it, and the need to create meals from the options. A folder containing pictures of complete meals and snacks was, therefore, tried, so that, instead of having to make up meals from appropriate foods, Jane could choose a meal in the
visits a om a home care assistant, week6 visits from a
knowledge that its component parts would be correct for her diet. As Bob did most of the cooking in the household, however, success very much depended upon his understanding of the diet folder as well. As the folder was given to Jane at the day centre, and its contents explained there, Bob was not involved. Consequently, that vital link in the communication process was missed. These problems were still not fully resolved when my contact with Jane and Bob ended.
The problems highlighted Jane’s experience points to some of the factors which
need to be taken into account when trying to teach people with mental handicaps the skills of dietary self- management. These have to be addressed if people are to learn the skills which will enable them to lead a more independent and “ordinary” life.
0 Self-management diet sheets and information Most people with mental handicaps, by virtue of the difficulties they experience with learning, have been unable to develop competent reading and writing skills. Thus, fundamental problems are posed by diet sheets which rely on the written word to communicate their content. Such sheets are only of use to them when they are in the presence of another person who can read. This situation, therefore, places them in a dependent role.
The right to choose what we eat is one valued by most people in Western Society and this is reflected in the concept of exchange in diets for people with diabetes. For people who, have mental handicaps, however, making choices can often be problematic. Many have been in a dependent role for a long time, either within the family or in an institution, where their opportunities to make choices have been limited. The concept may, therefore, be new to them, and the practice of making choices may need to be learned.
0 Recall and retrieval of information Although most people who have a “special” diet have diet sheets and information at hand, these are needed progressively less as they get to know what is required in order to maintain health. This is a function of memory and a process of learning. People who have mental handicaps are likely to take significantly longer to achieve this. Recall of information cannot be assumed, and ready access to understandable literature is, therefore, essential.
Dietary control of medical conditions may require an understanding of more than just food. For example, “energy”, “carbohydrate”, “glucose”, and “grams” were all words that Jane was faced with. Such words assume basic familiarity with the nutritional constituents of food, the functions of the body, and concepts of weights and measures - but these are areas of knowledge to which many people with mental handicaps will never have had access.
People with mental handicaps who are living independently in the community may have very
0 “Exchange” = “choice”
0 Terminology
0 Financial concerns
0 1990 BlMM Publications 1 57

MENTAL HANDICAP VOL. 18 DECEMBER 1990
0
0
limited financial resources, most surviving on DSS benefits. However, above average expenditure can be incurred when special dietary needs are combined with the need for foods that are relatively easy to cook and a varied diet. For example, the advice to “avoid fatty foods” may require that relatively inexpensive cuts of meat are replaced by more expensive ones; “convenience foods” may not be so desirable; and high fibre foods may be more expensive. Finances may thus be a cause for concern. Information for people in the support network My own lack of knowledge about the dietary needs of people with dabetes became apparent during my contact with Jane’s dietician. The home care assistant experienced the same problem. Because of our initial lack of information, Jane often received contradctory advice about her diet. This is one of the dangers if all those in the support network do not present a coordinated, collaborative approach. Information for living companions Many people with mental handicaps who are living independent lives share their homes with others who also have mental handicaps. In such situations people live as a group, and household tasks are divided amongst the members. It is, therefore, important that all the living companions have an understanding of the dietary needs of any group members with diabtes. In Jane’s case, exclusion of Bob from the education process jeopardised any improvement in her situation because of the central role he took in the household.
health care professional, are the ability to integrate information into meaningful concepts, to sequence, to remember and retrieve information, and to problem- solve and reason beyond immediate conditions”. These cannot be “taken for granted” when trying to teach people with mental handicaps the skills of dietary self- management.
The main requirement in teaching people to manage their own “special” diets is that the approach must be based upon each person’s individual needs and circumstances. Beyond this there are additional factors which have to be taken into account:
0 Verbal and written information should be given in language and form that is understandable and relevant to each individual’s experience of life. For example, pictures may be preferable to the use of the written word. Signs, such as those found in pictorial cookery books for adults, may be helpful (Day and Hollins, 1985). Reminder cards showing appropriate foods, which can be easily carried by the person to the shops, may aid information recall.
0 Everyone in the support network needs to be educated too, in the dietary needs of anyone requiring a “special” diet. A programme of education can be drawn up, involving the person, living companions, and support staff, so that learning and information is shared and clear.
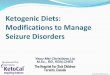
0 Education programmes must be designed to develop learning at a pace suitable for the person with a mental handicap, and must take into account the gradual development of choice and financial circumstances. A goal planning approach, involving an analysis of the knowledge and tasks required to be learned in order to achieve the overall goal of dietarv self-
Lessons from practice management, would apha r to k an Independent living presents people who have mental appropriate means to this end. An example of
handicaps with new found freedoms and opportunities how such a planned approach might look is to make choices. For those with particular dietary shown in Figure 1. In order to achieve each of needs, restraint and control over their diet may seem the short-term goals, the action element would contradictory to their new life style. Teaching people need to be broken down into smaller steps. how to manage their own diets in their new settings produces thought-provoking dilemmas: - - -
“Jane knows that chocolate is not a wise thing to eat, but she likes chocolate. Diabetic chocolate is expensive, and doesn’t taste so good, so she secretly eats ordinary chocolate...”.
She is making a choice, a decision about her own life. But - is she making an informed choice, an informed decision? Does Jane really understand what “coma” means? Does she know what the consequences of her choices and decisions might be? What does she know? What does she not know?
In such a situation it is all too easy to conclude that Jane cannot cope independently and, therefore, start to deny her some of that independence. The alternative IS to ensure that Jane really is “informed’, and that the requirements of her medical condition and diet are conveyed to her in ways which acknowledge and respond to her learning needs.
People with mental handicaps experience problems in recognising, retaining, and retrieving information. As Drumm and Schade (1986) have written: “Some of the prerequisite skills called upon for adherence to diabetes programmes, and taken for granted by the
158
To conclude The above points provide an outline for a coordinated
approach to teaching people with mental handicaps how to manage for themselves any special dietary needs they may have. It is an approach based upon individual needs, which aims to create the opportunity for people to learn how to take control of an aspect of their own health care. It is easy to allow our own fears about the risks involved in giving people greater independence to dictate our actions and make us over-protective. A structured approach can minimise risk whilst maintaining a clear developmental direction.
M own experience suggests, though, that staff may
information. There is a dearth of suitable, ready-made material, although the British Diabetic Association (address at end) has some publications, such as Z have diabetes, that could be adapted. These are largely aimed at children, so adaptation to the adult market is essential.
In An Ordinary Life (King’s Fund, 1980) it was stated: “A service is there to serve. It is its task to provide the right material and human resources. People who work
nee g to be quite creative in order to provide appropriate
0 1990 BlMH Publications

MENTAL HANDICAP VOL. 18 DECEMBER 1990 ~ ~
LONG-TERM GOAL: Jane and Bob will successfully control Jane’s diabetes through her diet
Aids/ notes Short-term goal Action
STEP 1: Jane and Bob will understand the link between Jane’s diet and her health, and the risks
Devise “educational input” appropriate to Jane and Bob’s learning needs
Possible use of BDA video, adapted BDA leaflet. Avoid jargon. Consult with dietician
STEP 2: Liaison, consultation and provision of appropriate information
Use of BDA material. Remember that some people may be worried about the risks. Have a tight plan so as to reassure them
People in Jane and Bobs sup rt network will understand thernk between Jane’s diet and her health, and the plan of action devised to achieve the long-term goal
Devise “educational input” appropriate to Jane and Bob’s learning needs. Find andior adapt weightslmeasures so that they can use them
Talk to Jane and Bob about their likes and dislikes, where they shop, what they buy etc, whilst carrying out Step 3
Involve Jane and Bob in this - finding pictures of “good” foods and “bad” foods. Make books. Make up pictures of healthy meals
STEP 3: Jane and Bob will understand that the type and amount of food are very important for Jane to stay healthy
Remember Jane and Bob’s rights to privacy and confidentiality. Involve them
STEP 4: People in the support network will understand what Jane and Bob like to eat, what they do not like, what their food budget is ... their circumstances
Do they need to learn new ways of cooking‘?
STEP 5: Jane and Bob will understand that the way in which they cook food is important for Jane to stay healthy
Devise “educational input” appropriate to Jane and Bob’s learning needs. Go shopping with them to find acceptable oils, fats, etc
Devise “educational input” appropriate to Jane and Bob’s learning needs. Let them practise in safety. Gradually give space to let them show their competence
Jane and Bob will understand that they can make choices in the diet, and what these are
Use teaching strategies, such as praise. Devise an aid with them to show choices of food
STEP 6:
STEP 7: Jane and Bob will know the “danger signs” and what to do if they occur
Devise “educational input” appropriate to their learning needs
Be clear and serious, but not frightening. Do they need to learn any other skills in order to achieve this goal?
FIGURE I . An example of a planned approach to dietary self-management
for the service are the servants of their clients”. In order to serve those clients well we can learn lessons from practice, and use them to develop approaches which really do enable people to master new skills which are valued by others. Most people who have diabetes, or other medical conditions which require a “special” diet, value having the opportunity to learn how to manage that diet because of the independence it brings. People who have mental handicaps have the right to such benefits too.
Drumm, D. A., Schade, D. S. How communication disorders destabilise diabetes. Clinical Diabetes, 1986; Jan/Feb, 16-22.
King’s Fund Centre. An Ordinary Life: comprehensive locally-based residential services for mentally handicapped people. London: King’s Fund, 1980.
Mental Handicap in Wales - Applied Research Unit. Zntmductory Leaflet. Cardiff Mental Handicap in Wales - A lied Research Unit, 1985.
OBrien, J., g e , A. The Pnnciple of Nonnalisatwn: a foundation for effective seruices. London: CMH, 1981.
Wolfensber er W. The Pnnciple of Nonnalizatwn in Human %erhces. Toronto: National Institute on Mental Retardation, 1972.
REFERENCES Day, S., Hollins, S. The role of the dietician. In Craft, M.,
Bicknell, J., Hollins, S. (Eds.). Mental Handicap.: Balliere-Tindal, 1985.
ment of Health and Social Security. Care in the DeF ommunity: a consultative document on moving resources for care. London: DHSS, 1981.
USEFUL ADDRESS Leaflets such as I Have Diabetes can be obtained from:
The British Diabetic Association, 10 Queen Anne Street, London, W 1M OBD.
0 1990 BlMH Publications 159