Embed Size (px)
Citation preview

Pediatric
LearningProgramforNurses
Teaching
Tube Feedingto Caregivers

© 1999, 2001 Ross Products Division, Abbott Laboratories
ContentsIntroduction and Objectives ............................................................................ 1When To Feed Children Enterally .................................................................... 2Special Needs of Children Who Are Tube-Fed ................................................ 3Selecting Feeding Tubes .................................................................................. 13Selecting a Formula ........................................................................................ 20Preparation and Storage Requirements .......................................................... 21Administering Tube Feedings to Children ...................................................... 23Administering Medications With Feedings...................................................... 36Tube-Site Care.................................................................................................. 37Potential Problems With Pediatric Tube Feeding .......................................... 42References........................................................................................................ 47
This module focuses on the tube feeding of infants and preadolescentchildren. Adolescents have special psychosocial needs, but their physicalcare is similar to that of adults. Unless otherwise noted, the term childrefers to infants and children.
Karen J. Suedkamp, RN, MSN President, Suedkamp Enterprise Inc.
Pat Larrimore, RN, MSPresident, Larrimore & AssociatesInc.
EditorsAngeline M. CameronJudith D. Gussler, PhDRoss Products DivisionAbbott Laboratories
AuthorVicky L. Armstrong, RNC, MSNPerinatal Outreach CoordinatorChildren’s Hospital, Columbus, OH
ReviewersKelly Strasbaugh, RN, BSNRoxanne Smarszcz, RN, BSNBonnie Gahn, MA, MSNRoss Products DivisionAbbott Laboratories

INTRODUCTION
nteral nutrition by means of afeeding tube can be used to meet thedaily nutritional needs of infants,
children, and adolescents when thoseneeds cannot be met by oral feedings (seeTable 1). With enteral nutrition, fluids andnutrients are delivered directly into thegastrointestinal (GI) tract, permittinggastric acids and other hormones torespond normally in the digestive process.Caring successfully for children receivingenteral nutrition requires that caregivershave not only working knowledge of thetechnical skills for providing the feedings,but also knowledge of the children’sdevelopmental and social needs. Thismodule will enable you to help caregiverscare for children who are tube-fed moreeffectively.
1
Ross Learning Program for Nurses
EOBJECTIVES
When you complete this module, you will be able to� Describe 3 age-appropriate developmental
interventions to use when caring for children whoare being fed enterally.
� Identify 3 anatomic and physiologic differencesbetween infants/children and adults.
� Differentiate 2 different types of tubes used toprovide enteral nutrition.
� Describe 3 procedures used in preparation, storage,and administration of enteral tube feedings.
� Describe 3 procedures for administeringmedication with enteral tube feedings.
� Describe 2 procedures to provide site care forenteral feeding tubes.
� Identify 3 potential problems associated withpediatric enteral tube feedings.
PediatricTeaching
Tube FeedingtoCaregivers

2
number of diseases and conditions of infants, children, and adolescents affecttheir ability to get adequate nutrition orally and are indications for tube feeding.Some of the most common are listed in Table 1 below.
Table 1. Indications for Pediatric Enteral Nutrition (not inclusive)
When To Feed Children Enterally
AGI Conditions� Short-bowel syndrome � Inflammatory bowel disease� Esophageal atresia/tracheo- � Liver disease
esophageal fistula � Malabsorption, chronic diarrhea� Surgery of GI tract
Hypermetabolic Conditions� Burns � Sepsis� Multiple trauma � Cardiac disease
Neurologic Impairments� Head injury, coma � Oral motor impairment� Suck-swallow dysfunction
Chronic Diseases� AIDS � Cystic fibrosis� Renal disease
Other Conditions� Prematurity � Anorexia or weight loss� Malnutrition—acute or chronic � Craniofacial malformations� Cancer with associated surgery,
radiation, chemotherapy

3
lthough some elements of tube feeding are consistentwhatever the age of the patient, infants and childrenalso have special developmental, social, and physical
needs that must be considered for tube feeding to succeed. Table 2 summarizes some of these developmental and socialneeds and techniques for meeting them.
ASpecial Needs of Children Who Are Tube-Fed
Infants and
children have
special
developmental,
social, and
physical needs
that must be
considered for
tube feeding to
succeed.
����

4
Special Needs of Children Who Are Tube-Fed
Neonate: Newborn to 1 Month
Key: - Trust vs mistrust stage
- Attachment to parent
- Time of learning through all senses
- Development of basic trust
- Primary socializing force—parents
� Looks at parent’s face
� Begins to fixate and track
� Begins to smile responsively
� Prefers faces, brightlycolored objects
� Hears well
Table 2. Developmental and Social Needs of Infants, Children, and Adolescents
� Establish eye contact, use calm approach
� Have parent hold child
� Touch, talk to, and comfort child whocannot be held
� Provide pacifier during enteral feedings
� Keep infant swaddled (if possible) topromote calming and self-organization
Developmental Stage Techniques To Meet Developmental/Social Needs

5
Keep infant swaddled
(if possible)
to promote
calming and
self-organization.
����
� Establish eye contact, use calmapproach
� Remember that the child understandsmore than he/she can vocalize
� Have parent hold child
� Touch, talk to, and comfort child whocannot be held
� Provide pacifier during enteral feedings
� Keep infant swaddled (if possible) topromote calming and self-organization
� Use distraction techniques (toys, rattles,music)
� Remember safety issues: Cover gastrostomy tube site with clothesso child cannot pull the tube; securenasal or oral tube so child cannot pull itout; at night, thread tubing through nightclothes to keep child from gettingtangled up in it
Developmental Stage Techniques To Meet Developmental/Social Needs
Infant: 2 to 12 Months
Key: - Trust vs mistrust stage
- Attachment to parent
- Time of learning through all senses
- Development of basic trust
- Primary socializing force—parents
� Watches another’s face
� Smiles spontaneously
� Babbles, laughs, imitates sounds
� Moves from lifting head tocrawling and pulling to stand
� Moves from grasping rattle toreaching for toys and finger foods
� Begins to have fear of strangers,separation from parent, andbeing left alone

6
Table 2. Developmental and Social Needs of Infants, Children, and Adolescents, continued
Toddler: 1 to 3 Years
Key: - Autonomy vs shame-and-doubt stage
- Developing independence
- Egocentric, magical thinking
- Mastery of locomotor and language skills
� Develops autonomy, negativism, ritualism
� Imitates activities
� Has temper tantrums
� Holds a cup, uses spoon and fork
� Undresses
� Begins to use words
� Walks, runs, climbs, kicks, throws, jumps
Developmental Stage
Special Needs of Children Who Are Tube-Fed

Allow child to
touch, hold, and
examine tube-feeding
equipment.
����
7
� Establish eye contact, use calm approach
� Remember that the child understands more than he/she can vocalize
� Use simple, concrete words and explanations
� Have parent stay with child
� Use comfort measures such as a blanket or favorite toy
� Explain all procedures as they occur and explain in terms of child’s perception;frequently reinforce idea that the child is not responsible for illness
� Demonstrate procedures on toy bear or doll
� Allow child to touch, hold, and examine tube-feeding equipment
� Use rewards and reinforcements such as stickers
� Use distraction techniques
� Offer choices rather than ask permission
� Try to maintain child’s routine to decrease loss of rituals
� Normalize routine so feeding can be administered during mealtimes with family
� Remember safety issues: Cover gastrostomy tube site with clothes so childcannot pull the tube; secure nasal or oral tube so child cannot pull it out; atnight, thread tubing through night clothes to keep child from getting tangledup in it
Techniques To Meet Developmental/Social Needs

8
Table 2. Developmental and Social Needs of Infants, Children, and Adolescents, continued
Developmental Stage Techniques To Meet Developmental/Social Needs
Preschooler: 4 to 6 Years
Key: - Initiative vs guilt stage
- Strong imagination, magicalthinking
- Egocentric (self-referenced perspective)
- Mastery of self-care skills
- Modesty emerges
� Develops sense of initiative, positiveself-concept, and conscience (senseof right from wrong, and good frombad)
� Begins to develop peer relationships
� Becomes independent in self-care
� Develops fear of body mutilation
� Becomes sociable and outgoing
� Learns new skillsand games
� Distinguishes sizes
� (See “Toddler,” page 7)
� Foster independence consistent withhome environment
� Consider child’s concern with bodyimage
� Provide positive feedback
� Allow child to help with care and toparticipate by undressing/dressing self
� Explain procedures in terms of child’sperception and frequently reinforce ideathat he or she is not responsible forillness
� Remember safety issues: Cover gastrostomy tube site with clothes sochild cannot pull the tube; secure nasalor oral tube so child cannot pull it out;at night, thread tubing through night
clothes to keep childfrom getting tangledup in it
Special Needs of Children Who Are Tube-Fed

9
Remember safety
issues at night
regarding gastrostomy
tube site and tubing.
����
School Age: 7 to 11 Years
Key: - Industry vs inferiority stage
- Learning rules
- Learning to compete and cooperate with others
- Increasing need for independence, peer relationships, and productivity
- Primary socializing force—peer group
� Develops positive self-esteemthrough skill acquisition andtask completion
� Learns through concreteoperations
� Has more private thoughts
� Develops strong same-sexfriendships
� Develops and increasesvocabulary
� Establish eye contact, use calm approach
� Have parent stay with child
� Use comfort measures such as a blanket orfavorite toy
� Tell child what youare expecting fromher or him
� Explain proceduresin advance
� Answer allquestions
� Use distractiontechniques such as music or videos
� Offer choices rather than ask permission
� Normalize routine so feeding can beadministered during mealtimes with family
� Remember safety issues:At night, thread tubing through nightclothes to keep child from getting tangledup in it
Developmental Stage Techniques To Meet Developmental/Social Needs

Developmental Stage Techniques To Meet Developmental/Social Needs
10
Adolescence: 12 to 18 Years
Key: - Identity vs role-confusion stage
- Rapid and marked physicalchanges
- Fantasy thoughts, adventurous
- Feelings of invincibility,immortality
- Independence
� Has rapid changes in developmentand altered body image
� Develops interest in opposite-sexfriendships
� Develops mature relationships withpeers
� Clarifies values and careerdirection
� Thinks and reasons abstractly
� Establishes autonomy from parents
� Is concerned with effects on bodyimage and peer relationships
Table 2. Developmental and Social Needs of Infants, Children, and Adolescents, continued
� Establish eye contact, use calm approach
� Focus on adolescent; use parents forclarification when necessary
� Tell adolescent what you expect
� Explain procedures in advance
� Answer all questions
� Offer choices rather than ask permission
� Include in decision making and teaching
� Provide positive feedback
� Normalize routine so feeding can beadministered during mealtimes withfamily
� Provide opportunityfor peerinteractions
Special Needs of Children Who Are Tube-Fed

11
Not only do infants,
children, and
adolescents have
different
developmental and
social needs than
adults, they also
differ physically
from adults in ways
that are relevant to
tube feeding.
�
Not only do infants, children, and adolescents have differentdevelopmental and social needs than adults, they also differphysically from adults in ways that are relevant to tube feeding.For instance, an infant’s body weight doubles by 7 months ofage and quadruples by 2 years of age. From 3 to 10 years ofage, an annual weight gain of 2 to 3 kg is expected. Duringadolescence, body weight increases by 7 to 30 kg. GI anatomyand physiology also differ from those of adults (see Table 3).The GI system is not fully mature until a child is approximately2 years of age.

12
Table 3. GI System Anatomy and Physiology of Infants/Children Compared With That of Adults
Implications for FeedingGI Anatomy/Physiology in Infants/Children
� Positive extrusion reflex (0-3 months of age)
� Saliva production (3-4 months of age)
� Gastric enzymes
� Immature muscle tone of lower esophageal sphincter
� Intestinal peristalsis faster
� Gastric emptying time- Newborn 21/2-3 hours- Older infant 3-6 hours
� Stomach capacity- Newborn 10-20 mL- 1 month old 80-150 mL- 1 year old 210-360 mL- 2 year old 500 mL- Adolescent 1500 mL
� Intestines
� Neuromuscular coordination
� Protects infant from ingesting food substancesthat GI system is too immature to digest;gradually disappears by 4-6 months of age
� Increased saliva production begins process ofdigestion in oral cavity and facilitates swallowingof solid foods
� Usually not present in sufficient quantities to aiddigestion until 4-6 months of age; thus, abdominaldistention from gas is common
� Prone to frequent regurgitation (spit-ups) afterfeeding
� Affects ability of digestive tract to break down andabsorb oral intake; thus, less water absorbed
� Need small, frequent feedings
� More liquid consistency of stool
� Less volume and more frequent feedings areneeded because of smaller stomach capacities ininfants and small children
� Growth spurt at 1-3 years of age and in later teenyears; before this age, smaller volume capacity
� Tongue is able to pass solid foods from front toback of mouth by 4-6 months of age
Special Needs of Children Who Are Tube-Fed

hen clinicians decide that a child needs nutritionsupport, they typically determine whether he or shecan be fed enterally (ie, whether the child has a
functioning gut). If so, clinicians must decide the best route offeeding and type of tube to use. A decision tree such as thatillustrated in Figure 1 can help clinicians determine the mostappropriate feeding plan for each child.
13
Clinicians must
decide the best
route of feeding
and type of tube
to use.
����
Selecting Feeding Tubes
W

14
nasoenteric tube feedingenterostomy tube feeding
nasogastrictube
nasojejunaltube
gastrostomyjejunostomy
Can the patient’s GI tract be used safely?
At risk of pulmonary aspiration?
Tube feeding longer than4 to 6 weeks?
Yes No
At risk of pulmonary aspiration?
Yes No
Yes No
Yes No
enteral nutrition parenteral nutrition*
Selecting Feeding Tubes
Figure 1. Decision Making for Tube Feeding
* May still be able to provide small amounts of enteral feeding into small intestine forphysiologic benefit.

15
Choice of tube type is
based on the child’s
physiologic
characteristics—
including age, weight,
disease state or
condition—and the
length of time that tube
feeding may be
needed.
����
As the decision tree suggests, the sites for tube feeding include thestomach and small intestine—either the duodenum or jejunum. Thechoice of tube type is based on the child’s physiologiccharacteristics—including age, weight, disease state or condition—and the length of time that tube feeding may be needed.
Nasoenteric and Oral Enteric FeedingIf the child will be tube-fed for a short time, the nasal route and anasoenteric tube can be used. The three types of nasoenteric tubesare passed through a nostril into one of the three following sites:
� Nasogastric tubes are passed into the stomach
� Nasoduodenal tubes are passed into the duodenum
� Nasojejunal tubes are passed into the jejunum
Administration of feedings into the small intestine may reduce therisk of gastric reflux and aspiration and is useful if poor gastricemptying is present. Oral enteral tubes are most commonly used forpremature infants or infants younger than 4 weeks of age. The tubeis passed through the mouth and into the stomach or intestine.Advantages and disadvantages of both the nasal and oral routes aresummarized in Table 4.

16
Selecting Feeding Tubes
Table 4. Advantages and Disadvantages of Nasoentericand Oral Enteric Feeding
Advantages Disadvantages
� Complications: - Sinusitis- Otitis media- Eustachian tube
dysfunction
� Risk of inappropriate tubeplacement
� < 2-kg infant: compromisedpulmonary function
� Ulceration/erosion of nasalseptum and mucosa
� Bradycardia due to vagalstimulation
� Prolonged use can lead to agrooved palate
� More difficult to secure
� Bradycardia due to vagalstimulation
� More commonly used forpremature infants or infants< 4 weeks of age; they are preferential nosebreathers
� Decrease gagging
� Avoid teeth and palate
� Avoid nasal trauma
� Avoid sinusitis
� Avoid compromised pulmonary function
� Eliminate risk of tube-induced epistaxis
� Nasoenteric tubes
� Oral enteric tubes

17
Careful monitoring and
prevention are the keys
to avoiding
complications when
tube feeding children.
����Enterostomy FeedingWhen enteric feedings are required for an extended period— morethan 4 to 6 weeks—or when passage of a tube through the mouth,esophagus, and cardiac sphincter of the stomach iscontraindicated, either a gastrostomy or jejunostomy may be used.A gastrostomy tube can be placed surgically, with generalanesthesia, through the abdominal wall into the stomach. The tubeis held in place inside the stomach by either a balloon or aninternal bumper. A securing mechanism on the outside of theabdomen is required to prevent the tube from migrating into thestomach. A percutaneous endoscopic gastrostomy tube (PEG) is anonsurgical option using local anesthesia and conscious sedation.The PEG tube is stabilized by some type of support device such asan internal and external bumper or disk to keep it in position.
Minimizing Risk of Tube MigrationTubes can migrate inward when no external fixationdevice is used. Resulting peristalsis can carry thetube through the pylorus, causing an outletobstruction. The nurse can minimize the risk ofinward migration by ensuring that an external tubeholder or skin disk is in place.
Tubes can migrate outward when they are pulled, or when there is stress on the internal bumpercaused by too snug a fit between it and the externalskin disk.
Routine assessment of tube placement and functionis critical for early identification of a problem.

18
Selecting Feeding Tubes
A jejunostomy is the placement of a tube,either by surgery or percutaneousendoscopy, into the jejunum. Theindications for jejunostomy (rather thangastrostomy) are the same as those for anasojejunal tube (eg, the patient is at highrisk of aspiration). Finally, a combinationgastrojejunal tube, which has two lumens,is available. One lumen is for the stomach,and the other for the jejunum. This type oftube can be used for the infant or childwho requires simultaneous gastricdecompression and jejunal tube feedingsbecause of, for instance, gastric outletobstruction.
For the infant or child who requiresfeedings for an extended period, a low-profile gastrostomy tube (also called askin-level or button gastrostomy tube) canbe used. The insertion of a low-profilegastrostomy tube usually requires a well-established gastrostomy site.
This tube has several advantages over theregular gastrostomy tube:
� Lies flat against the abdomen when not in use.
� Is less obvious and may be morecosmetically pleasing.
� Is less likely to be dislodged by tuggingor pulling by the child.
� Allows for increased mobility.
� Is fully immersible in water.
� Has a one-way valve to minimize refluxand eliminate the need for clamping.
A low-profile tube also is stabilized bysupport devices such as an internalballoon or bumper and external skin diskto keep it in position. There are also skin-level devices used for jejunal access.

19
For the infant or child
who requires feedings
for an extended period,
a low-profile
gastrostomy tube can
be used.
����
There are two contraindications to using a low-profilegastrostomy tube:
� Need for frequent gastric decompression- The child has an anatomic or medical condition suchas partial bowel obstruction that affects his/her needfor decompression. The amount of decompression achild requires should be assessed before it isdetermined whether a low-profile tube is appropriate.
- The internal bumper/balloon does not reach thedependent part of the stomach where secretions tendto pool.
� Morbid obesity
Protecting Tube From Inadvertent RemovalEarly, traumatic tube removal (before the stoma tract hasmatured) can have severe consequences, including tissuelaceration and trauma. The nurse is responsible for protectingthe tube and educating the caregivers about the implicationsof traumatic tube removal.
Below are some methods for protecting the tube fromremoval:
� Cover the tube with dressings
� Apply mittens to the child’s hands
� Use an abdominal binder, ostomy binder, or specially designed clothes

20
arious formulas are available forenteral tube feedings for infantsand children. These formulas
contain the protein, carbohydrate, fat,vitamins, minerals, and water required tomeet infants’ and children’s daily nutritionneeds. Several factors should beconsidered when selecting an enteralformula: age, clinical condition, nutrientneeds of the child, feeding tube capacity,
absorptive capacity of the intestine, GItolerance, cost, and ease of formulapreparation. Commercial formulas areoften recommended because their lowviscosity allows delivery through small-bore tubing. Home-prepared formulas maybe less expensive but are more time-consuming to prepare, usually requiredelivery by large-bore tubing, and aremore susceptible to contamination.
Selecting a Formula
V

21
roper preparation and storage of tube-feeding formulas areessential to successful tube feeding. The nurse shouldinstruct the child’s caregivers on how to prepare and store
formulas properly. Table 5 describes the steps that caregiversshould take to ensure that tube feeding is safe and effective.
Table 5. Steps in Preparing and Storing Tube-Feeding Formulas and Their Rationale
Proper
preparation and
storage of tube-
feeding formulas
are essential
to successful
tube feeding.
����
Steps Rationale
Preparation and StorageRequirements
P
1. Wash hands thoroughly with soap andwater before handling formula, tubing,or feeding tube
2. Handle ready-to-use liquid formula in asafe manner
� Store at room temperature until container opened
� Check expiration date on container� Check correct formula, eg,
concentration, additives (avoid adding water or other substances whenever possible)
� Shake container well� Sanitize top of container before
opening following hospital protocol� Write date and time on opened
container� Cover and refrigerate unused
formula� Discard unused formula after
48 hours*� If using ready-to-hang (RTH) formula
(formula in prefilled container), use within 36 hours*
� Follow instructions on formula container
� Minimize risk ofmicroorganismcontamination of bothformula and equipment
� Maintain productquality
� Ensure that formula ismixed
� Maintain productquality
� RTH formula reducesrisk of contaminationdue to less handling
* or in accordance with manufacturer’s recommendations and/or hospital policy

22
Preparation and Storage Requirements
Table 5. Steps in Preparing and Storing Tube-FeedingFormulas and Their Rationale, continued
Steps Rationale
3. Handle powdered products/nonsterile liquidproducts (hospital- or home-prepared product,reconstituted powdered product, and ready-to-useproducts to which additives have been added in a safemanner)
� Store in cool, dry place until container is opened� Sanitize all equipment and surfaces used for formula
preparation following hospital protocol
� Sanitize container before opening� Mix exact amount of powder, liquid, and other
additives (if any); mix well� Pour prepared formula into clean container� Write date and time on container� Cover and refrigerate unused formula� Discard unused formula after 24 hours*� Prepared formula should be hung no longer
than 4 hours*
� Maintain product quality� Reduce risk of contamination
(risk is higher with powdered or nonsterile liquid products because of increased handling required)
� Reduce risk of contamination
* or in accordance with manufacturer’s recommendations and/or hospital policy
23
The nurse should help
instruct the child’s
caregivers on the
proper procedures for
administering tube
feedings and caring for
tubes.
����
23
Administering Tube Feedingsto Children
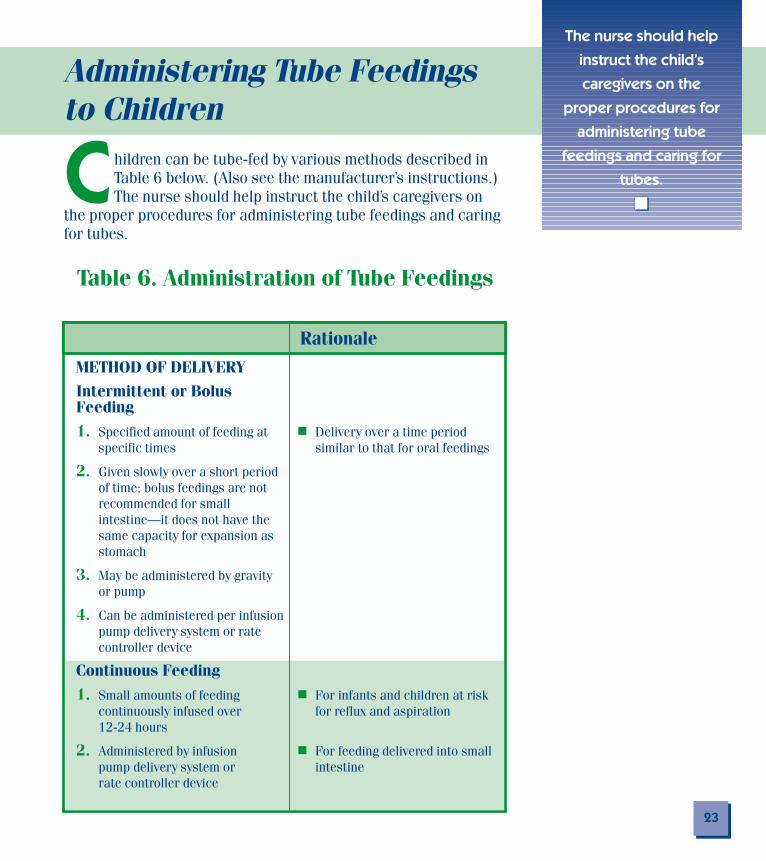
hildren can be tube-fed by various methods described inTable 6 below. (Also see the manufacturer’s instructions.)The nurse should help instruct the child’s caregivers on
the proper procedures for administering tube feedings and caringfor tubes.
Table 6. Administration of Tube Feedings
C
Rationale
METHOD OF DELIVERY
Intermittent or Bolus Feeding
1. Specified amount of feeding at � Delivery over a time period specific times similar to that for oral feedings
2. Given slowly over a short period of time; bolus feedings are not recommended for small intestine—it does not have the same capacity for expansion as stomach
3. May be administered by gravity or pump
4. Can be administered per infusionpump delivery system or ratecontroller device
Continuous Feeding
1. Small amounts of feeding � For infants and children at riskcontinuously infused over for reflux and aspiration12-24 hours
2. Administered by infusion � For feeding delivered into smallpump delivery system or intestinerate controller device

RationaleNASOENTERIC OR ORAL ENTERICTUBE-FEEDING PROCEDURESNote: Qualified nurses may place tubes in thismanner; however, it is important to check theorganization’s policy to determine whetherphysician placement is required.
1. Discuss procedure with child in a � Child will understand what to expectdevelopmentally appropriate manner andinform the child’s caregivers
2. Assemble equipment� Appropriate feeding tube � Enhance safety and effectiveness
Weight Tube Size≤ 2 kg 5 French3-9 kg 8 French10-20 kg 10 French20-30 kg 12 French30-50 kg 14 French> 50 kg 16 French
� Tubing generally made from polyurethane � Biocompatible materials are soft, smooth,or silicone materials flexible, for patient comfort
� Polyvinyl chloride tubes (PVC) become � Can cause skin necrosis or intestinalstiff and nonpliable with age and perforationsexposure to acids
� Guidewire or stylet, if applicable � Prevent soft and flexible tube from coiling(removed only after tube placement has during insertionbeen verified)
� Hypoallergenic tape and transparent � Secure tube in place; reduce skin irritationocclusive dressing
� Syringe � Can be used to aspirate stomach contents,inject air for tube placement, hold formula
� Formula at room temperature � Help prevent abdominal cramping or discomfort
� RTH spike set, if appropriate
� Water or water-soluble lubricant (use � Lubricate tube for ease of insertionwater only for infants)
� Stethoscope � Determine correct tube placement in stomach
� Gloves, nonsterile � Prevent possible contact with body fluids24
Table 6. Administration of Tube Feedings, continued
Administering Tube Feedings to Children

25
Rationale
3. Wash hands and put on gloves � Minimize risk of microorganismcontamination of both formulaand equipment
Inserting the Tube
4. Position infant or child� Infant: supine with head of � Elevation allows gravity to
bed elevated or held in facilitate tube passageparent’s arms with head onparent’s shoulder
� Older child: sitting up withhead slightly flexed
5. Restrain infant or young child, asneeded
� Have parent hold child
� Use blanket for swaddling/mummy wrap
6. Measure length of tubing to beinserted (two methods)
� Using tube, measure � To approximate length of tube distance from nose to needed to reach stomachearlobe, then to end ofxiphoid process (mark tubewith tape or indelible ink atpremeasured mark)

26
Table 6. Administration of Tube Feedings, continued
Administering Tube Feedings to Children
Rationale
7a. Insert nasogastric or orogastric tubing
� Lubricate tube with water (for infant � Facilitate passage of tube< 6 months old) or with water-solublelubricant
� Have infant suck on pacifier during � Facilitate passage of tube during insertion and have older children swallow during insertion
� Insert tube slowly through either mouth � Prevent pressure on any structures causingor nostril to premeasured mark using bleeding; prevent perforationgentle pressure; do not force tube
� If tube meets resistance, withdraw it andreinsert through other nostril
� Withdraw tube immediately if infant or � Assess to ensure tube is not insertedchild experiences any change in into trachearespiratory status (coughs excessively,chokes, nasal flaring, retractions,cyanosis, tachypnea)
If symptoms are present, notify thephysician.
7b. Insert oro- or nasojejunal or oro- ornasoduodenal tube
� Measure length of tubing to be inserted � To approximate length of tube needed toby measuring distance from bridge of reach duodenum or jejunumnose to ear, then to ankle; or from thebridge of nose to 10 cm below umbilicus(mark tube with tape or indelible ink atpremeasured mark)
� Follow technique for insertion of anasogastric or orogastric tube
� Position child on his/her right side � Facilitate passage through pylorus of stomachand into small intestine
� Allow the tube to advance over severalhours until the correct length of tube isinserted (may have tungsten weightswithin tubing)

27
Assess proper tube
placement by:
- aspiration
- auscultation
- checking tube position
- testing pH of aspirate
- abdominal radiograph
����
8. Assess proper tube placement: Methods (may need more than one for verification)
� Aspiration: With syringe, aspirate gastric contents
Gastric contents: white, clear, or yellow
Intestinal contents: yellow or green
Respiratory contents: clear, off-white, or yellow
� Auscultation: Listen over left upper quadrant of abdomen while injecting air into the tube
1-5 mL air for infant/young child
5-20 mL air for adolescent
� Tube position: Check location of premarked tubing (where tube exits nose or mouth)
� pH paper testing: Check pH of aspirate (Organization’s protocol should be followed) pH should be <4.0 for gastric contents
pH should be >6.0 for intestinal contents
� Abdominal radiograph(Requires order from authorized licensed practitioner)
� Assess tube placement by examination of aspirate
Note: Absence of gastric contents does not necessarily indicate improper position; stomach may be empty, the tube may not be in contact with stomach contents, or the soft tube may have collapsed under the pressure of aspiration
� Assess tube placement; should hear gurgling or a “swoosh” if tube is properly in stomach
Note: Sounds may be audible if tube is above the gastroesophageal sphincter
Note: Sounds generated through small-bore tubing can be unreliable
� Can detect tube migration
Note:Does not ensure that distal portion of tube is in intended position
� Assess tube placement by examination of pH of aspirate
Note: Antacids, gastric acid inhibitors, and reflux of intestinal bile alter pH
� Definitive method for tube placement
Rationale

28
Rationale
9. Secure tube
� Place a small dressing on cheek, not on � Prevent skin breakdown; avoid pressure andbridge of the nose, then secure tube ulceration on the nasal cartilageonto this dressing with tape
� Older child: Use a pin and a rubber band � Prevent dangling and reduce accidental to secure tube to clothing tube dislodgment
� Label a continuous indwelling tube with � Document length of time tube has been ininsertion date and time place
10. Changing tubes
� Continuous indwelling tubes aredesigned to reduce manipulation andstimulation of the larynx but can affectswallowing and breathing
� Orally placed feeding tubes may be � Reduce risk of gastroesophageal refluxremoved between feedings because tube partially opens the lower
esophageal sphincter
� Tubes made of PVC need to be changed � Promote patient comfort and reduce risk ofevery 2-3 days; they become stiff and complicationsnonpliable
� Tubes made of polyurethane or siliconematerials can remain in place up to3-4 weeks
� Frequency of tube changing is based ontype of tube and specific hospital orhome care policy
11. Removing tube
� Type of tube dictates removal methodPhysician’s orders should designatehow tube should be removed andwho should remove it
Table 6. Administration of Tube Feedings, continued
Administering Tube Feedings to Children
29
Rationale
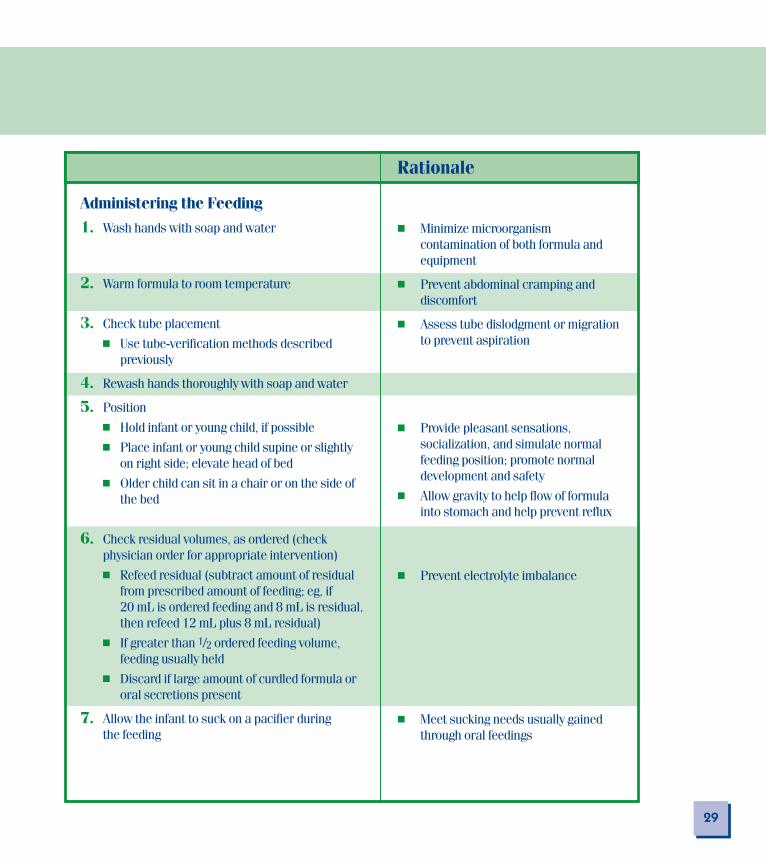
� Minimize microorganismcontamination of both formula andequipment
� Prevent abdominal cramping anddiscomfort
� Assess tube dislodgment or migrationto prevent aspiration
� Provide pleasant sensations,socialization, and simulate normalfeeding position; promote normaldevelopment and safety
� Allow gravity to help flow of formulainto stomach and help prevent reflux
� Prevent electrolyte imbalance
� Meet sucking needs usually gainedthrough oral feedings
Administering the Feeding
1. Wash hands with soap and water
2. Warm formula to room temperature
3. Check tube placement
� Use tube-verification methods described previously
4. Rewash hands thoroughly with soap and water
5. Position
� Hold infant or young child, if possible
� Place infant or young child supine or slightly on right side; elevate head of bed
� Older child can sit in a chair or on the side of the bed
6. Check residual volumes, as ordered (checkphysician order for appropriate intervention)
� Refeed residual (subtract amount of residual from prescribed amount of feeding; eg, if 20 mL is ordered feeding and 8 mL is residual, then refeed 12 mL plus 8 mL residual)
� If greater than 1/2 ordered feeding volume, feeding usually held
� Discard if large amount of curdled formula or oral secretions present
7. Allow the infant to suck on a pacifier during the feeding

30
Rationale
8a. Intermittent feedings
� Remove cap from feeding port of feeding tube or remove syringe from tube
� Remove plunger from syringe and attachsyringe to tubing
� Clamp the tubing
� Pour formula into syringe and unclamp � Ensure patient feeding tolerancetube; allow formula to flow slowly bygravity over 20-60 minutes into tubing
� Flow is regulated by raising and loweringsyringe
� The period of time for flow of formulashould be similar to that of oral feeding:
- 1 mL/minute flow for premature andsmall infants
- 10 mL/minute flow for older infantsand children
� Do not let tube run dry � Prevent air from entering stomach
� Infants: Clear tubing of formula byinjecting 1 mL air
� Older children: Clear tubing of formula byflushing the tubing with water, theninjecting 1-5 mL air
� Cap or clamp indwelling tubing � Prevent leakage of formula
� If tubing is removed after each feeding, � Help prevent aspiration by preventing pinch tubing firmly, then withdraw escape of fluid as tube is withdrawnit quickly
� Burp infant � Allow air to escape
� Keep infant and young child positioned � Minimize risk of regurgitation andon right side with head elevated aspiration
Table 6. Administration of Tube Feedings, continued
Administering Tube Feedings to Children

Rationale
31
8b. Continuous feedings
� Using sanitary technique, fill feeding container with formula and clamp tubing
or� Spike the port on the RTH closed-
system container; close clamp before inverting container
� Prime to clear the air from tubing, then connect it to feeding tube
� Infuse formula using a pump at prescribed volume and rate
� Do not add fresh formula � Help prevent contamination ofto remaining formula feeding
� Change formula in feeding � Reduce risk of contaminationcontainer or syringe every 8-12 hours; powdered formula, every 4-6 hours
� Change RTH formula at least every 24 hours
� Change feeding set and syringe every 36 hours
� Check tube placement andresidual volume every 4 hours
� Keep infant or young child � Decrease incidence of reflux andon his/her right side with aspiration; facilitate gastrichead of bed elevated emptying
� Older child or adolescent can sit in chair, or head of bed can be elevated at least 30˚

32
Rationale
GASTROSTOMY OR JEJUNOSTOMYTUBE-FEEDING PROCEDURES1. Discuss procedure with child in a � Help child understand what to expect and
developmentally appropriate manner and gain his/her cooperationinform the child’s caregivers
2. Assemble equipment
� Syringe with adapter or catheter-tipsyringe
� Formula or liquid food at room � Help prevent abdominal crampingtemperature
� Pour container, if appropriate
� Water; use sterile water as irrigant for � Help prevent microbial contaminationinfants < 6 months old and tap ordistilled water for older children
� RTH set, if appropriate
� Pump and tubing, if appropriate
� Gloves, nonsterile � Prevent possible contact with body fluids
Administering the Feeding1. Position
� Hold infant or young child, if possible � Provide socialization; cuddle to simulatenormal feeding position
� Place infant or young child supine or � Allow gravity to help flow of formula intoslightly on right side; elevate head of bed stomach and help prevent reflux
� Older child can sit in chair, or head ofbed can be elevated at least 30˚
2. Wash hands with soap and water � Minimize risk of microorganismcontamination of both formula and equipment
Table 6. Administration of Tube Feedings, continued
Administering Tube Feedings to Children

33
Rationale
3. Check tube placement
� Incremental measurements � Detect migration ofon tube located at entrance tubeinto stoma tract should be noted against recordedincremental measurementindicating correct tubeposition
� If tube has no incremental � Detect migration ofmeasurements, note tubeindelible ink mark indicatinglocation of tube entranceinto stoma tract
4. Warm formula to room � Help prevent abdominaltemperature cramping and discomfort
5. Check for residual volume byattaching empty syringe andobserving backflow of stomachcontents (see page 29, Step 6)
6. Provide infant with pacifier � Meet sucking needs usuallygained through oral feedings
7. Intermittent feedings
� See nasoenteric or oral entericintermittent feeding steps, page 30
� Older children: After feeding is � Maintain tube patencycompleted, flush the tube with10-20 mL water, unless directed otherwise by physician
� Leave tube open for � Allow air to escape5-10 minutes
� Clamp tube � Prevent escape of formula from tube
� Position infant or young � Facilitate gastric emptyingchild on right side withhead of bed elevated

34
Table 6. Administration of Tube Feedings, continued
Administering Tube Feedings to Children
Rationale
8. Continuous feedings
� See nasoenteric or oral enteric continuousfeeding steps, page 31
� Flush tube with water every 4-6 hours � Maintain tube patency and prevent fluidand monitor total fluid volumes overload
LOW-PROFILE GASTROSTOMY TUBEFEEDING PROCEDURES1. Discuss procedure with child in a � Help child understand what to expect and
developmentally appropriate manner and gain his/her cooperation inform the child’s caregivers
2. Assemble equipment
� Low-profile gastrostomy tube and extension tube
� Syringe
� Formula or liquid food at room � Help prevent abdominal cramping or discomforttemperature
� Pour container, if appropriate
� Water; use sterile water as irrigant for � Help prevent microbial contaminationinfants <6 months old and tap ordistilled water for older children
� RTH set, if appropriate
� Pump and tubing, if appropriate
� Decompression tube, if appropriate; usebefore feeding if abdominal distention ispresent
� Gloves, nonsterile � Prevent possible contact with body fluids
35
Rationale
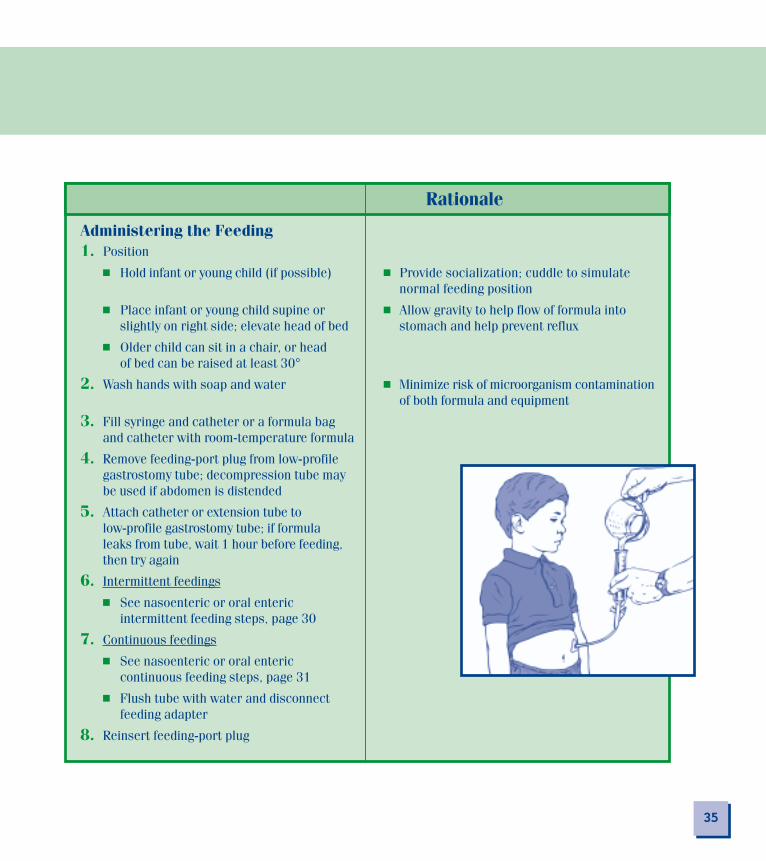
Administering the Feeding1. Position
� Hold infant or young child (if possible) � Provide socialization; cuddle to simulate normal feeding position
� Place infant or young child supine or � Allow gravity to help flow of formula intoslightly on right side; elevate head of bed stomach and help prevent reflux
� Older child can sit in a chair, or head of bed can be raised at least 30°
2. Wash hands with soap and water � Minimize risk of microorganism contamination of both formula and equipment
3. Fill syringe and catheter or a formula bag and catheter with room-temperature formula
4. Remove feeding-port plug from low-profile gastrostomy tube; decompression tube may be used if abdomen is distended
5. Attach catheter or extension tube to low-profile gastrostomy tube; if formula leaks from tube, wait 1 hour before feeding, then try again
6. Intermittent feedings
� See nasoenteric or oral enteric intermittent feeding steps, page 30
7. Continuous feedings
� See nasoenteric or oral entericcontinuous feeding steps, page 31
� Flush tube with water and disconnect feeding adapter
8. Reinsert feeding-port plug

36
ome children need to receive medications through their feeding tube. When that isthe case, the medications should be administered as ordered, and the children’scaregivers should be instructed on the proper administration techniques. The
following guidelines in Table 7 below can help minimize the risk of complications.
Administering Medications With Feedings
STable 7. Administering Medications via a Feeding Tube
Rationale
1. Do not mix medications with feedings � Reduce risk of clogging; some medications are incompatible with formula
2. Give medications either before or after � Some medications should be administered onfeedings an empty stomach
Consult with pharmacist regardingscheduling medications and feedings
3. Give medications in liquid form, if possible
4. Tablets should be crushed and dissolved in � Prevent tube cloggingsolution (except enteric-coated and time-release tablets)
Consult with pharmacist regardingappropriate solution for dissolvingmedications
5. Administer one medication at a time; do not � Reduce tube clogging; medications may becombine medications; flush tubing with water incompatiblebetween administration of each medication
6. Flush tubing with water before and after � Reduce potential for clogging or obstructingmedication administration tubing with medication fragments

37
Good care of the tube
site is essential for
successful tube feeding
and for the comfort of
the child.
����
Rationale
1. Frequency for changing tube is based on type of tubing and specific organization policies
� Alternate nostrils for tube � Decrease risk of irritationinsertion
� Clean nostrils and tubing � Prevent crusting ofwith cotton-tipped secretionsapplicator and water
� Change tape as needed
2. Observe nostrils for � Signs of necrosis or� Pressure areas ulceration; prevent� Redness complications� Irritation� Pain
If symptoms are present,notify physician
3. Apply cream or water-soluble � Provide comfort; decrease riskointment to nostrils and lips of chapping and trauma
4. Provide mouth care frequently � Provide comfort; prevent(older children can brush teeth) infection in oral cavity
ood care of the tube site is essential for successful tubefeeding and for the comfort of the child. Tables 8, 9, and10 summarize the care steps and their rationale.
Tube-Site Care
Table 8. Site Care for Nasoenteric and Oral Enteric Feeding Tubes
G

38
Tube-Site Care
There are two phases of care and management for gastrostomy and jejunostomy tube sites—initialpostplacement and long-term management. With initial postplacement, assessment and care areprovided frequently, generally every 4 hours, and the results documented. The nurse must knowthe normal skin response to tube insertion so that initial postplacement deviations can be detected early.Typically, the tube site has erythema, mild cellulitis, and serous or serosanguineous drainage. It is normal for the patient to experience some mild discomfort or pain. However, the followingsigns and symptoms should be reported to the physician: increased tenderness, firmness, localswelling, fever, induration, bleeding, gastric leakage, purulent drainage, and moderate to severe pain.Care to keep the tube secured and the site clean and dry is especially important immediately aftertube placement. The site often is cleaned with a nontoxic skin cleanser, but an antiseptic orantibacterial agent may be ordered. Dressings may be used initially if drainage is present or ifordered by the physician.Tables 9 and 10 summarize site care for long-term management.
Table 9. Site Care for Gastrostomy and Jejunostomy Feeding Tubes
Rationale1. Wash hands with soap and water � Minimize risk of microorganism
contamination of both formula and equipment
2. Observe the stoma site for � Help prevent irritation, infection
� Redness (initially may be sign of healingbut may indicate an infection or tape irritation)
� Skin breakdown (from tape, leakage, ortube movement)
� Bleeding
� Leakage of fluid around opening (cathetermay need to be repositioned or replaced)
� Pain, swelling, fever, yellow discharge(signs of infection)
� Yellow-green discharge (requiresappropriate cleansing only if withoutother signs of infection)If symptoms are present, notify physician.

39
Care to keep the tube
secured and the site
clean and dry is
especially important
immediately after tube
placement.
����Rationale
3. Cleanse established stoma site � Prevent irritation of stoma sitedaily and as needed with soap from too much cleaning and tooand warm water many chemical applications
� Use spiral pattern beginning � Prevent contaminationat stoma site and workingoutward, from clean area todirty area
� Follow with warm water � Remove soap to avoid skinrinse irritation
� Thoroughly pat dry � Prevent skin irritation
4. Cleanse and dry outside of tube with soap and water
� Follow with warm water rinse
� Thoroughly pat dry
5. Avoid covering stoma and tube � May cause friction and moisturesite with ointment or occlusive retention and may promotedressing granuloma formation
Consult with physician or ETnurse for orders.If additional skin protection is � Protect skin from leakage;needed at stoma site because of decrease risk of skin irritationperitubular leakage, try the and breakdownfollowing:
� Make a diagonal cut half-way into a 2" x 2" or 4" x 4"gauze pad, then place itaround the stoma and tube
� Change gauze 1-2 times per � Avoid trapped moisture;day and when soiled decrease risk of skin irritation
� Apply waterproof barrier � Avoid trapped moisture;product to the skin decrease risk of skin irritation
� If hypergranulation tissue ispresent, silver nitrateapplications may be indicated.
Requires physician order

Rationale6. Secure tube � Minimize rotation and movement and reduce
� Place secured tube under clothing risk of skin irritation and tube dislodgment
� Use flexible net dressing around abdomen � Reduce risk of tube manipulation and/orand over tubing unintentional removal
� Note incremental marking of tube at � Reduce risk of tube manipulation and/orstoma exit site or mark level on tubing unintentional removalwith indelible ink; suspect migration if � Detect and prevent migration of tubingmark disappears or moves farther awayfrom stoma site
If migration is suspected, notifyphysician for radiologic confirmation.
� Check position of external disk or � Prevent tube migration; decrease risk of tractsupportive device enlargement; prevent tissue necrosis
40
Tube-Site Care
Table 9. Site Care for Gastrostomy and Jejunostomy Feeding Tubes, continued

41
Table 10. Site Care for Low-ProfileGastrostomy Feeding Tubes
Rationale
1. Wash hands with soap and water � Minimize risk of microorganismcontamination of both formulaand equipment
2. Observe the stoma site for � Help prevent irritation, infection
� Redness (initially may be sign of healing but may indicate an infection or tape irritation)
� Skin breakdown (from tape,leakage, or tube movement)
� Bleeding
� Leakage of fluid aroundopening (tube may need tobe repositioned or replaced)
� Pain, swelling, fever, yellow discharge
� Yellow-green discharge (requires appropriate cleansing only if without other signs of infection)
If symptoms are present,notify physician
3. Cleanse around stoma site with soap and warm water; can be done with bath
4. Rotate tube in full circle during � Facilitate complete cleansing andcleansing prevent skin breakdown from � Check position of external pressure of tube; prevent tube from
disk or supportive device imbedding in gastric mucosa(disk or supportive device � Prevent tube migration; decreaseshould be approximately risk of tract enlargement;1/4 inch above skin level) prevent tissue necrosis
5. Dry stoma site thoroughly beforecovering area with clothes

ven when good tube-feeding care is provided, problems can emerge. Tube-feedingproblems stem from a number of sources—eg, from mechanical, physical,metabolic, or developmental factors. Table 11 below describes these problems.
The physician should be notified of any adverse event.
Table 11. Potential Problems With Pediatric Tube Feeding
Problem Source
Specific to Nasoenteric Tubes
� Nasal bleeding � Direct trauma from tube insertion
� Laryngeal edema � Mucosal irritation from tubeinsertion
� Nasal ulceration or necrosis � Pressure against nasal cartilage
� Sinusitis � Obstruction of sinus drainage
� Otitis media � Middle ear irritation and infection
� Esophageal perforation � Feeding tube penetrated esophagusduring insertion
42
Potential Problems With Pediatric Tube Feeding
E
Even when good
tube-feeding care is
provided, problems
can emerge.
����
43
Problem SourceSpecific to Gastrostomy orJejunostomy Tubes
� Pressure necrosis � Positioning external skin- Skin irritation/ disk or support device
ulceration too close to skin- Leakage- Bleeding
� Hypergranulation tissue � Body’s reaction to a- Usually nonpainful “foreign object” from- Red, fleshy tissue prolonged or excessive
movement of tube and/ortrapped moisture
� Tube-tract enlargement � Excess tube movement;- Enlarged opening tube too large or stiff;- Leakage tissue erosion- Skin irritation
� Buried bumper or disk � Bumper or disk- Bumper or disk does burrowing into gastric
not move freely mucosa or lodged intract, leading to pressure necrosis

44
Potential Problems With Pediatric Tube Feeding
Table 11. Potential Problems With Pediatric Tube Feeding, continued
Problem Source
Mechanical: General
1. Tube migration � Nasoenteric or oral enteric tube:usually from either perforation ormisdirection
� Outward migration: � Gastrostomy or jejunostomy:pressure necrosis, leakage, pain balloon deflation or rupture;
excess tension; migration outward into peritoneal space
� Inward migration: � No external skin disk or supportobstruction; blockage of pylorus device- Vomiting- Increased abdominal girth- Leakage- Pain
2. Tube occlusion/clogging � Tube too small for highly viscous or fiber formulas or medication;inadequate flushing after formula or medication; kinking of tube

45
Problem Source
Physical: General
� Nausea � Poor gastric emptying
� Abdominal cramping or discomfort � Formula cold or infused rapidly
� Abdominal distention � Tubing not primed with formula before administration; a largeamount of air is infused into feeding tube and stomach
� Diarrhea or dumping syndrome � Rapidly delivered formula, or hypertonic formula or medications
� Constipation � Long-term tube feedings without fiber; inadequate hydration
� Aspiration � Decreased cough or gag reflex; decreased gastric emptying; reflux problem
� Infection � Contaminated formula or equipment; local infection at stoma site

46
Potential Problems With Pediatric Tube Feeding
Table 11. Potential Problems With Pediatric Tube Feeding, continued
Careful monitoring and prevention are the keys to avoiding complications when tubefeeding children. It is important for clinicians to be knowledgeable about the routine care ofthese children, including insertion techniques, skin care, tube removal, and documentation,and to communicate proper procedures to the children’s caregivers.
Problem Source
Metabolic: General
� Electrolyte imbalance � Inadequate or excess water intake;excessive GI fluid losses; renalinsufficiency
� Dehydration � Underlying medical conditions or notreceiving adequate hydration; mostchildren need 11/2 oz fluid per bodyweight per day
� Overhydration � Underlying medical conditions or notreceiving appropriate hydration
� Hyperglycemia � Metabolic stress; insufficient insulinproduction or utilization; excessivecarbohydrate intake
Developmental: General
� Food aversion � Frequently occurs with smallchildren due to limited or lack ofopportunities for oral feedings

47
References
1. Ashwill JW, Droske SC: Nursing Care of Children: Principles and Practice. Philadelphia: WB Saunders Co, 1997.
2. Ball J, Bindler R: Pediatric Nursing: Caring for Children. Norwalk, Conn: Appleton & Lange, 1995.
3. Bowden VR, Dickey SB, Greenberg CS: Children and TheirFamilies: The Continuum of Care. Philadelphia: WB Saunders Co, 1998.
4. Committee on Nutrition, Kleinman RE (ed): Pediatric Nutrition Handbook, ed 4. Elk Grove Village, Ill: AmericanAcademy of Pediatrics, 1998.
5. Ellett MLC, Maahs J, Forsee S: Prevalence of feeding tubeplacement errors and associated risk factors in children. MCN 1998;23(5):234-239.
6. Lord LM: Enteral devices. Nurs Clin North Am 1997;32(4):685-704.
7. Luckmann J (ed): Saunders Manual of Nursing Care. Philadelphia: WB Saunders Co, 1997.
8. Marchand V, Baker SS, Baker RD: Enteral nutrition in the pediatric population. Gastrointest Endosc Clin North Am 1998;8(3):669-703.
9. Nardella MT: Practical tips on tube feedings for children. Nutr Focus 1995;10(2):1-8.
10. Pediatric Liaison Network: Caring for Kids: A Developmental Approach to Pediatric Care. Columbus, Oh: Children’s Hospital, 1996.
11. Pulhamas MS: Alterations in metabolic function, in Votroubek WL, Townsend JL (eds): Pediatric Home Care, ed 2. Gaithersburg, Md: Aspen, 1997, pp 155-191.
12. Repucci AR: (1996). Pediatric gastroenterology, in Taeusch HW, Christiansen RO, Buescher ES (eds): Pediatric and Neonatal Tests and Procedures. Philadelphia: WB Saunders Co, 1996, pp 477-552.

48
References
13. Shiao SP, Novotny DL: The features of different gastric tubes used in nurseries. Neonatal Network 1997;17(4):78-79.
14. Skale N: Manual of Pediatric Nursing Procedures. Philadelphia: JB Lippincott, 1992.
15. Speer KM, Swann CL: The Addison-Wesley Manual of Pediatric Nursing Procedures. Redwood, Ca: Addison-Wesley Nursing, 1993.
16. Wong DL: Whaley & Wong’s Clinical Manual of Pediatric Nursing, ed 4. St Louis: Mosby, 1996.
17. Wong DL: Whaley & Wong’s Essentials of Pediatric Nursing, ed 5. St Louis: Mosby, 1997.

62276/SEPTEMBER 2001 LITHO IN USA