Embed Size (px)
Citation preview

TCT 2011 | San Francisco, CA | November 10, 2011TCT 2011 | San Francisco, CA | November 10, 2011
Two-Year Outcomes of Transcatheter Aortic Two-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in “Inoperable” Valve Replacement (TAVR) in “Inoperable” Patients With Severe Aortic Stenosis: Patients With Severe Aortic Stenosis: The PARTNER TrialThe PARTNER Trial
Raj R. Makkar, MDRaj R. Makkar, MDOn behalf of The PARTNER Trial InvestigatorsOn behalf of The PARTNER Trial Investigators

DisclosuresDisclosures
Raj R. Makkar Raj R. Makkar is a principal site investigator for The is a principal site investigator for The PARTNER Trial (US) for Edwards Lifesciences and PARTNER Trial (US) for Edwards Lifesciences and is national principal investigator for the St Jude is national principal investigator for the St Jude TAVR study. He has received consulting fees, grant TAVR study. He has received consulting fees, grant support and lecture fees from Medtronic, equity from support and lecture fees from Medtronic, equity from Entourage Medical Technologies and grant support Entourage Medical Technologies and grant support from St Jude Medical.from St Jude Medical.

Background (1)Background (1)
• Transcatheter aortic valve replacement (TAVR) Transcatheter aortic valve replacement (TAVR) is the recommended treatment for is the recommended treatment for “inoperable” patients with severe aortic “inoperable” patients with severe aortic stenosis (AS), based upon 1-year results of stenosis (AS), based upon 1-year results of The PARTNER Trial which demonstrated The PARTNER Trial which demonstrated reduced mortality and improved quality of life.reduced mortality and improved quality of life.
• However, whether clinical benefit and valve However, whether clinical benefit and valve performance are sustained beyond one year is performance are sustained beyond one year is unknown and longer term outcomes will unknown and longer term outcomes will importantly alter clinical practice decisions.importantly alter clinical practice decisions.
3

Background (2)Background (2)
• Transcatheter Aortic Valve Replacement (TAVR) is the standard of care for inoperable patients with severe aortic stenosis (AS), demonstrating 1-year outcomes of the PARTNER Trial, offering reduced mortality and improved quality of life.
4
Published October 2010Published October 2010

ObjectivesObjectives
• To evaluate the clinical outcomes of To evaluate the clinical outcomes of TAVR compared to standard therapy at 2 TAVR compared to standard therapy at 2 years in “inoperable” aortic stenosis years in “inoperable” aortic stenosis patients.patients.
• To assess valve hemodynamics and To assess valve hemodynamics and durability using echocardiography.durability using echocardiography.
• To perform subgroup analyses to better To perform subgroup analyses to better define the impact of co-morbidities on define the impact of co-morbidities on outcomes.outcomes.
5

n = 358InoperableInoperable
StandardTherapyn = 179
StandardTherapyn = 179
ASSESSMENT: Transfemoral
Access
ASSESSMENT: Transfemoral
Access
TF TAVRn = 179
TF TAVRn = 179
Primary Endpoint: All-Cause Mortality Over Length of Trial (Superiority)
Primary Endpoint: All-Cause Mortality Over Length of Trial (Superiority)
1:1 Randomization1:1 Randomization
VS
TF TAVRTF TAVR AVRAVR
Primary Endpoint: All-Cause Mortality (1 yr)(Non-inferiority)
Primary Endpoint: All-Cause Mortality (1 yr)(Non-inferiority)
TA TAVRTA TAVR AVRAVR VS
VS
PARTNER Study DesignPARTNER Study Design
Symptomatic Severe Aortic StenosisSymptomatic Severe Aortic Stenosis
ASSESSMENT: High-Risk AVR Candidate3,105 Total Patients Screened
ASSESSMENT: High-Risk AVR Candidate3,105 Total Patients Screened
Total = 1,057 patients
2 Parallel Trials: Individually Powered
n = 699 High-RiskHigh-Risk
ASSESSMENT: Transfemoral
Access
ASSESSMENT: Transfemoral
Access
High-Risk TAHigh-Risk TAHigh-Risk TFHigh-Risk TF
1:1 Randomization1:1 Randomization1:1 Randomization1:1 Randomization
6

Inclusion CriteriaInclusion Criteria
• Severe calcific aortic stenosis defined as echo Severe calcific aortic stenosis defined as echo derived valve area of < 0.8 cmderived valve area of < 0.8 cm22 (EOA index < 0.5 (EOA index < 0.5 cmcm22), and mean gradient > 40 mmHg or jet velocity ), and mean gradient > 40 mmHg or jet velocity > 4.0 m/s.> 4.0 m/s.
• NYHA functional class II or greater.NYHA functional class II or greater.
• Risk of death or serious irreversible morbidity of Risk of death or serious irreversible morbidity of AVR as assessed by cardiologist and two AVR as assessed by cardiologist and two surgeons must exceed 50%.surgeons must exceed 50%.
Surgeons must agree and attest that before Surgeons must agree and attest that before PARTNER these patients would not have received PARTNER these patients would not have received AVR treatment!AVR treatment!
7

Key End-Points for 2 Year AnalysisKey End-Points for 2 Year Analysis
• All cause mortalityAll cause mortality
• Cardiac mortalityCardiac mortality
• RehospitalizationRehospitalization
• StrokeStroke
• NYHA functional classNYHA functional class
• Days alive and out of hospitalDays alive and out of hospital
• Echo-derived valve areas, transvalvular gradients, Echo-derived valve areas, transvalvular gradients, paravalvular aortic regurgitationparavalvular aortic regurgitation
• Mortality outcomes stratified by STS scoreMortality outcomes stratified by STS score8

n = 358Randomized Inoperable
n = 358Randomized Inoperable
n = 179TAVR
n = 179TAVR
n = 179Standard therapy
n = 179Standard therapy
124/124 patients100% followed at 1 Yr
124/124 patients100% followed at 1 Yr
85/85 patients100% followed at 1 Yr
85/85 patients100% followed at 1 Yr
99/102 patients*97.1% followed at 2 Yr
99/102 patients*97.1% followed at 2 Yr
56/56 patients100% followed at 2 Yr
56/56 patients100% followed at 2 Yr
Study FlowStudy FlowInoperable CohortInoperable Cohort
9
• 5 withdrawals in the first year in Standard Rx arm5 withdrawals in the first year in Standard Rx arm• *3 patients followed outside of protocol window in TAVR group*3 patients followed outside of protocol window in TAVR group• No patients were lost to follow-upNo patients were lost to follow-up

Statistical MethodStatistical Method
• Primary analysis was by “intention-to-treat” (ITT).Primary analysis was by “intention-to-treat” (ITT).
• Mortality was estimated by ITT, both with and Mortality was estimated by ITT, both with and without censoring of the cross-over patientswithout censoring of the cross-over patients(n = 11 cross-over patients from 1-2 years).(n = 11 cross-over patients from 1-2 years).
• Clinical outcomes were analyzed by ITT with Clinical outcomes were analyzed by ITT with censoring of Standard Rx cross-over patients.censoring of Standard Rx cross-over patients.
• Event rates are given as Kaplan-Meier estimates.Event rates are given as Kaplan-Meier estimates.
• Core lab echo results are presented from the “as Core lab echo results are presented from the “as treated” (AT) cohort.treated” (AT) cohort.
10

Patient Characteristics (1)Patient Characteristics (1)
11
CharacteristicCharacteristic TAVRTAVRn = 179n = 179
Standard RxStandard Rxn = 179n = 179
p valuep value
Age – yrAge – yr 83.1 ± 8.683.1 ± 8.6 83.2 ± 8.383.2 ± 8.3 0.950.95
Male sex (%)Male sex (%) 45.845.8 46.946.9 0.920.92
STS ScoreSTS Score 11.2 ± 5.811.2 ± 5.8 12.1 ± 6.112.1 ± 6.1 0.140.14
NYHANYHA I or II (%)I or II (%) III or IV (%)III or IV (%)
7.87.892.292.2
6.16.193.993.9
0.680.680.680.68
CAD (%)CAD (%) 67.667.6 74.374.3 0.200.20
Prior MI (%)Prior MI (%) 18.618.6 26.426.4 0.100.10
Prior CABG (%)Prior CABG (%) 37.437.4 45.645.6 0.170.17
Prior PCI (%)Prior PCI (%) 30.530.5 24.824.8 0.310.31
Prior BAV (%)Prior BAV (%) 16.216.2 24.424.4 0.090.09
CVD (%)CVD (%) 27.427.4 27.527.5 1.001.00

Patient Characteristics (2)Patient Characteristics (2)
12
CharacteristicCharacteristic TAVRTAVRn = 179n = 179
Standard RxStandard Rxn = 179n = 179
p valuep value
PVD (%)PVD (%) 30.330.3 25.125.1 0.290.29
COPDCOPD Any (%)Any (%) OO2 2 dependent (%)dependent (%)
41.341.321.221.2
52.552.525.725.7
0.040.040.380.38
Creatinine > 2 mg/dL (%)Creatinine > 2 mg/dL (%) 5.65.6 9.69.6 0.230.23
Atrial fibrillation (%)Atrial fibrillation (%) 32.932.9 48.848.8 0.040.04
Perm. pacemaker (%) Perm. pacemaker (%) 22.922.9 19.519.5 0.490.49
Pulmonary HTN (%)Pulmonary HTN (%) 42.442.4 43.843.8 0.900.90
Frailty (%)Frailty (%) 18.118.1 28.028.0 0.090.09
Porcelain aorta (%)Porcelain aorta (%) 19.019.0 11.211.2 0.050.05
Chest wall radiation (%)Chest wall radiation (%) 8.98.9 8.48.4 1.001.00
Chest wall deformity (%)Chest wall deformity (%) 8.48.4 5.05.0 0.290.29
Liver disease (%)Liver disease (%) 3.43.4 3.43.4 1.001.00

All Cause Mortality (ITT)All Cause Mortality (ITT)Crossover Patients FollowedCrossover Patients Followed
Numbers at RiskNumbers at Risk
TAVRTAVR 179179 138138 124124 110110 8383 Standard RxStandard Rx 179179 121121 8585 6767 5151
All
Cau
se M
orta
lity
(%)
Standard Rx
TAVR
∆ at 2 yr = 24.3%NNT = 4.1 pts
67.6%
43.3%
∆ at 1 yr = 20.0%NNT = 5.0 pts
50.7%
30.7%
13
Months
HR [95% CI] =0.57 [0.44, 0.75]
p (log rank) < 0.0001

All Cause Mortality (ITT)All Cause Mortality (ITT)Crossover Patients CensoredCrossover Patients Censored
Numbers at RiskNumbers at Risk
TAVRTAVR 179179 138138 124124 110110 8383 Standard RxStandard Rx 179179 121121 8585 6262 4242
All
Cau
se M
orta
lity
(%)
Standard Rx
TAVR
∆ at 2 yr = 24.7%NNT = 4.0 pts
68.0%
43.3%
∆ at 1 yr = 20.0%NNT = 5.0 pts
50.7%
30.7%
14
Months
HR [95% CI] =0.56 [0.43, 0.73]
p (log rank) < 0.0001

All Cause Mortality (ITT)All Cause Mortality (ITT)Landmark AnalysisLandmark Analysis
All
Cau
se M
orta
lity
(%)
Months
Mortality 0-1 yr Mortality 1-2yr
Standard Rx TAVR
HR [95% CI] =0.57 [0.44, 0.75]
p (log rank) < 0.0001
HR [95% CI] =0.58 [0.37, 0.92]
p (log rank) = 0.019450.7%
30.7%
35.1%
18.2%
Numbers at RiskNumbers at Risk
TAVRTAVR 179179 138138 124124 110110 8383 Standard RxStandard Rx 179179 121121 8585 6262 4242
15

Cardiovascular Mortality (ITT)Cardiovascular Mortality (ITT)Crossover Patients CensoredCrossover Patients Censored
Numbers at RiskNumbers at Risk
TAVRTAVR 179179 138138 124124 110110 8383 Standard RxStandard Rx 179179 121121 8585 6262 4242
Car
diov
ascu
lar
Mor
talit
y (%
)
Standard Rx
TAVR
∆ at 2 yr = 31.4%NNT = 3.2 pts
62.4%
31.0%
∆ at 1 yr = 24.1%NNT = 4.1 pts 44.6%
20.5%
16
Months
HR [95% CI] =0.44 [0.32, 0.60]
p (log rank) < 0.0001

Repeat Hospitalization (ITT)Repeat Hospitalization (ITT)
Numbers at RiskNumbers at Risk
TAVRTAVR 179179 115115 100100 8989 6464 Standard RxStandard Rx 179179 8686 4949 3030 1717
Rep
eat H
ospi
taliz
atio
n (%
)
Standard Rx
TAVR
∆ at 2 yr = 37.5%NNT = 2.7 pts
72.5%
35.0%
∆ at 1 yr = 26.9%NNT = 3.7 pts
53.9%
27.0%
18
Months
HR [95% CI] =0.41 [0.30, 0.58]
p (log rank) < 0.0001

Hospitalization Through 2 YearsHospitalization Through 2 Years
TAVRTAVR Standard TxStandard Tx p valuep value
Repeat Hospitalizations (No.)Repeat Hospitalizations (No.) 7878 151151 <.0001<.0001
Repeat Hospitalizations (%)Repeat Hospitalizations (%) 35.0%35.0% 72.5%72.5% <.0001<.0001
Days Alive Out of Hospital Days Alive Out of Hospital Median [IQR]Median [IQR] 699 [201-720]699 [201-720] 355 [116-712]355 [116-712] .0003.0003
19

Per
cent
Treatment VisitTreatment Visit Baseline 1 Year 2 Year
p = 0.61 p < 0.0001 p < 0.0001
92.2%
57.5%
16.9%23.7%
60.8%
93.9%
NYHA Class Over TimeNYHA Class Over TimeSurvivorsSurvivors
20

All Stroke (ITT)All Stroke (ITT)
Numbers at RiskNumbers at Risk
TAVRTAVR 179179 128128 116116 105105 7979 Standard RxStandard Rx 179179 118118 8484 6262 4242
Inci
denc
e (%
)
Months
Standard Rx
TAVR
∆ at 2 yr = 8.3%
5.5%
13.8%
∆ at 1 yr = 5.7%
5.5%
11.2%
21
HR [95% CI] =2.79 [1.25, 6.22]
p (log rank) = 0.009

All Cerebrovascular Events (%)All Cerebrovascular Events (%)
22
≤ ≤ 30 Days30 Days 31 Days – 1 Year31 Days – 1 Year 1 Year – 2 Years1 Year – 2 Years
All CVA p = 0.010 p = 0.387 p = 0.028
Ischemic Stroke p = 0.017 p = 0.155 p = 0.083
Hemorrhagic Stroke p = 0.316 p = 0.121 p = 0.415
Eve
nts
Note: Percents are of patients in the trial (n/179).

All Strokes (# pts)All Strokes (# pts)
24
≤ ≤ 30 Days30 Days 31 Days – 2 Years31 Days – 2 Years
All stroke p=0.010 p=0.319
Ischemic Stroke p = 0.017 p = 0.437
Hemorrhagic Stroke p = 0.316 p = 0.160
Eve
nts

Stroke - HemorrhagicStroke - Hemorrhagic
25
ITT armITT arm AgeAge Days post Days post randomizationrandomization DescriptionDescription TraumaTrauma MedicationMedication Procedure Procedure
related*related*Device Device related*related*
TAVR 91 9Right sided hemorrhage
NoCoumadin on
admissionYes No
TAVR 84 53Traumatic
subarachnoidFall Coumadin No No
TAVR 85 54Intraparenchy-
mal and subdural
Fall Not stated No No
TAVR 84 124 Intracranial Fall Not stated No No
TAVR 88 155Subdural
hematomaNot stated DAPT No No
Standard therapy (BAV)
91 243"Massive cerebral
hemorrhage"Not stated Not stated No n/a
*CEC adjudicated

Mortality or Stroke (ITT)Mortality or Stroke (ITT)
Numbers at RiskNumbers at Risk
TAVRTAVR 179179 128128 116116 105105 7979 Standard RxStandard Rx 179179 118118 8484 6262 4242
All
Cau
se M
orta
lity
or S
trok
e (%
)
Months
Standard Rx
TAVR
∆ at 2 yr = 21.9%NNT = 4.6 pts
68.0%
46.1%
∆ at 1 yr = 16.1%NNT = 6.2 pts 51.3%
35.2%
26
HR [95% CI] =0.64 [0.49, 0.84]
p (log rank) = 0.0009

1 Year1 Yearn = 179n = 179
OutcomeOutcomeTAVRTAVR Standard Standard
RxRx P valueP value
2 Year 2 Year n = 179n = 179
TAVRTAVR Standard Standard RxRx P valueP value
Acute kidney injuryAcute kidney injury
Creatinine > 3 mg/dL, % (n)Creatinine > 3 mg/dL, % (n) 1.1 (2)1.1 (2) 2.8 (5)2.8 (5) 0.4490.449 1.1 (2)1.1 (2) 2.8 (5)2.8 (5) 0.4490.449 Renal failure (CEC), % (n)Renal failure (CEC), % (n) 2.3 (4)2.3 (4) 4.7 (7)4.7 (7) 0.2570.257 3.2 (5)3.2 (5) 7.6 (9)7.6 (9) 0.1490.149
Cardiac re-interventionCardiac re-intervention
BAV, % (n)BAV, % (n) 1.1 (2)1.1 (2) 82.3 (138)82.3 (138) <.0001<.0001 2.8 (4)2.8 (4) 85.3 (140)85.3 (140) <.0001<.0001
Re-TAVR, % (n)Re-TAVR, % (n) 1.7* (3)1.7* (3) NANA -- 1.7* (3)1.7* (3) NANA --
AVR, % (n)AVR, % (n) 0 (0)0 (0) 7.6 (10)7.6 (10) 0.0020.002 0.9 (1)0.9 (1) 8.9 (11)8.9 (11) 0.0050.005
Endocarditis, % (n)Endocarditis, % (n) 1.4 (2)1.4 (2) 0.8 (1)0.8 (1) 0.6180.618 2.3 (3)2.3 (3) 0.8 (1)0.8 (1) 0.3160.316
Bleeding – major, % (n)Bleeding – major, % (n) 24.2 (42)24.2 (42) 14.9 (21)14.9 (21) 0.0380.038 28.9 (48)28.9 (48) 20.1 (25)20.1 (25) 0.0930.093
New pacemaker, % (n)New pacemaker, % (n) 4.7 (8)4.7 (8) 8.6 (14)8.6 (14) 0.1490.149 6.4 (10)6.4 (10) 8.6 (14)8.6 (14) 0.4690.469
Myocardial infarctionMyocardial infarction
All, % (n)All, % (n) 0.8 (1)0.8 (1) 0.7 (1)0.7 (1) 0.9060.906 1.6 (2)1.6 (2) 2.5 (2)2.5 (2) 0.6940.694
Clinical OutcomesClinical Outcomes1 Year and 2 Year (ITT)1 Year and 2 Year (ITT)
27

All Cause Mortality (ITT)All Cause Mortality (ITT)Control Patients Alive on First Crossover DateControl Patients Alive on First Crossover Date
Numbers at RiskNumbers at Risk
Not Crossed-OverNot Crossed-Over 3838 3232 2424 1717Crossed-OverCrossed-Over 2020 1919 1818 1717
All
Cau
se M
orta
lity
(%)
∆ at 1 yr = 11.0%
10.0%
21.0%
29
Months past first cross-over
Crossed-Over
Not Crossed-Over

Mea
n G
radi
ent (
mm
Hg)
Error bars = ± 1 Std DevError bars = ± 1 Std Dev
EOA
Mean Gradient
N = 158
N = 162
N = 137
N = 143
N = 84
N = 89
N = 65
N = 65
N = 9
N = 9
AV
A (cm
²)Mean Gradient & Valve AreaMean Gradient & Valve Area
30

Numbers at RiskNumbers at Risk
None to MildNone to Mild 147147 118118 107107 9595 7272 Moderate or SevereModerate or Severe 1717 1212 1111 1010 88
Dea
th In
cide
nce
(%)
Months
Moderate or Severe
None to Mild
41.2%
40.5%
35.3%
27.2%
Mortality Stratified by Paravalvular Leak (ITT)Mortality Stratified by Paravalvular Leak (ITT)Starting at DischargeStarting at Discharge
31
p (log rank) = 0.891

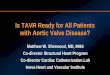
Echo Analysis PV Leak Changes Echo Analysis PV Leak Changes 30 Days Compared to 2 Years30 Days Compared to 2 Years
32
16.4% Progressed16.4% Progressed42.6% Improved42.6% Improved 41.0% Unchanged41.0% Unchanged
30 Day30 Day2 Year2 Year
NoneNone TraceTrace MildMild ModerateModerate SevereSevere
None 10 3 0 0 0
Trace 7 5 6 0 0
Mild 4 7 10 1 0
Moderate 0 4 3 0 0
Severe 0 0 1 0 0
Of the 61 patients alive with data at 2 years:
Patients With Data at Both Time Points

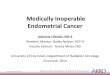
2828 2626 2525 2424 1616108108 8080 7676 6767 5252
4343 3232 2323 1919 1515
Dea
th In
cide
nce
(%)
Months
STS <5 STS 5-14.9
Months
STS ≥15
p value (log rank) = 0.012p value (log rank) = 0.676
1212 88 77 66 55119119 8484 5959 4242 2929
4747 2929 1919 1414 88
Mortality Stratified by STS Score (ITT)Mortality Stratified by STS Score (ITT)
TAVRTAVRStandard RxStandard Rx
Numbers at RiskNumbers at Risk
33

Conclusions (1)Conclusions (1)
At 2 years, At 2 years, in patients with symptomatic severe AS in patients with symptomatic severe AS who are not suitable candidates for surgery…who are not suitable candidates for surgery…
• TAVR remained superior to standard therapy with TAVR remained superior to standard therapy with incremental benefit from 1 to 2 years, markedly incremental benefit from 1 to 2 years, markedly reducing the rates of…reducing the rates of…
All cause mortalityAll cause mortality
Cardiovascular mortalityCardiovascular mortality
Repeat hospitalizationRepeat hospitalization
• TAVR improved NYHA functional status and TAVR improved NYHA functional status and decreased Class III/IV symptoms compared to decreased Class III/IV symptoms compared to standard therapy (17% vs 64%; p < 0.001).standard therapy (17% vs 64%; p < 0.001).
34

Conclusions (2)Conclusions (2)
At 2 years, At 2 years, in patients with symptomatic severe AS in patients with symptomatic severe AS who are not suitable candidates for surgery…who are not suitable candidates for surgery…
•There were more neurologic events in TAVR patients vs There were more neurologic events in TAVR patients vs Standard Rx (16.2% vs 5.5%; p = 0.003) with 5 new Standard Rx (16.2% vs 5.5%; p = 0.003) with 5 new events (3 strokes and 2 TIAs) between 1-2 years in TAVR events (3 strokes and 2 TIAs) between 1-2 years in TAVR patients.patients.
•After 30 days, differences in stroke frequency were After 30 days, differences in stroke frequency were largely due to increased hemorrhagic strokes in TAVR largely due to increased hemorrhagic strokes in TAVR patients.patients.
•A subgroup analysis according to surgical risk score A subgroup analysis according to surgical risk score suggests that the most pronounced benefit of TAVR is suggests that the most pronounced benefit of TAVR is in patients without extreme clinical co-morbidities.in patients without extreme clinical co-morbidities.35

Conclusions (3)Conclusions (3)
At 2 years, At 2 years, in patients with symptomatic severe AS in patients with symptomatic severe AS who are not suitable candidates for surgery…who are not suitable candidates for surgery…
•TAVR hemodynamics by echo showed durable TAVR hemodynamics by echo showed durable improvements in AVA and mean gradients up to improvements in AVA and mean gradients up to 3 years after implantation.3 years after implantation.
•Moderate or severe paravalvular AR in the TAVR Moderate or severe paravalvular AR in the TAVR patients did not influence 2-year survival and there was patients did not influence 2-year survival and there was a trend towards reduced paravalvular AR between 1 and a trend towards reduced paravalvular AR between 1 and 2 years.2 years.
36

Clinical Implications Clinical Implications
• Two year data continues to support the role of TAVR Two year data continues to support the role of TAVR as the standard-of-care for symptomatic patients with as the standard-of-care for symptomatic patients with aortic stenosis who are not surgical candidates.aortic stenosis who are not surgical candidates.
• The ultimate value of TAVR in “inoperable” patients The ultimate value of TAVR in “inoperable” patients will depend on careful selection of patients who are will depend on careful selection of patients who are not surgical candidates, and yet do not have extreme not surgical candidates, and yet do not have extreme co-morbidities that overwhelm the benefits of TAVR co-morbidities that overwhelm the benefits of TAVR and render the intervention futile.and render the intervention futile.
37

Thank You to the Dedicated Study Thank You to the Dedicated Study Teams at All PARTNER Teams at All PARTNER Investigational SitesInvestigational Sites