Embed Size (px)
Citation preview

Collaborative TB/HIVActivities in Cambodia
Khun Kim EamKhun Kim Eam, MD, MPH., MD, MPH.Chief of Planning, Statistics & IEC unit
National Center for TB & Leprosy Control
Coordination Meeting for Review of 2006 Work Plan & Revision of Coordination Meeting for Review of 2006 Work Plan & Revision of 2007 2007 Work Plan for NCHADS Program, Technical School for Medical CareWork Plan for NCHADS Program, Technical School for Medical Care
25-27 October 2006

Background•Population (based on WHO Report 2004):13,809,532
•TB infection rate among general population: 64%
•Incidence Rate of TB all forms 549/100,000
•Incidence Rate of TB SS+: 225/100,000
•Death rate due to TB : 107/100,000
•Prevalence HIV in TB patients (2005) : 10%
•Prevalence HIV in persons aged 15‐49 yrs: 1.9%
•No. of HIV infected persons (15‐49yrs): 123,100

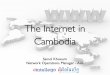
Trends in TB Notification (1982‐2005)
0
5000
10000
15000
20000
25000
30000
35000
40000
198219831984198519861987198819891990199119
921993199419951996199719981999200020
012002200320042005
Year of Notification
No.
of T
B C
ases
SM(+)SM(-)Extra-PTotal

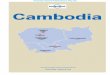
2.50%
3.90%
5.20%
7.90%
6.70%
11.80%
10%
0.00%
2.00%
4.00%
6.00%
8.00%
10.00%
12.00%
1995 1996 1997 1999 2000 2003 2005
HIV sero‐prevalence trend among TB cases

• Achievements: What we have done?– Strong surveillance data thru repeat surveys of HIV in TB
– Successful pilots– Increase in access to VCCT– Upgrade of TB information system to capture HIV information
TB‐HIV (from joint program review evaluation)

Scaling up TB/HIV Activities
Joint TB/HIV plan and action focusing on OD which:
‐ High HIV prevalence or increasing trend‐ Existing VCT‐ TB/DOTS services‐ Full package of CoCTB/DOTS services and CoC must Go Hand in Hand

What is on going?What is on going?Trained OD TB/HIV and PlanTrained OD TB/HIV and Plan
• Trained OD with TB/HIV collaboration:24 ODs– Pilot sites (9 ODs): BTB(2), BMC(2), PP(4) & SHV– SReap(2), KK(1), PV(2), SRieng(1), Takeo(1), Kg Thom(1), Pursat(2), Kandal(1), Kg Speu(1), Kg Cham(1), Kg Chhnang(1), Kampot(2),
• OD to be trained for TB/HIV by end of 2006: – Kirivong, Angroka, Koh Thom, Tbaung Khmom, Cheung Prey, Memot.

Principles for Collaborative effortsfor diagnosis & treatment
TB Control TB Control ProgrammeProgramme
HIV Control HIV Control ProgrammeProgramme
TB SuspectTB Suspect HIV SuspectHIV Suspect
DOTSDOTS HIV/AIDS CareHIV/AIDS Care
HC/TB UnitHC/TB Unit(smear/CXR)(smear/CXR)
VCCTVCCT(HIV Test)(HIV Test)
No TBNo TB Active TBActive TB HIV PositiveHIV Positive HIV negativeHIV negative
TB Health TB Health EducationEducation
HIV HIV PreventionPrevention
TB Services :DOTS AIDS Services: COC

TB/HIV activities in Cambodia<HIV screening among TB patients>
HC/FDH/RH
•TB treatment(DOTS)•HC staff shouldencourage TB patientto go to VCCT
RH
VCCTSupport
fromHBCT
Health education at post-test counseling.HIV-
HIV+ HBCTRH
OI/ART
TB patients
PLHARH
OI/ART•TB screening
TB+HC/FDH/RH
TB treatment(DOTS)
TB- RHOI/ART
•TB screening follow up every 6 month•IPT(only in BTB and Moung Russey)
<TB screening among PLHA>
Supportfrom
HBCT
Supportfrom
HBCT

• SOP for prompt testing of TB/HIV and rapid access to treatment and care services– TB services/DOT at HC and/or FDH with no VCCT services:
Option 1TB patients receiving DOT should be supported with funds for transportation to the nearest VCCT site in order to have a test for HIV/AIDS.
Significant Developments in CollaborationSignificant Developments in Collaboration

Option 2HC/FDH with the capacity to provide pre‐test and post‐test counseling and draw blood samples from TB patients volunteering for HIV/AIDS testing should send specimens to the nearest VCCT laboratory.
Option 2VCCT staff will visit HC/FDH where TB patients have been group‐counseled and gathered by health personnel in collaboration with HBC teams. VCCT staff will provide pre‐test‐counseling, take blood to do rapid test at the facilities visited and provide post‐test counseling.
Significant Developments in CollaborationSignificant Developments in Collaboration

No of PLHA referred for TB screening from VCCT
0
500
1000
1500
2000
1st Q- 06 2nd Q- 06
NO
1.# HIV+ newly registered at VCT# HIV+ refered for TB screening from VCCT(among#1)

TB screening and TB prevalence among PLHA
171
1174
20 10615
11411
17819 27
0200400600800
100012001400
1st Q- 06 2nd Q- 06
No
# HIV+ screened for TB # PTB S(+) # PTB S(- )# EPTB # PLHA under IPT

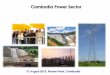
HIV prevalence in TB patients
321
1968
19
259
15
301
1791
0
500
1000
1500
2000
2500
Q1/06 Q2/06Registered TB patients Referred TB patients TB patients tested for HIVHIV+ CPT Joint HBC/OIART

• Issues :What problems are remained?– Inactive national coordination committee– Care providers have no access to HIV test results
– Access to services, including HIV testing, CPT, TB screening
– Information exchange between VCCT, OI clinics, and TB health care staff
– Insufficient TB specific data in HIV reporting system
– Unclear policy on infection control
TB‐HIV (from joint program review evaluation)

• Recommendations (1/2)– Reactivate national coordination mechanism, with bi‐monthly meetings of a core‐group
– Appoint TB‐HIV coordinators at PHD and OD levels
– Fund and implement the policy for provider‐initiated HIV testing
– Expand HIV counseling & testing (sending blood vs. onsite testing) at HC level
TB‐HIV (from joint program review evaluation)

• Recommendations (2/2)– Ensure early access to CPT (consider making available at HC level)
– Ensure transfer of patient data between facilities
– Fund CXR for screening of TB in HIV– Upgrade HIV reporting to include TB data– Develop a policy on infection control
TB‐HIV (from joint program review evaluation)

Main Collaborative TB/HIV Main Collaborative TB/HIV IndicatorsIndicators
• Proportion of TB patients referred to VCT for HIV testing
• Proportion of TB patients tested for HIV• Proportion of TB patients tested HIV (+)• Proportion of TB patients with HIV(+) receive CPT• Proportion of TB/HIV patients received ART• Proportion of PLHA screened for TB• Proportion of PLHA found TB • Proportion of PLHA with TB receive TB treatment• Proportion of PLHA received IPT

Conclusion & Recommendations
• Develop an effective monitoring & surveillance system based on standardized data collection forms & registers (?)
• Organize sustainable mechanisms to support PLHA for TB screening & IPT where appropriate
• Study feasibility of offering VCT to all HIV suspects among new TB patients beforeinitiation of DOTS to increase detection of co‐infected cases

Conclusion & Recommendations
• Design and disseminate appropriate IEC materials on TB/HIV to reduce discrimination in the community
• Conduct intensive training for health workers in TB/HIV counselling to enhance treatment adherence & follow up
• Plan expansion of TB/HIV collaborative activities to ODs having well established VCTs, CoC and NGO network (ongoing process).

IEC materials of IEC materials of TB/HIV activitiesTB/HIV activities