Embed Size (px)
DESCRIPTION
TB Latente Treatmenttratamiento de tuberculosis en fase latente
Citation preview

Official reprint from UpToDate
www.uptodate.com ©2015 UpToDate
AuthorsMadhukar Pai, MD, PhDDick Menzies, MD, MSc
Section EditorC Fordham von Reyn, MD
Deputy EditorElinor L Baron, MD, DTMH
Diagnosis of latent tuberculosis infection (tuberculosis screening) in HIV-uninfected adults
All topics are updated as new evidence becomes available and our peer review process is complete.
Literature review current through: Jul 2015. | This topic last updated: Jul 28, 2015.
INTRODUCTION — Treatment of individuals with active tuberculosis (TB) is the first priority for tuberculosis control;
an important second priority is identification and treatment of individuals with latent tuberculosis infection (LTBI).
In most individuals, Mycobacterium tuberculosis infection is contained initially by host defenses, and infection
remains latent. However, latent infection has the potential to develop into active disease at any time. Identification
and treatment of latent tuberculosis infection can reduce the risk of development of disease by as much as 90
percent [1] and so has potential to protect the health of the individuals as well as the public by reducing the number
of potential sources of infection [2,3].
There are two major tests for identification of latent tuberculosis infection: the tuberculin skin test (TST) and the
interferon gamma release assay (IGRA) [4]. Both tests evaluate cell-mediated immunity.
Use of TST for diagnosis of LTBI in HIV-uninfected patients will be reviewed here. Management of LTBI for patients
with HIV or receiving tumor necrosis factor-alpha inhibitors is discussed in detail separately, as are issues related to
TB screening in children and treatment of latent tuberculosis infection in HIV-uninfected patients. (See "Treatment of
latent tuberculosis infection in HIV-infected patients" and "Latent tuberculosis infection in children" and "Tumor
necrosis factor-alpha inhibitors and mycobacterial infections" and "Interferon-gamma release assays for diagnosis of
latent tuberculosis infection".)
INDICATIONS FOR TESTING — The goal of testing for latent tuberculosis infection (LTBI) is to identify individuals
who are at increased risk for the development of tuberculosis (TB) and therefore would benefit from treatment of
LTBI [5,6]. Only those who would benefit from treatment should be tested, so a decision to test presupposes a
decision to treat if the test is positive.
In general, testing for latent TB infection is warranted to identify individuals who are at risk of new infection and to
identify individuals at increased risk of reactivation due to associated conditions (table 1). Diagnostic tools for
diagnosis of latent TB include tuberculin skin testing (TST) and interferon gamma release assays (IGRAs). Use of
the TST for diagnosis of latent TB infection will be reviewed here; the use of IGRAs for diagnosis of latent TB
infection is discussed separately. (See "Interferon-gamma release assays for diagnosis of latent tuberculosis
infection".)
The optimal approach to screening immigrants from high-incidence countries after arrival in low-incidence countries
is uncertain. Early decision analyses suggested minimal benefit of screening for migrants [7] and that investment in
TB control within the source countries would be more cost-effective [8]. A systematic review and meta-analysis
including 45 studies with 93,249 participants found that prevalence of positive TST was significantly higher than
positive IGRA (odds ratio 1.5, 95% CI 1.1 to 2.0), and initiation of LTBI therapy occurred more often among patients
with positive TST than positive IGRA (59 versus 28 percent) [9].
In general, use of TST or IGRA for the diagnosis of active TB in adults is discouraged. (See "Diagnosis of pulmonary
tuberculosis in HIV-uninfected patients".)
Risk of new infection — Testing for latent TB should be performed in asymptomatic individuals for whom new
infection is suspected. This includes close contacts of patients with active pulmonary TB (eg, those living in the
same household), as well as casual contacts of patients with highly contagious active TB (such as healthcare
®
®
Diagnosis of latent tuberculosis infection (tuberculosis screening) in HIV... http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/diagnosis-of-...
1 de 18 03/08/2015 07:18 p.m.

workers). Because the risk of developing active disease is very high in the next few years following exposure, all
patients at increased risk for new TB infection should be evaluated for LTBI, regardless of age (table 1).
In general, close contacts of patients with active pulmonary TB should undergo a second test 8 to 12 weeks later if
the first test is negative. Healthcare workers should undergo baseline two step testing followed by annual testing
(see 'Repeat and serial testing' below).
The risk of disease in the first two years following infection is age dependent. The decline of risk with increasing age
reflects greater innate and acquired immunity [10]:
Increased risk of reactivation — Identifying those at risk for reactivation who warrant testing depends on age and
the degree of risk for reactivation (relative to healthy individuals) (table 1 and table 2). In general, individuals at
increased risk of reactivation require a single test only; if it is negative, no further testing is needed.
Normal healthy individuals with LTBI have an annual risk of 0.1 percent (1 per 1000) of developing active TB [11].
Annual risk of disease if infected can range from more than 10 percent (with HIV infection) to 1 to 2 percent (if on
hemodialysis or following solid organ transplant) to 0.1 percent (if healthy with a normal chest radiograph). Estimated
risks for TB relative to healthy individuals in the setting of various conditions are outlined in the Table (table 2):
Age — The risk of isoniazid-induced hepatitis and other adverse events increases with age; risk of hepatitis
increases over the age of 35 and substantially over the age of 50 [12,13]. Therefore, age is an important
consideration in the decision to test for LTBI, since testing implies that treatment will be administered if the test is
positive [12-14]. Although the annual risk of disease is relatively high, with increasing age the cumulative risk of
reactivation diminishes as does the benefit of therapy. To estimate the cumulative lifetime risk with various
conditions, a web-based algorithm can be used [15].
We favor the following age parameters for LTBI testing (with intention to treat if test is positive) (table 1):
Infants (ages ≤1): 50 percent●
Children (ages 1 to 2): 12 to 25 percent●
Children (ages 2 to 5): 5 percent●
Children (ages 5 to 10): 2 percent●
Age >10 years: 10 to 20 percent●
High risk – High risk individuals are those whose risk for reactivation is at least six times higher than normal
healthy individuals. These include individuals with major immunocompromising conditions (eg, lymphoma,
leukemia, head and neck cancer, chemotherapy, solid organ transplant, HIV infection, tumor necrosis factor
[TNF]-alpha inhibitors), and those with chest radiograph demonstrating fibronodular changes typical of healed
TB (so-called "inactive TB"). All individuals in these categories should have a single test to evaluate for latent
TB infection, regardless of age.
●
Moderate risk – Moderate risk individuals are those whose risk for reactivation is three to six times higher than
normal healthy individuals. These include individuals with diabetes mellitus (regardless of insulin dependence)
or corticosteroid therapy. All individuals in these categories ≤65 should have a single test to evaluate for latent
TB infection.
●
Slightly increased risk – Individuals at slightly increased risk for reactivation are those whose risk is 1.5 to 3
times higher than normal healthy individuals. This includes individuals who are underweight, smoke cigarettes,
or have small granulomas on chest radiograph. All individuals ≤50 in this category should have a single test to
evaluate for latent TB infection.
●
For individuals ≥65, the risk of hepatitis is ≥5 percent, so testing and treatment are indicated only if risk of
reactivation is high [12].
●
For individuals between 50 and 65, the risk of hepatitis is 3 to 5 percent, which is sufficiently high that testing
and treatment are indicated if risk of reactivation is high or moderate.
●
Diagnosis of latent tuberculosis infection (tuberculosis screening) in HIV... http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/diagnosis-of-...
2 de 18 03/08/2015 07:18 p.m.

Testing and treatment are not warranted for individuals ≥50 with only slightly increased risk and individuals ≥65 with
moderate or slightly increased risk for reactivation.
TUBERCULIN SKIN TEST — The tuberculin skin test (TST) is used to identify individuals with previous sensitization
to mycobacterial antigens. It consists of intradermal injection of tuberculin material, which stimulates a delayed-type
hypersensitivity response mediated by T lymphocytes and causes induration within 48 to 72 hours.
Performing the TST — In North America, the tuberculin material is purified protein derivative (PPD); the
recommend dose is 5 tuberculin units (0.1 mL). In other regions, RT-23 may be the tuberculin material used; the
standard dose is 2 tuberculin units. These doses have been shown to be equivalent [16].
The only recommended method of tuberculin skin testing is the Mantoux technique, which consists of intradermal
injection of tuberculin material on the inner surface of the forearm [14,17]. To read the test, the transverse diameter
of the induration (not erythema) should be demarcated, measured, and recorded in millimeters. The test should be
read 48 to 72 hours following intradermal injection.
The results are less reliable if the test is read after 72 hours. Among 400 individuals with positive TST at 48 to 72
hours, about 20 percent had negative results when the TST was read seven days after placement [18]. While a
strongly positive reaction after 96 hours may be accepted, results become increasingly doubtful with longer intervals
between injection and reading; in such circumstances, it is best is to repeat the TST. If the TST is repeated after
seven days, then the boosting effect may cause a positive TST (see 'Booster response' below). However, in the
absence of a documented negative first TST, there is no way to know if the TST represents a boosted reaction.
Hence, the TST must be interpreted in the same way as a single initial TST. This potential problem reinforces the
importance of reading at the correct time.
Multipuncture methods (including the Tine test and the Heaf test) may be easier to administer but are not accurate
because it is not possible to precisely control the amount of tuberculin. Therefore, these should not be used [17].
Repeat and serial testing — If the TST is documented to be positive, it should never be repeated. Once the test is
positive, it will remain positive, and repeating the test has no clinical utility. If there is a history of a positive TST but
this is not documented, then it may be appropriate to confirm this.
If the TST is negative, there are three circumstances in which the TST should be repeated:
For individuals <50, risk of hepatitis is less than 3 percent (for individuals <35, it is less than 1 percent), so
testing and treatment are indicated if risk of reactivation is slightly increased, moderate, or high.
●
Close contacts of patients with active pulmonary tuberculosis – These individuals may have an initial negative
TST because the tuberculosis (TB) infection was so recent that delayed hypersensitivity has not yet developed.
In these individuals, the TST should be repeated eight weeks after the last exposure, since it takes three to
seven weeks for tuberculin conversion to occur after new infection [19]. The same technique and dose is used,
but the test is applied on the opposite forearm.
●
Individuals with ongoing potential exposure – In North America, ongoing potential exposure occurs in the
setting of occupational risk; healthcare workers in institutions with a substantial risk of unrecognized exposure
to tuberculosis represent the major group for which serial annual testing is warranted. Those undergoing serial
annual testing should also receive additional testing after a known episode of exposure [20].
Individuals with ongoing potential exposure who have a history of a positive test for latent TB infection (LTBI)
and have completed a course of LTBI treatment should undergo baseline chest radiograph. Reevaluation with
chest radiograph should be pursued if symptoms develop that raise the possibility of active tuberculosis. There
are no additional mechanisms to evaluate for subsequent TB exposure in these individuals.
Serial testing is NOT warranted for groups other than those with occupational risk (such as those with
increased risk of reactivation) in settings where the incidence of TB is very low (less than 1 per 1000 per year).
●
Diagnosis of latent tuberculosis infection (tuberculosis screening) in HIV... http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/diagnosis-of-...
3 de 18 03/08/2015 07:18 p.m.

Interpretation of repeat and serial skin testing is discussed below. (See 'Repeat TST interpretation' below.)
INTERPRETING THE TST — The tuberculin skin test (TST) reading must establish a positive or negative result in
order to determine subsequent management (figure 1 and table 3).
Sensitivity is 98 percent using the 5 mm threshold, 90 percent using the 10 mm threshold, but only 50 to 60 percent
using the 15 mm threshold [25]. As the cutoff for mm of induration is increased, the sensitivity decreases and the
specificity increases. A higher cutoff is useful for evaluation of individuals in regions with high prevalence of
nontuberculous mycobacterial exposure and low likelihood of true TB infection.
If the TST is negative, the possibility of a false-negative result must be considered, as discussed in the following
section. Repeat testing is warranted in the circumstances outlined above. (See 'Repeat and serial testing' above.).
If the test is positive, no further testing is warranted. The patient should be referred for medical evaluation to exclude
active tuberculosis (TB), followed by initiation of treatment for latent TB infection (LTBI). (See 'Positive tests' below.)
Negative tests
False-negative tests — False-negative tuberculin skin test results may occur in the setting of biological and
technical limitations (table 4). Biologic limitations include immunosuppression or natural waning of immunity.
Technical limitations include improper tuberculin handling and interpretation.
Anergy testing with control antigens such as mumps and Candida was previously thought to help determine between
true-negative and false-negative tuberculin tests. However, the role of anergy testing in the diagnosis of LTBI is not
well defined, and such testing is not recommended [14,17].
Measles vaccination may temporarily suppress tuberculin reactivity. Measles-mumps-rubella (MMR) vaccine may be
given after, or on the same day as, the TST. If MMR has been given recently, TST should be postponed until four to
six weeks after administration of MMR [26].
Treating negative tests — In the setting of recent close contact to individuals known to have infectious
tuberculosis, treatment for LTBI should be considered for adults who are severely immunocompromised (such as
HIV infected or organ transplant recipient), even with negative TST or interferon gamma release assay (IGRA).
For these patients, LTBI therapy should be initiated (following clinical evaluation to rule out active tuberculosis) and
the TST or IGRA repeated after eight weeks [19]. If the second test is positive, treatment should be continued; if the
test is negative, treatment is usually stopped, although continued therapy may be considered on an individual basis.
The approach to treatment is discussed in detail separately. (See "Treatment of latent tuberculosis infection in
HIV-negative adults".)
Positive tests — The positive predictive value (PPV) denotes the probability of true infection in the setting of a
positive test. The greater the risk of exposure (due to risk factors such as close contacts with active TB cases and
In areas where TB incidence and the annual risk of infection are high, routine serial testing is usually not
performed because of limited resources in these settings [21].
To establish a correct baseline prior to serial testing ("two-step testing") – In individuals with remote exposure to
mycobacterial antigens (eg, due to prior Bacillus Calmette-Guérin [BCG] vaccination, nontuberculous
mycobacteria exposure, or remote TB infection), the tuberculin reaction may have waned and an initial
tuberculin test may be negative [22-24]. However, placement of the initial tuberculin test stimulates anamnestic
recall of immunity, such that a second tuberculin test ("booster") will be positive. Therefore, in the setting of a
positive tuberculin test performed a year after initial screening, it may be difficult to distinguish between recent
infection and remote mycobacterial exposure. For this reason, evaluation for the "booster phenomenon" should
be performed by repeating the TST (on the opposite forearm) one to four weeks after the first test. The
induration observed with the second test is the baseline that should be used for subsequent evaluation of skin
test conversion.
●
Diagnosis of latent tuberculosis infection (tuberculosis screening) in HIV... http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/diagnosis-of-...
4 de 18 03/08/2015 07:18 p.m.

foreign-born status), the higher the PPV. A computer-based algorithm is available to assist in the interpretation of
TST [15].
False-positive tests — There are two important causes of false-positive tests: nontuberculous mycobacteria
infection and Bacillus Calmette-Guérin (BCG) vaccination. However, in individuals with high likelihood of LTBI and/or
high risk of development of disease if infected, potential causes of false-positive tests should not influence the
decision to administer LTBI therapy.
Treating positive tests — Patients with positive tuberculin skin test or IGRA results must undergo clinical
evaluation to rule out active tuberculosis prior to treatment for latent infection. This includes evaluation for symptoms
(eg, fever, cough, weight loss), physical examination, and radiographic examination of the chest.
A chest radiograph is considered abnormal if it demonstrates parenchymal abnormalities, particularly upper lobe
opacification. Radiographs demonstrating stable upper lobe fibro-nodular disease or calcified granulomas are
considered to have evidence of previous tuberculosis and indicate the patient is at increased risk of reactivation
(table 2). There is no role for routine radiography for patients with positive tuberculin skin test who do not complete
treatment for LTBI [29-31].
Patients with symptoms or radiographic signs suggestive of active disease should undergo evaluation with sputum
microscopy and culture and receive treatment as appropriate. Sputum induction should be performed if patients
cannot expectorate spontaneously. Symptoms related to extrapulmonary sites should also be evaluated as
appropriate. In addition, HIV testing should be considered in patients with LTBI. (See "Diagnosis of pulmonary
tuberculosis in HIV-uninfected patients" and "Treatment of pulmonary tuberculosis in HIV-uninfected patients" and
"Screening and diagnostic testing for HIV infection".).
The approach to treatment is discussed in detail separately. (See "Treatment of latent tuberculosis infection in
HIV-negative adults".)
Healthcare workers — Healthcare workers should undergo baseline two-step testing followed by annual testing.
(See 'Repeat and serial testing' above.)
The clinical approach for healthcare worker exposure to active contagious TB varies depending on TST status and
the interval since the exposure episode. In general, if primary TB infection develops following clinical exposure, TST
Nontuberculous mycobacteria – Infection with nontuberculous mycobacteria (NTM) may cause false-positive
reactions to tuberculin. Estimates of the frequency of false-positive TSTs due to NTM range from 1 to 5 percent
of positive tuberculin tests [27] to as many as 50 percent of 9 to 14 mm reactions in United States healthcare
workers [15]. Therefore, the effect is important only if prevalence of true TB infection is low (ie, less than 5
percent). This situation occurs in low incidence countries with tropical, subtropical, or temperate climates
[15,27].
●
BCG vaccination – BCG vaccination is a well known but frequently misunderstood cause of false-positive
tuberculin reactions. The effect of BCG on TST depends primarily on the age when vaccinated [27]. BCG
vaccination in the first year of life causes no discernible effect on TST after 10 years or more. Vaccination after
the first year of life (such as at entrance to primary school at age 5 to 6) causes a stronger and longer lasting
effect. As many as 20 percent of individuals remain positive 10 years or more after vaccination at this age. In
pediatric populations, the interval since vaccination is important since there is progressive waning over the first
10 years after vaccination.
Since many foreign-born persons do not know their BCG vaccination status or age at vaccination, current and
past BCG vaccination policies for most countries of the world may be reviewed online at the World Atlas of
BCG Policies and Practices [28].
TST reactivity caused by BCG sensitization can be distinguished from latent TB infection by interferon-gamma
release assays. (See "Interferon-gamma release assays for diagnosis of latent tuberculosis infection".)
●
Diagnosis of latent tuberculosis infection (tuberculosis screening) in HIV... http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/diagnosis-of-...
5 de 18 03/08/2015 07:18 p.m.

conversion occurs three to eight weeks later. Therefore, for TST to reflect recent TB infection, it must be performed
≥3 weeks following exposure. The clinical approach is outlined below:
The role of interferon-gamma release assay for diagnosis of latent tuberculosis infection in healthcare workers is
uncertain; further study is needed. This issue is discussed further separately. (See "Interferon-gamma release
assays for diagnosis of latent tuberculosis infection", section on 'Reproducibility'.)
Allergic reactions — Early reaction within 24 hours with absence of induration at 48 to 72 hours is considered an
allergic reaction [32]. Immediate hypersensitivity skin reactions to the TST are possible; these consist of wheal and
flare response at the testing site within 20 minutes of purified protein derivative (PPD) placement. In a case series of
3248 allergy clinic patients, immediate hypersensitivity to skin testing with PPD was observed in 2 to 3 percent of
patients, without systemic reactions [32]. Systemic allergic reactions (including urticaria, angioedema, dyspnea, and
anaphylaxis) are rarely reported [33,34]. The incidence is estimated to be 1 to 3 per million distributed doses, which
is similar to the rate of anaphylaxis with vaccines [34]. (See "Allergic reactions to vaccines".)
In our experience, a diffuse maculopapular rash can appear within 12 hours and resolve within a day or two,
although such allergic reactions to the TST are relatively uncommon. The incidence of these reactions in our clinic is
in the range of 1 reaction per 2000 to 3000 patients [35]. These allergic reactions are unrelated to the TST result at
48 to 72 hours.
Patients with immediate skin test reactions or other types of allergic reactions to the TST should not receive it again.
The best approach for individuals who require serial testing has not been studied. Our practice is to assess patients
annually for symptoms of active disease and obtain a chest radiograph if new symptoms develop.
Managing referrals — Patients may be referred after a TST is performed for expert guidance regarding initiation of
LTBI therapy. In such cases, it is imperative to review the indications for skin testing as outlined in the preceding
sections. LTBI treatment should be initiated only for patients in the categories for which treatment confers benefit.
Those who have undergone testing who fall outside these categories should not receive LTBI therapy, as risk
outweighs potential benefit. (See 'Indications for testing' above.)
REPEAT TST INTERPRETATION — The interpretation of serial or repeated tuberculin skin test (TST) depends on
the context [19]. (See 'Repeat and serial testing' above.)
Booster response — Booster response refers to a positive TST performed one to four weeks after an initial
negative TST in the absence of exposure (such as preemployment screening of healthcare workers). The booster
For individuals with prior negative tuberculin test (ideally a negative two-step TST) and low likelihood of interim
exposure, a single tuberculin test should be performed eight weeks following exposure. If positive at ≥5 mm,
this should be interpreted as a recent TST conversion.
●
For individuals without prior tuberculin testing born in a low TB-incidence country and no history of BCG
vaccination, a baseline tuberculin test could be performed immediately (ie, ≤2.5 weeks or about 18 days
following exposure). If positive, this is suggestive of prior LTBI infection. If negative, a second TST can be
performed eight weeks after the end of exposure. If positive at ≥5 mm, this should be managed as a recent
TST conversion.
●
For individuals without prior tuberculin testing born in a medium to high TB incidence country and/or who have
history of BCG vaccination, baseline two step tuberculin testing could be performed promptly so long as both
first and second steps can be completed within ≤2.5 weeks (ie, about 18 days) from the start of exposure. If
positive at ≥5 mm, this is suggestive of prior LTBI infection. If negative, a second TST can be performed eight
weeks after the end of exposure. If the second TST is positive, this should be managed as a recent TST
conversion. IGRA is not an appropriate diagnostic tool for such circumstances, as the interval between primary
TB infection and IGRA conversion is not fully understood, and there is no consensus on how to interpret IGRA
conversions and reversions. (See "Interferon-gamma release assays for diagnosis of latent tuberculosis
infection".)
●
Diagnosis of latent tuberculosis infection (tuberculosis screening) in HIV... http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/diagnosis-of-...
6 de 18 03/08/2015 07:18 p.m.

response is less specific for diagnosis of latent tuberculosis infection (LTBI) than the initial TST since the booster
response may be caused by prior Bacillus Calmette-Guérin (BCG) vaccination, sensitization to nontuberculous
mycobacteria, or remote tuberculosis (TB) infection. Therefore, the risk of developing active TB among individuals
with a booster response is lower than the risk of developing active TB among individuals with an initial positive TST
[12,36].
Conversion — Skin test conversion refers to one of the following:
The risk of developing active TB is much higher in the setting of skin test conversion than booster response.
Definition — For both boosting and conversion, the second TST is defined as positive if the induration measures 10
mm or greater and has increased by ≥6 mm since the previous test [19]. This definition is used because test
variability may cause increases in induration of up to 6 mm.
Criteria for boosting and conversion of 12 mm, 15 mm, or even 18 mm have been suggested; these may be more
specific but are much less sensitive. Individuals with reactions of ≥10 mm should be referred for medical evaluation
to exclude active TB prior to initiation of LTBI therapy. The reaction should be documented, and no further tuberculin
testing should be done.
INTERFERON GAMMA RELEASE ASSAYS — Issues related to interferon-gamma release assays (IGRAs) and
their use are discussed in detail separately. (See "Interferon-gamma release assays for diagnosis of latent
tuberculosis infection".)
INFORMATION FOR PATIENTS — UpToDate offers two types of patient education materials, “The Basics” and
“Beyond the Basics.” The Basics patient education pieces are written in plain language, at the 5 to 6 grade
reading level, and they answer the four or five key questions a patient might have about a given condition. These
articles are best for patients who want a general overview and who prefer short, easy-to-read materials. Beyond the
Basics patient education pieces are longer, more sophisticated, and more detailed. These articles are written at the
10 to 12 grade reading level and are best for patients who want in-depth information and are comfortable with
some medical jargon.
Here are the patient education articles that are relevant to this topic. We encourage you to print or e-mail these
topics to your patients. (You can also locate patient education articles on a variety of subjects by searching on
“patient info” and the keyword(s) of interest.)
SUMMARY AND RECOMMENDATIONS
A positive TST up to eight weeks after an initial negative TST in the setting of recent exposure (see 'Risk of
new infection' above)
●
A positive TST detected as part of serial testing with ongoing risk of exposure (such as healthcare workers), in
the setting of baseline negative TST
●
th th
th th
Beyond the Basics topics (see "Patient information: Tuberculosis (Beyond the Basics)")●
Identification and treatment of latent tuberculosis infection (LTBI) can greatly reduce the likelihood of
reactivation. Hence, this has the potential to protect both individual and public health by reducing the number of
potential sources of infection. (See 'Introduction' above.)
●
Testing for and treatment of LTBI should be pursued in patients at increased risk for tuberculosis because of
certain clinical conditions and/or in patients with recent close contact to persons known to have infectious
tuberculosis (table 1). LTBI testing is appropriate only for those who would benefit from treatment; a decision to
test implies a decision to treat if the test is positive. (See 'Indications for testing' above.)
●
Since isoniazid-induced hepatitis increases with age, we suggest the following age parameters for LTBI testing
(with intention to treat if test is positive) (table 1 and table 2) (Grade 2C):
●
For individuals ≥65, testing is indicated if risk of reactivation is high.•
Diagnosis of latent tuberculosis infection (tuberculosis screening) in HIV... http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/diagnosis-of-...
7 de 18 03/08/2015 07:18 p.m.

Use of UpToDate is subject to the Subscription and License Agreement.
REFERENCES
Comstock GW. How much isoniazid is needed for prevention of tuberculosis among immunocompetent adults?Int J Tuberc Lung Dis 1999; 3:847.
1.
Horsburgh CR Jr. Priorities for the treatment of latent tuberculosis infection in the United States. N Engl J Med2004; 350:2060.
2.
Rieder HL. Interventions for Tuberculosis Control and Elimination. International Union Against Tuberculosisand Lung Disease, 2002.
3.
Getahun H, Matteelli A, Chaisson RE, Raviglione M. Latent Mycobacterium tuberculosis infection. N Engl JMed 2015; 372:2127.
4.
Horsburgh CR Jr, Rubin EJ. Clinical practice. Latent tuberculosis infection in the United States. N Engl J Med
2011; 364:1441.
5.
Mancuso JD, Tribble D, Mazurek GH, et al. Impact of targeted testing for latent tuberculosis infection usingcommercially available diagnostics. Clin Infect Dis 2011; 53:234.
6.
Schwartzman K, Menzies D. Tuberculosis screening of immigrants to low-prevalence countries. Acost-effectiveness analysis. Am J Respir Crit Care Med 2000; 161:780.
7.
For individuals between 50 and 65, testing is indicated if risk of reactivation is moderate or high.•
For individuals <50, testing is indicated if risk of reactivation is slightly increased, moderate, or high. (See
'Age' above.)
•
The tuberculin skin test (TST) assesses the intradermal delayed-type hypersensitivity response produced by
administration of purified protein derivative (PPD) from Mycobacterium tuberculosis. The interpretation is
outlined in the Table (table 3). (See 'Tuberculin skin test' above.)
●
A period of up to eight weeks after primary tuberculosis (TB) infection may be required for tuberculin skin test
conversion to occur. Individuals with recent close contact to a known infectious case of tuberculosis, whose
initial TST is negative, should have repeat TST eight weeks after the end of exposure. (See 'Repeat and serial
testing' above.)
●
TST can be false negative because of because of biologic problems (such as immune suppression) or because
of technical problems with the TST administration, PPD material, or reading (table 4). TST can be false positive
because of nontuberculous mycobacteria or Bacillus Calmette-Guérin (BCG) vaccination. However, in
individuals with high likelihood of LTBI and/or high risk of development of disease if infected, potential causes
of false-positive tests should not influence the decision to administer LTBI therapy. (See 'Interpreting the TST'
above.)
●
For severely immunocompromised persons who have had recent close contact with known infectious cases of
tuberculosis, LTBI therapy may be started even if the initial TST is negative. These tests for LTBI should be
repeated after eight weeks. If the second test is now positive, treatment is continued. (See 'Treating negative
tests' above.)
●
Patients with positive TST or IGRA results must undergo clinical evaluation to rule out active tuberculosis and
to assess need for LTBI therapy. This includes evaluation for symptoms (eg, fever, cough, weight loss),
physical exam, and radiographic examination of the chest. (See 'Treating positive tests' above.)
●
Tuberculin boosting is defined as an increase to an induration of at least 10 mm, compared with a TST that was
previously negative (<10 mm) in the absence of any exposure (and usually within one to four weeks).
Tuberculin conversion is defined as an increase in induration of at least 10 mm, compared with a TST that was
previously negative (<10 mm) in the setting of potential exposure. (See 'Repeat TST interpretation' above.)
●
Diagnosis of latent tuberculosis infection (tuberculosis screening) in HIV... http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/diagnosis-of-...
8 de 18 03/08/2015 07:18 p.m.

Schwartzman K, Oxlade O, Barr RG, et al. Domestic returns from investment in the control of tuberculosis inother countries. N Engl J Med 2005; 353:1008.
8.
Campbell JR, Chen W, Johnston J, et al. Latent tuberculosis infection screening in immigrants to low-incidencecountries: a meta-analysis. Mol Diagn Ther 2015; 19:107.
9.
Marais BJ, Gie RP, Schaaf HS, et al. The natural history of childhood intra-thoracic tuberculosis: a criticalreview of literature from the pre-chemotherapy era. Int J Tuberc Lung Dis 2004; 8:392.
10.
Comstock GW, Edwards LB, Livesay VT. Tuberculosis morbidity in the U.S. Navy: its distribution and decline.
Am Rev Respir Dis 1974; 110:572.
11.
Stead WW, To T, Harrison RW, Abraham JH 3rd. Benefit-risk considerations in preventive treatment fortuberculosis in elderly persons. Ann Intern Med 1987; 107:843.
12.
Kopanoff DE, Snider DE Jr, Caras GJ. Isoniazid-related hepatitis: a U.S. Public Health Service cooperativesurveillance study. Am Rev Respir Dis 1978; 117:991.
13.
Targeted tuberculin testing and treatment of latent tuberculosis infection. This official statement of theAmerican Thoracic Society was adopted by the ATS Board of Directors, July 1999. This is a Joint Statement ofthe American Thoracic Society (ATS) and the Centers for Disease Control and Prevention (CDC). Thisstatement was endorsed by the Council of the Infectious Diseases Society of America. (IDSA), September1999, and the sections of this statement. Am J Respir Crit Care Med 2000; 161:S221.
14.
The Online TST/QFT Interpreter. Version 2.0. http://www.tstin3d.com/index.html (Accessed on September 24,2010).
15.
COMSTOCK GW, EDWARDS LB, PHILIP RN, WINN WA. A COMPARISON IN THE UNITED STATES OFAMERICA OF TWO TUBERCULINS, PPD-S AND RT 23. Bull World Health Organ 1964; 31:161.
16.
Menzies D, Doherty TM. Diagnosis of latent tuberculosis infection. In: Reichman and Hershfield's Tuberculosis,a comprehensive international approach, Raviglione MC (Ed), Informa Healthcare USA, New York 2006.p.215.
17.
DUBOCZY BO, BROWN BT. Multiple readings and determination of maximal intensity of tuberculin reaction.Am Rev Respir Dis 1961; 84:60.
18.
Menzies D. Interpretation of repeated tuberculin tests. Boosting, conversion, and reversion. Am J Respir CritCare Med 1999; 159:15.
19.
Jensen PA, Lambert LA, Iademarco MF, et al. Guidelines for preventing the transmission of Mycobacteriumtuberculosis in health-care settings, 2005. MMWR Recomm Rep 2005; 54:1.
20.
World Health Organization. Guidelines for the prevention of tuberculosis in health care facilities in resource-
limited settings. WHO/CDS/TB/99.269. IJTLD 1999.
21.
Menzies R, Vissandjee B, Rocher I, St Germain Y. The booster effect in two-step tuberculin testing amongyoung adults in Montreal. Ann Intern Med 1994; 120:190.
22.
Richards NM, Nelson KE, Batt MD, et al. Tuberculin test conversion during repeated skin testing, associatedwith sensitivity to nontuberculous mycobacteria. Am Rev Respir Dis 1979; 120:59.
23.
Gordin FM, Perez-Stable EJ, Flaherty D, et al. Evaluation of a third sequential tuberculin skin test in a chroniccare population. Am Rev Respir Dis 1988; 137:153.
24.
FURTHER studies of geographic variation in naturally acquired tuberculin sensitivity. Bull World Health Organ1955; 12:63.
25.
Centers for Disease Control and Prevention. Guide to Vaccine Contraindications and Precautions. Departmentof Health and Human Services. Available at: http://www.cdc.gov/vaccines/recs/vac-admin/downloads/contraindications-guide-508.pdf
26.
Farhat M, Greenaway C, Pai M, Menzies D. False-positive tuberculin skin tests: what is the absolute effect ofBCG and non-tuberculous mycobacteria? Int J Tuberc Lung Dis 2006; 10:1192.
27.
A World Atlas of BCG Vaccination Policies and Practices http://www.bcgatlas.org/ (Accessed on April 01,2009).
28.
Vinkeles Melchers NV, van Elsland SL, Lange JM, et al. State of affairs of tuberculosis in prison facilities: asystematic review of screening practices and recommendations for best TB control. PLoS One 2013;
29.
Diagnosis of latent tuberculosis infection (tuberculosis screening) in HIV... http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/diagnosis-of-...
9 de 18 03/08/2015 07:18 p.m.

8:e53644.
Arshad S, Bavan L, Gajari K, et al. Active screening at entry for tuberculosis among new immigrants: asystematic review and meta-analysis. Eur Respir J 2010; 35:1336.
30.
Rieder H. What is the role of case detection by periodic mass radiographic examination in tuberculosiscontrol?. In: Toman’s Tuberculosis: Case detection, treatment, and monitoring – questions and answers, 2nded, Frieden, T. (Eds), World Health Organization, Geneva 2004. p.72.
31.
Tarlo SM, Day JH, Mann P, Day MP. Immediate hypersensitivity to tuberculin. In vivo and in vitro studies. Chest1977; 71:33.
32.
Youssef E, Wooltorton E. Serious allergic reactions following tuberculin skin tests. CMAJ 2005; 173:34.33.
Froeschle JE, Ruben FL, Bloh AM. Immediate hypersensitivity reactions after use of tuberculin skin testing.Clin Infect Dis 2002; 34:E12.
34.
Richard Menzies, MD, MSc, personal communication.35.
Ferebee SH. Controlled chemoprophylaxis trials in tuberculosis. Adv Tuberc Res 1969; 17:28.36.
Topic 8005 Version 23.0
Diagnosis of latent tuberculosis infection (tuberculosis screening) in HIV... http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/diagnosis-of-...
10 de 18 03/08/2015 07:18 p.m.

GRAPHICS
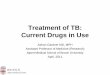
Who should be tested for latent TB infection?*
Those with increased risk of new TB infection (all patients should be tested
regardless of age)
Close contacts of patients with active pulmonary/respiratory TB
Casual contacts of patients with highly contagious active TB
Healthcare workers and other occupations in which there is risk of exposure to patients with
untreated contagious active TB (prison facilities, homeless shelters)
Those with increased risk of reactivation
High risk (all patients should be tested regardless of age)
HIV infection (any stage of illness)
Transplant, chemotherapy, or other major immunocompromising condition
Lymphoma, leukemia, head and neck cancer
Abnormal chest radiograph with apical fibronodular changes typical of healed TB (not including
granuloma)
Silicosis
Renal failure (requiring dialysis)
Treatment with TNF-alpha inhibitors
Moderate risk (patients under age 65 should be tested)
Diabetes mellitus
Systemic glucocorticoids (≥15 mg/day for ≥1 month)
Slightly increased risk (patients under age 50 should be tested)
Underweight (<85 percent of ideal body weight); for most individuals, this is equivalent to body
mass index (BMI) ≤20
Cigarette smoker (1 pack/day)
Chest radiograph with solitary granuloma
TB: tuberculosis; TNF: tumor necrosis factor.
* Only those who would benefit from treatment should be tested, so a decision to test presupposes a
decision to treat if the test is positive.
¶ A second test is warranted if the first test is negative (refer to text).
Δ Baseline two-step testing should be performed, followed by annual testing.
◊ Generally need a single test.
§ The United States Centers for Disease Control and Prevention (CDC) recommends skin testing for all
patients in this category. However, population-based studies demonstrate that the relative risk for
development of active tuberculosis in this category is moderate (2 to 4x that of healthy individuals).
Therefore, an age cutoff of ≤65 is indicated, so that potential risks of isoniazid toxicity in older patients do
not outweigh potential benefit. (Refer to separate table summarizing relative risk for development of active
tuberculosis).
Graphic 74584 Version 5.0
¶
¶
Δ
◊
§
Diagnosis of latent tuberculosis infection (tuberculosis screening) in HIV... http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/diagnosis-of-...
11 de 18 03/08/2015 07:18 p.m.

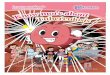
Risk factors for the development of active tuberculosis among persons
infected with Mycobacterium tuberculosis
Risk factor
Estimated risk for TB relative
to persons with no known
risk factor
References
High risk
Acquired immunodeficiency syndrome
(AIDS)
110 to 170 1,2
Human immunodeficiency virus
infection (HIV)
50 to 110 3,4
Transplantation (related to immune-
suppressant therapy)
20 to 74 5 to 8
Silicosis 30 9,10
Chronic renal failure requiring
hemodialysis
10 to 25 11 to 14
Carcinoma of head and neck 16.0 15
Recent tuberculosis (TB) infection (≤2
years)
15.0 16,17
Abnormal chest radiograph with apical
fibronodular changes typical of healed
TB (not granuloma)
6 to 19 18 to 20
Tumor necrosis factor (TNF)-alpha
inhibitors
1.7 to 9 21,22,35,36
Moderate risk
Treatment with glucocorticoids 4.9 23
Diabetes mellitus (all types) 2 to 3.6 24 to 27
Young age when infected (≤4 years) 2.2 to 5 28
Slightly increased risk
Underweight (<85 percent of ideal
body weight); for most individuals
this is equivalent to body mass index
(BMI) ≤20
2 to 3 29
Cigarette smoker (1 pack/day) 2 to 3 30,31
Chest radiograph with solitary
granuloma
2 20,32
Low risk
Infected person, no known risk factor,
normal chest radiograph ("low-risk
reactor")
1 33
Very low risk
Diagnosis of latent tuberculosis infection (tuberculosis screening) in HIV... http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/diagnosis-of-...
12 de 18 03/08/2015 07:18 p.m.

Positive booster (two-step test) with
no other known risk factor and
normal chest radiograph)
0.5 Extrapolated
from 33 and
34
References:
Guelar A, Gatell JM, Verdejo J, et al. A prospective study of the risk of tuberculosis among
HIV-infected patients. AIDS 1993; 7:1345.
1.
Antonucci G, Girardi E, Raviglione MC, et al. Risk factors for tuberculosis in HIV-infected persons. A
prospective cohort study. JAMA 1995; 274:143.
2.
Wood R, Maartens G, Lombard CJ. Risk factors for developing tuberculosis in HIV-1 - Infected adults
from communities with low or very high incidence of tuberculosis. J Acquir Immune Defic Syndr
2000; 23:75.
3.
Selwyn PA, Hartel D, Lewis VA, et al. A prospective study of the risk of tuberculosis among
intravenous drug users with human immunodeficiency virus infection. New Engl J Med 1989;
320:545.
4.
Sakhuja V, Jha V, Varma PP, et al. The high incidence of tuberculosis among renal transplant
recipients in India. Transplantation 1996; 61:211.
5.
Aguado JM, Herrero JA, Gavalda J, et al. Clinical presentation and outcome of tuberculosis in kidney,
liver, and heart transplant recipients in Spain. Spanish Transplantation Infection Study Group,
GESITRA. Transplantation 1997; 63:1278.
6.
Miller RA, Lanza LA, Kline JN, Geist LJ. Mycobacterium tuberculosis in lung transplant recipients. Am
J Respir Crit Care Med 1995; 152:374.
7.
Meyers BR, Halpern M, Sheiner P, et al. Tuberculosis in liver transplant patients. Transplantation
1994; 58:301.
8.
Hong Kong Chest Service/Tuberculosis Research Centre, Madras/British Medical Research Council. A
Double-blind placebo-controlled clinical trial of three antituberculosis chemoprophylaxis regimens in
patients with silicosis in Hong Kong. Am Rev Respir Dis 1992; 145:36.
9.
Cowie RL. The epidemiology of tuberculosis in gold miners with silicosis. Am J Respir Crit Care Med
1994; 150:1460.
10.
Malhotra KK, Parashar MK, Sharma RK, et al. Tuberculosis in maintenance haemodialysis patients.
Study from an endemic area. Postgrad Med J 1981; 57:492.
11.
Lundin AP, Adler AJ, Berlyne GM, Friedman EA. Tuberculosis in patients undergoing maintenance
hemodialysis. Am J Med 1979; 67:597.
12.
Andrew OT, Schoenfeld PY, Hopewell PC, Humphreys MH. Tuberculosis in patients with end-stage
renal disease. Am J Med 1980; 68:59.
13.
Pradhan RP, Katz LA, Nidus BD, et al. Tuberculosis in dialyzed patients. JAMA 1974; 229:798.14.
Rieder HL, Cauthen GM, Comstock GW, Snider DE Jr. Epidemiology of tuberculosis in the United
States. Epidemiol Rev 1989; 11:79.
15.
Sutherland I. Recent studies in the epidemiology of tuberculosis, based on the risk of being infected
with tubercle bacilli. Adv Tuberc Res 1976; 19:1.
16.
Sutherland I. The evolution of clinical tuberculosis in adolescents. Tuberc 1966; 47:308.17.
Nolan CM, Elarth AM. Tuberculosis in a cohort of Southeast Asian refugees: A five-year surveillance
study. Am Rev Resp Dis 1988; 137:805.
18.
Grzybowksi S, McKinnon NE, Tuters L, et al. Reactivations in inactive pulmonary tuberculosis. Am
Rev Resp Dis 1966; 93:352.
19.
Grzybowski S, Fishaut H, Rowe J, Brown A. Tuberculosis among patients with various radiologic
abnormalities, followed by the chest clinic service. Am Rev Resp Dis 1971; 104:605.
20.
Keane J, Gershon S, Wise RP, et al. Tuberculosis associated with infliximab, a tumor necrosis factor ?
- neutralizing agent. N Engl J Med 2001; 345:1098.
21.
Brassard P, Kezouh A, Suissa S. Antirheumatic drugs and the risk of tuberculosis. Clin Infect Dis
2006; 43:717.
22.
Jick SS, Lieberman ES, Rahman MU, Choi HK. Glucocorticoid use, other associated factors, and the
risk of tuberculosis. Arthritis Rheum 2006; 55:19.
23.
Diagnosis of latent tuberculosis infection (tuberculosis screening) in HIV... http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/diagnosis-of-...
13 de 18 03/08/2015 07:18 p.m.

Kim SJ, Hong YP, Lew WJ, et al. Incidence of pulmonary tuberculosis among diabetics. Tuber Lung
Dis 1995; 76:529.
24.
Silwer H, Oscarsson PN. Incidence and coincidence of diabetes mellitus and pulmonary tuberculosis
in a Swedish county. Acta Med Scand 1958; 161:1.
25.
Pablos-Mendez A, Blustein J, Knirsch CA. The role of diabetes mellitus in the higher prevalence of
tuberculosis among Hispanics. Am J Public Health 1997; 87:574.
26.
Boucot KR. Diabetes mellitus and pulmonary tuberculosis. J Chronic Dis 1957; 6:256.27.
Comstock GW, Livesay VT, Woolpert SF. The prognosis of a positive tuberculin reaction in childhood
and adolescence. Am J Epidemiol 1974; 99:131.
28.
Comstock GW. Frost Revisited: The modern epidemiology of tuberculosis. Am J Epidemiol 1975;
101:263.
29.
Maurya V, Vijayan VK, Shah A. Smoking and tuberculosis: an association overlooked. Int J Tuberc
Lung Dis 2002; 6:942.
30.
Gajalakshmi V, Peto R, Kanaka T, Jha P. Smoking and mortality from tuberculosis and other diseases
in India: retrospective study of 43000 adult male deaths and 35000 controls. Lancet 2003; 362:507.
31.
Horwitz O, Wilbek E, Erickson PA. Epidemiological basis of tuberculosis eradication. Longitudinal
studies on the risk of tuberculosis in the general population of a low-prevalence area. Bull World
Health Organ 1969; 41:95.
32.
Comstock GW, Edwards LB, Livesay VT. Tuberculosis morbidity in the US Navy: its distribution and
decline. Am Rev Respir Dis 1974; 110:572.
33.
Ferebee SH. Controlled chemoprophylaxis trials in tuberculosis. Adv Tuberc Res 1969; 17:28.34.
Wolfe F, Michaud K, Anderson J, et al. Tuberculosis infection in patients with rheumatoid arthritis and
the effect of infliximab therapy. Arthritis Rheum 2004; 50:372.
35.
Carmona L, Gómez-Reino JJ, Rodríguez-Valverde V, et al. Effectiveness of recommendations to
prevent reactivation of latent tuberculosis infection in patients treated with tumor necrosis factor
antagonists. Arthritis Rheum 2005; 52:1766.
36.
Graphic 60941 Version 5.0
Diagnosis of latent tuberculosis infection (tuberculosis screening) in HIV... http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/diagnosis-of-...
14 de 18 03/08/2015 07:18 p.m.

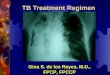
Measuring a reaction to the tuberculin skin test
This figure shows the correct method for measuring a reaction to the
tuberculin skin test. The size of the reaction is measured by the width of
induration, not erythema. In the example shown, the reaction measures
10 mm.
Redrawn from: Testing for Tuberculosis Infection and Disease. In: Core
Curriculum on Tuberculosis: What the Clinician Should Know, Sixth
Edition, Centers for Disease Control and Prevention, 2013. Available at:
http://www.cdc.gov/tb/education/corecurr/default.htm.
Graphic 80766 Version 3.0
Diagnosis of latent tuberculosis infection (tuberculosis screening) in HIV... http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/diagnosis-of-...
15 de 18 03/08/2015 07:18 p.m.

Interpretation of tuberculin skin test
Tuberculin
skin test
reaction
size (mm)
Situation in which reaction is considered positive*
≥5 HIV infection
Close contact of active contagious case
Abnormal chest radiograph with fibrotic changes consistent with old TB
Immunosuppressed patients: TNF-alpha inhibitors, chemotherapy, organ
transplantation, glucocorticoid treatment (equivalent of ≥15 mg/day prednisone for
≥1 month)
≥10 Persons with clinical conditions that increase the risk of reactivation, including
silicosis , chronic renal failure requiring dialysis , diabetes mellitus, some
malignancies (leukemias, lymphomas, carcinoma of the head, neck, or lung),
underweight (≥10 percent ideal body weight), jejunoileal bypass, injection drug
users
Children less than 4 years of age
Foreign born from countries with incidence >25/100,000
Residents and employees in high-risk settings, such as prisons, jails, healthcare
facilities, mycobacteriology labs, and homeless shelters
≥15 Healthy individuals age 4 years and older with low likelihood of true TB infection
TB: tuberculosis; TNF: tumor necrosis factor; TST: tuberculin skin test.
* The goal of testing for latent tuberculosis infection is to identify individuals who are at increased risk for
the development of tuberculosis and therefore would benefit from treatment of latent TB infection. Only
those who would benefit from treatment should be tested, so a decision to test presupposes a decision to
treat if the test is positive (refer to text).
¶ The United States Centers for Disease Control and Prevention (CDC) recommends a 10 mm induration
definition for patients with silicosis or chronic renal failure. However, population-based studies demonstrate
that the relative risk for development of active tuberculosis in this category is high (≥10x that of healthy
individuals). For this reason, many favor a lower threshold for a positive test (≥5 mm).
Δ The CDC indicates that only those foreign-born individuals who immigrated within the past 5 years should
be tested (regardless of age), although others do not favor this practice since most recently arrived foreign
born with positive TST have old (not recent) infection.
◊ Persons with a low likelihood of true TB infection should not be tested routinely unless they are entering a
high-risk setting such as starting employment at a healthcare facility. A threshold of 15 mm is used in the
United States, and is appropriate for healthy individuals with low likelihood of true TB infection and high
likelihood of exposure to nontuberculous mycobacteria (eg, southern United States). However, Canadian
guidelines use a threshold of 10 mm for healthy individuals given the lower likelihood of exposure to
nontuberculous mycobacteria. (Refer to the topic on Epidemiology of nontuberculous mycobacterial
infections.).
Graphic 67357 Version 6.0
¶ ¶
Δ
◊
Diagnosis of latent tuberculosis infection (tuberculosis screening) in HIV... http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/diagnosis-of-...
16 de 18 03/08/2015 07:18 p.m.

Potential causes of false-negative tuberculin tests
Technical (potentially correctable)
Tuberculin material:
Improper storage (exposure to light or heat)
Contamination, improper dilution, or chemical denaturation
Administration:
Injection of too little tuberculin or too deeply (should be intradermal)
Administration more than 20 minutes after drawing up into the syringe
Reading:
Inexperienced or biased reader
Error in recording
Biologic (not correctable)
Infections:
Active tuberculosis (especially if advanced)
Other bacterial infection (typhoid fever, brucellosis, typhus, leprosy, pertussis)
HIV infection (especially if CD4 count <200)
Other viral infection (measles, mumps, varicella)
Fungal infection (South American blastomycosis)
Recent live-virus vaccination (measles, mumps, polio)
Immunosuppressive drugs (corticosteroids, tumor necrosis factor inhibitors, and others)
Metabolic disease (chronic renal failure, severe malnutrition, stress [surgery, burns])
Diseases of lymphoid organs (lymphoma, chronic lymphocytic leukemia, sarcoidosis)
Age (infants <6 months, older adults)
Graphic 58908 Version 9.0
Diagnosis of latent tuberculosis infection (tuberculosis screening) in HIV... http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/diagnosis-of-...
17 de 18 03/08/2015 07:18 p.m.

Disclosures: Madhukar Pai, MD, PhD Nothing to disclose. Dick Menzies, MD, MSc Nothing to disclose. C Fordham von Reyn, MD Nothingto disclose. Elinor L Baron, MD, DTMH Nothing to disclose.
Contributor disclosures are reviewed for conflicts of interest by the editorial group. When found, these are addressed by vetting through amulti-level review process, and through requirements for references to be provided to support the content. Appropriately referenced content isrequired of all authors and must conform to UpToDate standards of evidence.
Conflict of interest policy
Disclosures
Diagnosis of latent tuberculosis infection (tuberculosis screening) in HIV... http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/diagnosis-of-...
18 de 18 03/08/2015 07:18 p.m.