Embed Size (px)
Citation preview

Taste and Smell Lossesin Normal Aging and DiseaseSusan S. Schiffman, PhD
Objective.\p=m-\To review the scientific literature on the alterations in the senses oftaste and smell in the elderly, including causes, diagnosis, prognosis, and treatment.
Data Sources.\p=m-\Original reports and reviews obtained through MEDLINEsearches from 1966 through June 1997 using the MeSH headings of "taste," "tastebuds," "taste disorders," "taste thresholds," "smell," "odors," "aged," and "aging." Ar-ticles frequently cited in reference lists were also included.
Study Selection.\p=m-\All articles were reviewed, tabulated, and summarized.Data Extraction.\p=m-\Criteria for extraction included data quality and validity, sta-
tistical treatment of the data, venue of publication, and relevance to clinical care.Conclusion.\p=m-\Losses of taste and smell are common in the elderly and result
from normal aging, certain disease states (especially Alzheimer disease), medica-tions, surgical interventions, and environmental exposure. Deficits in these chemi-cal senses cannot only reduce the pleasure and comfort from food, but representrisk factors for nutritional and immune deficiencies as well as adherence to specificdietary regimens. Chemosensory decrements can lead to food poisoning or over-$exposure to environmentally hazardous chemicals that are otherwise detectable bytaste and smell. Use of flavor-enhanced food can increase enjoyment of food andhave a positive effect on food intake and immune status.
JAMA. 1997;278:1357-1362
STUDIES OF population trends demon¬strate massive increases in both the ab¬solute numbers and percentage ofour ag¬ing population. From 1900 to 1995, thenumber ofAmericans older than 65 yearsincreased 11 times (from 3.1 million to 33.5million).1·2 During the same period, thepercentage of Americans older than 65years has more than tripled (4.1% in 1900to 12.8% in 1995). By the year2030,20% ofthe US population (69.4 million) will beolder than 65 years.1 In addition, the olderpopulation itself has been getting older.3
A large proportion of the populationolder than 65 years has age-related sen¬
sory losses that impairoverall health, self-sufficiency, and quality of life.4"7 Decre¬ments in the chemical senses of taste andsmell are an unfortunate but common as¬
pect of aging.5"14 These deficits can alterfood choices and intake and subsequentlyexacerbate disease states, impair nutri¬tional status and immunity, and produceweight loss.7·15"17 Conversely, nutritionaldeficits may cause chemosensory loss.Taste and smell decrements can also putthe elderly at risk from noxious chemicalsand poisonings since chemosensory cues
provide warning signals about chemicalsafety.7
Chemosensory impairments are usu¬
ally classified as follows: ageusia (absenceof taste), hypogeusia (diminished sensi¬tivity of taste), dysgeusia (distortion ofnormal taste), anosmia (absence ofsmell),hyposmia (diminished sensitivity ofsmell), and dysosmia (distortion ofnormalsmell).7 Dysgeusia and dysosmia are notnecessarily correlated with loss of sensi¬tivity18 and can occur in the presence orabsence of a stimulus. For example, par-osmia refers to distortion of odor percep¬tion when an odor is present, and phan-tosmia refers to odor sensations in ab¬sence ofan odor stimulus.19 Another term,"cacosmia," is currentlybut notuniformlyused to describe the subjective sense offeeling ill in response to odors.20 Progres¬sive impairment in taste and smell per¬ception occurs with advancing age. Hy¬posmia and hypogeusia tend to becomenoticeable around 60 years of age, al¬though they can occur earlier. Losses be¬come more severe in persons older than70 years.8·15·21 The incidence of chemosen¬sory disorders will increase significantlyover the next decades because of the in¬creasing elderly population.
Intact senses of taste and smell are im¬portant because these chemosensory sys¬tems prepare the body to digest food bytriggeringsalivary, gastric, pancreatic, andintestinal secretions, which are termed "ce¬phalic phase responses."2224 Human andanimal studies show that there is a learnedassociation ofa food's taste and smell sen-
sations with its postingestive effects.23·25"28These associations enable the consumer tomodulate food choice and/or meal size in an¬
ticipation of these postingestive effects.Foods that are generally preferred arethose that are energy dense26 and are as¬sociated with elevated opioid levels.27 Theintensity of taste responses can be modu¬lated by levels of nutrients and digestiveenzymes.29 Importantly, chemosensorysensations enhance feelings ofsatiety andpleasure from a meal and are primary re-inforcers of eating.7·30"32 Sensory stimula¬tion derived from food is especially impor¬tant in old age when other sources ofgratification may be less frequent.
This article provides an overview ofthetaste and smell systems and how theychange with age and describes potentialmethods for treating the chemosensorylosses.
TASTERange of Taste Qualities
Current medical texts generally statethat there are only 4 basic tastes: sweet,sour, salty, and bitter. However, experi¬mental data in a variety ofspecies, includ¬ing humans, monkeys, and rodents, indi¬cate that the full range of taste quality isbroaderthan these 4 prototypical tastes.33Taste qualities such as metallic (ironsalts), umami (monosodium glutamate/5'-nucleotides), and chalky (calcium salts)are also mediated by taste nerves. Aminoacids other than monosodium glutamatehave unique taste qualities.33·34 Fat sensa¬tions can be detected on the lateral pos¬terior sides ofthe tongue without tonguemovement, which suggests that some
component of fat may also activate tastenerves.35 While the English vocabularylacks adequate words to describe the fullrange of taste sensations, other cultureshave more words for taste qualities. Forexample, in Japan the word "umami" isused to describe the taste ofmonosodiumglutamate as well as the meaty taste ofcertain fish and broths.
Losses of Taste PerceptionTaste losses in the elderly result from
normal aging, but mainly from certain dis¬ease states (especially Alzheimer dis¬ease), medications, surgical interven¬tions, and environmental exposure (Tables1 and 2). These losses occur atboth thresh¬old and suprathreshold concentrations. In
From the Department of Psychiatry, Duke UniversityMedical Center, Durham, NC 27710 (e-mail: [email protected]).
Reprints: Susan S. Schiffman, PhD, Department ofPsychiatry, Duke University Medical Center, Box 3259,Durham, NC 27710.
Downloaded From: http://jama.jamanetwork.com/ by a Northern Ontario School of Medicine User on 10/30/2013

Table 1.—Representative Medications or Treat¬ments That Alter Taste and Smell
Lipid-Lowering DrugsCholestyramine, clofibrate, fluvastatin sodium,gemfibrozil, lovastatin, pravastatin sodium
AntihistaminesChlorphenlramine maléate, loratadine, terfenadineand pseudoephedrine
AntimicrobialsAmpicillin, ciprofloxacin, clarithromycin, ofloxacln,streptomycin, tetracyclines
Anti neoplastiesCisplatin, doxorubicin and methotrexate, vincristinesulfate
Anti-inflammatoriesAuranofin, colchicine, dexamethasone, diclofenacpotassium/diclofenac sodium, dimethyl sulfoxlde,gold, hydrocortisone, D-penicillamine andpenicillamine
Bronchodilators and Other Asthma MedicationsAlbuterol sulfate, cromolyn sodium, flunisolide,metaproterenol sulfate, terbutaline sulfate
Antihypertenslves and Cardiac MedicationsAcetazolamide, adenosine, amiloride, benazeprilhydrochloride and hydrochlorothiazide, betaxololhydrochloride, captopril, clonidine, diltiazem,enalapril, ethacrynic acid, nifedipine, propranolol,spironolactone
Muscle Relaxants and Drugs for the Treatmentof Parkinson Disease
Baclofen, dantrolene sodium, levodopaAntidepressants and Anticonvulsants
Amitriptyline hydrochloride, carbamazepine,clomipramine hydrochloride, clozapine,desipramine hydrochloride, doxepin hydrochloride,fluoxetine hydrochloride, imipramine, lithiumcarbonate, phenytoin, trifluoperazine
Radiation TherapyRadiation to head
VasodilatorsDipyridamole, nitroglycerin patch
most cases the sense of taste is not totallyabsent (ageusia), but rather it is reduced(hypogeusia) or distorted (dysgeusia).
Impairment At Threshold Concen¬trations.—Two types of taste thresholds(detection thresholds and recognitionthresholds) are elevated in older per¬sons.6·10·13 Ataste detection threshold is theconcentration for the absolute threshold oftaste sensation; a taste recognition thresh¬old is the lowest concentration at which atastant is correctly identified. Elevatedthresholds (ie, reduced sensitivity) forsweet, sour, salty, and bitter as well as fortastes ofamino acids, including glutamatesalts, occur in healthy older individuals.6·10The degree of loss depends on the chemi¬cal structure of the compounds tested aswell as the medical condition and pharma¬cological regimen of the individual.6"7·36"39Forprototypical tastes such as sodium chlo¬ride (NaCl) (salty), sucrose (sweet), citricacid (sour), and quinine hydrochloride (bit¬ter), decrements in taste using whole-mouth stimulation in elderly persons whosuffer from no diseases and take no medi¬cations are modest. Greater losses in tastesensitivity at threshold levels occur, how¬ever, for elderly individuals who take amoderate number ofmedications but oth¬erwise live active, normal lives.6·39 Com¬pared with a young cohort, the average de¬tection thresholds for elderly individualswith 1 or more medical conditions and tak-
Table 2.—Representative Medical Conditions ThatAffect the Senses of Taste or Smell
NervousAlzheimer diseaseBell palsyDamage to chorda tympanlEpilepsyHead traumaKorsakoff syndromeMultiple sclerosisParkinson diseaseTumors and lesions
NutritionalCancerChronic renal failureLiver disease including cirrhosisNiacin (vitamin B3) deficiencyVitamin B12 deficiencyZinc deficiency
EndocrineCushing syndromeDiabetes mellitusHypothyroidismKailman syndromeTurner syndrome
LocalAllergic rhinitis, atopy, and bronchial asthmaSinusitis and polyposisXerostomic conditions including Sjögren syndrome
Viral infectionsAcute viral hepatitisInfluenzalike infections
ing an average of3.4 medications were 11.6times higher for sodium salts; 4.3 timeshigher for acids; 7.0 times higher for bit¬ter compounds; 2.5 times higher for aminoacids; 5.0 times higher for glutamate salts;and 2.7 times higher for sweeteners.6 Clini¬cal studies ofpatients with protein malnu¬trition (wasting) indicate that taste lossesat the threshold level are even more se¬vere.15
Impairment ofSuprathreshold TastePerception.—The majority of supra¬threshold studies have shown that elder¬ly persons perceive a broad range oftastes as being less intense than youngpersons.6·13·15 Differences across studiesregarding the degree of loss probablyarise in part from the medical status andpharmaceutical agents used by the sub¬jects as well as their cognitive status. Re¬ductions in perceived suprathresholdtaste intensity of sweeteners40 and aminoacids41 using whole-mouth testing varywiththechemicalstructureofthetastant.Elderly persons also have reduced abilityto discriminate intensity differences be¬tween various concentrations of a tas-tant.6,15'42 Marked age-related changes inregional taste sensitivity also occur overdifferent areas ofthe tongue.43·44
Age-related impairments also occurin perception of complex food systems,which requires integration of taste andsmell sensations. Elderly persons havereduced ability to identify foods on thebasis of taste (and smell).5 Malnutritionand wasting make it even more difficultto identify foods and food ingredientsbased on sensory cues.15
Taste losses in perception of sweetand salty qualities can have health con-
sequences for the elderly. Decrementsin sweet taste perception make elderlypersons with diabetes more vulnerableto adverse effects from excess consump¬tion of sugar. Losses in salt (NaCl) per¬ception can make it difficult for hyper¬tensive patients to comply with severesalt restriction simply because food tothem may seem relatively tasteless. Ifelderly persons add NaCl to reduce bit¬terness of foods (one effect of addingNaCl45), this can increase blood pressureand the chance ofstroke in salt-sensitivehypertensive patients. Reductions insalt intake should be gradual becausesevere reduction in salt intake can back¬fire and increase preference for salt.46
Anatomy and Physiology of TasteTaste sensations occur when chemicals
in foods and beverages come in contactwith polarized neuroepithelial cells thatare clustered into buds scattered on thedorsal surfaceofthe tongue, tonguecheekmargin, base of the tongue near ducts ofthe sublingual glands, the soft palate,pharynx, larynx, epiglottis, uvula, andfirst third of the esophagus.7·47 Recently,taste receptor-like cells have also beenidentified in the mucosa of the stomachand intestine.48 Chemicals from foodstimulate taste buds during chewing andswallowing, while tongue movements, es¬
pecially pressing food (eg, chocolate)against the roof of the mouth, prolong or
improve taste sensations on the soft pal¬ate. Persons with dentures that cover thesoft palate lose sensory input from food inthis mouth region. The temporal sequenceof taste sensations during oral manipula¬tion and swallowing of food provides theuniqueness or "melody" of each recipe.
Taste buds are ovoid structures thatconsist of 50 to 100 specialized cells ar¬
ranged like segments in an orange. Tastecells constantly reproduce themselveswith a lifespan ofapproximately 10 to lOVédays. This continuous renewal processmakes the sense oftaste vulnerable to mal¬nutrition, which can impair reproductionof taste cells and reduce taste sensitivity.7Lingual taste buds are located on elevatedstructures called papillae. The papillae dis¬tributed on the anterior two thirds ofthetongue are called fungiform papillae andusually contain 1 to 18 taste buds. Foliatepapillae consist of vertical folds and arelocated on the posterior lateral sides ofthetongue; they contain taste receptor cellsthat are especially sensitive to sour tastes.The circumvallate papillae are located onthe back ofthe tongue and are arranged ina chevron-shaped form pointing caudally;they are called circumvallate papillae be¬cause they are surrounded by "moats." Avariety of structural components in tastecells have been shown to play a role in tastetransduction, including sodium channels,
Downloaded From: http://jama.jamanetwork.com/ by a Northern Ontario School of Medicine User on 10/30/2013

potassium channels, and 2 second messen¬
ger systems, the adenylate cyclase sys¬tem and the phosphatidylinositol sys¬tem,49,50 but little is known about how theychange with age.
Three cranial nerves (Figure 1) trans¬mit taste signals from taste receptor cellsto the medulla in the brainstem.7·30 Tastebuds located in fungiform papillae and theanterior walls of the foliate papillae areinnervated by the chorda tympani nerve,which is a branch of the seventh cranialnerve. Most of the taste buds on the softpalate are innervated by another branchof the seventh cranial nerve called the"greater superficial petrosal nerve." Theremaining taste buds on the soft palateare innervated by the deep petrosalbranch of the ninth cranial nerve. Tastebuds on the circumvallate papillae, thepharyngeal part of the tongue, the oralpart of the pharynx, and the posteriorwalls ofthe foliate papillae are innervatedby the ninth (glossopharyngeal) nerve.Taste buds on the far posterior tongue,the epiglottis, the larynx, and the esopha¬gus are innervated by the superior laryn-geal branch ofthe vagus nerve.
The 7th, 9th, and 10th nerves project tothe rostral portion of the nucleus of thesolitary tract (NST),23·30 which is a longi¬tudinally organized column of neurons inthe dorsal medulla. The NST receives in¬formation not only from the gustatorysystem, but also from visceral sensory fi¬bers originating in the esophagus, stom¬ach, intestines, and liver.23·30 Visceral in¬formation is distributed caudally in thesolitary tract.23·51·52 Information from thefirst cranial nerve (olfactory nerve) alsoconverges in the NST.53 Thus, the NST isthe first processing area in which tastesignals can affect ingestive and digestiveactivitybyproducinggastric secretion, in¬creased pancreatic exocrine secretion,and increased secretion of insulin.
Axons from the gustatory part of NSTproject to the ventroposteromedial nucleusof the thalamus based on monkeyanatomy.52 Neurons in the caudal divi¬sion of NST branch to the parabrachialnucleus, which sends further projectionsto lateral hypothalamus, amygdala, and thebed nucleus of stria terminalis. Finally,taste neurons in the ventroposterome¬dial nucleus ofthe thalamus project to theprimary gustatory cortex, which consistsof 2 discontinuous areas: the insula-operculum and a spatially separate area onthe lateral convexity. Neurons on the an¬terior insula project to secondary cortexlocated on the orbitofrontal surface.
Chemesthetic (pungent) qualities in theoral cavity are transduced by the trigemi-nal nerve as well as free nerve endings ofthe chorda tympani nerve, the glossopha¬ryngeal nerve, and the vagus nerves.54Examples of chemesthetic qualities are
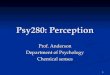
Figure 1.—Peripheral taste pathways.
pungent sensations such as those fromnicotine, capsaicin, and piperine (chemi¬cals in red and black peppers, respec¬tively). Pungency in the oral cavity is gen¬erally not regarded a taste, but rather adifferent sense related to nociception.Causes of Taste Losses
The cause of taste changes in normalaging in the absence of disease and medi¬cations is not fully understood. Studies ofanatomical losses in the structures ofthetaste system in older individuals havebeen equivocal.47·55 While some studieshave found reduced numbers of papillaeand/or taste buds, other studies have notfound losses during normal aging. Mis-tretta65 concluded that taste losses fromnormal aging are due to changes in tastecell membranes (eg, altered functioningof ion channels and receptors) rather thanlosses of taste buds.
Medications (Table 1) and medical con¬ditions (Table 2) play the major role in tastelosses and distortions in both healthy andwasting older patients.6·7·15·66 Clinical stud¬ies have implicated over 250 drugs in al¬tered taste sensations.7,56·57 Prescriptionmedications are consumed disproportion¬ately by the elderly with per capita con¬
sumption 3 times higher than theiryounger counterparts.58 According toLewis et al,59 the average number ofmedi¬cations used by community-dwelling el¬derly persons older than 65 years rangesfrom 2.9 to 3.7 medications, and this num¬ber increases significantly for elderly per¬sons living in nursing homes.
Neither the site nor mechanism of ac¬tion for most pharmaceutical compoundsthat induce taste losses is known, but medi¬cations can act at several levels, including
peripheral receptors, chemosensory neu¬ral pathways, and/or the brain. Drugs se¬creted into the saliva can exert adverse ef-fects on the taste system either bymodifying taste transduction mecha¬nisms orby producing a taste oftheir own.
Drugs can also diffuse from the blood tostimulate receptors on thebasolateral sideof taste receptor cells. Taste losses asso¬ciated with drugs or concurrent with pro¬tein malnutrition and wasting may also becaused by impaired turnover oftaste cells,although there have been no formal ex¬
periments to test this hypothesis. The rela¬tive frequencies with which drugs altertaste and smell have not yet been deter¬mined using quantitative experimentaltesting procedures.SMELLSmell Perception in the Elderly
The qualitative range of odor is verybroad. Olfactory losses in the elderly, liketaste losses, result fromnormalaging, cer¬tain disease states (especially Alzheimerand Parkinson disease), medications, sur¬
gical interventions, and environmentalexposure. Most studies suggest that thesense of smell is even more impaired byaging than the sense oftaste. These lossesoccur at both threshold and suprathresh¬old concentrations.
Impairment of Smell at ThresholdConcentrations.—Psychophysical stud¬ies of smell indicate that significant age-related losses occur at threshold concen-trations.5·11·12·60·61 Elevated detection andrecognition thresholds have been re¬
ported for a broad range offood odors andvolatile compounds. Anoverviewofthesestudies indicates that for most odors, thethresholds in a normal elderly cohort are
Downloaded From: http://jama.jamanetwork.com/ by a Northern Ontario School of Medicine User on 10/30/2013

Figure 2.—Olfactory pathways.
2 to 15 times higher than in a young co¬hort. Olfactory threshold measures arenot strongly affected by cognitive losses,although suprathreshold performance isseverely impaired. In Alzheimer disease,olfactory detection deficits are similar tothose of age-matched controls until thecognitive deficits become fairly ad¬vanced.61 Olfactory detection losses inParkinson disease are independent ofcognitive status.60 The degree ofolfactoryloss tends to be more uniform across vola¬tile compounds with different struc¬tures11 than for taste where degree oflosstends to be more structure specific. Wast¬ing further exacerbates olfactory losses,and many patients with "failure to thrive"suffer from severe hyposmia.15
Impairment ofSuprathreshold OdorPerception.—A variety of methodologi¬cal approaches have shown that the elder¬ly have diminished suprathreshold func¬tioning of olfaction,5·14,21,62 and thechemesthetic sense in the nose (eg, car¬bon dioxide, which stimulates the trigemi-nal nerve).63 Elderly individuals have re¬duced capacity to discriminate the degreeof difference between odors of differentqualities compared with their youngercounterparts.5,21 Performance on tasks thatrequire identification of odors is impairedin healthy elderly persons,69 but there isheterogeneity among individuals.64 Morethan three fourths ofelderly persons olderthan 80 years have major difficulty per¬ceiving and identifying odors.9 Odor iden¬tification is especially impaired in pa-
tients with certain neurodegenerativediseases, including Alzheimer disease.9,65
Elderly persons often attribute re¬duced intensity of foods to decrements intheir taste perception. The reason for thisis that sensations of food in the mouth are
presumed to be tastes, but are in fact par¬tially produced by aroma or smell. Whenfood is placed in the oral cavity, the odor¬ous molecules move up the back of thethroat, and the smell is perceived retro-nasally. Odors sensed at a meal are pre¬dominantly perceived retronasally.Anatomy of the Olfactory System
Olfactory receptor cells are bipolar neu¬rons that are located in the olfactory epi¬thelium (Figure 2) on the dorsal aspect ofthe nasal cavity, the septum, and part ofthe superior turbinâtes. The turbinâtes inthe nose create airflow patterns that al¬low volatile compounds to reach the olfac¬tory cells. Olfactory cells, like taste cells,undergo constant renewal althoughthe av¬
erage turnover time is 3 times longer, ie,about 30 days. Odorants bind to recep¬tors on the olfactory receptor cells. Thesereceptors belong to a G-protein-coupledreceptor superfamily associated with theadenylate cyclase and phosphoinositol sig¬naling systems.66,67 Coding ofodor qualitymay involve specific temporal sequencesof firing that is compound specific.68
The axons ofolfactory bipolar cells tra¬verse through small holes in the cribri¬form plate of the ethmoid bone to the ol¬factory bulb where they form synapses
in intricate neural masses called "glo-meruli."People who fall can sever the neu¬rons that course through the cribriformplate. Falls are common among the elder¬ly and account for some ofthe odor lossesthey experience. During the aging pro¬cess, the glomeruli atrophy as fibers de¬generate and disappear such that the ol¬factory bulb takes on a moth-eaten ap¬pearance.
The olfactory tract projects caudallythrough the medial aspects of the olfac¬tory bulb to the anterior olfactory nucleus,the olfactory tubercle, the prepiriform cor¬
tex, and the amygdala. Many of thesestructures are part ofthe so-called limbicsystem ofthe brain, which also processesemotions and memories. This neuroana-tomical overlap between olfaction and emo¬tions may provide an anatomical basis forthe capacity of odors to produce hedonicresponses. Olfactory information is ulti¬mately transmitted to the hypothalamus,and this anatomical projection empha¬sizes the importance of olfaction in eatingand nutrition.
Causes of Olfactory LossesIn healthy elderly persons, olfactory
losses result from 1 or more causes, in¬cluding normal aging, medications, viralinsult, cumulated exposure to toxic fumes,and head trauma (Tables 1 and 2). Mag¬netic resonance imaging suggests thatposttraumatic olfactory dysfunction is as¬sociated with damage primarily in the ol¬factory bulbs and tracts and the inferiorfrontal lobes.69 During aging, anatomicaland physiological changes also occur in thestructure of the upper airway, the olfac¬tory epithelium, olfactory bulb andnerves, hippocampus and amygdaloidcomplex, and hypothalamus, including re¬ductions in cell number, damage to cells,and diminished levels of neurotransmit-ters.7'70,71 In certain disease states, such asAlzheimer disease and Parkinson disease,the losses can be profound.9Impact of Chemosensory Losses onFood Intake, Digestion, and Immunity
Chemosensory losses in the elderly can
play a major role in their nutritional andimmune status.15·72·73 When chemosensorysystems are compromised, taste and smellsignals cannot serve as cues for the meta¬bolic consequences of food ingestion. Thiscan be troublesome for elderly personswho no longer have control over foodchoices. While readjusting intake whenflavor-calorie cues are switched is diffi¬cult for most persons,74 it may be espe¬cially difficult for elderly persons in hos¬pital and nursing homes when they ini¬tially eat unfamiliar food.
Lost oftaste and smell also reduces themotivation to eat. Undernutrition result¬ing from taste and smell losses is a major
Downloaded From: http://jama.jamanetwork.com/ by a Northern Ontario School of Medicine User on 10/30/2013

cause of progressive involuntary weightloss (wasting) and ultimately increased dis¬ease susceptibility and decreased immu-nocompetence.7·15 Other causes of wast¬ing in older cohorts are malignancy, chronicdisease, or chronic infection, which pro¬duce cachexia or loss of lean body massfrom hypermetabolism, despite adequateor increased nutrient intake. Cachexia maybe accompanied by elevated cytokine pro¬duction, including tumor necrosis fac¬tor.76 The key to effective treatment ofwasting is to identify the précipitants andintervene early to prevent progression.76Thus, it is important to determine if theprecipitant of wasting is undernutritiondue to taste and smell losses or ifthe causeis cachexia. Ifthe cause is loss oftaste andsmell, flavor enhancement (see below) hasbeen found to be helpful.7·16Clinical Evaluation of Tasteand Smell Disorders
Clinical evaluation of elderly patientswith chemosensory complaints should in¬clude 4 steps: (1) medical history, (2) physi¬cal examination, (3) psychophysical test¬ing, and (4) medical imaging.77 First, thehistory oftaste and smell complaints playsan important role in diagnosis because itprovides information about the events as¬sociated with the onset ofthe loss. For ex¬
ample, taste alterations may occur afterstarting a new medication. Odor losses maybe associated with a virus. However, manychemosensory losses in the elderly are
gradual and progressive overyears and arenot associated with a particular event. Sec¬ond, a physical examination should be per¬formed. This should include examinationof the head and neck, including ears andupper respiratory tract. Nasal airwaysshould be examined for obstructions; a va¬soconstrictor can be applied to improve vi¬sualization. Nasal mucous membranesshould be examined for abnormal condi¬tions. Examination of the olfactory epi¬thelium itself is difficult even with smallmodern instruments. A neurological ex¬amination is essential, including a mentalstatus examination, memory testing (eg,for Alzheimer disease), and testing ofmo¬
tor, gait, and cranial nerve functioning (aswell as peripheral nerves and autonomiefunctioning). Third, thorough psychophysi¬cal evaluations of taste and smell shouldbe performed by a specialist trained to as¬sess patients with taste and smell com¬
plaints. A variety of quantitative psycho-physical tests can be used in clinicalsettings6·8·10"12·38·41 to evaluate chemosen¬sory functioning in the elderly. These in¬clude threshold tests that determine whena taste or odor can first be detected andrecognized as well as suprathreshold teststhat measure the ability to discriminateand identify tastes and smells. Thoroughquantitative testing provides far more ac-
curate assessment of the degree of lossthan perfunctory taste and smell exami¬nations commonly used that simply test forageusia or anosmia. Fourth, medical im¬aging ofthe head may assist in diagnosiswhen structural causes are suspected,69 butthey are negative in the majority ofcases.
Treatment of ChemosensoryLosses in the Elderly:Use of Flavor Enhancement
There are no proven pharmacologicalmethods to treat age-related chemosen¬sory decrements,7 and the prognosis forrecovery of smell and taste sensations ispoor. Hyposmia (but not anosmia) can betreated by adding simulated food flavorsto meats, vegetables, and nutritious foodsto amplify the odor intensity. Simulatedflavors are mixtures ofodorous moleculesthat are extracted from natural productsor are synthesized after chemical analysisofthe target food. They are basically con¬centrated essences that are comparableto frozen concentrated orange juice or ex¬tract ofvanilla. Flavors are not spices anddo not irritate the stomach, which is im¬portant because gastric intolerance tospices is a common complaint in elderlyindividuals.78
Amplification ofthe flavor levels in foodsto optimal concentrations for the elderlycan improve food enjoyment, have a posi¬tive effect on food intake, and foster ap¬propriate nutritional intake.5'72·73 For ex¬
ample, chicken can be marinated withchicken flavor to amplify its aroma. A va¬
riety of flavors (eg, bacon or cheese fla¬vor) can be added to soups and veg¬etables. The elderly often complain that"food doesn't taste the way it used to" andbelieve that food quality was better intimes past, ie, when they were young. Forsuch persons, elevated concentrations offlavor may compensate for their losses intaste and smell that have occurred dur¬ing the aging process.
Flavor enhancement of foods for wast¬ingpatients has been used over the last 25years to increase intake ofnutrient-densefoods.5,7·15·72·73 Flavor amplification of foodfor elderly retirement home residents re¬sulted in improved immune status.72 Con¬sumption of foods flavor enhanced withlow-sodium beef, bacon, and ham flavorsamong others produced increased bloodlevels of and lymphocytes and im¬proved physical strength, but did not al¬ter total dietary intake and other bio¬chemical measures.
Sensory interventions in addition to fla¬vorenhancement can be helpful when tasteand smell losses impair appetite. First, pro¬viding meals with a variety of tastes andflavors may improve intake.7·79 Switchingamong different foods on the plate at a mealreduces sensory adaptation or fatigue, andproviding meals with a variety of tastes
and flavors increases the likelihood that atleast 1 item on the plate will be appealing.Varying texture quality as well as tasteand smell can also improve intake. Vari¬ety of taste and smell is especially impor¬tant for wasting patients who frequentlyreceive only oral liquid formulations forsubsistence.15 Monosodium glutamate hasalso been used as a palatability en¬hancer.80 Dietary supplementation withzinc sulfate, vitamin A, or niacin has beenused inthe past,7butevidence fortheiref¬fectiveness is not compelling.
Bitter tastes can be problematic forolder persons who have reduced sense ofsmell because the bitterness becomes moresalient. When bitter substances are in¬gested, they tend to linger on the back ofthe tongue as bitter tastante fill the"moats" ofthe circumvallate papillae. Add¬ing coffee and chocolate extracts to foodsor medications can partially mask the bit¬terness. Bitter tastes are potentially mostproblematic for "supertasters"81 who per¬ceive bitterness as more intense becauseoftheirgenetics. Tolerance forbitter taste,however, varies by culture.82
Sensory interventions are not neces¬
sary for all elderly persons. Some olderindividuals are willing to eat monotonousdiets.83 There also appear to be fewer foodaversions in the elderly probably due toreductions in the sense of smell.78·84 In ad¬dition, the degree ofsensory loss does notalways predict intake or the degree of re¬duction ofpleasure obtained from food.85This is probably due to differences in cop¬ing skills as well as the type of losses sus¬tained. Many elderly persons are simplyunaware of smell loss in normal aging.86
In summary, elderly persons whocomplain of changes in taste of food andthose who have weight loss may have a
variety ofdisorders oftaste and smell. Athorough evaluation may reveal under¬lying causes such as medications ormedical disorders, but many causes arenot easily reversed. Enhancing food fla¬vors and understanding triggers fortaste and smell can help older patientsadjust to the physiologic changes thatoccur with age and help maintain appe¬tite and food enjoyment.
This work was supported by grant NIA AG00443from the National Institute on Aging.References1. StatisticalAbstract ofthe United States1996.Wash-ington, DC: US Bureau of the Census; 1996:15-16.2. Wattenberg BJ. The Statistical History of theUnited States: From Colonial Times to the Present.New York, NY: Basic Books; 1976:15.3. A Profile of Older Americans. Washington, DC:American Association of Retired Persons; 1995:1-13.4. Kline DW. Optimizing the visibility of displaysfor older observers. Exp Aging Res. 1994;20:11-23.5. Schiffman S. Changes in taste and smell with age:psychophysical aspects. In: OrdyJM, Brizzee K, eds.Sensory Systems and Communication in the El-derly: Aging, Volume 10. New York, NY: RavenPress; 1979:227-246.6. Schiffman SS. Perception of taste and smell in el-
Downloaded From: http://jama.jamanetwork.com/ by a Northern Ontario School of Medicine User on 10/30/2013

derly persons. Crit Rev Food SciNutr. 1993;33:17-26.7. Schiffman SS. Taste and smell in disease. NEngl JMed. 1983;308:1275-1279,1337-1343.8. Doty RL, Shaman P, Applebaum SL, et al. Smellidentification ability: changes with age. Science. 1984;226:1441-1443.9. Doty RL. Olfactory capacities in aging and Alzhei-mer's disease. Ann N Y Acad Sci. 1991;640:20-27.10. Stevens JC, Cruz LA, Hoffman JM, PattersonMQ. Taste sensitivity and aging. Chem Senses. 1995;20:451-459.11. Cain WS, Gent JF. Olfactory sensitivity. J ExpPsychol Hum Percept Perform. 1991;17:382-391.12. Cain WS, Stevens JC. Uniformityofolfactory lossin aging. Ann N YAcad Sci. 1989;561:29-38.13. Murphy C. Nutrition and chemosensory percep-tion in the elderly. Crit Rev Food Sci Nutr. 1993;33:3-15.14. Murphy C. Age-related effects on the threshold,psychophysical function, and pleasantness of men-thol. J Gerontol. 1983;38:217-222.15. Schiffman SS, Wedral E. Contribution of tasteand smell losses to the wasting syndrome. Age Nutr.1996;7:106-120.16. Mattes RD, Cowart BJ. Dietary assessment ofpatients with chemosensory disorders. JAmDietAs-soc. 1994;94:50-56.17. Duffy VB, Backstrand JR, Ferris AM. Olfactorydysfunction and related nutritional risk in free-living,elderly women. J Am Diet Assoc. 1995;95:879-886.18. Cowart BJ, Garrison LB, Young IM, Lowry LD.A discrepancy between odor thresholds and identifi-cation in dysosmia. Chem Senses. 1989;14:692.19. Nordin S, Murphy C, Davidson TM, et al. Preva-lence and assessment ofqualitative olfactory dysfunc-tion in different age groups. Laryngoscope. 1996;106:739-744.20. Bell IR, Schwartz GE, Peterson JM, Amend D.Self-reported illness from chemical odors in youngadults without clinical syndromes or occupational ex-
posures. Arch Environ Health. 1993;48:6-13.21. Schiffman SS, Warwick ZS. Changes in tasteand smell over the lifespan. In: Friedman MI,Tordoff MG, Kare MR, eds. Chemical Senses: Ap-petite and Nutrition, Volume 4. New York, NY:Marcel Dekker; 1991:341-365.22. Teff KL, Engelman K. Palatability and dietaryrestraint. Physiol Behav. 1996;60:567-573.23. Schiffman SS, Warwick ZS. The biology of tasteand food intake. In: Bray GA, Ryan DH, eds. The Sci-ence of Food Regulation. Baton Rouge: LouisianaState University Press; 1992:293-312. PenningtonCenter Nutrition Series, Volume 2.24. Giduck SA, Threatte RM, Kare MR. Cephalic re-flexes. J Nutr. 1987;117:1191-1196.25. Warwick ZS, Schiffman SS. Flavor-calorie rela-tionships. Physiol Behav. 1991;50:465-470.26. Booth DA. Food-conditioned eating preferencesand aversions with interoceptive elements. Ann N YAcad Sci. 1985;443:22-41.27. DrewnowskiA, Krahn DD, Demitrack MA, NairnK, Gosnell BA. Naloxone, an opiate blocker, reducesthe consumption of sweet high-fat foods in obese andlean female binge eaters. Am J Clin Nutr. 1995;61:1206-1212.28. Friedman MI. Metabolic control of food intake.Bol Asoc Med P R. 1989;81:111-113.29. Giza BK, Scott TR, Vanderweele DA. Adminis-tration of satiety factors and gustatory responsive-ness in the nucleus tractus solitarius of the rat. BrainRes Bull. 1992;28:637-639.30. Scott TR. Taste. World Rev Nutr Diet. 1992;67:1-39.31. Scott TR, Yan J, Rolls ET. Brain mechanisms ofsatiety and taste in macaques. Neurobiology. 1995;3:281-292.32. Warwick ZS, Hall WG, Pappas TN, Schiffman SS.Taste and smell sensations enhance the satiating ef-fect ofboth a high-carbohydrate and a high-fat meal inhumans. Physiol Behav. 1993;53:553-563.33. Schiffman SS, Erickson RP. Psychophysics. In:Simon SA, Roper SD, eds. Mechanisms of TasteTransduction. Boca Raton, Fla: CRC Press; 1993:395-424.34. Plata-Salaman CR, Scott TR, Smith-Swintosky
VL. Gustatory neural coding in the monkey cortex:L-amino acids. J Neurophysiol. 1992;67:1552-1561.35. Schiffman SS, Graham BG, Vance AR, et al. De-tection thresholds for emulsified oils in young and el-derly subjects. Chem Senses. 1992;17:693.36. Frank ME, Hettinger TP, Mott AE. The sense oftaste. CritRev Oral Biol Med. 1992;3:371-393.37. Cowart BJ, Yokomukai Y, Beauchamp GK. Bit-ter taste in aging. Physiol Behav. 1994;56:1237-1241.38. Schiffman SS, Crumbliss AL, Warwick ZS, Gra-ham BG. Thresholds for sodium salts in young andelderly subjects. Chem Senses. 1990;15:671-678.39. Schiffman SS. The role of taste and smell in ap-petite and satiety. In: Wahlqvist ML, Truswell AS,Smith R, Nestell PJ, eds. Nutrition in a SustainableEnvironment: Proceedings of the XV InternationalCongress ofNutrition: IUNSAdelaide. London, En-gland: Smith-Gordon; Niigata-Shi, Japan: Nishimura;1994:728-731.40. Schiffman SS, Lindley MG, Clark TB, Makino C.Molecular mechanism of sweet taste: relationship ofhydrogen bonding to taste sensitivity for both youngand elderly. Neurobiol Aging. 1981;2:173-185.41. Schiffman SS, Clark TB. Magnitude estimates ofamino acids for young andelderly subjects. NeurobiolAging. 1980;1:81-91.42. Gilmore MM, Murphy C. Aging is associated withincreased Weber ratios for caffeine, but not for su-crose. Percept Psychophys. 1989;46:555-559.43. Matsuda T, Doty RL. Regional taste sensitivityto NaCl. Chem Senses. 1995;20:283-290.44. Bartoshuk LM, Desnoyers S, Hudson C, et al.Tasting on localized areas. Ann N Y Acad Sci. 1987;510:166-168.45. Breslin PA, Beauchamp GK. Suppression of bit-terness by sodium. Chem Senses. 1995;20:609-623.46. Beauchamp GK, Bertino M, Burke D, EngelmanK. Experimental sodium depletion and salt taste innormal human volunteers. Am J Clin Nutr. 1990;51:881-889.47. Bradley RM. Effects of aging on the anatomyand neurophysiology of taste. Gerodontics. 1988;4:244-248.48. H\l=o"\fer D, Puschel B, Drenckhahn D. Taste re-
ceptor-like cells in the rat gut identified by expres-sion ofalpha-gustducin. Proc Natl Acad Sci U S A.
1996;93:6631-6634.49. Kinnamon SC, Margolskee RF. Mechanisms oftaste transduction. Curr Opin Neurobiol. 1996;6:506-513.50. Spielman AI, Huque T, Whitney G, Brand JG.The diversity of bitter taste signal transductionmechanisms. Soc Gen Physiol Ser. 1992;47:307-324.51. Glenn JF, Erickson RP. Gastric modulation ofgustatory afferent activity. Physiol Behav. 1976;16:561-568.52. Pritchard TC. The primate gustatory system. In:Getchell TV, Doty RL, Bartoshuk LM, Snow JB, eds.Smell and Taste in Health and Disease. New York,NY: Raven Press; 1991:109-125.53. Van Buskirk RL, Erickson RP. Odorant re-
sponses in taste neurons of the rat NTS. Brain Res.1977;135:287-303.54. Green BG. Chemesthesis. Trends Food Sci Tech-nol. 1996;7:415-420.55. Mistretta CM. Aging effects on anatomy andneurophysiology of taste and smell. Gerontology.1984;3:131-136.56. Schiffman SS. Drugs influencing taste and smellperception. In: Getchell TV, Doty RL, Bartoshuk LM,Snow JB, eds. Smell and Taste in Health and Dis-ease. New York, NY: Raven Press; 1991:845-850.57. Physicians'Desk Reference. 49th ed. Des Moines,Iowa: Medical Economics; 1995.58. Kasper J. Prescribed medicines: use, expendi-tures, and sources ofpayment. In: US Dept ofHealthand Human Services. National Health Care Expen-ditures Study Data Preview 9. Hyattsville, Md: USDept of Health and Human Services, Public HealthService, National Center for Health Services Re-search; 1982. DHHS publication PHS 82-3320.59. Lewis IK, Hanlon JT, Hobbins MJ, Beck JD.Use ofmedications with potential oral adverse drugreactions in community-dwelling elderly. Spec CareDent. 1993;13:171-176.
60. Doty RL, Riklan M, Deems DA, et al. The olfac-toryand cognitive deficits ofParkinson's disease. AnnNeurol. 1989;25:166-171.61. Serby M, Larson P, Kalkstein D. The nature andcourse ofolfactorydeficits in Alzheimer's disease. AmJ Psychiatry. 1991;148:357-360.62. Stevens JC, Cain WS. Age-related deficiency inthe perceived strength ofsix odorants. Chem Senses.1985;10:517-529.63. Stevens JC, Plantinga A, Cain WS. Reduction ofodor and nasal pungency associated with aging. Neu-robiol Aging. 1982;3:125-132.64. Wysocki CJ, Gilbert AN. National GeographicSmell Survey. Ann N Y Acad Sci. 1989;561:12-28.65. Schiffman SS, Clark CM, Warwick ZS. Gustatoryand olfactory dysfunction in dementia. Neurobiol Ag-ing. 1990;11:597-600.66. Breer H. Odor recognition and second messengersignaling in olfactory receptor neurons. Semin CellBiol. 1994;5:25-32.67. Sullivan SL, Ressler KJ, Buck LB. Odorant re-
ceptordiversity and patterned gene expression in themammalian olfactory epithelium. Prog Clin Biol Res.1994;390:75-84.68. Wehr M, Laurent G.Odour encoding by temporalsequences of firing in oscillating neural assemblies.Nature. 1996;384:162-166.69. Yousem DM, Geckle RJ, Bilker WB, et al. Post-$traumatic olfactory dysfunction. AJNR Am J Neu-roradiol. 1996;17:1171-1179.70. Leopold DA, Bartoshuk L, Doty RL, et al. Agingof theupper airway and the senses of taste and smell.Otolaryngol Head Neck Surg. 1989;100:287-289.71. Morrison EE, Costanzo RM. Morphology of ol-factory epithelium in humans and other vertebrates.Microsc Res Tech. 1992;23:49-61.72. Schiffman SS, Warwick ZS. Effect of flavor en-hancement of foods for the elderly on nutritional sta-tus. Physiol Behav. 1993;53:395-402.73. Schiffman SS. Food acceptability and nutritionalstatus. In: Leathwood P, HorisbergerM,James WPT,ed. For a Better Nutrition in the 21st Century. NewYork, NY: Raven Press; 1992:149-162.74. Shaffer SE, Tepper BJ. Effects of learned flavorcues on single meal and daily food intake in humans.Physiol Behav. 1994;55:979-986.75. Espat NJ, Copeland EM, Moldawer LL. Tumornecrosis factor and cachexia: a current perspective.Surg Oncol. 1994;3:255-262.76. Egbert AM. 'The dwindles'. Postgrad Med. 1993;94:199-201,204-206,210-212.77. Snow JB Jr, Doty RL, Bartoshuk LM. Clinicalevaluation of olfactory and gustatory disorders. In:Getchell TV, Doty RL, Bartoshuk LM, Snow JB Jr,eds. Smell and Taste in Health and Disease. NewYork, NY: Raven Press; 1991:463-467.78. Schiffman SS, Covey E. Changes in taste andsmell with age: nutritional aspects. In: Ordy JM, Har-man D, Alfin-Slater R, eds. Nutrition in Gerontology.New York, NY: Raven Press; 1984:43-64.79. Hetherington MM. Sensory-specific satiety andits importance in meal termination. Neurosci Biobe-hav Rev. 1996;20:113-117.80. Bellisle F, Monneuse MO, Chabert M, et al. Mono-sodium glutamate as a palatability enhancer in theEuropean diet. Physiol Behav. 1991;49:869-873.81. Bartoshuk LM, Duffy VB, Reed D, Williams A.Supertasting, earaches and head injury. NeurosciBiobehav Rev. 1996;20:79-87.82. Moskowitz HW, Kumaraiah V, Sharma KN, et al.Cross-cultural differences in simple taste preferences.Science. 1975;190:1217-1218.83. Rolls BJ. Appetite, hunger, and satiety in the el-derly. Crit Rev Food SciNutr. 1993;33:39-44.84. Pelchat M, LaChaussee JL. Food cravings andtaste aversions in the elderly. Appetite. 1994;23:193.85. Drewnowski A, Henderson SA, Driscoll A, RollsBJ. Salt taste perceptions and preferences are unre-lated to sodium consumption in healthy older adults.J Am Diet Assoc. 1996;96:471-474.86. Nordin S, Monsch AU, Murphy C. Unaware-ness of smell loss in normal aging and Alzheimer'sdisease. J Gerontol B Psychol Sci Soc Sci. 1995;50:187-192.
Downloaded From: http://jama.jamanetwork.com/ by a Northern Ontario School of Medicine User on 10/30/2013