Embed Size (px)
Citation preview
Med J Malaysia Vol 60 No 1 March 2005 71
Introduction
Injury of the tarsometatarsal joint is not common. It isa spectrum encompassing soft tissue and bony injuries.In a bony injury, the diagnosis made after history andphysical examination is readily confirmed by x-rays.However, when only soft tissue is involved, the subtleradiographic signs might not be appreciated by theuntrained eye and can lead to delay in the diagnosisand treatment of the ligamentous injury. Studies haveshown that the outcome is better with stable anatomicalreduction 1-8. The treatment trend is towards openreduction and screw fixation 1,2,4-6. The authors advocatetreating all bony and displaced ligamentoustarsometatarsal joint injuries with open anatomicalreduction utilising 4.5 mm cancellous screws and 1.6mm K-wires. Kuo et al 9 had noted the comparativepoorer outcome in the solely ligamentous injuries aftersurgery. We reviewed eighteen consecutive cases oftarsometatarsal injuries that had undergone surgery andevaluated the outcome in terms of function (AOFASmidfoot score) and anatomical reduction (radiographs).
Materials and Methods
A retrospective study of all the patients withtarsometatarsal injuries that underwent surgery atChangi General Hospital between Jan 1997 to Dec 2001was carried out. The inclusion criterion was openreduction and internal fixation of the tarsometatarsaljoint. The indications for surgery were fractures anddisplacement. The ligamentous injuries were includedwhen they showed instability on stress x-rays (morethan 1 mm displacement of bony alignment) 28 patientswere identified from the trauma registry database andcontacted by telephone. The history was evaluated withattention to trauma mechanism, concurrent injuries,open or closed fractures, and interval between injuryand surgery. The initial x-ray findings were alsodocumented. The functional outcome was assessedwith the AOFAS (American Orthopedic Foot and AnkleSociety) midfoot score by only one author (J L Soon) toprevent interobserver variability. The AOFAS score isbased on a scale of 0 to 100 points, with 100 pointsindicating an excellent or maximum outcome. The
Tarsometatarsal Joint Injuries – Review of ClinicalPresentation and Surgical Treatment
ORIGINAL ARTICLE
This article was accepted: 3 June 2004Corresponding Author: James Sir-Young Loh, Department of Orthopedic Surgery, Alexandra Hospital, 378, Alexandra Road,Singapore 159964
S Y Loh, FRCS (Orth)*, J L Soon, MBBS**, W J Verhoeven, FRCS***
*Department of Orthopedic Surgery, Alexandra Hospital, 378, Alexandra Road, Singapore 159964, **Singapore Health Services,***Department of Orthopedic Surgery, Changi General Hospital
Summary
The tarsometatarsal (Lisfranc) joint suffers a spectrum of injuries ranging from solely ligamentous injury to fracturedislocation. The authors evaluated eighteen consecutive patients who underwent surgery for tarsometatarsal jointinjuries, utilising 4.5 mm cancellous screws and 1.6 mm K-wires. The outcome of function and anatomicalreduction were assessed by AOFAS (American Orthopedic Foot and Ankle Society) midfoot score and radiography.Patients with only ligamentous injury scored poorer partly due to delay in diagnosis and the nature of the injury.The technique used maintained anatomical reduction at the time of review.
Key Words: Lisfranc fracture, Surgery, Anatomical reduction
11/TARSOMETATARSAL 21/03/2005 8:50am Page 71

ORIGINAL ARTICLE
72 Med J Malaysia Vol 60 No 1 March 2005
clinical and radiographic results and functionaloutcomes were analysed to evaluate the effect of injuryand treatment parameters. The main components of thescoring scale consisted of pain, function (furthersubdivided into activity limitation, footwearrequirement, maximum walking distance, walkingsurfaces and gait abnormality) and alignment of thefoot.
Surgical TechniqueThe senior author (W J Verhoeven) performed thesurgeries. The surgical approach was via 2 incisions.The medial incision between the proximal first andsecond metatarsals enabled access to the medialcolumn. The first metatarsal-medial cuneiform jointwas first reduced, followed by the second metatarsal-middle cuneiform joint and the third metatarsal-lateralcuneiform joints. 4.5mm cannulated screws were used.The dorsalis pedis and nerves were identified andpreserved. The lateral column was approached via thelateral incision over the proximal forth metatarsal. 1.6mm K-wires were used to reduce the forth and fifthmetatarsal-cuboid joint. Attention was given to ensurean adequate skin bridge between the 2 incisions.
Concurrent fractures were treated at the same surgery.The image intensifier was used intra-operatively toassess the fracture reduction and aid in implantplacement. Intra-operative radiographs were done forall the surgeries before reversal. Post-operatively, thepatient was splinted below the knee for a minimal of 6weeks and non weight bearing was instructed. Anyincrease in duration of the non weight bearing statusdepended on x-ray and clinical assessment of healing.The implants are removed at the end of 3 to 4 monthsafter surgery.
Results
Twenty-eight patients were found suitable for the study.However, ten were not available: four refusedparticipation and six were foreign workers who hadreturned to their country. The remaining eighteenpatients with eighteen tarsometatarsal injuriesparticipated in the study. The age ranged from twenty-one to sixty-seven years old, with a mean of 32.2 years.There were fifteen male and three female patients. Allpatients were Asian. There were eleven left feet andseven right feet. Ten patients had sustained high energytrauma (four fall from height and six crush). Theremaining eight patients sustained low energy trauma
(twist and blunt trauma). Nine were polytrauma andnine were isolated injuries.
There were nine cases with associated injuries. Of these,one was a ligamentous injury with an associated fibulafracture (the fibula fracture was treated conservatively).The other eight were obvious tarsometatarsal fractureswith associated injuries. There was a single case of openfracture involving the tarsometatarsal joint. Eleven wereobvious fractures at the time of first presentation to themedical practitioner (Fig 1). The diagnosis was evidenton radiological assessment. The other seven wereligamentous injuries and the radiographs only showedsubtle bony mal-alignment. They had been referred tothe orthopedic clinic by the emergency or familyphysician for a symptomatic foot with normalradiographic finding. The shortest interval betweeninjury and surgery was within one day involving atarsometatarsal fracture dislocation. The mean intervalbetween injury and surgery for bony tarsometatarsaljoint injury was 5.5 days while that of ligamentous injurywas 30 days (excluding the case of a military personnelwith a seven month delay).
A number of reasons contributed to the delay in surgery.In polytrauma, basic resuscitation and stabilization weregiven priority. Skin injury also necessitated a delay insurgery to avoid incision wound complications. Openinjury also required initial debridement before definitivesurgery. All the ligamentous injuries were referred tothe orthopedic clinic before they were admitted forsurgery. The average follow-up period was thirtymonths, the shortest was twelve months and the longestwas thirty-nine months.
There were no post-operative complications noted inthe follow-up review. No broken implants were noted.The single case of open fracture required split thicknessskin grafting. The average AOFAS score was 81.4 points(ranging from 54 points to 100 points). Patients lostpoints for mild pain, mal-alignment and reducedfunction. The average was lower for the ligamentousinjury subgroup (76.3 points) compared to the bonyinjury subgroup (84.6 points). The highest score forboth groups were 100 points. The lowest score for theligamentous injury subgroup was 54 points while thatfor the bony injury subgroup was 58 points. Sevenwere asymptomatic (one ligamentous injury and sixbony injury). The remaining eleven (six ligamentousinjury and three bony injury) had symptoms of varyingseverity (eight sustaining mild pain and stiffness;remaining three affected in walking, sports and work).
11/TARSOMETATARSAL 21/03/2005 8:50am Page 72

Tarsometatarsal Joint Injuries
Med J Malaysia Vol 60 No 1 March 2005 73
Fig 1: Bony tarsometatarsal joint injury attime of presentation
Fig 2: Ligamentous tarsometatarsal jointinjury presented as a symptomatic footwith no obvious x-ray findings in nonweight bearing films
Fig 3: Subtle diastasis widening can bedetected in the antero-posterior weightbearing comparison film
Fig 4: Reduction with screws in the medialcolumn and K-wires in the lateralcolumn
11/TARSOMETATARSAL 21/03/2005 8:50am Page 73
Discussion
The tarsometatarsal joint injury accounts for only 0.2percent of all fractures. In the ligamentous injury withits associated subtle radiographic signs (Fig 2), thediagnosis is easily missed 10. A weight bearinganteroposterior film of bilateral feet is helpful in theassessment (Fig 3). However, this is not alwayspossible in an acute injury. A high index of suspicionis needed and it is advisable to seek the opinion of theorthopedic surgeon. The nature of this injury mighthave resulted in the greater interval between injury andsurgery. One series showed poor functional results inpatients with delayed diagnosis 1,11. Other studiessuggested a delay of up to six weeks could stillproduce a favorable outcome 12-14. Thus early diagnosisis crucial to facilitate early treatment and obtain afavorable outcome.
Though the ligamentous injuries were the result ofseemingly minor trauma, the average AOFAS midfootscore after surgery was less than that of bony injury(Table I). The statistical significance of this observation
cannot be determined in the current study because ofits small number. Kuo et al 9 had noted a similaroutcome. When it is a bony injury, the healing is betterthan ligamentous injury. The delay in diagnosisresulted in a greater interval between injury andsurgery, could have resulted in further damage to thearticular surfaces, due to prolonged malpositioning andinstability. Dissection and reduction was made moredifficult by fibrosis that set in. There was one workmancompensation case and 3 military recruits who hadsustained ligamentous injury, However, there was noobvious reason to suspect secondary gain.
No classification system was used in this study. Thereis no single classification that comprehensively coversthe broad spectrum of this condition, enablesprognostication and directs treatment. We advocateopen reduction and internal fixation with the aim ofachieving stable anatomical reduction. Surgery enablesdirect visualization and assessment for osteochondralinjury, comminution, loose fragments and soft tissueinterposition 2. This facilitates reduction of the fractureand prognostication. The importance of stable
ORIGINAL ARTICLE
74 Med J Malaysia Vol 60 No 1 March 2005
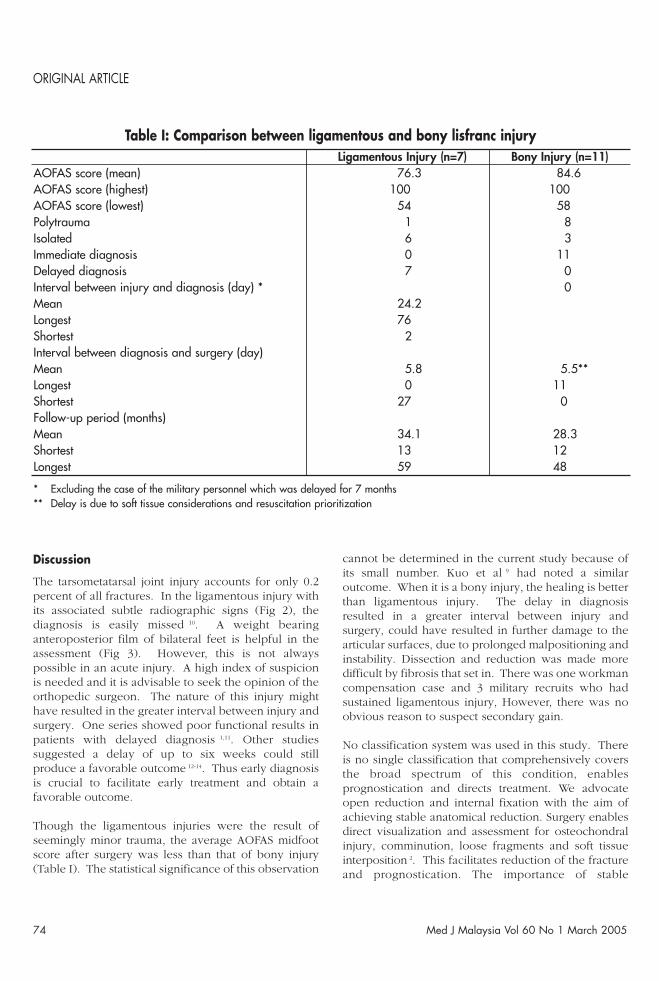
Ligamentous Injury (n=7) Bony Injury (n=11)AOFAS score (mean) 76.3 84.6AOFAS score (highest) 100 100AOFAS score (lowest) 54 58Polytrauma 1 8Isolated 6 3Immediate diagnosis 0 11Delayed diagnosis 7 0Interval between injury and diagnosis (day) * 0Mean 24.2Longest 76Shortest 2Interval between diagnosis and surgery (day)Mean 5.8 5.5**Longest 0 11Shortest 27 0Follow-up period (months)Mean 34.1 28.3Shortest 13 12Longest 59 48
* Excluding the case of the military personnel which was delayed for 7 months** Delay is due to soft tissue considerations and resuscitation prioritization
Table I: Comparison between ligamentous and bony lisfranc injury
11/TARSOMETATARSAL 21/03/2005 8:50am Page 74
Tarsometatarsal Joint Injuries
Med J Malaysia Vol 60 No 1 March 2005 75
1. Curtis MJ, Myerson MS, Szura B: Tarsometatarsal jointinjuries in the athlete. Am J Sports Med 1993; 21: 497-502.
2. Arntz CT, Veith RG, Hansen ST: Fractures and fracturedislocation of the tarsometatarsal joint. J Bone and JointSurg 1988; 70-A: 173-81.
3. Myerson MS, Fisher RT, Burgess AR, Kenzora JE: Fracturedislocations of the tarsometatarsal joints: end resultscorrelated with pathology and treatment. Foot and Ankle1986; 6: 225-42.
4. Myerson M: The diagnosis and treatment of injuries to theLisfranc joint complex. Orthop Clin North Am 1989; 20:655-64.
5. Rosenberg GA, Patterson BM: Tarsometatarsal (Lisfranc’s)fracture dislocation. Am J Orthop 1995; supplement: 7-16.
6. Buzzard BM and Briggs P J: Surgical management ofacute tarsometatarsal fracture dislocation in the adult. ClinOrthop 1998; 353: 125-33.
7. Myerson M: Injuries to the forefoot and toes. In Disordersof the Foot and Ankle: Medical and Surgical Management,M H Jahss (ed). Ed 2, vol 3, p2233-2272. Philadelphia, WB Saunders, 1991.
8. Teng AL, Pinzur MS, Lomasney L, Mahoney L, Havey R:Functional outcome following anatomic restoration of
tarsal-metatarsal fracture dislocation. Foot Ankle Int 2002;23(10): 922-6.
9. Kuo RS, Tejwani NC, DiGiovanni CW et al: Outcome afteropen reduction and internal fixation of Lisfranc jointinjuries. J Bone and Joint Surgery 2000; 82-A (11): 1609-618.
10. Perron AD, Brady WJ, Keats TE: Orthopedic pitfalls in theED: Lisfranc fracture-dislocation. Am J Emerg Med 2001;19(1): 71-5.
11. Richter M, Wipperman B, Krettek C, Schratt H E, HufnerT, Therman H: Fractures and fracture dislocations of themidfoot: occurrence, causes and long-term results. FootAnkle Int 2001; 22(5): 392-8.
12. Arntz CT, Hansen ST: Dislocations and fracturedislocations of the tarsometatarsal joints. Clin Orthop1987; 18: 105-14.
13. Trevino SG, Baumhauer JF: Lisfranc injuries. In MyersonM S (ed): Current therapy in foot and ankle surgery. StLouis, Mosby year book, 1993.
14. Trevino S G, Kodros S: Controversies in tarsometatarsalinjuries. Orthop Clin of North Am 1995; 26; 229-38.
15. Mulier T, Reynders P, Dereymaeker G, Broos P: SevereLisfranc injuries: Primary arthrodesis or open reductionand internal fixation? Foot Ankle Int 2002; 23(10): 902-5.
References
anatomical reduction is supported by a number ofstudies1-8. The combination of 4.5 cannulated screwsand 1.6 mm K-wires were used (Fig 4). The medialcolumn is inherently more rigid than the lateral column.Therefore, screws were used to secure the stabilityrequired for anatomical reduction and healing. 4.5 mmcannulated screws were chosen over 3.5 mm as theywere stronger. Compared to 1.6 mm K-wires, thearticular surface damage is greater but the benefit ofgreater stability outweighs this consideration. K-wiresafforded sufficient stability to the lateral column that isinherently a relatively mobile column. Removal ofimplants was approximately 3 to 4 months aftersurgery. This reduced implant complications such asbreakage and K-wire migration. Primary arthrodesiswas reserved as a salvage procedure for complicationssuch as persistent pain or non-union. Mulier et al 15 hadsuggested that primary complete arthrodesis should bereserved as a salvage procedure. Limitations of thecurrent study included the 64.3 percent follow-up rate
and the mean duration of 30 months. The studypopulation was small. A prospective study would bebetter suited to analyze the fixation technique.
Conclusion
A longer interval between injury and surgery was notedin the ligamentous subgroup. This observationhighlighted the subtlety in presentation and diagnosticdifficulty of this subgroup. The delay might havecontributed to the lower AOFAS score, despite similartreatment and the minor trauma involved. Anatomicalreduction was maintained in all cases at the time ofreview.
Acknowledgements
The authors thank Mercy Christian and Dr Leong WaiMay for the administrative and technical support.
11/TARSOMETATARSAL 21/03/2005 8:50am Page 75





























