Embed Size (px)
Citation preview
T A R G E T I N G S E R I O U S D I S E A S E S O F I M M U N O - I N F L A M M A T I O N A N D F I B R O S I S
June 2016
NASDAQ: TBRA
Corporate Presentation
Forward Looking Statements
This presentation and other matters discussed today or answers that may be given in response to questions may include statements that are, or may be deemed, “forward-looking statements.” Any statements that we make today, other than historical facts, are forward looking statements made pursuant to the safe harbor provisions of the Private Securities Litigation Reform Act of 1995. All statements, other than statements of historical facts, included in this presentation regarding our future results of operations and financial position, strategy and plans, and our expectations for future operations are forward-looking statements. In some cases, you can identify forward-looking statements by terms such as “believe,” “may,” “will,” “estimate,” “continue,” “anticipate,” “design,” “intend,” “expect,” “could,” “plan,” “potential,” “predict,” “seek,” “should,” “would” or the negative version of these words and similar expressions intended to identify forward-looking statements, and similar expression and comparable terminology intended to identify forward-looking statements.
Forward-looking statements reflect management's current expectations, are based on certain assumptions and involve certain risks and uncertainties. Forward-looking statements include, but are not limited to, statements about: financial projections and estimates and their underlying assumptions, including, without limitation, sufficiency of our cash resources and needs for and ability to obtain additional financing; anticipated timing of patient enrollment in our clinical studies and availability of clinical data; anticipated timing of completing our clinical studies; the size and growth of our potential patient population; the mechanism of action of our product candidates; the ability to obtain and maintain regulatory approval of our product candidates; and the timing and success of the development and commercialization of our anticipated product candidates and the availability of alternative therapies for our target market. The Company's actual results could differ materially from those anticipated in these forward-looking statements as a result of various factors. Additional information regarding factors that could cause results to differ are available in the Company's other periodic filings with the SEC.
2
Changing the Course of NASH & Liver Disease
3
Building a leading NASH program• Cenicriviroc (CVC) Phase 2b CENTAUR data Q3 2016• Evogliptin (EVO) + CVC combination study planned for 2016
Building long-term value• Transition to Phase 3 for CVC single-agent, combinations to follow• Q1 2016 cash balance: $53 million; cash runway to H2 2017
CVC: potent immuno-inflammatory agent• Once-daily dosing & favorable safety profile; cornerstone potential for NASH• Phase 2 in Primary Sclerosing Cholangitis: potential to be disease modifying
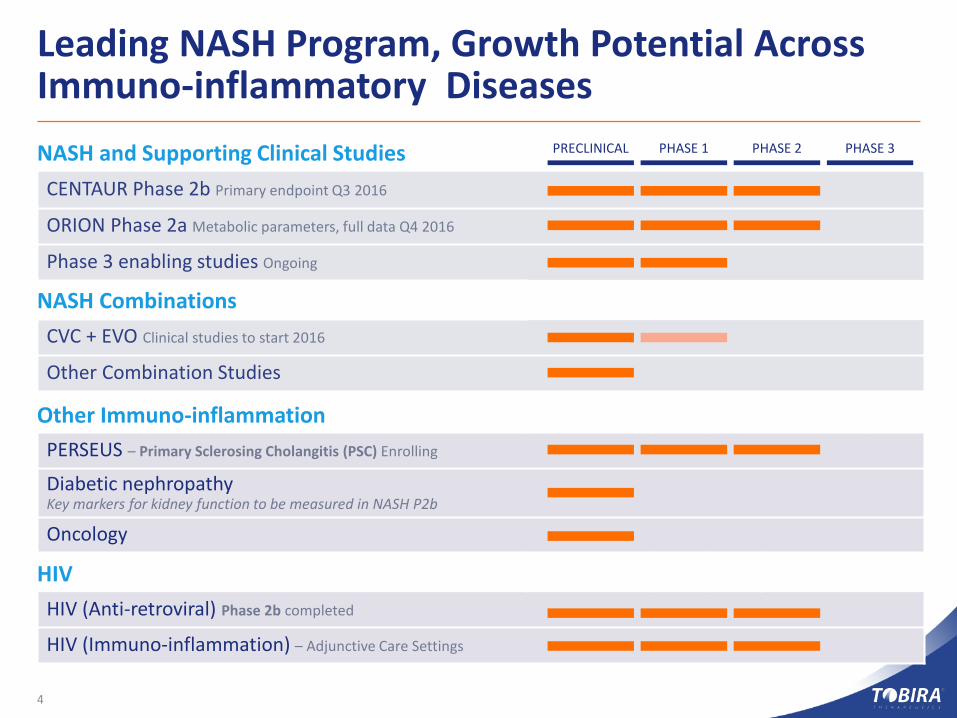
Leading NASH Program, Growth Potential Across Immuno-inflammatory Diseases
4
NASH and Supporting Clinical StudiesCENTAUR Phase 2b Primary endpoint Q3 2016
ORION Phase 2a Metabolic parameters, full data Q4 2016
Phase 3 enabling studies Ongoing
NASH CombinationsCVC + EVO Clinical studies to start 2016
Other Combination Studies
Other Immuno-inflammationPERSEUS – Primary Sclerosing Cholangitis (PSC) Enrolling
Diabetic nephropathy Key markers for kidney function to be measured in NASH P2b
Oncology
HIVHIV (Anti-retroviral) Phase 2b completed
HIV (Immuno-inflammation) – Adjunctive Care Settings
PRECLINICAL PHASE 1 PHASE 2 PHASE 3

5
NASH Unmet Need
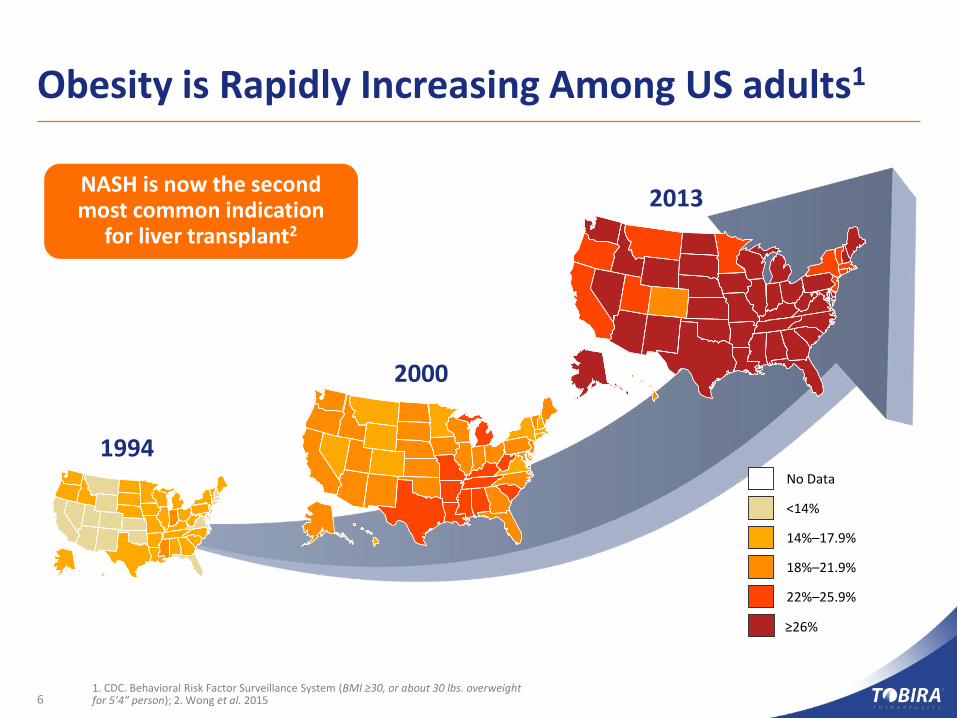
Obesity is Rapidly Increasing Among US adults1
61. CDC. Behavioral Risk Factor Surveillance System (BMI ≥30, or about 30 lbs. overweight for 5’4” person); 2. Wong et al. 2015
No Data
<14%
14%–17.9%
18%–21.9%
22%–25.9%
≥26%
2013
1994
2000
NASH is now the second most common indication
for liver transplant2
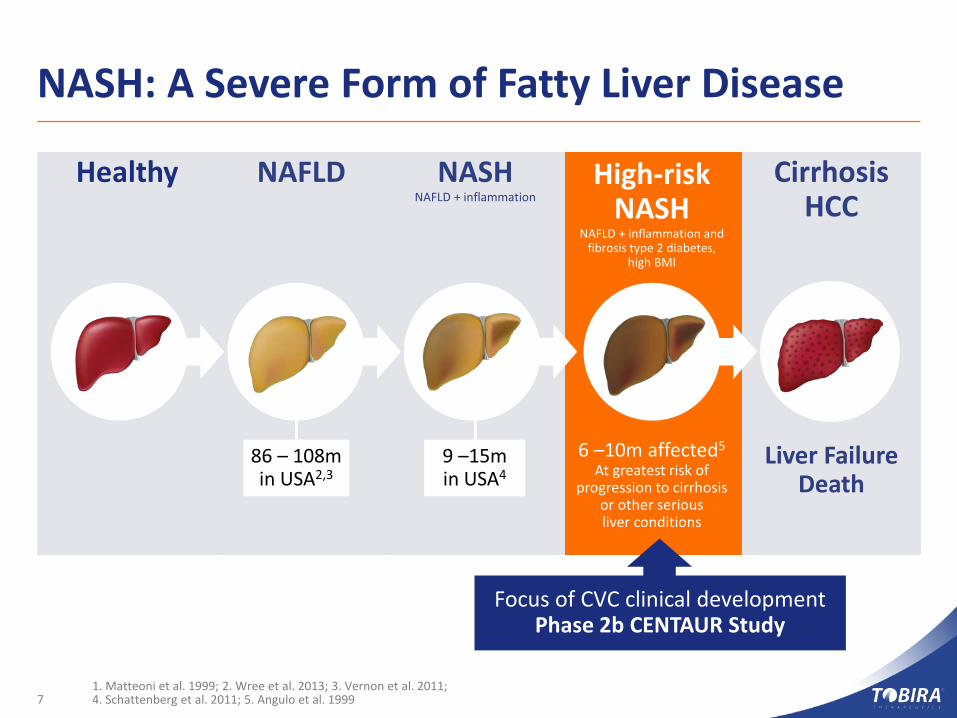
NASH: A Severe Form of Fatty Liver Disease
CirrhosisHCC
Liver FailureDeath
High-riskNASH
NAFLD + inflammation and fibrosis type 2 diabetes,
high BMI
6 –10m affected5
At greatest risk of progression to cirrhosis
or other serious liver conditions
NAFLDHealthy NASHNAFLD + inflammation
1. Matteoni et al. 1999; 2. Wree et al. 2013; 3. Vernon et al. 2011; 4. Schattenberg et al. 2011; 5. Angulo et al. 1999
86 – 108min USA2,3
9 –15min USA4
Focus of CVC clinical developmentPhase 2b CENTAUR Study
7

8
CVC for NASH
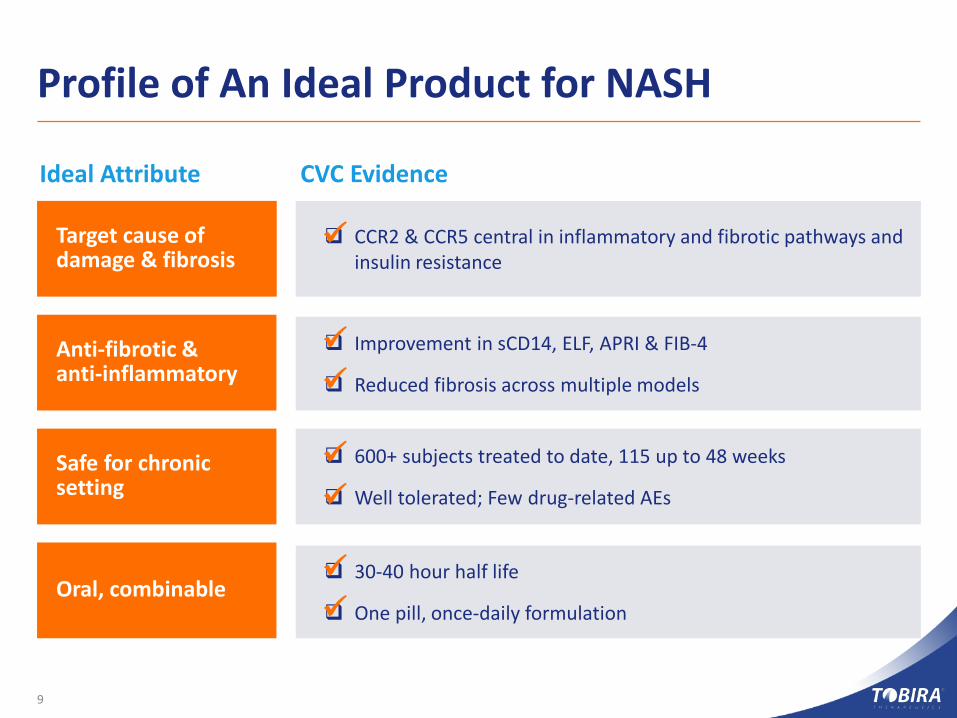
Profile of An Ideal Product for NASH
9
Target cause of damage & fibrosis
Anti-fibrotic & anti-inflammatory
Safe for chronic setting
Oral, combinable
CCR2 & CCR5 central in inflammatory and fibrotic pathways and insulin resistance
Improvement in sCD14, ELF, APRI & FIB-4
Reduced fibrosis across multiple models
600+ subjects treated to date, 115 up to 48 weeks
Well tolerated; Few drug-related AEs
30-40 hour half life
One pill, once-daily formulation
Ideal Attribute CVC Evidence
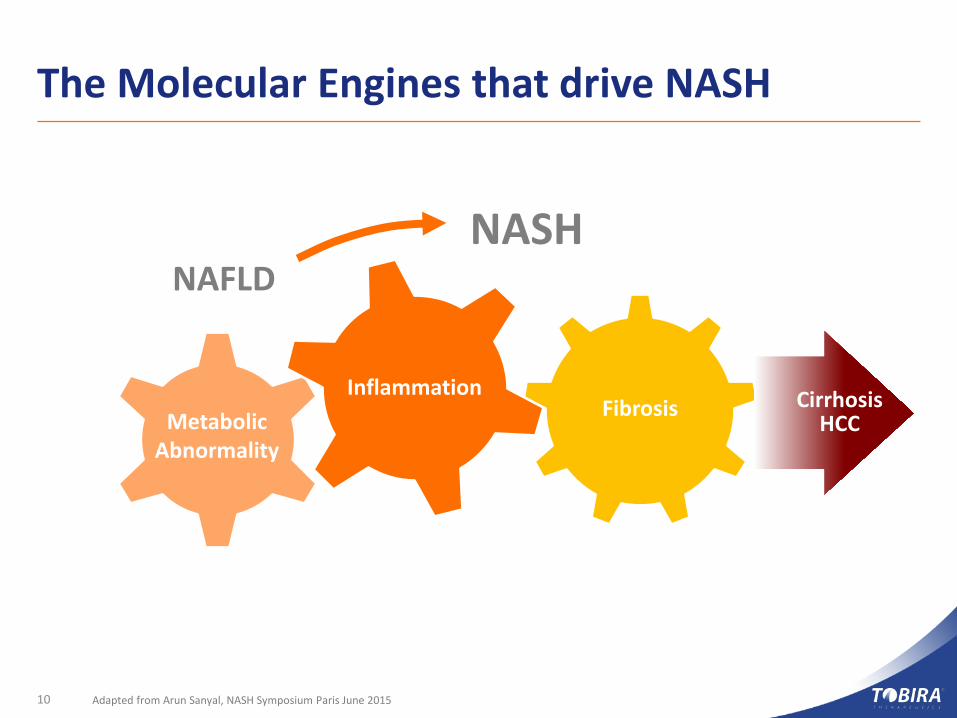
FibrosisInflammation
The Molecular Engines that drive NASH
Adapted from Arun Sanyal, NASH Symposium Paris June 2015
NAFLDNASH
Cirrhosis HCCMetabolic
Abnormality
10
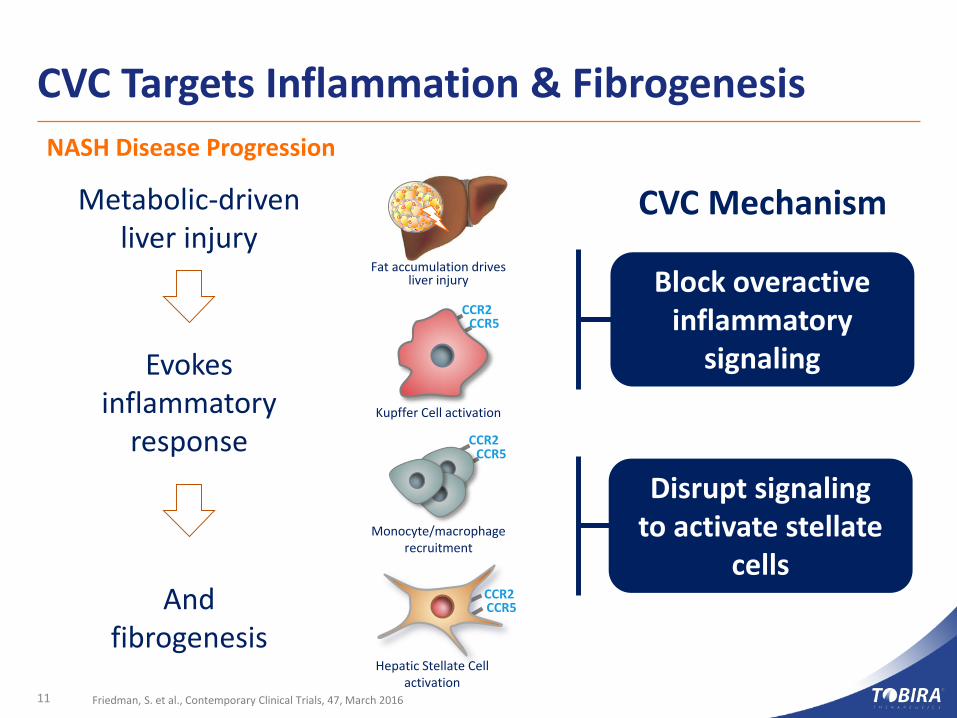
CVC Targets Inflammation & Fibrogenesis
11 Friedman, S. et al., Contemporary Clinical Trials, 47, March 2016
Metabolic-driven liver injury
Evokes inflammatory
response
And fibrogenesis
CVC Mechanism
Block overactive inflammatory
signaling
Disrupt signaling to activate stellate
cells
Hepatic Stellate Cell activation
CCR2CCR5
CCR2CCR5
Kupffer Cell activation
Fat accumulation drives liver injury
CCR2CCR5
Monocyte/macrophage recruitment
NASH Disease Progression
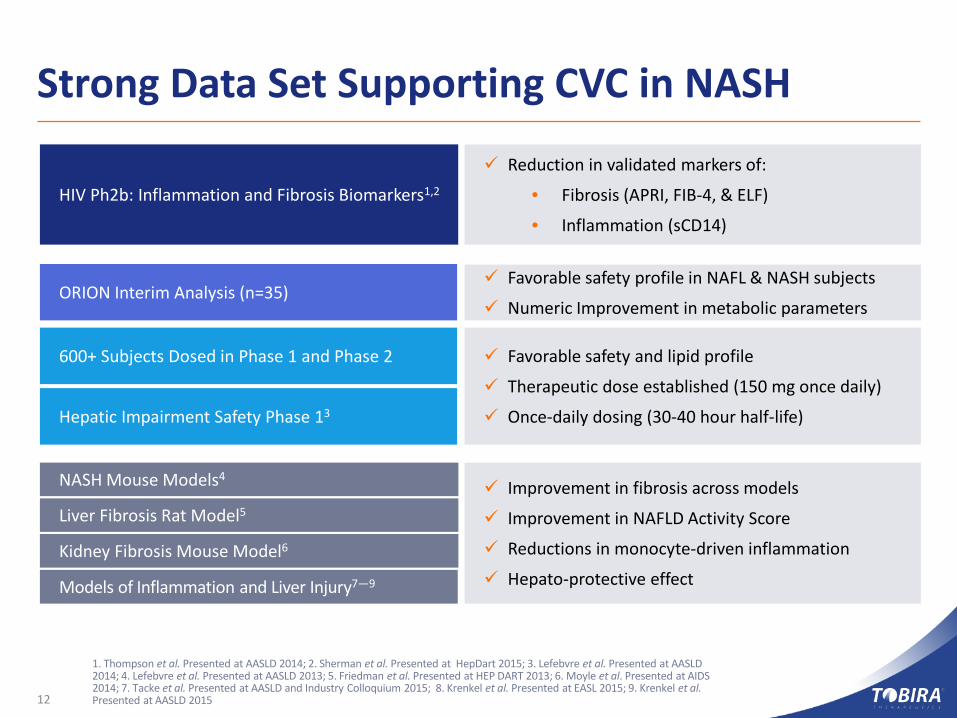
Strong Data Set Supporting CVC in NASH
12
1. Thompson et al. Presented at AASLD 2014; 2. Sherman et al. Presented at HepDart 2015; 3. Lefebvre et al. Presented at AASLD 2014; 4. Lefebvre et al. Presented at AASLD 2013; 5. Friedman et al. Presented at HEP DART 2013; 6. Moyle et al. Presented at AIDS 2014; 7. Tacke et al. Presented at AASLD and Industry Colloquium 2015; 8. Krenkel et al. Presented at EASL 2015; 9. Krenkel et al. Presented at AASLD 2015
Hepatic Impairment Safety Phase 13
600+ Subjects Dosed in Phase 1 and Phase 2
HIV Ph2b: Inflammation and Fibrosis Biomarkers1,2
NASH Mouse Models4
Liver Fibrosis Rat Model5
Kidney Fibrosis Mouse Model6
Reduction in validated markers of:
• Fibrosis (APRI, FIB-4, & ELF)
• Inflammation (sCD14)
Favorable safety and lipid profile
Therapeutic dose established (150 mg once daily)
Once-daily dosing (30-40 hour half-life)
Improvement in fibrosis across models
Improvement in NAFLD Activity Score
Reductions in monocyte-driven inflammation
Hepato-protective effectModels of Inflammation and Liver Injury7—9
ORION Interim Analysis (n=35) Favorable safety profile in NAFL & NASH subjects
Numeric Improvement in metabolic parameters
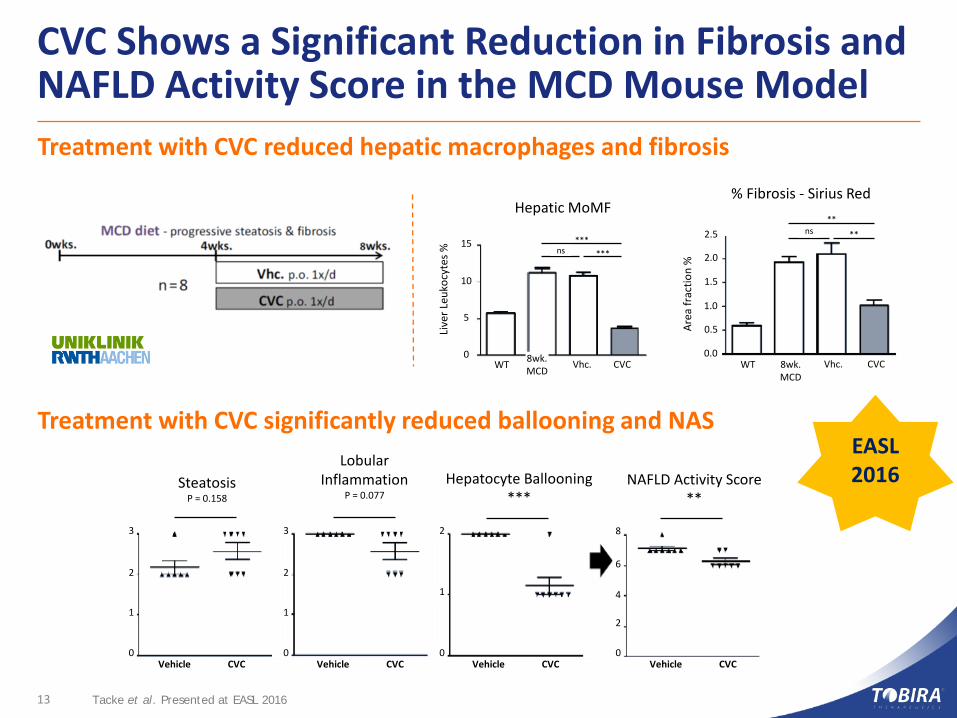
CVC Shows a Significant Reduction in Fibrosis and NAFLD Activity Score in the MCD Mouse Model
13 Tacke et al. Presented at EASL 2016
SteatosisP = 0.158
Lobular Inflammation
P = 0.077Hepatocyte Ballooning
***NAFLD Activity Score
**
0 0 0 0
1 1
1
2
2 2
3 3 2
4
6
8
Vehicle CVC Vehicle CVC Vehicle CVC Vehicle CVC
Area
frac
tion
%
0.0
0.5
1.0
1.5
2.0
2.5 ns **
**
CVCVhc.8wk.MCD
WTCVCVhc.8wk.MCDWT
0
5
10
15
Live
r Leu
kocy
tes % ns ***
***
Hepatic MoMF% Fibrosis - Sirius Red
Treatment with CVC reduced hepatic macrophages and fibrosis
Treatment with CVC significantly reduced ballooning and NASEASL 2016

CVC Clinical Data
14
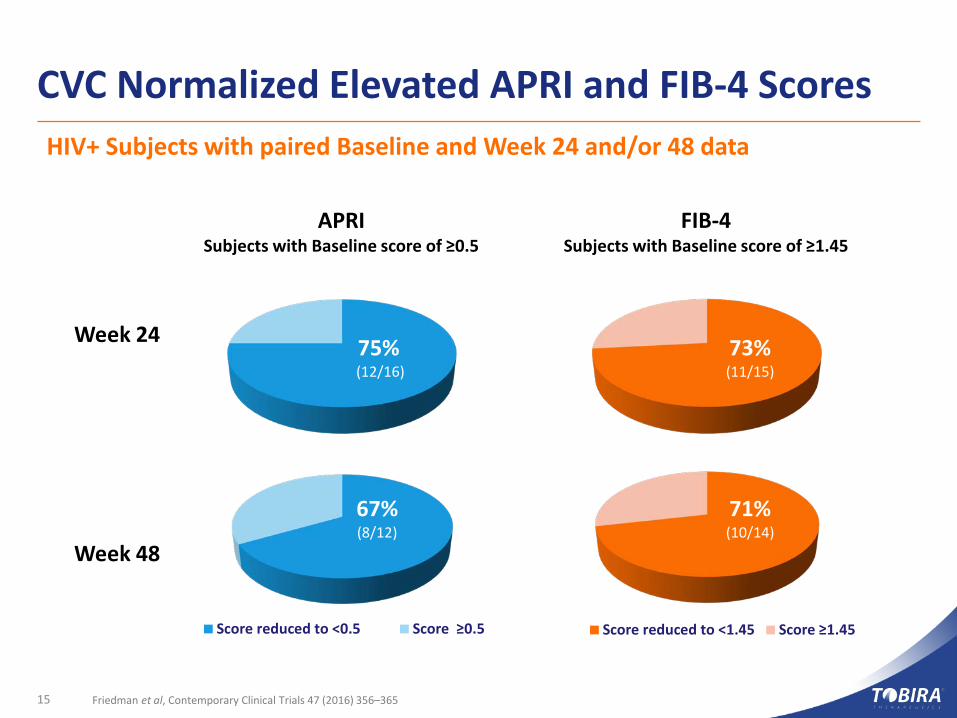
CVC Normalized Elevated APRI and FIB-4 Scores
15 Friedman et al, Contemporary Clinical Trials 47 (2016) 356–365
Score reduced to <0.5 Score ≥0.5 Score reduced to <1.45 Score ≥1.45
Week 24
Week 48
APRISubjects with Baseline score of ≥0.5
FIB-4Subjects with Baseline score of ≥1.45
75%(12/16)
67%(8/12)
73% (11/15)
71% (10/14)
HIV+ Subjects with paired Baseline and Week 24 and/or 48 data
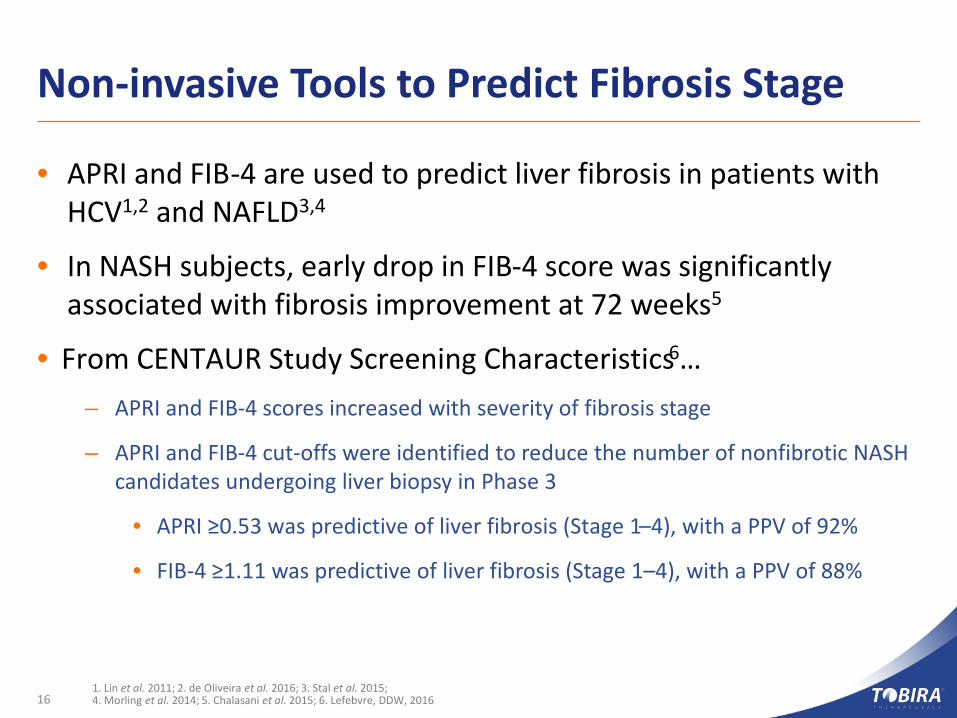
Non-invasive Tools to Predict Fibrosis Stage
• APRI and FIB-4 are used to predict liver fibrosis in patients with HCV1,2 and NAFLD3,4
• In NASH subjects, early drop in FIB-4 score was significantly associated with fibrosis improvement at 72 weeks5
• From CENTAUR Study Screening Characteristics6…– APRI and FIB-4 scores increased with severity of fibrosis stage
– APRI and FIB-4 cut-offs were identified to reduce the number of nonfibrotic NASH candidates undergoing liver biopsy in Phase 3
• APRI ≥0.53 was predictive of liver fibrosis (Stage 1–4), with a PPV of 92%
• FIB-4 ≥1.11 was predictive of liver fibrosis (Stage 1–4), with a PPV of 88%
161. Lin et al. 2011; 2. de Oliveira et al. 2016; 3. Stal et al. 2015; 4. Morling et al. 2014; 5. Chalasani et al. 2015; 6. Lefebvre, DDW, 2016
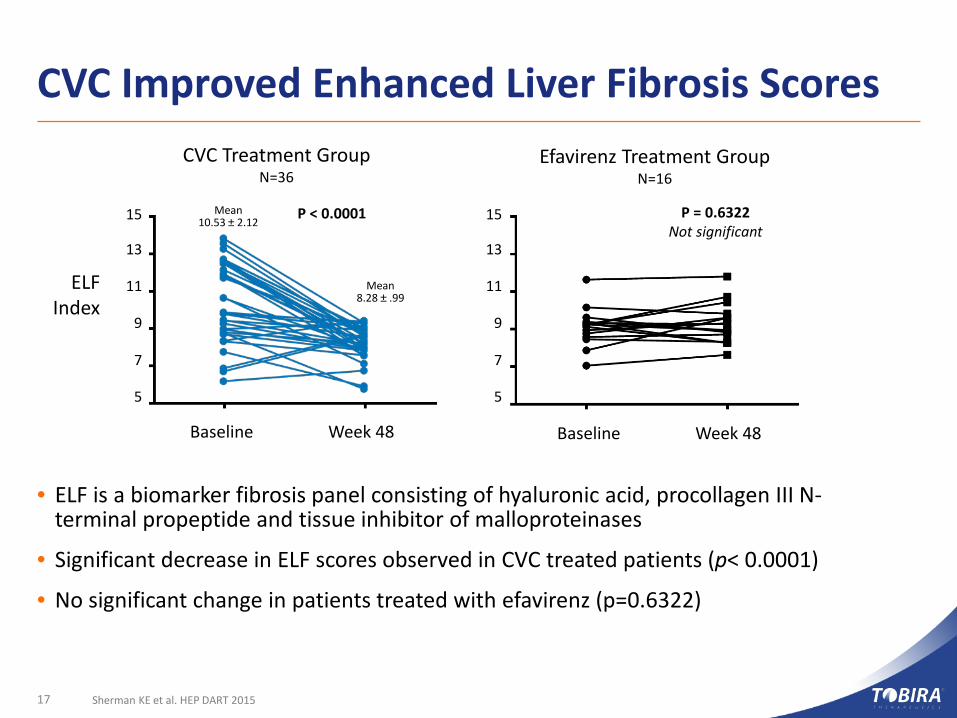
CVC Improved Enhanced Liver Fibrosis Scores
17 Sherman KE et al. HEP DART 2015
Baseline Week 48
5
7
9
11
13
15
Baseline Week 48
ELF Index
P < 0.0001 P = 0.6322Not significant
CVC Treatment GroupN=36
Efavirenz Treatment GroupN=16
5
7
9
11
13
15Mean10.53 ± 2.12
Mean 8.28 ± .99
• ELF is a biomarker fibrosis panel consisting of hyaluronic acid, procollagen III N-terminal propeptide and tissue inhibitor of malloproteinases
• Significant decrease in ELF scores observed in CVC treated patients (p< 0.0001)
• No significant change in patients treated with efavirenz (p=0.6322)
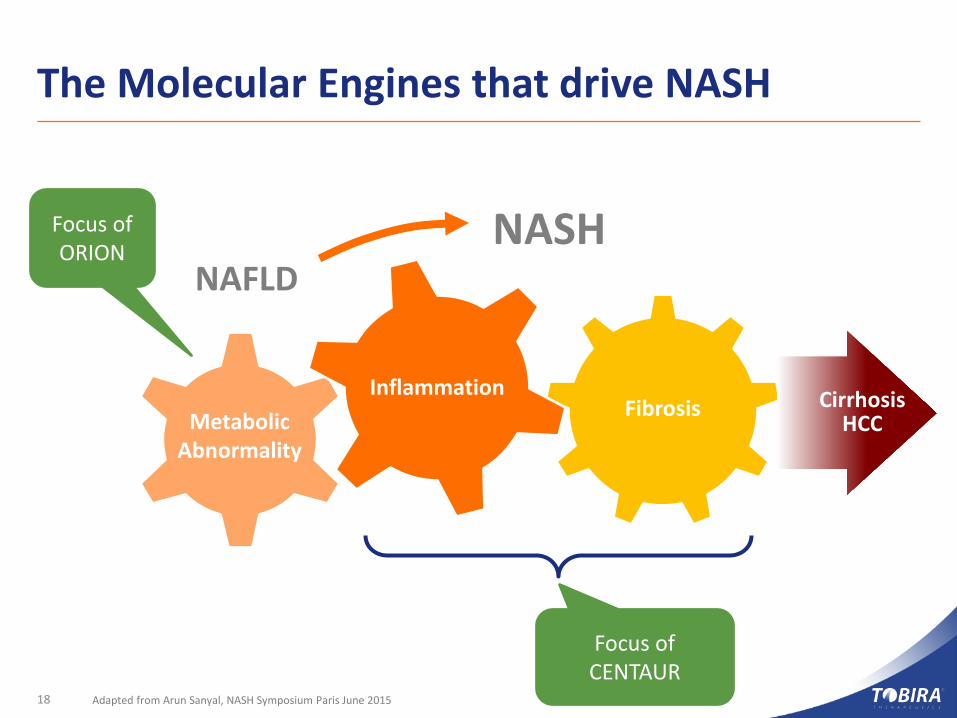
FibrosisInflammation
The Molecular Engines that drive NASH
Adapted from Arun Sanyal, NASH Symposium Paris June 2015
Focus of ORION
Focus of CENTAUR
NAFLDNASH
Cirrhosis HCCMetabolic
Abnormality
18
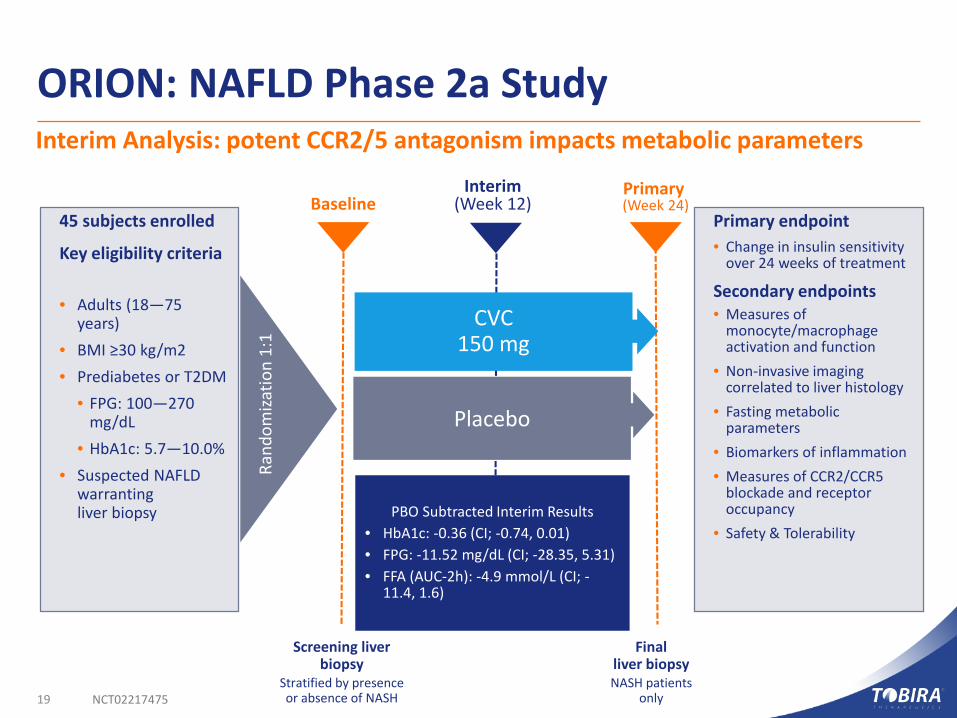
ORION: NAFLD Phase 2a StudyInterim Analysis: potent CCR2/5 antagonism impacts metabolic parameters
19 NCT02217475
Screening liver biopsy
Stratified by presence or absence of NASH
CVC150 mg
Placebo
45 subjects enrolled
Key eligibility criteria
• Adults (18—75 years)
• BMI ≥30 kg/m2• Prediabetes or T2DM
• FPG: 100—270 mg/dL
• HbA1c: 5.7—10.0%• Suspected NAFLD
warranting liver biopsy
Primary endpoint• Change in insulin sensitivity
over 24 weeks of treatment
Secondary endpoints• Measures of
monocyte/macrophage activation and function
• Non-invasive imaging correlated to liver histology
• Fasting metabolic parameters
• Biomarkers of inflammation• Measures of CCR2/CCR5
blockade and receptor occupancy
• Safety & Tolerability
Finalliver biopsyNASH patients
only
PBO Subtracted Interim Results• HbA1c: -0.36 (CI; -0.74, 0.01)• FPG: -11.52 mg/dL (CI; -28.35, 5.31)• FFA (AUC-2h): -4.9 mmol/L (CI; -
11.4, 1.6)
Primary (Week 24)Baseline
Interim(Week 12)
Rand
omiza
tion
1:1

20
CENTAUR Phase 2b Study
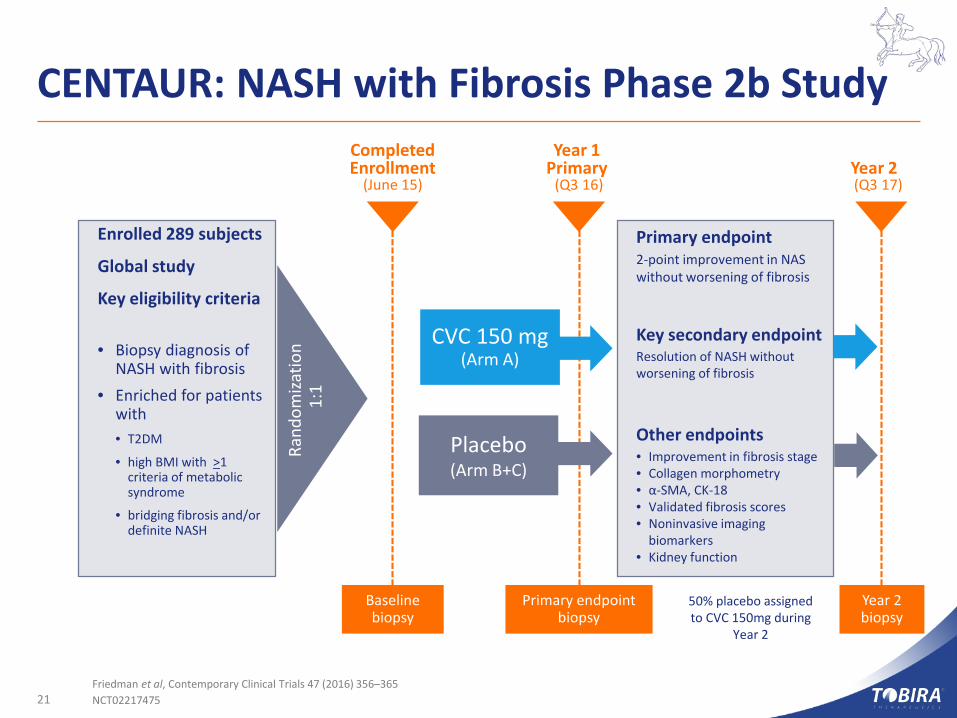
CENTAUR: NASH with Fibrosis Phase 2b Study
21Friedman et al, Contemporary Clinical Trials 47 (2016) 356–365NCT02217475
Primary endpoint biopsy
Baselinebiopsy
Year 2 (Q3 17)
Year 1 Primary
(Q3 16)
CompletedEnrollment
(June 15)
Year 2biopsy
Enrolled 289 subjects
Global study
Key eligibility criteria
• Biopsy diagnosis of NASH with fibrosis
• Enriched for patients with• T2DM
• high BMI with >1 criteria of metabolic syndrome
• bridging fibrosis and/or definite NASH
50% placebo assigned to CVC 150mg during
Year 2
Primary endpoint2-point improvement in NAS without worsening of fibrosis
Key secondary endpointResolution of NASH without worsening of fibrosis
Other endpoints• Improvement in fibrosis stage • Collagen morphometry• α-SMA, CK-18• Validated fibrosis scores• Noninvasive imaging
biomarkers• Kidney function
CVC 150 mg(Arm A)
Placebo(Arm B+C)
Rand
omiza
tion
1:1
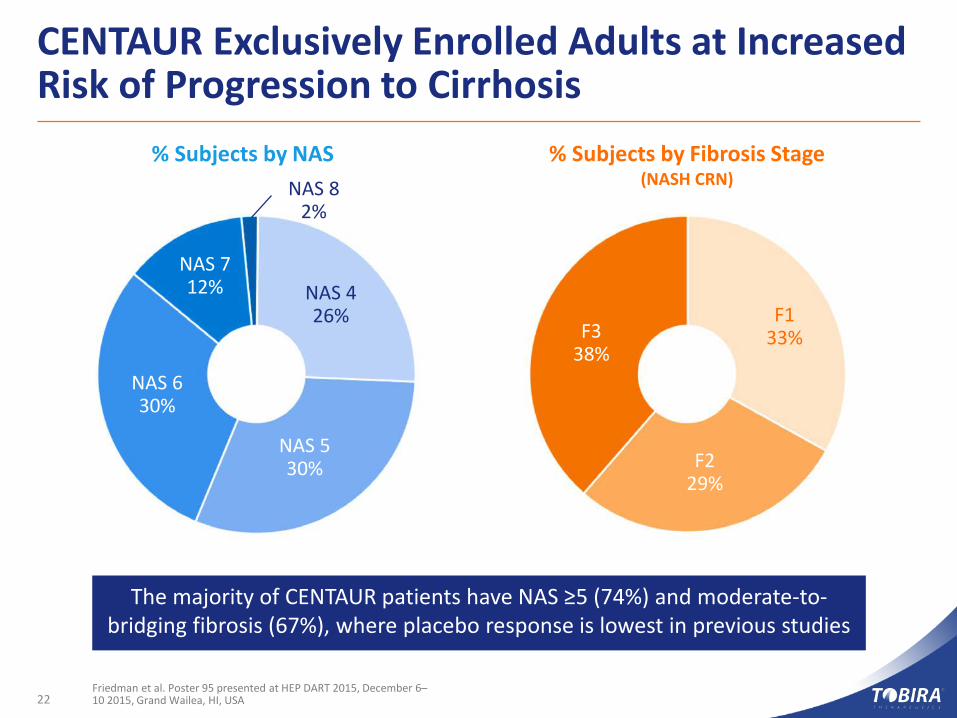
CENTAUR Exclusively Enrolled Adults at Increased Risk of Progression to Cirrhosis
Friedman et al. Poster 95 presented at HEP DART 2015, December 6–10 2015, Grand Wailea, HI, USA
The majority of CENTAUR patients have NAS ≥5 (74%) and moderate-to-bridging fibrosis (67%), where placebo response is lowest in previous studies
NAS 630%
% Subjects by NAS % Subjects by Fibrosis Stage(NASH CRN)
NAS 530%
NAS 426%
NAS 712%
NAS 82%
F338%
F229%
F133%
22

23
EVO for NASH
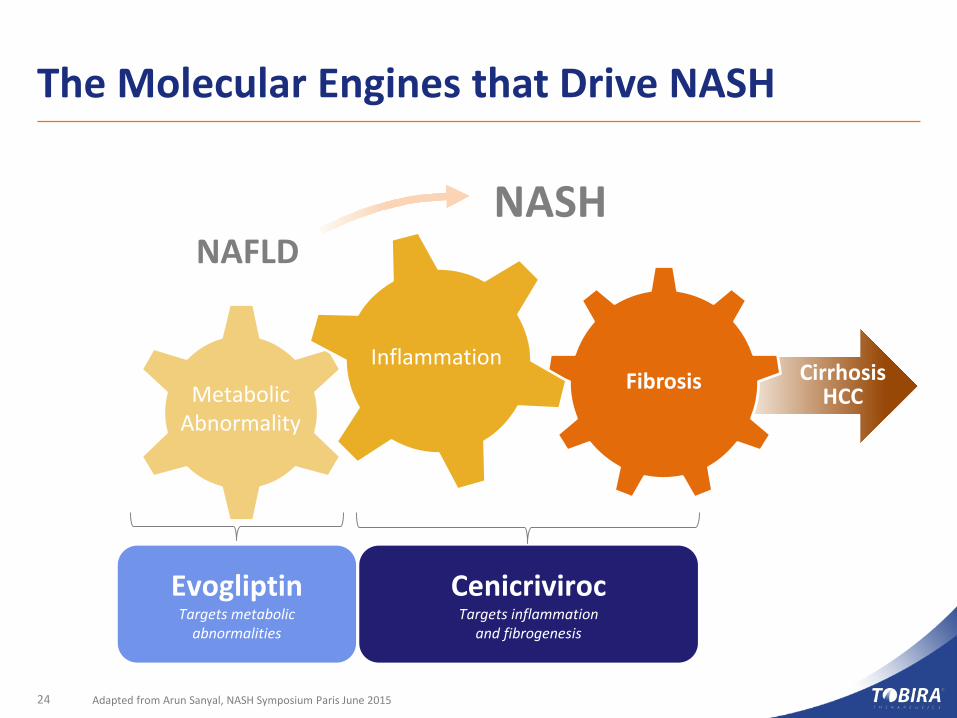
The Molecular Engines that Drive NASH
24 Adapted from Arun Sanyal, NASH Symposium Paris June 2015
Fibrosis
NAFLDNASH
Cirrhosis HCCMetabolic
Abnormality
CenicrivirocTargets inflammation
and fibrogenesis
EvogliptinTargets metabolic
abnormalities
Inflammation
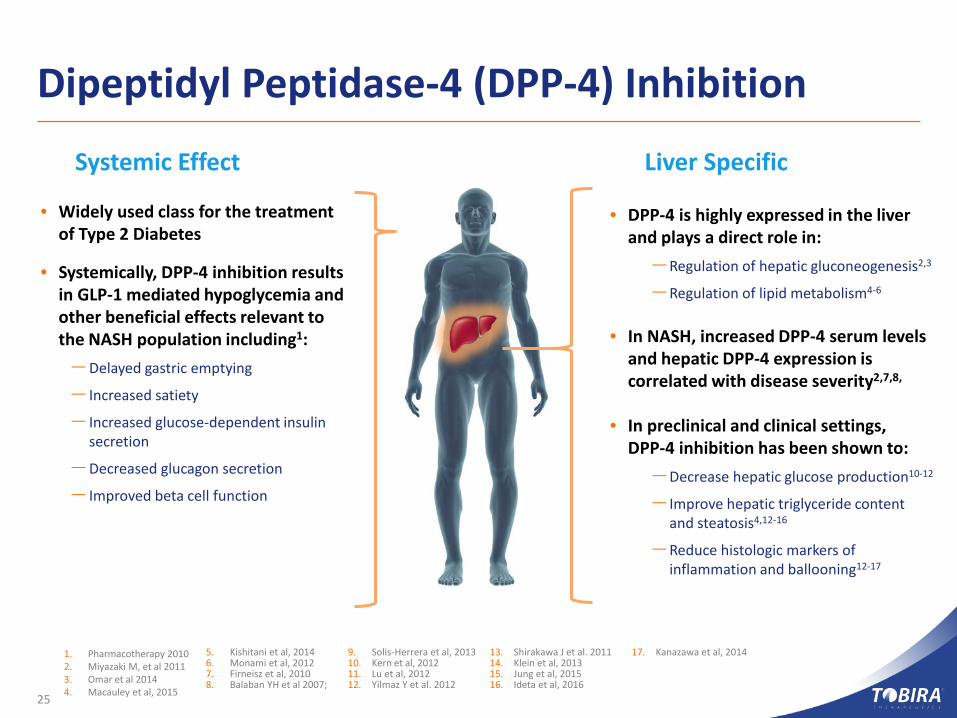
Dipeptidyl Peptidase-4 (DPP-4) Inhibition
25
• Widely used class for the treatment of Type 2 Diabetes
• Systemically, DPP-4 inhibition results in GLP-1 mediated hypoglycemia and other beneficial effects relevant to the NASH population including1:–Delayed gastric emptying
– Increased satiety
– Increased glucose-dependent insulin secretion
–Decreased glucagon secretion
– Improved beta cell function
• DPP-4 is highly expressed in the liver and plays a direct role in:–Regulation of hepatic gluconeogenesis2,3
–Regulation of lipid metabolism4-6
• In NASH, increased DPP-4 serum levels and hepatic DPP-4 expression is correlated with disease severity2,7,8,
• In preclinical and clinical settings, DPP-4 inhibition has been shown to:–Decrease hepatic glucose production10-12
– Improve hepatic triglyceride content and steatosis4,12-16
–Reduce histologic markers of inflammation and ballooning12-17
Systemic Effect Liver Specific
1. Pharmacotherapy 20102. Miyazaki M, et al 20113. Omar et al 20144. Macauley et al, 2015
5. Kishitani et al, 20146. Monami et al, 20127. Firneisz et al, 20108. Balaban YH et al 2007;
13. Shirakawa J et al. 201114. Klein et al, 201315. Jung et al, 201516. Ideta et al, 2016
9. Solis-Herrera et al, 201310. Kern et al, 201211. Lu et al, 201212. Yilmaz Y et al. 2012
17. Kanazawa et al, 2014
Evogliptin Overview
26
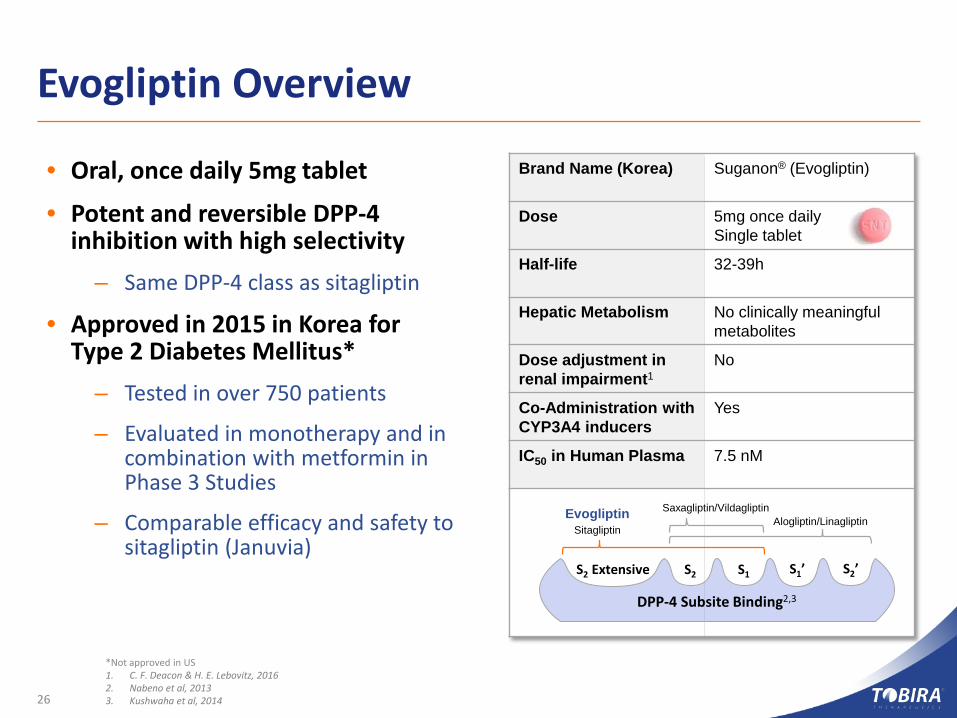
• Oral, once daily 5mg tablet
• Potent and reversible DPP-4 inhibition with high selectivity
– Same DPP-4 class as sitagliptin
• Approved in 2015 in Korea for Type 2 Diabetes Mellitus*
– Tested in over 750 patients
– Evaluated in monotherapy and in combination with metformin in Phase 3 Studies
– Comparable efficacy and safety to sitagliptin (Januvia)
*Not approved in US1. C. F. Deacon & H. E. Lebovitz, 20162. Nabeno et al, 20133. Kushwaha et al, 2014
Brand Name (Korea) Suganon® (Evogliptin)
Dose 5mg once dailySingle tablet
Half-life 32-39h
Hepatic Metabolism No clinically meaningful metabolites
Dose adjustment inrenal impairment1
No
Co-Administration with CYP3A4 inducers
Yes
IC50 in Human Plasma 7.5 nM
DPP-4 Subsite Binding2,3
S2 Extensive S2 S1 S1’ S2’
EvogliptinSitagliptin
Saxagliptin/VildagliptinAlogliptin/Linagliptin
Transaction Overview
27
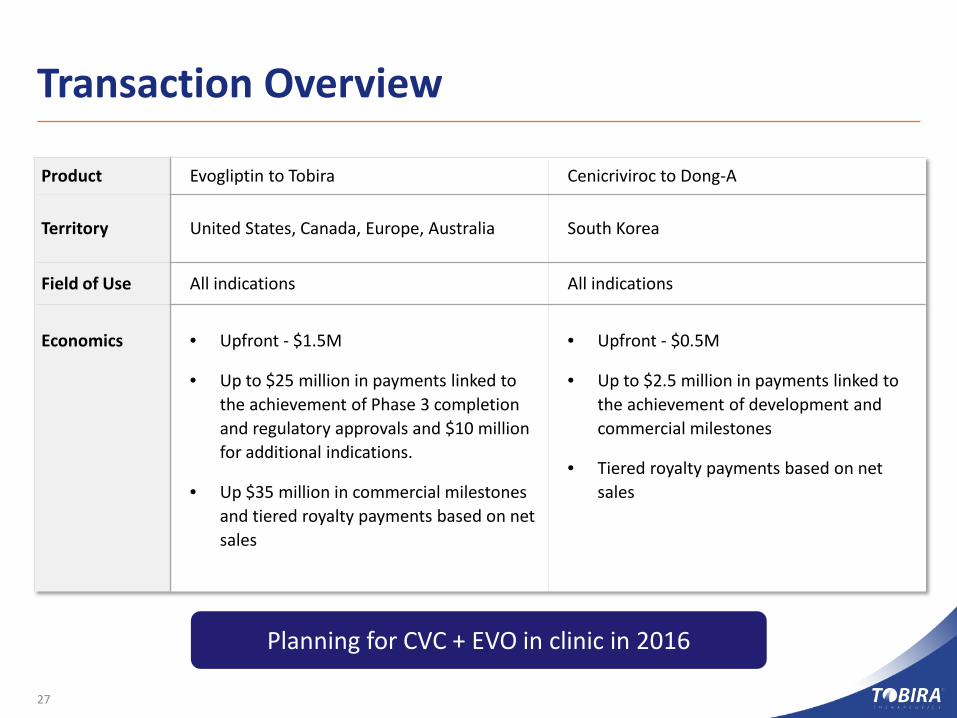
Product Evogliptin to Tobira Cenicriviroc to Dong-A
Territory United States, Canada, Europe, Australia South Korea
Field of Use All indications All indications
Economics • Upfront - $1.5M
• Up to $25 million in payments linked to the achievement of Phase 3 completion and regulatory approvals and $10 million for additional indications.
• Up $35 million in commercial milestones and tiered royalty payments based on net sales
• Upfront - $0.5M
• Up to $2.5 million in payments linked to the achievement of development andcommercial milestones
• Tiered royalty payments based on net sales
Planning for CVC + EVO in clinic in 2016

28
CVC for Primary SclerosingCholangitis
Primary Sclerosing Cholangitis (PSC)
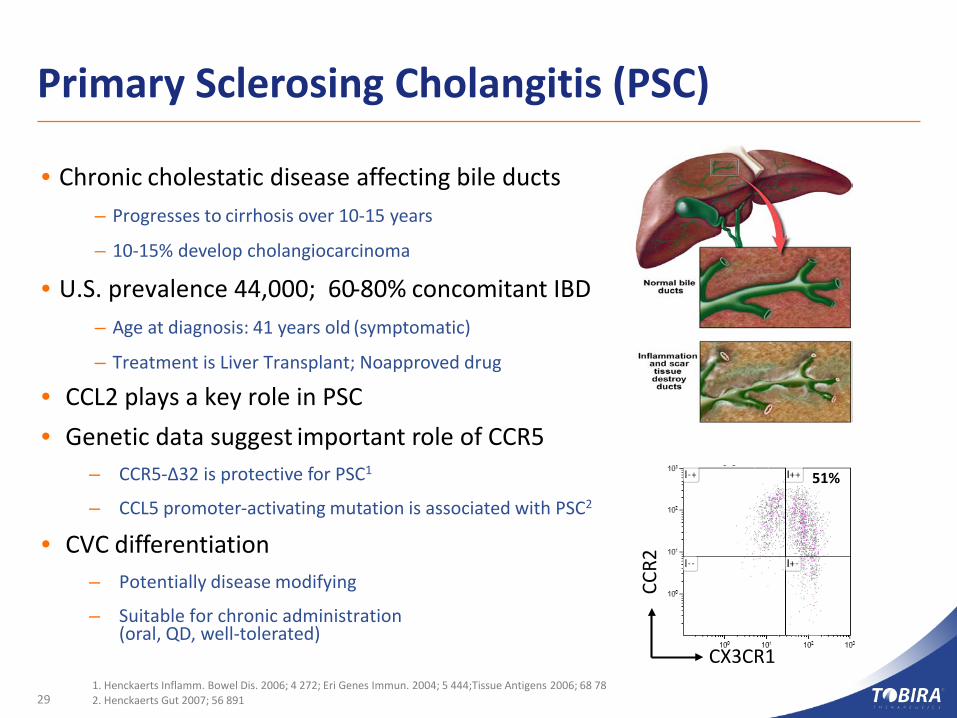
• Chronic cholestatic disease affecting bile ducts– Progresses to cirrhosis over 10-15 years
– 10-15% develop cholangiocarcinoma
• U.S. prevalence 44,000; 60-80% concomitant IBD– Age at diagnosis: 41 years old (symptomatic)
– Treatment is Liver Transplant; No approved drug
• CCL2 plays a key role in PSC• Genetic data suggest important role of CCR5
– CCR5-Δ32 is protective for PSC1
– CCL5 promoter-activating mutation is associated with PSC2
• CVC differentiation– Potentially disease modifying
– Suitable for chronic administration (oral, QD, well-tolerated)
1. Henckaerts Inflamm. Bowel Dis. 2006; 4 272; Eri Genes Immun. 2004; 5 444;Tissue Antigens 2006; 68 782. Henckaerts Gut 2007; 56 89129
CX3CR1CC
R2
51%
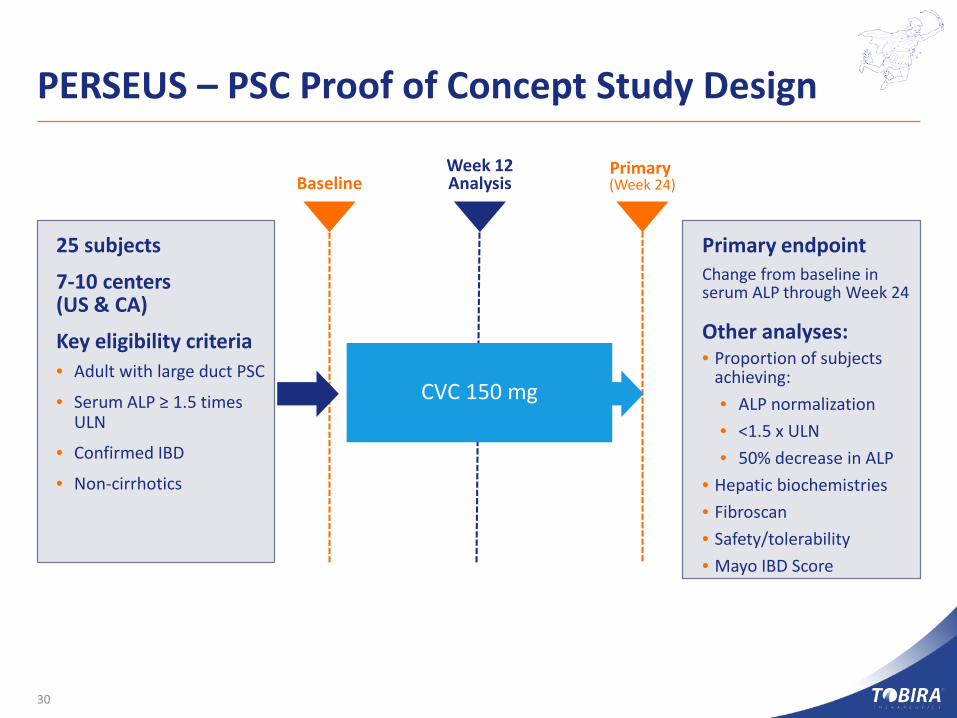
PERSEUS – PSC Proof of Concept Study Design
CVC 150 mg
25 subjects
7-10 centers (US & CA)
Key eligibility criteria• Adult with large duct PSC
• Serum ALP ≥ 1.5 times ULN
• Confirmed IBD
• Non-cirrhotics
Primary endpointChange from baseline in serum ALP through Week 24
Other analyses:• Proportion of subjects
achieving:• ALP normalization• <1.5 x ULN • 50% decrease in ALP
• Hepatic biochemistries• Fibroscan• Safety/tolerability• Mayo IBD Score
Primary (Week 24)Baseline
Week 12Analysis
30

Summary
31
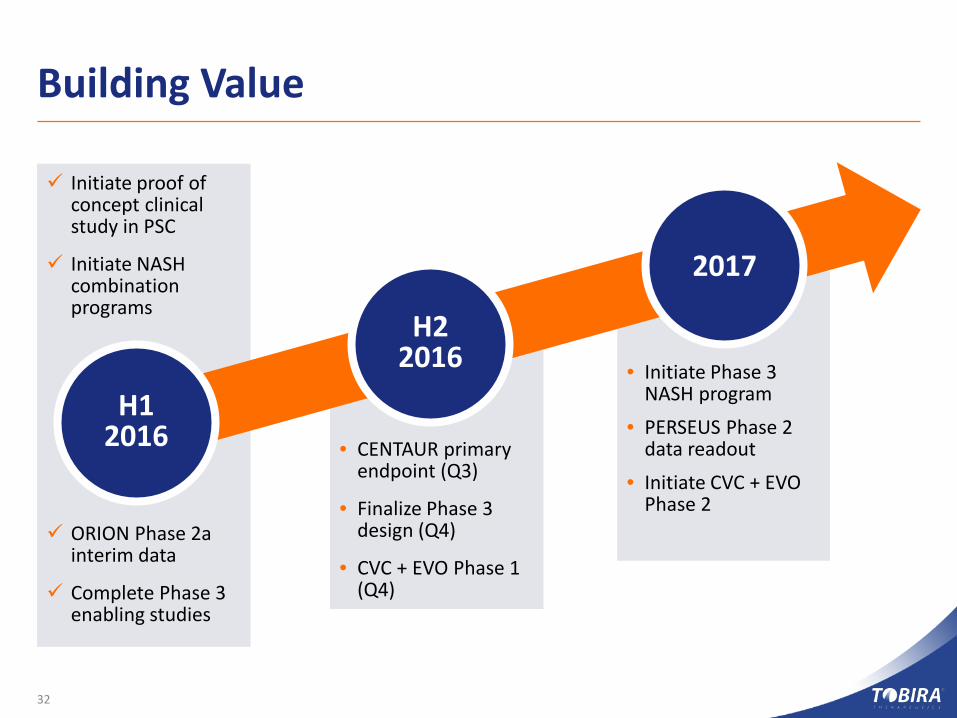
• Initiate Phase 3 NASH program
• PERSEUS Phase 2 data readout
• Initiate CVC + EVO Phase 2
• CENTAUR primary endpoint (Q3)
• Finalize Phase 3 design (Q4)
• CVC + EVO Phase 1 (Q4)
Initiate proof of concept clinical study in PSC
Initiate NASH combination programs
ORION Phase 2a interim data
Complete Phase 3 enabling studies
Building Value
32
H12016
H22016
2017
Changing the Course of NASH & Liver Disease
33
Building a leading NASH program• Cenicriviroc (CVC) Phase 2b CENTAUR data Q3 2016• Evogliptin (EVO) + CVC combination study planned for 2016
Building long-term value• Transition to Phase 3 for CVC single-agent, combinations to follow• Q1 2016 cash balance: $53 million; cash runway to H2 2017
CVC: potent immuno-inflammatory agent• Once-daily dosing & favorable safety profile; cornerstone potential for NASH• Phase 2 in Primary Sclerosing Cholangitis: potential to be disease modifying

T A R G E T I N G S E R I O U S D I S E A S E S O F I M M U N O - I N F L A M M A T I O N A N D F I B R O S I S
Company Contact:Ian Clements, [email protected]
www.tobiratx.com
©2016 Tobira Therapeutics, Inc. All rights reserved. Tobira® is a trademark or registered trademarks of Tobira Therapeutics, Inc. in the United States and other countries. All other trademarks are the property of their respective owners. The information herein is for informational purposes only and represents the current view of Tobira Therapeutics, Inc. as of the date of this presentation. Tobira cannot guarantee the accuracy of any information provided after the date of this presentation. Tobira makes no warranties, express, implied or statutory, as to the information in this presentation.
34






![Review Advances in CRISPR/Cas-based Gene Therapy in Human ... · setting to investigate and treat genetic diseases , [26] infectious diseases [27], cancers [28], and immuno-logical](https://img.pdfslide.us/doc/110x75/5ecaf70131e6bc613a32fd19/review-advances-in-crisprcas-based-gene-therapy-in-human-setting-to-investigate.jpg)





















