Embed Size (px)
Citation preview

MGM Resorts InternationalInnovative Health Programs
Lauren BendixHealth Programs ManagerMGM Resorts International
DSL #13-0511Ethicon Endo-Surgery, Inc. (EES) is the sponsor of this program and Lauren Bendix is a consultant for EES. EES has no independent knowledge concerning the information contained in this presentation and the findings and conclusions expressed are those reached by the presenter.

MGM Resorts International•MGM Resorts International is the largest private employer in the State of Nevada, with over 50,000 employees residing in Nevada and a total of 62,000 company-wide.
•One of the world’s leading global hospitality companies, operating a portfolio of destination resort brands, including ARIA, Bellagio, MGM Grand, Mandalay Bay and The Mirage, to name a few.
•Owns and operates 15 properties located in Nevada, Mississippi and Michigan, and has 50% investments in properties in Nevada, Illinois and Macau.

MGM and a Culture of Health“We know our people are our most valuable asset so we have designed an innovative weight management program across a continuum of care that is inclusive
of bariatric surgery coverage and a medically supervised weight management program.”
Our Goals:• Foster emotional well-being and improve quality of life for employees• Encourage behavior modification and maintenance of a healthy lifestyle• Decrease direct and indirect healthcare costs.
3
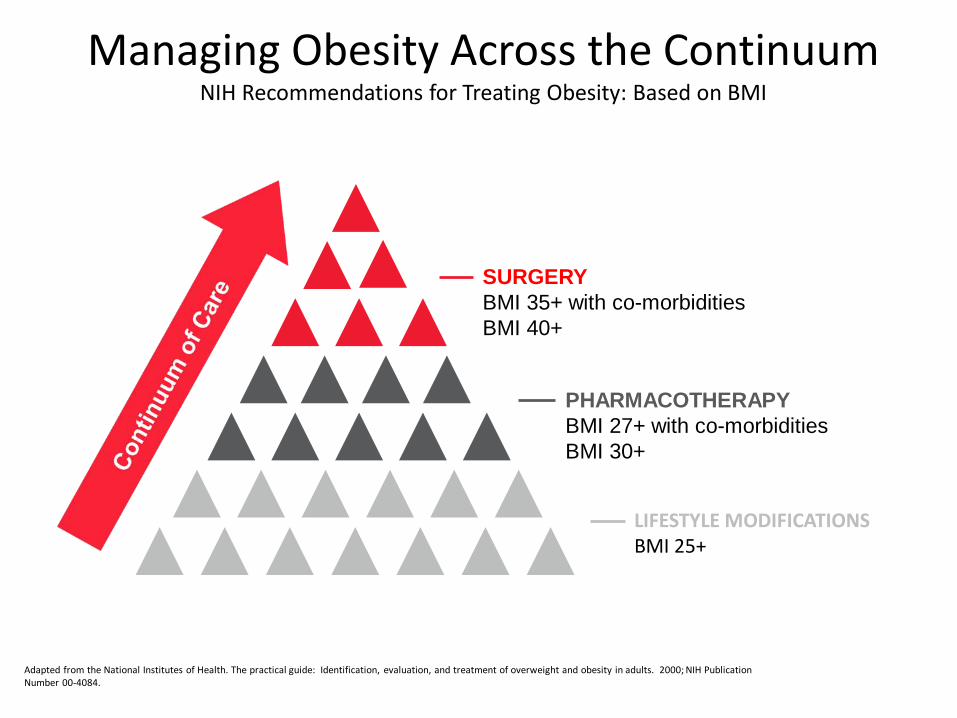
Managing Obesity Across the ContinuumNIH Recommendations for Treating Obesity: Based on BMI
Adapted from the National Institutes of Health. The practical guide: Identification, evaluation, and treatment of overweight and obesity in adults. 2000; NIH Publication Number 00-4084.
LIFESTYLE MODIFICATIONSBMI 25+
PHARMACOTHERAPYBMI 27+ with co-morbiditiesBMI 30+
SURGERYBMI 35+ with co-morbiditiesBMI 40+

Incorporating Innovative Benefit DesignsMetabolic Surgery for Comorbid Resolution
Goal: To create a surgical weight loss alternative to those meeting specific qualifications which will ultimately help
program members achieve a healthier status.• Eligibility • Employees are eligible after 91 days of employment • Must be age 18 and over • Maintain continuous enrollment in the MGM-sponsored
Health Plan• Includes COBRA members who maintain eligibility in the Health Plan
5
Program Requirements of the Patient
• Evaluation by a designated program physician to ensure all requirements are met
Program criteria include the following.• A body Mass Index (BMI) of 40 or greater; or• A BMI between 35-39.9 with at least one clinically significant health issue, including
but not limited to, cardiovascular disease, Type 2 diabetes, hypertension, coronary artery disease or pulmonary hypertension.
• Participation in a medically supervised nutritional counseling• 6 month educational process inclusive of 13 classes covering nutrition,
exercise and weight management. • Psychological Evaluation• Participation in a pre-op/post-op program
6
Metabolic/Bariatric Surgery Benefit Design• Covered Procedures:
• Bypass• Sleeve Gastrectomy• Gastric Band
• $5,000 copay• 20% coinsurance related to incidentals related to pre-
operative clearance tests, prescription co-pays • $20 co-pay for office visits associated with the medically
supervised weight loss program• A stop loss benefit to minimize plan exposure for
expenses related to complications.
7
Incentive Program
***Reimbursement of $5,000 copay post surgery if requirements are met.***
***$5,000 cosmetic surgery benefit is available upon successful completion of requirements.***
8
The Results: Surgical Program
• 88 patients have had surgery • Average weight loss during pre-surgery medically
supervised weight management program was 18 pounds.• Average weight loss was 55 pounds, up to 227 pounds for
14 months post-surgery. • 56.6% reduction in medications taken post-surgery
during the first 6 months of the program.• 80.3% reduction in co-morbidities post-surgery during
the first 6 months of the program.• Quality of Life Improvements
Surgical Weight Control Center. MGM Properties Weight Loss Data, Medical & Surgical. January 11, 2013
9
The Results:Non-Surgical Program
• 227 patients since inception • 106 active participants • 40 participants - 3 month plan • 66 participants - 6 month plan • Average beginning weight= 224 • Highest initial weight= 410 • Lowest weight= 139 • Greatest amount of weight loss= 108 pounds • Total pounds lost since inception= 2804
10
Lessons Learned
• Benefits of having an exclusive COE provider• Importance of the non-surgical benefit• High-touch and collaborative culture
• Patient• Provider• Plan
11

Keys to Success:Benefit Plan Considerations
• Require employees to be treated by Centers of Excellence– Through health plan (TPA) or ASMBS/SRC COE lists
• Cover bariatric surgery at a greater benefit level than other conditions– Thoughtful co-pay, deductibles, etc.
• Incent patients for long-term compliance– Co-pay reimbursement– Pay for plastic surgery with compliance to follow-up physician/care team
appointments
• Continued support through onsite weight loss & wellness programs– Jim’s Plate– Onsite wellness coaches
12
The Direct Care Health Plan
• Conducted extensive research on best practices for health care delivery.
• Sought input from health care delivery thought leaders, and reviewed case studies of established programs.
• Every source lead back to the importance of a delivery system predicated upon the direction of care provided by the primary care physician.
• Created a plan called the Direct Care Health Plan, built upon the principles of a patient-centered medical home.
The Direct Care Health Plan• Developed direct contractual relationships with 18 PCPs and spent countless hours
discussing how best to adapt the principles of the medical home model to the unique challenges that Nevada’s health care system presents.
– Patient access to medical care - Wait times delay timely identification and treatment of conditions
– Appropriate physician reimbursement - Value physicians for their time, which allows sufficient time to accurately diagnose, treat and answer patient questions. In short, we have built this plan to reimburse providers more for quality and outcomes.
– Patient engagement in and accountability of their health - Prevention/early detection/annual physical
– Use of technology - Physician collection and review of medical data to increase the efficiency of medical care provided and proactively manage the health of their patient population

The Direct Care Health Plan• More than 2,500 employees enrolled in the Direct Care Plan, representing
over 5,000 people
• After 8 months of experience, the early results are extremely encouraging.
– 97% of Plan members obtained annual physical• 98% of employees• 95% of spouses• 90% of adult age dependents
– 3% who did not obtain represent• 67 employees• 115 dependents
– Success stories - We found patients who were “lost” in the system finally getting the help they needed to patients who were immediately admitted to the hospital upon arrival to their primary care physician’s office for an annual wellness physical.
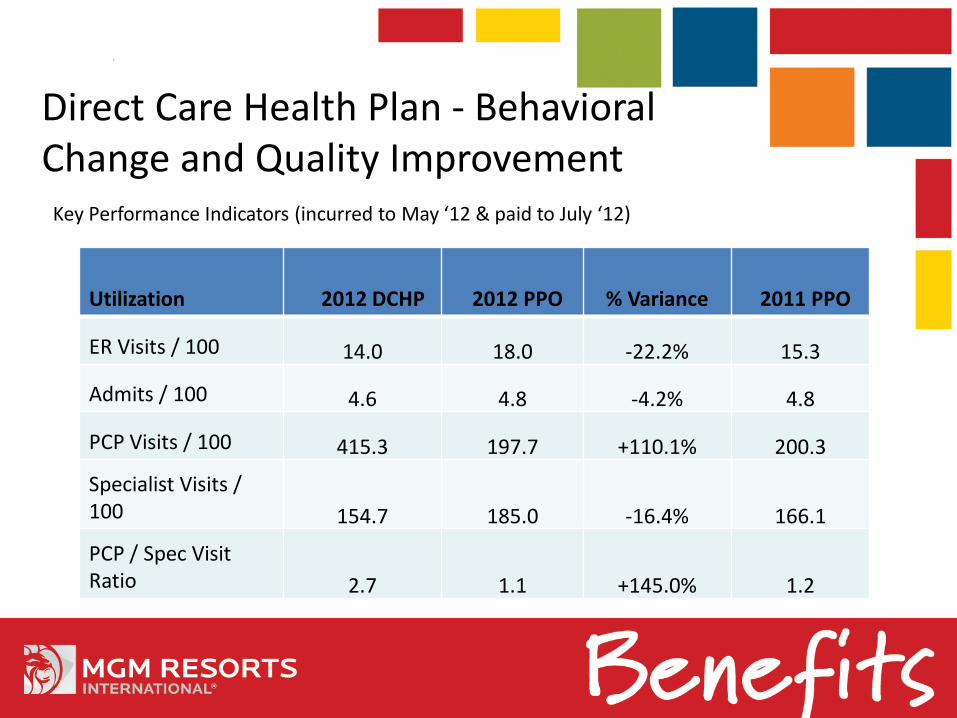
Direct Care Health Plan - Behavioral Change and Quality Improvement
Key Performance Indicators (incurred to May ‘12 & paid to July ‘12)
Utilization 2012 DCHP 2012 PPO % Variance 2011 PPO
ER Visits / 100 14.0 18.0 -22.2% 15.3
Admits / 100 4.6 4.8 -4.2% 4.8
PCP Visits / 100 415.3 197.7 +110.1% 200.3
Specialist Visits / 100 154.7 185.0 -16.4% 166.1
PCP / Spec Visit Ratio 2.7 1.1 +145.0% 1.2
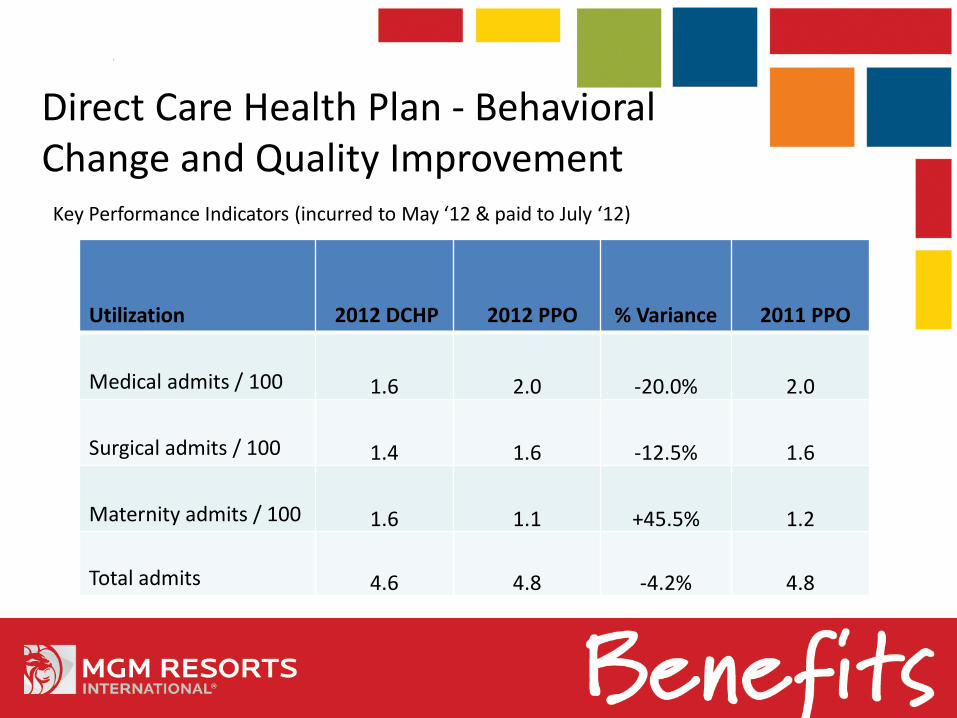
Direct Care Health Plan - Behavioral Change and Quality Improvement
Key Performance Indicators (incurred to May ‘12 & paid to July ‘12)
Utilization 2012 DCHP 2012 PPO % Variance 2011 PPO
Medical admits / 100 1.6 2.0 -20.0% 2.0
Surgical admits / 100 1.4 1.6 -12.5% 1.6
Maternity admits / 100 1.6 1.1 +45.5% 1.2
Total admits 4.6 4.8 -4.2% 4.8
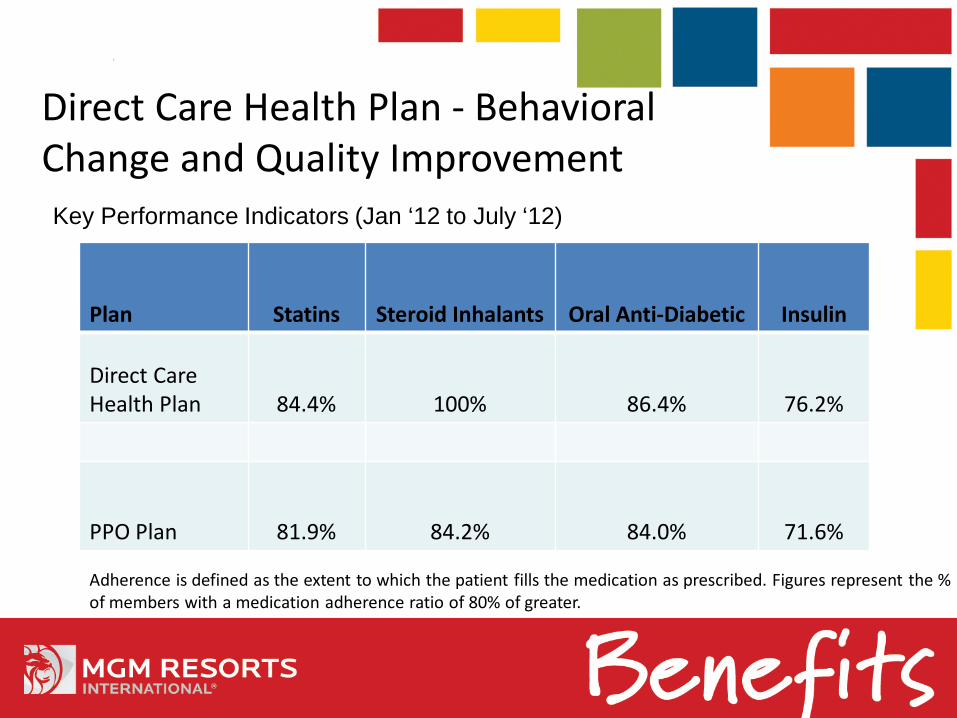
Direct Care Health Plan - Behavioral Change and Quality ImprovementKey Performance Indicators (Jan ‘12 to July ‘12)
Plan Statins Steroid Inhalants Oral Anti-Diabetic Insulin
Direct Care Health Plan 84.4% 100% 86.4% 76.2%
PPO Plan 81.9% 84.2% 84.0% 71.6%
Adherence is defined as the extent to which the patient fills the medication as prescribed. Figures represent the % of members with a medication adherence ratio of 80% of greater.
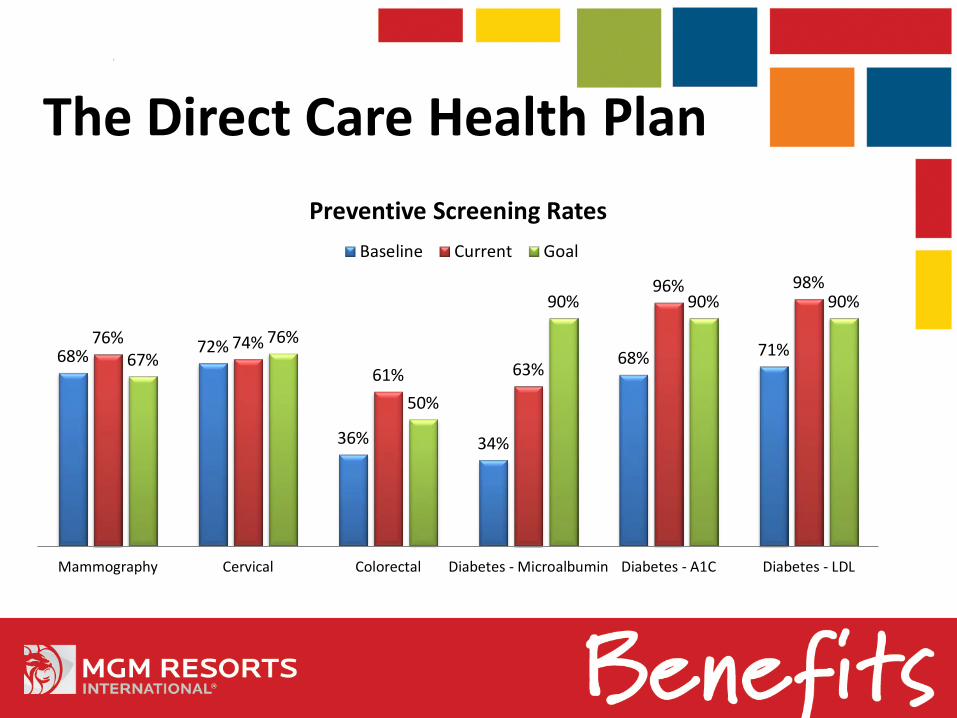
68% 72%
36% 34%
68% 71%76% 74%
61% 63%
96% 98%
67%76%
50%
90% 90% 90%
Mammography Cervical Colorectal Diabetes - Microalbumin Diabetes - A1C Diabetes - LDL
Preventive Screening RatesBaseline Current Goal
The Direct Care Health Plan
The Direct Care Health PlanUPDATES FOR 2013
• Patient-Centered Medical Care, not Data-Centered• Identification of gaps in care• Proactive outreach• Informed office visits• Follow up between visits
• Physical Exams• Evidence-based recommendations about clinical preventive services such as screenings,
counseling services, or preventive medications• Based on recommendations from the United States Preventative Services Task Force• Will serve as valuable tool to help PCP and patients have a conversation about which
clinical preventative services are best for them
• Added three new PCPs• Added 1,940 employees for 2013 for a total of approx 4,500 employees

Healthy Eating. Healthy You.Commitment to remove and reduce barriers to making healthier eating decisions

Healthier Eating at Home
Provide a solution for employees to eat healthier at home
•“Based on the published literature, the most cost-effective way to prevent obesity in youth is the Coordinated Approach to Child Health (CATCH), a comprehensive intervention to promote healthy eating and physical activity in elementary schools, which costs $900 per QALY saved” CORNELL ECONOMIST JOHN CAWLEY
•Health Affairs, 2010

There’s an App for that!

Questions?

Appendix
Surgical Out-of-Pocket Reimbursement Requirements
• 1 year post- surgery, program member must have attained 40% targeted weight loss, with an additional loss of 10% per year at the 2 year, 3 year, and 4 year surgical anniversary (a total of 70% at year 4). Weight loss target to be determined by the Surgery Center/Surgeon and agreed upon by program member prior to surgery.
• Weight loss will be monitored by the Surgery Center and will be reported to the Health Plan for consideration of reimbursement.
• Program member must maintain continuous Health Plan enrollment to be eligible to receive the reimbursement. Continuation of coverage under COBRA meets this requirement.
• The reimbursement will be in the form of a check issued by Health Plan’s claim administrator and payable to program member.
• Out of pocket expenses include the surgery co-pay of $5,000 (prescription drug co-pays or over the counter supplements are not included).
• Reimbursement request forms are to be completed by both the Surgery Center and the program member attesting to adherence to program requirements.
Cosmetic Surgery Reimbursement Requirements
• Minimum of 2 years post-surgery, or when member has lost 70% of excess weight
• Weight loss will be monitored by the Surgery Center to be reported back to Health Plan to receive this incentive
• The total contribution for the plastic surgery incentive is $5,000 which can be used with a physician of the member’s choice.
• Member must maintain active and continuous enrollment in health plan to receive this incentive
• Member must have participated in a minimum of 6 support groups per year in addition to the 4 mandatory psychological post-op consultations.
• The Surgery Center will determine if member meets criteria for cosmetic services prior to cosmetic procedure
• Cosmetic services must be performed and the member must submit for reimbursement, including receipt showing payment of $5,000.00.
Testimonial #1“It is said that we cannot enter the womb to be born again, but SWCC
has done the next best thing. I have a new life thanks to the surgery, classes, and nutritional guidance provided at SWCC. Having lost 95 lbs over the last year has given me a new life. The energy levels are up, I am able to do some of the simplest things, like tying shoes, that I was not able to do before. Truly, I have been born anew. Thank you SWCC!” - CC, Poker Room Manager at MGM

Testimonial #2
“I came to one of the seminars Dr. Soong gave. I was weighing about
274 lbs. I’m a 62 year-old man. I was done weighing this much…I
had the surgery in July 2011 and as of now I’m at 214 lbs. I feel
wonderful…I no longer take any pills for anything. I go to the gym 3
or 4 times a week…I would do this all over again if I had to.” - FM,
Supervisor at MGM Hotel

Testimonial #3“My experience with this entire program has been phenomenal. The
Mind Over Eating classes were an amazing learning experience and an invaluable tool. I have had no complaints or problems after the surgery. I feel so much better, and have so much more energy. I have successfully eliminated all of my medications. The opportunity to participate in this program and have the surgery is truly a gift that I otherwise would not have been able to do and I am truly thankful.” - DS, Cage Cashier at Aria

Testimonial #4“Since enrolling into MGM’s Direct Care program, I feel as if the quality
of my care improved tenfold. My Direct Care doctor, reminds me of the old-fashioned doctors that used to do house calls; patient, caring, attentive, and pays attention to every detail. I had only been a patient under the Direct Care program for one month before needing their services and never once was I denied services because of my short membership period. Every specialist I’ve been referred to by my doctor has had the same professional attitude, concern for my well-being and ready to “fix” whatever was “broken”. - Employee

“The Direct Care plan looked interesting for us because it encourages the medical practices to provide comprehensive care for patients while compensating providers with above average reimbursement rates, compared to other health plans,” he said. “For my patients, it encourages them to establish a relationship with me, which ultimately results in better overall health care for the patient.”
– Direct Care Primary Care Physician
Testimonial #5
Direct Care Health PlanPhysician Reimbursements
Global Fee for Service
• Per office visit reimbursement is averaging $60 greater than PPO pricing (84% increase)
Care Management Fee
• Projected Jan – Dec 2012 total of $235k• $6 PMPM• Average per physician payment $12,900
Performance Bonus (total available up to $72 per member per year)
Benchmark Bonus criteria ($36 PMPY)
• Patient satisfaction Registry usage Mammography rates• Cervical screening Colon screening Diabetes screenings• Physical completion rate Generic efficiency Formulary rate
Peer Comparison Bonus criteria ($36 PMPY)
• Readmission rate ER utilization Medication adherence• Preventable admission rate Cost efficiency
Direct Care Health PlanPhysician Reimbursements





























