Embed Size (px)
Citation preview

Targeted Therapy in Head & Neck Cancer
Anti-EGFR Treatment
Jan B. Vermorken, MD, PhD
University Hospital Antwerp
Edegem, Belgium
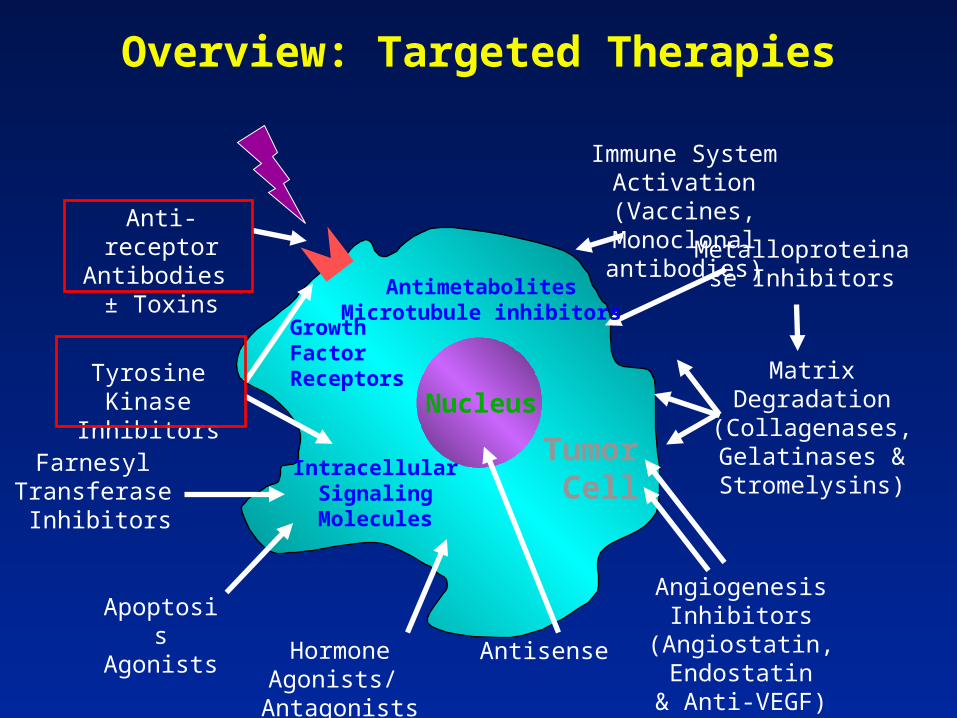
Nucleus
Anti-receptor Antibodies
± Toxins
Tyrosine Kinase Inhibitors
Hormone Agonists/ Antagonists
Farnesyl Transferase
Inhibitors
Apoptosis Agonists
Antisense
Angiogenesis Inhibitors (Angiostatin, Endostatin
& Anti-VEGF)
Metalloproteinase Inhibitors
Matrix Degradation(Collagenases,Gelatinases &Stromelysins)
Immune System Activation (Vaccines,
Monoclonal antibodies)
Tumor Cell
Growth Factor Receptors
Intracellular Signaling Molecules
Overview: Targeted Therapies
AntimetabolitesMicrotubule inhibitors
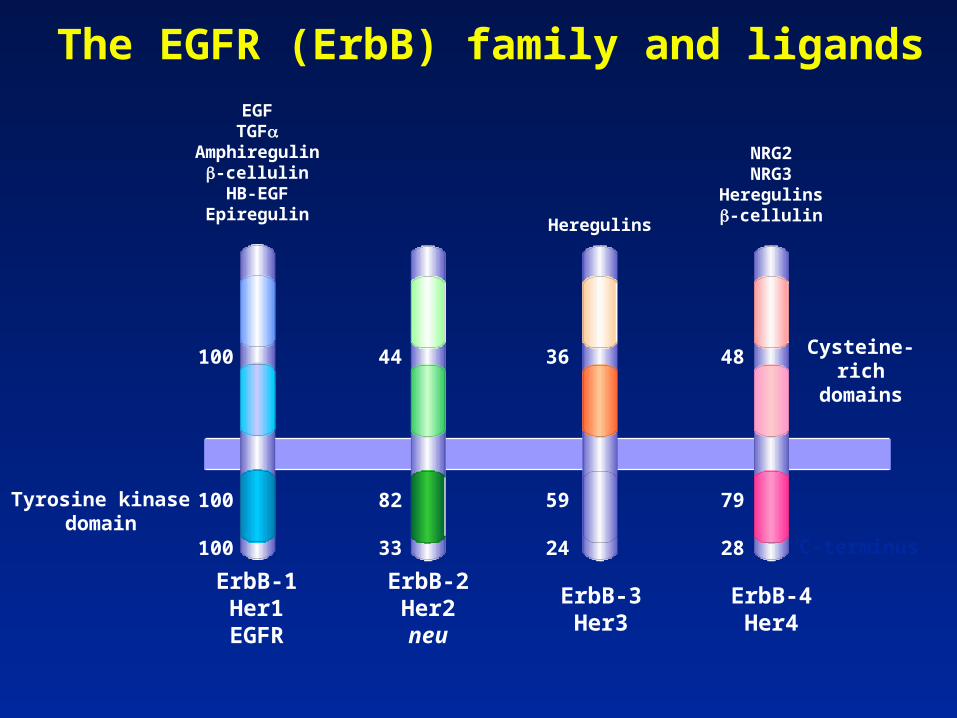
EGFTGF
Amphiregulin-cellulinHB-EGF
EpiregulinHeregulins
NRG2NRG3
Heregulins-cellulin
Cysteine-richdomains
Tyrosine kinasedomain
ErbB-1Her1
EGFR
ErbB-2Her2neu
ErbB-3Her3
ErbB-4Her4
C-terminus
100
100
100
44
82
33
36
59
24
48
79
28
The EGFR (ErbB) family and ligands
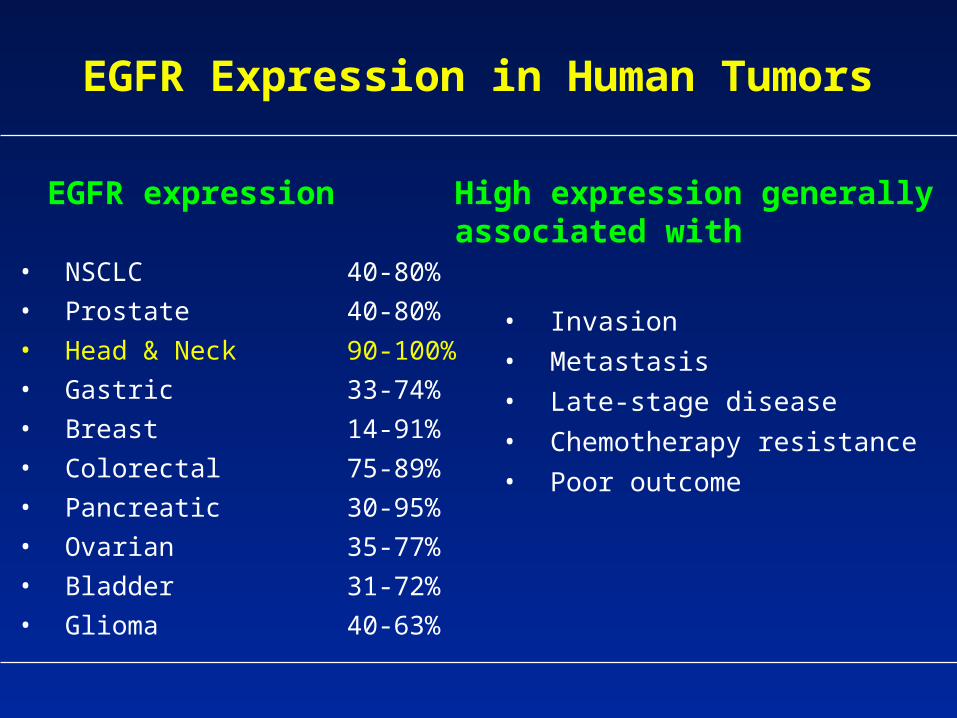
EGFR Expression in Human Tumors
• NSCLC 40-80%
• Prostate 40-80%
• Head & Neck 90-100%
• Gastric 33-74%
• Breast 14-91%
• Colorectal 75-89%
• Pancreatic 30-95%
• Ovarian 35-77%
• Bladder 31-72%
• Glioma 40-63%
• Invasion
• Metastasis
• Late-stage disease
• Chemotherapy resistance
• Poor outcome
EGFR expression High expression generallyassociated with
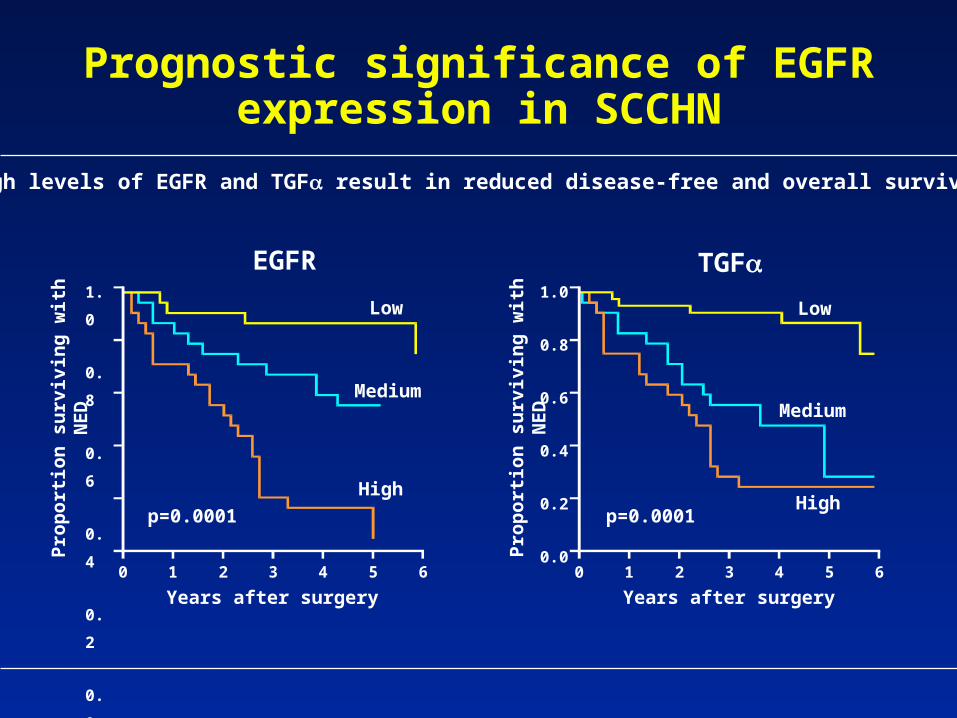
Prognostic significance of EGFR expression in SCCHN
High levels of EGFR and TGF result in reduced disease-free and overall survival
EGFR TGF
Low
Medium
High
p=0.0001
1.
0
0.
8
0.
6
0.
4
0.
2
0.
0
Pro
po
rtio
n s
urv
ivin
g w
ith
NE
D
0 1 2 3 4 5 6
Years after surgery
p=0.0001
Low
Medium
High
1.0
0.8
0.6
0.4
0.2
0.0
Pro
po
rtio
n s
urv
ivin
g w
ith
NE
D
0 1 2 3 4 5 6
Years after surgery
Grandis et al, 1998
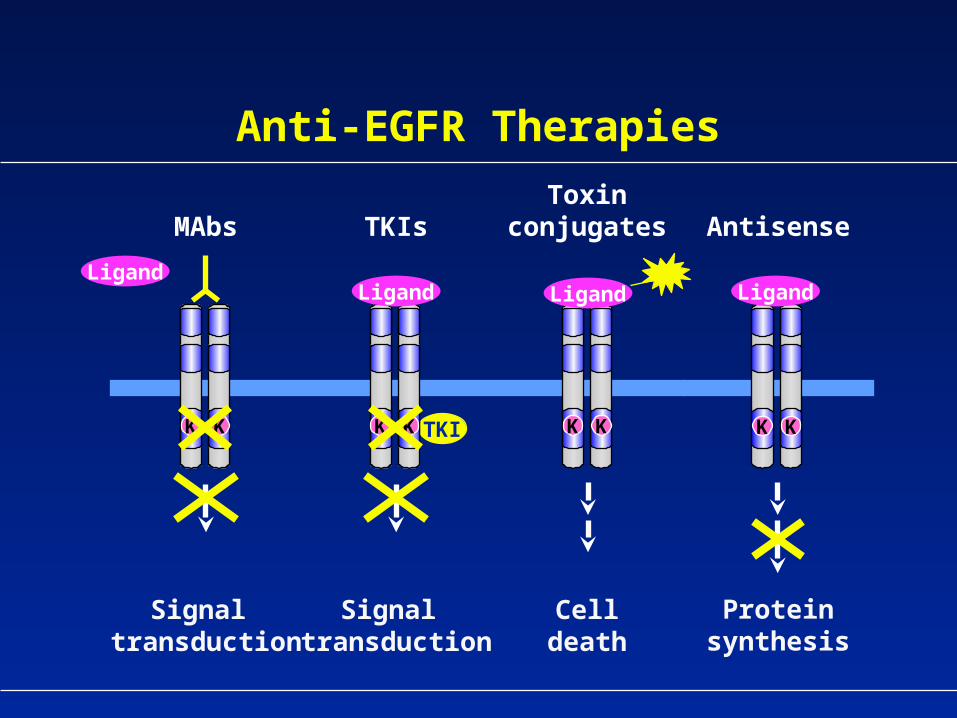
Anti-EGFR Therapies
Signal transduction
Signal transduction
Celldeath
MAbs TKIsToxin
conjugates Antisense
Proteinsynthesis
KKKK
Ligand
KK TKIKK
Ligand Ligand Ligand
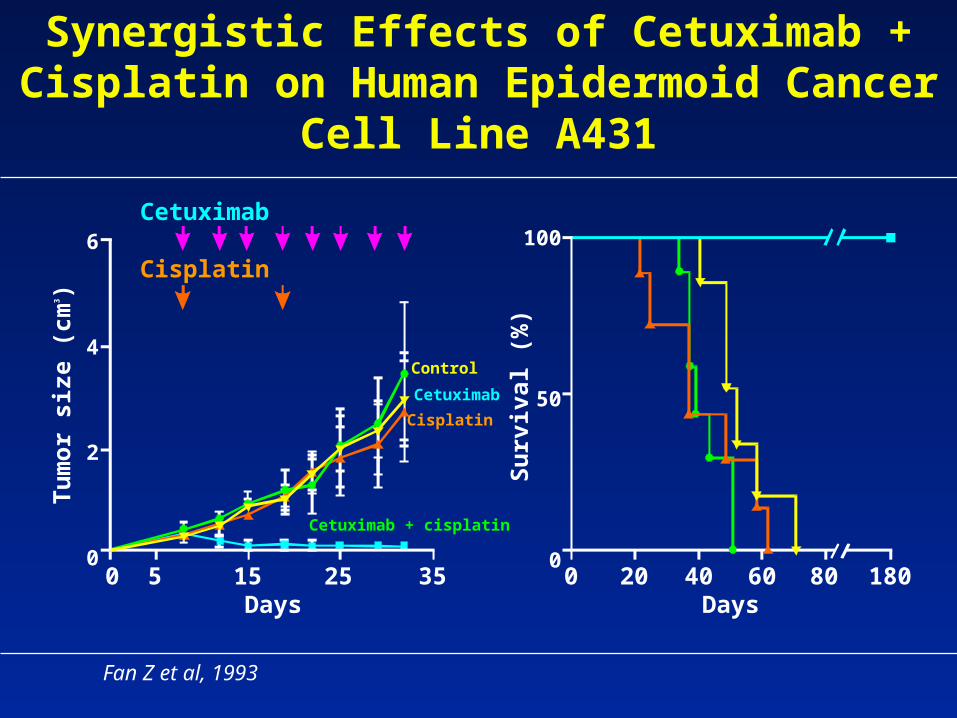
Synergistic Effects of Cetuximab + Cisplatin on Human Epidermoid Cancer Cell Line A431
6
4
2
0
Tu
mo
r si
ze (
cm3 )
Cetuximab
Cisplatin
Days0 20 40 60 80 180
Days
100
50
0
Su
rviv
al (
%)
Control
Cetuximab
Cisplatin
Cetuximab + cisplatin
Fan Z et al, 1993
0 5 15 25 35
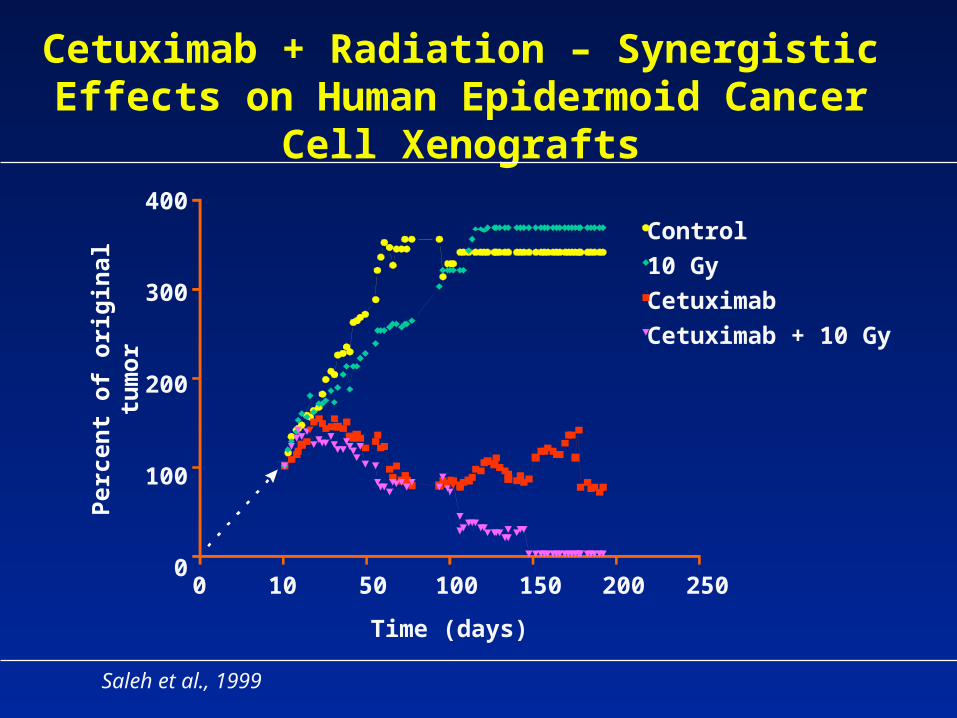
Cetuximab + Radiation – Synergistic Effects on Human Epidermoid Cancer Cell Xenografts
Saleh et al., 1999
0 10 50 100 150 200 250
400
300
200
100
0
Control
10 Gy
Cetuximab
Cetuximab + 10 Gy
Time (days)
Per
cen
t o
f o
rig
inal
tu
mo
r
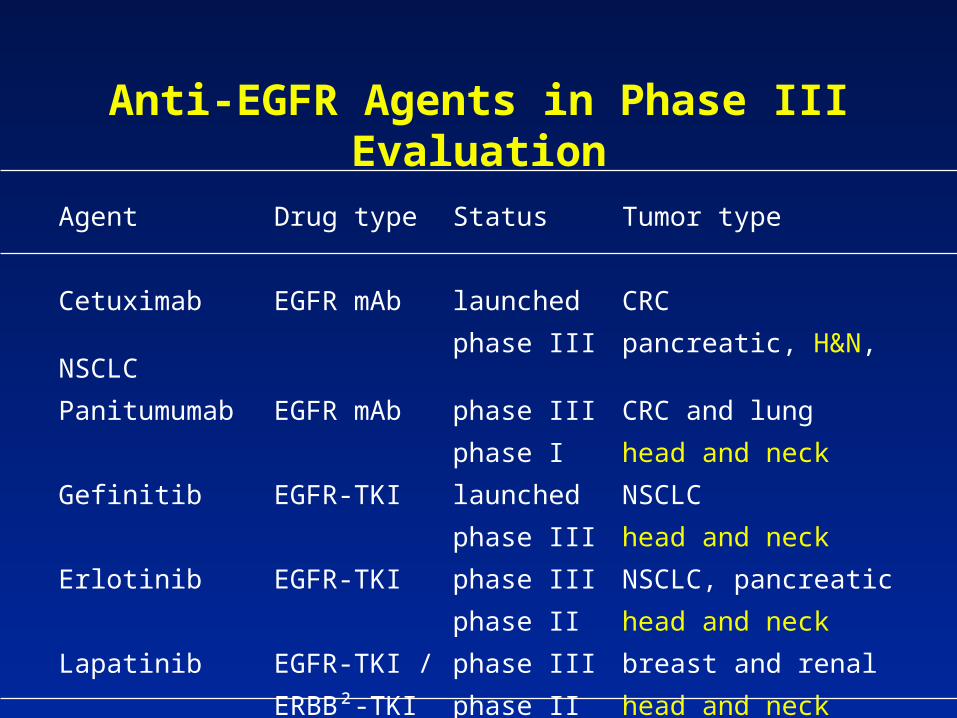
Anti-EGFR Agents in Phase III Evaluation
Agent Drug type Status Tumor type
Cetuximab EGFR mAb launched CRC
phase III pancreatic, H&N, NSCLC
Panitumumab EGFR mAb phase III CRC and lung
phase I head and neck
Gefinitib EGFR-TKI launched NSCLC
phase III head and neck
Erlotinib EGFR-TKI phase III NSCLC, pancreatic
phase II head and neck
Lapatinib EGFR-TKI / phase III breast and renal
ERBB²-TKI phase II head and neck
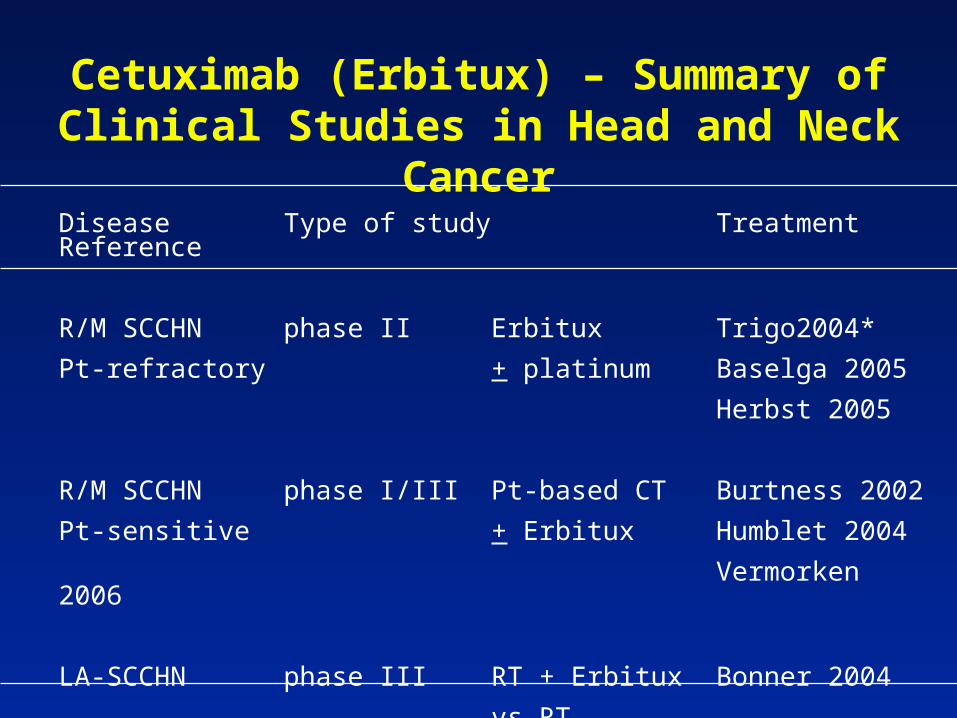
Cetuximab (Erbitux) – Summary of Clinical Studies in Head and Neck Cancer
Disease Type of study Treatment Reference
R/M SCCHN phase II Erbitux Trigo2004*
Pt-refractory + platinum Baselga 2005
Herbst 2005
R/M SCCHN phase I/III Pt-based CT Burtness 2002
Pt-sensitive + Erbitux Humblet 2004
Vermorken 2006
LA-SCCHN phase III RT + Erbitux Bonner 2004
vs RT* Updated Vermorken et al, 2006
Disease progression
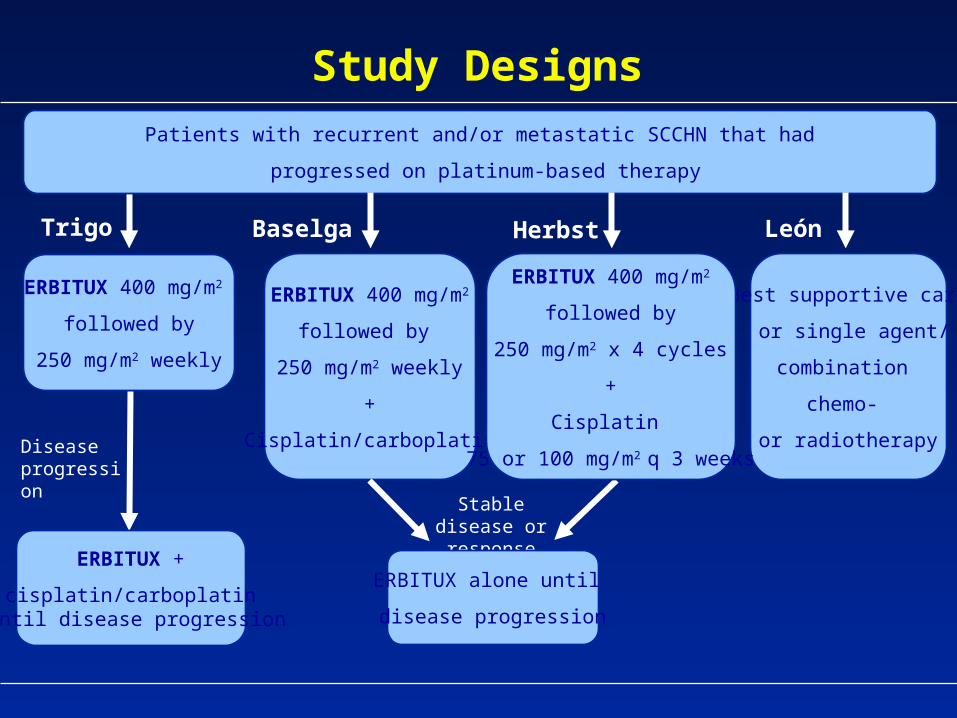
Patients with recurrent and/or metastatic SCCHN that had
progressed on platinum-based therapy
ERBITUX 400 mg/m2
followed by
250 mg/m2 weekly
Best supportive care
or single agent/
combination
chemo-
or radiotherapy
ERBITUX 400 mg/m2
followed by
250 mg/m2 weekly
+
Cisplatin/carboplatin
Stable disease or response
ERBITUX 400 mg/m2
followed by
250 mg/m2 x 4 cycles
+
Cisplatin
75 or 100 mg/m2 q 3 weeks
ERBITUX +
cisplatin/carboplatin until disease progression
ERBITUX alone until
disease progression
Trigo Baselga Herbst León
Study Designs
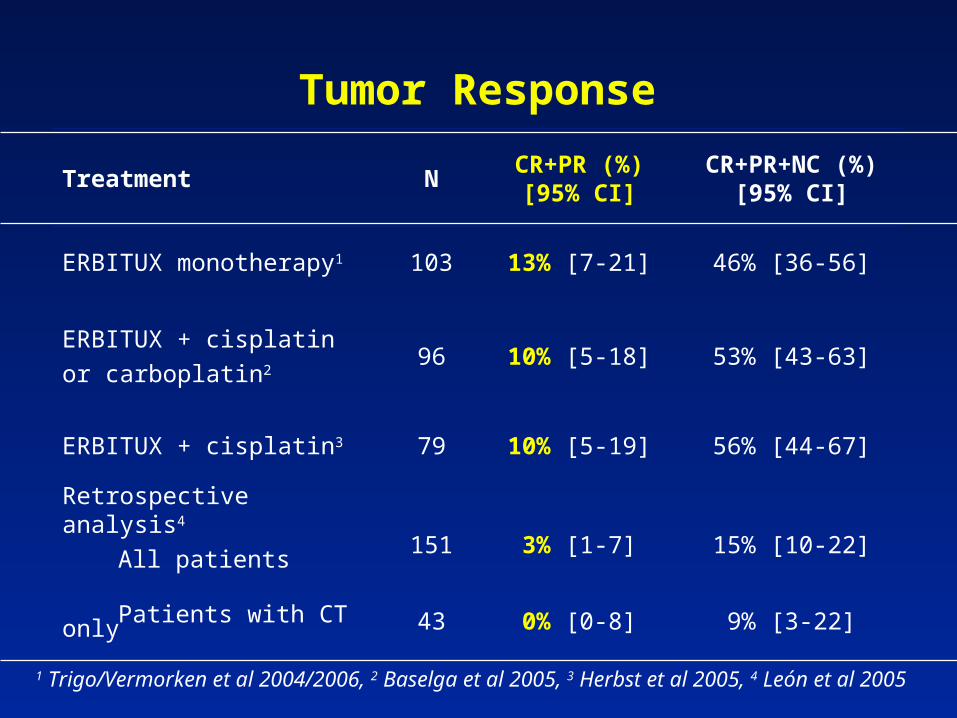
Tumor Response
Treatment NCR+PR (%)
[95% CI]CR+PR+NC (%)
[95% CI]
ERBITUX monotherapy1 103 13% [7-21] 46% [36-56]
ERBITUX + cisplatin
or carboplatin296 10% [5-18] 53% [43-63]
ERBITUX + cisplatin3 79 10% [5-19] 56% [44-67]
Retrospective analysis4
All patients 151 3% [1-7] 15% [10-22]
Patients with CT only 43 0% [0-8] 9% [3-22]
1 Trigo/Vermorken et al 2004/2006, 2 Baselga et al 2005, 3 Herbst et al 2005, 4 León et al 2005
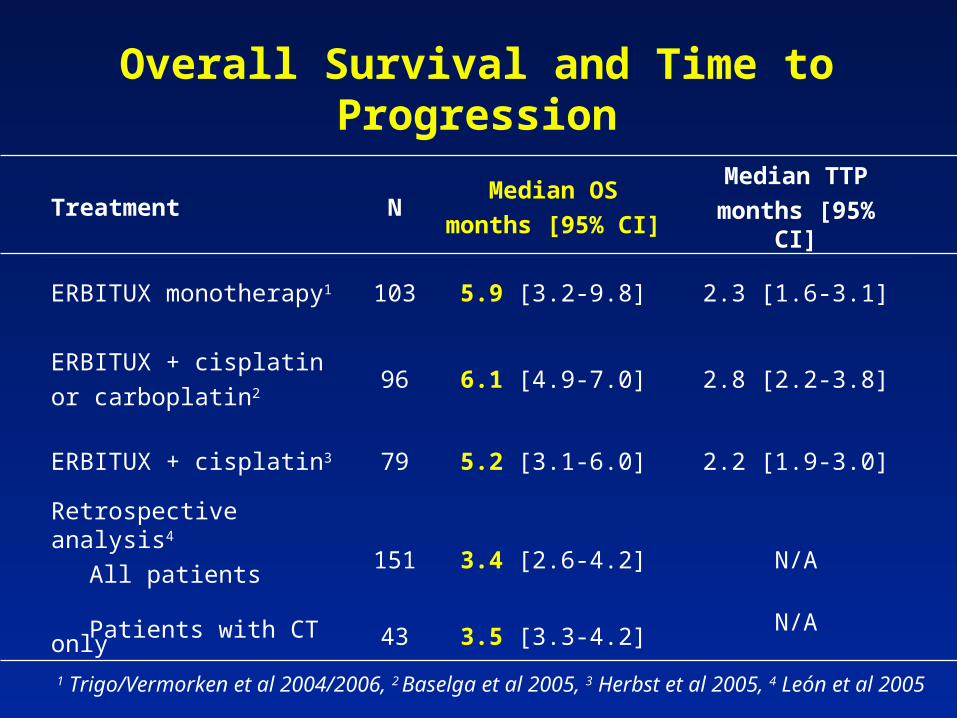
Overall Survival and Time to Progression
Treatment NMedian OS
months [95% CI]
Median TTP
months [95% CI]
ERBITUX monotherapy1 103 5.9 [3.2-9.8] 2.3 [1.6-3.1]
ERBITUX + cisplatin
or carboplatin296 6.1 [4.9-7.0] 2.8 [2.2-3.8]
ERBITUX + cisplatin3 79 5.2 [3.1-6.0] 2.2 [1.9-3.0]
Retrospective analysis4
All patients 151 3.4 [2.6-4.2] N/A
Patients with CT only 43 3.5 [3.3-4.2]N/A
1 Trigo/Vermorken et al 2004/2006, 2 Baselga et al 2005, 3 Herbst et al 2005, 4 León et al 2005
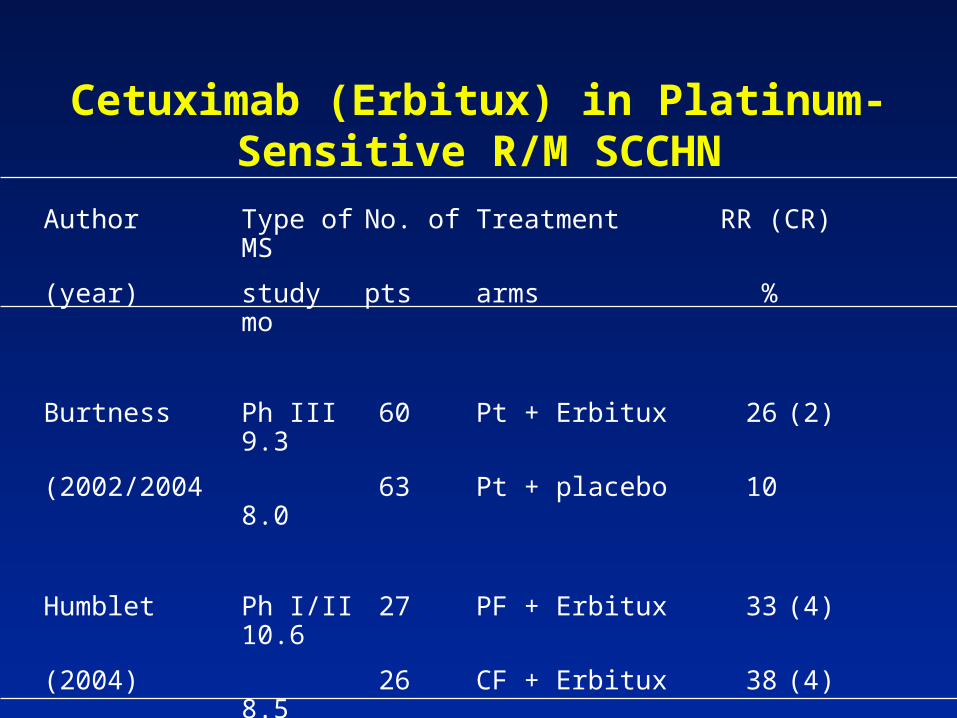
Cetuximab (Erbitux) in Platinum-Sensitive R/M SCCHN
Author Type of No. of Treatment RR (CR)MS
(year) study pts arms %mo
Burtness Ph III 60 Pt + Erbitux 26 (2)9.3
(2002/2004 63 Pt + placebo 108.0
Humblet Ph I/II 27 PF + Erbitux 33 (4)10.6
(2004) 26 CF + Erbitux 38 (4)8.5
Vermorken Ph III 222 Pt/5FU + Erbitux TETE
(2006) 220 Pt/5FU TETE
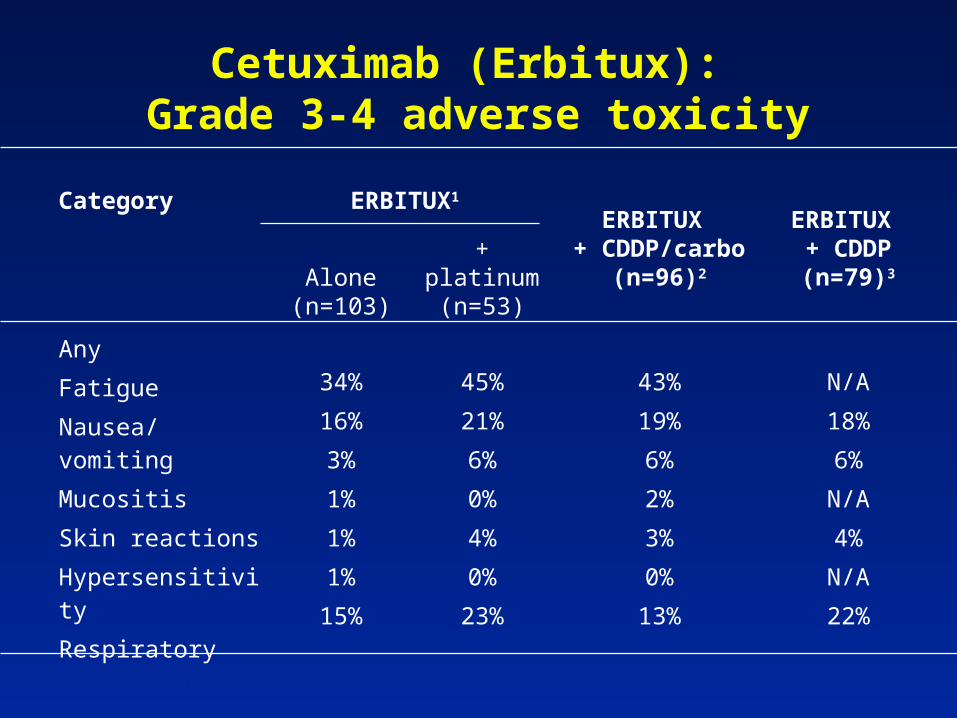
Cetuximab (Erbitux): Grade 3-4 adverse toxicity
Category ERBITUX1 ERBITUX
+ CDDP/carbo (n=96)2
ERBITUX + CDDP (n=79)3Alone
(n=103)
+ platinum (n=53)
Any
Fatigue
Nausea/vomiting
Mucositis
Skin reactions
Hypersensitivity
Respiratory
34%
16%
3%
1%
1%
1%
15%
45%
21%
6%
0%
4%
0%
23%
43%
19%
6%
2%
3%
0%
13%
N/A
18%
6%
N/A
4%
N/A
22%
1 Trigo et al 2004, 2 Baselga et al 2005, 3 Herbst et al 2005
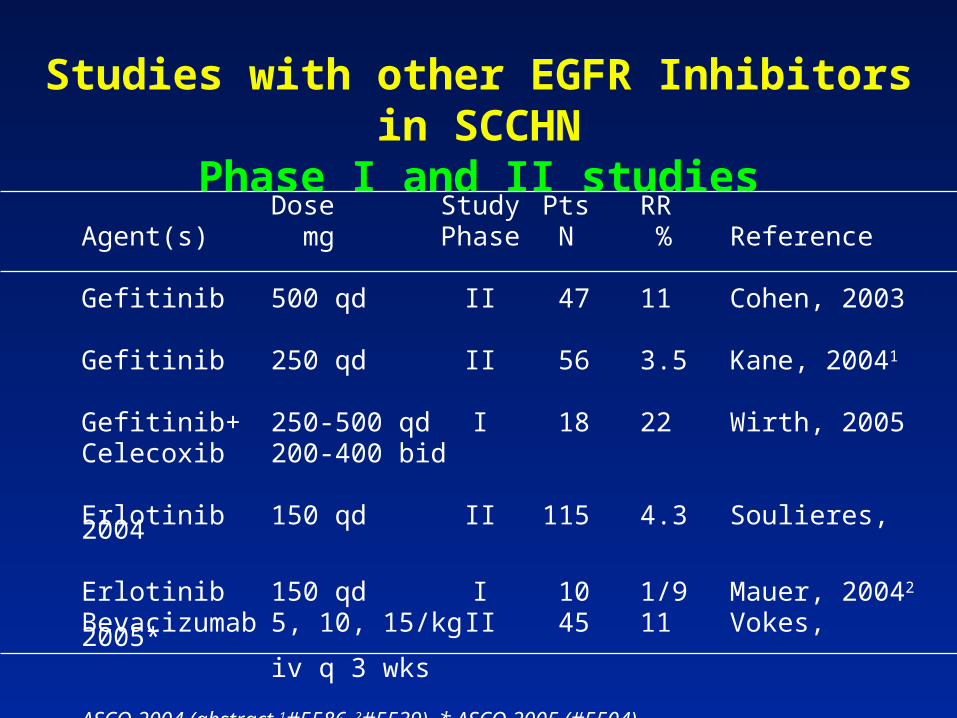
Studies with other EGFR Inhibitors in SCCHNPhase I and II studiesDose Study Pts RR
Agent(s) mg Phase N % Reference
Gefitinib 500 qd II 47 11 Cohen, 2003
Gefitinib 250 qd II 56 3.5 Kane, 20041
Gefitinib+ 250-500 qd I 18 22 Wirth, 2005Celecoxib 200-400 bid
Erlotinib 150 qd II 115 4.3 Soulieres, 2004
Erlotinib 150 qd I 10 1/9 Mauer, 20042
Bevacizumab 5, 10, 15/kg II 45 11 Vokes, 2005*iv q 3 wks
ASCO 2004 (abstract 1#5586, 2#5539), * ASCO 2005 (#5504)
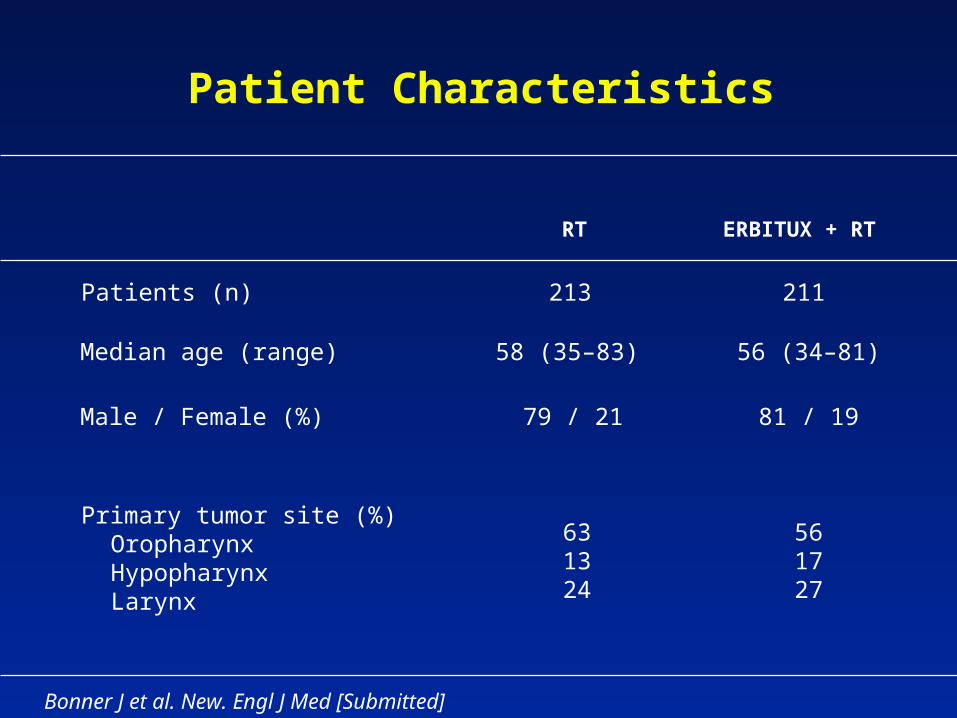
Patient Characteristics
56 (34–81)58 (35–83) Median age (range)
561727
631324
Primary tumor site (%)OropharynxHypopharynxLarynx
81 / 1979 / 21Male / Female (%)
ERBITUX + RTRT
Bonner J et al. New. Engl J Med [Submitted]
Patients (n) 213 211
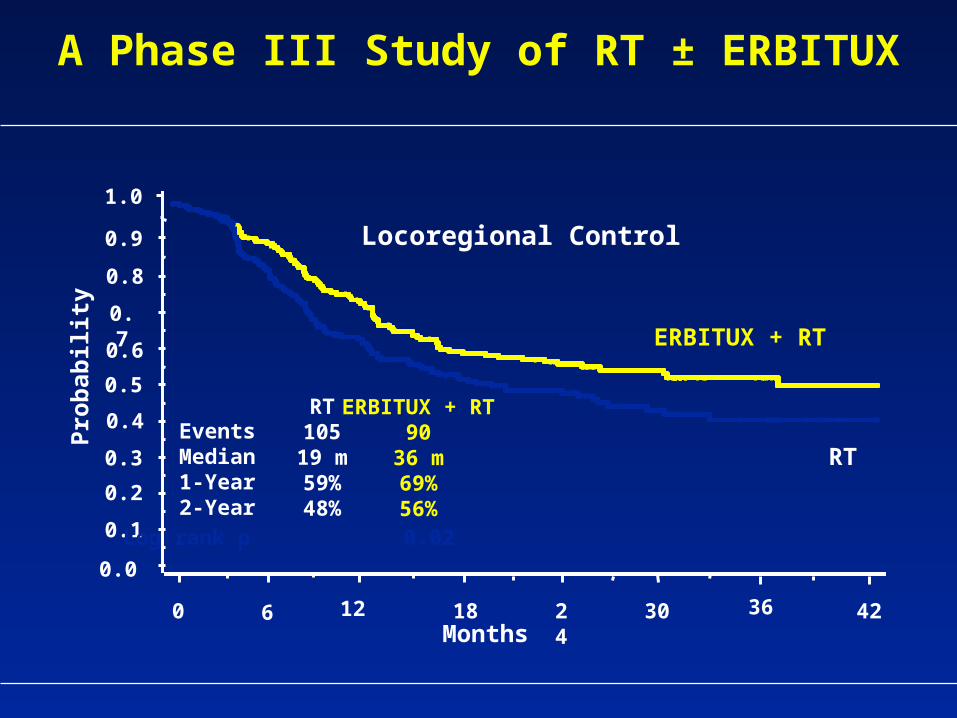
A Phase III Study of RT ± ERBITUX
1.0
0.8
0.7
0.9
0.6
0.5
0.4
0.3
0.2
0.1
0.0
Months
Locoregional Control
Pro
bab
ilit
y
ERBITUX + RT
RT
ERBITUX + RT90
36 m69%56%
RT105
19 m59%48%
EventsMedian1-Year2-Year
0 6 12 18 24 30 36 42
Log rank p 0.02
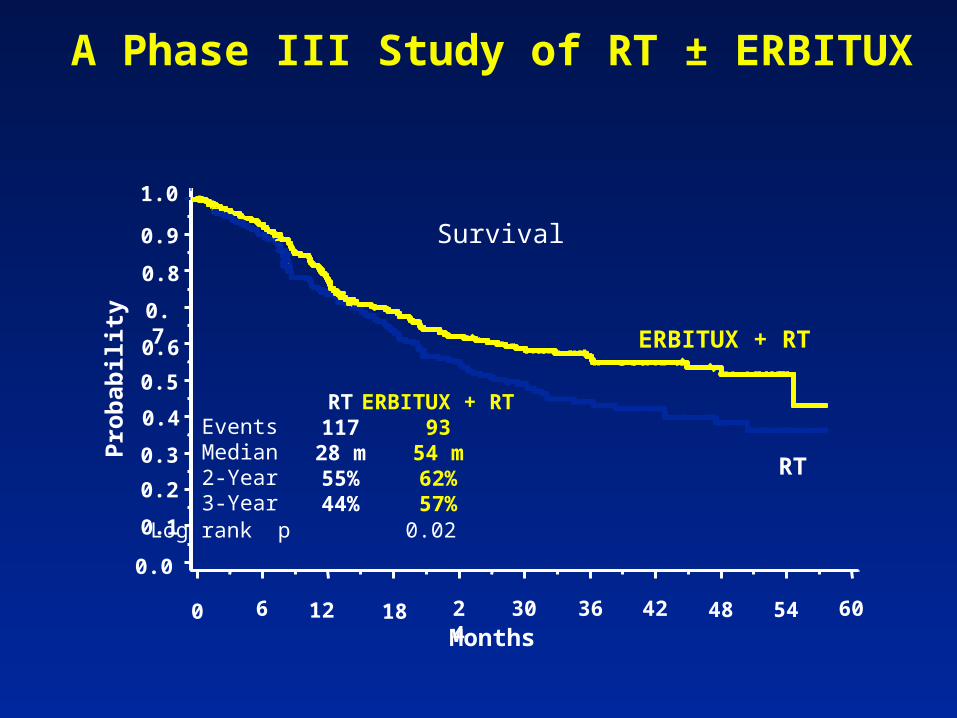
A Phase III Study of RT ± ERBITUX
Months
Pro
bab
ilit
y
1.0
0.8
0.7
0.9
0.6
0.5
0.4
0.3
0.2
0.1
0.0
Survival
ERBITUX + RT
RT
ERBITUX + RT93
54 m62%57%
RT117
28 m55%44%
EventsMedian2-Year3-Year
0 6 12 18 24 30 36 42 48 54 60
Log rank p 0.02
0 12 18
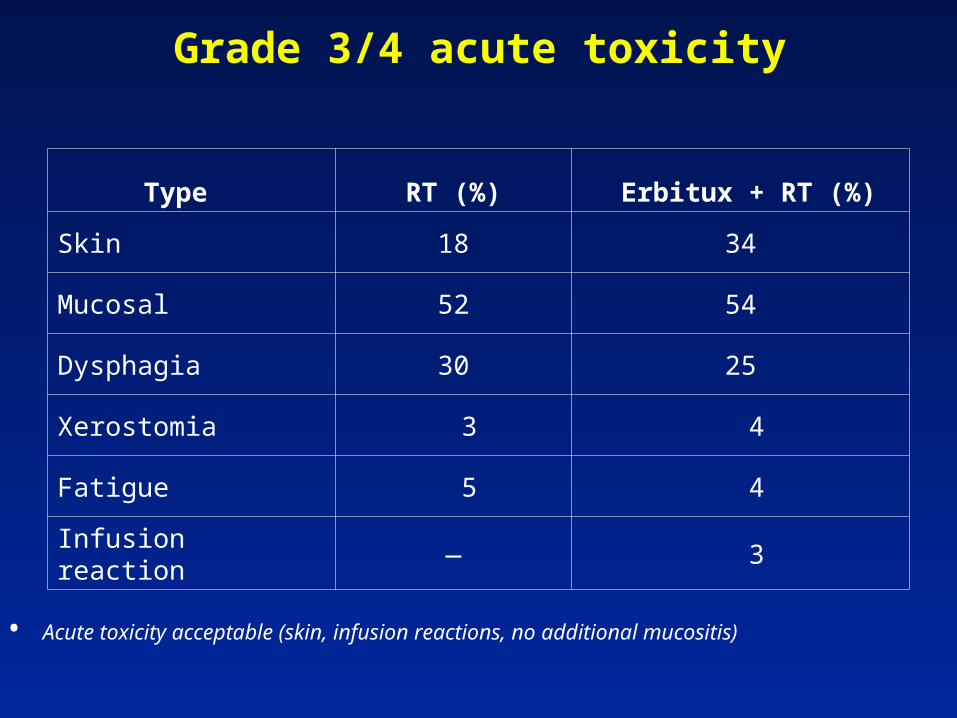
Grade 3/4 acute toxicity
Type RT (%) Erbitux + RT (%)
Skin 18 34
Mucosal 52 54
Dysphagia 30 25
Xerostomia 3 4
Fatigue 5 4
Infusion reaction — 3
• Acute toxicity acceptable (skin, infusion reactions, no additional mucositis)
Bonner J et al. New. Engl J Med [Submitted]
1.0
Pro
bab
ilit
y
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.00 6 12 18 24 30 36 42 48 54 60
Months
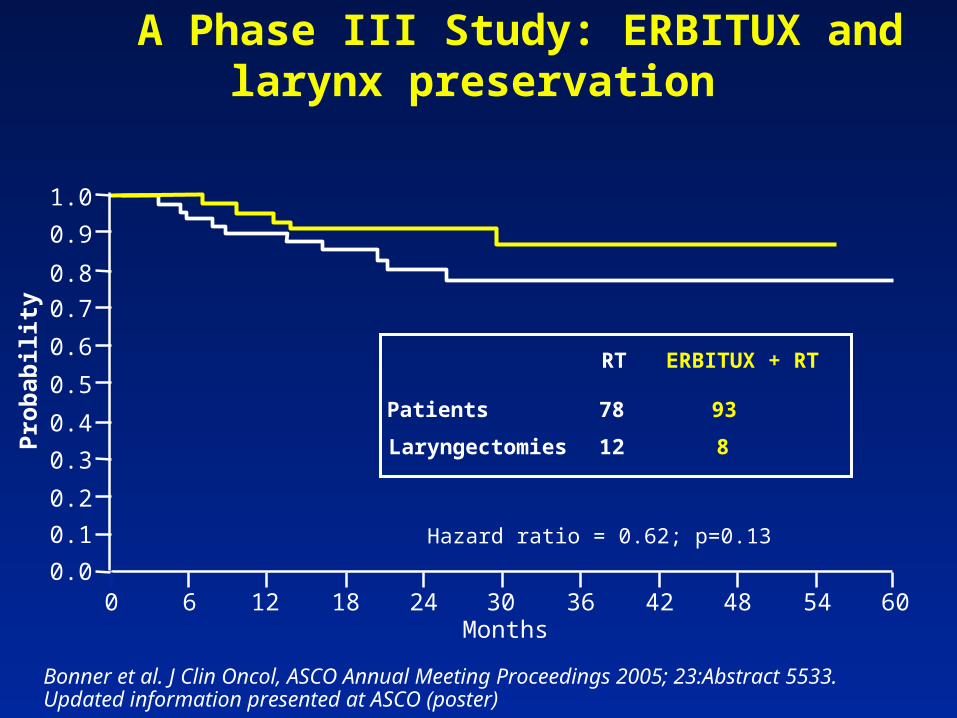
Hazard ratio = 0.62; p=0.13
Patients
Laryngectomies
78
12
RT
93
8
ERBITUX + RT
A Phase III Study: ERBITUX and larynx preservation
Bonner et al. J Clin Oncol, ASCO Annual Meeting Proceedings 2005; 23:Abstract 5533. Updated information presented at ASCO (poster)
A Phase III Study: ERBITUX and Wound Healing
• Subgroup of n=39 patients undergoing neck dissections
• No significant prolongation in key parameters in the RT alone and ERBITUX + RT groups, respectively:
– average length of hospital stay following dissection (2.1 days vs 2.8 days)
– average time until neck drain removal (3.3 days vs 3.1 days)
• ERBITUX does not significantly affect wound healing following neck dissection
Harari et al. Int J Radiat Oncol Biol Phys 2003; 57: S245-S246
Anti-EGFR Treatment in H&N CancerConclusions (1)
• Synergism with platinum compounds and RT • Survival benefit in R/M SCCHN?• Survival benefit in LA-SCCHN! (one trial)• EGFR inhibitors + RT could replace RT alone for the
treatment of intermediate risk LA-SCCHN• EGFR inhibitors + RT offers an alternative for patients
with high-risk LA-SCCHN* who are unable to tolerate concurrent CT and RT
* Stage III, IV disease, excluding T1-2N1 and T3N0
Anti-EGFR Treatment in H&N CancerConclusions (2)
Future need of clinical trials
• Chemoradiation vs EGFR inhibitors + RT• Chemoradiation + EGFR inhibitors• Induction CT CRT + EGFR inhibitors• Induction CT + EGFR inhibitors• Interaction of EGFR inhibitors – other CT agents• Interaction of EGFR inhibitors – other biologicals








![New Trends In Internal Medicine2009hocc.medicine.psu.ac.th/files/acadamic/New_Trends... · cytopenia EGF-R profile EGFR FISH EGFR FISH docetaxel gefitinib ñu EGFR FISH Lf-]utnn EGF-R](https://img.pdfslide.us/doc/110x75/60098f15be7b15544f1b652e/new-trends-in-internal-cytopenia-egf-r-profile-egfr-fish-egfr-fish-docetaxel-gefitinib.jpg)


















