Embed Size (px)
Citation preview
Targeted Cancer TherapiesBeyond PARP – Next Generation DDR Therapeutics
Safe Harbor Statement
Except for statements of historical fact, any information contained in this presentation may be a forward‐looking statement thatreflects the Company’s current views about future events and are subject to risks, uncertainties, assumptions and changes incircumstances that may cause events or the Company’s actual activities or results to differ significantly from those expressed inany forward‐looking statement. In some cases, you can identify forward‐looking statements by terminology such as “may”, “will”,“should”, “plan”, “predict”, “expect,” “estimate,” “anticipate,” “intend,” “goal,” “strategy,” “believe,” and similar expressions andvariations thereof. Forward‐looking statements may include statements regarding the Company’s business strategy, potentialgrowth opportunities, clinical development activities, the timing and results of preclinical research, clinical trials and potentialregulatory approval and commercialization of product candidates. Although the Company believes that the expectations reflectedin such forward‐looking statements are reasonable, the Company cannot guarantee future events, results, actions, levels ofactivity, performance or achievements. These forward‐looking statements are subject to a number of risks, uncertainties andassumptions, including those described under the heading “Risk Factors” in documents the Company has filed with the SEC. Theseforward‐looking statements speak only as of the date of this presentation and the Company undertakes no obligation to revise orupdate any forward‐looking statements to reflect events or circumstances after the date hereof.
Certain information contained in this presentation may be derived from information provided by industry sources. The Companybelieves such information is accurate and that the sources from which it has been obtained are reliable. However, the Companycannot guarantee the accuracy of, and has not independently verified, such information.
Trademarks:
The trademarks included herein are the property of the owners thereof and are used for reference purposes only. Such use shouldnot be construed as an endorsement of such products.
2
ProNAi Therapeutics
A clinical‐stage drug development company advancing targeted cancer therapies
NASDAQ: DNAI
Headquarters: Vancouver, BCDevelopment: San Francisco, CA
IPO: July 2015
Shares (30/9/16): 30.35M outstanding 36.98M fully diluted
Cash on hand (30/9/16): $122.7M*
3
• We are an ambitious oncology drug development company oriented to registration and commercialization.
• We have a world‐class management team with a proven track record in oncology drug development.
• We are building a broad and diverse pipeline of promising assets against emerging targets on the leading edge of cancer biology.
• Our two product candidates, PNT737 and PNT141, target the DNA Damage Response (DDR) network, a scientifically validated approach with broad potential across oncology.
• Our DDR program expands beyond PARP inhibitors, to provide for broader clinical and commercial opportunity.
*$7.0M upfront fee to CPF paid subsequent to the end of the quarter
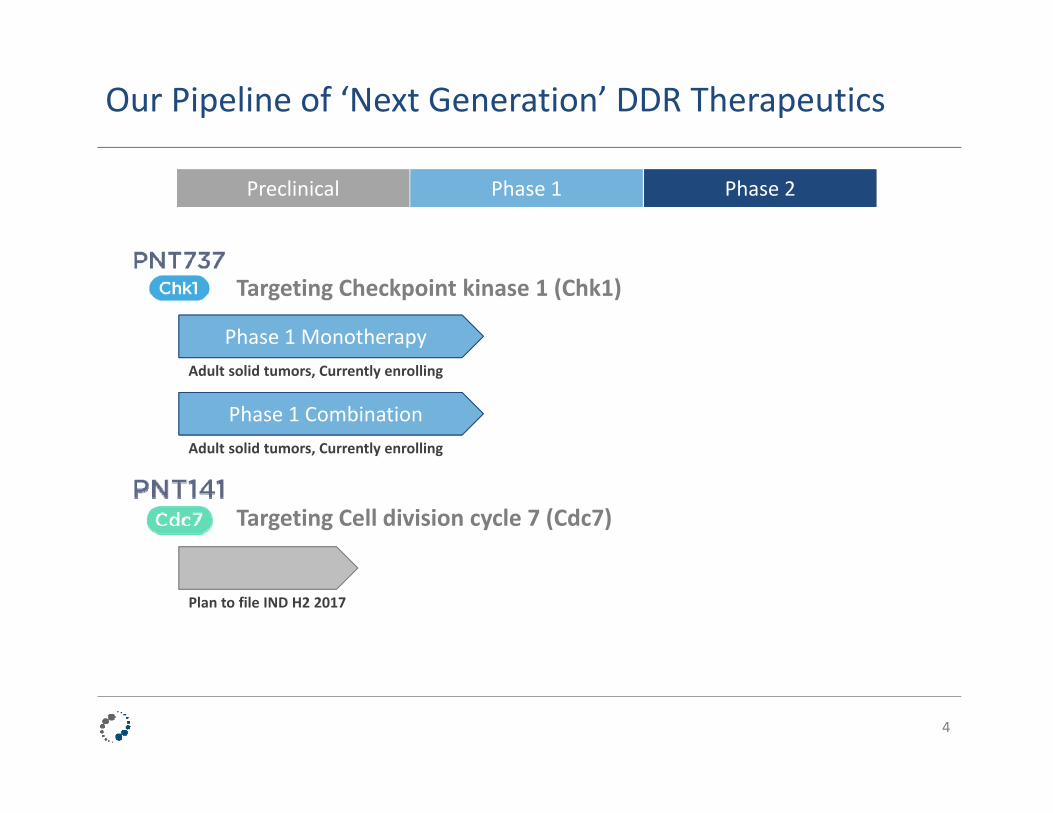
Our Pipeline of ‘Next Generation’ DDR Therapeutics
4
PreclinicalPreclinical Phase 1Phase 1 Phase 2Phase 2
Targeting Cell division cycle 7 (Cdc7)
Phase 1 MonotherapyAdult solid tumors, Currently enrolling
Phase 1 CombinationAdult solid tumors, Currently enrolling
Plan to file IND H2 2017
Targeting Checkpoint kinase 1 (Chk1)

Beyond PARP:Our DNA Damage Response (DDR) Program
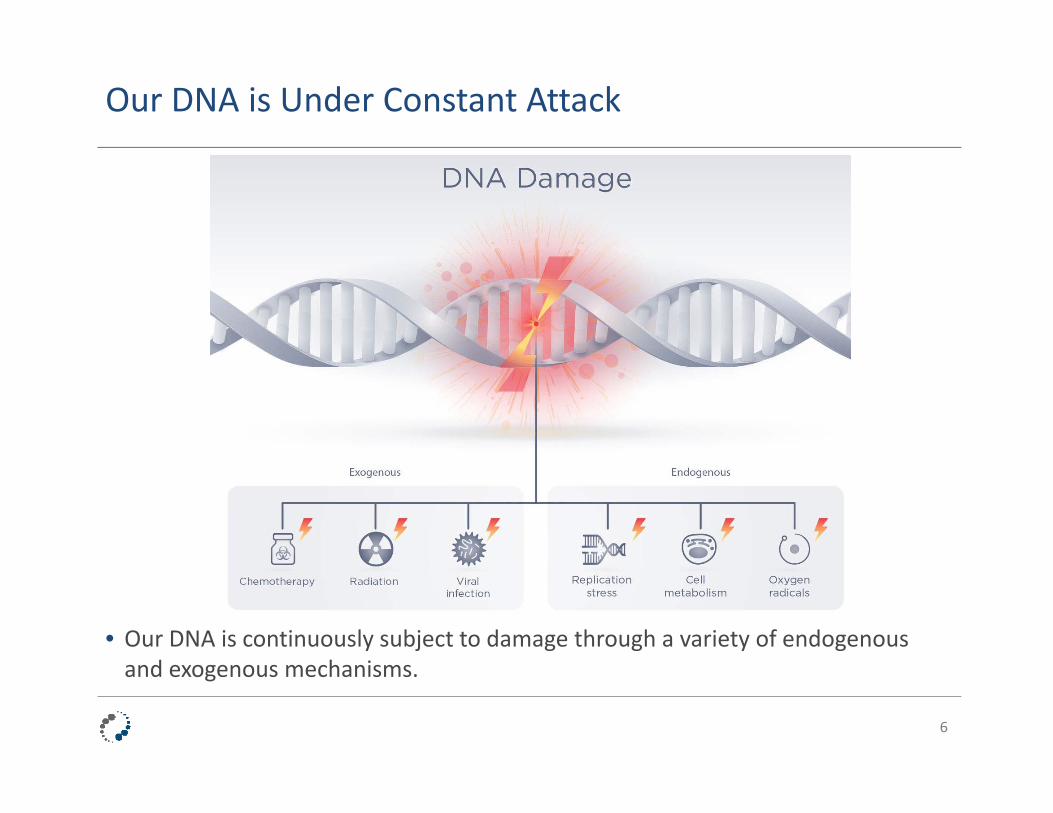
Our DNA is Under Constant Attack
• Our DNA is continuously subject to damage through a variety of endogenous and exogenous mechanisms.
6
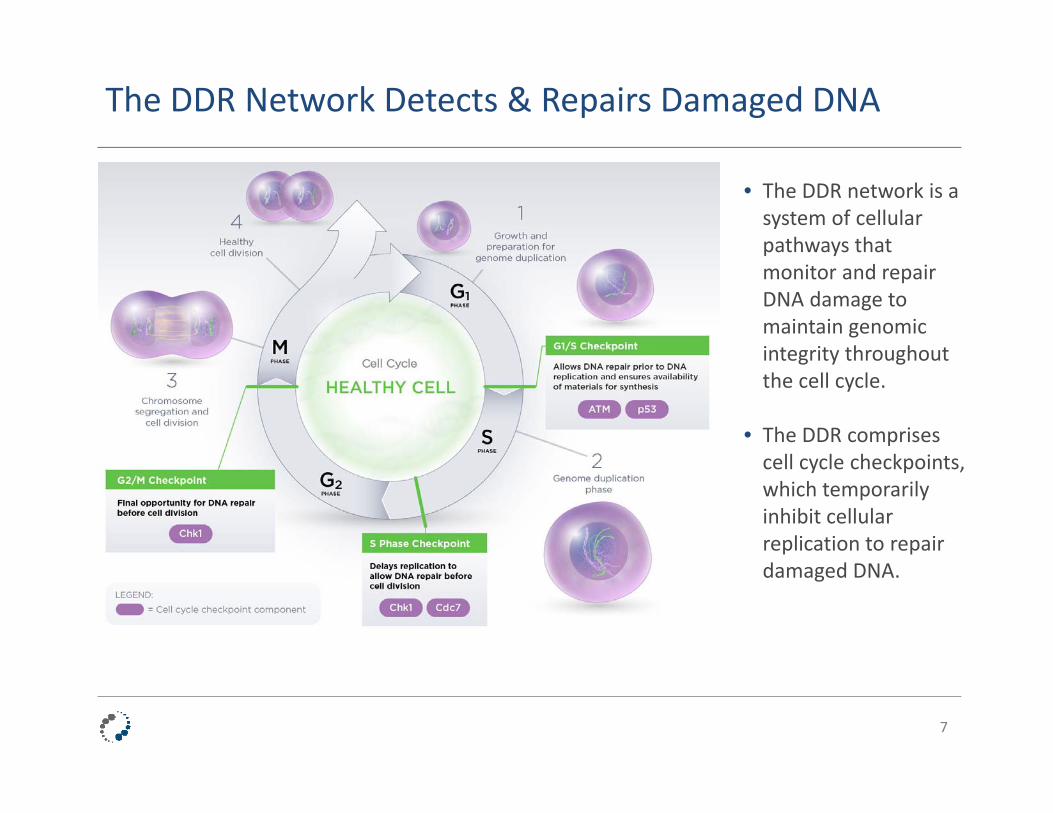
The DDR Network Detects & Repairs Damaged DNA
7
• The DDR network is a system of cellular pathways that monitor and repair DNA damage to maintain genomic integrity throughout the cell cycle.
• The DDR comprises cell cycle checkpoints, which temporarily inhibit cellular replication to repair damaged DNA.

Burgeoning Scientific Validation for Targeting DDR
8
Focus Issue: DNA Damage RepairJune 2016
June 2016

Industry Validation of DDR’s Potential in Cancer: PARP Inhibitors Lead The Way
9
May 2016
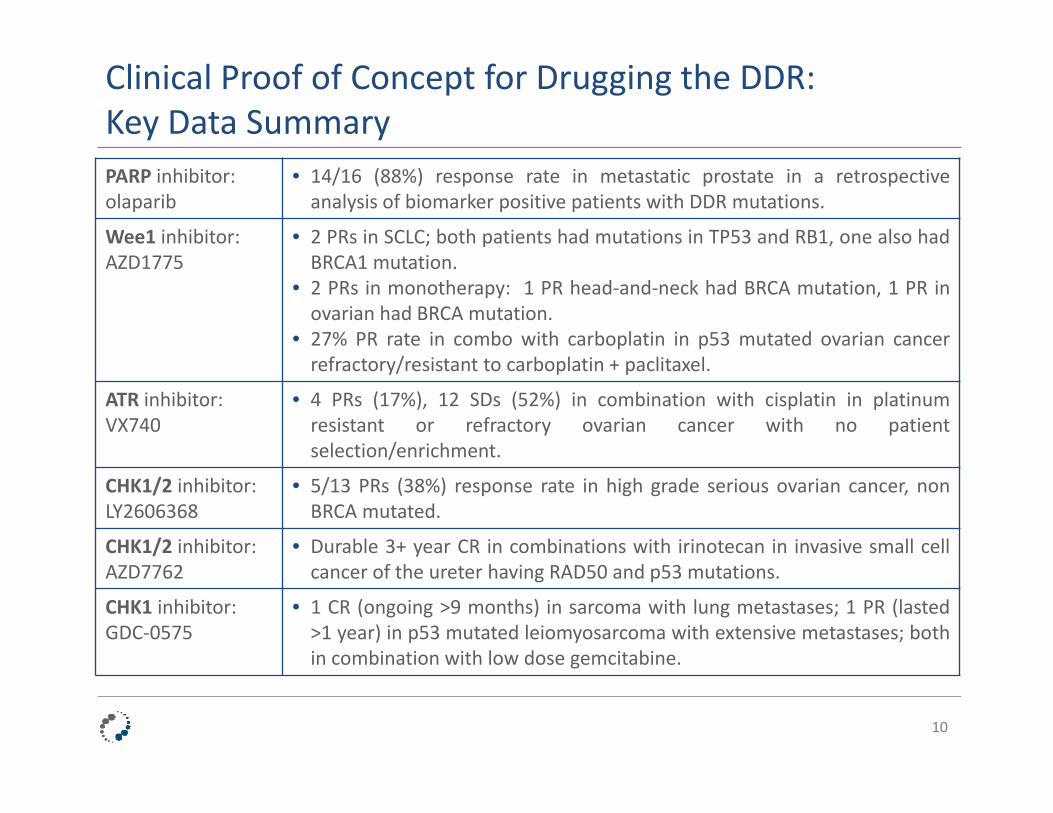
Clinical Proof of Concept for Drugging the DDR: Key Data Summary
10
PARP inhibitor: olaparib
• 14/16 (88%) response rate in metastatic prostate in a retrospectiveanalysis of biomarker positive patients with DDR mutations.
Wee1 inhibitor: AZD1775
• 2 PRs in SCLC; both patients had mutations in TP53 and RB1, one also hadBRCA1 mutation.
• 2 PRs in monotherapy: 1 PR head‐and‐neck had BRCA mutation, 1 PR inovarian had BRCA mutation.
• 27% PR rate in combo with carboplatin in p53 mutated ovarian cancerrefractory/resistant to carboplatin + paclitaxel.
ATR inhibitor:VX740
• 4 PRs (17%), 12 SDs (52%) in combination with cisplatin in platinumresistant or refractory ovarian cancer with no patientselection/enrichment.
CHK1/2 inhibitor: LY2606368
• 5/13 PRs (38%) response rate in high grade serious ovarian cancer, nonBRCA mutated.
CHK1/2 inhibitor: AZD7762
• Durable 3+ year CR in combinations with irinotecan in invasive small cellcancer of the ureter having RAD50 and p53 mutations.
CHK1 inhibitor: GDC‐0575
• 1 CR (ongoing >9 months) in sarcoma with lung metastases; 1 PR (lasted>1 year) in p53 mutated leiomyosarcoma with extensive metastases; bothin combination with low dose gemcitabine.

ProNAi’s DDR Program: Expanding Beyond PARP
11
• PARP inhibitors are intended to prevent the repair of DNA single strand breaks.
• Our DDR program expands beyond the scope of PARP inhibitors.
• We focus on impeding the repair of DNA double strand breaks, the most deleterious form of DNA damage, as well as by striking at targets that control DNA replication and cell cycle progression.

Cancer’s Genomic Instability:Over‐Reliance on Key Cell Cycle Checkpoints
12
• Replication stress induced by oncogenic drivers (e.g. MYC and RAS) combined with loss of function in tumor suppressors (e.g. p53 and ATM) results in persistent DNA damage and genomic instability.
• Cancer cells tolerate genomic instability and elevated DNA damage via an over‐reliance on checkpoints such as Chk1 and Cdc7.
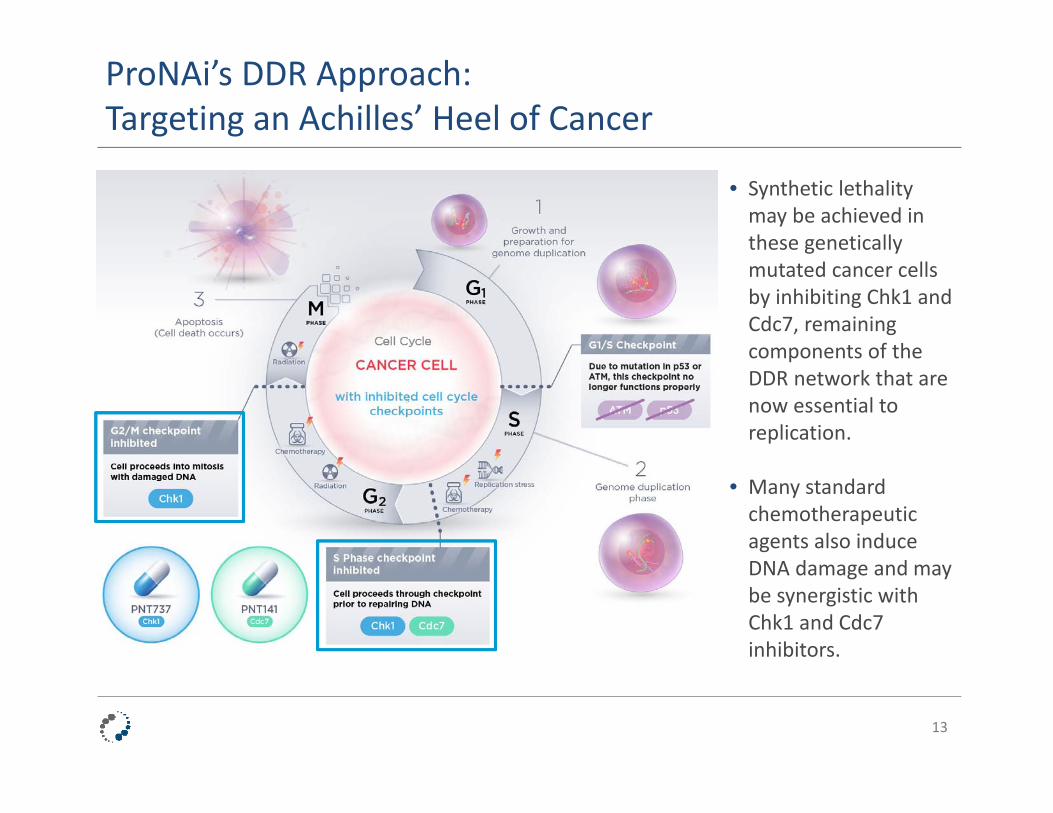
ProNAi’s DDR Approach: Targeting an Achilles’ Heel of Cancer
13
• Synthetic lethality may be achieved in these genetically mutated cancer cells by inhibiting Chk1 and Cdc7, remaining components of the DDR network that are now essential to replication.
• Many standard chemotherapeutic agents also induce DNA damage and may be synergistic with Chk1 and Cdc7 inhibitors.
Our Next Generation DDR Portfolio: PNT737 & PNT141
14
• Highly‐selective small molecule inhibitor of the serine‐threonine kinase Checkpoint kinase 1 (Chk1).
• Chk1 is a central regulator of the DDR network and of multiple cell cycle checkpoints.
• Oral bioavailability of PNT737 affords greater flexibility in dosing strategies compared to IV agents.
• Currently in two Phase 1 clinical trials in patients with advanced cancer.
• Highly‐selective small molecule inhibitor of the serine‐threonine kinase Cell division cycle 7 (Cdc7).
• Cdc7 is a key regulator of DNA replication and the DDR network.
• Broad development scope in solid and liquid tumors.
• Mono‐ and combo‐ therapy development potential.
• Clinical studies expected to begin by the end of 2017.
Our DDR Program: Significant Potential in Oncology
15
ChemotherapyCombinations with DNA damaging chemotherapy
DDR CombinationsSynergy with other DDR targeting agents to maximize DNA
damage
RadiotherapySensitize to ionizing radiation
Immuno‐OncologyDDR targeting agents coupled
with immune activation
DDR MonotherapyExploit replicative stress and genetic instability for
synthetic lethality

PNT737 Targeting Chk1

PNT737: Best‐In‐Class Pedigree
17
Discovered and initially developed by scientists at: • The Cancer Research UK Cancer
Therapeutics Unit at The Institute of Cancer Research (ICR)
• Sareum Holdings
Clinical development currently taking place in facilities funded by:• Cancer Research UK (CRUK)• The National Institute for Health
Research (NIHR) Biomedical Research Centre (BRC) at The Royal Marsden and ICR
• The Experimental Cancer Medicine Centre Network
Biomedical Research Centreat The Royal Marsden NHS Foundation Trustand The Institute of Cancer Research, London

PNT737: Best‐In‐Class Characteristics
Criterion PNT737 LY2606368
Presentation: Oral i.v.
Biochemical IC50: Chk1 1.4 nM ~1 nM
Biochemical IC50: Chk2 1850 nM 8 nM
Selectivity: Chk1 vs. Chk2 1320x ~10x
18
10 mg/kg in BALB/c mice
• PNT737 is orally bioavailable, potent, and highly selective for Chk1 over Chk2.
• PNT737 has an excellent PK profile, and demonstrates robust efficacy in numerous in vivo cancer models as a single agent and in combination.
HT29 CRC
• PNT737 selectivity: 15/124 kinases at 10 µMERK8 = 100x All other kinases >200xCDK2 = 2750xCDK1 = 6750x
Cmin
PNT737 Targets Chk1 – A Critical DDR Component
19
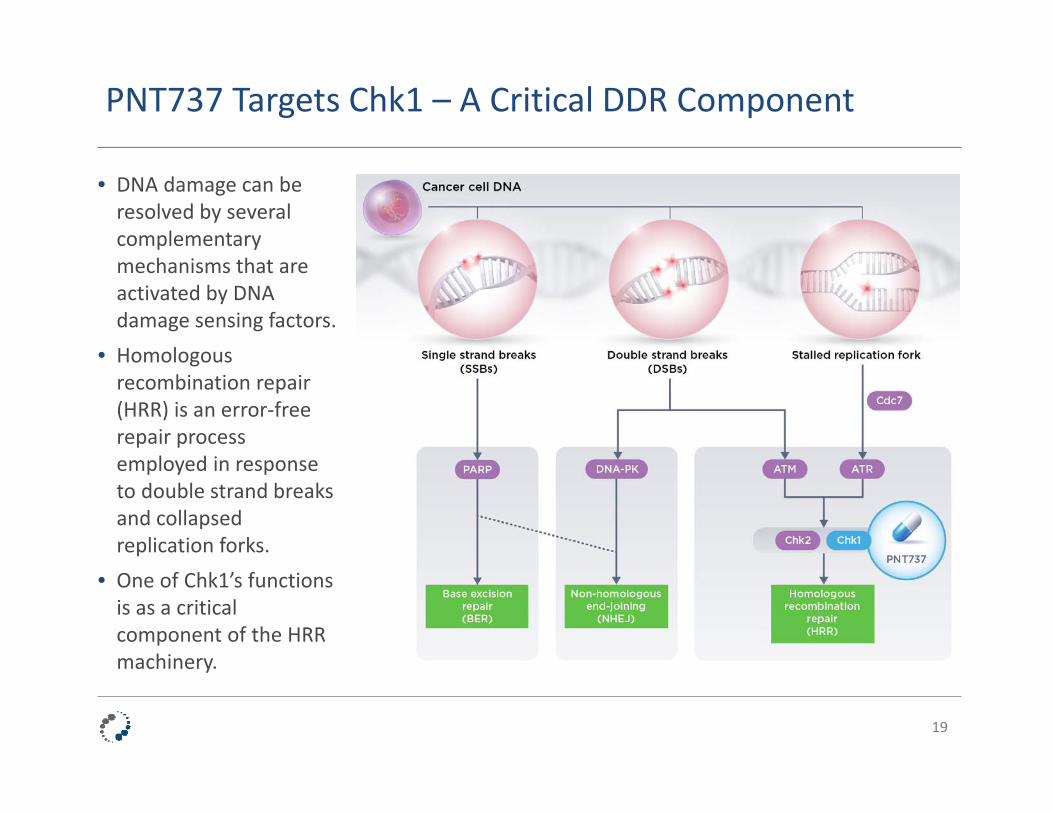
• DNA damage can be resolved by several complementary mechanisms that are activated by DNA damage sensing factors.
• Homologous recombination repair (HRR) is an error‐free repair process employed in response to double strand breaks and collapsed replication forks.
• One of Chk1’s functions is as a critical component of the HRR machinery.
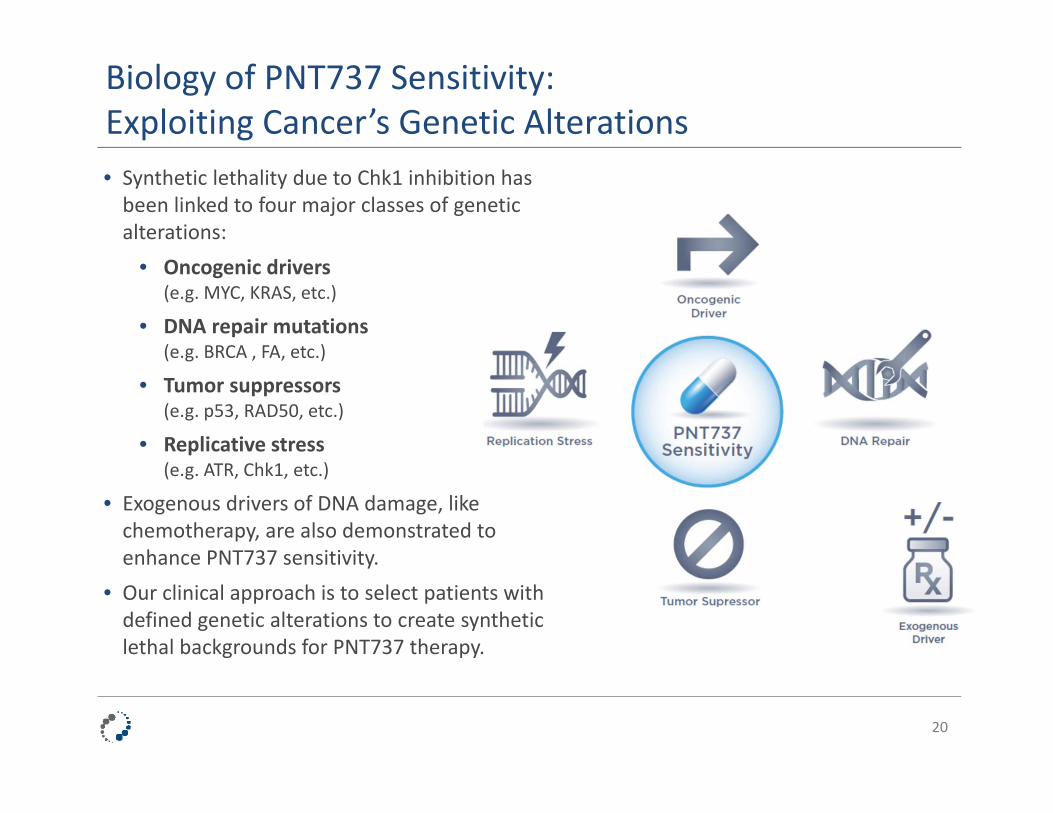
Biology of PNT737 Sensitivity:Exploiting Cancer’s Genetic Alterations • Synthetic lethality due to Chk1 inhibition has been linked to four major classes of genetic alterations:
• Oncogenic drivers (e.g. MYC, KRAS, etc.)
• DNA repair mutations (e.g. BRCA , FA, etc.)
• Tumor suppressors (e.g. p53, RAD50, etc.)
• Replicative stress(e.g. ATR, Chk1, etc.)
• Exogenous drivers of DNA damage, like chemotherapy, are also demonstrated to enhance PNT737 sensitivity.
• Our clinical approach is to select patients with defined genetic alterations to create synthetic lethal backgrounds for PNT737 therapy.
20
Optimize Sensitivity to PNT737 in the Clinic
21
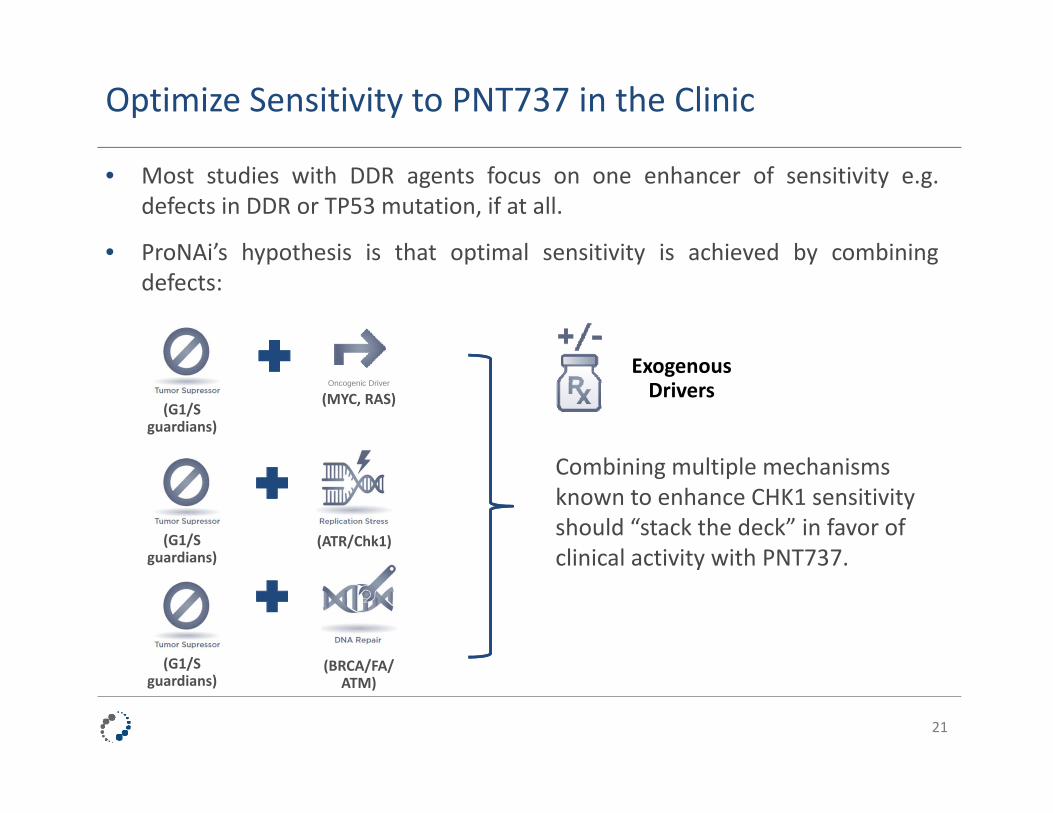
• Most studies with DDR agents focus on one enhancer of sensitivity e.g.defects in DDR or TP53 mutation, if at all.
• ProNAi’s hypothesis is that optimal sensitivity is achieved by combiningdefects:
Combining multiple mechanisms known to enhance CHK1 sensitivity should “stack the deck” in favor of clinical activity with PNT737.
(G1/S guardians)
(BRCA/FA/ATM)
Oncogenic Driver
(MYC, RAS)
(ATR/Chk1)
(G1/S guardians)
(G1/S guardians)
Exogenous Drivers

Genomic Alterations Differ Across Indications: ‘Right Genetics In The Right Patients’
22
• Mutational frequencies (oncogenic drivers; replications stress; DNA repair; tumorsuppressors) differ across indications.
• Certain indications harbor significant genomic instability, and are promising targetindications for therapeutic intervention with PNT737.
• ProNAi’s clinical development strategy ‐ genetically‐defined patient selection inindications predicted to be sensitive to PNT737 inhibition.
Red = most frequently mutated; Green = least frequently mutated
Bladder6 5 10 10
Squamous NSCLC5 10 7 8
Ovarian Cancer9 9 5 6
Prostate7 7 9 5
Lung Adenocarcinoma8 6 6 4
Head & Neck2 8 4 9
Pancreatic10 1 2 7
Cholangiocarcinoma3 1 8 2
Invasive Breast4 4 3 3
AML1 1 1 1

PNT737: Overall Development Strategy
23
I/O Combo
ChemotherapyGemcitabine and Gemcitabine/Cisplatin combinations exploit known potentiatingeffects of Chk1i.
Chk1i + PARPi might expand/enhance PARPisensitivity.
PD‐1/PDL‐1 combination marries known drivers of neoantigen presentation in “double checkpoint” strategy.
MonotherapyExploit synthetic lethality in genetically‐defined populations with predicted high sensitivity to PNT737.
PARP Combo
Potential Clinical Opportunities
Current Clinical Trials
Pre‐clinically, Chk1i + Cdc7i combination is extremely synergistic. Cdc7 Combo

Two Clinical Trials Initiated at Royal Marsden, UK Current Study Designs
• Being conducted at three sites in the UK:• Dr. Udai Banerji (Chief Investigator) – ICR / The Royal Marsden• Dr. Ruth Plummer – Newcastle University• Dr. Robert Jones – Cardiff University
• Design: Dose escalation design to establish the recommenced Phase 2 dose for further evaluation. Expansion cohorts to evaluate promising patient populations. Possibility to define additional genetically‐selected cohorts.
• Primary outcome measures: Safety and tolerability, drug‐related dose limiting toxicity.
A Phase I Trial of CCT245737 (PNT737) in Patients with Advanced CancerClinicalTrials.gov Identifier: NCT02797964
Estimated Enrollment: 40 patients• Advanced Solid Tumors
A Phase I Trial of CCT245737 (PNT737) in Combination with Gemcitabine Plus Cisplatin or Gemcitabine Alone in Patients with Advanced CancerClinicalTrials.gov Identifier: NCT02797977
Estimated enrollment: 70 patients• Advanced Solid Tumors• Non‐small Cell Lung Cancer expansion• Pancreatic Cancer expansion

PNT737: Monotherapy Clinical Development –Exploiting Synthetic Lethality
25
• Inhibition of Chk1 by PNT737 may be synthetically lethal to cancer cells harboring genetic mutations in genes such as MYC, RAS, ATR, ATM and p53.
• Clinical opportunities include:
• DLBCL: ~20% MYC• Prostate: ~20% MYC• Ovarian: ~40% MYC• TNBC: ~30% BRCA1/2• SCCHN: ~10% ATR
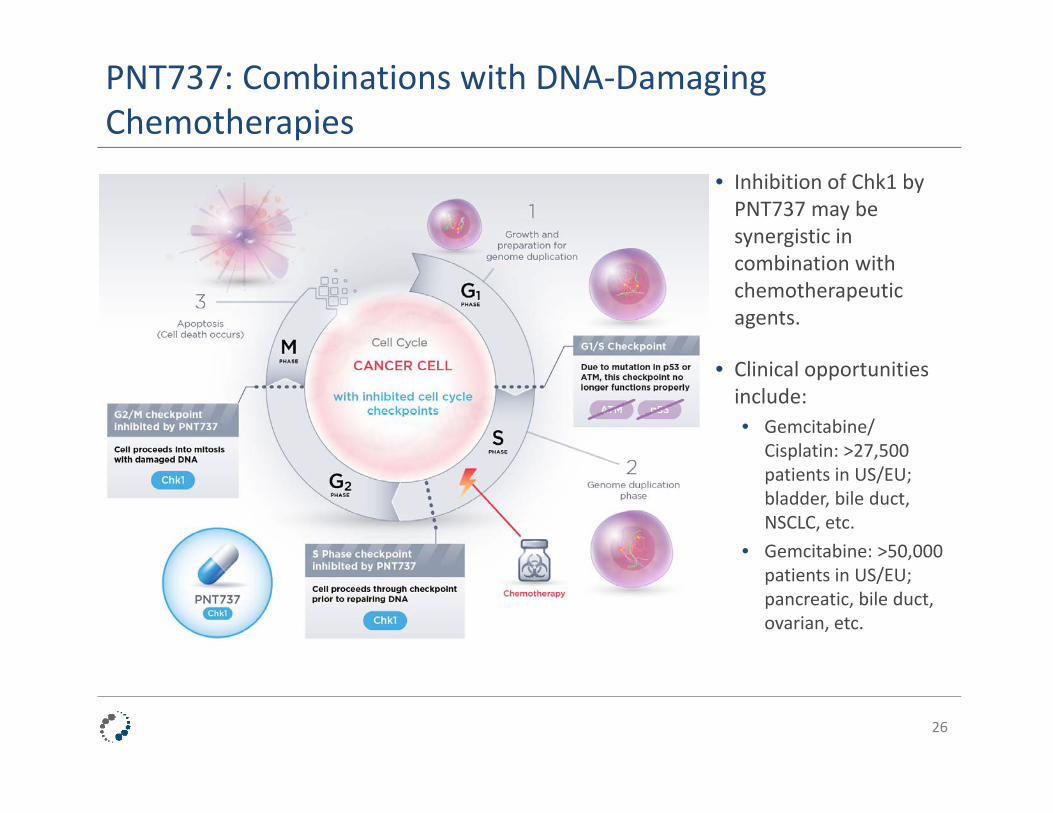
PNT737: Combinations with DNA‐Damaging Chemotherapies
26
• Inhibition of Chk1 by PNT737 may be synergistic in combination with chemotherapeutic agents.
• Clinical opportunities include:• Gemcitabine/
Cisplatin: >27,500 patients in US/EU; bladder, bile duct, NSCLC, etc.
• Gemcitabine: >50,000 patients in US/EU; pancreatic, bile duct, ovarian, etc.
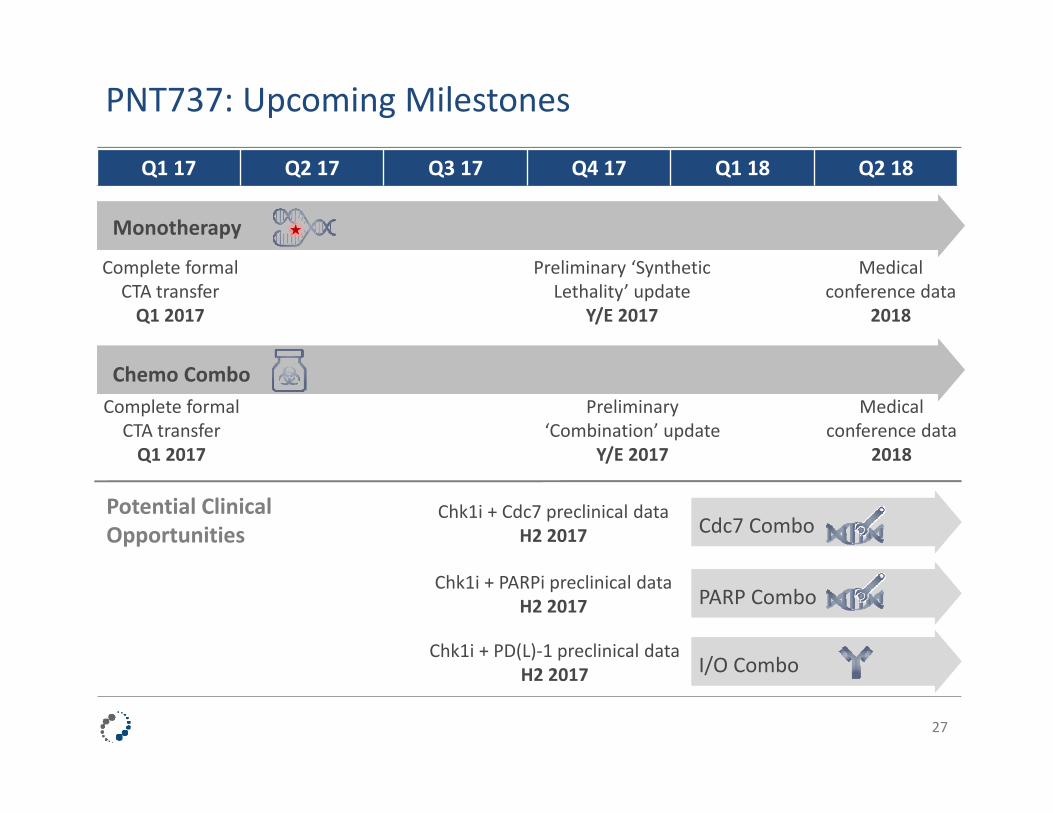
PNT737: Upcoming Milestones
27
Medical conference data
2018
Complete formal CTA transferQ1 2017
Preliminary ‘Synthetic Lethality’ update
Y/E 2017
Medical conference data
2018
Complete formal CTA transferQ1 2017
Preliminary ‘Combination’ update
Y/E 2017
Chk1i + PARPi preclinical dataH2 2017
Chk1i + PD(L)‐1 preclinical dataH2 2017
Chk1i + Cdc7 preclinical dataH2 2017
Q1 17 Q2 17 Q3 17 Q4 17 Q1 18 Q2 18
Monotherapy
Chemo Combo
Cdc7 Combo
PARP Combo
I/O Combo
Potential Clinical Opportunities

PNT141 Targeting Cdc7
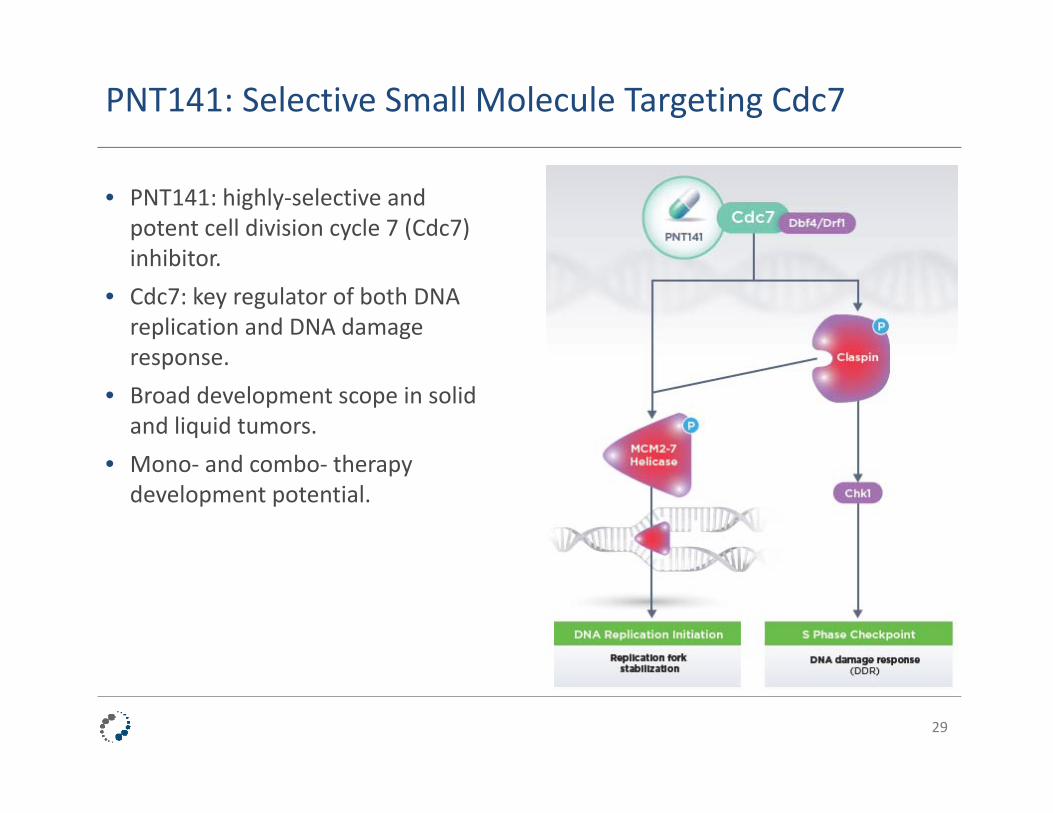
PNT141: Selective Small Molecule Targeting Cdc7
29
• PNT141: highly‐selective and potent cell division cycle 7 (Cdc7) inhibitor.
• Cdc7: key regulator of both DNA replication and DNA damage response.
• Broad development scope in solid and liquid tumors.
• Mono‐ and combo‐ therapy development potential.
Cdc7: Key Function in the DDR Network
30
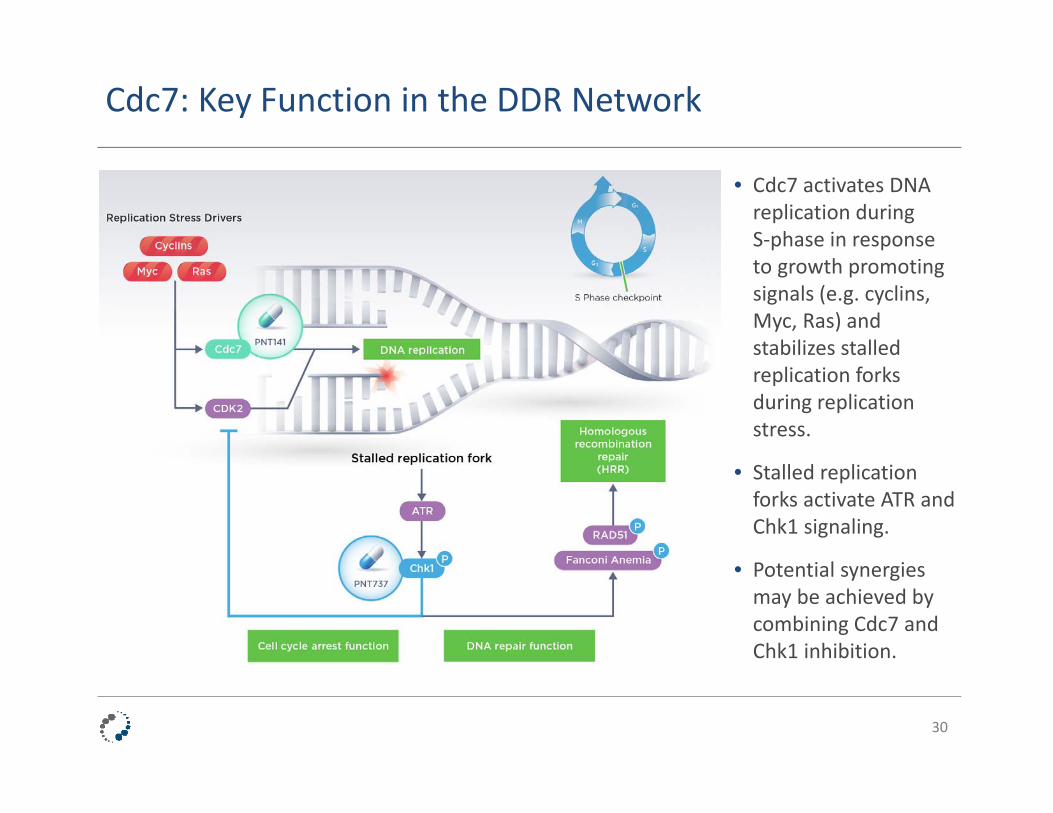
• Cdc7 activates DNA replication during S‐phase in response to growth promoting signals (e.g. cyclins, Myc, Ras) and stabilizes stalled replication forks during replication stress.
• Stalled replication forks activate ATR and Chk1 signaling.
• Potential synergies may be achieved by combining Cdc7 and Chk1 inhibition.
PNT141: First‐In‐Class/Best‐In‐Class Opportunity
• Preclinical data and published literature suggest a variety of indications with potential for response to Cdc7 inhibitors:
– Solid tumors: breast, ovarian, pancreatic, melanoma, colorectal, uterine, thyroid, etc.
– Hematological malignancies: AML, DLBCL, etc.
• PNT141’s selectivity profile offers possible differentiation and potential safety and efficacy advantages.
• A biomarker‐driven patient selection strategy focusing on drivers of replication stress, genomic instability and proliferation (e.g. p53, BRCA, MYC, KRAS, etc.) may help facilitate clinical trial execution.
• Clinical studies expected to begin by the end of 2017.
31
Advancing Targeted Cancer Therapies

Proven Leadership in Oncology Development
Nick Glover, PhDPresident and CEO
Barbara Klencke, MDChief Development Officer
Angie You, PhDChief Business & Strategy Officer and Head of Commercial
Sukhi Jagpal, CA, CBV, MBAChief Financial Officer
33
Keith Anderson, PhDSenior Vice President, Technical Operations
Wendy ChapmanSenior Vice President, Clinical Operations
Diane GardinerSenior Vice President, Human Resources and Administration
Christian Hassig, PhDSenior Vice President, Research
Chandra LovejoySenior Vice President, Global Regulatory Affairs and Head of Quality
Emma McCannSenior Vice President, Program Management
Gregg Smith, PhD, MBASenior Vice President, Preclinical

Our DDR Program Expands Beyond PARP
We have established a promising portfolio of DDR assets:
• PNT737 and PNT141 target the DNA Damage Response network, a promising approach to treating cancer based on leading‐edge discoveries in cancer biology.
• Our DDR program expands beyond the scope of PARP inhibitors by focusing on double strand breaks, DNA replication, genomic instability and cell cycle checkpoints.
• Our near‐term development plans for PNT737 and PNT141 encompass synthetic lethality strategies as monotherapy, and in combination with DNA‐damaging chemotherapy. Two Phase 1 clinical trials with PNT737 underway; preliminary update Y/E 2017.
• In addition, we plan to explore the potential synergy of combining PNT737 and PNT141 in a proprietary combination.
• Beyond this initial focus, these assets could be combined with other DDR agents (e.g. +PARPi), and in combinations with immuno‐oncology.
34
Targeted Cancer Therapieswww.pronai.com





























