Embed Size (px)
Citation preview
The Prostate l2:173-177 (1988)
Tamoxifen in Advanced Prostate Cancer: An ECOG Pilot Study John Horton, Charles Rosenbaum, and Frank J. Cummings
Albany Medical College, Albany, New York (J. H.), Tuits University, Walpole, Massachusetts (C. R.), and Brown University and Roger Williams General Hospital, Providence, Rhode Island (F. J. C.)
A group of 19 patients with advanced (Stage D) prostate cancer were treated with one of three dose levels of the anti-estrogen tamoxifen, 10 mg (3 patients), 20 mg (8 patients), or 30 mg (8 patients) daily. Five patients had received no prior systemic therapy. The treatment was tolerated well, but no objective responses occurred.
Key words: tamoden, prostate cancer
INTRODUCTION
Tamoxifen is a non-steroidal synthetic anti-estrogen that is clinically effective in patients with hormone sensitive advanced breast cancer [l], and when used as an adjuvant to local treatment of stages 1 and 2 breast cancer [2]. Advanced prostate cancer is a hormonally dependent disease, with responses occurring following orchiectomy, estrogen therapy, and with total androgen blockage. Prostate tissue has been demonstrated to contain estrogen receptors as well as androgen receptors [3]. Since tamoxifen is usually well tolerated, we decided to test whether responses would occur from three different dose levels of tamoxifen in a group of patients with advanced prostate cancer.
METHODS AND RESULTS
Eligible patients for study had biopsy proven recurrent, advanced or metastatic carcinoma of the prostate not amenable to curative surgery or radiation (Stage D). Evaluable aspects of the tumor, including elevated serum acid phosphatase, progres- sive osteoblastic bone metastases, or soft tissue tumors were required. Patients who had received any antiestrogens, had an ECOG performance status of 4, an active second malignancy, platelets <50,000/m3 or WBC <2,500/mm3 were excluded. Dose levels of orally administered tamoxifen were 10 mg daily (3 patients), 10 mg b.i.d. (8 patients), and 10 mg t.i.d. (8 patients). The dosage levels were escalated sequentially in groups. All patients gave written informed consent for study.
Received June 29, 1987; accepted November 30, 1987.
Address reprint requests to Dr. John Horton, Albany Medical College, Division of Oncology, Albany, NY 12208.
0 1988 Alan R. Liss, Inc.
TA
BL
E I.
Ind
ivid
ual C
hara
cter
istic
s of
Pat
ient
s T
reat
ed w
ith T
amox
ifen
Tim
e “8 f
Prio
r The
rapy
* D
aily
on
RT
RT
do
se
stud
y su
rviv
al
1 Pa
tient
A
ge
PS
Orc
hiec
tom
y Es
troge
n (lo
cal)
(met
s)
Che
mo
(mg)
(mos
) (m
onth
s)
Com
men
ts
AD
75
1
X X
10
16
18
AT
71
1 X
X
10
2
3 M
V
59
1 X
10
3 10
BW
75
1
X
X X
20
1 11
TC
73
0
X X
20
un
know
n 1.
5 N
o FU
for
resp
onse
JT
6
01
X
X X
20
3 10
AV
66
0
X X
20
6 6
RK
76
2 X
X
X
20
2 7
JO
90
2 20
1
1 A
B
55
I X
20
un
know
n 17
N
o FU fo
r res
pons
e SM
74
2
X X
20
3 4
cc
57
2 X
X
X
30
1 8
AG
79
2
X X
30
1
3 LD
a3
0
30
8 BJ
78
I
30
I 24
PN
74
1
X
30
5 16
D
A
60
0
X 30
3
60
No
mea
s. di
seas
e FI
73
1 X
30
1 18
A
P 59
0
30
7 54
.. g a I un
know
n
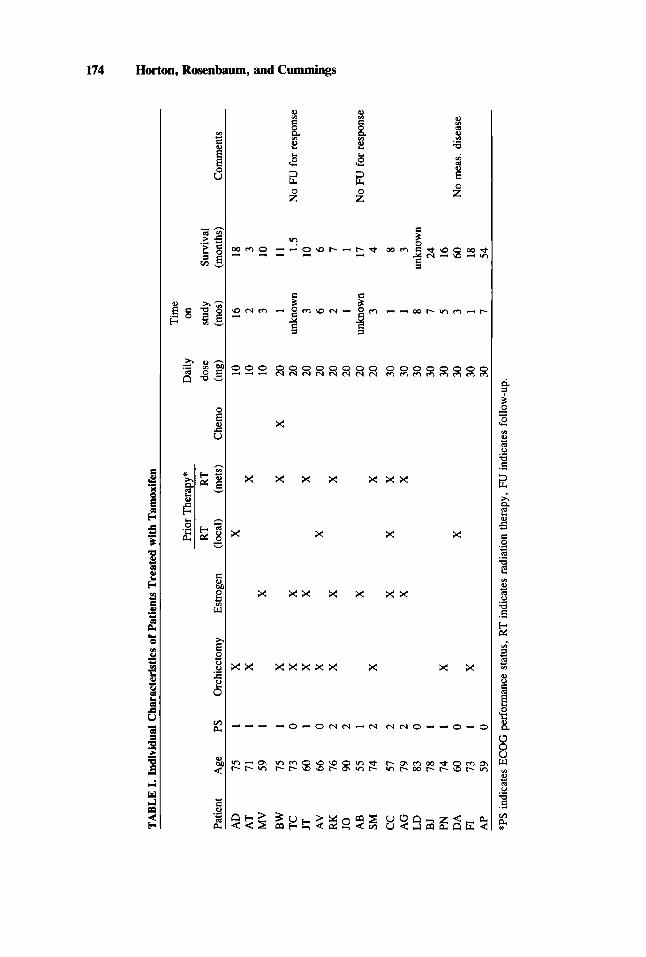
*PS
indi
cate
s EC
OG
per
form
ance
sta
tus,
RT
indi
cate
s ra
diat
ion
ther
apy,
FU
indi
cate
s fo
llow
-up.
Tamoxifen in Advanced Prostate Cancer 175
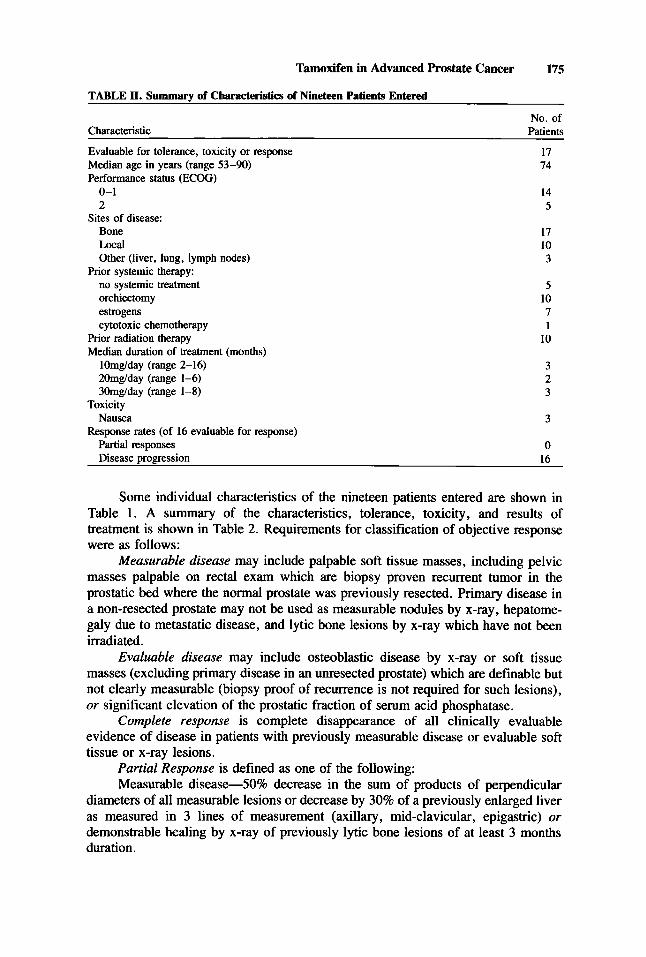
TABLE 11. Summary of Characteristics of Nineteen Patients Entered
No. of Characteristic Patients
Evaluable for tolerance, toxicity or response
Performance status (ECOG)
17 74
0-1 14 2 5
Bone 17 Local 10 Other (liver, lung, lymph nodes) 3
no systemic treatment 5 orchiectomy 10 estrogens 7 cytotoxic chemotherapy 1
Prior radiation therapy 10
lOmg/day (range 2-16) 3 20mg/day (range 1-6) 2 3Omg/day (range 1-8) 3
Nausea 3
Partial responses 0
Median age in years (range 53-90)
Sites of disease:
Prior systemic therapy:
Median duration of treatment (months)
Toxicity
Response rates (of 16 evaluable for response)
Disease progression 16
Some individual characteristics of the nineteen patients entered are shown in Table 1. A summary of the characteristics, tolerance, toxicity, and results of treatment is shown in Table 2. Requirements for classification of objective response were as follows:
Measurable disease may include palpable soft tissue masses, including pelvic masses palpable on rectal exam which are biopsy proven recurrent tumor in the prostatic bed where the normal prostate was previously resected. Primary disease in a non-resected prostate may not be used as measurable nodules by x-ray, hepatome- galy due to metastatic disease, and lytic bone lesions by x-ray which have not been irradiated.
Evaluable disease may include osteoblastic disease by x-ray or soft tissue masses (excluding primary disease in an unresected prostate) which are definable but not clearly measurable (biopsy proof of recurrence is not required for such lesions), or significant elevation of the prostatic fraction of serum acid phosphatase.
Complete response is complete disappearance of all clinically evaluable evidence of disease in patients with previously measurable disease or evaluable soft tissue or x-ray lesions.
Partial Response is defined as one of the following: Measurable disease-50% decrease in the sum of products of perpendicular
diameters of all measurable lesions or decrease by 30% of a previously enlarged liver as measured in 3 lines of measurement (axillary, mid-clavicular, epigastric) or demonstrable healing by x-ray of previously lytic bone lesions of at least 3 months duration.
176 Horton, Rosenbaum, and Cummings
Evaluable disease-clinically significant (> 50%) decrease in evaluable non- measurable soft tissue lesions which is accompanied by relief of previously documented symptoms clearly secondary to disease or stabilization of previously progressing osteoblastic bone metastasis by x-ray which is accompanied by relief of previously documented bone pain or other symptoms clearly secondary to disease, or > 50% decrease in previously elevated acid phosphatase which is accompanied by a response of either osteoblastic or evaluable soft-tissue with or without symptomatic change.
Biochemical response-> 50% decrease in previously elevated level of prostatic fraction of acid phosphatase which persists for 12 wk without other evidence of objective response or progression.
Stable disease-< 50% decrease or less than 25% increase in all parameters of measurable disease; or relief of previously documented bone pain or other symptoms clearly secondary to disease without objective response or progression; or decrease in previously elevated acid phosphatase of less than 50% without objective response or progression.
Progression is defined as one of the following: Measurable disease-25% increase in all parameters of measurable disease or
appearance of new lesions (does not include blastic bone lesions which become radiographically evident as a sign of healing) or progression or appearance of lytic bone lesions.
Evaluable disease-increase of acid phosphatase to within 25% of pretreatment levels or reappearance or new Occurrence of disease related symptoms, or progression of bone metastases by x-ray.
CONCLUSION This report indicates that tamoxifen used in doses from 10 mg to 30 mg daily
was well tolerated but not effective in providing tumor shrinkage for any patient in this group of 19 patients with advanced prostate cancer. No benefit was seen even in the 5 patients who had received no prior systemic therapy.
Other investigators, including Arnold et al., Glick et al., Morgan et al., and Spremulli et al.[4] have reported responses from the use of tamoxifen in advanced prostate cancer. The results from our study, however, are consonant with those of Torti et al.[5] who evaluated twenty-nine courses of tamoxifen in doses escalating from 10 to 50 mg orally twice daily in 17 patients all of whom had measurable sites of disease and who had received minimal or no prior systemic therapy. These investigators also showed no objective responses at any dose level. We conclude that tamoxifen has no useful antitumor activity in metastatic prostate cancer.
ACKNOWLEDGMENTS This study was conducted by the Eastern Cooperative Oncology Group (Paul P.
Carbone, M.D., Chairman, CA 21115) and supported by Public Health Service grants from the NCI, National Institutes of Health, and the Department of Health and Human Services.
REFERENCES 1. Lerner, HJ, Band, PR, Israel, L, Leung, BS. Phase II study of tamoxifen: report of 74 patients with
stage IV breast cancer. Cancer Treat Rep 60:1431-1435, 1976.
Tamoxifen in Advanced Prostate Cancer 177
2. Baum, M, Brinkley, DM, Dossett, JA et al. Controlled trial of tamoxifen as single adjuvant agent in management of early breast cancer: Analysis at six years by the Nolvadex adjuvant trial organization. Lancet 1:836-840, April 13, 1985.
3. Sandberg, AA, Muntzing, J, et al. Some new approaches to potential test systems for drugs against prostate cancer. Cancer Treat Rep 61:289-295, 1977.
4. deVoost, HJ. Second-line endocrine management: anti-androgens and anti-estrogens. In EORTC Genitourinary Group Monograph 2, Part A: Therapeutic Principles in Metastatic Prostate Cancer. Alan R. Liss, Inc., 351-357, 1985.
5. Torti, FM, Lum, BL, Lo, R, et al. Tamoxifen in advanced prostate carcinoma: a dose escalation study. Cancer 54:739-743, 1984.