Embed Size (px)
Citation preview

TalkingSpace & TalkingHealth
The IAPT service, Oxfordshire and Buckinghamshire NHS Foundation Trust
Christina Surawy: Oxford Mindfulness Centre, Oxford University Department of Psychiatry
With thanks to: Emma Evans, Clinical Supervisor and Clinical Psychologist
Outline of the session
Overview of TalkingSpace TalkingHealth: Services for people with long-
term health conditions MBCT within IAPT Questions and answers
Referrals to TalkingSpace
TS receives 6500 referrals a year Primarily self-referral The service is meeting nationally agreed
recovery rates (40-50%)
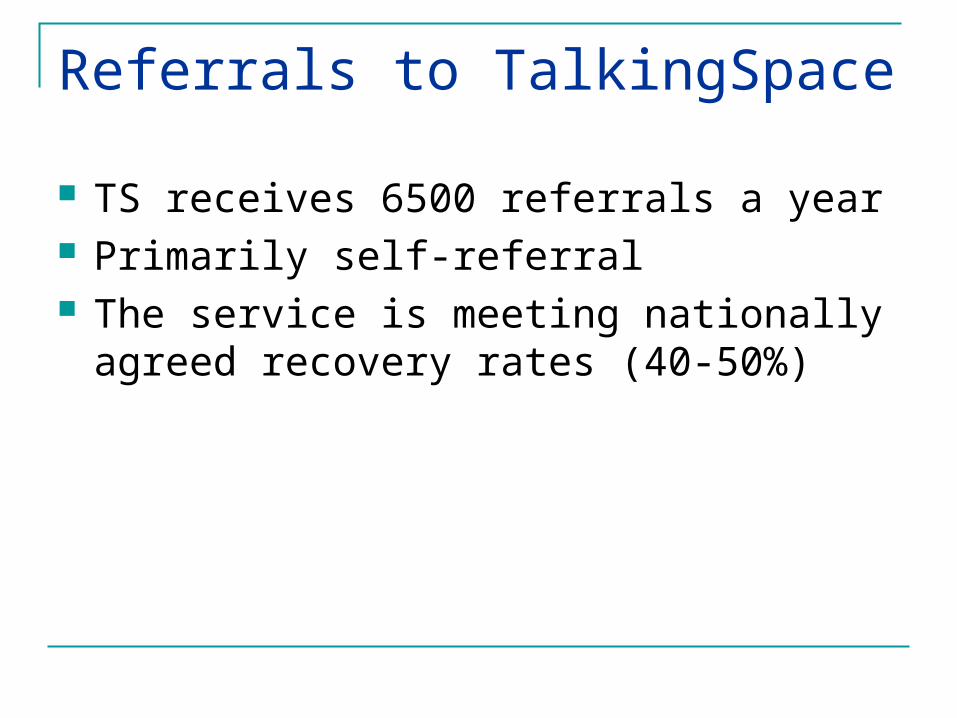
The stepped care model
Step 4 – Secondary Care (e.g. CMHT)
Eating Disorders, Drug and Alcohol addictions, Severe OCD, Severe depression, Bipolar disorder, Psychosis
Step 3 – Primary Care (High Intensity Therapy)Moderate to severe depression, mild to moderate anxiety, including GAD and health anxiety, OCD, social phobia, PTSD
Step 2 – Primary Care (Low Intensity Therapy)
Mild to moderate depression or anxiety
Step 1 – Active monitoring (often GP)
Psychological problem identified
PHQ-9 and GAD-7 completed at least 5 weeks apart
Patient direct to self-help materials
Typical patient journey
ROUTE A: Patient consults GP and mental health concerns are raised
GP: Discuss and assess patient suitability for IAPT. GP gives patient TalkingSpace leaflet
Patient:Calls in to book initial telephone assessment (or sends in brief form)
ROUTE B: Self-referral
Typical patient journey
Route C: Mental health concerns identified during consultation with other health professional
Health professional: Discuss and assess patient suitability for IAPT. Gives patient TalkingHealth leaflet OR recommends further assessment
with GP
Patient: Calls in to book initial telephone assessment (or sends in brief form) OR
sees GP
Patient journey continuedPatient booked for initial brief telephone assessment (20-30 minutes maximum)
If appears appropriate for TalkingSpace: Step 2 class Step 2 guided self help for anxiety and depression or computerised CBT for
depression Step 3 High Intensity CBT assessment
BUT IF Primarily seeking help with adjustment/transition/loss/relationship issues AND/OR prefers a non-structured treatment
Referral to GP practice-based counselling (PML)
If referral appears inappropriate or unclear:
May involve: liaison with GP,CMHT/Psychological Therapies (Step 4)
Treatments offered
Step 2 (LI)
Psychoeducation courses – anxiety, depression, insomnia, emotional well being in diabetes
Information giving Bibliotherapy & Guided-self help Computerised CBT (Beating the Blues) 3-month follow ups as standard
Psychoeducation courses
Offered in various locations throughout Oxfordshire
Depression, anxiety or insomnia Four sessions (five for insomnia) Stand-alone treatment or an introduction to CBT
skills 1 month follow up call
Psychoeducation classes: patient comments It would do a majority of people good. It’s really helpful/reassuring to meet other people
suffering from the same thing. It’s nice to talk within a group and not just one to
one which is quite intense. Excellent and friendly presentation. Useful and informative. Has certainly helped me
to overcome some of my problems.
Treatments offered
Step 3 (High Intensity) Groups – depression, OCD, anxiety (transdiagnostic),
carers’ groups for people caring for people with dementia Individual CBT Mindfulness Based CT group for depression (relapse
prevention) Mindfulness Based CT group for long-term conditions IPT (Interpersonal therapy) DIPT (Brief Dynamic Interpersonal Therapy)
Additional interventions and services
Employment support (Restore) to liaise, provide signposting and support for people struggling to stay in employment
Who can’t we see? Children (under 18) Acute mental health crisis/ high risk to self or others Previous unsuccessful treatment at Step 3 Severe depression/anxiety Severe OCD Eating disorder Psychosis/Bipolar disorder Personality disorder Significant substance misuse Currently seen by another mental health service/
already receiving psychological therapy or counselling Not registered with Oxfordshire GP
TalkingHealth: A service for people with long-term physical health conditions Part of TalkingSpace Initially developing services for people living
with: Diabetes Cardiac rehab and heart failure CFS Long term conditions (including MS and MUS)
TalkingHealth
Higher rates of depression and anxiety when living with a long-term health condition
People do not access services at the expected rates – possible reasons: Focus on physical health? Mental health symptoms considered ‘inevitable’? Interaction between physical health and mental
health difficulties results in typical mental health treatments not seen as relevant/appropriate?
Self-referral or referral from any health professional
Work flexibly (telephone, GP practices and other settings)
Aim to work closely with those involved in physical health care
Priorities
Cardiac services
Input to classes run by nursing staff (psychoeducation)
Guided self help (step 2) Individual CBT and staff supervision groups
(step 3)
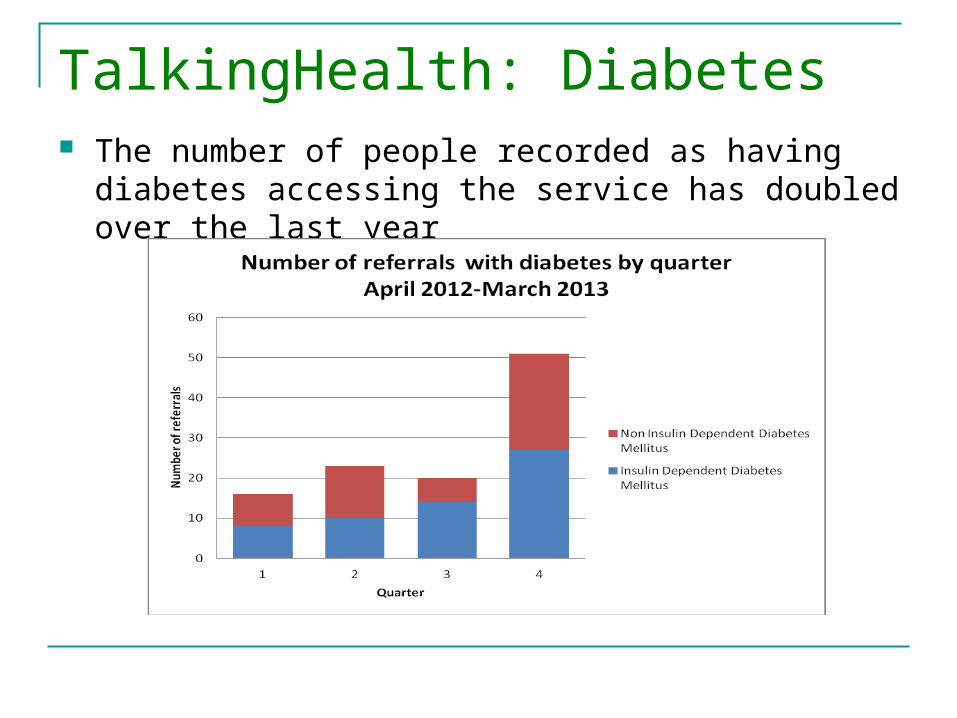
TalkingHealth: Diabetes The number of people recorded as having diabetes
accessing the service has doubled over the last year
Emotional well-being in diabetes course Four session psychoeducation group for people with
diabetes and depression. CBT based Adapted from step 2 class ‘Managing your mood’ Looks at interaction between physical and mental health Topics covers:
Behavioural activation Problem solving Goal setting Cognitive challenging
Evidence to support a course
Initial outcomes suggest:
Greater improvements in mood (PHQ-9) than in standard class Improvements in physical health (HBA1c)
MBCT in TalkingSpace and TalkingHealth OMC have undertaken to train step 3 IAPT
practitioners to deliver MBCT for recurrent depression and anxiety (TS) and LTC’s including MUS). Also a specific MBCT course for CFS
Hoffman et al. (2011) showed that MBCT reduces anxiety and depression across a range of physical diagnoses
So far 8 courses have run Average no. of participants in TS= 16 Fewer in talking health
MBCT for LTC’s
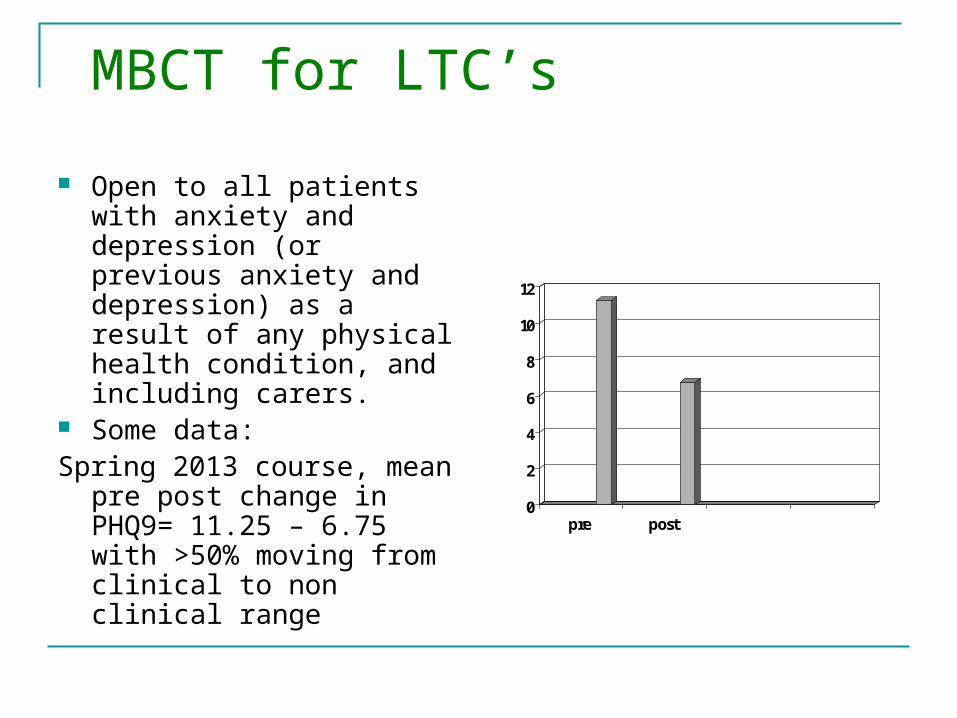
Open to all patients with anxiety and depression (or previous anxiety and depression) as a result of any physical health condition, and including carers.
Some data: Spring 2013 course, mean pre
post change in PHQ9= 11.25 – 6.75 with >50% moving from clinical to non clinical range
0
2
4
6
8
10
12
pre post
MBCT for LTC’s
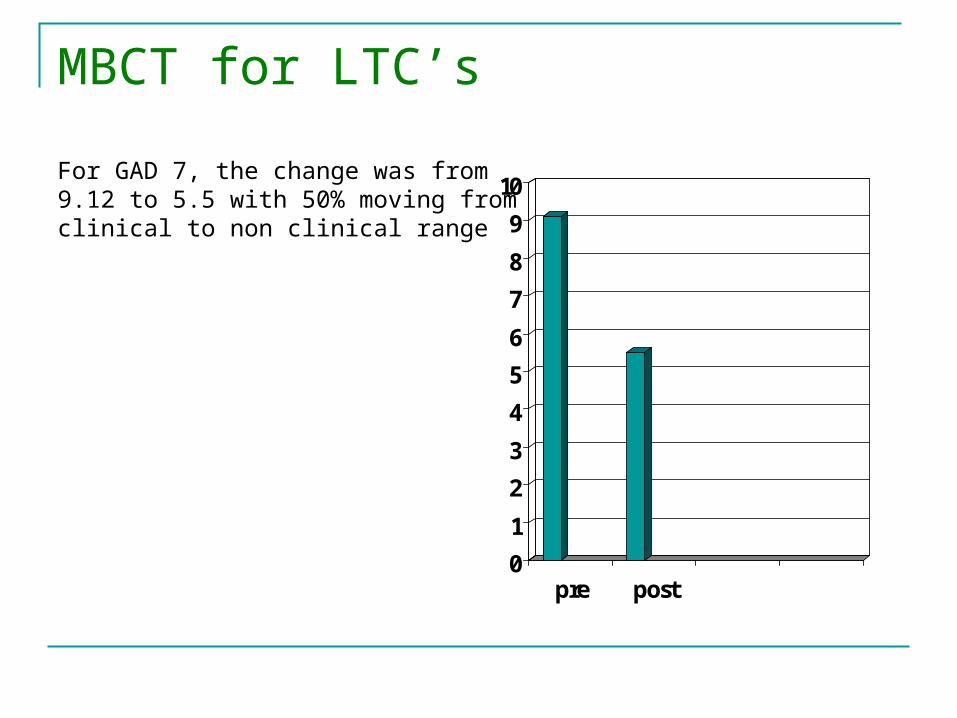
For GAD 7, the change was from 9.12 to 5.5 with 50% moving fromclinical to non clinical range
0
1
2
3
4
5
6
7
8
9
10
pre post
Case example – Bill
66 year old male Physical health: Multiple sclerosis (diagnosed 25
years), neuropathic pain, referred by pain clinic Mental health: Low mood, self-critical, frustration,
tense, restless, body/pain the enemy (constant battle) Treatment: Mindfulness based cognitive therapy
group (8 week programme) Outcome: improved mood, more relaxed, not fighting
pain/body, reduced scores on PHQ-9 & GAD-7
Future directions
Continue to adapt and develop MBCT for LTC’s and MUS
Individualised measures Developing links with pain services

Questions?