Embed Size (px)
Citation preview

TALKING POLITICS AND HEALTH
REFORMReflections from Chile
Jorge Jiménez MD MPHProfessor of PH- PUC
January 2008

PROBLEMS &SOLUTIONS IN HEALTH
• Income related to health status: the Poor and Disadvanteged have much worse health indicators
• Access to health services relates to income in non equitable societies
• Lifestyle, Feeding Patterns, Preventive Care, do more for Health than Medicine
• Medicine goes fast to hightech, high cost solutions: Inequity again

POLITICS AND HEALTHQuestions
• Is Democracy better than Non Democracy for Health?
• How much has the Religion, Culture, Tradition and other factors to do with Health Outcomes?
• Is Politics a good Mediator for Health Policy?• Should Technocrats have a bigger influence in
Polcy Decissions?• If positive, how to build pathways for sound, EB,
technical influence?

MONEY MAKES THE WORLD GO ROUND…
• Health Financing is one major limitating factor
• Equity in health access is related to Health Insurance
• But also the form and the organiztion of health services delivery

HEALTH REFORM
The never ending agenda
Always late always too little
Always inequious

WHERE’S THE BEEF?
• Health Reform continues to be a highly political issue
• Health Policy is a more continuous and well connected chain of events
• Ideally Health Policy should be based on evidency, consensus, participation and have a reasonable planning ( strategies, objectives, indicators)

DRAFTING OF HEALTH POLICY
• A Health Policy is a set of ideas with a plan to address certain problems
• Problems in health are quantitated by means of epidemiology and other methods
• Solutions have the cycle of an innovation: from idea, to pilot, to project, to program, to policy, to evaluation

CRITICAL ELEMENTS FOR A POLICY DESIGN
• Health Information Systems
• Properly trained experts in design and practical implementing levels
• Capacity to obtain resources for the different stages of policy innovation
• Forums and “political markets” in which to sell the goods

MARKET ECONOMY AND HEALTH POLICY: NEVER
ENDING DEBATE• Tradition in PH favours Public
interventions over private initiative. Chile is no exemption
• Debate between pro market versus pro public continues over time
• Integration and Harmonization is the reality
• Public Private mix of responsibilities

PUBLIC PRIVATE MIX IN HEALTH
• Reality tells that we have a real mix, with private provision of public goods and public provision of private services
• Market and Public failures exist and are evident• Different political positions have diverse
approaches: Ideological or Pragmatical• People tend to distribute in this axis transversally
& at random• Very Emotional debate, Never ending...

CHILE a test-tube shaped country?
• Populism 1950-1960• Moderate Right wing
1960-1965• Democratic Reform 1965-
1970• Leftwing Democratic
Marxist 1970-1973• Neoliberal Dictatorship
1973-1990• Democracy Restaured
1990 on, BUT…

HEALTH SYSTEMS IN PARALELL TO POLITICS?
• No, mostly Public Oriented, Government involvement (1920-19780)
• Private sector opportunity in neoliberal environment since 1981
• Public sector recovery since 1990

HEALTH POLICY DRAFTING: CHILE,1980-90
• Exercise in– Consensus building– Search of evidence for policy: good local and
international experiences– Assemblying of human resources and Team
building– Intersectoral coordination– Political constraints under dictatorship

HS RESEARCH IN THE 80’S
• Basic policy research at a few NGO’s, universities under political control
• Mainly funded by european sources: Adenauer Foundation, Italian Government,Canadian IDRC
• No more than 100 professionals involved: small elite
• Main issues were Adjustment and Child mortality, Malnutrition, Market economy and health reform, Health Systems description

HEALTH POLICY STUDIES 85-90
• “Alternative Project”, funded by German Christian democrats (Adenauer), National Democratic Initiative (US Dems), Ford Foundation(1982)
• World Bank gives grant of ¡5.000 US!! For a hospital productivity study at a Jesuit Research centre (ILADES, 1985)

DEMOCRATIC HEALTH PLATFORM DRAFTING
• At Corporación de Promoción Universitaria, 1988-1990
• Several publications, hundreds of seminars
• 600 people involved• Elite formation with young professionals
with high moral and technical motivations• Platform Aproved in 1989, before
presidential election of December

HEALTH PLATFORM CONTENTS
3 Principles:* Make Justice in Health: Equity: access & distribution
* Add Years to Life: Life Expectancy
* Add Health to Years: Healthy and Quality more
years

HEALTH PLATFORM CONTENTS
5 Priority Tasks:• Improve access to healthcare• Solve the hospital crisis• Give big impulse to prevention and protection
of health• Improve quality of environment for helath• Rescue the public sector and integrate private
and NGOBIG AMBITIONS, IDEALISTIC PROGRAM

PRODUCTS COMMUNICATED IN BOOKS

SPECIFIC PROGRAMAS AND INITIATIVES: PHC
• Free service at point of delivery• Extended working hours at facilities:
SAPUS• Improve work status of staff, including
salaries, training, incentives• Incorporation of new programs: ARI,
Mental health, Drug Addiction, the Elderly, Rural poor

HOSPITAL CRISIS: BIG PROBLEM, SOME PROPOSALS
• Increases in salaries
• Renovation of medical technology
• New hospitals and renovation of decrepit ones
• Big investment program with no projects to develop, need to study and write thos projects.

DEMOCRACY IS RESTORED, 1990
• Better information improved quality of diagnosis and proved severity of damage in health systems
• New Platform formulation had premises such as:– Epidemiological transition– Insuficient management capacity– Prolonged financial restriction in public
sector– Inorganic development, lack of
coordination of subsectors

HEALTH REFORM: 1ST FORMULATION,1991
• “Agenda para el Cambio” was its name• It included the new diagnosis plus some
innovative ideas such as• Purchaser Provider split• New financial allocation mechanisms• Hospitals Autonomy, Ambulatory care
emphasis• Performance Agreement as a planning
tool

POLICY STRATEGIES AND ACHIEVEMENTS, PHC
• Increase Number of Consultorios (Health Ambulatory Centres)
• Increase opening hours: To Servicios de Atención Primaria de Urgencia: SAPU
• Promote the Family Medicine Model in Centros de Salud Familiar (CESFAM)
• Increase financial resources via Per Capita payment
• Improve quality, training, income of staff

POLICY STRATEGIES AND ACHIEVEMENTS: HEALTH
PROGRAMS• Burden of Disease Study with Harvard
SPH (1994)
• Priority setting at regional and local level
• Special programs for Adult: Examen de Salud Preventivo del Adulto, ESPA.
• Mental Health Centers: Addictions, Deppresion

POLICY STRATEGIES AND ACHIEVEMENTS: INFRASTRUCTURE
• Investment program of US 950 million in ten years
• More than 15 new hospitals,• 10 Ambulatory High Tech centers• 400 outpatients clinics for ambulatory
care• Imaging devices, Intensive care renovation
for public hospitals

INNOVATIONS WITH POPULATION IMPACT
• Some initiatives have higher impact in population indicators
• Child Survival Strategies
• Colecistectomy for Gallblader Cancer prevention
• Idea is to promote best use of evidence for Policy Design and Implementation

HEALTH REFORM 2000
• After the initial 10 years Chile was prepared to build a new set of methods and policies to achieve better standards of health
• It has been a typical HR cycle in many senses, but successful so far

AUGE: a big step forward?
• GUARANTEED diagnosis and treatment of prioritized health conditions
• Excesses in perception of capacities of medicine
• A neo-liberal extreme? or
• A central planning delirium??
• Or both or none of the above?

IT IS A COMPLEX PROCEDURE
• Requires valid information systems• Evidence based and cost-effectiveness
studies• It includes many conditions of which
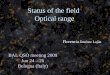
predictions are difficult or impossible• But finally, big numbers in few conditions
explain most of impact• Common, manageable conditions explain
80% of total cases

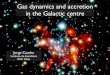
NECESIDADESDE SALUD
• Epidemiología• Sist. de Salud
• Muerte• Recupera-ción
NecesidadLatente
NecesidadesPercibidas
• Características Clínicas Enf ermedad• Percepción Indiv idual Enf ermedad• Conocimiento Social y Cultura• Acción del Agente Principal (Médico)
• Auto cuidado• Demanda aAtención No Formal• No hacer nada
DemandaExpresada
Atención Formal
• Percepción Indiv idual Riesgo• Conocimiento Social y Cultural• Acción del Agente Principal (Screening)
• Características Clínicas Enf ermedad• Costo $•Prioridades, costo alternativ o•Tiempo•Percepción de benef icio potencial•Características de la oferta (disponibilidad, Acceso)
• Demanda a Red NO GES
DemandaInsatisf echa en Red GES
Ambos GES y no GES
Utilización SIGGES
•Conocimiento social sobre GES•Características de la Enf ermedad y grado de comorbilidad.•Copago $•Características Of erta de prestadores pref erenciales•Acción agente principal•Características de la Canasta GES (Sistema entrada, restricciones)
• Integridad del registro•Acción del agente principal
PRINCIPALES ETAPAS Y DETERMINANTES DEL PROCESO DE DEMANDA DE ATENCION A LA RED GES
A
B C
D
E
G
Demanda sumada
Determinantes de
Demanda restada
A,B,C,D,E,F,G : Supuestosexpresados en %
Demanda a red GES
F

FLUJOGRAMA DE DEMANDA EN SALUD
Necesidad Necesidad
percibida
Demanda Formal
Demanda GES 1
Demanda GES 2
Demanda TIS E IS
FC 1 FC 2
FC 3a
FC 3b
Gradiente ISAPRE / FONASA

DEMANDA ACUMULADA POR PROBLEMA DE SALUD EN RED GES FONASA. PROYECCION 2007
0500.000
1.000.0001.500.0002.000.0002.500.0003.000.0003.500.0004.000.0004.500.000
Hip
erte
nsió
n
Dia
bete
s M
ellitu
s
Salu
d O
ral I
nteg
ral
Artro
sis
de
Aten
ción
Inte
gral
Asm
a Br
onqu
ial
Trat
amie
nto
Neu
mon
ías
Ret
inop
atía
Col
icis
tect
omía
Aten
ción
Parto
s Pr
emat
uros
Estra
bism
o en
Trau
mat
ism
o
Aliv
io d
el D
olor
Sínd
rom
e de
Car
diop
atía
s
Sínd
rom
e de
Tras
torn
os d
e
Cán
cer d
e
Cán
cer G
ástri
co
Tum
ores
y
Trau
ma
Ocu
lar
Prem
atur
os
Rup
tura
de
Gra
n Q
uem
ado
Linf
omas
Trat
amie
nto
Fisu
ra P
alat
ina
Dia
bete
s M
ellitu
s
Dis
rraf
ias
Dep
ende
ncia
al
PROBLEMA GES
CASO
S
80%
1 Hipertensión Arterial Primaria o Esencial
2 Infección Respiratoria Aguda (IRA) Baja de Manejo Ambulatorio en Menores de 5 años
3 Diabetes Mellitus Tipo II
4 Depresión
5 Salud Oral Integral para Niños de 6 años Prevención y Educación
6 Vicios de Refracción en Adulto Mayor
7 Artrosis de Cadera Leve y Moderada en Mayores de 60 años; Artrosis de Rodilla Leve y Moderada en mayores de 55 años
8 Atención Integral del Embarazo y Parto

FINAL COMMENTS BEFORE Q&A
• Health Reform in Chile continues to be a fascinating issue
• Its an adventure, an audacious attempt to equity
• It requires better conditions for management
• So far it has produced equity in the pioritized conditions

MUCHAS GRACIAS