Embed Size (px)
DESCRIPTION
First in a series of four original patient guides, "Understanding My Disease" is for the newly diagnosed kidney cancer patient. Updated June 20, 2013
Citation preview

Taking Charge of Kidney CancerUnderstanding My Disease
First of a Series of Four Patient Guides
Published by Action to Cure Kidney Cancer

About ACKC
Action to Cure Kidney Cancer (ACKC) is a grassroots group of kidney cancer survivors and family/caregivers who estab-lished a new not-for-profit health-advocacy organization in 2003. Our mission is to educate the public about kidney cancer, empower kidney cancer patients and their families, endow grants, and lobby for research towards finding a cure.
Our “Taking Charge” Guides
ACKC’s set of four guides provides kidney patients and their caregivers with the information they need to take a proactive role in their health care and their lives. Guide 1 Understanding My Disease is written for the newly diagnosed patient. Guide 2 Managing My Cancer is about the care and treatment of kidney cancer patients with metastatic disease. Guide 3 Supporting My Caregiver is intended for the people in your life who are helping you. Guide 4 When Treatment Ends is designed for both patients and their loved ones.
© 2012 Action to Cure Kidney Cancer

Understanding My Disease Page 3
P A T I E N T G U I D E 1
Understanding My Disease
Welcome 5
Introduction to Kidney Cancer 7
Basic Kidney Facts 7
Who Gets Kidney Cancer? 8
Detecting Kidney Cancer 8
Risk Factors 8
Reducing the Risk 10
Tests to Expect 10
Types of Kidney Cancer 11
Just Diagnosed 12
Getting a Second Opinion 12
Finding the Best Treatment Center 12
How to Choose My Urologist 13
Knowing My Treatment Options 14
Nephrectomy 15
Open Surgery versus Laparoscopy 16
Alternatives to Surgery 17
Prognosis and Statistics 18

Page 4 Taking Charge of Kidney Cancer
“Virtually all people are patients at some point in their lives.
Improving a person’s ability to understand and manage his or her own
health and disease, negotiate with different cadres of health professionals,
and navigate the complexities of health systems is crucial to achieving
better health outcomes.”
T H E L A N C E T “Patient Empowerment — Who Empowers Whom”
May 5, 2012

Understanding My Disease Page 5
Welcome to the first of four “Taking Charge of Kidney Cancer” guides.
You have just been told you have kidney cancer. You think, what am I going to do? Has it spread? Where do I turn for help? The ACKC “Taking Charge” guides, which are written from the perspective of kidney cancer survivors, will give you and your caregiver the knowledge, tactics, and strategies you need to arm yourself in your war against kidney cancer.
Today, the outlook for kidney cancer patients is much better than even a few years ago. There are a number of successful surgical and nonsurgical treatments that may be available to you. This means that no sooner are you diagnosed, then you are faced with some of the most important questions of your life: Which urologist do I go to? Where is the best place to be treated? Should I get a second opinion? What are my surgical options? Can I be treated without surgery? How do I build a medical team?
Our guides are designed to help you and your caregiver navigate every step of the way as you face these difficult decisions. Studies have shown that the best informed patients have the best outcomes.
As an eleven-year survivor of kidney cancer and the founder and president of ACKC, I hope these guides will be useful to you in your personal battle with kidney cancer. Get to know our organization. If there are additional ways that we can be helpful to you, please do not hesitate to let me know.
This first brochure is for the newly diagnosed patient.
Respectfully,
Jay Bitkower President, Action to Cure Kidney Cancer

Page 6 Taking Charge of Kidney Cancer
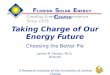
The Human Urinary System
Kidney Functions. As the body’s main filtering system, the kidneys control fluid balance, regulate electrolytes, help regulate blood pressure, and prevent acid buildup. The kidneys also secrete erythropoietin, a hormone which stimulates the bone marrow to produce red blood cells.
adrenal glandkidney
vena cavaabdominal aorta
ureter
bladderprostateurethra
Illus
trat
ion:
Kim
berly
Bat
tista

Understanding My Disease Page 7
Introduction to Kidney CancerCancer is not one disease but many different diseases depending upon the part of the body where it occurs and its genetic profile (see Types of Kidney Cancer on page 11 for more details). Each cancer has its unique characteristics, rate of growth, and treatment options. Unlike cancers of the breast, cervix, and colon, there are no reliable screening tests for early detection of kidney cancer.
Fortunately the majority of kidney cancers are detected as an incidental finding. If your disease was discovered early, your chances for survival or even a complete cure are very high. Ac-cording to the American Urological Association, the long-term survival rate for patients with early kidney cancer ranges from 79 to 100%. According to the National Cancer Institute, there are over 320,000 men and women alive in the U.S. who have a history of kidney cancer.
There are a number of successful surgical treatment options in-cluding nephrectomy and partial nephrectomy as well as abla-tion therapy (see treatment options on page 15). In healthy pa-tients with small tumors, laparoscopy and partial nephrectomy are rapidly becoming the standard of care. Even in patients who are not candidates for surgery or have more advanced kidney cancer, treatments such as immunotherapy and targeted treat-ments are extending lives.
New discoveries, drugs, and ongoing clinical trials justify an opti-mistic outlook.
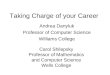
Basic Kidney FactsYour kidneys are bean-shaped organs about the size of your fist just below the rib cage on either side of your spine. They are part of the liquid waste removal system of the body. The kidneys filter excess water and waste products from the bloodstream, turning them into urine. Urine collects in the renal pelvis (see kidney dia-gram on page 8), flows down long slender tubes, called ureters, which connect to the bladder, and finally leaves the body through the urethra when you urinate.
genetic profile: Mutations, or changes, in genes that regulategrowth of cells.
incidental finding: Discovery of a tumor(s) during tests done forsomething else. These are usu-ally smaller, easier to treat, and have a better prognosis.
nephrectomy: Removal of the kidney.
ablation: Using energy to de-stroy the tumor.laparoscopy: Minimally invasive surgery through small incisions using a laparoscope, a long tube with a video camera. May be combined with robotics.partial nephrectomy: Surgical removal of only the part of the kidney that contains the tumor.immunotherapy: Using the body’s own immune defenses to attack the tumor.targeted treatments: Designer drugs that target the cancer’s proteins or other tumor- producing factors.

Page 8 Taking Charge of Kidney Cancer
Who Gets Kidney Cancer? Although kidney cancer was once considered rare, in the last 50 years, the number of people diagnosed with this disease has risen 2 to 3% a year in the U.S. It is now the 8th most common cancer over all. In 2012, the American Cancer Society projects that an estimated 64,770 new cases will be diagnosed. Part of the increase is due to earlier detection with better imaging techniques and part is possibly due to the obesity epidemic among Americans.
Detecting Kidney CancerKidney cancer is usually asymptomatic until the disease is more advanced. Common symptoms include:
• Bloodinyoururine(mayberust-coloredordarkerred)• Persistentpaininyourbackorside• Alumpormassinyoursideorabdomen• Feelingmoretiredthanusual• Unexplainedfeverorlossofweight• Swollenanklesandlegs• Highbloodpressureoranemia• Varicocele on the left side of the scrotum
Most often these symptoms are signs of infection, kidney cysts, kidney stones, or other benign conditions. In addition, these symp-toms may not appear until the kidney mass is large or metastatic.
Risk FactorsThese are some of the risk factors that researchers have found that increase the possibility of getting the disease.
Age and Gender. Most kidney cancer is found in people between the ages of 50 and 70, with men developing it at about twice as oftenaswomen.However,therateamongwomenisincreasing.
Obesity. The rise in obesity since the 1990s is a major factor in the increase in kidney cancer, accounting for as much as 30 to 40% of cases. It is speculated that being highly overweight may cause changes in certain hormones that might lead to kidney cancer. Fat cells may also retain chemicals that are toxic.
Varicocele: Abnormal enlargement of the vein that drains the testicles.

Understanding My Disease Page 9
Smoking. Cigarette smoking is highly associated with kidney cancer, especially renal cell carcinoma, a major category of kidney cancers. The more one smokes, the greater the chances of develop-ing the disease. Among men, smoking accounts for an estimated 30% of kidney cancer cases and about 25% in women.
High Blood Pressure. Several cancer websites indicate that hyper-tensionisariskfactorforkidneycancer.However,somestudieshave shown that kidney tumors cause hypertension so the caus-ative factor is unclear.
Family History. Although inherited forms of renal cell carcinoma only account for 2 to 4% of cases, a family history is associated with an increased risk for kidney cancer. Certain genetic diseases and syndromes greatly increase the tendency to develop kidney cancer.
Chemical Exposure. Researchers have found that occupational exposure to trichloroethylene, cadmium, and other toxic chemi-cals may be associated with increased kidney cancer risk.
Examples of Genetic Diseases
VonHippel-LindauSyndrome,Birt-Hogg-Dubé,andotherhereditary renal cell carcinomas. If the patient is identified as hav-ing one of these diseases, other family members should undergo genetic testing to determine if they are carriers. People who have one of these syndromes will need different treatment and require different care.
The Human Kidney
adrenal gland
renal cortex
medulla (renal pyramid)
renal vein renal artery
renal pelvis
ureter
outer lining (Gerota’s fascia)
Illus
trat
ion:
Kim
berly
Bat
tista

Page 10 Taking Charge of Kidney Cancer
Reducing the Risk
While there is no known way to prevent kidney cancer, certain lifestyle measures can reduce the risk. Most important is stopping smoking, maintaining normal body weight, and controlling your blood pressure. Several studies have found that moderate amounts of alcohol, a diet high in fruits and vegetables, and eating fatty fish are associated with lower risk of getting kidney cancer.
Tests To ExpectIf your family history, physical exam, or symptoms indicate the possible presence of a kidney tumor, your doctor will usually or-der one or more of the imaging tests, listed below. These highly sophisticated imaging techniques can usually provide enough in-formation so that invasive biopsies are not necessary. Sometimes the doctor will order a combination of different scanning methods to fully evaluate the extent of the tumor.
Ultrasound or sonogram is a painless external test that uses high frequency sonar technology to visualize internal body parts.
CT scan, also known as computed tomography or CAT scan, often combined with intravenous contrast dye, uses x-ray and computer technology to create detailed cross-sectional views of the kidney and surrounding areas. If you take a CT scan with intravenous contrast dye be sure to drink plenty of water after the scan to flush out the dye and prevent kidney damage. Your doctor can often determine just from the scans the size, shape, and location of the mass in the kidney as well as enlarged lymph nodes that may indi-cate metastatic spread. If your doctor suspects that the kidney can-cer has metastasized, she may order scans for the suspicious areas.
MRI scan (magnetic resonance imaging) uses strong magnets and radio waves to look inside the body. MRIs are often used if a person is allergic to the contrast dye used in CT scans. They are also better than CT scans in looking for evidence of “tumor thrombus”— the extension of the cancer into the renal vein and vena cava.
Needle biopsy of the kidney tumor tissue is sometimes needed to determine malignancy.
Incidentally Good Findings
Recent studies have shown that 20% of early stage kidney tumors — the kind most often found on diagnosis — turn out to be benign, while 60% are in-dolent, meaning slow-growing, and only 20% are potentially aggressive.
Biopsy: Removal of the tumortissue to look for malignant(or cancerous) cells.
Metastasis: Spread of the cancer to other body parts.

Understanding My Disease Page 11
Types of Kidney Cancer Kidney cancer is in fact not a single disease, but a series of differ-ent diseases that often have very different outcomes. Knowing the type of kidney cancer you have can only be determined by looking at the actual cancer tissue which has been taken from a biopsy or removal of the tumor. Once the cancer type is determined, the information can help your urologist or oncologist determine your treatment options. Your type of cancer will be determined after the tumor has been removed and a pathologist has examined the tumor cells under the microscope.
Type
Renal Cell Carcinoma
Description
• Papillary
• Clear Cell
• Chromophobe
• Collecting Duct
Transitional Cell Carcinoma of the Renal Pelvis and Ureter
Oncocytoma
Wilms Tumor
Angiomyolipoma
Renal Cell Carcinoma (RCC) is a series of cancers of the kidney that originate from the functioning part of the kidney. These types of cancer comprise 90% of all kidney cancers. RCC is divided into four main subtypes according to the type of cell where it origi-nated and its microscopic appearance.*
Also known as conventional renal cell carcinoma, this is the most common form, accounting for about 75 to 80% of all renal cell carcinomas. The stained cell appears clear when viewed through the microscope.
About 10 to 15% are of this subtype, which is further subdivided into type 1 and type 2. Type 1 is usually slow growing, while type 2 is often a very aggressive cancer. The distinction between types 1 and 2 is really a function of their genetic profile.
About 5% are of this type, which rarely metastasizes outside the kidneys.
Its histology is more related to transitional cell carcinoma than
The second most common form of kidney cancer found in 7% of adults with kidney cancer. Occurring in transitional cells, it is related to bladder cancer.
Not actually cancer but a benign tumor (from 3 to 7%)
Occurs mostly in children. Unlike adult kidney cancer, it usually responds well to chemotherapy and radiation.
A usually benign tumor of fat and muscle tissue.
*There are other subtypes like sarcomatoid and medullary. But these account for fewer than 1 to 2% of the cases.
Renal Cell Carcinoma: Kidney cancer that develops inthe lining of the renaltubules that produce urine.
RCC.

Page 12 Taking Charge of Kidney Cancer
Just Diagnosed
Getting a Second Opinion
Beingproactiveisahardjobforboththepatientandthecaregiver.It means gathering as much information about your disease as you can from the internet, medical studies, and other patients.
Websites including ackc.org (Action to Cure Kidney Cancer), kidneycancerinstitute.com, kidneycancer.org, and acor.org (where patients share their experience and knowledge about the disease) are other great resources. Armed with this information, you will gain the knowledge and the confidence to seek out the best doctors and hospitals to get the treatment you need. Often what one medical expert says can’t be done has already been done elsewhere successfully.
Many proactive patients seek out a second opinion or even a third opinion even if they feel satisfied with their present urologist or oncologist. First, you may wish to have another specialist confirm the diagnosis and staging. Second, there are usually a number of treatment options available and having another expert review your medical history and records may help you decide which course to take. Your doctor should welcome your getting another opinion and most insurance companies will cover it.
Finding the Best Treatment Center
Usually, the best place to be is at a large cancer research center with an excellent reputation and experience in treating kidney cancer patients. These centers are magnets for the best clinicians and researchers, who are aware of the latest developments, the cutting edge reports, the most up-to-date treatment guidelines, and the most recent results of clinical trials. The interdisciplinary nature of these centers assures the sharing of information from other specialists in related fields. The National Cancer Institute can give you information about treatment centers in your area. Call1-800-4-cancer (1-800-422-6237)or chatusingLiveHelpathttps://livehelp.cancer.gov for NCI’s instant messaging service.
Allen’s Story
When my kidney tumor was found, the surgeon at my local hospital said he could do the operation laparoscopically. Buthecouldnotdoapartialnephrectomy—which is what I wanted—because of where the tumor was located. My wife and I sought out two different doc-tors at two major cancer centers, both of whom said they could do a partial nephrectomy. We found the first doctor too cocky and went with the second, who was a lovely man. So personality played a role in our selection.
Staging: Tests and exams to determine extent of cancer in the body. Staging will be comprehensively covered in Guide 2.

Understanding My Disease Page 13
Making the Rounds (Patient Style)
If you live near a large research hospital with a known reputa-tion in treating cancer, you can ask for a referral to a kidney cancer specialist associated with that hospital. Some of the top cancer centers in the U.S. offerthisserviceonline.Butit is probably best to do it in person where the kidney cancer specialist can perform a physical examination, order more tests if deemed necessary, or request further records or a biopsy.
U.S. News and World Report lists 500 cancer hospitals whose staff have a high level of expertise in treating difficult cases. They also rank the top 50 urology departments in the country as well as the top 50 cancer centers according to criteria such as their reputa-tion among specialists, nurse staffing, and patient survival. ACKC combined these rankings and posted the results on our website at http://www.ackc.org/resources/us-news-world-reports-medical-center-ratings.
How to Choose My Urologist
A good place to start looking for a urologist in your area is on the American Urological Association website. Go to http://www.urologyhealth.org with special interest area: Oncology/Cancer. Things to consider in choosing a specialist are the doctor’s medical training, including medical school and residency; board certifica-tion as a specialist; whether they are a diplomate or fellow of their medical specialty society (these are individuals who demonstrate outstanding performance); and their hospital affiliation. Most urologistsdoprostatecancersurgery.Lookforsomeonewhodoeskidney surgery as well. You want to ensure that the surgeon is ex-perienced in laparoscopy and/or doing partial nephrectomies if that is what you choose.
Top cancer treatment centers attract the best interdisciplinary teams.

Page 14 Taking Charge of Kidney Cancer
Your primary care physician can be a good source of referral and can usually get you an appointment much more quickly. Other re-ferral sources are your county or state medical society and friends or family members whose judgment you trust. Online listservs such as ACOR enable you to reach out to other patients for their recommendations. You may wish to interview several doctors to see what surgical and treatment options they offer.
Take your time to find the right doctor, even if it means delaying surgery for a few weeks. You should interview a surgeon or sur-geons who have experience in all treatment modalities including open surgery, laparoscopic and robotic surgery, and ablation op-tions. This way you will have the best chance of getting the right surgery for you rather than the procedure with which the surgeon is most comfortable.
Knowing My Treatment OptionsThe first step is to make a decision about how to deal with your pri-mary tumor, i.e., the one in your kidney. Today there is a wide va-riety of treatments available depending on the size of your tumor, your general health, your age, and whether or not your cancer has
Questions to Ask
•Howmanynephrectomies do you perform each year?
•Howmanyoftheseare radical compared with partial surgeries?
•Doyoudoopenorlaparo-scopic nephrectomies?
•Areyouexperiencedin doing laparoscopic partial nephrectomies?
A good doctor heeds your concerns, welcomes your ideas, inspires your trust.

Understanding My Disease Page 15
spread. If the tumor is contained within the kidney, you have three main options — surgery to remove the tumor, tumor ablation, which destroys the tumor, and active surveillance through regu-lar scans. In most cases of kidney cancer, surgery is the preferred treatment.Buttheextentofthesurgeryandthemethodusedaredecisions to be made between you and your doctor.
NephrectomyIn the past, the gold standard of treatment for a tumor contained within the kidney was radical nephrectomy. While in most cas-es this was effective in stopping the progression of cancer and achieving a high five-year survival rate, it also raised the chances of reduced renal function and chronic kidney disease. These days, surgical treatments have improved, more surgeons have experi-ence doing these types of operations, and more types of surgical treatments are available.
Partial nephrectomy (or nephron-sparing surgery), which re-moves just part of the kidney with the tumor, is now preferred for small tumors confined to the kidney so that the patient retains as much kidney function as possible. This is especially important if a patient has a high risk of dialysis or has only one kidney.
Studies have shown that both types of surgery are equally effective so that partial nephrectomies, if feasible, are now considered stan-dard treatment. Note that the size and position of the tumor in the kidney can determine whether a partial nephrectomy is an option. Although partial nephrectomy, where possible, may be standard of care at large cancer centers, “community” urologists, who have less experience with kidney cancer, may still be doing radical ne-phrectomies exclusively. In this case, you should seek the opinion of another urologist. That being said, for larger tumors that may have invaded critical areas of the kidney, a radical nephrectomy is called for.
If a tumor is very large, doctors may use drugs to try to shrink the tumor before removing it.
radical nephrectomy: Removal of the whole kidney, adrenal gland on top of the kidney, and surrounding lymph nodes.
partial nephrectomy: Surgical removal of only the part of the kidney that contains the tumor.

Page 16 Taking Charge of Kidney Cancer
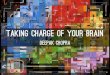
Open Surgery versus LaparoscopyLaparoscopy has a quicker recovery time, reduced hospital stay, and less pain. The complication rates are about the same. Since 2000, robotic surgery has been used by some, but not most, lapa-roscopic surgeons. This provides greater precision and 3-D vision which is particularly useful for tumors that are difficult to reach. While laparoscopic partial nephrectomy is a good treatment op-tion for small localized tumors confined to the kidney, it is not for everyone, including patients who have had a history of ex-tensive abdominal surgery. Even in those patients, surgeons who are experienced in a technique called retroperitoneoscopic ne-phrectomy can spare the abdomen by inserting small telescopes (laparoscopes) into the cavity that surrounds the kidney. Note that in about 5% of patients undergoing laparoscopic partial nephrec-tomy, the surgeon may have to enlarge the incision and remove the entire kidney. In either case, if you should choose to have partial nephrectomy either through the traditional method or laparos-copy, it is vitally important that you choose a surgeon who is ac-complished in these techniques.
The view through the laparoscope can be seen on the TV monitor.
© P
hilip
Rin
k Ph
otog
raph
y

Understanding My Disease Page 17
Alternatives to Surgery
ABLATION
While surgery is the treatment of choice for almost all patients with kidney cancer, there is another method that destroys the tu-mor in place known as ablation. Patients who are at high risk for surgery, have multiple medical problems, are elderly or frail, or don’t wish to have surgery, can opt for some form of tumor abla-tion. It is best used on patients with small, localized tumors. Im-provements in ablative technologies are making it possible for a healthy patient with a tumor less than 3 cm to consider it as an alternative to surgery. Again, this should be done in consultation with your doctor.
Types of Ablation Techniques. There are a number of ablative technologies including cryoablation and radiofrequency abla-tion (RFA). In cryoablation, extreme cold, to the point of freezing, is used to destroy the tumor. Radiofrequency ablation destroys the cancer cells by heating them with high-energy radio waves. Abla-tion procedures are performed by a urologist, an interventional radiologist, or a team that includes both specialties. Ablation tech-nologies can use a laparoscopic approach with an incision to insert a scope and a probe to deliver either heat or cold, or through the skin (using just the probe through the skin directly into the tu-mor under the guidance of a CT scan or MRI). Other techniques include high-intensity focused ultrasound, cyberknife, microwave thermotherapy, and laser coagulation, but these are still consid-ered experimental methods.
Effectiveness. To be successful, the interventional radiologist must completely destroy all tumor cells and a rim of normal cells with minimal damage to the surrounding healthy tissue. While these techniques show promising results, there has not been the long-term follow-up to assess their effectiveness in preventing tu-mor progression and extending survival, although the short-term results are promising.
Pros and Cons. The advantages of ablative techniques are that they are generally less invasive and may be better at preserving kidney
Choosing an Interventional Radiologist
Interventional radiologists are board-certified specialists in both vascular and interventional radiology and diagnostic radiol-ogy. As with choosing a surgeon, you want someone who is highly experienced in these techniques. Affiliation with a top cancer research center is a plus. You can start your search by asking for a referral from your surgeon or oncologist. The Society of Interventional Radiologists has a doctor finder on their website for your area. Again, social me-dia sites, such as ACOR, where patients share their experience, can be helpful.
interventional radiation: Nonsurgical techniques (also called ablation) thatuse a variety of methods todestroy the tumor.

Page 18 Taking Charge of Kidney Cancer
functionwhenmultipletumorsarepresent.Butifyoudecidetohave ablation rather than surgery, you must be prepared for close follow-up and possible repeat biopsy after treatment. Complica-tions of cryoablation and RFA are uncommon but may include bleeding and damage to the kidneys or nearby organs. The risks of ablation include not getting all the cancer cells the first time around, requiring further treatments, a greater risk of recurrence compared with surgery, and the fact that this is fairly new technol-ogy and there are not the kind of survival data that are available for surgical treatment.
ACTIVE SURVEILLANCE
Finally, for small tumors that are confined to the kidney, in spe-cial cases one may choose active surveillance in lieu of surgery. In such cases, the doctor closely monitors the patient via sequential imaging studies for signs of tumor progression before intervening with surgery or medical treatment. Candidates for this approach include patients who have limited life expectancy, are unfit for sur-gery, or are comfortable with taking the calculated risk that their tumor is benign or slow-growing. If you choose this option, you should discuss with your doctors the potential risks, such as tumor growth, loss of a possible opportunity for partial nephrectomy, and the current limitations of tumor biopsy in guiding your decision.
Prognosis and StatisticsA number of factors influence your prognosis, including whether you had symptoms at the time of diagnosis, if the cancer has me-tastasized, and the results of laboratory biochemical tests. Your chances of five-year survival if you have early stage kidney cancer areveryhigh.Butevenifyouhavemetastaticcancer,newtreat-ments and approaches are extending survival. Remember, you are not a statistic. The more proactive you and your caregiver are in researching and interviewing doctors about new treatments, the better your chances of surviving kidney cancer.
Embolization If the patient cannot tolerate surgery or ablation, emboliza-tion may be tried where the blood supply to the tumor is cut off with the intention of reduc-ing tumor spread.

Understanding My Disease Page 19
“Taking Charge” Guide 2
In Guide 2 Managing My Cancer, we will lead you through the next steps after removal of your tumor including pathological staging of the tumor, treatment options for metastatic disease, and maintaining your health and kidney function.
Stay in Touch with ACKC
LikeusonFacebook facebook.com/ActionToCureKidneyCancer
Follow us on Twitter twitter.com/cureRCCcancer
Read our Newsletter to keep up to date regarding ACKC news and activities. Email us at [email protected] to subscribe.
Join our Committee. Meetings are held in New York City. Contact us for more information.
Contact ACKC
Action to Cure Kidney Cancer 150 West 75th Street, New York, NY 10023
Telephone 212 714 5341 Email: [email protected]
Credits
Written and Researched by Carol Kahn Designed by Sara Mears | Communication By Design
Page 6 and 9 illustration: Kimberly Battista Page 13, 14 and cover images: istockphoto.com Page 16 image: © Philip Rink Photography
© 2013 Action to Cure Kidney Cancer
062913

Page 20 Taking Charge of Kidney Cancer
Action to Cure Kidney Cancer 150 West 75th Street, Suite 4, New York, NY 10023
212 714 5341 • [email protected]
ackc.org