Embed Size (px)
Citation preview
Taking a Weight off Health Care Systems
Arya M. Sharma, MD/PhD, FRCPC
Scientific DirectorCanadian Obesity Network
Professor and Chair in Obesity Research & ManagementUniversity of Alberta
Medical DirectorAlberta Health Services Provincial Obesity Strategy

Vital Statistic: Waist Circumference
Sharma AM, 1995

Overweight
Obesity in Canada
1985 2010
30% 60%Obese 20%6%
Severely Obese1% 6%
Statistics Canada 2010

Obesities are heterogeneous complex disorders of multiple etiologies characterized by excess body fat that threatens or affects socioeconomic, mental or physical health
Sharma 2007

After covariate adjustment, the hospitalization and physician costs were respectively 40% and 22% higher
among obese and overweight adults than among normal-weight adults.
2008 Cost of Obesity in Australia estimated at $ 58 Billion
Cost of Obesity in Canada?
58 Billion / 20 Million x 33 Million =
$ 95 Billion!
www.drsharma.ca

All interventions affect 15-50 year olds except the lastwhich is for all ages 15-100yr
England’s predicted future Health Service costs based on either no action or reductions in adult BMI
0
2
4
6
88
Annual Costs£Billion
22.2
20.9
19.7
18.4
17.1
2009 2019 2029 2039 2049 2059
Reduction in BMI units

BMI All ages Cap at 30;50% effective
20+yrs: BMI -4 units
No Action
Childhood prevention
6-10 yrs
2004 2014 2024 2034 2044
1049
654
240
-164
-366
38
1453
Year
Ann
ual c
osts
£ M
illio
nsAnnual Diabetes Costs in England with Different Obesity Prevention Strategies
http://www.bis.gov.uk/foresight/our-work/projects/current-projects/tackling-obesities


Transport, Mobility &
Patient Safety
Wound and Skin Care
Personal Hygiene
Instrumentation
Provider Safety
Sensitivity
Exercise & Physical Therapy
Bariatric Care
Nursing
Medicine
Physiotherapy
Occupational Therapy
Exercise
Nutrition
EMS
Transportation Services

Can we Change Weight Bias in Health Professionals?
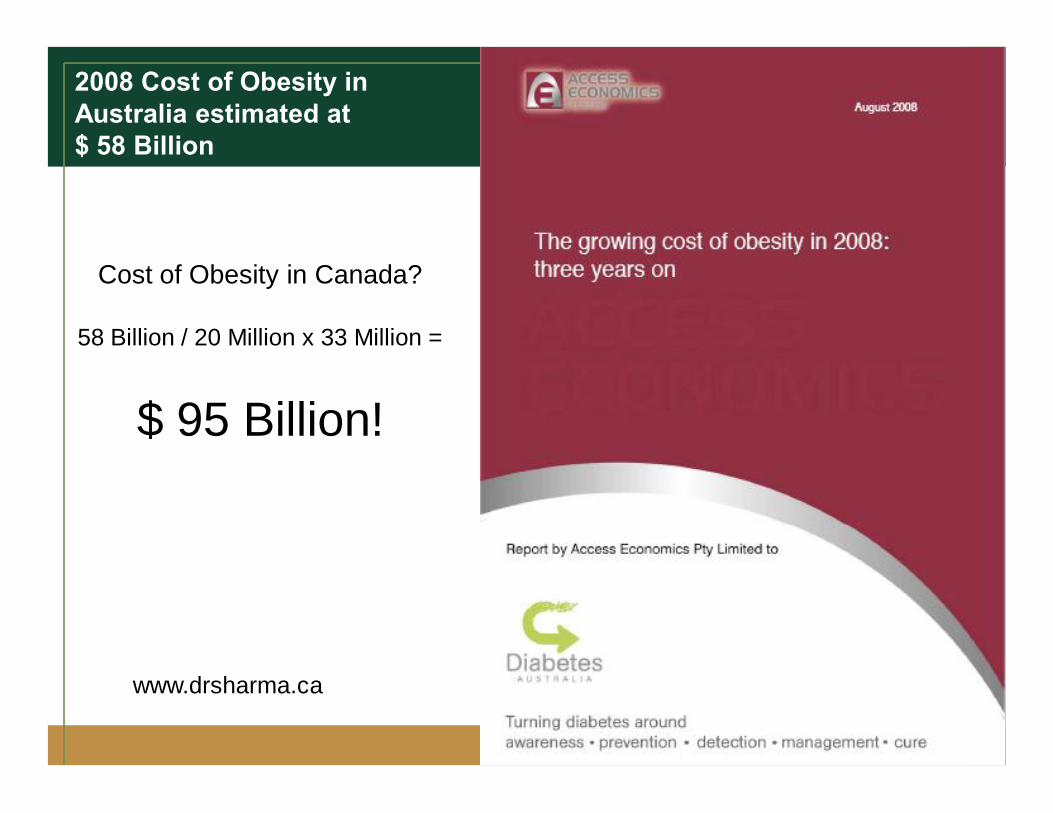
Behaviour
Overeating
Undermoving
What?
Biology
Culture
Environment
Psychology
Why?
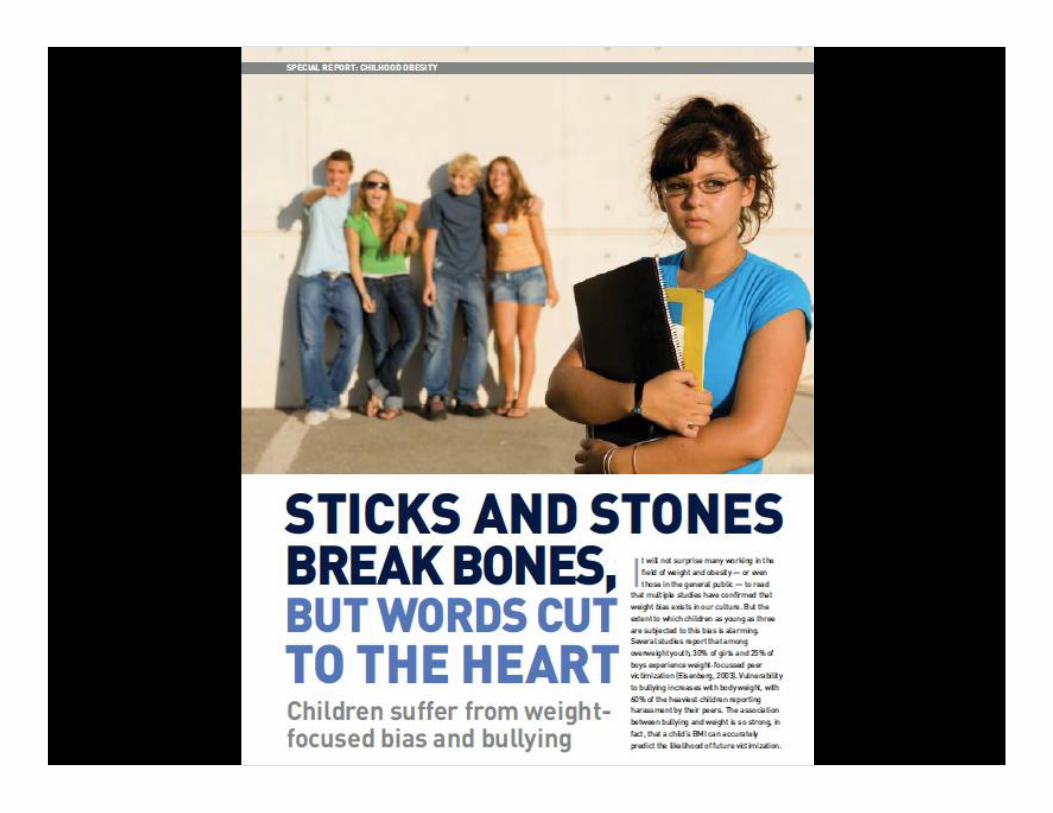
Bias & Stigma éBias & Stigma ê
Sharma AM, 2011
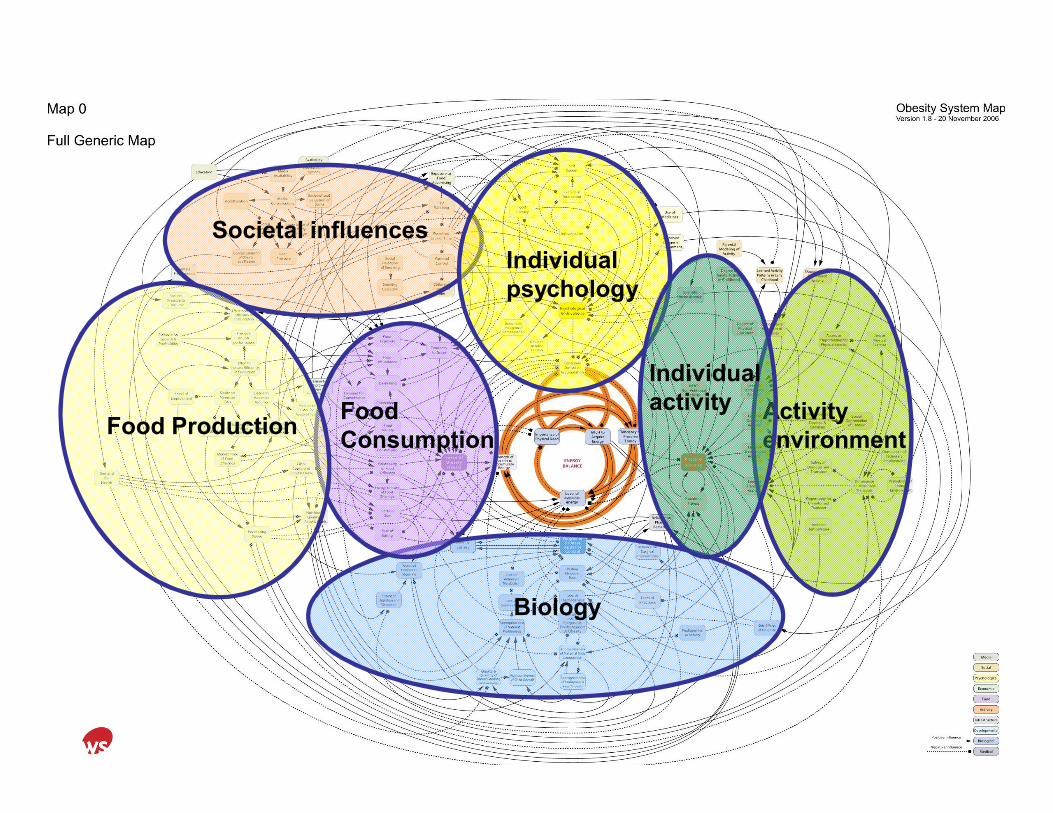
Societal influencesIndividual psychology
Biology
Activity environment
Individual activityFood
ConsumptionFood Production

June 20, 2011June 20, 2011

Why Obesity is More About Calories In than Out
Number of Kcal you can burnburn in a minute
Number of Kcal you can eat or drink in a minute
~5 Kcals>500 Kcals


Our Genes Have Changed!






Depression and Appetite

Addictions

Protection

BMI and Body Fat
DXA scan of two individuals with the same BMI but markedly different percent body fat
European South Asian
Yajnik CS, Lancet. 2004 Jan 10;363(9403):163.
Yudkin & Yainik, Lancet 2004

Edmonton Obesity Staging System (EOSS)
Stage 0
Sharma AM & Kushner RF, Int J Obes 2009
Stage 1
Stage 2
Stage 3
Stage 4
co-morbidity
moderate
moderate
Obesity


EOSS Predicts Mortality in NHANES III
Padwal R, Sharma AM et al. CMAJ 2011

EOSS Predicts Mortality at Every Level of BMINHANES III
Padwal R, Sharma AM et al. CMAJ 2011
Overweight

EOSS Distribution Across BMI CategoriesNHANES III (1988-1994)
15%
28%
47%
10%
5%
17%
64%
14%
Class II
8%
19%
59%
14%
Class I
5%14%
67%
14%EOSS Stage 0EOSS Stage 1EOSS Stage 2
Overweight
ClassIII
Padwal R, Sharma AM et al. CMAJ 2011
50 million
23 million
10 million
6 million

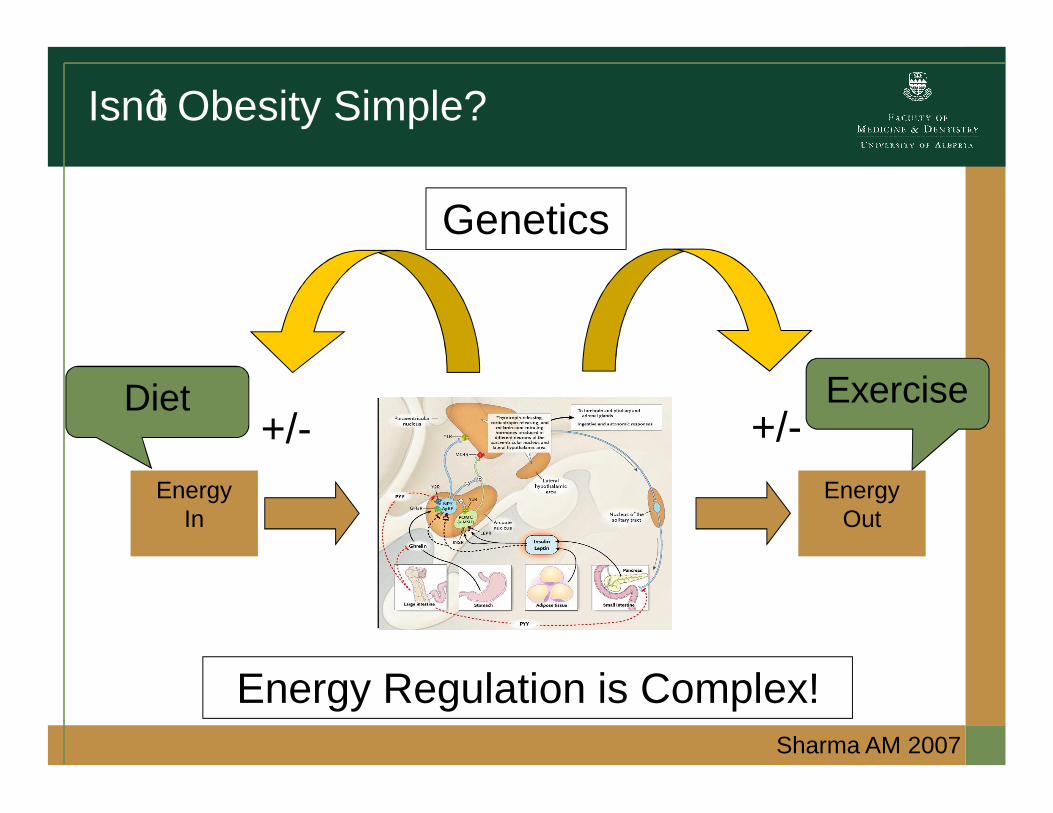
Isn’t Obesity Simple?
EnergyIn
EnergyOut
+/- +/-
Energy Regulation is Complex!
Diet Exercise
Sharma AM 2007
Genetics
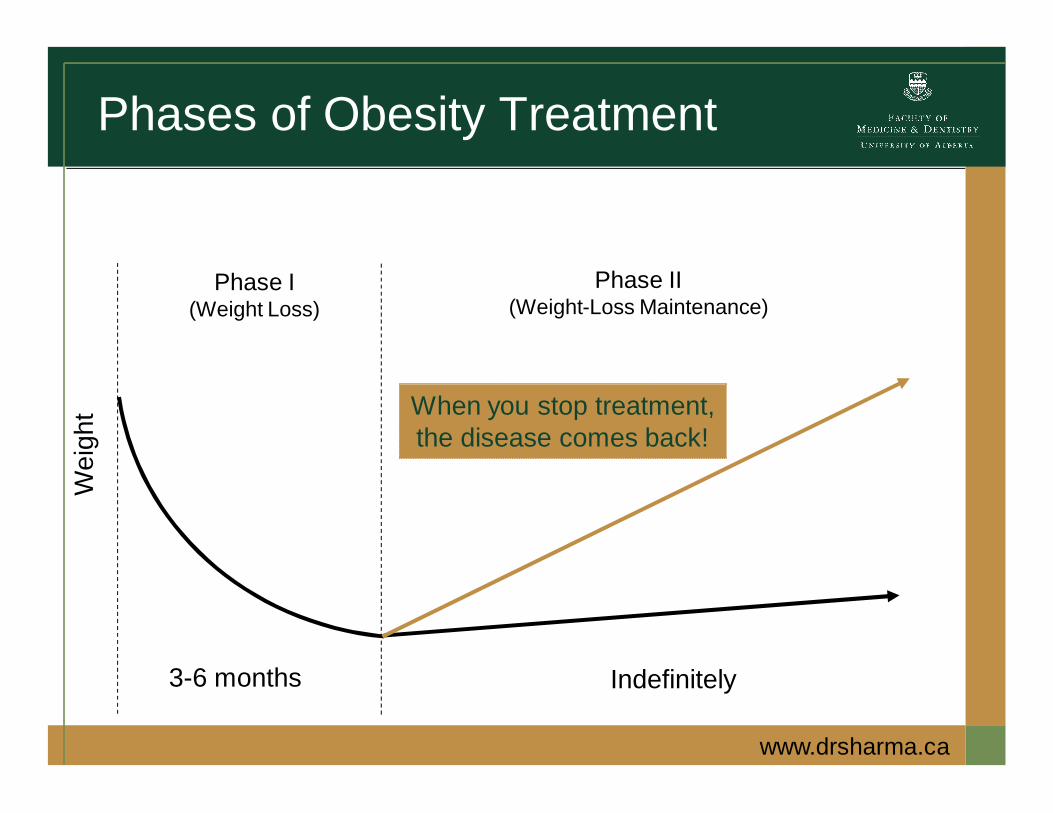
Phases of Obesity Treatment
Phase I(Weight Loss)
3-6 months
Phase II(Weight-Loss Maintenance)
Indefinitely
When you stop treatment,the disease comes back!
Wei
ght
www.drsharma.ca
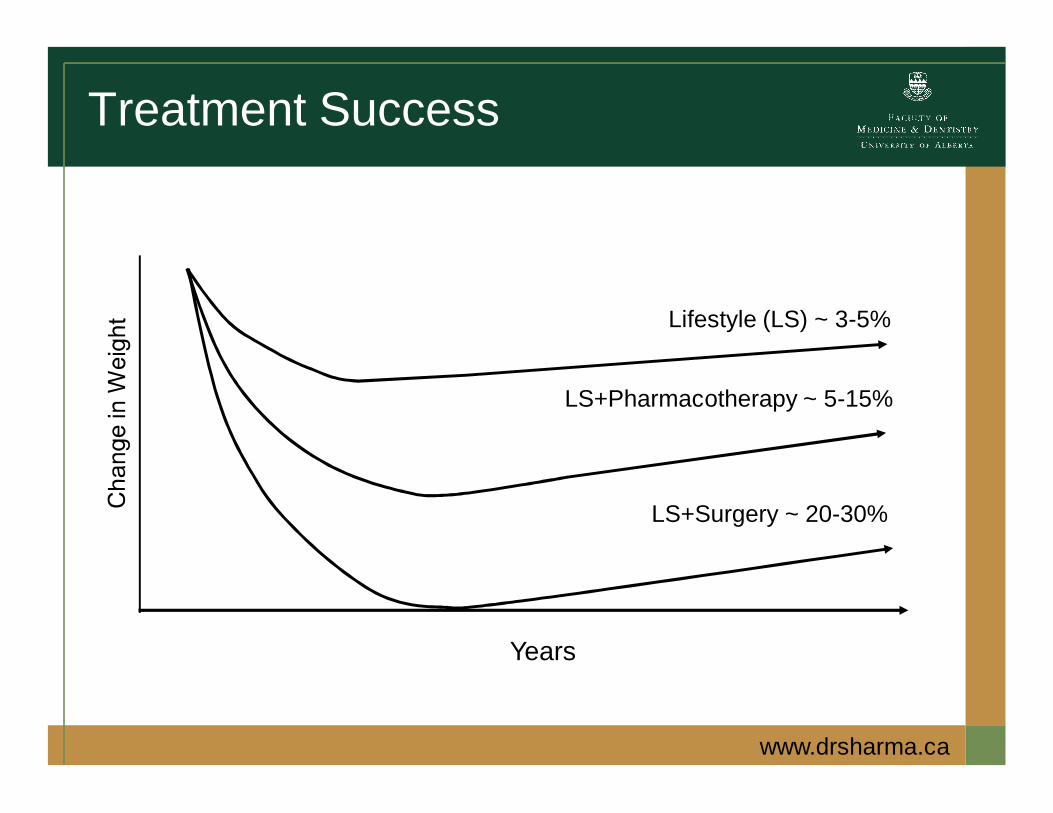
Treatment Success
Years
Lifestyle (LS) ~ 3-5%
LS+Surgery ~ 20-30%
LS+Pharmacotherapy ~ 5-15%
www.drsharma.ca

-8
-6
-4
-2
0
0 1 2 3 4
Wei
ght C
hang
e (k
g)
Years from Randomization
Placebo
Metformin
Lifestyle
Diabetes Prevention StudyMean Weight Change
The DPP Research Group, NEJM 346:393-403, 2002
1 2 3 4
Risk reduction for Type 2 Diabetes:
• Metformin: 31% • Lifestyle: 58%

Common Bariatric Surgical Procedures
AdjustableGastric-Banding
VerticalSleeve-Gastrectomy
Roux-n-YGastric Bypass
www.drsharma.ca

Bariatric Surgery Reduces Mortality in Swedish Obese Subjects (n=2010 vs. 2037)
Sjostrom L et al. NEJM 2007;357:741-52
30% Reduction in All Cause Mortality

Use of Diabetes Medication Before and After Bariatric Surgery (n=2235)
Makary MA et al. Arch Surg 2010;145:726

Surgery resulted in long-term incremental cost–utility ratios of $ <1.000–$40,000 (2009 USD) per quality-
adjusted-life-year compared with non-surgical treatment.
J Gen Intern Med 2011; 26:1183–94



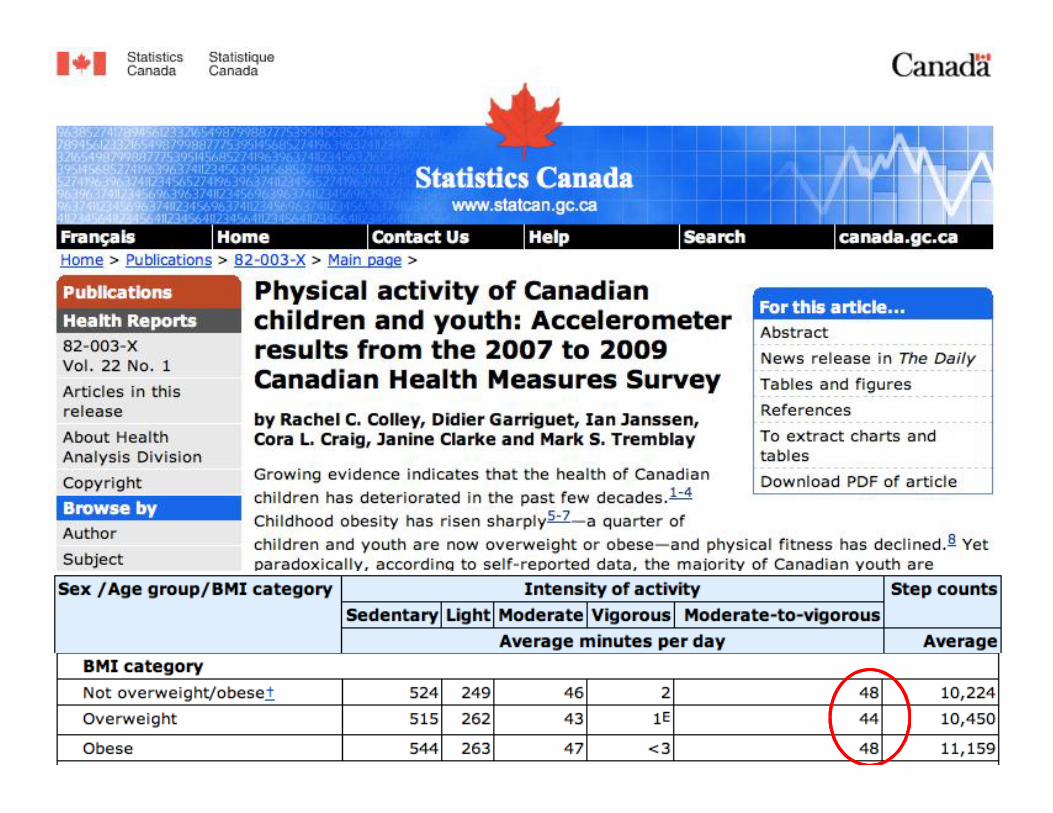
46
Obesity is a Chronic DiseaseRecognize that obesity is a chronicdisease and a root cause of many
other chronic diseases
Obesity care should reflect a chronic disease treatment approach that
is scalable based on patient needs
The service delivery model shouldbe driven by patient needs and
clear clinical objectives
Obesity care should be an integral part of the core health service
delivery system

47
Building the Foundation for Optimal Chronic Disease Management

48
Program Pathway for Coordinating Care

49
Clinical Pathways for Standardization of care
50
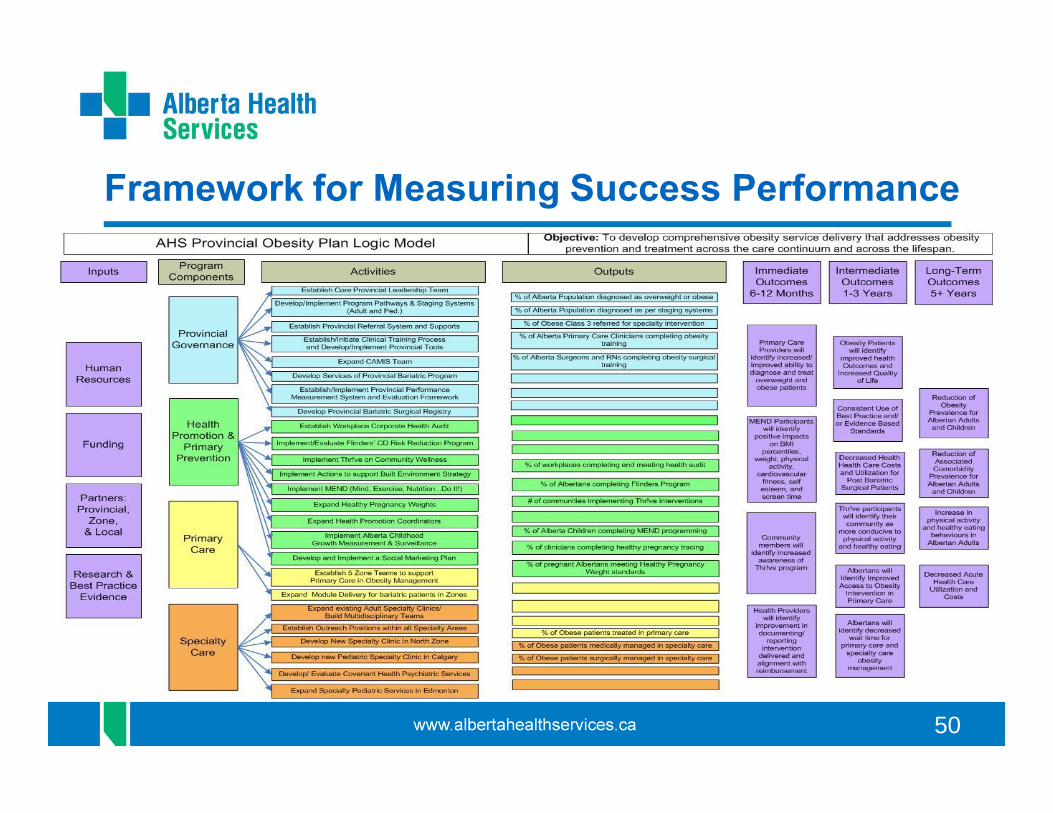
Framework for Measuring Success Performance

www.obesitynetwork.ca