Embed Size (px)
Citation preview

Queensland University of Technology Faculty of Health School of Nursing
TAIWANESE PEOPLE WITH CANCER AND
NON WESTERN MEDICINE (NWM) USE:
A GROUNDED THEORY STUDY
By
王守玉
WANG, SHOU-YU (CINDY WANG), MNurs, BSc
Submitted for the degree of Doctor of Philosophy 2007

i
DISSEMINATION OF THE FINDINGS
Dissemination of the research findings has been undertaken through the course of my
enrolment in Doctor of Philosophy at the Queensland University of Technology
through the following means:
In campus presentation: Wang, S. Y. (2004). Exploring the Use of Non Western medicine (NWM) by People with Cancer in Taiwan: A Grounded Theory Study. Queensland University of Technology, Brisbane, Australia. International conferences: Wang, C., Han, C., Hsu, T. H., Windsor, C., & Barnard, A. (2006). Translation in qualitative research: what is evidence? The 7th International Interdisciplinary Conference-Looking to the Future: Opportunities & Challenges for Qualitative Research, 2006, 14th - 16th July, Gold Coast, Queensland, Australia. Wang, S. Y., Yates, P., & Windsor, C. (2006). Exploring The Use of Non Western medicine By People With Cancer in Taiwan: A Ground Theory Study. 14th International Conference on Cancer Nursing, September 27th – 1st October 2006, The Sheraton Centre, Toronto, Canada.

ii
ABSTRACT
Because of the long and entrenched history of Chinese medicine in Taiwan, people
have traditionally incorporated this knowledge into their health care. With the
appearance and growing acceptance of Western medical practices, multiple medical
approaches have become more and more popular. Yet, despite the strong foundations
of Western medicine in the treatment of cancer in Taiwan, the use of Chinese
medicine continues to be popular (Lin, 1992, p. 114).
The focus of this research is the contextual construction of meanings about non
Western medicine (NWM). The context for the study is Taiwan, the researcher’s
home country. The purpose of the research is to explore the motivations for, and the
processes by which, Taiwanese people with cancer incorporate NWM into their
cancer treatment journey. Utilising a grounded theory approach, this research sought
to explore the social processes by which Taiwanese people with cancer come to use
non Western medicine. Twenty four in depth interviews were undertaken in the
study.
iii
The findings of the study demonstrate that the interactions between people with
cancer and their use of NWM are complex. Taken-for-grantedness emerges as the
core category in the study. The core category situates the use of non Western
medicine outside the institutionalised and regulated domains of health care. More
specifically, the meanings attributed to NWM are embedded in the philosophical
beliefs and social relationships that constitute the lives of the participants.
These findings suggest implications for our understanding of the co-existence of
NWM and Western medicine by Taiwanese people with cancer and the social
processes with which they engage.
Key words: non Western medicine (NWM), complementary and alternative
medicine (CAM), symbolic interactionism, grounded theory, cancer, Taiwan

iv
STATEMENT OF ORIGINAL AUTHORSHIP
The work contained in this thesis has not been previously submitted for a degree or
diploma at any other higher education institution. To the best of my knowledge and
belief, the thesis contains no material previously published or written by another
person except where due reference is made.
Signed:
Date:

v
ACKNOWLEDGMENTS
I would like to express my appreciation to my supervisors, Patsy Yates, Carol
Windsor and Chouh-Jiaun Lin (林綽娟) for their thoughtful guidance, continuing
challenge my thinking, patience, encouragement and tireless support of my work in
completing this PhD thesis. Especially, Carol, she is very generous with her time. We
spend quite a lot of time together to discuss grounded theory and other qualitative
approaches. It is sad that we may not have regular Friday appointment in the future. I
will definitely miss it. In those one or two hours during the years of my PhD study, I
have been learned a lot from her. It had been a great learning experience during my
PhD journey. I am so much in love with grounded theory and qualitative research
now.
I would also like to show my gratitude to my parents (王大全, 陳惠美) for
supporting my study in Australia. They are very generous with their financial support
to provide education to their children. My appreciation is hard to put in words. I also
want to thank my elder brother, Devin (王守吉), my younger sister, Lucy (王守貞),
my friends, Anderson (邱添福), 張貞慧 and Yeats (鄭森) for their encouragement

vi
from Taiwan and my Australian family Gwen and Merv for their English corrections,
emotional support and share their life experiences with me to help me cope with my
PhD study in Australia. I am also grateful to my friends in Australia, especially Tracy
and Katherine (we go through doing qualitative research together and we know how
hard it is), Naomi, Jamie, Sarah and all the other PhD student friends for their
support and company during the highs and lows of my PhD study.
Finally, a very special thank is extended to the anonymous cancer patients in Taiwan
who were very generous and supportive to this study. Without their participation, this
study could not be completed.

vii
誌謝
首先我要感謝我的指導教授,Patsy Yates、Carol Windsor 及林綽
娟老師。感謝她們耐心的指導、訓練我的批判性思考,鼓勵及支持
我完成博士學位。尤其是我的指導教授 Carol,我們花了很多時間討
論紮根理論及其他質性研究法,想到以後與她星期五的討論因博士
論文的完成而結束不免有些感傷,在每週一到兩個小時的討論,在
博士的學習過程中,我從她那兒學到很多。這是一個很棒的學習經
驗,現在我很喜歡紮根理論及其他質性研究法了。
我也要對我的父母致上最誠摯的謝意,感謝他們支持我在澳大利亞
念書,他們總是無私的支持對子女的教育,感謝之心真是筆墨難能
形容。我也要感謝哥哥守吉、妹妹守貞、我在台灣的朋友阿福、貞
慧、鄭森,他們對我的鼓勵。我也要感謝 Gwen 及 Merv 他們英文上
的指導、情緒上的支持和分享他們的人生經驗幫助我渡過博士的學
習過程。我也要感謝在澳大利亞一起學習的朋友們,尤其是翠華、
凱微(我們都是一起做質性研究,我們知道真的很難)。另外還有
Naomi、倢伃、玉苹及其他博士班的朋友們,感謝他們陪我渡過在
博士學習過程中的高潮及低潮期。
viii
最後還要感謝一群台灣的癌症病人們非常支持這個研究,沒有他們
的參與,這個研究就無法完成。

ix
TABLE OF CONTENTS
DISSEMINATION OF THE FINDINGS.................................................................. i ABSTRACT................................................................................................................ ii STATEMENT OF ORIGINAL AUTHORSHIP..................................................... iv ACKNOWLEDGMENTS ......................................................................................... v TABLE OF CONTENTS .......................................................................................... ix LIST OF TABLES....................................................................................................xii LIST OF FIGURES ................................................................................................xiii CHAPTER 1 ............................................................................................................... 1 Introduction ................................................................................................................ 1
Background .......................................................................................................... 1 Cancer and Treatment Approaches in Taiwan...................................................... 4 Purpose of This Study .......................................................................................... 7 Structure of The Dissertation ............................................................................... 9
CHAPTER 2 ............................................................................................................. 10 Literature Review..................................................................................................... 10
Background ........................................................................................................ 10 The Location of NWM in Contemporary Society: A Global Perspective.......... 11 What Is CAM?-The Western Perspective .......................................................... 14 The Use of CAM in Western Societies .............................................................. 20 Eastern Perspectives on Health Care.................................................................. 25
Approaches to Medical Treatment in Eastern Societies............................. 28 The Use of Non Western medicine in Eastern Societies............................ 30
Why Do This Study? .......................................................................................... 36 Summary ............................................................................................................ 38
CHAPTER 3 ............................................................................................................. 40 Methodology ............................................................................................................. 40
Symbolic Interactionism .................................................................................... 41 Origins of Grounded Theory.............................................................................. 46
Grounded Theory ....................................................................................... 48 Definition of Grounded Theory ................................................................. 49 Contested Areas in Grounded Theory ........................................................ 51
Verification versus Generation........................................................... 52

x
Theoretical Saturation ........................................................................ 56 The Use of Literature ......................................................................... 57 Interpretation versus Truth ................................................................. 58 Full Conceptual Descriptions versus Theoretical Codes and Theory 61 Micro versus Macro-Social World ..................................................... 63 Substantive versus Formal Theory..................................................... 64
Methodological Approach.................................................................................. 66 Summary ............................................................................................................ 68
CHAPTER 4 ............................................................................................................. 69 Methods..................................................................................................................... 69
The Elements of Grounded Theory.................................................................... 70 Sample Selection (Participants) ................................................................. 70 Participant Demographics .......................................................................... 73 Interview Approach.................................................................................... 75
One to one interview .......................................................................... 78 Data Collection .......................................................................................... 79 The Utilisation of Memos .......................................................................... 80 Data Analysis ............................................................................................. 81
Theoretical Sensitivity ....................................................................... 82 Comparative Analysis ........................................................................ 84 Open Coding ...................................................................................... 85 Axial Coding ...................................................................................... 86 Selective Coding (Core Category) ..................................................... 88
Validity in Translation of Interview Data........................................................... 90 The Role of the Researcher ................................................................................ 95 Ethical Implications ........................................................................................... 96 Validity and Reliability of This Study................................................................ 98 Summary .......................................................................................................... 102
CHAPTER 5 ........................................................................................................... 103 Incorporating NWM: The Taiwanese Context .................................................... 103
The Context...................................................................................................... 105 The Patterns of Use of Western Medicine and NWM.............................. 107 Forms of NWM Use................................................................................. 126 Regulation of Diet as Therapy ................................................................. 133
Summary (NWM Use as a Social Process)...................................................... 135

xi
CHAPTER 6 ........................................................................................................... 138 Philosophical Beliefs .............................................................................................. 138
Philosophical Beliefs........................................................................................ 139 Traditional Chinese Philosophy ............................................................... 141 Religious Practices ................................................................................... 147 Chinese Proverbs and Self Destiny.......................................................... 165
Belief in Fate .................................................................................... 166 The “Will” of People with Cancer ................................................... 169 The Ethos of “Doing Anything”....................................................... 173
Summary .......................................................................................................... 183 CHAPTER 7 ........................................................................................................... 185 Social Relationships ............................................................................................... 185
Family Connections ......................................................................................... 186 Community Connections.................................................................................. 198 Professional Relationships and Practices ......................................................... 209 Summary .......................................................................................................... 224
CHAPTER 8 ........................................................................................................... 225 Taken-For-Grantedness......................................................................................... 225 “Because after all we are Chinese…” .................................................................... 225
Taken-for-Grantedness ..................................................................................... 229 Implications of the Findings ............................................................................ 231 Limitations of This Study................................................................................. 234 Recommendations for Future Research ........................................................... 236 Conclusion ....................................................................................................... 237
References ............................................................................................................... 238 Appendix I: Participant Information Sheet......................................................... 266
昆士蘭科技大學 研究說明.................................................................................... 269
Appendix II: Consent Form .................................................................................. 271
昆士蘭科技大學 同意書........................................................................................ 273
Appendix III: The Interview Theme List............................................................. 275
會談主題.................................................................................................................. 276

xii
LIST OF TABLES
Table 1 . Age distribution of participants………………………………………….74
Table 2. Educational level of participants………………………………………….75

xiii
LIST OF FIGURES
Figure 1: Taiwanese People with Cancer and Non Western Medicine (NWM) Use ........................................................................................................................... 226

1
CHAPTER 1
Introduction
Background
People with cancer typically confront substantial physical and psychological
alteration to their lives. These alterations often require a long process of adjustment
as patients face many stressors and disruptions. The nature of contemporary cancer
therapy means that patients are often faced with many complex decisions during the
process of adjustment as they consider a variety of different treatment options. For
some patients, this may involve consideration of non-medical approaches to cancer
treatment or, from a Western perspective, treatments commonly referred to as
complementary or alternative (Wang, Yates, & Windsor, 2006).
Treatments as alternatives to accepted orthodox medicine have existed in human
society for as long as therapies have been documented. The ascendency of scientific
medicine from the early 20th century, however, had the effect of suppressing the use
of such therapies. But in the past few decades there has been a growing demand for
2
therapies that have become termed, in Western societies, complementary and
alternative medicine (CAM). In the United Kingdom, in 1998, there were a reported
15 million alternative medicine consultations and more than 40% of general
practitioners who actively advocated CAM (Hunt & Millar, 2000, p. 68; Lewith,
Kenyon & Lewis, 1996, p. 3). In the US it was estimated that $21.2 billion was spent
on CAM in 1997, with $12.2 billion attributed to patient spending (Eisenberg et al.,
1998, pp. 1569, 1571-1572).
In the oncology field, there is also an increasing population in the Western world
using CAM (Cassileth & Chapman, 1996, p. 1026) and this is evidenced in the
growing number of cancer centres integrating selected CAM into their daily care
(Peace & Simons, 1996, pp. 53-54). Yet, despite widespread use, few studies have
explored the perspectives of people with cancer who use CAM and how and why
people come to use CAM. Moreover, while definitions of CAM will depend on the
social and cultural contexts in which health care is provided, the role and meaning of
various contemporary and traditional therapeutic modalities in the treatment of
cancer among different cultural groups has not been explored in any depth.

3
In an earlier study, the responses of nurses working in several Australian
metropolitan hospitals and community care institutions towards people with cancer
who use CAM were explored (Wang & Yates, 2006). The study indicated that nurses
respond in a variety of ways to patients who use CAM. Specifically, this study found
that nurses may be open, sceptical, or ambivalent towards patients who have chosen
to use CAM. Importantly, nurses’ responses to different patients appeared to be
influenced by a range of social and clinical factors. For example, nurses perceived
that patients used CAM for a range of reasons including patients’ past experiences
with health care and the impact of the cancer treatments on patients. Nurses were
also of the view that patients had various different motives for using CAM which
included a desire to achieve comfort or to achieve a cure. These different motives
often resulted in differing nursing responses. The study conclusion argued the
importance of exploring the use of CAM from the perspectives of patients to better
understand the processes by which a person with cancer comes to use CAM (Wang
& Yates, 2006, pp. 289-293).
The researcher has long had an interest in the field of cancer nursing and worked in
this area in Taiwan. When studying for a Master of Nursing (Cancer Nursing) in
Australia, her research focus was an exploration of nurses’ responses to people with

4
cancer who use complementary and alternative medicine. This further developed an
interest in this field. In particular and when working in Taiwan, the researcher
observed cancer patients using both Western medicine and non Western medicine
(NWM). This observation prompted an interest in exploring how and why people use
NWM.
For Taiwanese patients with cancer, the context of cancer treatment decision making
varies considerably from the Western world. In particular, the dominant paradigm
underpinning the meanings and definitions of cancer treatments differ in Western and
non-Western countries. This difference highlights the importance of examining issues
associated with the use of various treatment approaches within different sociocultural
contexts.
Cancer and Treatment Approaches in Taiwan
Cancer has been the leading cause of mortality in Taiwan since 1982 and the death
rate from cancer is increasing each year in Taiwan. The mortality rate from cancer
was 152.88 per 100,000 in the population in 2003 and increased to 163.8 per 100,000

5
of the population in 2005 (Department of Health Taiwan, R.O.C., 2003, pp. 51-53;
Department of Health Taiwan, R.O.C., 2005).
Modern approaches to cancer treatment in both Taiwan and the Western world
generally include one, or a combination of, therapeutic modalities including surgery,
chemotherapy, radiotherapy or biotherapy. Such medical treatments are widely
available in Taiwan and constitute a major component of the health care system.
However, while generally considered CAM in the Western medical world,
Traditional Chinese Medicine and Folk Medicine also constitute dominant health
care systems in Taiwan. The current and official profile of the medical workforce
refers to both physicians (Western Medicine) and Chinese medicine doctors
(Traditional Chinese Medicine) (Department of Health Taiwan, R.O.C., 2001, p. 22).
However, the numbers of practitioners who engage in folk medicine is not clear and
such information is not included in official reports.
In Taiwan, consultation and prescriptions related to Western medicine and
Traditional Chinese Medicine are covered by National Health Insurance (apart from
a certain percentage fee) (Traditional Chinese Medicine Committee, 2001, pp.
280-281). Legislation relating to Traditional Chinese Medicine was also established

6
by the Taiwan Health Department and approved by the Legislative Yuan in 1994
(Department of Health Taiwan, R.O.C., 2001, p. 34). Since then, the use of
Traditional Chinese Medicine has been the subject of greater regulation in Taiwan.
Like Traditional Chinese Medicine, folk medicine is also reported to be popular
amongst Taiwanese people. The main difference between Traditional Chinese
Medicine and folk medicine is that the former stresses the importance of balance
within the body in order to avoid disease, while the latter is closely connected to
religious practices such as going to the temple, using secret herb remedies and
fortune-telling (Chen et al., 1999, pp. 295-296). Folk medicine in Taiwan has thus a
close relationship with Taiwanese religious beliefs and cultural behaviour.
Taoism and Buddhism are the two main religions in Taiwan and they share the
similar aims of a better life and enlightenment (Rodgers & Yen, 2002, p. 215), both
of which maintain a strong influence in Chinese culture. For example, both stress the
principle of “Inn” and “Ko” (cause and effect), that is, a belief that fate determines
health and diseases (Chen, 2001, p. 270). The concept of “knowing fate” involves the
belief that from the moment of birth your life is controlled by fate. No matter what
you do to avoid it, fate will always predominate. Some writers suggest this

7
perception may help people to cope when their disease outcome is not as originally
expected (Chao, 1995, p. 149).
Taiwanese patients may thus hold a diverse range of beliefs about different
approaches to the management of various diseases or symptoms. Patients may
choose one or combination of therapies, including Western medicine, Traditional
Chinese Medicine and folk medicine.
While some suggest that Traditional Chinese Medicine and folk medicine are still,
for most people, a second choice and are mainly used for the management of chronic
disease (Chen, 2001, p. 79), the specific reasons that patients make certain choices
for treatment of diseases such as cancer, are not well understood.
Purpose of This Study
Although the definition of CAM (which will be explored in Chapter 2) is complex,
the term “CAM” is commonly used in Western society to describe a wide range of
therapies including Traditional Chinese Medicine and folk medicine. However, the
term CAM may not adequately describe such therapies in the context of non Western

8
health care systems such as in Taiwan, since in this context, such therapies may not
have the same historical and social meanings.
People with cancer in Taiwan may face a range of decisions and choices about
treatment. These may include choices about whether to use Western medicine, a non
Western medicine approach such as Traditional Chinese Medicine and folk medicine,
or a combination of these two approaches.
The focus of this research is on the contextual construction of meanings about the
use of non Western medicine (NWM). The context for the study is Taiwan, the
researcher’s home country. The purpose of the research is to explore the motivations
for, and the processes by which, Taiwanese people with cancer incorporate non
Western medicine into their cancer treatment journey. Utilising a grounded theory
approach, this study aims to explore the processes by which Taiwanese people with
cancer use non Western medicine.

9
Structure of The Dissertation
This chapter has presented the background of CAM, or so called NWM approaches
to cancer treatments in Taiwan and the purpose of this study. In the second chapter, a
review of the literature is presented which includes the location of CAM in
contemporary society, the use of CAM in Western societies, Eastern perspectives on
health care and the use of non Western medicine in Eastern societies.
The methodology is addressed in the third chapter. The focus of this chapter is on the
symbolic interactionist underpinnings of the study methodology and some contested
areas in grounded theory. Chapter 4 explores the methods used in this study
including sample selection, data collection and data analysis. Further, the role of the
researcher, ethical implications and validity and reliability of this study are also
discussed.
Chapters 5 to 7 present the findings of this study and also examine and compare them
with current literature in the relevant field. The final chapter explores further the
findings and their implications, addresses limitations of the study and pose
recommendations for the future research.
10
CHAPTER 2
Literature Review
Background
Complementary and alternative medicines (CAM) have long existed in human
society. Long before the emergence of modern medical technology, humans relied on
treatments that modern medicine now refers to as CAM to treat diseases in Western
society. Yet, although exposure to modern medicine has continued for a number of
centuries, more and more people are seeking alternative ways to manage their
diseases.
In contrast to the West and because of a long and sustained history of the use of
traditional therapeutic forms in the East, such as Traditional Chinese Medicine in
China and Ayurveda in India, the term “CAM” is not as meaningful. Thus, for the
purposes of the present study, the term “non Western medicine” will be utilised when

11
referring to treatments based on Eastern traditions and other alternative approaches
which may in Western society be referred to as CAM.
The aim of this chapter is to explore the concept of non Western medicine and the
current status of and issues associated with the use of non Western medicine in both
Western and Eastern societies.
The Location of NWM in Contemporary Society: A
Global Perspective
The use of NWM or CAM is a worldwide phenomenon and has received recognition
as such. International organizations and national institutions have successively
established departments or published reports regarding CAM. For example, the
Research Council for Complementary Medicine was established in 1983 in the
United Kingdom (The Research Council for Complementary Medicine, 2003, p. 1).
In 1992, the National Institute of Health of the U.S. Department of Health and
Human Services, established the National Centre for Complementary and Alternative
Medicine (NCCAM) (National Centre for Complementary and Alternative Medicine,

12
2003, p. 1).
The World Health Organization (WHO) states that complementary and alternative
medicine (CAM) is used alongside traditional medicine (TM). WHO refers to CAM
as a wide range of health care interventions that were not originally developed in
Western countries or are not integrated into the mainstream health care system
(World Health Organization, 2002, p. 7). In 2001, a major report on the Legal Status
of Traditional Medicine and Complementary/Alternative Medicine: A Worldwide
View was published by the WHO and a total of 123 out of 191 member countries
contributed to this report from six continents worldwide (WHO, 2001, p. ix). This
report provides comprehensive references regarding the utilisation of traditional
medicine and complementary and alternative medicine in different countries.
Background information, statistics, regulation, training and education, insurance
coverage and various models of care and policy are amongst the many issues
discussed in this report (WHO, 2001, p. 4). However, as Taiwan is not a member of
WHO, the report does not include information about Taiwan.

13
Subsequent to the 2001 report, a number of short or long term plans related to CAM
have been published by the WHO and other key health organizations. For example, a
report on Traditional Medicine (TM)/complementary and alternative medicine
(CAM) was presented in the WHO Traditional Medicine Strategy 2002-2005 in
2002. This three year strategy sets out plans for action regarding CAM in the areas of
policy, safety, efficacy, quality, access and reasons for use (World Health
Organization, 2002, p. iv). Similarly, the National Centre for Complementary and
Alternative Medicine (NCCAM) in the United States published Expanding Horizons
of Healthcare: Five Year Strategic Plan 2001-2005 in 2001. The NCCAM report
identifies strategic areas including investing in research, training CAM investigators,
expanding outreach and facilitating integration (NCCAM, 2001, p. 3).
In addition, a number of journals dedicated to CAM have emerged1. Such journals
explore the many uses of CAM and present various forms of evidence in support of
CAM. Hundreds of websites regarding CAM have also appeared on the internet,
although these sites often present little valid evidence on the therapies they are
promoting (Spencer, 1999, p. 10).
1 The journals include Evidence-based Complementary and Alternative Medicine, Alternative Therapies in Clinical Practice, Alternative Therapies, Journal of Alternative and Complementary Therapies, Alternative Therapies in Health and Medicine and Mind-Body Medicine.
14
Such reports and publications highlight the important role of CAM in modern health
care systems across the world. More and more organizations have subsequently
established departments or sub-departments to research CAM. An example is the
National Health and Medical Research Council (NHMRC) in Australia which has
just provided AUS$ 5 million to fund research into CAM (NHMRC, 2006, p. 1).
What Is CAM?-The Western Perspective
There is a long history of the use of CAM in the search for effective treatment
processes. Yet, with the evolution of medical treatment, those therapies perceived as
alternatives to mainstream treatments have varied considerably. In fact, in Western
society, many accepted medical treatments that preceded contemporary technological
advances are today referred to as CAM.
15
Definitions of mainstream and other forms of treatments in Western societies thus
derive from the dominance of the scientifically based medical model. As a result,
CAMs and their predecessors are generally described in Western societies as
unproven remedies and techniques (Cassileth & Chapman, 1996, pp. 1026-1027).
The term CAM has only appeared in the past few decades. Terms similar in meaning
have been used over the centuries to delineate types of approaches to the treatment of
the ill. For example, natural healing (nineteenth century), drugless healing (early
twentieth century) and holistic healing (since the 1970s) are all terms which have
been used to describe other than mainstream approaches to maintaining health
(Whorton, 1999, pp. 16-17). In the 1970s and 1980s, terms such as “self-contained”
and “alternative medicine systems” were utilised in many fields to describe diagnosis
and aetiology of diseases. Gradually, such therapies have come to be referred to as
alternative medicine (Peters et al., 2002, p. 5).
In addition, there are a variety of treatments that are increasingly perceived as
complementary to conventional therapies, including relaxation, massage or
aromatherapy and are referred to as complementary medicines. The boundary

16
between alternative and complementary medicine is, however, not clear as some
authorities use the terms as synonyms (Peters et al., 2002, p. 5).
In Western Society, CAM has been defined as “diagnosis, treatment and/or
prevention which complements mainstream medicine by contributing to the common
whole, by satisfying a demand not met by orthodoxy or by diversifying the
conceptual frameworks of medicine” (Ernst & Fugh-Berman, 2002, p. 140). The
Cochrane Collaboration has accepted the foregoing definition (Engebretson, 2002, p.
177; Ernst & Fugh-Berman, 2002, p. 140). The National Centre for Complementary
and Alternative Medicine (2003) in the United States also defines complementary
and alternative medicine as “a group of diverse medical and health care systems,
practice, and products that are not presently considered to be part of conventional
medicine” (p. 1).
The American Cancer Society (2006) guide for the use of complementary and
alternative methods states that these forms of therapies are distinct. Complementary
medicine is described as therapy that is used alongside mainstream health care and
alternative medicine is that which is used instead of the standard medical approach.

17
(p. 1). In this definition, alternative therapies thus refer to (scientifically) unproven
methods that are used as substitutes for conventional therapies, while complementary
therapies are perceived as supportive therapies to assist conventional therapies
(American Cancer Society, 2000, p. 23).
This distinction is similar to that proposed by a number of authors who define
complementary therapies as those that supplement conventional therapies to promote
healing, increase comfort and enhance health. In contrast, alternative therapies are
conceived of as remedies or regimens that substitute for mainstream treatment
(DeKeyser et al, 2001, p. 42; Stevenson, 1997, p. 49; Engebretson, 1999, p. 214).
Other authors argue that complementary and alternative therapies are recognised as
those treatments that, at a particular historical point, do not integrate into the
conventional treatment system, but that may become less marginalised over time
(Chez et al., 1999, p. 33). In addition, CAMs are also defined as those treatments
generally not taught in western medical schools or are perceived as less applicable in
medical curricula (Eisenberg et al., 1993, p. 246).

18
Thus, a predominant view in the Western literature is that complementary therapies
supplement orthodox medical treatment and alternative therapies are perceived as
non-mainstream and are used instead of conventional therapies. While these
distinctions may appear to provide some clarity, there is a notable lack of precise
definition of what comprises conventional and non-conventional therapies.
Various terms are thus used to describe these treatments; such as, complementary
therapy, alternative therapy, unconventional therapy, complementary medicine (CM),
alternative medicine (AM) and complementary and alternative medicine (CAM).
One feature of these therapies is that most have a tradition that is not based in
Western culture or in earlier Western medicine. Moreover, these therapies are often
seen as more holistic, viewing the individual as a whole person rather than focusing
on physical signs and symptoms (Albrecht, Higginbotham & Freeman, 2001, p. 27).
According to the literature and based on the above definitions, the most popular
CAM in Western countries include:
∗ Herbal medicine, such as, Traditional Chinese Medicine or ayurveda

19
∗ Acupuncture
∗ Diet and nutrition; for example, macrobiotics and shark cartilage
∗ Mind-body techniques, such as, reflexology, prayer and meditation
∗ Manual healing methods; for example, chiropractic therapy
(Cassileth & Chapman, 1996, pp. 1028-1031; Parkman, 2001, p. 37; Cassileth, 1998,
p. 299; Cunningham & Herbert, 2000, pp. 165-166).
From the above, we can conclude that just as approaches to maintaining health and
the treatment of disease have differed considerably across cultures throughout history,
meanings attributed to CAM may diversify or shift within different social contexts
(Low, 2001, p. 107).

20
The Use of CAM in Western Societies
During recent decades, there has been a growing tendency towards the use of CAM
in Western society. Ott’s (2002) study estimated that 7%-64% of people worldwide
with cancer use CAM alongside other treatments (p. 162). A survey of 1539 adult
respondents in the United States indicated that 34% had used at least one kind of
CAM in the previous year, the most commonly used being acupuncture and
chiropractic (Eisenberg et al., 1993, pp. 246, 248-249).
In assessing this trend, a 1997 survey of 1500 Americans estimated that 42% of the
sample had used some kind of CAM during the previous year (National Council
Against Health Fraud, 1998, p. 1). A comparison of surveys of random samples of
1539 American householders in 1990 and 2055 American householders in 1997,
found a 380% increase in the use of herbal medicine (one kind of alternative therapy)
(Eisenberg, et al., 1998, p. 1574).

21
In England, a population based survey (n=2668) found that 10.6% of adults in
England had visited a CAM practitioner in the last 12 months and 46.6% of the
population were life-time users. Furthermore, it was estimated that annual
out-of-pocket expenses for these therapies constituted ₤450 million (AUD 1224
million dollars) (Thomas, Nicholl, & Coleman, 2001, pp. 2-6). Similarly, an
Australian study identified that 57% of the population in the state of Victoria had
utilised CAM in the past five years and had spent $AU50 million dollars per year on
these therapies (MacLennan et al., 1996, p. 569).
Thus, the above studies indicate that the use of CAM has grown significantly in
Western society and it has assumed an increasingly important role in the Western
health care system. Furthermore, results from a national survey in the US of people
who use both approaches (CAM and conventional treatment), found that 79% of
participants perceived that a combination of both achieved a better outcome
(Eisenberg et al., 2001, p. 344).
Despite the apparent popularity and extensive usage of CAM in the West, a 1997
survey reported that only 38.5% of Americans discussed CAM with their physicians

22
(Decker, 2000, p. 49). Although patients and doctors are often seen as mutually
deciding upon optimal treatment choices (Charles, Gafni & Whelan, 1999, p. 652), a
1997 national survey which investigated perceptions about CAM relative to orthodox
treatment reported that 63%-72% of study participants did not tell or only partially
informed their medical doctors that they were using CAM. The most common
reasons cited (more than 60% of participants) were that “it wasn’t important for the
doctor to know” and “the doctor never asked” (Eisenberg et al., 2001, pp. 344,
348-349).
One explanation for this situation is that health providers may not provide a trusting
environment in which patients feel comfortable and relaxed talking about CAM.
Moreover, some health professionals lack knowledge of CAM (Cassileth, 1998, p.
301; Cassileth & Chapman, 1996, p. 1032). As a result, studies suggest that patients
seek information about CAM from alternative sources such as complementary
medicine networks or by word of mouth (Strasen, 1999, p. 250; Ades & Yarbro,
2000, p. 625). This suggests that health professionals may not be aware that patients
are using CAM and that the extent of use of CAM, as an option for maintaining
health and/or treating disease, is under-reported.

23
As noted, the predominant criticism of CAM in Western societies is that they do not
have scientific evidence to support their use. Yet, for some therapies classified as
CAM, there is increasing scientific evidence to support their efficacy. Vickers and
Cassileth (2001) reviewed sixteen clinical trials of acupuncture-point stimulation for
nausea and vomiting related to chemotherapy, eleven of which found significant
improvements following the use of acupuncture treatment (p. 229). An earlier
meta-analysis of 22 randomised controlled trials (RCTs), involving 1042 patients in
total, found that acupuncture is effective in treating migraine (Melchart, et al., 1999,
p. 784). There is also some evidence that acupuncture is particularly helpful for
painful muscle spasms. In a survey of 183 cancer patients who had used acupuncture
treatment, 52% reported that the treatment relieved their cancer pain (Twycross,
1994, pp. 533-534).
While the evidence base is limited and contradictory, such research has seen a
blurring of the boundaries between orthodox Western medicine and CAM in the
Western world. For example, America’s Food and Drug Administration (FDA) has
now identified acupuncture as a safe and effective medical intervention (Gecesdi &
24
Decker, 2001, p. 37). The World Health Organization (WHO) has also acknowledged
that acupuncture can effectively treat more than 100 different signs and symptoms,
such as headache and chronic pain (Gecesdi & Decker, 2001, p. 37). The relatively
recent endorsement of acupuncture as an effective treatment has occurred with the
emergence of some empirical evidence that acupuncture may stimulate the brain to
release endorphins, the natural pain-killing hormones, which reduce the perception of
pain (Shen & Glaspy, 2001, pp. 148-149).
Nonetheless, a major obstacle to the effective co-existence of CAM in Western
societies is still a lack of scientific evidence to support its use. Critics claim that the
evidence available is not of a high level and often flawed (Tulder et al., 2002, p. 7).
For example, a Cochrane Library systematic review of eleven randomised controlled
trials (RCTs) on the use of acupuncture for low back pain concluded that there is
limited evidence of the effectiveness of this treatment (Tulder et al., 2002, p. 10).
A lack of agreement over what constitutes evidence further contributes to a diversity
of views in this area. Chi (1994) argues that the monopoly Western medical
practitioners enjoy over medical resources reinforces the scientific approach to
25
evaluation of treatment and ignores the integral link between culture and the efficacy
of traditional or alternative treatments. In other words, as Chi (1994) notes, it is
culture rather than science that defines the efficacy of alternative treatments. What is
important, according to Chi (1994), are the effects that people are looking for in their
use of other than mainstream Western medicines (pp. 308-309).
Eastern Perspectives on Health Care
Differences exist in the meanings attributed to non Western medicine in Western and
Eastern cultures. Culture may influence health care professionals’ practices, beliefs,
preferences and standards, thereby guiding their practice (Thomas, 2002, p. 78).
Culture refers to views about social, physical, biological and economic
environments. Differences in perspectives derive from social requirements and
various types of beliefs, behaviour and values (Gilbert, 2002, p. 75). Hence, it is
necessary to explicate the different philosophical approaches towards diseases and
health in Western and Eastern cultures.

26
Western medicine focuses on evidence-based practice and emphasises the critical
requirement that practices are based on plausible evidence established by scientific
research methods and in particular, randomised controlled trials. In contrast, Eastern
medicine places emphasis on experience more so than scientific evidence. Qi (Chi)
(energy flows inside the human body, one of the elements that is important in
utilising Traditional Chinese Medicine) is one example that can be used to explain
the implications of these differences. That is, there is no evidence to explain the
existence of Qi (Chi) in the scientific world and indeed there may be no scientific
methods available to show that Qi (Chi) does exist (Hufford, 2002, p. 20). Supporters
of non-Western approaches to health care argue, however, that while it is difficult to
scientifically test such treatments, there is no reason to forsake their use (Vickers,
2000, p. 26).
Western medicine also typically focuses on the treatment of specific diseases and
diseases are conceptualised as malfunctions of particular parts of the body. The
objective of Western medicine is to then improve or reverse malfunctions through
medication or surgical intervention.

27
Eastern medicine (such as Traditional Chinese Medicine), on the other hand, is
focused on what is wrong with the body as a whole rather than specific parts of the
body. Diseases are often seen, for example, as being caused by the disturbance of
Yin and Yang inside the body. The purpose of therapy or medicine is to restore these
two components (Spencer, 1999, p. 6).
Therefore, Western medicine generally perceives the human body as a machine and
medicine as a mechanism to eliminate symptoms and enhance the body’s
performance. However, according to Eastern medicine, the body is viewed as a
“garden” where medicine cultivates health in order to maintain or improve the
human body’s functions (O’Connor, 2000, pp. 46-47; Thomas & Bright, 2002, p.
84). The human body is seen as a whole entity that needs to be cultivated in order to
maintain normal function (Shih, 1999, p. 6).
Furthermore, Engebretson (2002) argues that therapies typically defined as CAM in
the Western world are more focused on systemic problems rather than specific
symptoms or diseases. As such and from an Eastern philosophical stance, the
randomised controlled trial (RCT), by attempting to isolate cause and effect

28
relationships, may block aspects of the remedy that may affect the interventions and
outcomes (pp. 183-184). As such, Engebretson (2002) notes, “it is important to keep
in mind that absence of evidence is not evidence of absence” (p. 184).
Understanding this contradiction is important in understanding the differing
epistemologies of Western medicine and Eastern medicines. The approaches to
obtaining evidence in Western medicine may not apply to many non Western
medicines, including Traditional Chinese Medicine (Easthope, 2003, p. 2; Carter,
2003, p. 134).
Approaches to Medical Treatment in Eastern Societies
In Western countries, patients who are ill are more likely to seek conventional
approaches (Western Medicine). However, if not satisfied, patients may look for
alternatives such as Traditional Chinese Medicine and acupuncture (non Western
medicine). On the other hand, Traditional Chinese Medicine and acupuncture have

29
been used to treat and prevent diseases for over 3000 years in China and are viewed
by many as mainstream health–enhancing procedures from the point of view of
Eastern tradition (Smith-Fassler & Lopez-Bushnell, 2001, pp. 36-37). People who
come from an Eastern background, therefore, may not view Traditional Chinese
Medicine or acupuncture as complementary or alternative, but rather as the only
treatment, or at least an integral medical procedure to be used for maintaining health
or treating health problems.
There have, however, been substantial changes over the past century in the nature of
health care systems in many Eastern countries, as the rise of modern scientific
medicine and its achievements have become integrated into Eastern systems.
Historically and before the appearance of Western missionaries in 1860, Traditional
Chinese Medicine was the mainstream medical treatment in Taiwan. However, the
Western influence was significant in transforming health care and this was reflected
in the relatively rapid and widespread establishment of Western medical clinics (Hu,
1999, p. 92). This transformation was reinforced during the five decades of Japan’s
occupation of Taiwan (1895-1947) when the practice of Chinese medicine was
suppressed and Western medicine schools flourished.

30
During this period (1895-1947), over 2800 practitioners were trained in Western
medicine and thus the Western model rapidly assumed the status of mainstream
treatment within the health care system in Taiwan (Chi, 1994, pp. 310-311; Hu,
1999, p. 92; Hu, 1999, p. 187). It is within the context of the relatively recent
introduction of Western medicine into health care in Taiwan that this study seeks to
explore perceptions of and motivations for the use of non Western medicine.
The Use of Non Western medicine in Eastern Societies
The following studies show the popularity of NWM in Eastern cultures. A Taiwanese
cancer study reported that 64% of the participants use Chinese Medicine, with the
cost of US$40-2000 dollars per month for 70% of participants (Liu et al., 1997, p.
37). A Japanese cancer study reported that 32% of the patient informants were non
Western medicine users (Eguchi, Hyodo, & Saeki, 2000, p. 30).

31
While changes within health care systems and government policies have been
substantial, traditional cultural beliefs about health and illness amongst Eastern
populations remain important for many. In Taiwan, although Western Medicine
became increasingly dominant during the early twentieth century, Traditional
Chinese Medicine retained an important role in Taiwanese people’s daily lives. For
example, the Traditional Chinese Medicine Committee was established in 1987 by
the Health Department to plan for and deal with issues such as administrative matters
and research and development regarding Traditional Chinese Medicine in Taiwan
(Department of Health Taiwan, R.O.C., 2001, p. 34). Since its establishment, this
committee has completed a range of projects, including setting up regulatory systems
for Traditional Chinese Medicine, giving licences to pharmaceutical companies,
encouraging pharmaceutical companies to develop new types of medication, and
establishing a clinical trial environment for Traditional Chinese Medicine
(Traditional Chinese Medicine Committee, 2003, p. 195).
Therapeutic modalities that are commonly used include those based on different
ethnic traditions (for example, Traditional Chinese Medicine and Ayurveda),
understanding of wellness and health (reflexology and aromatherapy as examples)

32
and other alternative approaches to scientific reasoning (such as, naturopathy and
chiropractic) (Thorne et al., 2002, p. 671).
According to the committee, certain treatments are considered medical procedures;
such as Traditional Chinese Medicine for internal use and acupuncture treatment.
However, other items not considered medical procedures include herbs for external
use, massage, foot massage, qigong and prayer, because all are non internal
medicines or non invasive procedures (Traditional Chinese Medicine Committee,
2001, p. 29; Traditional Chinese Medicine Committee, 2003, pp. 195-196).
Nevertheless, all such therapies are reported to be commonly used among Taiwanese
people.
The importance of some cultural beliefs in shaping the meanings attributed to such
therapies in Eastern countries is suggested by a number of authors. For example,
according to Domino and Lin’s (1993) study, which investigated 138 Taiwanese
college students, the cancer metaphor identified as the most important was “a
thunderclap in fine weather” (p. 52). Such beliefs influenced a person’s view about
the type of treatment that may be sought for an illness such as cancer. A Taiwanese

33
study by Duh (1992), similarly reported that only 32% of breast cancer patients
relied on Western medicine alone and 68% of patients sought a combination of both
Western medicine and folk medicine. Moreover, religious ceremonies were used by
92% of the study patients (p. 130).
Wang (1990) found that the choices of Taiwanese patients in relation to treatment
were dependent upon the specific diseases or symptoms that manifested. His study
found that more than 80% of participants chose Western medicine in the cases of
fever or external bleeding and 83.6% perceived Western medicine as the better
approach in the case of cancer. However, only 44.1% of participants chose Western
medicine when suffering from less specific symptoms such as low back pain (Wang,
1990, p. 26). Wang’s (1990) study also reported that more than two thirds of
participants incorporated Chinese medical treatment and Chinese medicine remedies
when recovering from an illness and 85.7% supported the use of these treatments
following the delivery of a baby (p. 26). Chiou’s (1999) study of people with ESRD
(end-stage renal disease) receiving hemodialysis in Taiwan found that folk remedies
such as herbs and food, Traditional Chinese Medicine prescribed by doctors, and

34
Chinese exercises were commonly used in combination with the scientific
technological approach of dialysis (p. 401).
The above studies indicate that Traditional Chinese Medicine and folk medicine
continue to flourish, despite the growth of Western medicine. Importantly, the
studies also suggest Taiwanese patients seem to have particular conceptions of the
role of such therapies in different health situations. Traditional Chinese Medicine,
seen by many Taiwanese as gentle and traditional health concepts, continues to be
valued by patients for maintaining and restoring health in many different situations
(Chen et al., 1999, pp. 295-296). In fact, more and more hospitals have combined
Eastern and Western medicine in health care systems to accommodate traditional
cultural beliefs, a practice rarely observed in Western medical systems.
The perceptions of patients from Eastern countries about the use of non Western
medicine are thus likely to vary from those of Western countries. The use of some
types of treatment, such as Traditional Chinese Medicine and acupuncture, notably in
palliative settings, are more common in Eastern countries than in Western society.

35
While many forms of traditional treatments continue to be used by Taiwanese
people, the extent to which they are openly discussed between health professionals
and cancer patients today is unclear. For example, one survey of 138 terminal cancer
patients in Taiwan found that 81.9% of patients had used at least one kind of
treatment defined in Western terms as a CAM, but more than half the users (56.3%)
had not informed their doctors of this practice. Moreover, 12.3% of the participants
discounted Western medicine because they were using non Western medicine (Hsin
et al., 1996, p. 129). A further Taiwanese study found that 67.2% of study
participants used non Western medicine while undergoing chemotherapy and that
information on non Western medicine was drawn from sources other than physicians.
In this study 10.9% gained information from Chinese Medicine practitioners with
most information (79%) obtained by word of mouth (Liu, et al., 1997, p. 39).
The term “CAM” has been created in the Western literature. However, the meaning
of “CAM” in Eastern cultures differs to that described in Western literature.
Traditional Chinese Medicine and acupuncture for example may not be defined as
CAM in this context. As such, studies which explore the meaning and role as well as

36
the process of using different treatment approaches need to acknowledge the
importance of this sociocultural context. Since the use of non Western medicine is
likely to have different meanings in Eastern countries, it is important that further
research is undertaken to explore these issues.
Why Do This Study?
As noted, many people across the world today have embraced non Western medicine
and sought to combine western medical care and non Western medicine in order to
maintain health or overcome health problems (McCabe & Kenny, 2003, pp.
259-260). In Western societies, there are increasing numbers of people using non
Western medicine (CAM), and notably people with cancer. In Eastern societies,
despite the expansion of western medical systems, the use of non Western medicine
has remained a central part of health care.

37
Because there are significant differences between Western and Eastern cultures in
relation to how people view and approach their disease, the understanding of
people’s uses of non Western medicine (CAM) from different cultures is especially
important. Very few published studies (Hsin et al., 1996, pp. 127-137; Chiou, 1999,
pp. 398-407; Cho, 2000, pp. 123-135) have addressed the use of various treatment
options within an Eastern culture and no published interpretive studies have been
identified. Furthermore, very little is known about Taiwanese people with cancer and
their NWM use.
The purpose of this study is to explore the motivations for Taiwanese patients’ use of
NWM and the processes by which people with cancer incorporate NWM into their
cancer treatment journey.

38
Summary
According to the literature, NWM is widely used by people in both Western and
Eastern societies. This chapter has explored the background to the use of what has
been defined as CAM in the Western world. It has also considered various different
perspectives on the use of such therapies. It has been argued that different views exist
between Western and Eastern societies regarding NWM. As such, it has been
suggested that people with cancer may make different choices and decisions
regarding their treatment and care.
It is important therefore to explore why and how people from various sociocultural
contexts use and integrate NWM into their health care. There is a paucity of studies
in Eastern literature which explore this issue, especially from a qualitative
perspective. This study aims to explore the motivations for patients’ use of NWM
and the processes by which Taiwanese people with cancer incorporate non Western
medicine into the cancer treatment journey.

39
The following chapter presents a discussion of and justification for the methodology
of grounded theory which was applied in this study.

40
CHAPTER 3
Methodology
This chapter develops the theoretical framework that underpins this study. In so
doing, the chapter addresses the theoretical concepts that inform grounded theory and
some dilemmas that have arisen in the interpretation and application of those
concepts. The intent here is to construct a coherent grounded theory framework that
is explicit in its implications and as such seeks to overcome some of the problems
inherent to many grounded theory works.
Grounded theory was first developed by Glaser and Strauss in the 1960s and was
introduced into nursing education as a distinct research methodology in the 1970s.
The work of these authors was grounded in a critique of the dominant tradition of
social inquiry that sought to impose “enduring” theoretical propositions on to data in
the study of the social world. Glaser and Strauss (1967) argued that this approach, in
assuming an priori “fit” between theory and empirical data, was merely
“opportunistic” and provided little opportunity for genuine knowledge development
(pp.1-3). In so arguing, these authors proposed an approach to social inquiry that

41
focused on the discovery, rather than the testing, of theoretical explanations. Thus
“generation” rather than “verification” was the essential rationale for the
development of grounded theory.
Although Glaser and Strauss largely avoid any explanation of the theoretical origins
of their work, the assumptions that underpin grounded theory clearly derive from the
sociological orientation of symbolic interactionism. Hence, it is necessary to address
the key tenets of symbolic interactionism in order to provide some background
understanding of grounded theory.
Symbolic Interactionism
Symbolic interactionism developed, in large part, as a critique of the biologically
based explanations of the social world and the individual. The two most notable
contributors to the interactionist body of thought are George Herbert Mead
(1863-1931) and Herbert Blumer (1900-1987).
At the start of the twentieth century, Mead was a lecturer in philosophy at the
University of Chicago and it was through his work with philosophy students that the

42
basic theoretical tenets of symbolic interactionism were formulated. Subsequently,
through the work of theorists such as Blumer, Lindsmith and Becker (Strauss in
Mead, 1956, p. xiv), and later Glaser and Strauss, Mead’s influence extended to
sociology (Cheek et. al., 1996, p. 113). Mead’s influence on the tradition of
sociology is largely through his conceptualisation of the (human) self. Mead (1932)
indicated that human beings have selves unlike other animals and further, that the
self is constructed through a process and this process establishes the human’s mind
(p. 80). Furthermore, he argued that the process was one wherein the human mind
and the world are engaged in an ongoing process of interaction and that this process
has dimensions both internal and external to individuals (Mead, 1932, p. 180).
According to Mead (1956), we “get at” the social process by moving from the
outside to the inside “to determine how such experience does arise within the
process” (p. 122). In other words, understanding the social process starts with
observable activities (or social acts) and moves to the experience (or mind or
consciousness) that is not readily observable. The observable activities might
include, for example, language. Language serves the observable process of
organising the content of experience but it is also part of the process of creating the
experience or situation (Mead, 1956, p. 167). This occurs in communication through
43
language where the communication from the self and the response creates the social
meaning of the context of communication and thus a meaningful world.
This is so, Mead (1932) argued, because human beings have thoughts of themselves
and a sense of themselves and the capacity therefore to both communicate with and
behave towards themselves. As a consequence, they are able to interact with
themselves, including expressing themselves, responding to themselves and
addressing themselves again (Blumer, 1969, p. 62). In addition, Mead (1932), and
later Blumer (1969), argued that human beings have the ability, through cognition, to
stand outside themselves and perceive different perspectives. It is through this
process and within the process of social interaction that social meanings are
constructed (Mead, 1932, p. 62; Blumer, 1969, p. 62). In other words, the social
process is the factor that decides people’s thinking. In Mead’s (1956) words:
The self-conscious human individual…takes or assumes the organized
social attitudes of the given social group or community to which he
(sic) belongs, toward the social problems of various kinds which
confront that group or community at any given time and which arise
in connection with the correspondingly different social projects or
organized co-operative enterprises in which that group of community
as such is engaged: and as an individual participant in these social

44
projects or co-operatives, he (sic) governs his own conduct
accordingly (pp. 220-221).
The essential purpose of Blumer’s work was to challenge the premises of the
empirical sciences (by which he means the physical and biological sciences) as they
were applied to the study of the social world (Blumer, 1954, p. 3). Blumer argued
that the “fixed” techniques and experimental procedures characteristic of empirical
inquiry isolated or abstracted study phenomena from the “natural social world” and
subjected them to inquiry based on preconceived theoretical concepts. The use of
specific procedures and predetermined concepts has lead to a singular emphasis on
the refinement of the research process to ensure verification (or generalisation) rather
than on the empirical world that is the concern of social inquiry. Social theory thus
becomes “primarily an interpretation which orders the world into its mould (and) not
a studious cultivation of empirical facts to see if the theory fits” (Blumer, 1954, pp.
3-4). The result is a “glaring divorcement” of social theory from the empirical world
(Blumer, 1954, p. 3). Yet, Blumer argues, social phenomena and/or processes are not
essentially generic and the social world is constantly changing. Thus the process of
social change and its distinctive constituents can not be predicted or understood
through the empirical method (Hammersely, 1989, pp. 114-115).

45
From this starting point Blumer (1969) sought to develop an alternative approach to
social inquiry that captured the “meaning” of social processes and the ways in which
situations and actions are constructed and reconstructed over time. Drawing
foremostly on the work of Mead, Blumer proposed a theoretical exposition of society
as a process of human action which, in 1937, he termed “symbolic interactionism”
(Blumer, 1969, p. vii, 1, 60).
Blumer (1969) argued that there are two levels of social interaction; the
non-symbolic and symbolic. Individuals respond to other’s gestures and actions
directly in the former situation but also interpret other’s gestures and actions based
on the meaning that is given through interpretation (pp. 65-66).
Thus by symbolic, Blumer (1969) means “the fact that human beings interpret or
define each other’s actions instead of merely reacting to each other’s actions” (p.79).
In other words, humans construct and define their actions rather than simply respond
to the actions of others (Blumer, 1969, p. 91). The individual, then, according to
Blumer, is of uppermost importance because the meaning of an object is constructed
by the individual’s action rather than stimulated from the world outside. In other
words, individuals construct meanings of objects based on their ongoing activity

46
(Blumer, 1978, p. 92). As a result, according to Blumer, social reality is an uncertain,
accidental and ongoing process (Morrione, 1998, p. 197).
As such, Blumer (1969) argues that the nature of symbolic interactionism possesses
three prerequisites. Firstly, human beings behave on the basis of the incidents which
affect them. These incidents may include other human beings or physical objects and
may happen individually or collectively in human beings. Secondly, the meaning of
the incident is able to lead to, or form, the social interaction of human’s behaviour.
Thirdly, the way that people deal with the situations they confront is influenced or
altered by the meanings of incidents (p. 2). The meanings that a person attributes to
an object, therefore, provide the basis for explaining behaviours. These meanings
develop in the process of social interaction and within particular settings. Thus, the
ways in which people act and construct their world will vary from context to context.
Origins of Grounded Theory
It is clear that grounded theory is fundamentally grounded in symbolic
interactionism. The purpose of symbolic interactionism is to elicit an understanding
of interactions, responses to interactions and the social processes that these give rise

47
to. Through a process of analysis and explanation or what is called a “digestive
process”, different experiences can be compared and transmitted into human’s daily
activities (Blumer, 1969, p. 133).
In the application of the interactionist perspective, a researcher seeks to investigate
the meanings that constitute and are constituted by interactions with others
(Cutcliffe, 2000, p. 1477; Sheldon, 1998, p. 47). “Others” can mean other people,
organizations, objects and actions within the situation or a mix of the foregoing
elements (Chenitz & Swanson, 1986, p. 5). Similarly, grounded theory seeks to
describe and explain human behaviour and to explore the social processes in human
interactions (Cutcliffe, 2000, p. 1477). Yet, grounded theory is distinctive in its
particular explication of methods for social inquiry. Glaser and Strauss moved
beyond the symbolic interactionism of Mead and Blumer in setting down a detailed
exposition of what they perceived were procedures essential to the generation of
social knowledge. And they brought to grounded theory quite diverse knowledge
bases which have shaped both the methods and the controversies characteristic of
this methodology.

48
Grounded Theory
Prior to their first publication on grounded theory in 1967, Glaser and Strauss
collaborated on a qualitative research project which culminated in the publication, in
1965, of the book “Awareness of Dying”. The methods of collection and analysis
articulated in that book delineated the embryo of grounded theory and the 1967
publication “The Discovery of Grounded Theory” by Glaser and Strauss provided a
systematic explanation of the methodology.
Although both Glaser and Strauss were educated and worked within sociological
schools, their knowledge bases differed. Strauss was strongly influenced by the
interactionist writings of such theorists as Mead and Blumer while attending the
University of Chicago. Glaser, whose ideas were shaped by the works of Paul
Lazarsfeld, trained in inductive quantitative sociology at Columbia University (Beck,
1999, p. 206; Eaves, 2001, p. 655; Rennie, 1998, p. 114). Strauss’s exposure to
naturalistic or field research informed his emphasis on the necessity of a description
and understanding the way of people shape the world in which they live. Glaser
attached importance to systematic data collection and analytical procedures and thus
systematic techniques and procedures in coding processes for qualitative methods

49
(Eaves, 2001, p. 656). Glaser and Strauss brought both perspectives to the
development of grounded theory.
Definition of Grounded Theory
In formulating a definition of their methodological approach, Glaser and Strauss
(1967) stated that a grounded theory will:
…fit the situation being researched, and work when put into use. By “fit”
we mean that categories must be readily (not forcibly) applicable to and
indicated by the data under study; by “work” we mean that they must be
meaningfully relevant to and be able to explain the behaviour under study
(p. 3).
Several decades later, Strauss and Corbin (1990) noted that:
A grounded theory is one that is inductively derived from the study of the
phenomenon it represents. That is, it is discovered, developed, and
provisionally verified through systematic data collection and analysis of
data pertaining to that phenomenon….One does not begin with a theory,
50
then prove. Rather, one begins with an area of study and what is relevant to
that area is allowed to emerge (p. 23).
It can be seen from the above that an important concept inherent to grounded theory
is that it does not begin with theory. Rather, from generated data researchers
distinguish meaningful constructs and thus theory emerges from the data (Streubert
& Carpenter, 1999, p. 100). It is argued, therefore, that grounded theory is
particularly useful in the investigation of complex areas and behaviours where
distinct varieties are yet to be identified (Stern, 1980, p. 20). In other words, the
approach is considered useful in exploring phenomena that have not been previously
addressed, or where concepts and relationships in particular populations or places are
undeveloped or weakly connected (Strauss & Corbin, 1990, p. 37).
The objective of a grounded theory investigation is to discover theoretical
explanations and explore human interactions related to particular phenomena
(Streubert & Carpenter, 1999, pp. 99-100). Grounded theory is, in the first instance,
understood as a social process. Thus investigators endeavour to reveal the social
processes (or theory) that people use to deal with circumstances about which they are
not aware (Benoliel, 1996, p. 408). In other words, grounded theory has the value

51
and ability to explain a theory (that develops from process) that is related to basic
sociological activity (Glaser & Strauss, 1967, pp. 5-6).
Despite the detailed approach taken in the seminal work of Glaser and Strauss, an
examination of the evolution of grounded theory reveals a range of methodological
and conceptual positions that draw on for example, traditional symbolic
interactionism, Strauss’s pragmatist theory of action, eclecticism and, more recently,
the intellectual movement of postmodernism. The variations in theoretical
perspectives point to some conceptual dilemmas inherent in the traditional mode of
grounded theory (Annells, 1997, pp. 177-178). A consideration of these points of
departure is important in articulating a coherent approach to grounded theory.
Contested Areas in Grounded Theory
There are a number of conceptual issues contested in grounded theory. Differing
views prevail over issues such as verification versus generation, theoretical
saturation, the relevance of a literature review, interpretation versus truth, full
conceptual descriptions versus theoretical codes and theory, the micro versus
macro-social world and substantive versus formal theory.

52
Verification versus Generation
Glaser and Strauss wrote in 1965 that their innovative approach to research takes two
directions. First, is the discovery of new concepts and hypotheses and second, is the
testing of these new concepts or hypotheses within a broad range of contexts (Glaser
& Strauss, 1965, p. 261). Similarly, Glaser’s (1965) early work on the constant
comparative method of qualitative analysis indicated two expressed functions in
qualitative research; the generation of theoretical ideas and theory-testing (p. 436).
Therefore, as Hammersely (1989) argues, both Glaser and Strauss were unequivocal
about grounded theory as a hypothetic-deductive approach (p. 198).
However, the emphasis in the 1967 work of Glaser and Strauss shifted significantly.
In this work it was argued that grounded theory was conceived explicitly as a method
to inductively generate theory through comparative analysis (Glaser & Strauss, 1967,
p. 21) and thus the inductive analysis must be regarded as a self sufficient approach.
Glaser and Strauss argued that theory development involves the identification of
sufficient ‘definite’ categories and hypotheses to be verified only in separate
quantitative studies when and where appropriate (Glaser & Strauss, 1967, p. 3). Thus
53
the implication is that grounded theory is foremostly concerned with the generation
of theory and that verification is optional and posed as a process external to the
primary concern of grounded theory. However, an ongoing analytical issue in
grounded theory relates to whether the application of the methodology leads to
verification or generation. This argument is also related to inductive and deductive
concerns regarding grounded theory.
In more recent work, Strauss (1987) has argued that grounded theory includes three
different aspects of enquiry; induction, deduction and verification. These are
perceived by Strauss to be essential components of the methodology (p. 12). In
Strauss’s view, although induction remains the first consideration in grounded theory,
deduction is necessary to enable a logical and thorough examination of the data.
Moreover, Strauss argues that deduction without verification or verification without
deduction means that the inquiry would be incomplete (Strauss, 1987, p. 11-14). As
Strauss (1987) notes:
….the theory is not just discovered but verified, because the
provisional character of the linkages - of answers and
hypotheses concerning them - get checked out during the
succeeding phases of inquiry, with new data and new coding

54
(p. 17).
Thus, Strauss and Corbin (if belatedly) derived from Dewey’s instrumentalism (an
emphasis on the experimental method) to introduce a hypothetico-deductivism into
the grounded theory method.
But this occurred not without challenge. Glaser continued to argue strongly that
grounded theory is properly only inductive and leads to theory generation (Glaser,
1992, p. 16). Others, such as Rennie (1998), defend Glaser in arguing that
verification is an inherently positivist concept and presumes a “theory of truth” (p.
133). Hammersely (1989) also proposes that grounded theory must be inductive
rather than deductive because of its underlying premise that grounded theory was not
conceived for theory testing (p. 173). An emphasis on flexibility to allow the
researcher to find out “what is going on” means that a theory will not be
predetermined but will be worked out as the research progresses (Hammersely, 1989,
p. 173). However, while rigidly adhering to the view that theory must emerge from
the generation of data, Glaser then argues that an inductively produced theory may
be empirically tested to prophesy the principles of some deductive research methods
(Streubert & Carpenter, 1999, p. 104).

55
A key issue central to this debate is the legitimacy of an emergent grounded theory.
Glaser in his early writing stated that the constant comparative method was not able
to both discover and test theory. Grounded theory data is not coded comprehensively
enough to test the theory but only enough to generate and then suggest the theory
(Glaser, 1965, p. 438). The implication is that this methodology does not generate
theory as such. Glaser (1992) addresses this conceptual issue simply by arguing that
grounded theory leads to generation and not verification (p. 67). Grounded theory
focuses on generating hypotheses as they appear from the data; the verificational
model is not the purpose in grounded theory (Glaser, 1992, p. 67). Yet, this leaves the
status of the generated, or ‘suggested’, theory unexplained. Thus, Hammersley (1989)
argues that Glaser, in particular, is ambiguous on the issue of verification (p. 198).
The differences in views on methodological procedures have implications for the
ways in which the verification and justification of grounded theory are articulated.
Some grounded theory studies, for example, focus on theoretical saturation, where
new data fit into the categories already contrived (deduction) (Charmaz, 2000, p.
520). In contrast, other researchers define the study as inductive and theory building
(induction) (Locke, 1996, p. 243).

56
Theoretical Saturation
According to Strauss and Corbin (1998), theoretical saturation is defined as “the
point in category development at which no new properties, dimensions, or
relationships emerge during analysis” (p. 143). In grounded theory, data is initially
collected from a single group and therefore, the researcher may collect data from
older groups or return to participants in order to seek potential new categories. When
similar situations appear again and again, the researcher is able to indicate that a
particular category is saturated (Glaser & Strauss, 1967, p. 61).
However, Glaser and Strauss (1967) also argue that when saturation is reached, the
researcher will often find gaps in his/her theory. In this situation, the investigator
attempts to maximise the varieties of data in one category, integrate and “dense” the
theory and finally rely on the researcher’s theoretical sensitivity (pp. 61-62). But as
Glaser and Strauss (1967) had initially determined, saturation may require “dozens
and dozens of situations in many diverse groups must be observed and analysed
comparatively” (p. 62). Therefore, the process of determining theoretical saturation
and the point at which saturation can be claimed is poorly defined.
57
The Use of Literature
A literature review has a specific purpose in traditional research and that is to help
the researcher understand what has been discovered about the research problem and
if gaps exist between reality and literature (Castles, 1987, p. 45; Strauss & Corbin,
1990, p. 49). However, in grounded theory research, the proposed objective is to
discover relevant concepts and their interrelationships within specific contexts. Thus
it is argued that the imposition of pre-determined categories or knowledge may
influence or distort the process of discovery. As Flick (1998) argues, researchers do
not want to be controlled by previously developed theoretical propositions which
may not be suitable for use in the area under investigation (p. 222).
In light of the above noted tenets of grounded theory, many suggest that researchers
should avoid conducting a literature study before data collection and analysis simply
because the emerging theory must be grounded in the data (Cutcliffe, 2000, p. 1480).
Glaser (1992) clearly argues that the literature review should be eschewed to ensure
that the discovery of the researcher is not conceived from pre-empting thoughts.
Literature assumes a role in sorting and grounding the data only as the theory
emerges (Glaser, 1992, pp. 32-33; Holloway & Wheeler, 2002, p. 166).

58
Nonetheless, a compelling argument points to the necessity for the researcher to
obtain some information about the investigation area before generating theoretical
propositions (Parry, 1998, pp. 93-94). Thus other theorists argue that appropriate use
of previous knowledge is able to realise better the processes that are being observed
(Baker, Wuest, & Stern, 1992, p. 1357). From this perspective, a literature review
assists in the formulation of research inquiry and is helpful in providing parameters
for initial interviews and observations. Furthermore, during the research process, the
literature may help an investigator to find examples of similar circumstances and
when researchers have finished their data collection and analysis and during the
writing stage, the literature can be utilised as a source to confirm their findings
(Strauss & Corbin, 1998, p. 44, 51). Therefore, general reading of the literature may
help the researcher to identify the issues in the particular area and find any gaps to be
filled by utilising grounded theory.
Interpretation versus Truth
A related issue is whether grounded theory research outcomes constitute an
interpretation or the ‘truth’. Here again we find important variations in the body of

59
grounded theory work. In their early work, Glaser and Strauss adhered to traditional
methodological terms in emphasising the predictive and explanatory powers of
grounded theory. Indeed, the authors argued that the primary focus on data, as
opposed to the common practice of testing predetermined concepts, would heighten
the explanatory power of grounded theory. Yet forty or so years of grounded theory
studies suggest that this approach does not produce the kind of generalisable results
that its adherents had proposed.
It has since been argued that in exploring the results of grounded theory research,
researchers seek only to interpret or approach “the truth”. This is so because the very
interaction between the researchers and the worlds they are studying influence the
forming process of theory. The extent to which the emerging theory should and is
affected by this interaction remains an issue for debate (Cutcliffe, 2000, p. 1479).
Indeed, Strauss and Corbin (1990) argue that “reality can not actually be known but
is always interpreted” (p. 22). Furthermore, they also assert that a theory can not be
seen as some discovered or pre-existing reality “out there”. The “truth” is that
“theories are interpretations made from given perspectives as adopted or researched
by researchers” (Strauss & Corbin, 1998, p. 171). Nonetheless, judgments still can be
made and lead to usefulness and soundness of a theory (Strauss & Corbin, 1998, p.

60
171). Thus the “reality” in social enquiry is seen as relative for it is the result of an
interpretation or an investigator’s explanation (Annells, 1997, pp. 122-123).
Furthermore, “social reality is dynamic but that does not contradict the factuality of
social reality” (Lomborg & Kirkevold, 2003, p. 198).
The implication here is that there are many possible alternative interpretations of
qualitative data (Corbin, 1998, p. 122). Social reality is interpreted from given
viewpoints that are adopted or researched by investigators and are informed by
culture, history and a researcher’s attitude (Benoliel, 1996, p. 407). Moreover, in an
intellectual process, knowledge or concepts are not dormant. People are undergoing
change and those changes may influence people’s goals and social processes and
directly or indirectly change their thoughts and behaviours (Benoliel, 1996, p. 416).
In other words, a researcher will not know the realities or indeed if there are realities.
What is depicted as a representation or interpretation of reality is dependent upon a
complex interplay of factors including the investigator’s point of view. In adopting
this view, Annells (1997) suggests that:
…readers of grounded theory research reports need an awareness of the
varying views of what is “reality” and how it can be known, as intrinsic to

61
varying modes of the method. There are encoded assumptions and values
about the social world within such reports that position us as readers of
research (pp. 128-129).
Full Conceptual Descriptions versus Theoretical Codes and Theory
The generating concept of grounded theory requires “theoretical sensitivity” (as
Glaser termed it). Theoretical sensitivity combines interpersonal perceptiveness with
conceptual thinking, not an importing concept (Wilson, & Hutchinson, 1996, p. 124).
Full conceptual descriptions and theoretical codes both have this characteristic.
Conceptual descriptions serve to answer the question “what is going on here?”
Theoretical codes extend the analysis to “what is going on and how?”
The concepts of “full conceptual description” and “theoretical codes” draw from two
conflicting points of view. Glaser argues that there are substantive codes from which
then emerge the theoretical codes. In contrast, Strauss and Corbin propose a coding
technique which extends to “conditions, contexts and consequences” and which they
term a “logic diagram” that will not be influenced as the research moves (Corbin,
1998, p. 126). As a result, full conceptual descriptions are formed.

62
Glaser, however, argues that the emphasis of grounded theory must be on
“emergence”. Hence, he criticises the Strauss and Corbin approach of a “full
conceptual description” which, in Glaser’s view, reflects a “forcing” of data and
theory rather than allowing each to appear independently (Eaves, 2001, p. 656).
Glaser argues that this method is more accurately termed a conceptual description
rather than grounded theory (Benoliel, 1996, p. 415). Moreover, he indicates that
Strauss does this without satisfactory reference to their seminal work on grounded
theory (Melia, 1996, p. 369). In Glaser’s (1992) words:
Full conceptual description is a wholly different method from
grounded theory. It grew up from the same research as grounded
theory, but at the hands of a different research analyst. It is a “new”
conceptual method, uniquely suited to qualitative research, that
simply uses the grounded theory name…. (p. 123).
These two contrasting positions have given impetus to substantial arguments over
grounded theory research.

63
Micro versus Macro-Social World
A related proposition in grounded theory research is that investigations are usually
confined to specific contexts or certain cases (micro-social world). If researchers
seek to generalise the findings (macro-social world), the contextual link needs to be
abandoned in order to obtain findings that are valid independently of and outside
certain contexts (Flick, 1998, pp. 233-234). However, this poses a dilemma.
A consideration of macro-conditions will arguably increase an understanding of the
phenomenon of interest (Rennie, 1998, p. 132). Nevertheless, the traditional mode of
grounded theory research does not address this dimension. Indeed, an acknowledged
criticism of grounded theory is that it constitutes a study of the micro-social world
and it may therefore include a distortion of macro-conditions (Rennie, 1998, p. 132).
In other words, grounded theory studies may not show readers the whole picture.
Some authors claim the existence of two grounded theory approaches that focus
either on the micro-social or the macro-social world. The classic grounded theory
method concentrates at the micro level (micro-social world) of analysis. In contrast,

64
Strauss and Corbin’s approach seeks to combine the micro and macro levels
(micro-social world and macro-social world) of analysis (Annells, 1997, p. 125).
However, a conceptual distinction between these two levels of research can not be
reconciled within an inductive approach that gives primacy to data. The Strauss and
Corbin remedy is to argue, as noted, for both inductive and deductive phases in
research. This involves bringing to the research analysis explanatory factors that are
not immediately related to the phenomenon under study. Arguably this strengthens
the grounded theory project. But perhaps Glaser (1992) is then justified in arguing
that Strauss and Corbin have diverged from the “focus and criteria of grounded
theory as it was originally intended and written” (p. 119).
Substantive versus Formal Theory
As Strauss and Corbin (1994) argue, the essential purpose of grounded theory is to
further develop an effective theory (p. 278). An effective theory in their terms means:
fit of substantive grounded theories in terms of what the researcher has
actually seen and/or heard, and later more will be said about the

65
relevance of theory in its application (Strauss and Corbin, 1994, p.
278).
In addition, an effective theory is not only able to trace back to the data that is its
source but also adapt to the feature of “striking fluidity”. An effective theory may be
seen as “systematic statements of plausible relationships” (Strauss & Corbin, 1994,
pp. 278-279). Strauss and Corbin also suggest that the role of interpretation in
grounded theory is no less important than theory creation and as such theory should
only be grounded in the “interplay with data and developed through the course of
actual research” (Strauss & Corbin, 1994, p. 278).
The issue then is whether grounded theory produces substantive theory or formal
theory. Glaser and Strauss (1967) see both theories as “middle range”, or in other
words, “minor working hypotheses” or “all-inclusive” theories of every day life
phenomena (pp. 32-33). Furthermore, grounded theory is designed to produce
“conceptually dense” theory that articulates the relationships within a theoretical
framework. The relationships are posed only as propositions and although theory can
be presented, it is considered only momentary.

66
However, Glaser (1978) argues that grounded theory researchers should construct a
theory that is readable and modifiable. Furthermore, they should highlight the points
in the writing, because most readers may read the writing as “a fixed conceptual
description, not explanation” (p. 129).
Debate surrounding these issues will continue and as such there is no one definitive
position, the position stands with researchers or readers.
Methodological Approach
In addressing the conceptual dilemmas in developing a grounded theory study, it is
clear that the researcher’s perspective is an important factor in both shaping and
conducting a research study. The framework of grounded theory applied in this study
draws predominantly on the works of Strauss and Corbin (1990) and this framework
is referred to here as a reconceptualisation of grounded theory.
The reformed framework emphasises the following methodological and conceptual
points pertinent to this study. The first of these is that grounded theory leads to both
the generation and verification of theoretical propositions and as such incorporates

67
both inductive and deductive elements. The second conceptual issue relates to
saturation. The concept of saturation in this study refers not to the phase of data
collection, but to the analysis phase and the point at which no new dimensions are
discovered in the analytical process. Third, a general literature review may be
undertaken, as was the case in this research, prior to data collection in order to
enhance an understanding of the study issue. However, the knowledge derived from
a literature review should not distort data analysis. Fourth, reality is understood in
this study as a relative concept and thus hard to achieve or may not be known. In
other words, reality is interpreted. A further and essential conceptual issue
particularly pertinent to the study is the recognition of the interconnectedness of the
micro and macro social worlds. Finally, a formal theory may not be the outcome of a
grounded theory study. Rather, the research has suggested to produce a “conceptually
dense” theory may be produced and posed as propositions regarding the issue that
has been studied.
This framework presents a coherent methodological approach to grounded theory
inquiry and one that centres on the discovery of a conceptually “dense” theoretical
explanation of the issue under study.

68
Summary
This chapter has addressed both the theoretical tenets underlying grounded theory
and some conceptual dilemmas that have emerged in the development of the
methodology. The discussion has included explanations of symbolic interactionism
(as it underpins grounded theory), the origins of grounded theory and a historical
review of this methodology and related conceptual issues. On the basis of this
analysis, the key conceptional points that inform this study have been explicated.
The following chapter provides a detailed rationale for the methods of grounded
theory as they were employed in the study.

69
CHAPTER 4
Methods
This chapter addresses the methods utilised in this study. Although the following
presentation of methods assumes a linear form the application of methods is
premised on an understanding of grounded theory as a process rather than
constituting discrete techniques. Grounded theory method, as a process, seeks to
explicate a connection from qualitative data to theoretical propositions. It is,
therefore, the conceptual relationship between the methods, not the order in which
they are employed, that enables a systematic and cumulative construction of an
analysis. In this sense, the process is almost in the data and naturally emerges from
the data analysis if the researcher follows the steps of grounded theory analysis
(Stern, 1980, p. 21; Strauss & Corbin, 1990, pp. 143-144).
The methods outlined include purposeful and theoretical sampling, data collection,
the use of memos, data analysis and validity in translation of interview data. In
addition the role of the researcher, the ethical dimensions of the study and validity
and reliability of this study are addressed.

70
The Elements of Grounded Theory
Sample Selection (Participants)
The study employed both purposeful and theoretical sampling. Sampling strategies
employed by qualitative researchers are used to obtain rich and in-depth information
from participants (Patton, 1990, p. 169). Because samples (participants) are generally
selected for a particular purpose the term “purposeful” or “purposive” sampling is
used. Here participants were chosen because they had experience related to the
phenomena under study and were able to share these experiences to the researcher.
As the research analysis developed initial concepts or categories, theoretical
sampling entered the research process. Strauss and Corbin (1998) define theoretical
sampling as “sampling on the basis of emerging concepts, with the aim being to
explore the dimensional range or varied conditions along which the properties of
concepts vary” (p. 73). Theoretical sampling is thus guided by significant ideas that
emerge from the data. New things emerge from the data that should draw analytic

71
attention. If something seems present but not articulated, additional data are requisite
(Clarke, 2003, p. 561). Theoretical sampling can not be pre-determined and
continues throughout a grounded theory study. Thus initial data collection and
analysis directs the process of enquiry and, in turn, the direction of theoretical
sampling (Cutcliffe, 2000, p. 1477; Holloway & Wheeler, 2002, p. 157). In other
words, theoretical sampling reflects “the emerging theory (which) controls the
research process throughout” (Alvesson & Sköldberg, 2000, p. 11).
Fourteen participants constituted the initial sample in this study. This sample size
allowed for a depth and range of data to facilitate early analysis. Using the principle
of theoretical sampling, an initial number of participants was increased dependent
upon the emergent data analysis (Streubert & Carpenter, 1999, p. 106). When the
data collected was deemed rich enough to explore the different dimensions of the
research, then the sample size was judged appropriate. Too few participants would
have resulted in insufficient data and too many participants may have lead to data
redundancy (Berry, 1993, p. 906). On this basis, the final sample size for this study
was twenty four.

72
The twenty four participants were recruited from two health care settings. The
participants were chosen from patients who were hospitalised in one medical centre
hospital (the largest) and one regional hospital (the second largest) in Taiwan. The
nursing department in the respective hospitals received a letter from the researcher
which included the research proposal, a participant information sheet and a consent
form. These documents were also submitted to the relevant hospital committees in
seeking approval for the research.
Participants were recruited from those who were hospitalised in cancer wards and
those cancer outpatients who were cared for by the home care department in the
hospitals. The criteria for participant selection were as follows:
∗ First, participants have been diagnosed with cancer;
∗ Second, participants had used at least one type of non Western medicine during
their cancer treatment journey for any length of time; and
∗ Third, the participant’s health status was such that she/he could participate fully
and without adverse effects in the interview process.

73
In the first instance, the researcher communicated fully with nursing and medical
staff in seeking advice on and access to patients who may be potential research
participants. The head nurse in the ward and the head of the home care department
were the first persons to mediate the process and nurses in the ward identified
appropriate patients. The researcher then approached individual patients to explain
the research process and objectives and to identify those who met the criteria for the
research. Potential participants received a letter, including an information sheet and
consent form in Chinese (see Appendix I and Appendix II for both English and
Chinese format) that sought their consent to be involved in the research project. All
but one participant could read. For the participant who could not read, the
information sheet and consent form were explained by a nurse in the ward after
which the participant signed the consent form.
Participant Demographics
The sample of twenty four participants consisted of thirteen males and eleven
females. The age distribution is presented in Table 1. The sample had a mean age of
45.7 years with a range from 16 to 69 years. With regard to marital status, most
(18/24) were married, with only four being single. Two participants were widowed.
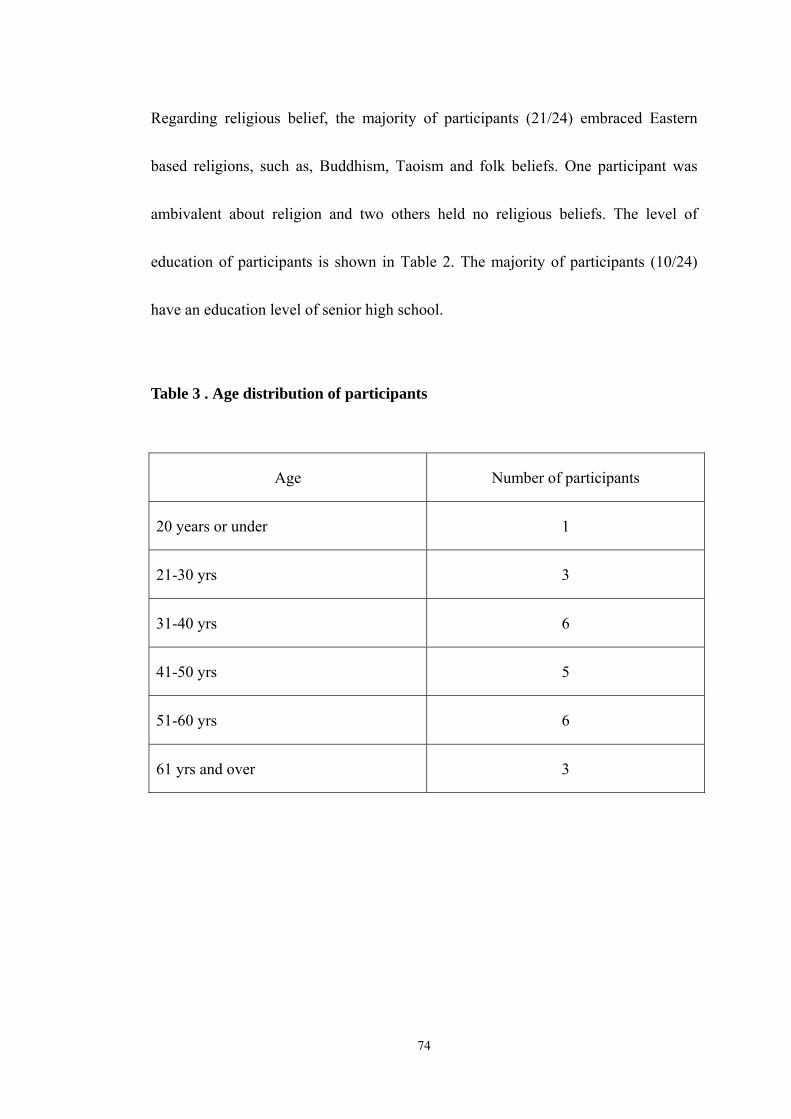
74
Regarding religious belief, the majority of participants (21/24) embraced Eastern
based religions, such as, Buddhism, Taoism and folk beliefs. One participant was
ambivalent about religion and two others held no religious beliefs. The level of
education of participants is shown in Table 2. The majority of participants (10/24)
have an education level of senior high school.
Table 3 . Age distribution of participants
Age Number of participants
20 years or under 1
21-30 yrs 3
31-40 yrs 6
41-50 yrs 5
51-60 yrs 6
61 yrs and over 3

75
Table 4. Educational level of participants
Highest level of education Number of participants
Primary school 7
Junior high school 4
Senior high school (including junior college) 10
University 2
Higher than university 1
The twenty four participants included in this study are identified through family
names (pseudonyms) such as Mr. Zhao or Ms. Qian. These family names were
carefully chosen from “one hundred family names” (百家姓) so that they do not
reveal the participant identity in order to protect confidentiality and anonymity.
Interview Approach
The purpose of any form of interviewing is to retrieve data required for the research
project. Yet, interviewing styles differ significantly in accordance with the objectives
of the research and the chosen methodology. Although interviewing in qualitative
76
inquiry is generally described as semi-structured or informal, the degree of structure
varies. For example, Keats (2000) argues that the researcher needs to ensure that the
question format does not radically change for different participants in order to avoid
bias and so the data can be codified in a certain way and be analysed effectively (pp.
19-20). However, in grounded theory it is important that the interview is flexible to
ensure that data generation is not constrained by the structure of questions. As such,
the grounded theory interview should be seen as a process of utilising broad and
open modes of gathering respondents’ perspectives on views of the particular
phenomena (Wimpenny & Gass, 2000, p. 1490).
Thus, in-depth interviews were used in this study to facilitate a broad articulation of
viewpoints that would not occur within a more structured interview situation (Flick,
1998, p. 76). The purpose of the in-depth interview was to elucidate an
understanding of participants’ experiences and the meanings that they construct from
those experiences (Seidman, 1998, p. 3). In-depth interviews were more likely to
obtain data that reflect the in-process nature and the complexity of the meanings or
interpretations that researchers intend to explore (Rice & Ezzy, 1999, p. 53).

77
The advantages of this approach were first, that it gave the researcher some
manoeuverability in pursuing both the obvious and the unexpected dimensions of a
research topic. Second, a flexible and unstructured interview permitted the researcher
to enter the subject area in a natural way. Third, this style of interview allowed the
researcher to know the participants as people and to see how they perceive their
world and eventually, to see the incidents the way they do (Chenitz, 1986, p. 82).
Furthermore, in order to communicate effectively, an interviewer’s language should
be understood by the participants and interviews must be conducted in the
participants’ language (Fontana & Frey, 2000, pp. 654-655). As such, Mandarin,
Taiwanese or a mix of two languages were used in the interview process in this
study. Gaining trust and establishing rapport were critical in the conduct of the
interviews (Fontana & Frey, 2000, p. 655).
In addition, during the interview the researcher considered first, what was said and
what it meant; and second, how and when the researcher posed the next question. A
third consideration was determining when the full pattern of incidents had been
discussed and the pattern of the interview had been utilised in the interview process.
Finally, the researcher observed the participants for any signs of disinterest,

78
discomfort, or on the other hand, excitement or interest (Sullivan in Chenitz, 1986, p.
83).
Some open-ended and pre-determined questions were posed at the outset for the
purpose of determining the parameters of communication and to optimise the
interview time. However, the on going data analysis characteristic of grounded
theory, gave rise to what Strauss (1987) refers to as “momentary” theory and
categories (emerging from on going data analysis) that changed the direction of
inquiry (pp. 26-27).
One to one interview
The method of data collection was the one to one in-depth interview, with a few
exceptions where family were present. Interviews ranged from thirty to seventy
minutes in length. Each interview took place in a private environment and one agreed
upon by the participant. Where participants were hospitalised, the interviews were
conducted in a participant’s room or, where appropriate, in a separate meeting room
in the hospital. For those participants who were outpatients, the interviews were
arranged at either their homes or, by mutual agreement, at alternative settings.

79
Data Collection
For data collection an interview theme list was used to enable the researcher to probe
themes without leading the discussion. It is necessary to note that qualitative
approaches determine to understand a specific phenomenon from the perspective of
the people who are experiencing or have experienced that particular phenomenon
(Streubert-Speziale & Carpenter, 2003, p. 19; Woodgate, 2000, p. 194).
The interview questions in this study were guided from an interview theme list and
began with an open question such as: “Could you describe your history of using non
Western medicine?” This question was followed by a series of open questions (see
Appendix III). As noted, however, in grounded theory ongoing analysis may change
the direction of inquiry. As such, these questions served as a guide only, as
interviewer responses and additional questions were directed by the participants’
responses.
In this study, the opening and guiding question was broadened in the second stage of
interviews in order to engage with the whole process of using NWM among

80
Taiwanese cancer patients. The opening question then became “Could you describe
your cancer journey?”
The Utilisation of Memos
Researcher memos are an important data source in grounded theory. Memos are not
traditional tools of communication but a special form of written word that reflect the
researcher’s ongoing speculation of the data. The writing of memos starts with the
initial stages of research and continues through the research process. Thus, memos
are an important source of conceptual data in the sense that they help the researcher
to draw relationships among the data (Strauss & Corbin, 1998, pp. 217-218).
Although memos may appear as rough notes at the outset, more data may change,
support or correct initial notes. The emergent concepts then become more dense and
refined as the research progresses (Strauss & Corbin, 1998, p. 218). The writing of
detailed and descriptive memos also ensures some transparency in the research
process in reflecting the researcher’s investments in his/her thinking (Martin &
Turner, 1986, p. 145). Furthermore, Corbin and Strauss (1990) also argue that if the
researcher skips the memo procedure and simply moves from coding to writing,
81
some conceptual details may be underdeveloped. As such, this may result in a less
satisfactory integrated data analysis (p. 10).
In this study, memos were utilised through out the whole research process and
particularly as an adjunct to coding. The researcher wrote memos in both Chinese
and English. At each level of coding these memos assisted in the data analysis
process and stimulated the researcher’s thinking. For example, the researcher noted
that, in coming to use NWM, much information was sourced through word of mouth
from family and friends. This emerged as an important analytical point particularly
as it contrasted with the use of western medicine for the participants.
Data Analysis
The methods used in data analysis were based on the grounded theory processes
outlined by Strauss and Corbin (1990) and included the levels of open, axial and
selective coding (p. 58). While presented in a given sequence below it is noted that
these steps in analysis did not occur in a linear fashion. In other words, the researcher
continually moved back and forward between different levels of coding in order to
thoroughly analyse and compare the data.

82
Most qualitative studies are presented in a discursive way with thick conceptual and
descriptive writing (Glaser & Strauss, 1967, pp. 31-32; Strauss, 1987, pp. 263-264;
Strauss & Corbin, 1994, p. 278). Two important features of the analytical process
and central to this study were theoretical sensitivity and comparative analysis.
Theoretical Sensitivity
The term “theoretical sensitivity” is associated with grounded theory and is defined
as “a personal quality of the researcher” or how the researcher interprets the meaning
of data and minor differences among data (Strauss & Corbin, 1990, p. 41).
Glaser (1978) suggests that the way to ensure theoretical sensitivity is to enter a
research environment with few preconceived opinions or ideas and particularly
without prior hypotheses. In so doing, the researcher is able to both maintain a
sensitivity towards the data and to understand what is happening without being
influenced by pre-existing biases or hypotheses. This allows the researcher to detect
what is actually going on (pp. 2-3). Strauss and Corbin (1990) assert that theoretical
sensitivity may be drawn from a range of sources including literature, professional
experiences and personal experiences (pp. 42-43). In this study, as noted in the
83
previous chapter, the use of literature was integral to all phases of data analysis in
validating the emergent interpretations.
This research sought to maintain a balance between those sources and the discovery
of theoretical propositions. In so doing, the researcher drew on the conceptualisation
of the process by Strauss and Corbin (1990). First there was an endeavour to step
back and ask “what is going on here?”. Second, the researcher sought to assume a
sceptical attitude towards all factors of the research including for example, the
emergent categories, the literature or questions about the data. These were all seen as
provisional until they are supported by actual data. Moreover, it was necessary to
follow the research procedures. The data collection and analytic procedures were
designed for grounded theory to give rigour to a study. The intent was to prevent the
researcher from imposing bias on the research by examining assumptions that may
come from unrealistic readings of the data (pp. 44-46).
In this study, the researcher did the interviews and data analysis at the same time and
constantly asked herself “what is going on here?” Here theoretical sensitivity was
enhanced through an ongoing process of comparing data with, and grounding data in
the literature.
84
Comparative Analysis
Comparative analysis was an important technique adopted in the study in order to
enhance theoretical sensitivity. It required the asking of questions and making
comparisons (Strauss & Corbin, 1998, p. 73). Through systematic comparison with
two or more phenomena, the researcher may sensitise properties and dimensions that
are yet to be found. Strauss and Corbin (1998) note that the comparisons may come
from either the literature or the researcher’s experiences (pp. 87-88).
In addition, it is important to compare different categories. In comparing different
and similar concepts, new dimensions may emerge to the investigator or reveal
already existing dimensions that the researcher has not yet identified (Strauss &
Corbin, 1998, p. 94). As Strauss and Corbin (1998) state, theoretical comparisons
may offer some thoughts on theoretical sampling in order to seek out variation (p.
94).

85
Open Coding
Open coding is defined by Strauss and Corbin (1998) as “the analytic process
through which concepts are identified and their properties and dimensions are
discovered in data” (p. 101). Open coding of the interview transcripts, as the first
step in analysis, involves breaking down, examining and categorising data by
labelling the phenomena that emerges from the data (Strauss & Corbin, 1990, p. 63;
Strauss & Corbin, 1997, p. 39; Sheldon, 1998, pp. 47-48).
Strauss (1987) describes open coding as “vivo codes” or codes that seek to explain,
through processes or behaviours, how the problems are resolved (p. 33). There are
two properties of vivo codes; “analytic usefulness and imagery”. These codes may
consist of words or phrases that directly reflect a participant’s description of a
particular phenomenon (Holloway & Wheeler, 2002, p. 158; Strauss, 1987, p. 33).
Therefore, line-by-line analysis in vivo coding was the defining feature of open
coding and to be methodologically effective had to be exhaustive. This process is
time consuming simply because the codes are drawn directly from the data and not
from preconceived concepts or ideas which may shape the formulation of codes
(Eaves, 2001, p. 658; Holloway & Wheeler, 2002, p. 158).

86
To achieve this, the researcher read through the transcripts carefully and used words
as they appeared in the interviews to reflect concepts, issues and perceptions that
arose. This is the descriptive phase of analysis whereby the data is reduced to
concrete and representative concepts. For example, in the open coding phase of this
study, numerous codes were drawn from the transcripts such as “did a special pray”,
“did something bad in the previous life” and “can’t say it does not exist”. All these
codes then entered the next phase of coding.
Axial Coding
The second phase of analysis involves connecting categories and is referred to as
theoretical or axial coding. The definition of axial coding is:
the process of relating categories to their subcategories and is termed
“axial” because coding occurs around the axis of a category, linking
categories at the level of properties and dimensions (Strauss & Corbin,
1998, p. 123).

87
Thus the purpose of axial coding is to bring together concepts to form categories that
are obviously connected (Strauss & Corbin, 1990, p. 97). The construction of distinct
categories, each of which constitutes obviously linked codes, allows for categories
(and therefore codes) to be compared to one another and attached to a particular
phenomenon (Eaves, 2001, p. 659).
During this stage, the researcher sought to connect the existing categories and to
draw possible relationships between them. These relationships were written into
existing memos and at times constructed in diagrammatic form to see where gaps
may have existed. Thus, this coding phase involved two levels of analysis. The first,
as Strauss and Corbin (1998) advise, was the use of exact words or phrases that
appeared in the data and the second involved the researcher’s conceptualisation of
these data extracts (p. 126). A significant feature of axial coding is the movement
between inductive and deductive interpretation. Here, the researcher induced “what
is going on” from the data and deduced through a comparison of categories and
relevant literature. In other words, the researcher sought to validate the interpretation
of data through a comparative examination of related bodies of knowledge (Strauss
& Corbin, 1998, pp. 136-137).

88
In this study, the numerous codes from open coding were further interpreted to
produce broad (inclusive) themes and related sub themes. An example of a broad
theme is “philosophical beliefs” which incorporates the sub-themes of traditional
Chinese philosophy, religious practices and Chinese proverbs and self destiny.
Selective Coding (Core Category)
The third and most abstract level of analysis is termed selective coding. At this level
of coding, the researcher constructs a core category that links all other categories.
Thus, selective coding is referred to as “the process of integrating and refining the
theory” (Strauss & Corbin, 1998, p. 143). The function of the core category is to
explain the whole story and to reflect the different dimensional levels of categories
and their interrelationships. In other words, a core category should have considerable
variation among different subcategories (Strauss & Corbin, 1990, pp. 117-118;
Strauss & Corbin, 1998, p. 146).
At this point of the analysis, the researcher is able to create a conditional matrix
which constitutes the basic framework of the emergent theory. The core category is
able to lead to the discovery of what Strauss and Corbin term a basic social process

89
(BSP). Essentially, a core category and basic social process are similar as both need
to fit the properties of change and movement over time (Eaves, 2001, p. 659; Glaser,
1978, pp. 96-97).
The conduct of further interviews may be necessary following one or all levels of
coding to further explore and refine categories. This step, which reflects theoretical
sampling, will not only test the credibility of the data but will reveal and address any
gaps that the researcher needs to fill (Strauss & Corbin, 1997, p. 39; Strauss &
Corbin, 1990, p. 192). Thus the process of analysis is a recursive process, which
means it may move back and forth between the different levels of coding (Strauss &
Corbin, 1990, pp. 117-118).
In this study, the interviews were divided into two stages. Fourteen interviews were
conducted during the first stage. The researcher then concentrated on data analysis of
those interview transcripts and identified themes or categories that needed further
exploration. The following ten interviews were conducted with the purpose of filling
conceptual gaps and producing further themes.

90
To conclude, the process of data analysis applied in this study included the following
elements. First, the researcher interpreted vivo material and articulated concepts that
directly reflected the data. Second, the investigator examined the relationships
among the different concepts and categories and attempted to identify major
categories. Moreover, throughout this process, the analytical process continued to
engage with methodological issues (Charmaz, 1983, pp. 114-115).
The core category that emerged from this study is “taken for grantedness”. The core
category connects the two main categories identified in the axial coding process.
These categories are philosophical beliefs (religious practices as one of its
subcategories) and social relationships.
Validity in Translation of Interview Data
Human beings utilise complex communication approaches to raise ideas and the
meanings of ideas are transmitted and created through language. People also respond
to the meaning of things through symbols (Gusfield, 2003, pp. 123-124). In addition,
human actions and interactions occur through linguistic exchange. By using
numerous and diverse expressions, meanings and situations are transmitted through
91
language (Gusfield, 2003, p. 124). The languages of the interviews conducted in this
study were in Mandarin and Taiwanese or a combination of both. Prior to each
interview, the researcher determined which language the participant used. During the
interview, the researcher utilised the elected language to interview the participant. If
the participant switched language in the interview process, either from Mandarin to
Taiwanese, or Taiwanese to Mandarin, the researcher followed suit in order to ensure
clarity of meaning.
Therefore, the interviews were conducted in either Mandarin or Taiwanese, or in a
combination of both. The transcriptions were written in Chinese. It is important to
note, however, that some Taiwanese words do not translate readily into Chinese. In
such cases, the researcher would write the pronunciation of those words in Chinese
characters with the Chinese translation in brackets.
The interview transcripts then were analysed in Chinese by the researcher. However,
the researcher also recorded the key themes in English during each coding process.
Although the processes of translation were time consuming, the conduct of
interviews in the participants’ first language was necessary to produce authentic data
(Esposito, 2001, p. 574).

92
At the commencement of data translation in this study, only selected quotes were
initially translated into English. When translating these selected quotes, the
researcher placed to one side the original Chinese transcripts and to the other side,
the key themes of those original quotes translated into English. In addition, the
researcher had these selected quotes translated in English as far as practicable in their
entirety. If doubts arose about key themes in the selected quotes, which were written
in English, these were verified by re-examining the original Chinese transcripts.
Sometimes, whole quotes in Chinese are not completely translated into English due
to their length and to avoid redundancy. The researcher used several dots to indicate
this situation. Because the researcher is a native speaker of Mandarin and Taiwanese,
she was able to immerse herself in the actual words utilised by the participants. In
this way, the process of translation was considered as transparent as possible.
With regards to the translation process, Nelson McDermott and Palchances (1994)
state that it is difficult to translate data when two languages are so dissimilar in
grammatical structure (p. 113). Thus, the challenges that emerge in data translation
when doing qualitative research include different sentence structure and
untranslatability (Wang et al., 2006, p. 179). It is particularly true when it comes to

93
Chinese. For example, the Chinese language does not have tenses. Thus, when the
researcher translated quotes into English, the researcher used different tenses
depending upon the meaning that the participant was seeking to impart. Furthermore,
different Chinese utterances may lead to only one English translation. In addition,
there are, at times, no subjects and verbs in colloquial Mandarin and Taiwanese. In
order to make sense in English, the subject and verb were entered in brackets in the
English translation. These issues may contribute to translation complexity when the
Chinese data are translated into English, and this may have implications for the data
quality (Twinn, 1998, p. 657).
There are further issues regarding translation which may affect the quality of the data.
Firstly, at times there are no exact equivalent words in the target language. The
challenge of searching for suitable English words to express and capture the meaning
of Chinese data was a permanent issue throughout the data translation (Twinn, 1997,
pp. 420-421; Twinn, 1998, p. 657). Secondly, during the interviews, sometimes
colloquial Mandarin and Taiwanese were used. These situations raised a question
about the extent to which the English translation of data truly reflected the
experiences of the participants (Twinn, 1998, p. 657).

94
In light of the above, the researcher adhered to the following principles regarding
data translation in the study. Firstly, the researcher undertook the translations with
the objective of reaching the meaning closest as possible both to the source (Chinese)
and to the target language (English). However, not every concept could be translated
and in such cases, meaning-based translations were used rather than word-for-word
translations (Esposito, 2001, p. 572).
Secondly, any ambiguities in meanings of words were noted in the data analysis and
in the subsequent write-up of the results of analysis. Further, both English
translations (meaning-based) and original Chinese characters, if indicated, were
included in the text of the results discussion. In addition, where certain Chinese
expressions or concepts do not appear in the English language, the researcher used
pronunciation translation and put footnotes to explain the concepts and meanings. In
so doing, the impact on analysis of differences between the two languages was
minimised.

95
The Role of the Researcher
Researchers bring their experiences and knowledge to studies and this can enhance
an understanding of the issues (Streubert & Carpenter, 1999, p. 106). The
researcher’s perspective may also influence the questions to be asked; the
researcher’s own experiences, values, and priority may lead to sensitising the
thoughts of the researcher and all of these may be affected by a school of thought or
a philosophical stance (Charmaz, 1990, p. 1165; Pidgeon, 1996, p. 77). When
interviews are conducted, researchers attempt to distance themselves from their
experiences and to assume an impartial mindset. Yet, as Corbin and Strauss (1990)
argue, the researcher's ability to “maintain analytical distance” needs to be combined
with a capacity to draw on past experiences and theoretical knowledge in interpreting
data (p. 18). The role of the researcher in this study was shaped by past experiences
in oncological nursing and accumulated knowledge of the theoretical groundings of
interpretive inquiry.
In addition, it is also the researcher’s responsibility to maintain the anonymity of
participants in studies of this type. Interviewees may not want information about
themselves to be recognised in the public domain (Behi & Nolan, 1995, p. 712).

96
During the research process, the researcher engaged in frequent discussions with
supervisors, or one or two colleague(s), about the data transcripts. However, to
ensure anonymity no names were identified in these situations.
Ethical Implications
Researchers have a responsibility to ensure that the rights of participants are
protected. In this research, participants may have felt that they had diminished
autonomy because of their location within the health care system. The most accepted
way to ensure the dignity and autonomy of participants is through the use of fully
informed consent. Informed consent involves disclosure of information,
comprehension, and voluntarism, and competence in the decision to participate or not
participate.
Participants received a written information sheet and consent form in Chinese (see
Appendix I and Appendix II for both English and Chinese format). Prior to the
interview, written consent was obtained from the participants. During the interview,
it was possible that participants might recall some unpleasant memories or

97
experiences. If participants were to experience any distress as a result of participation
in this project, they were to be offered the opportunity to contact a hospital
counselling service on (04) 2205 2121-4252 (A Hospital) or (04) 2662 5111-2152 (B
Hospital) for assistance, free of charge. This did not occur throughout this project.
Full information about the purpose of this study and the topic to be discussed was
explained prior to the interview in the participant’s most familiar language.
Furthermore, participants were informed that they were free to withdraw at any time
from the research, without comment or penalty and without endangering their
relationship with the researcher or the hospital.
In addition, it is also the researcher’s responsibility to maintain the anonymity of
participants in studies of this type. Although the findings of this study may be
published, no names or information which could identify any individual or
organisation will be recorded. Furthermore, the tapes will be erased after safe
keeping for a certain period (5 years). Only the researcher and her research
supervisors will have access to this information, so that the anonymity of the
participants can be assured.

98
Validity and Reliability of This Study
The issues of validity, credibility and reliability are as relevant to qualitative research
as any other research. However, it is a challenge to develop validity standards for
qualitative research because it is not only necessary to integrate rigour and
subjectivity but also to ensure creativity (to enhance creative findings and to
challenge traditional thinking) (Whittemore, Chase, & Mandle, 2001, p. 522).
Furthermore, the purpose of qualitative research is to seek a depth of understanding
in order to elicit the subtle nuances in life experiences (Ambert et al., 1995, p. 880).
Detailed description constitutes evidence for validation. This refers to both the
transparency of the research process and the presentation of research findings. At a
fundamental level, validity is judged on the extent to which a description is detailed
enough “for the meaning or context of interpretation to be visible or apparent”
(Burns, 1989, p. 48; Popay et al., 1998, p. 345). As Ambert et al. (1995) assert:
“qualitative work should vividly colour in the meanings, motivations,
and details of what quantitative research conveys only in broader
aggregates” (p. 885).

99
However, as Marshall (1990) argues, a researcher makes a decision on which study is
more valid than another and whose biases are more correct and thus “(e)valuating the
goodness and value of research requires a judgement call” (p. 191).
Maxwell (1992) also argues that validity is not born with a particular method, but is
connected to the data or conclusions that are utilised for specific contexts for
particular purposes (p. 284). In other words, methods provide the vehicle for
obtaining evidence to support validity (Maxwell, 1996, p. 87).
Other authors point to the potentially conflicting objectives of ensuring creativity
within the research process and demonstrating rigour in data collection and analysis.
This may present an enduring problem within qualitative research. As Patton (1990)
argues, it is important that qualitative research is highly creative as well as
analytically distinct and rigorous (p. 462). Thus, researchers need to answer the
following questions. Do the findings explain the experiences of interviewees or the
whole context in a reliable way? Are the interpretations shown in a trustworthy way
and reveal some truth external to the researcher’s own experience? Does the
interpretation fit what has been described by participants? (Whittemore, Chase, &
Mandle, 2001, p. 529).

100
Theoretical sampling utilised in grounded theory attempts to address the questions
posed above. Further, it also makes various phenomena understood and tests
developing categories which are found in the particular settings. This is significant in
establishing the validity of data in qualitative research (Maxwell, 1992, p. 293). In
addition, although generalisation is a difficult concept in qualitative research, study
findings should also fit into other situations outside the study contexts (Sandelowski,
1986, p. 32).
Furthermore, to ensure validity, each sampling criteria, data collection, analysis
techniques, and procedures should be clearly delineated (Whittemore, Chase, &
Mandle, 2001, p. 524). Open inquiry, reflection and critical analysis are all aspects of
inquiry that lead to validity in qualitative research (Marshall, 1990, p. 192).
Researchers who use grounded theory as a methodology may attempt to elaborate,
generate or test a theory, or as relevant to this research, a substantive category.
Hence, there are three points investigators need to address in order to validate this
kind of research. First, the adequacy of the research process needs to be judged,
because it may affect the substantive category which is being tested or elaborated

101
(Strauss & Corbin, 1990, p. 252). A second point of validation is determining the
usefulness of the substantive category. The substantive category needs to be well
integrated, relevant to the question and must justify the major variation in the
phenomenon or process that has been studied (Baker, et al., 1992, p. 1359).
Finally, the substantive category (core categories) needs to have “fit”, and “work”.
Fit means that all categories must be clearly evident in the data. Moreover, the
theoretical proposition must have relevance to the participant group and practice
group. To work, a theoretical proposition should also explain what has happened,
describe what is happening and predict what will happen (Baker, et al., 1992, pp.
1358-1359; Cutcliffe & McKenna, 1999, pp. 376-377; Glaser & Strauss, 1967, p. 3).
As Lomborg and Kirkevold (2003) argue:
“What we are looking for is a position that simultaneously
acknowledges the human constructed nature of social reality and retains
the objective character of this very same social area” (p. 197).
In this study, the research process can claim validity and reliability as a result of the
following steps. First, there was a clear understanding grounded theory methodology
and methods prior to the commencement of the study. This understanding is

102
demonstrated in the application of the theoretical tenets of grounded theory to each
phase of the study. Second, the substantive category, the core category (“taken for
grantedness”), in this study directly informs the research purpose which was to
determine how and why Taiwanese people with cancer are using NWM. Furthermore,
the substantive category or core category is relevant to the participant group in this
study and this is demonstrated in the data analysis.
Summary
This chapter has addressed the methods that were utilised in this study and the range
of strategies that were adopted to ensure both ethical and methodological rigour.
These include how participants were recruited, interviews were approached, and data
were analysed and the utilisation of memos. In addition, validity in translation of
interview data, the role of the researcher, ethical implications and validity and
reliability of this study have also been explicated.
The following chapters address the findings and analysis in this study. These are
presented in three chapters, the first of which addresses “the context” of decision
making of philosophical beliefs and social practices.

103
CHAPTER 5
Incorporating NWM: The Taiwanese Context
Studies indicate that more than 40% of people world wide use complementary and
alternative medicines (Astin, 1998; Eisenberg, 1998 & Eisenberg, 1993), either
separately from, or combined with, conventional care (Robinson & McGrail, 2004, p.
90). It is further estimated that approximately 75.5 % of the Taiwanese population
use non Western medicine to treat diseases or alleviate symptoms (Lew-Ting, 2005, p.
2112). In this study, decision making that brings Taiwanese people with cancer to use
non Western medicine (NWM) emerges as a complex and multi-faceted process.
In applying the theoretical premises of symbolic interaction, this chapter addresses
the patterns of use of NWM and Western medicine of the study participants and how
they came to integrate both forms of therapy into their cancer treatment regimes. As
Blumer (1969) argues, society as a whole may be viewed as symbolic interaction (p.
78). Consistent with this premise, the study of human life and social action considers
the realm of life under study as a dynamic process whereby participants give
meaning to the actions of others and, as a consequence, define and interpret their

104
own actions. In other words, people construct their actions through an interpretation
of the contexts within which they live. Interaction takes place between human beings
and these interactions are mediated by symbols, by interpretation, or by determining
other’s actions. Further, the interpretation process maintains, redirects and changes
the way participants construct their lines of action (Blumer, 1969, p. 53).
Using this perspective, we are able to enter the life world of the individual and to
obtain an interpretive understanding of an individual’s actions and meanings and the
motives behind actions (McCraken, 1988, p. 9). The reality that exists in social
enquiry is the result of interpretation (Annells, 1997, pp. 122-123). But although
social reality is ongoing, changing and dynamic, it does not go against the essence of
social reality (Lomborg & Kirkevold, 2003, p. 198).
The context is important and a focus on human action does not constitute a denial of
social structures. As Maines (2001) argues, meaning construction occurs through the
interaction of social structural pasts and symbolic interpretative processes (p. 54).
Thus, this chapter, in providing a starting point for extending our understanding of
the processes whereby people with cancer in Taiwan come to use different forms of
therapy, first considers historical factors that have been important in conditioning
105
(although not determining) the context of the study phenomenon. Second, the chapter
explores the ways in which the participants perceive and integrate the use of NWM
and Western medicine.
The Context
During the past century, the health care system in Taiwan has undergone significant
transformation. Prior to the Japanese occupation of 1895, the mainstream health care
system was dominated by Traditional Chinese Medicine. During the Japanese
occupational period, the practice of Chinese medicine was discouraged and priority
was given to the development of modern Western medicine (Chi, 1994, p. 310).
Many Western medical schools were established and as a result more and more
Taiwanese people were exposed to Western medicine. The health care system was,
therefore, transformed as Western medicine was systematically established in Taiwan
during the late nineteenth and the early twentieth centuries.
However, since the time of the transfer of political power to the independent
government within Taiwan (Republic of China) at the end of World War II,
Traditional Chinese Medicine and Western medicine have both been acknowledged

106
as integral to the Taiwanese health care system. During this time, as in the Republic
of China, the policy emphasis in Taiwan shifted to the co-existence of Chinese and
Western medicine (Chi, 1994, p. 311).
Soon after the transference of political power, the Taiwanese government established
a medical college in 1958 that focused on developing and retaining Traditional
Chinese Medicine (China Medical College, now China Medical University). This led
to a gradual resurgence of Chinese medicine in Taiwan. More recently, a
commitment to the co-existence of approaches to health care was reflected in and
reinforced through the 1995 national health insurance policy coverage of both
Traditional Chinese Medicine and Western medicine.
Taiwanese people have, therefore, experienced differing health care cultures within
different political environments. The legacy of this historical trajectory is that people
interact with Traditional Chinese Medicine, Western medicine and a combination of
both in contemporary Taiwan.
Many different classifications are utilised in Chinese medicine. This structure of
health care is made more complex by the variety of therapies that constitute Chinese

107
medicine and which are generally categorised into three forms (the most well known
and most comprehensive). The first is classical, or traditional, Chinese medicine
based on the intellectual concepts of Yin and Yang and the five elements2 (a
philosophy that has existed and evolved for over 3000 years) and its key components
are acupuncture and herbal medicine. This form of medicinal therapy is formally
institutionalised and practitioners are required to qualify following a regulated period
of training. The second category is the folk medicine tradition which has its origins
in various locations in China and consists of practices that are not regulated and are
passed on by word of mouth. The third form of traditional healing refers to the use of
religious practices which adhere to a belief in the supernatural determination of
disease and thus magical procedures (Lee, 1981, p. 259). Perceptions of health and
illness are thus mediated through ongoing interaction with a range of therapy forms.
The Patterns of Use of Western Medicine and NWM
Most people with cancer today typically undergo a complex (surgery, chemotherapy
and radiotherapy and so on) and long term treatment journey when diagnosed with
this disease. In circumstances where two distinct health cultures exist, as is the case
2 The five elements (Wu Xing, 五行) include metal, wood, water, fire and earth.

108
for the participants in this study, people arguably encounter a more complex decision
making process regarding their cancer treatment. This often includes the processes of
making decisions that determine whether they will seek to utilise NWM (short term
or long term), Western medicine, or a combination of these in their cancer treatment
journey. The process whereby such decisions are made is, in Blumer’s (1969) terms,
one of mediation between incentive and response in human behaviour (p. 79).
There was considerable variation in the extent to which the participants in this study
demonstrated commitment to the use of NWM and in the way in which they
combined NWM and Western medicine. For example, there are those who firmly
believed in Western medicine: “I mainly use Western medicine. After all, this is more
based. Those non traditional (treatments) are mostly word of mouth.” (Ms. Han) And
“Cancer cells need to rely on Western medicine…this disease needs to rely on
Western medicine, others are complementary.” (Ms. Zhu)
Mr. Shi’s family also portrayed Mr. Shi’s beliefs in Western medicine in the
following account:
My husband relied on Western medicine; he did not take something else
so he kept so long. He did not take secret remedies. He did not take

109
anything. The friend, who is dead, he took herb medicine or healthy
products. He still died after taking them. When my husband heard this,
he did not dare to take (Chinese medicine).
Similarly, for Ms. Qian, Western medicine was the only therapy to be considered for
cancer. She made the following comments about how she perceived NWM and
Western medicine:
I think the most correct way…for example, now you are more serious,
(you) should use Western medicine. Western medicine is the best
treatment. (Western medicine) suppresses it (cancer) down. When (you)
get well and stable then (you think about) maintenance. It is right. This
is more correct…when you get a serious disease, (it is) impossible to
use Chinese medicine. (It is) still Western medicine that saves people.
It’s my feeling. It’s my experience. I feel (it is) still Western medicine
that saves people. Chinese medicine is impossible to save people.
Chinese medicine takes good care of health. (If) we don’t have serious
disease, (we) use Chinese medicine to take good care of health. Now (I
am) ill, (I) still use Western medicine when it is serious, (it is) more
correct. (It) won’t delay your disease, it is more correct to use Western
medicine.3
3 Some quotes used in this study may look repetitive. However, the extracts were used as a whole and not edited, to avoid altering the meanings.

110
Ms. Qian’s perceptions are considered neither unusual nor dominant. Studies of
Taiwanese patients, suggest that there are differences in views regarding the use of
non Western medicine. For example, the Chi et al. study (1997) concluded that
participants were equally divided over perceptions of the effectiveness of either
Chinese medicine or Western medicine as treatment for cancer and other potentially
terminal diseases (p. 45). The study found that 24.2% of participants perceived
Chinese medicine as more or much more effective and 27.5% considered Western
medicine more or much more effective (Chi et al., 1997, p. 45). These findings
suggest that after decades of development and following the institution of an
independent government within Taiwan (Republic of China), Traditional Chinese
Medicine, although not as institutionally strong as Western medicine, has endured as
an important health practice.
Mr. Shi’s words reflect the view that both Western and non Western medicine hold an
important place in Taiwanese health care. Mr. Shi stated that Western medicine and
Chinese medicine performed quite different functions in cancer treatment.
Chinese medicine, if (they are) symptoms, (they) can be treated. If it is
cancer, Chinese medicine may not be able to deal with…so Chinese
medicine has its benefits; it can deal with small symptoms. If they are

111
big ones, it can’t deal with them. (But for conditions)…such as a cold,
bones, soreness, Chinese medicine can deal with. As far as cancer cells,
it just can’t.
Mr. Shi’s views are consistent with the findings of the Chi et al. study (1997) where
more than half the participants considered Chinese medicine a better option in
treating conditions such as a fracture or sprain (p. 44). Hu’s study (1999) similarly
found that people in Taiwan tend to seek traditional treatment (Chinese medicine) in
fracture situations and for nourishing the body after illness (p. 189). In addition, a
recent Taiwanese study indicates that people in Taiwan are very satisfied (92-96%)
with the practice of combining Chinese and Western medicine (Lee & Liang, 2006,
p. 234). Some, therefore, believe that Western medicine is the superior treatment for
acute or serious health situations. Chinese medicine, on the other hand, may be seen
as being slower and less effective, but as not having the damaging side effects of
some Western medicines (Holroyd, 2002, p. 735).
Studies involving patients from Eastern backgrounds suggest non Western medicine
approaches may be commonly used to maintain health (Zhong, 2001, p. 343).
Consistent with Eastern views of health, these studies reaffirm the view that such

112
therapies may be used since they are seen to supplement the body and are a key to
recovery from illness (Chen & Mao, 2001, p. 40).
Such a view may explain the perception of some that NWM treats symptoms only
and not the disease. In other words, NWM may be considered an interim measure
and one that will not affect a permanent cure. For example, Mr. Chen stated:
I think that my personal opinion (is that), it is impossible to treat cancer
by using Chinese medicine… (In Chinese medicine) you take something
poison and see if it leads to (cancer cell’s) death. Yes, but that is 治標不
是治本 (it is a stopgap measure that is not effective for achieving a
permanent cure)…China, from ancient times to the present, (Chinese
medicine) is to deal with tendon and bone (problems). That is more
useful…from ancient China, there are many death with unknown
(reasons). That may be cancer. It can’t be cured. It can’t be cured by
Chinese medicine. Five thousand years history, It can’t be cured before,
why now?...
Mr. Yang had similar thoughts towards NWM. As he stated:
I feel the Chinese Medicine does not effect a permanent cure; it only takes

113
stopgap measures…he (the Chinese Medicine doctor) 把脈 (takes your
pulse in Chinese Medicine way). How much can you understand by
taking the pulse of the patients? Sometimes, even my disease, the Chinese
medicine may not know what it is…
These participants see NWM, in this case Chinese medicine, to be “a stopgap
measure that is not effective for achieving a permanent cure” (治標不是治本).
Where NWM is used among people with cancer, it is to alleviate symptoms.
The social reality of these views has undergone a significant shift over recent
decades. In Martin’s early research (1975), which investigated medical systems in a
Taiwan village, we see that the most common response obtained was that “Chinese
medicine cures the cause; Western medicine cures the symptoms” (pp. 128-129). This
finding was reinforced some decades later in Wang’s (1990) study of people living in
the middle of Taiwan where nearly 90% of participants found fewer side effects
when using Traditional Chinese Medicine and thought that Traditional Chinese
Medicine had a greater possibility (66.1%) of eradicating a disease than Western
medicine (p. 27).

114
The data in this research suggests that the environment of health care in Taiwan is
changing and this is reflected in the meanings the participants attribute NWM and
Western medicine. The social process here is one of the individual responding to the
environment based on past and present beliefs, individual actions and new
circumstances, all of which may either reinforce existing beliefs or lead to change
(Mead in Chang, 2004, p. 414). This means that human beings act on the basis of the
meanings that things have for them. We recognise and define the situations that we
encounter and put meanings to them and in addition, we also create new meanings as
we encounter something new or different (Blumer, 1969, p. 132). In other words,
human beings are continually devising new meanings as they interpret situations and
events that are confronted.
The social process involved in generating new meanings perhaps explains why some
participants alternated between using Western medicine and NWM. Ms. Qin, for
example, before she was diagnosed with cancer, thought that she had a cold and
dealt with this situation as follows:
(I) caught a cold, (I) could not get well after catching a cold for a long
time. (I) then tried Chinese medicine, and then Western medicine. I went

115
to see the ear, nose and throat doctor. Then, I came back to see Chinese
medicine doctor… then again the ear, nose and throat doctor…
Mr. Wei also accepted both NWM and Western medicine:
I originally accepted Chinese medicine therapy. It is natural from the
concepts since childhood…as far as Western medicine and Chinese
medicine are concerned, we have no conflicts. If (you) feel very
uncomfortable, (you) try Western medicine first; (when you) get better,
(you go to) see a Chinese medicine doctor…like my family, if they
catch a cold, they go to see Western medicine doctor first and have a
shot and take medicine. Then, (when they) get better, (they) start to
take Chinese medicine…we do not repel non Western medicine, we
accept both…like my parents, same time, (they) see Western medicine
doctor, after that, (they) see Chinese medicine doctor in the afternoon.
It is very natural. (They won’t) feel special, strange or conflict.
However, others firmly believed in NWM. For example, Ms. Zhang’s husband had
an affirming experience from the use of Chinese medicine. He stated:
I had bleeding in my brain at that time. ╳╳ (the doctor in the hospital)
wanted me to be operated on, I escape. He (the doctor) asked me to
shave my hair. I said it was too much trouble to shave hair, I went

116
home. (Somebody) told me (to take) the core of moon peaches (and to)
add lots of honey. (I) added lots of honey and drank it. Then (I) went to
the Chinese pharmacy, had a prescription for 五寶散 (Wu Bao San,
the name of the prescription). (I) took (it) for a while. I went to check
up in ╳╳ (the hospital) after two weeks, the blood (in the brain) is 20%
left.
For others with cancer, no clear distinction was made between Western medicine and
Chinese medicine in terms of their potential to cure illness. As Ms. Zhu commented:
I feel everything has its best kick and has its advantages and
disadvantages (各有千秋啦,各有利弊 )…somebody takes Chinese
medicine or herb medicine then gets well…somebody controls quite well,
somebody is cured by Western medicine. How to explain it? (He or she is)
cured by Western medicine. But during the treatment, he or she may try
something else. You can’t be sure. Like me, I try something, but (I) did not
improve, this is my situation, but I feel some herbs are not bad, many
people take then and get well.
“Each has its expertise, each has its advantages and disadvantages (各有千秋, 各
有所長)” indicates the views of people with cancer regarding Western medicine and
NWM and why they may be using multiple approaches. Martin’s (1975) field work
117
study on medical systems identified similar responses (p. 128). In addition, a recent
Singaporean study similarly suggested that the majority of NWM users (86%)
believed both Western medicine and NWM had distinctive benefits (Lim et al., 2005,
p. 20).
However, while some participants saw Western medicine as fundamental to their
cancer treatment and others saw NWM as just as valid a therapy, there was a strong
sense that Western medicine weakened the body and that NWM supported the body.
As Mr. Zhou stated:
(I) had worse appetite when (I was) taking Western medicine. It got
better after taking Chinese medicine…(I) ate more after taking Chinese
medicine. (pause)…(I) ate more meals, (I had) more than five meals
each day.
Mr. Sun similarly described the following account:
There was no (oral) Western medicine; (I) mainly took healthy products,
because they (healthy products) had fewer side effects and less damage
to the body. If (I) took Western medicine, (it) might cause liver, stomach
or kidney (pause) so I avoided it if I could. I took less medicine; I relied

118
on exercise. Then, (I) took nutritious (foods), enough nutrition to keep
healthy.
Thus people who undergo Western cancer treatments experience and respond in
various ways to these treatments. A significant factor is the perception that Western
medicine is toxic and that it weakens the body systems. As Ms. Han commented:
My left leg is painful. It becomes difficult to move. Then, (I) rely on pain
killers; it is not a good way. Pain killers are not good for the liver, not
good for the liver…medicines need to excrete. Don’t they need to go
through liver or kidney?
Moreover, Mr. Zhou described his experience:
(We came to) see a Western medicine doctor first…after several weeks,
about one month, (We) gradually complemented with Chinese medicine,
because taking Western medicine would damage the liver.
Ms. Zhu also illustrated this point:
Of course, it’s quicker to see a Western medicine doctor. I feel Western
medicine is quicker in treatment, but Western medicine would damage

119
the body…Western medicine is a slow poison, everybody knows…you
take Western medicine at the end, (your) stomach ache, like
chemotherapy has also (damaged the body). My eye (sight) is blurred.
Do you know? It is blurred, I can see it clearly only when it is close. If I
see (somebody) in distance, the face is blurred.
In addition, Mrs. Shi in reflecting upon her husband’s experiences said:
The whole person became unconscious after the injection…(it is) agony
and couldn’t get up. (The effect) is just for short time, it still grows
again. (I want to) ask him to give up.
These comments reflect concern about aspects of Western medicine and specifically
the side effects of invasive treatments. Indeed, a number of studies (Andrews, 2003;
Verthoef et al., 1998; Wysong, 1998) point to a perception that Western medicine is
over-reliant on medication administration and that this is associated with drug side
effects. Andrews’s (2003) UK study indicated that 21% of participants were of the
view that orthodox medicine over medicated and that complementary medicine was a
more natural alternative (p. 345). People may therefore seek to avoid uncomfortable
side effects from orthodox therapies by using alternative medicine (Wysong, 1998, p.
40).

120
Some participants started to use NWM immediately following diagnosis and not in
conjunction with Western medicine. These participants often saw NWM as an
alternative rather than complementary therapy.
Doctor X told me that I was diagnosed as lymphoma. After three or four
days, I started to take 牛樟菇 (Niu Zhang Gu, one kind of mushroom). I
knew it from more than twenty years ago…I do not want to have conflict
with Western medicine…I then avoided it as much as I can. I stopped one
week because of chemotherapy. Then, I took it everyday…(but) I stopped
them (Niu Zhang Gu and other herbs) when I was admitted into the
hospital…stopped all of them. (Mr. Wei)
Others ceased NWM when receiving chemotherapy:
I did not want to take anything else (NWM) when (I was) doing
chemotherapy. Then (they) won’t conflict with each other. (Ms. Wu)
The majority of participants, however, used a combination of Western medicine and
NWM which they took simultaneously. Several studies (Chiou, 1999, p. 398; Teng et
al., 2000, p. 217; Xin et al., 1996, p. 127) report that the practice of combining

121
Western medicine and NWM at the same time is common (between 60-82% of
people) in Taiwanese daily life. This is consistent with the findings of this study. Ms.
Chu made the following comments about this issue:
I still mainly use Western medicine and use Chinese medicine as
complementary. (I use) that (healthy products) as dessert…I take Western
medicine before meals and after meals, I take Chinese medicine after
meals, one hour apart between the two…following the Western medicine,
he (the doctor) said to do the chemotherapy then I did. I take Chinese
medicine taken after meal. There is one hour apart between Western
medicine and Chinese medicine.
The significance of NWM use in the treatment programs for people in this study was
also reflected in the timing with which such therapies were used. For example, some
participants modified their treatment programs depending on their perceived
responses to treatment. For example, Ms. Qin also stated:
If sometimes you take Western medicine, but it is not effective, (you) try
Chinese medicine. (You) take Chinese medicine for a while and then (you)
take Western medicine for a while. Like this, you change back and
forwards.

122
As the Chi et al. (1997) study indicated, almost a third of participants indicated that
they would choose to use Chinese medicine if it appeared to be more effective than
Western medicine under certain health conditions (p. 44).
Similarly, where there was a recurrence of cancer and a sense that Western medicine
had failed, some then turned to NWM. As Ms. Shen stated:
At that time, my thinking was (it) may still be more effective by using
(Western medicine) doctor’s way. This was the thought at that time.
Later on I wanted to try (NWM), because I also did the chemotherapy.
But why do I still have a recurrence? I felt in my mind a little bit
disappointed. I would like to try something different.
In contrast, Ms. Zhang ceased herbal medicine when her health deteriorated and
sought further advice and treatment from Western medical practitioners. In her own
words:
(I) couldn’t walk; suddenly (I) couldn’t walk. I told you that before (I)
could walk by placing a hand on something for support… suddenly (I)
couldn’t walk with support. (We) went to hospital otherwise. I stopped
taking (herbal medicine) then, my son worried, too, (We) went to the
hospital quickly otherwise.
123
Changing experiences thus result in an ongoing and unfolding process of an
individual’s conceptualisation of health and his/her priorities and values (Chan et al.,
2006, p. 303). As Mr. Shi reflected in the following account:
I had body strength when I took them (nutrition supplements), right, it got
better, but I tried not to take for a while, I lost (body strength) all over
again…I test if it is effective. The result is that it is effective when I take
them, it is not effective when I stop taking them...
Ms. Xu had higher expectations of NWM (Fa Lun Gong, 法輪功) that she had used.
In her own words:
I thought to get cured when I try this (Fa Lun Gong), because there are
always side effects in Western medicine. I felt scared. I was afraid of
what would happen after taking (Western medicine). It may get more
serious after treatment. I was scared. (My immune) resistance was
worse at that time. (I had) an oral ulcer. (I had) an oral ulcer after
treatment. One time, after I took and injected medicine (for a period of
time), I developed earache. Nothing was found after examination. (It)
can’t be treated. (It) was very painful. (My) ears were suddenly cured
after I practiced Fa Lun Gong.

124
We see, therefore, that new experiences or situations lead to the formation of new
definitions. The interpretative process goes through a digestive phase in which an
individual compares experiences and then transforms an interpretation into action
(Blumer, 1969, p. 133). When a developing concept leads to action that does not
have the desired outcome, new actions are developed (Blumer, 1969, p. 157). Thus,
people act after they interpret the actions of others and the places and incidents that
are the context within which an act takes place (Gusfield, 2003, p. 122). This can be
seen in Mr. Shi’s decision to cease using NWM.
Thus an individual’s conceptualisation of health and his/her priorities and values is
an ongoing process and this helps to explain why the participants in this study made
a range of decisions about the use of Western medicine and NWM. Some utilised
different therapies at the same time and others vacillated between using one or the
other treatment mode depending on issues such as beliefs and perceptions about
treatments. This is depicted in Mr. You’s reflection on his experiences:
(I) lifted oranges (the participant is an orange farmer), (I) hurt my back.
(I) went to ╳╳ hospital. (I) had X ray…nothing was found and he (the
doctor) said (you) may be too tired, hurting the nerve. After one month,
125
(I) was still sore. (I) changed to Chinese medicine massage for four
times. (I) got very sore in the middle of the night after the fourth time.
Then (I) changed to Western medicine the second day. (I) had a needle
and injected pain killers. (I) saw Western medicine doctor, took the
medicine and had a needle. (I) still felt pain the second day…(and) a
dry cough, dry cough. Sometimes (I) took Chinese medicine, sometimes
(I) took Western medicine. Then, it got better, not coughing…
This process was also reflected in Ms. Qin’s account:
The doctor asked me to do chemotherapy. (I) heard somebody say
doing chemotherapy is terrible…(I) did not dare to do it, it was
delayed for one month and I went to see the Chinese medicine doctor.
Somebody introduced (him to me), it is not the one I see now. Then, I
took (Chinese) medicine for one month. I had a very serious cough at
that time. It was a very serious cough. I almost couldn’t breath. At
that time, I decided I still needed to do chemotherapy…
Others pointed to various reasons for engaging with NWM. Although Ms. Zhang
sought advice on Western medicine, she chose to take a herbal remedy:
(Somebody) takes it (herb remedy) and gets well…he (the friend) said it
is necessary to have patient to take that (herb remedy), someone takes

126
300 prescriptions of them, (he or she) still takes. It costs only NT 70 (AS
2.9) dollars for each prescription, (it is) not expensive…I am not afraid
of medicine, but it becomes my worry after taken. (I) worry why the
more I take, the more painful in the whole body…no, I just take this, I
think I can not mix the two (Western medicine and herb remedy).
Forms of NWM Use
This study has also found that people integrate many different forms of NWM with
Western medicine during their cancer treatment journey. Some people with cancer
use nutritional supplements, some forms of which are considered to be Traditional
Chinese Medicine. This therapy was the dominant form of NWM used by the
participants in this study. Participants introduced nutritional supplements either at the
point of diagnosis or at some point during the cancer treatment. Mr. Jiang used
Chinese Medicine and commented:
Personally I mostly take Chinese medicine…medicine would not damage
the stomach so much. Although it is not so quick to be effective, it is
better for the body.
Further, Ms. Zheng explained how she came to use nutritional supplements:

127
That is because other patients introduced it. He said it (nutritional
supplement) is effective after taken. I tried. It focused on the disease and
it would be better if (we) take it. Then, I tried…when I couldn’t eat other
things, I ate that (nutrition supplement). I felt that it could maintain
physical strength and I would get well sooner…I felt first I am still young,
(my) father considered (I) am still young and have enough resistance.
Second, it (Ya Pei, one kind of high protein formula milk) is like medicine.
Ya Pei is like chemotherapy medicine, only it is lighter, it is a lighter
medicine. I felt it is only complementary. (I) did not mean to use as
medicine…I am afraid that I do not get enough nutrition. I then went to
take medicine (Ya Pei) in order to supply the nutrition I do not get.
Others also have long held beliefs about healthy products and these informed their
choices of therapy during the illness trajectory. 有病治病, 無病強身 (it treated
your disease if you had one; if you did not have disease, it could help you to take
care of (your) body) is a common belief of Chinese people regarding healthy
products or nutrition supplements. As Mr. Zhao illustrates here:
After I took this (healthy product), (my) body became very healthy and
in very good spirits. (It)(healthy product) treated your disease if you
had one; if you did not have disease, it could help you to take care of
(your) body. My friend… who is a teacher…I also gave (it to) him. He

128
said it was good after taking (it) (healthy product).
Ms. Wang similarly utilised nutritional supplements, but here to deal with loss of
appetite due to side effects of cancer treatment. As she reflects in the following
account:
(I saw) it as snack, like water. (I) drank it when (I) had time…(it is)
effective, not bad…I did chemotherapy and radiotherapy together at
that time. (My) body was weaker, (I) couldn’t eat anything at that time.
I even couldn’t drink An Su (high protein milk). I was retching. After
injecting chemotherapy, (I) would vomit; (I) couldn’t eat at all. (I)
drank milk later on and ate rice soup. (My family) cook pork rib rice
soup. There was a period of time where the oily (foods made me retch)
(I) couldn’t eat.
Other participants combined Western medicine and nutritional supplements because
they considered that the supplements (or so called healthy products) are good for the
body. As Mr. He stated:
But the doctor also injected that (the medicine), he injected beforehand
(chemotherapy) to stop the vomiting…healthy products are all good no
bad…I take as usual. It is quite smooth after taken.

129
Mr. Lu also had similar views of nutrition supplements and stated:
Doctors know if healthy products are good or bad…healthy products
are all good not bad…they (healthy products) are made from big
factories and many people are taking them…(We) need enough
nutrition. If nutrition is not enough, if we don’t have enough nutrition,
it will be awful.
Of those who decided to use nutritional substances during the cancer treatment
journey some adjusted treatments to suit their perceived changing health needs. Mr.
Chen stated that:
I took green algae sometimes, because it is more alkaline…(I had) more
energy (after taking)…I took double dose. It doesn’t matter.
The cancer journey is thus a process whereby people with cancer interact with both
Western medicine and NWM. Some people hold the belief that natural remedies may
be safer and more effective than drugs prescribed by physicians (O’Callaghan &
Jordan, 2003, p. 31). People come to know of these healthy products, or so called
nutritional supplements, either through consultation with a doctor of Chinese
130
medicine or through word of mouth. However, although Chinese medical
practitioners may be regulated, the selling of nutritional supplements and other
similar products is not controlled. Providers of NWM often disperse information
about such treatments in an incomplete form and without endorsement from
regulatory authorities. In this study, most participants who used nutritional
supplements as NWM did so without discussion with health care professionals.
Some participants made a clear distinction between nutritional supplements and other
therapies. Some also indicated that they were not yet at the stage where they were
willing to try alternatives to nutritional supplements. An example is Ms. Wu who
stated: I did not feel very uncomfortable in the body now, so I did not want to try
(other NWMs) yet. Mr. Jiang also saw the use of Western medicine and NWM as a
process. Because he did not finish one (Western medicine), he did not want to start
others (NWMs). In his own words:
You finish one process then start the next process. Because I do not
finish yet, I don’t know…these are too far to consider. After (I) finish
this, then (I) start another treatment…you do chemotherapy. Follow
Western medicine then use Western medicine as possible. Don’t mix
them. Then, when you do regularly check up, regularly check up, you
can find something else. (You can have) more ways to increase

131
effectiveness.
While nutritional supplements were most common, the participants did use other
forms of NWM. For example, Mr. Chen stated:
(I) started when the disease was found…Hei Teng (one kind of
herbs)…grinding into powder. (I) sent (it) to somebody to grind into
powder and take it as powder, or boil it with water and drink as tea…(I)
stopped (it) when (I was) doing chemotherapy, this is anti-poison. That
(chemotherapy) is poison, I was afraid they would clash with each
other. I did not dare to take them at the same time…I feel this is
effective. I felt numbness on my hand, not be able to touch a pen…I felt
numbness like was shocked by electronic. It was so painful, too painful
to touch anything. It (Hei Teng) can improve this, I feel very good.
A study involving Taiwanese patients with metastatic cancer found that although
herb medicine (23.7%) and acupuncture (40%) had no effect on the cancer itself,
patients reported that these therapies were able to relieve palliative symptoms caused
by cancer or cancer treatments (Xin et al., 1996, p. 132).
In addition, Mr. Li utilised Chi Gong to regain the physical strength he had lost as a

132
result of radiotherapy side effects. He made the following comments:
So (the neck) becomes harder, no saliva. I went to subsequent (doctor)
visit, I asked the doctor, can it improve or not and he said (it) can’t be
improved. I said I can think by myself. I trained my body stronger…then
I (practise) Chi Gong. (pause) If (the things) I like, I watch, learn and
practise. Guo Lin Xin Chi Gong, I practised everyday in one stage…
Mr. Li also perceived the practice of Guo Lin Xin Chi Gong as an effective treatment
for cancer:
I feel this (Guo Lin Xin Chi Gong) is better. Why? The reasons are said
inside (point the book of Guo Lin Xin Chi Gong). The reason, because
the cancer cells do not like oxygen, (you) breathe in (with the action of
breathing in) and bring in a lot of oxygen in red blood cells. At this time,
it (the oxygen) can control cancer cells, even kill cancer cells. So, it
(the cancer cells) shrinks. Cancer cells shrink and shrink. Let it (the
cancer cells) withers away...
Chi gong consists of exercises that combine meditation, non-impact movements, and
breathing activities. It is argued that the practice of chi gong re-establishes a balance
between the mind and body thereby addressing physical problems and strengthening

133
the immune system (Bottomley, 2004, p. 253). In addition, chi gong is seen as energy
exercise and combines physical exercise and meditation in order to eliminate energy
obstruction and harmonise the different sections of the body. The overriding
principle is one that underpin Traditional Chinese Medicine and this is that for any
part of a person to be healthy the whole body must be taken into account; body, mind,
and spirit at once (Graham, 1999, p. 78).
Although chi gong has its origins in ancient China, few participants practiced this
form of therapy. Chang and Li (2004) found similarly and suggested that this may be
because cancer sufferers are too fatigued to practice this exercise (p. 42, 44). Only
three participants (Mr. Li, Mr. Jiang and Ms. Xu) made reference to the use of some
form of chi gong during their cancer treatment journey. Two participants (Ms. Shen
and Ms. Han) noted that they used to practice chi gong but were now too weak to
practice.
Regulation of Diet as Therapy
The preparation of specific foods is seen, by some, as a form of Chinese medicine.
The use of food as medicine exists in everyday conversation and thus is deeply

134
entrenched in Chinese everyday life (Holroyd, 2002, p. 743). Families believe that
diet and traditional Chinese medicine can be integrated and adopted into self-care
strategies (Simpson, 2003, p. 834). Mr. You’s family referred to the use of Chinese
medicine as a diet therapy to enhance body strength:
My husband’s good friend, he had liver cirrhosis. He had an operation
and he told me to use those Chinese medicines, Astragali Radix add red
Chinese dates and Lycii Fuctus, cook into water and let him drink it. He
said (it can) supply body strength. I cook everyday for him to drink…we
keep cooking pork rib rice soup for him to eat, that Astragali Radix,
Lycii Fuctus and red Chinese dates cook into water and drink as water.
They said (it can) supply body strength. (He) always eat like that.
Occasionally, because of wounds at that time, the doctor said (to us) to
drink orange juice. I let him drink ╳╳ (the brand name of orange juice).
(I) added collagen.
During the process of combining Western medicine and NWM, many people living
with cancer believe that there are certain dietary taboos which inform what they
should or should not eat. Mr. Chen made the following comments about this issue:
The Western medicine doctors do not believe what you can’t eat and what
you can eat, only Chinese medicine. The meat of chicken, duck and goose

135
are more poison…because chicken, duck and goose usually inject
antibiotics, too many injections, they are not good in meat. Animals
without tears, such as fish and prawns…do not eat if possible...those
without tears, do not eat if possible, because they are poison, too.
Certain dietary taboos are common to Taiwanese society. Chang and Li’s (2004)
study shows that 60% of the cancer participants consider that they should not eat
“toxic” foods such as duck, goose, eggplant, certain kinds of fish and sea food (p.
43).
In addition, Mr. Sun stated:
I feel eating natural foods is better. Those are not polluted. There are
many chemicals now and they damage the body a lot…those vegetables
with pesticides and fruits with pesticides, like we got cancer, we like to
eat organic more. Organic (foods) are chosen specially, (they) do not
have so much chemical pollution, so (we) eat those things better for the
body.
Summary (NWM Use as a Social Process)
136
During this journey, a person with cancer draws on concepts of health and each
individual’s conceptualisation of health is shaped by complex interactions between
the personal and the social dimensions (Chan et al., 2006, p. 302).
People adjust their therapies depending not only on perceived responses to the effects
of treatments but in accordance with belief systems that are grounded in cultural and
social systems. As such, people with cancer may combine both NWM and Western
medicine for short or long periods during their cancer treatment. They may also
alternate between NWM and Western medicine and between various forms of NWM.
We see, therefore, that the overall picture of the use of NWM and Western medicine
is a complex one.
The following chapters explore why and how people with cancer in Taiwan come to
use NWM. A number of significant dimensions have emerged from the data that
portray a process of interaction between philosophical beliefs, family connections,
community connections and professional relationships and practices. Each of these
dimensions is discussed, in turn, in Chapters 6 and 7. In their totality, these aspects
characterise the ways in which interactions at both the micro and macro levels inform
the decisions of those with cancer to use NWM. The analytical focus is on an

137
interpretative process which is used to discover relationships and concepts in the raw
data and to organise these relationships and concepts into a theoretical explanatory
scheme (Strauss & Corbin, 1998, p. 11).

138
CHAPTER 6
Philosophical Beliefs
The previous chapter explored the ways in which people with cancer in Taiwan use
both Western medicine and NWM. We noted in the chapter that human beings take
action when things have meanings for them and such meanings develop from, or
draw on, the social dialogue one has with others and from interaction with social
structures.
Two key points emerge from this understanding. First human actions exist as a
relationship between subject and object and not simply as a response by subject to
object (Gusfield, 2003, p. 124). Second, context and structure are integral to the
conditioning of meaning and human actions take different forms within different
contexts (Gusfield, 2003, p. 121). Thus, social interaction and context and how these
inform perceptions of the role of NWM appear to be complex and dynamic.
This chapter focuses on the contextual dimension of philosophical beliefs and how
such beliefs inform the views and perceptions of participants as they encounter the

139
experience of cancer and cancer treatment in their everyday lives. The theme
“philosophical beliefs” reflects an interactionist process whereby a person
communicates with others and checks, chooses, reorganises and transforms actions
within particular social contexts (Blumer, 1969, p. 5; Haworth-Hoeppner, 2005, p. 5).
In other words, philosophical beliefs provide an important context within which
meanings that surround a diagnosis of cancer are mediated.
Philosophical Beliefs
Health beliefs are accumulated from the experiences of individuals and from the
collective memories of a community and these form a human being’s interpretation
of life, birth and death, right and wrong and other beliefs and values (Quah, 2003, p.
2001). For example, studies conducted in western countries identify cultural
differences as a factor that may affect a person’s health and illness behaviours
(Thomas, 2002, p. 80). People from different cultural contexts may have different
explanatory models to define health and illness behaviours and they are likely,
therefore, to seek out different health care systems consistent with their beliefs about
their disease (Lin & Ji, 1998, pp. 6-7; Lai, 1997, p. 169).

140
As with people from other cultural backgrounds, Taiwanese people draw on
communal philosophical beliefs in constructing the meanings they attribute to illness.
Such beliefs provide explanations of disease and thus also construct the personal and
social meanings of disease. A person may, therefore, utilise a treatment which is
consistent with her/his explanation, an explanation which is contextual. For example,
a study by O’Callaghan and Jordan (2003) concluded that people who hold positive
attitudes towards complementary and alternative medicine may use these therapies
because the philosophies that underpin them are in harmony with a self-belief system
(p. 31).
In the context of this study, the emergent themes of traditional Chinese philosophy,
religious practices, and traditional Chinese proverbs and a belief in self destiny, are
conceptualised under the broad umbrella of philosophical beliefs. The relationships
between each of these dimensions present as a web comprising numerous
connections and interconnections.

141
An ancient Chinese medical textbook, Huang Ti Nei Ching Su Wên4, points out that
medicine is considered a part of philosophy, religion, general ethics, and life regimen.
Furthermore, it represents a oneness with nature (Veith, 1972, p. 10). Such traditional
philosophical beliefs thus see medicine as an integral component of all dimensions of
life, and these beliefs have endured in Taiwan.
Traditional Chinese Philosophy
The purpose of this study is not to focus on Traditional Chinese philosophy and
therefore the participants did not explicitly articulate their views on this tradition.
However, an understanding of Traditional Chinese philosophy is shown as a key to
how and why people with cancer in Taiwan use NWM.
Traditional Chinese philosophy is integral to the views and values of people in
Taiwan and is significant because it has been sustained in Chinese culture for many
thousands of years. This philosophical context is, in turn, important in shaping
perceptions of disease and affects the ways in which people interpret their symptoms,
communicate these to others and give meaning to them (Taylor, 2001, p. 199). For
4 Huang Ti Nei Ching Su Wên: a seminal work on traditional Chinese medicine, written four thousand years ago, in 2697 B. C. The original text is written in Chinese. The reference referred to here was translated by Ilza Veith in 1972.

142
more than 2000 years, Confucianism and Taoism have shaped Chinese traditions and
these belief systems continue to be a significant part of the Chinese traditional
cultural inheritance. Furthermore, Confucianism and Taoism are central to social,
moral, philosophical, political and cultural affairs (Woo, 1997, p. 85) and, as such,
influence concepts of health and health seeking behaviours.
Confucianism holds that where there is a discord of heart and mind a person can not
remain healthy and mental well being is, therefore, essential to good health (Ni,
1999, p. 30). The Confucian belief is that the human being is formed at three levels:
the physical, emotional and spiritual. To sustain a state of good health, a balance
must exist among these forces and between a human and the environment. There is
no separation between body and mind; they are always related in a dynamic way.
Thus, the human state is seen as a dynamic process, not fragmented, and closely
related to the environment (Graham, 1999, pp. 80-81).
In addition, the Tao philosophy in Taoism sees humans as a whole and exalts the
notion that civilisation should assist humans to be with nature or unite with nature
(Ma, 1990, p. 238). Taoists seek the best possible way for a person to live a life in
harmony with the cosmological and natural realms (Tsai, 2006, p. 685).

143
This belief in the importance of maintaining a balance of body, and body and
environment, is a central tenet of traditional philosophical beliefs which inform
traditional Chinese health practices. The Confucian belief of balance and the Taoist
naturalistic thinking both have an impact on the healing philosophy of Chinese
people. Hence, those who practice traditional Chinese medicine do not treat parts of a
person as isolated entities nor the person in isolation from the environment (Ni, 1999,
p. 30). This is illustrated in Ms Han’s comment:
Because taking those (NWMs) do not have so many side effects, I hope
then, if it is effective…these are not awful to take...If (I) can, (I) can keep
going to take all the way through to see if (I) can get a balance point...
According to Huang Ti Nei Ching Su Wên, traditional Chinese medicine originates
from the dual power of Yin and Yang theory (Lao, 1999, pp. 216-217; Veith, 1972,
p. 6, p. 13) which, in turn, is considered symbolic of both Confucianism and Taoism.
The phenomena underlying this theory classifies pairs of seemingly opposites where
Yang symbolises the sun, heat and light and Yin, the moon, coolness and darkness.
These pairs do not exist in conflict but are produced cyclically so that every
experience reflects the point at which either Yin or Yang dominates (Shih, 1996, p.

144
209, Veith, 1972, p. 14). This means that every phenomena, including sickness and
health, has the potential to appear as its opposite, or to change. A belief in the
concept of the body as a whole leads to the further belief that the imbalance of Yin
and Yang may cause diseases (Spencer, 1999, p. 6).
In order to put forth their dual power, Yin and Yang are connected by metal, wood,
water, fire and earth (known as the five elements). Yin and Yang and the five
elements theory (Wu Xing) explain Chinese perspectives on the natural sciences
including transformations in the universe, the nature of phenomena, and in human
beings (Lao, 1999, p. 217; Veith, 1972, p. 6, p. 19). These thoughts are deeply rooted
in Chinese culture (Du, 1997, p. 162) and they combine and construct the basic
theory of Traditional Chinese Medicine. In Chinese medical knowledge, the notion
that heaven sits in contrast to the earth, is also considered a reflection of our inner
body landscapes (Schroën, 2002, p. 94). Traditional Chinese medicine and
Traditional Chinese philosophy converge on this conceptualisation of nature and this
in turn shapes social behaviours.
Thus we see that one of the characteristic features of oral and written healing
traditions which demonstrate a community’s health knowledge within the cosmology
145
is Traditional Chinese medicine. The ancient Chinese developed these theories to
illustrate and define the nature of phenomena, such as illness and health (Shih, 1996,
p. 209). Where a balance is disrupted, disease occurs. For example, Ms. Chu
explained that:
Taiwanese may believe more in Chinese medicine…they consider that
Chi is needed to nourish. Because you do not have enough energy, Chi,
spirit (精氣神, Jing, Chi, Shen), then (you) get sick.
A belief in the balance of Yin and Yang is thus an important factor in understanding
the social behaviours of Chinese people (Shih, 1996, p. 209). This is significant
because it points to the importance of a belief system that underpins the use of NWM
in emphasising harmony with the body. It not only interprets nature and natural
phenomena but also reveals the subsequent social construction of the meanings of
symptoms, situations and relationships (Quah, 2003, p. 2001). Mr. Yang reflected on
the complementary nature of NWM in the following account:
Chinese medicine takes more care of you in complementing your body. I
think only about this. It (Chinese medicine) does not treat you. It does
not treat your original (disease).

146
The extent of the use of NWM in Chinese communities is evident in a range of
studies. Lim et al.’s (2005) study concluded that 99% of Chinese living in Singapore
utilise various types of Chinese medicine (77% of the population in Singapore is of
Chinese origin) (pp. 17, 19-20). Furthermore, people who use NWM consider that
the philosophies that underpin NWM are consistent with their own belief systems
(O’Callaghan & Jordan, 2003, p. 31). In other words and as noted previously, in this
tradition it is culture and not science that defines the usefulness of NWM (Chi, 1994,
pp. 308-309).
A study undertaken in the People’s Republic of China found that, of doctors who
received Western medicine training, 76% treated their patients with Traditional
Chinese Medicine, 90% used Traditional Chinese Medicine to treat their family and
friends and 82% would refer their patients to Traditional Chinese Medicine
specialists (Harmsworth & Lewith, 2001, p. 149). Despite the development of
Western medicine, Traditional Chinese Medicine continues to be a fundamental
component of healthcare in China. Although Western medicine is readily available in
most Asian countries, traditional medicine remains attractive because of historical
and cultural influences (Zhang, 2000, p. 139).

147
The concepts surrounding philosophical beliefs thus influence people’s attitudes
about cancer and behaviours in response to cancer. Yet, this is an interactionist, not a
static process. Consistent with Chinese philosophy, just as the existence of one
phenomena is never devoid of its opposite, so the thoughts and actions of people alter
according to changing experiences. In pursuing action, behaviours are purposive and
continuous and constructed in particular contexts (Millers & Hintz, 1997, p. 88).
Religious Practices
Religious traditions and practices are part of the daily lives of many Taiwanese
people and have a long evolutionary history. Chinese religious practice is particularly
complex because it has been formed from the different traditions of Taoism5 and
Buddhism (Veith, 1972, p. 10) and has developed and been reformed over thousands
of years. In addition, Chinese religion has a deeply entrenched connection with
Chinese philosophy (including Confucianism and Taoism) dating back to the Sui and
Tang Dynasties of 581-907 A. D. (Woo, 1997, p. 85).
5Religious Taoism is also referred to as Daoism. It is noted that Taoism as a religious practice differs from Taoist philosophy. Furthermore, Confucianism is not considered a religion (Budenholzer, 2001, p. 759).

148
The major religious beliefs in Taiwan include the dominant folk beliefs, Taoism and
Buddhism. However, the boundaries between these various religions are often
blurred. In Taiwan, for example, Buddhist deities exist in Taoist temples and vice
versa (Budenholzer, 2001, p. 756). The characteristics of Taiwan’s popular religions
are thus quite complex and they intersect or even transcend to a range of different
manifestations (Katz, 1999, p. 70). While it is a complex process, Carone et al. (2001)
argue that religion is the means by which people interpret their own lives and the
world around them (p. 999).
Religious tolerance has long been a feature of Taiwanese society. Over the centuries,
Buddhism and Taoism have allowed significant integration with Confucianism and
vice versa (Lee & Sun, 1995, p. 101). It is because Chinese religion has absorbed a
variety of influences from a range of belief systems that Chinese folk religion exists
as a combination of religious practices which include ancestor worship or veneration,
Buddhism and Taoism. This system of beliefs and the vast range of associated
practices have been passed down from generation to generation through various ways
such as oral tradition, formal cultural activities and rituals and literature.
149
Folk belief and the temple are everyday aspects of many Taiwanese people’s lives
because religious activities associated with folk beliefs are usually combined with
ritual and traditional customs (Chen, 1995, p. 58; Cai, 1992, p. 172). It is not unusual,
therefore, to find that people with cancer in Taiwan draw on a combination of
religious practices:
犯太歲 (Fan Tai Sui)6 is known every year. It is shown on 農民曆
(Nong Min Li)7…(I) felt not very smooth then. To start with, thieves
stole from the house at start of this year. How was this? (I had) never
been so unsettled. (I) had no ideas. Then, I suddenly got sick. It was just
on July in (the) lunar calendar8 (Ms. Zheng)
It is estimated that 70% of people in Taiwan adhere to some form of folk belief and
this may be a conservative estimate because, as Budenholzer (2001) argues, many
are reluctant to acknowledge openly their folk beliefs. The practices include fortune
telling, a belief in ghosts and spirits and burning ghost money to ancestors (p. 756).
As Budenholzer (2001) also points out, religion for Taiwanese people is far less a
6犯太歲 Fan Tai Sui: According to the lunar calendar (twelve animals symbolising designate years), if someone comes across the year of animal that is the same as the year that he/she was born, it is called Fan Tai Sui. This usually means bad luck. 7農民曆 Nong Min Li: This calendar has informed farmers since ancient China and is still widely used in Taiwanese culture. It guides the growing of crops and the prediction of a person’s luck in the coming year. 8 July in the lunar calendar: According to the lunar calendar, July is a ghost month. People believe that the ghosts can be released during this month to find their followers. In this way, people can avoid sickness and hospitalisation.

150
faith than a set of ‘activities’ for dealing with life situations (p. 757). This is
illustrated in the following examples. Ms. Qian’s folk belief influenced her decision
to seek guidance from a “fortune teller” (temple assistant or religious counsellor)
from household shrines and to combine this with Western medicine. She stated:
If you heard 算命先生 (the fortune teller)9 say you may have more
disease and agony this year…when we got sick, we went there to ask
him (the fortune teller). He said (you need to) pay more attention this
year; there is more disease and agony this year. Fate is more
long-winded and lousy. My feeling is different. I did not go last year
and the year before, but he said then you are not bad. It is true, my body
felt well. (I) went overseas, nothing happened. He said you need to pay
more attention this year, there may be something wrong with the body.
True, it is true. I said I have no choice but to believe it. My feelings and
my experiences (told me) the differences…My feeling is that he (the
fortune teller) is truly accurate. He told us our past and our future, not
100%, but at least 80%. We have no choice but to believe it…
9算命先生 (the fortune teller): The roles of fortune teller in Taiwan are varied. Ms. Qian actually means temple assistant or religious counsellor in the context of the interview. These roles usually exist in temples and involve special skills, such as tell the fortune and spirit calling.

151
Mr. Chen also stated:
(We) ask the Deity10, the Deity knows…the Deity said that it can’t be
delayed anymore. (You need to) go to a bigger hospital. It is true, I need
to have the operation after seeing the doctor…the Deity said it can’t be
delayed, this is not an ordinary disease.
Ms. Qian and Mr. Chen are what might be termed practical believers where religious
practice is based on practical usefulness and evidence. The concept of practical belief
is noted in this study and corresponds with the findings of an earlier study by Harrell
(1977) on modes of beliefs in Chinese folk religion in Taiwan. Harrell’s (1977) study
found that Taiwanese people’s beliefs can be categorised into four types: intellectual
belief (trying to make sense out of reality), true belief (accepting everything with
total innocence), practical belief (evaluating religion based on evidence) and
non-belief (denying religion is relevant) (p. 55). The tenets of religious practice for
practical believers rest on explanations from past experiences in particular situations
(Harrell, 1977, p. 59). In addition, the role of fortune tellers or so called Taoist
10 The Deity: the particular deity that Mr. Chen mentioned (he revealed the name of the deity later on in the interview) is the deity who is in charge of health and medicine.

152
priests is similar to healers in the local Chinese community. In so doing parts of folk
beliefs are thus common realms within health care (Kleinman, 1975, p. 608).
There are several forms of religious practice in Taiwan. It is common for people in
Taiwan to pray to the deity, whether Buddhist or Taoist and to chant A Mi Tuo Fo
(an incantation) when they have a serious illness. Several studies have found that the
most common religious practice of cancer patients in Taiwan is praying and chanting
Buddhist or Taoist scriptures (Chang & Li, 2004, p. 43; Lin, Liou & Wang, p. 1996,
p. 38). As Ms. Wang stated:
(I would) ask the Deity sometimes. (I would) ask somebody to 改運 (to
change fate through some special ritual ceremonies) sometimes… (I)
had this habit before (I was) sick…when I was in agony in the hospital,
I would pray. I would pray to 觀音菩薩 (the Goddess of Mercy)11 to
make me not feel so much agony or let me get well soon. Doing
chemotherapy and radiotherapy are sometimes very hard. (I would do)
the same at home, I would pray. A Mi Tuo Fo (an incantation), the
Goddess of Mercy, help me.
11觀音菩薩 (the Goddess of Mercy) is a common deity in Taoism.

153
Holroyd’s study (2002) found that where a participant’s experiences of hardship had
gone beyond social and physical possibilities, that person drew support from
supernatural causes and methods of treatment. For example, daily religious activities
and visits to temples are utilised to help the restructuring of a person’s world and to
rationalise suffering (p. 741). Because of the level of suffering, many participants in
this study looked to religious beliefs to give some sense to their situation. As Ms.
Chu illustrated:
A believer forever believes. (If) you believe (in religion), it is better
than being absent-minded…in fact, some people are really helpless.
He/she is helpless because he/she can’t find a way out. You feel some
people are in this (situation)…(I become) more calm in mind, more
accepting of the truth( that I have cancer) gradually (through religion).
A further study which investigated folk medicine utilisation behaviour in peritoneal
dialysis patients in Taiwan, found that 87.5 % of participants prayed to the Deity,
half of participants went to see fortune tellers and 12.5% of participants engaged in
spirit calling ceremonies. Almost three quarters (70.8%) of participants indicated no
obvious changes in the body; however, 79.2% of participants pointed out that they
obtained psychological support and had more confidence in the body (Liang et al.,
2002, p. 110, 112). In addition, Yeager et al.’s (2006) study shows positive

154
relationships between religious practice and a range of health outcomes in the
Taiwanese elder population (p. 2238).
These latter findings reflect the perceptions of Ms. Qin who stated:
I feel change a lot, it is true. I feel it is true…because when I was
diagnosed, it was not the first stage, it was the third stage, not easy then.
(I) saw many people, those (patients) who were doing chemotherapy,
(they) already have died…I feel religious belief really seems to help you
imperceptibly.
Religious practices were also important to Mr. Chen:
I believe in 密宗 (Lamaism, one kind of Buddhism), (I) would memorise
some spells. Before sleep, I memorise, say some spells and imagine
cancer cells disappearing…(You) can’t say it does not exist, it’s
mysterious…otherwise, from May to now (October), it is only a few
months. The doctor said to me I am stage III and have metastases. It went
to both my tummy and neck’s lymph nodes. It was treated up until now,
only a few months. Only 1.8 cm is left on the neck and other parts have

155
almost disappeared…I felt it couldn’t be repelled from Chinese medicine
or Western medicine. You need to cooperate with them (both).
One study which investigated the motivation and need for “spirit calling” in southern
Taiwan found that 80% of participants participated in the practice of seeking spirit
calling (Teng et al., 1999, p. 217, 222). For some of these patients, one explanation
for the cause of their disease was invasion by a ghost or the deity.
Participants sought guidance from the Deity to assist them to make decisions in
various situations including which hospital to attend. As Ms. Zheng stated:
(We) asked the Deity which one is better (and he said this one) ╳╳ is
better, so I transferred to here. (pause)(I) had no choice but to believe
this because the whole treatment was very smooth. (I) was hospitalised
for 28 days and fine. (I) recovered to be very normal except for side
effects in the middle, nothing else.
As has been noted, what is notable in this study is the pattern of co-existence of
religious practices and Western medicine. In Ms. Zheng’s view, when faced with
cancer, both medicine and religion are needed.

156
Both the person (the doctor) and the Deity are needed. It is true.
Because my disease occurred in July in lunar calendar, my mum
especially worried a lot, I 犯太歲 (Fan Tai Sui) this year.
Thus, although Western medicine is considered important, Chinese medicine and
folk medicine assume an essential role in determining the actions of people with
serious illnesses (Yang, 1992, p. 122). Many Taiwanese conceive of treatment where
“both the person (the doctor) and the Deity are needed” (要人也要神) (Zhang in
Wang, 2001, p. 93).
Indeed, even though over the last few decades Taiwan has become increasingly
westernised both economically and politically, a notable feature has been the growth
in the number of Buddhist and Taoist temples. Temples have a long history as one of
the most significant public arenas or public spaces in Taiwanese society (Katz, 2003,
p. 412). As Katz (2003) points out, the number of Buddhist and Taoist temples
increased from 3661 in 1930, to 5531 in 1981 and by 2001, there were 9,707 such
temples registered with the state (p. 396). Religious practices thus remain an
important facet of Taiwanese life.

157
As Budenholzer (2001) argues, science has not become the philosophy of life for
people in Taiwan but is valued for its capacity to address problems (p. 756). Over
100 years of development of Western medicine in Taiwan, the link between religion
and Western medicine has gradually strengthened if not philosophically, certainly in
economic and practical terms. This is reflected in an increase and particularly since
the end of martial law in 1987, in the appearance of religious sponsored hospitals and
clinics. In 2001, Buddhist and Taoist temples were operating 20 hospitals and clinics
and these are predominantly Western medicine based.
We see, for example, that for Ms. Qian, the combination of Western medicine and
religion is important. Her view was that one sustains the body and the other the mind.
I feel if a person is sick, the most important (thing) is to see a doctor. (It
is) most correct, I feel this is most correct. This is most correct. (It is)
impossible to get well by going to pray. Still if you are sick, first is the
doctor, (you) go to the hospital and see a doctor is most correct. (It is)
most correct. (The person who) can treat your disease and save your
life is the doctor. These are my feelings and my experiences. Secondly,
(pause) you should find sustenance in mind and consolation, (you) pray
to the Deity, go to pray and feel comfort. Otherwise, will you get well

158
by only going to pray and 收驚 (spirit calling, doing the special ritual
ceremony)? (It is) impossible. We need to have the knowledge of that…
Ms. Chu referred to religious therapy as an effective form of support. As she
commented:
I feel spiritual therapy is more important…for example, I am reading
Buddhist Scriptures…(I) believe a little in Buddhism…(it) calms (my)
mind down…because when (I) just heard the news (diagnosed with
cancer), (I was) shocked, I couldn’t sleep for more than a week. (I)
worried about the children…my mum was frightened. (She) hurried to
do 收驚 (spirit calling, doing the special ritual ceremony) and prayed.
My friends also did 收驚 (spirit calling, doing the special ritual
ceremony) and prayed. Anyway, doing the things they know. Put all
(blessing symbols) on then…平安符 (Ping An Fu, some kinds of
blessing symbols)12.
In addition, some participants experienced the ritual of taking “Fu” water13. For
example, Ms. Zheng stated: Somebody gives you “Fu” for you to take…“Fu” water.
12平安符 (Ping An Fu): it is usually a silk or cloth pouch amulet filled with prayers written on small pieces of paper, pinned on a person’s clothes and worn for protection from evil spirits. 13“Fu” water is often used for curing disease. People go to a Taoist temple assistant (Taoist priest) for blessed water which usually includes a piece of paper with some magic words written on it. People burn this piece of paper into ashes and add water. People either drink it or put it on clothes they wear.

159
She further indicated she had taken “Fu” water twice. This is consistent with the Yeh
study findings (2001) which investigated religious beliefs and practices of Taiwanese
parents of pediatric patients with cancer and found that it is common for the parents
to give “Fu” water to their children with cancer (p. 476).
Spirit calling, the wearing of blessing symbols (Ping An Fu) and taking “Fu” water
are all religious activities engaged in to keep diseases away or to restore health.
Hence, religious communal support may help some to increase their ability to cope
with illness (Yeager, et al., 2006, p. 2229). Furthermore, religious practice or a desire
to participate in communal events is believed to be a means to extend one’s life
(Johnson, 2004, p. 19). In this study, communal religious practices, conducted in
temples or at shrines, such as spirit calling, wearing Ping An Fu and taking the
blessing water (“Fu” water) provide examples of such beliefs.
Further studies in this area illustrate the importance of these practices. For example, a
study investigating the use of folk medicine among patients diagnosed with
colorectal cancer in Taiwan found that 80.5% of participants used folk medicine
which included addressing a deity, going to the temple and chanting the “A Mi Tuo
Fo” (an incantation) (Lin et al., 1996, p. 40). Similarly, Du’s study (1992)

160
investigated the cultural influences on medical behaviour of female breast cancer
patients and found a high percentage (92%) of participants used religion as a form of
NWM (p. 131).
Whether religious beliefs are practiced in an organised form or not, they present a
world view that addresses questions about suffering and more broadly, life’s
meaning. As noted, in Taiwan, religion gives guidance on how to live harmoniously
with ourselves, others and with nature (Taylor, 2001, p. 198). Through various
religions, using Buddhism and Taoism as examples, some specific rituals have
developed.
Mr. Chen believed his religion could help him with cancer in various ways, as
portrayed in the following account:
Our Lamaism…it is one kind of consciousness. (It is) possibly stronger
on consciousness, the more possible to achieve your consciousness.
Why? You have watched super power on TV. They rely on
consciousness to achieve (things) (pause) and we used this (which is
called) meditation. I imagined cancer cells were getting smaller, cancer
cells disappeared. (I) used the consciousness to control cancer cells.

161
(pause) and 迴向 (Hui Xiang)14. (It is) possible that I did something
bad in the previous life or something else. (pause) (I) read some
(scriptures) 迴向 (Hui Xiang) to 冤親債主 (Yuan Qin Zhai Zhu)15.
Ms. Han also followed similar practices although with the expectation that this would
have a psychological rather than physical effect. As she illustrates here:
Religion, he (the master) asked you to read scripture and confess…yes,
Buddhism, (they) think (the reason) for getting this disease, (it is)
possible 冤親債主 (Yuan Qin Zhai Zhu) (in the previous life., (The
master) asked you to read the scripture, confess and 迴向 (Hui Xiang).
Mental support…yes, after (I got) sick, religion would naturally come
along. Very strange, I didn’t know…I would pray before, but not so
pious…
Studies suggest that the actions of Mr. Chen and Ms. Han are not uncommon among
Chinese people with cancer. Yeo et al.’s (2005) study, which investigated the
community beliefs of Chinese-Australians about cancer, found that some people with
cancer attribute the cause to bad karma or to some wrongdoing in the present or
� 迴向 (Hui Xiang): Through certain kind of ceremonies, people usually practice scripture to give back blessing to the spirits. 15 冤親債主 (Yuan Qin Zhai Zhu): Those spirits to whom I owe to them in the previous life.

162
previous life (p. 179). As such, decisions about which treatments to use may be
influenced by religious beliefs and practice. In the case of Chinese societies, such
beliefs may include religious beliefs of “Inn” and “Ko” (cause and effect) (Chen,
2001, p. 270).
Chiu’s study (2000), which investigated transcending breast cancer and transcending
death among Taiwanese cancer patients, reached similar conclusions; the idea of
karma, originating from Buddhism, has impacted on Chinese worldviews for decades
and cancer patients believe that they are able to reduce their suffering by undoing
their mistakes in their past lives (p. 68). Because Taiwanese religious belief, the deity
and ghosts may inflict disease upon humans, when modern medicine can not explain
or treat the disease, Taiwanese people go back to religion rather than science (Zhang
in Lin, 1992, p. 112; Chen et al., 2005, p. 63).
Religious beliefs may lead people to seek guidance from the Deity on the use of
herbal medicines for particular situations. Du’s (1997) study on medicine, society
and culture indicates that folk medicine and substances and folk therapies are
inseparable and are usually combined with religious practices (pp. 152-153) or the so
163
called folk perspective. In Taiwan, the combination of folk beliefs and the use of
herbal medicine is a common occurrence.
In the whole sick process, one Deity asked me to take Qie Dong, the
root of Qie Dong tree…another friend, she took for her breast cancer.
(I) searched for the root of the tree. I was discharged at that time, (I)
did not drink milk, (I) took that (the soup made of tree roots)…the Deity
pointed out a particular one (tree)…we asked somebody to take us to
find; that (place) is a very remote area. You won’t know it would have
that sort of thing, it is hard to walk on the road. (Ms. Zheng)
Studies which have investigated Chinese populations with cancer (in Taiwan and in
USA) confirm that religion is an important resource during treatment for their
disease (Chiu, 2000, p. 68; Chiu, 2001, pp. 179-180). In addition, it is believed that
these resources help in decision making and offer hope and consolation (Tatsumura
et al., 2003, p. 69). As Holroyd (2002) argues, Chinese religion provides continuity,
linkage, strength and hope and these are ‘acted out’ as health seeking behaviours (p.
742). Similarly, Yates et al.’s (1993) study on an Australian sample of patients with
terminal cancer who were using alternative therapies found that a number of patients
used psychic healers, attended Bible groups or used Reiki (p. 208). However, in
contrast to the present study only very few patients in the above study used such

164
religious practices as a practical health seeking strategy.
Carone et al. (2001) argue that although religious beliefs may have a positive effect,
on occasions strong religious beliefs can persuade people to reject medical treatment
(p. 1000). However, this was not a finding of this study, although some participants
did delay seeking Western medicine treatment. For example, Ms. Zheng and Mr.
Chen looked to religious guidance before seriously taking on Western medical
therapy.
In this study, religion informed participants’ decisions in two key ways. First,
religion was used to influence treatment decisions and second, religion was used as
an alternative therapy in itself. In the latter case, some participants adopted religion
as an adjunct to Western medicine, while others viewed religious practice as separate
from Western medicine.
However, some participants did not believe in the effects of religion and therefore
there was little change in their religious actions after they were diagnosed. Mr. Yang
further elaborated:

165
(We do not necessarily) need to change (our) belief after getting sick.
(Do we) need to change the belief?...I only take incenses to pray for
the ancestor…Christians go to the church, Buddhists read the
scripture. I do not do any of (these). (I) do not see these
enthusiastically...
From the discussion of traditional Chinese philosophy and religious practices, the
various healing beliefs and practices in Chinese society are well demonstrated. There
are, however, other less obvious but important dimensions of belief systems that
shape the meanings of illness.
Chinese Proverbs and Self Destiny
People’s beliefs and attitudes construct intentions to act or not act in particular ways
and such intentions influence people’s health behaviours (Abraham & Sheeran, 2000,
p. 8). Furthermore, people construct their worlds through their interactions with each
other and within particular contexts. As we have seen, the health beliefs of Chinese
people are drawn from culture and are grounded in the social context in which
people with chronic illnesses live. Therefore, the influence of such beliefs is

166
inevitable (Hwu et al., 2001, p. 638). Along with philosophical beliefs and religious
practices, the study has identified the importance of the dimensions of a belief in fate,
the “will” of people with cancer and an ethos of “doing anything” where the
participants will engage with any form of therapy available.
Belief in Fate
A sense of fate is important to the beliefs of people in Taiwanese society. Some hold
an attitude towards cancer that it is a matter of fate. As Ms. Zhu stated “It is not the
same condition for every patient. Everyone has his/her fate, it’s different.” Further,
Mr. Lu said “I took (medicine) here, it gets better, I simply just take this. If things go
wrong, you can’t do anything about it.” In addition, Ms. Zhang made the following
comments about this issue:
I also feel strange. I do not eat so (outrageous). I am also careful
about my diet. How come I get this (disease)? (I) am also careful
about my diet sometimes. If things go wrong, you can’t do anything
about it.

167
There are similar findings from the Fee et al. (1999) research which investigated the
health and social needs of older people in England. This study found that a belief in
the will of God, fate or a matter of chance meant that it was impossible to prevent ill
health (p. 49). Chao (1995) argues that the concept of knowing fate means an
individual is aware of his/her destiny and will strive towards his/her ordained destiny.
But knowing fate also means a person knows the limitations of one’s own force; the
universe has the power behind one’s control (p. 149).
Some western studies define fatalism as “belief that some health issues are beyond
human control” or “one’s actions cannot influence outcome, or cancer was a
punishment for wrongdoings” (Conrad, et al., 1996, p. 941; Straughan & Seow, 1998,
p. 85). While participants in the above studies were not cancer patients, their
statements about fatalism reflect those found in this study. Importantly, beliefs such
as cancer fatalism may influence decision making and responses of people diagnosed
with cancer (Powe & Finnie, 2003, p. 461).
For example, some cancer patients in this study expressed the fatalistic belief that
they would simply coexist with their cancer. Ms. Han sought the advice of a Chinese
medicine doctor who explained the importance of NWM in sustaining a balance to

168
the body:
He (the Chinese medicine doctor) said (it is needed to) coexist with
cancer cells. Then, keep the balance. You don’t disturb it; it doesn’t
disturb you. Then (you) have to take it each day as it comes…
Ms. Han also referred to a “coexistence with cancer”. She indicated “the children
would be a trigger. (I) would be aggressive, continue want to live and see if (I) could
prolong (my) life”. Such beliefs arguably reflect a fatalistic view that cancer is
something to be accepted and that one needs to live with the disease.
In addition, Ms. Chu referred to the importance of “coexisting with cancer” when she
used NWM. She reflected these beliefs in the following account:
I hope it can help by taking it (Chinese medicine). People always think
that, as long as (cancer) can be controlled, as long as (they) can coexist
with each other, (I) do not hope to destroy it or it destroy me. We like
each other. I hope it (cancer) likes me. I like it (cancer). We can become
one (and I) don’t want it to attack. Let me keep healthy like a tree sitting
there and seeing children grow up.
Other people with cancer described the use of NWM as being consistent with the

169
philosophy of “taking each day as it comes”(一天過一天), as there is no certainty
about the future. For example, Mr. Yang stated that “(I) do not think of those (curing
the disease). (I) think (you) have to take it each day as it comes…”. This account
similarly reflects a type of fatalistic view that while one can act to treat a disease, one
also has to accept the responses whatever they may be.
The “Will” of People with Cancer
In this study and although some participants regarded the diagnosis of their disease
or the progression of the disease as being due to fate, at the same time, most
continued to actively seek treatment for their disease. Furthermore, although some
participants expressed a belief in fate, volition or so called “will” was seen by some
as being more important. The “will” of the individual thus emerged as an important
factor in the response of many participants to cancer in this study. For example, some
described the “self” as a key point in how one responds to a cancer diagnosis and its
treatment: “Myself is very important…myself is very important. Yes, the thoughts of
yourself are very important.” (Ms. Qin). Further, Mr. Chen also stated:
Keep in a good mood. Somebody said (they) couldn’t tell that I have

170
cancer. Do not worry that something is a nuisance…cooperate with the
doctor as much as you can. Keep in a good mood. Don’t think that I
have cancer; (I) mainly keep in a good mood. Do not worry that
something is a nuisance…(this is) better for yourself…
Mr. Li refers directly to the importance of personal will:
Like the treatment, of course (I) handed over to the doctor, but (I) relied
on my own will. (I) didn’t say that (I) got cancer, I am finished. Yes, you
needed to cooperate with exercise, exercise not only Guo Lin Xin Chi
Gong but also others. As long as you did exercise, the body would get
healthy. (If you are) healthy then (you will) enhance immunity. Yes, (it is)
true. It made sense. So regarding treating cancer, in the perspective of
treating cancer, (your) own will is very important…that is to say (I)
would fight with cancer. So you see Guo Lin Xin Chi Gong, it could, if
you practiced well, it could fight with cancer, just like competition, I
wanted to win over you...
A participant’s belief may be based on some sense of hope in the future such as the
belief that cancer can be cured (Wright, Watson & Bell, 1996, p. 22). The concept of
“positive mental attitude” in promoting good health has been explored by Fee et al.
(1999, p. 58). Similarly, Hwu et al.’s (2001) study reported that people with chronic
illness hold the attitude that positive thinking and an optimistic and moderate attitude
171
can bring internal strength to the body (p. 638). For some participants in this study,
such positive thinking was an important feature of their approach to cancer.
I think the important thing is not what you take, but you need to be
optimistic. You definitely think this disease can be cured, somebody
was cured before. You will be the person who is cured. You should have
confidence in yourself…I think (you should) build yourself in the mind.
Somebody can be cured, so can I. (Ms. Zheng)
Furthermore, Ms. Xu made the following comments:
Attitude is very important…it is better to live well yourself…don’t
worry all the time; the more you worry, the worse it is. I don’t worry at
all. I live as usual and nothing changes. I won’t ask my family to treat
me better. (I) live as usual.
Mr. He also reflected upon this issue:
Taking it easy on myself after (I got) sick. Taking it easy, taking it easy.
(I) don’t think too much…Taking it easy is most important. The body is
most important.

172
Alexander (1990) argues that self is consciously essential because consciousness is
able to achieve the self’s interest when some impediment to well being is confronted
(p. 291). In addition, “will to live” has been described as a predominant attitude held
when people face a disease such as cancer (Yates et al., 1993, p. 205). The
impediment to overcome, in the context of this study, is “diagnosed with cancer”.
The findings of this study thus reflect, at times, the contradictory nature of people’s
beliefs. On the one hand, people with cancer hold the belief that everyone has his/her
limitations and fate is beyond one’s control. On the other hand, some believe that
“will” holds the key when encountering cancer. Indeed, studies suggest people with
cancer often convey the dilemma of experiencing feelings of fear while at the same
time being strongly encouraged to “stay positive” by family and friends (Cordova et
al., 2003, p. 465). The two concepts (a belief in fate and the importance of individual
will), may appear to be contradictory (helplessness and positivism) and yet the
concepts appear to coexist for many during the cancer journey.
For example, Mr. Li enthusiastically practises Guo Lin Xin Chi Gong as an approach
of NWM when he faces cancer. Nevertheless, he also noted later on in the interview:
“It’s a pity, I am finished. My third lobe in right side lung seems to have water in it.

173
Even the doctor said it is fibrosed…”. In addition, while Mr. Yang decided to consult
a Chinese medicine doctor about his illness, he also stated later that: “This disease is
agonising, (I) resign myself to my fate.”
The above examples illustrate a philosophy that Jiang (1997) argues is characteristic
of Chinese philosophy. That is, a positive perspective on the philosophy of life
means that Chinese people fight diseases and natural disasters; they may blame God
or man, but they still submit to the will of Heaven (pp. 44-45). Arguably, the fact that
all participants in this study actively sought to do something about their disease (in
agreeing to enter hospital and in using NWM), illustrates that these two beliefs can
coexist and affect people’s responses to cancer.
The Ethos of “Doing Anything”
This study has found that people with cancer may be guided by traditional Chinese
philosophy, religious practice or other beliefs, such as fatalism. For some people, a
belief in the need to do anything they might when facing cancer was also described.
According to Quah (2003), an “ethos of pragmatic healing” is that which

174
“eschews conceptual analysis and the measurement of errors and biases,
ignores the paradigmatic divide with biomedicine, and focuses on using
whatever works” (p. 2009).
People in Taiwan do not clearly divide the health care system into two: science and
non science. They may make multiple choices and for multiple reasons (Xu, 1992, p.
118). “Using whatever works” may explain why a person with cancer decides to use
NWM during their cancer treatment journey.
In traditional Chinese medicine, the ethos of pragmatic healing is based on
modification of therapy through clinical practice. This contrasts with the ethos of
science where treatment is based on predetermined evidence. Traditional Chinese
medicine may be considered to offer this sense of pragmatic healing that exists as an
icon in Chinese culture (Quah, 2003, p. 1997). This ethos is reflected in the actions
of participants in this study, such as Ms. Chu. Traditional Chinese Medicine focuses
on what is wrong with the whole body rather than parts of the body and on disease as
caused by a disturbance of Yin and Yang inside the body. The purpose of traditional
medicine is, then, to restore these two components (Spencer, 1999, p. 6).
Because after all we are Chinese, (we) still believe in Chinese medicine.

175
Then in passing (I) went to see him (Chinese medicine doctor). (I) may
get help in Chinese medicine contingently…Chinese medicine may have
a little bit help, help me to recover physical strength, help me to have
more resistance (to disease), help me… (Ms. Chu)
Chinese traditions and beliefs inform the ways in which people view NWM and
provide insight into why they use NWM. However, a diagnosis of cancer is generally
a traumatic life occurrence and people typically experience a range of emotions and
fears. These initial reactions to this serious diagnosis help to explain how NWM can
be seen by some as a legitimate option in one’s attempt to respond to the threat
presented by the diagnosis.
病急亂投醫 (You go anywhere and do whatever if it is a serious
disease) the first time. That is my feelings. (It was) so painful at that
time…(Mr. Jiang)
Similarly, people with cancer may also start to use NWM because the progression of
the disease is unexpected. When people experience such unexpected circumstances,
they may seek a range of treatment options. For example, as Ms. Shen experienced
different phases in her illness, so her decision making and actions changed. In her
own words:

176
I thought of myself as carcinoma in situ. I thought of doing the
operation then chemotherapy just in case. It supposed no problem then.
Later on, it was metastases to ovary; I thought that things are not so
simple. (It) might be metastases again. Because of panic in mind, I tried
something different. (It) might slow down or avoid it (metastases)
happening again…I have used Brazil mushroom (巴西蘑菇), extracted
Ginseng (人蔘皂苷), five elements vegetable soup (五行蔬菜湯) and
XXX (brand name) nutritional supplements (XXX 的營養品).
One study, which investigated CAM use among colorectal cancer patients in Canada,
found that the most important reason why people with cancer use CAM as an option
is a desire to try everything available (77%) (Tough et al., 2002, p. 58). “A desire to
try everything available” and “go anywhere if it is serious disease” is characteristic
of the actions of some people with cancer in Taiwan in deciding their cancer
treatment.
Ms. Xu referred to her emotional responses which reflected both fear and uncertainty
in response to cancer:
I copied down his (a stranger who approached Ms. Xu and talked about

177
NWM) telephone number. Then, I asked my husband if it is true, my
husband said we may try to call. My husband was more alert, he was
more doubtful. We sick people 病急就會亂投醫 (would go anywhere and
do whatever if it is serious disease). (We) would do anything. My husband
stopped me later on; he said it may be a fraud. (We) were nearly cheated.
Ms. Zhu also indicated “只有生病的人才會急病亂投醫 (Only sick people would
go anywhere and do whatever if it is serious disease)”. These participants have a
desire to do anything to fight the disease. This is consistent with Algier et al.’s study
(2005) which investigated the use of complementary and alternative
(non-conventional) medicine in cancer patients in Turkey. In this study, 36% of
participants used CAM. Of those participants, 18.9% indicated that they were “doing
everything possible to fight the disease” (pp. 142-143).
The study which investigated the use of complementary and alternative
(non-conventional) medicine in cancer patients in Turkey, also found some people
reflected a belief that “it may be helpful, at least it is not harmful” (Algier et al.,
2005, p. 143, p. 145). Furthermore, Scott et al.’s (2005) UK survey on the use of
complementary and alternative medicine in patients with cancer also reported that the

178
participants (24%) held the view “might help, can’t hurt” (p. 135). Similar findings
were revealed in this study.
Behaviours are enlightened by past actions, present situations and a will to find
solutions to the problem (Mead in Millers and Hintz, 1997, p. 89). The fear
associated with a cancer diagnosis gives rise to beliefs that it is better to do anything
than nothing. People are willing to actively seek a range of treatment options to be
participants in the process of healing (O’Callaghan & Jordan, 2003, p. 31). As Mr.
Chen stated when asked why he tried various NWM treatments:
死馬當活馬醫 (It is better to try anything than try nothing), it is so
effective for other people. This medicine is not so expensive, so I tried. (I)
won’t die anyway.
The sources of this strong desire to seek a range of treatment options are numerous.
They include a strong desire to avoid death. Also, family caring responsibilities
provided the impetus for some people to pursue every avenue of therapy. This was
the case for Ms. Chu who explained that her concern for her children was a strong
source of will to respond to her cancer. She stated:

179
(I) do not know the effect. It can be said as 死馬當活馬醫 (it is better to
try anything than try nothing)…(I) hope I can get well sooner, because my
youngest child is only eight years old. I can’t leave them (children) all
alone, so will is important, too.
You go anywhere and do whatever if it is a serious disease (病急亂投醫) and it is
better to try anything than try nothing (死馬當活馬醫). When people face health
problems that do not go away, they may pursue remedies or therapies from different
cultures or healing systems in an attempt to resolve their particular health concerns.
The Scott et al. (2005) study, noted above, revealed that people with cancer (41%)
want to do everything they can to fight the disease (pp. 134-135). Thus an “ethos of
pragmatic healing” exists where he/she is not concerned with measurement of
outcomes or evidence of biomedicine and only focuses on whatever is working or
available (Quah, 2003, pp. 2008-2009).
This concept of pragmatic healing continually emerged in the data of this study
where participants sought multiple forms of therapy. For example, Ms. Chu used the
phrase “多管齊下 (employing multiple methods to achieve one goal)”. Chiu’s study
(2001), which explored the spiritual resources of Chinese immigrants with breast

180
cancer in the USA, reported that alternative therapies were used as they were
believed to achieve better results (p. 180). In addition, Du’s study (1992) of the
cultural influences on the medical behaviour of the female breast cancer patients
found women with cancer employed multiple methods of cancer therapy during their
hospitalisation. Ritual ceremonies and diet therapies were mostly used (p. 127).
Employing multiple methods to achieve one goal (多管齊下) may be one of the
many ways people respond to a cancer diagnosis.
For others, NWM represents “a ray of hope” (一線希望) when other treatments
appear to be adverse in effect. Using Chinese medicine as an example, Ms. Qin made
the following comments about this issue:
I do not have particular thoughts…somebody told me that many people
went there, so I went (the Chinese medicine clinic). The situation is that
(you) hold a ray of hope. Because after you had chemotherapy, the body
became worse. I saw many people did not finish (chemotherapy) and die.
The bodies of some people became very bad. (Chemotherapy) kills cancer
cells; it also kills body cells, too.
Also, some participants just simply want to optimise their chances. For example, Ms.
Shen stated:

181
(I) want to give myself more chances. Because when they (NWM
product promoters) talked about these, counted as alternative medicine,
they also offered a lot of eyewitnesses, (I) felt since they had those
eyewitnesses, it might be not without any sense. (I) felt that (they,
healthy products) also worth a try.
Some participants saw NWM as the last weapon in the struggle with cancer. As Ms.
Zheng stated in the following account:
Many people, many patients, no matter if they have cancer or whatever,
would search for folk remedies when they encountered these sort of
things. In fact, my father had many folk remedies, but my father said that
he still insisted on trying the doctor first. If the doctor didn’t work, (we)
would start to use folk remedies.
Some western authors have suggested people with cancer may adopt different
treatment approaches, because they seem to provide more self-control and hope. For
example, where there is a belief in individual control over one’s health, NWM may
be chosen because it enhances a person’s sense of control (Ade & Yarbro, 2000, p.
618; Astin, 1998, p. 1548). Moreover, some patients may want to participate more

182
actively in their own healing process (Adamson, 2003, p. 112), while others may
perceive that they have nothing to lose by using NWM (Boon et al., 1999, p. 647). It
has also been suggested that while some people use NWM in conjunction with
conventional medicine, in other cases, patients believe NWM provides a new
opportunity to confront their disease when orthodox medicine has failed (Clavarino
& Yates, 1995, p. 267).
Yet, people do not always use NWM because they are desperate. Most also believe
that NWM is able to prevent cancer spread and alleviate symptoms (Tough et al.,
2002, p. 58). Although participants spoke of “doing anything” or “using whatever
works” in their cancer treatment journey, this does not mean literally doing anything.
In this study, many of the participants mentioned that other people propagated
information regarding forms of NWM through word of mouth. Another group of
participants noted that they actively pursued information on NWM and made
decisions about the therapies that they were prepared to engage with. Ms. Han is a
good example of one who was not prepared to try anything.
Of course many people introduce Chinese medicine and herb medicine
during the process. My important organs are not affected, so regarding

183
those herbs, nobody yet used in the clinical, through word of mouth,
most of them I won’t try. Yes. I am afraid to increase the burden of my
body, so I am not trying anything that others introduce. I will give a
thought.
Therefore, people with cancer do make decisions about NWM within the parameters
of a long tradition of its use and these decisions are further mediated by such factors
as the stage of the disease, family traditions and social and community influences.
In conclusion, the concepts of “doing anything” and “trying different actions” as
noted above, are influenced by interaction with various social contexts and
experiences, such as traditional Chinese philosophy and religious practices.
Summary
The dimensions of philosophical beliefs addressed in this chapter provide insight into
the context within which the participants form meanings about cancer treatment and
more so into the social process whereby the participants act on these meanings.

184
Thus people with cancer engage with Chinese philosophy, religious practices and old
sayings and beliefs in negotiating actions towards cancer treatment. The dimensions
also expand to the context of other social relationships of the decision making
process including family, community and health care professionals. These themes
will be further discussed in Chapter 7.
185
CHAPTER 7
Social Relationships
We have addressed the process whereby philosophical beliefs mediate decisions to
use or not use NWM among people with cancer in Taiwan. Philosophical beliefs,
furthermore, appear as a connecting point for other social relationships that further
influence people with cancer in Taiwan as they interact with NWM.
Social action, as Blumer (1969) has argued, consists of “individual and collective
activities of people who are engaged in social interaction” (p. 54). Activities are
formed by observing the activities of others within groups that may be as small as a
family or community, or as large as a nation (Blumer, 1969, p. 54). And so human
activities happen in situations and are related to communication; communication is
intrinsic (Maines, 2003, p. 6). The communication of experiences is a pivotal
element in the formation of people’s concepts (Blumer, 1969, p. 159).
The focus of this chapter is on communication, social relationships and associated
social interactions as they are shaped by family connections, community connections

186
and professional relationships and practices. This provides a context for broadening
our understanding of the ways in which the person with cancer adopts various
treatments during the cancer journey.
Family Connections
Family can be seen as integral to the original units of all societies. As Bubolz (2001)
argues, the functions of a family act as “the glue” that assists other segments of a
social-economic system to operate simultaneously (p. 129). Furthermore, the
functions and formations of a family are influenced by social, cultural, economic and
political systems in particular cultural and geographic contexts (Kuroda, 1994, p. 54).
The belief systems that emerge within such contexts develop our identities within our
families, community, and professions (Wright, Watson & Bell, 1996, pp. 19-20).
The definition of the family is vague and may contain a lot of meanings depending
on the study context (Allan & Crow, 2001, p. 2). Becker and Charles (2006), for
example, define family as family of origin, including parents, siblings and a range of
relatives. But these authors found in their study of the meanings people attribute to
family that some referred to friends as “like family” which inferred a particular

187
quality of relationship (p. 107). However, the understanding of family, according to
the participants and in the context of this study, is one of a domestic group with
common ancestry and in-laws.
As argued previously, philosophical beliefs emerge in this study as the focal point of
Chinese social systems and one of the most dominant belief systems, Confucianism,
is the guiding framework for family traditions. Confucianism gives primacy to
responsibility for others over and above individual rights and therefore human
relations over individualism (Degui, 2005, p. 129). Huang’s model of “face and
favour in Chinese society”, which explains human relationships based on relationship
closeness, demonstrates that the first level of influence in Chinese society is often the
relationships between family members or other congenial groups (Huang, 2000, pp.
224-225). This is reflected in Lu’s study (2002) which found that a sense of
obligation to significant others is considered essential to well-being in Chinese
communities (p. 179).
Social interaction is therefore embedded in what Lu (2002) refers to as “the
supremacy of collective (social) welfare over individual desires” (p. 187). This in
turn positions the family as the foundation of the society (Hsieh, 1967, p. 175) and as

188
central to life (Lu, 2002, p. 182). Thus Confucian values translate into reciprocity,
mutual respect and thoughtfulness between family members and thus an
interdependency in terms of responsibilities and obligations to other family members
(Bowman & Singer, 2001, p. 461; Bubolz, 2001, p. 131). In addition, Confucianism
underpins the family structures of Chinese people (Jensen, 1997, p. 14) and we
understand that social relationships include social support and family functioning.
The family usually provides the primary and most important of our social
relationships for most people (Franks et al., 1992, pp. 779-780). The dynamic of such
relations includes engagement with earlier experiences and this demonstrates the
importance of the past. Parents or their ancestors are seen as a shelter for the
individual (Isay, 2005, p. 443).
Family connections and belief systems have a strong influence on individuals. For
example, one study on understanding Canadian South Asian women’s experience of
breast cancer reported that most women indicated that they obtained much family
support and that family was also involved in decision making (Gurm et al., 2006, p.
7).

189
When making a decision on disease treatment or the use of NWM and in contrast to
the dominant individualism of Western cultures, family opinions often have
precedence in other modern and traditional cultures. Many Korean or Japanese
families, for example, when informed of a relative’s diagnosis, will make decisions
about treatment (Kemp, 2005, p. 47). In this study, the family, although not
appearing as the decision maker, plays a paramount role in the process of decision
making over the use of NWM. The experience and actions of a family interact with
decisions to engage or to not engage with certain practices such as the use of NWM.
As Mr. Sun explained:
My father brought it (healthy product) (to me). My father bought it
regularly. My father takes it (and), he feels good. He introduced (it) to me.
He brought it to me; how much; I gave him the money…
Ms. Zhang’s husband sought to persuade Ms. Zhang to use Chinese medicine
because of his past positive experience. He stated:
He (the doctor) said to inject interferon first, (and he said the patient) will
be in agony after the injection. If there will be agony, (better) to take
Chinese medicine at home to live at home. It is better to live at home
taking Chinese medicine rather than staying in the hospital suffering.

190
Then, (we) went home. Ms. Zhang continued on to say: (My) brother said
we don’t have to stay there (the hospital) and be in agony.
Furthermore and in reflecting a sense of obligation, participants make compromises
with others over decisions on NWM. For example, Mr. Jiang stated:
(I was) forced by my mum continuously, (I was) forced to take this
(healthy product). She forced (me) after I was sick. She surrounded you.
You don’t have other ways to go…
The above quote reflects the emphasis Chinese society places on the family system
and especially on the relationship between parents and children (Hsieh, 1967, p.
175). It is expected that since parents have invested so much to raise their children,
those children will show their appreciation through respect for their parents
(Liu-Wang, 1959, p. 85). This is evident in Taiwanese research that demonstrates the
importance of filial piety (Lin et al., 1996, p. 41).
The tenet of filial piety, one of Confucianism’s central thoughts, is an essential
component of Chinese society and the whole Chinese cultural tradition (Hwang,
1999, p. 163; Cheung et al., 2006, p. 618). The Confucian idea of filial piety or xiao
is based on the fact that one exists solely because of one’s parents. There is a

191
requisite obligation expected of children to respect, support and be loyal to parents
(Hwang, 1999, p. 169).
We see therefore the importance of the interactive context of families. Illness is
experienced within interpersonal contexts that create people’s beliefs and behaviours
(Wright, Watson & Bell, 1996, p. 23). Although this is a universal phenomenon,
in the Chinese social world, as noted, collectivism presides over individualism.
Therefore, it is understandable that the processes of illness in a family, experiences
of NWM and the use of NWM and their interactions with each other will shape the
experiences of people with cancer. Ms. Qian made the following comments:
My husband died in (Min Guo) 85 (1996); (he) died of esophageal
cancer…(the)doctor said (we) need to do the operation. His brothers and
sisters stopped me and said don’t operate, don’t operate. Then it was
delayed (pause) for three months (and) my husband took Chinese
medicine for three months. It took six months in total, half a year, from
the diagnosis to the time he died… His sisters hurried to get him to take
Chinese medicine and said (to him) somebody also had hepatoma and
was cured by taking Chinese medicine. (His sister) also took him to take
Chinese medicine for half a year but it got more serious. Later on I found
(I had) leukaemia the next year. Many people said to me to take Chinese
192
medicine, take Chinese medicine (but) because of my husband’s
experiences, I was afraid.
Mr. Wei and his aunt, both of whom had been diagnosed with cancer, shared their
NWM information. As Mr Wei stated:
My aunt, she was a patient here, too. She had lung cancer. She had
been diagnosed for more than six months. She finished her
treatment…she always took that (four herbs). She didn’t know Niu
Zhang Gu (one kind of mushroom, 牛樟菇) before. She started to take
(them) when I started. She started to take Niu Zhang Gu, so she
recovered very quickly.
Here we see that a combination of interaction and reflection determines action. A
person’s insights may be influenced by external factors and his/her actions may be
affected by other people’s behaviours (Moldoveanu & Stevenson, 2001, p. 305). In
this case, it is the participant’s own family.
If a family holds strongly to beliefs surrounding NWM and those beliefs are
compatible with a dominant tradition, the family will support a member’s use of
NWM. Views on Western medicine and NWM are influenced and gain legitimacy

193
from different structures within a community. When a profession is legitimised by
society and the practice is congruent with the dominant values in the society, a
profession enjoys a high degree of authenticity (Lee, 1981, p. 269), such as Chinese
medicine.
Mr Chen and his mother talked about their faith in Chinese medicine:
Mr Chen: My grandfather, he was a Chinese medicine doctor… he has
passed away already. When (we) had some difficult symptoms, (we) went
back to ask him. He gave us Chinese medicine. It is useful….
Mr. Chen’s mother: After I deliver the baby, I can’t even sit for a meal, (I)
want to lie down quickly, (I) can’t stand the sore (on the back). (I) called
to ask my father-in-law. He said it was simple, only a few (Chinese)
medicines. I took two prescriptions with pig tail bones. I got well.
The Confucian principle of obligation extends to all aspects of family relationships.
Because, as Hwang (1999) points out, family members “are conceived of as a whole
body”, they are compelled to share their resources with each other including
“wisdom” (p. 170). For example, Ms. Xu’s brother-in-law shared NWM information
with her. Her comments are as follows:

194
My brother-in-law suggested to me to practice Fa Lun Gong later on…he
sells noodles. The Fa Lun Gong people chatted with him. My
brother-in-law’s attitude was not very good. He thought the people who
were seriously ill, practiced Fa Lun Gong…He knew I got this disease
after a few days…He (brother-in-law) asked me if I wanted to practice
then; I started to practice Fa Lun Gong…I used to eat white sweet
potatoes’ leaves…my father-in-law read 善書 (Shan Shu, morality books
published by temples), there is an interview inside; that person was cured,
actually cured…
Similarly, Mr. Wei also shares the family views on the use of NWM. This is evident
in the following comments:
It is quite normal that (my) family members take Chinese medicine.
Families originally accept Chinese medicine so we won’t repel Chinese
medicine in our family. I think Western medicine is for emergency. It is
necessary to deal with Western medicine in serious conditions…regarding
nourishing the body or some small diseases, my family use more Chinese
medicine.

195
Furthermore, as another participant commented:
They all said that healthy products won’t harm the body. If (they are)
taken continuously, it will show better results on the body. Because
friends were talking and my father also encouraged me, I decided to take
(healthy products). I feel the result is not bad after taken. (Mr. Sun)
If people have a regular source of care such as Chinese medicine and have families
who favour Chinese medicine, they are more likely to seek this sort of therapy (Chi
et al., 1997, pp. 47, 49).
It follows from the above that where a close family member is diagnosed with cancer,
relatives will seek to provide tangible help, such as NWM, to show their support.
My aunt bought two small tins (of milk products) and then another big
tin…my daughter said we almost can open a shop…somebody bought for
us, (they) brought to us to eat…we did not buy it ourselves, all somebody
gave to us…it is true that those (things) are expensive, but somebody
bought for us, we did not buy it ourselves…they (the relative) would buy a
lot of things such as concentrate chicken soup, good friends and relatives
bought all for us…those milk products take years to take…many milk
products, everyone bought a big tin, some two (tins)…I said to them don’t

196
buy any more…(Mr. You)
But in these circumstances, the reactions of cancer patients may vary. For example, if
NWM is regarded as a nutritional supplement, it may be accepted. As Ms. Wang
stated:
My body was weaker at that time; (my) children bought them (healthy
products). They knew better what to take. They bought for me…the
children help me…(I took) a blood test, white blood cells were very low. It
can’t keep so low like that. My children said “can’t stay like that”… The
children said later on “you do not have radiotherapy now; eat as much
as you can”. I ate as much as I could. (I) ate whatever I could, (I) ate
whatever I could…(my) children said “you can’t be without eating”…
children bought all of them (healthy products); children bought all of
these.
One of the Confucian filial obligations in families is to take respectful care of one’s
aged parents and this view holds enormous sway in shaping Chinese perceptions of
morality (Wang, 1999, pp. 243-244). Therefore, most elderly are taken care of by
their family in traditional Chinese society. The affections of Confucian filial piety
suggest that children provide not only respect but subsistence (Sun & Liu, 1994, p.
320). In addition, children have an obligation to help their parents or other family

197
members to sustain good health and general well being (Bowman & Singer, 2001, p.
461).
Mr. Lu was also encouraged by his family to take nutritional supplements:
My daughter works in ╳╳ company; my wife, too. Someone works there;
(we) buy from them. If (it is) a birthday sale, it can be up to 50% or 20%
discount…my wife and daughter keep asking me to take these (healthy
products)…they encourage me to take these…I felt uncomfortable at that
time, (she, patient’s wife) took back for me to take…yes, she already took
(healthy products), my daughter took first.
The findings of this study suggest that where people with cancer are making
decisions about the use of NWM, the family is a significant influence. Lim et al.’s
(2005) Singaporean study on complementary and alternative medicine similarly
found that family tradition is important regarding the use of NWM (p. 20). In
contrast, the importance of family in decision making regarding NWM use by people
in Western countries appears to assume a lesser role. As studies have found, in
western cultures the influence of friends and acquaintances may be more significant
than blood relations (Low, 1999, p. 108; Wellman, 1995, p. 225).

198
Community Connections
As mentioned in the foregoing section, the first layer for an individual’s social
interaction with others is often family. Yet, people also live in a community. How
community interaction shapes behaviours, such as in using or not using NWM,
emerged from the interviews. Holroyd (2002) suggests that “divisions between the
individual and society commonly distort how health-seeking behaviours are enacted
in a given culture” (p. 735). This simply means that we can not interpret the
individual without understanding society and in this case, community. These social
concepts are interrelated.
As with the family, a conceptual difficulty is ascertaining how far a community
extends or what exactly constitutes a community. A community can be defined as
people who live in a common area, share similar values, do various activities
together and have high level of cohesion (Phillips, 1993, p. 14). In the context of this
study, community is a social group of people who share life experience together,
such as, friends, neighbourhood and other cancer patients.

199
This sharing, as Blumer reminds us, is a process of ‘joint action’ where people take
account of the actions of others and then relinquish an intention, postpone an action
or have behaviour endorsed (Blumer, 1969, p. 8).
People gain information from observing directly to communicating symbolically.
People think through obtained information, either consciously or unconsciously, and
judge if it is useful (Flinn, 1997, p. 35). For example, some participants in this study
who were given herbal medicine by their friends described more cautious responses.
Although acceptance of the herbs was important, there was some ambivalence and
uncertainty about the use of this form of therapy in conjunction with Western
medicine. As Ms. Wu commented:
Somebody told me to take herbs. They gave (them) to me; I did not take. I
did not dare take them. Somebody gave me (and) I said “thank you”, (I
will) wait after finishing chemotherapy then (I) will decide if I take or not.
(I am) afraid of medicine. (I) don’t know if it is good or not if (I) mix
Western medicine and Chinese medicine together…they knew my
situation and gave it to me. Friends knew what I had. (She) heard of such
medicine, many people got cured after taking (this medicine). She
encouraged me to take it. I received it, but (I) did not take it. Friend is
kindness, I received it anyway, but I did not dare to take it. If we believed
in Chinese medicine, I would take it. But we believed in Western medicine

200
now, then we believed in the Western medicine doctor. If (I) mix (them),
will it be wrong? You don’t know which medicine makes you get better.
Mr. Chen expressed similar feelings:
That (Zhang Zhi Gu, one kind of mushroom) is for cancer. No, it is better
for hepatoma. I also have it in my house; I did not take it. Friends gave it
to me, it is also very expensive…(I) do not know if it is effective. I am
afraid if I take it, (I) do not know the result after taking (it).
Blumer also reminds us that meanings are not imposed upon situations but given to
those situations by those involved (Blumer, 1969, p. 134). For example, networking
by women and especially those within similar groups, is a significant means of
transmitting folk healing beliefs and knowledge (Sharp, 1986, p. 243). Ms. Zhang
made the following comments about this issue:
I was (a volunteer) in the temple, at the very beginning. Those women
friend, (one of those women), she took (Chinese medicine) and got cured
for over twenty years, twenty years. She brought it for me…two of my
friends, two friends took (Chinese medicine) and were cured. She heard
of my situation. She came again and again to my house to ask me to take
(Chinese medicine)…my thoughts, she already took more than twenty

201
years. She has a determination to take more than 300 prescriptions, I
would also have that patience. I have that kind of determination. God
knows I can’t walk after taking (the herbal remedy). (Cancer cells) went
to the brain. She was fine after. (But) she couldn’t do anything hard, but
she could take care of grandchildren and cook three meals. That’s great.
Social networks focus on collective processes for example, sharing of community
values and maintaining social control (VoyDanoff, 2001, p. 142). Where NWM has
been observed to work well for others, this may induce people with cancer to try the
same (Tough et al., 2002, p. 58). Mr. Wei was also influenced by the experiences of
friends who had achieved impressive results from using NWM. Mr. Wei used NWM
in conjunction with Western medicine treatment. He stated that:
(I) naturally accepted (NWM), but (I) still did Western medicine
treatment, definitely chemotherapy. I thought cancer cells shrank very
quickly by doing so (taking NWM). When I did the second
chemotherapy, I was told by the consultant the cancer cells had
disappeared, all of them shrank…He (the doctor) said I could drink it
(Niu Zhang Gu, 牛樟菇, one kind of mushroom). I knew some friends;
they did not do chemotherapy when they found (cancer). They did not
do chemotherapy, (they) then went back take those herbs and took Niu
Zhang Gu. After four to five months, (they) went back to the hospital for
examination; cancer cells, the tumour, had disappeared.

202
Mr. Chen described a similar situation:
My father knew some people in Mainland China, (and) they said (pause)
this person had business in Taiwan. (He, the friend of Mr. Chen’s father)
was seen as useless (means terminal) by the ╳╳ hospital and asked his
family to take him home. After he came back (home), he used this
medicine (Hei Teng, one kind of herb), everyday until now. (He) is still
alive. He had many kinds of cancer…many of them and many
complications. He relied on this medicine to convalesce through care
and nourishment. (He) convalesces through care and nourishment until
now; he is still taking (this medicine).
People deal with an ongoing changing environment. The cancer journey is a dynamic
process and within this process beliefs shift and change. Beliefs and actions are
communicated, employed, tested and adjusted by individuals in real circumstances.
Where something is working, there is a reason to continue to use it; if it does not
work, then it may be changed (Charon, 2004, p. 167).
However, others who had observed poor results from the use of NWM were less
likely to use this kind of treatment. As Mr. Shi stated:

203
Some are suited to take (herb medicines), but some are not. One of my
friends…he has acute leukemia; he said he took herb medicine. It costs
NT 600 dollars a day. He took Chinese medicine, he did not take Western
medicine. (He) did not take the doctor’s prescriptions. It takes no more
than half a year, no more than half a year; he died…
Furthermore, in many cases people have learned about the NWM through interacting
with others. Mr. Chen told the researcher that “In fact, the person who told us this
medicine said this medicine is for cancer” and requested that the person’s name not
be mentioned. Mr. Wei also stated: Twenty years ago, some friends got cancer, they
said it is better for recovering by taking 牛樟菇 (Niu Zhang Gu, one kind of
mushroom). This information can be seen as a form of “secret” remedy that is
informally recommended to people with cancer.
Moreover, social reciprocity is impossible without consciousness, planning and
scenario building (Alexander, 1990, p. 288). People with cancer may develop
informal groups to support each other in using NWM during their cancer treatment
journey. This kind of community support provides informal help and allows
exchange for experiences within a network (VoyDanoff, 2001, p. 150). People with
cancer in the community who hold similar beliefs may gather together, talk and

204
encourage each other. For example, Ms. Qin stated:
They (the patients in the clinic) all had chemotherapy. I met several of
them. We got to know each other there. They finished chemotherapy.
During chemotherapy, they took his (the Chinese medicine doctor)
medicine, then, they continued (to take it). They finished chemotherapy
and they continued to take his medicine. (They) are quite well now…I
have seen several (of them). After they finished chemotherapy…(they
have) only regular check ups and keep taking Chinese medicine.
Ms. Xu also referred to her experiences of support groups. She said:
I attended their ritual meeting (Fa Lun Gong). A terminal cancer patient,
the doctor said to him that he only had four months to live…he (the
patient) said only four months to live. The first year I saw him, he said he
lived four days more. Next year, I was wondering was he still there? I
attended again, he was still there, in very good health. I went the end of
last year, he was still there, already three or four years. I knew and saw
him the first year. Now (I) see him again, in very good health. He is a
veteran. He is in very good health, (his) face colour is quite good…they
have ritual meetings every year and exchange what one has learned. How
is your practice? Everybody talks.
Chan’s (2005) study also indicates the power of community traditions. As noted

205
previously, although Western medicine came to dominate in Taiwan following World
War II, the use of traditional Chinese medicine has remained a fundamental part of
Taiwanese life. Chinese medicine products in herb shops are popular because some
tonic herbs, such as, Danggui (Radix Angelica sinesis) and Renshen (Radix Panax
ginseng) are commonly used in many Taiwanese families (Chan, 2005, p. 3).
As noted above, community traditions and beliefs spread, when needed, gradually
like a stone put into a pond and this is evident in ways that the participants perceive
their interactions with other people with cancer. Mr. Li stated:
All cancer (patients) were on that floor, when (they were) walking, there
is no vitality. I held an IV stand, another hand did breathing exercise, the
hand was moving. Sometimes some people saw and asked “what is this,
what kind of exercise?” I told them where (they) teach this. Then, after a
period of time, you practice by yourself…I went to meet almost twenty
(people). We chatted with each other, they were same with Guo Lin Xin
Chi Gong. Whichever disease you have, (you) face west or (you) face east.
They had certain rules. Like me, nasal pharyngeal cancer (NPC) faced
west…when (I) practice, people would look. I introduced (Guo Lin Xin
Chi Gong) to somebody. Sometimes, other patients in the same floor had
that treatment and had cancer cells. When he saw me, (I) seemed not to
have the disease. (He) asked me or my wife. I said I practiced Guo Lin

206
Xin Chi Gong…
Moreover, Mr. Feng shared his experiences of using NWM with other cancer
patients:
If you are sick of food, few people eat that (milk, nutrition supplement) if
(you are) normal. Later on in the basement, I went to do radiotherapy.
One person had retired from government, he has nasal pharyngeal cancer.
He was in the same situation…I introduced him to take that (nutritional
supplement).
Some participants share the positive experiences of others in order to provide support
in the struggle with cancer. As Ms. Chu stated:
I heard something that day. I don’t know what he took…I felt sad that day,
I went to chat with others in the outpatient department. He just saw us
chatting, he would like to share the happiness. (They) then came to talk
with us, “my husband has lung cancer or some kind of cancer, stage III,
he is cured. Then we said to him “congratulations”. He was very happy
then; she took her husband home…
207
Other people’s influences are significant and community support is therefore very
important in the cancer patient’s journey. Mr. Yang noted:
(I) thought of life later on; many people suggested to me “don’t be in so
much depression”. (I) still need to walk out, see people, see (the doctor)
in the hospital or take Chinese medicine…
Furthermore, Ms. Qin also made the following statement with regard to use of
Western medicine or NWM. Community support is very important:
I saw many people…some did chemotherapy. He felt very
uncomfortable. Then, he couldn’t eat anything and was very low
emotionally. (The situation) is not good, so (he) couldn’t eat anything.
Just like no hope. Because for somebody after doing (chemotherapy)
the body gets worse and worse and then in very bad emotion. Oneself is
very important; people around are also important. The importance is
for people surrounding to encourage him/her.
Being able to share the experiences and information and gain support from peers,
especially other cancer patients, is essential. Gurm et al’s. (2006) study shows that
being able to talk with peers provides strength and encouragement. As women said in

208
the study “…with the exchange of ideas; you also feel relieved and know new things.
We can share each others feelings, whatever good or bad” (p. 8).
Community social cohesion is an important source of qualitative support that extends
beyond an individual’s family and friends (Mulvaney-Day et al., 2007, p. 479).
Family, friends and media, including television and the internet may be factors that
construct patients’ treatment decisions (National Breast Cancer Centre, 2003, p. 56).
For example, through word of mouth communication, patients obtain information
from their family and friends about a range of different approaches to managing a
health problem. Such social interactions may directly or indirectly influence patients’
decisions along their cancer treatment journey.
Through an examination of family and community connections, we understand that
human actions are not simple. People encounter incidents everyday and the meanings
of all sorts of things go through an interpretative process. Nevertheless, in Blumer’s
terms, interpretation should not be seen as the automatic imposition of meanings but
a process of meaning being actively used as a guide for action (Blumer, 1969, p. 2, p.
5). The above testimonies of study participants are pertinent to this concept.

209
As has been argued, family and community connections are important bindings in
Chinese society. In accordance with Confucian values, Chinese clan rules combine
with practical experiences and realities; they include parent-children relationships,
relationships between brothers, marriage relationships, clan relationships, friendship
and community relationships (Liu-Wang, 1959, p. 84). All contribute to the social
milieu of family and community connections as found in this study. This social
milieu is a complex and continuous interplay of consensus and change. Individuals
reconfirm or add to that consensus through their actions and interactions which may
both authenticate past experiences and adjust what is known (Charon, 2004, p. 167).
We understand, therefore, that individuals and society can not be separated. These are
simply different stages of a social process. A further social relationship and stage in
the social process under this study is that between the healthcare professional and the
patient.
Professional Relationships and Practices
Relationships between people with cancer and health care professionals emerged as a
key factor in determining treatment regimes as far as Western medicine treatment is
210
concerned. However, this study also determined that people living with cancer may
or may not discuss the use of NWM with their health care professionals. The
participants of this study were all interviewed in Western medicine care settings, had
all been admitted to a Western medicine hospital for treatment and had all used
NWM at some stage in their cancer journey.
Western medicine assumes a leading role in Taiwan’s health care system. Traditional
Chinese Medicine still takes a subsidiary role in Taiwan16 (Chi, 1994, p. 307).
According to the Taiwan Public Health Report (2001), one hundred and twenty seven
teaching hospitals were accredited by the Ministry of Education and the Department
in 2000, twenty eight of which have Chinese medicine departments. In addition,
there are two Chinese medicine public hospitals and eleven others have Chinese
medicine departments (p. 35).
In the context of this study, the health care professionals that participants were
referred to were mainly Western medicine doctors. Some participants clearly
indicated that they would not try non-western therapies without a doctor’s permission.
For example, Ms. Wang had permission from a Western medicine doctor before she
16 This is evident in figures which show that in 2000, the number of physicians in practice was 29,585 compared to 3,733 practicing Chinese medicine doctors (Department of Health Taiwan, 2001, p. 22).
211
went to see a Chinese medicine doctor within the same hospital.
Somebody induced me to take something. I did not dare (to do it)…Yes,
many people (induced me). Somebody said take something to get well,
take something to get well. I just said (I was) treated here (in the
hospital)…that is Chinese medicine here (in this hospital), then I went,
if (it is) somewhere else, I do not dare to go…the tumour doctor, I asked
him. May I go (to see Chinese medicine doctor)? (He said) yes…(we)
need to ask, (the doctor said) yes, then we go. You can’t go to see
(Chinese medicine doctor) without asking. It is not good if the medicine
(you) take that conflict (each other)…
A reason for informing a doctor was the fear that the different forms of therapies
would counteract each other. Other participants did not discuss the use of NWM with
the doctor directly. But rather, they posed more general questions with doctors. For
example, Ms. Zheng stated:
I feel many people are taking healthy products. I asked the doctor “can
I take healthy products?” He said if it is like 亞培 (nutrition product,
brand name) to supply calcium. I said many people said wheat grass
and organic things may help the body. He (the doctor) said it’s fine to
try a little bit, don’t rely on it. I feel so, too. In addition to listening to
the doctor, that is additional. It’s fine to take a little bit, (I) still do (what)

212
the doctor (says) as possible…
The fear of disapproval was a reason for “forgetting” to tell the doctor about the use
of NWM. As Ms. Zhu illustrated here:
No, I prepare to tell him (the doctor) now, (I) wanted to ask him this
morning, (I) forget again…patients will always be afraid that the doctor
(will) stop (us using NWM)…(I) eat by myself quietly. These few days,
my sister and I went down stairs; we just happened to see the doctor.
My sister suggested to me to tell the doctor. I said O.K. You go and ask
him. Every time I want to ask, then I forget. After telling the doctor
some questions, then the doctor was gone, (I) forgot something else. (I)
forgot something else. Usually (I would like to) tell some of my little
problems. I forgot, too.
However, Ms. Qin described her doctor’s reactions when she discussed NWM:
(I) did not mention before in XX (hospital). But recently, several times (I)
had conversations with the doctor and mentioned it (uses of NWM)…he
(the doctor) had no reaction…he (the doctor) just listened and passed.
It appears, therefore, that people may not communicate about use of NWM with their

213
health care professionals because they are afraid of a negative response.
A further reason was that nutritional supplements were not considered “real
medicine” by participants and therefore not the concern of medical doctors. As Mr.
Jiang stated:
It is not necessary to tell the doctor. I directly take (nutrition
supplements). I (took them) when I was resting at home, (I was) not
taking them during chemotherapy period. I took them when I was resting
at home…
Ms. Shen also made the following comments: Because I felt I was only taking
nutrition products, they were not medicines, they were supposed to be fine…Studies
show that people do not think it is necessary to inform health care professionals
about their use of NWM based on the view that it will not influence current treatment
(Robinson & McGrail, 2004, p. 93; Stevenson et al., 2003, p. 521).
Indeed, doctors at times did disapprove and this experience encouraged the
withholding of information on NWM. Mr. Shi made the following comments:
214
He (the doctor) asked me not to take something as I like…Doctor ╳╳
told me if you took herb medicine, I won’t treat you. I quietly took
healthy products, (I) then stopped after half an year.
Furthermore, the sense that if “the doctor did not ask, don’t want to tell” also
emerges from this study when people with cancer were asked about the
communication regarding NWM. Although NWM is accepted by many Taiwanese,
the evidence above suggests patients do not readily discuss their use of NWM with
health care professionals. As such, the use of non Western medicine is often not
known by health care professionals in Taiwan (Xie, 1998, pp. 172-173). Several
studies (Nam et al., 1999; Powell et al., 2002; Rao et al., 1999) have also found that a
lack of inquiry from the health care professionals is one of the main reasons people
do not discuss NWM with health providers. In addition, Lim et al.’s (2005) study on
complementary and alternative medicine (CAM) use in multiracial Singapore
reported that 74% participants did not discuss their use of CAM with their Western
medicine trained doctors (p. 19).
On the other hand, Stevenson et al.’s study (2003) reported that only four out of sixty
two participants receive positive responses from their doctors regarding their self
treatment with NWM. Other participants found that their doctors generally reacted

215
with “right” “yeah” and “mm” (p. 522). In addition, practitioners may not support the
use of NWM and that they may seek to convince them against the utilisation of
NWM (Robinson & McGrail, 2004, p. 93).
The interactions between people with cancer and the health care professionals may
also lead people to try other options, such as NWM. For example, Ms. Zhang stated:
He (the doctor) said (for) your (disease) there is no medicine to treat
(you). I think (it’s) fine. (I) came back to take Chinese medicine, to take
Chinese medicine.
There is a perception that Western medicine causes sickness and that is why some
refuse this treatment. For example, Ms. Xu saw other cancer patients’ situations in
the hospital. She focused on trying NWM and stopped all her Western medicine
treatment. As she stated:
No, I did not come for treatment, I did not come at all…because when (I
went) to the hospital, I saw many people the same as me. Not long later,
they were in wheel chairs. I felt very uncomfortable after I saw
them…so (I) was scared after I saw (them)…Now (I) walk, almost can’t
climb up stairs…climbing to second floor, (I) need to have a rest. (I)
216
can’t climb up…(my) heart was exhausted and short of breath, my
husband kept asking me to come (to the hospital). Then, I came for an
examination.
The following testimony was also reflected by Ms. Zhang:
No, I did not come then…I did not come, did not come to the
appointment…(I) can’t walk when I come (again to the hospital), (I)
have a hope to let him (the doctor) treat. (I would) talk about others
when I could walk…if it is very effective after I took at home, I would tell.
I came here to be treated because of a bad effect after taking (NWM) …If
I felt it was effective after taking, I would introduce others.
Other people with cancer do discuss the use of NWM with their doctors. For some,
this was to obtain an assurance from doctors that they can use NWM and that doctors
approve of what they are using. As Mr. Zhao stated:
I also gave to Dr.╳. He knew the benefits after taking this (nutrition
supplement). This is not cheating, not like direct selling. Let me explain,
if this is a good product, we should share with other friends. It can take
care of our body…during the New Year’s holiday at that time, the
doctor did the surgery on me. After three days, I went home for Chinese
New Year, although Dr.╳ said no. He was very worried about me. When

217
I came again, (he) said “why is your complexion so good?”, I told him
“I am taking this (nutrition supplement).”
Mr. Wei communicated with doctors regarding NWM and the doctor was aware. He
reflected in the following account:
He was hoping that I finished all chemotherapy treatment. It may be
better not to recur later on. I then follow the doctor’s instructions.
When I stayed at home, the doctor knew I was taking 牛樟菇 (Niu
Zhang Gu, one kind of mushroom). I kept taking then…
A doctor’s attitudes towards NWM may be tested by people with cancer. In other
words they seek to determine the doctor’s position on NWM. For example, we see
the tension between scientifically based medicine and other therapies in Mr. Feng’s
communication with a doctor.
(I) wanted to take Chinese medicine at the beginning…╳╳ (doctor), do
you know? He resigned in August. In fact, at the cancer appointment,
he told me “don’t listen to the folk’s secret remedies”. They have no
bases. It makes sense what he said. If (they) are good, take them to the

218
hospital and do experiment, nobody is sick then…he reminded me of
this point when I went to see him.
This tension is also evident in Mr. Chen’s experience:
Doctor ╳ said there was no clinical experiment for that medicine
(extract from ginseng, 人參皂苷). He did not know (the effect) and the
price is high. He asked me not to try. He said I could try Chinese
medicines which were cheaper. Go ahead to take those and take care of
myself. He did not suggest to take that (extract from ginseng, 人參皂
苷).
In referring to the influence of a doctor on a decision to use NWM, Ms. Shen noted:
If the doctor said to me (it) (NWM) could be tried, I then try. If the
doctor said it (NWM) might not help, I might also try, because no help
at least is no hazard. (It) still has the possibility to try.
The above data suggests that if health care professionals support the decisions of
219
cancer patients to use NWM, patients will often try these therapies. However, if
health care professionals do not agree with the use of such therapies, patients may
still be willing to try NWM and will be encouraged to make such decisions
themselves.
In addition to NWM use, some people with cancer believe there are certain diet
taboos in Asian culture. Therefore, even where a health care professional says “you
can eat anything”, cancer patients still tended to follow diet taboos. As Mr. Chen
reflected in the following account:
He (the doctor) said you can eat anything; it’s fine. Nothing you can’t
eat. (You) can eat anything. Western doctors are like that. (They) ask
you to take care of your nutrition status and don’t be fussy about
food…I still think that it has credibility (寧可信其有) (diet taboos)…
The Chen et al. (2005) study on attitudes of patients with malignant brain tumours
towards food and alternative treatment found that 7.1% of participants had diet
taboos before being diagnosed with cancer and 77% of participants had diet taboos
after cancer diagnosis. More than two thirds (77%) thought meat and sea food were
“poison”, especially duck and goose’s meat. This concept of diet taboos among

220
people with cancer came from themselves, family and friends (p. 62).
Some health care professionals reject NWM treatments, while others adopt an open
attitude and support cancer patients’ use of NWM. Mr. Wei made the following
comment:
He (the doctor) said if I got used to it, ok, no hazard, it was fine. 牛樟
菇 (Niu Zhang Gu), Dr. ╳ knew this. He usually listened to patients. He
did not reject. He did not reject.
Ms. Han portrayed her doctors’ open attitudes towards NWM:
I had asked Dr. X, I asked if there was any conflict (between Chinese
medicine and Western medicine). He said no. He said if you felt any
better, then you could take, (you) just needed to take two medicines at
separate times…(When I was) in ╳╳ (hospital), they (the doctors) are
also the same. They felt if you didn’t feel uncomfortable in the body then
it is helpful for yourself. They suggested to me to try. They won’t reject,
always encourage (us to try).
Further, Ms. Zhang’s husband also stated:

221
The Western medicine doctor said that Chinese medicine is not
ineffective. But nobody does serious testing (of Chinese medicine).
Otherwise, there are many Chinese medicine secret remedies. Nobody
does the serious test…Dr. X also said he listened to what patients use
and he would write down what patients said. If patients wanted to, he
also introduced Chinese medicine to the patients.
Because the participants in this study were receiving treatment in hospital, many
noted that they would listen to the doctors and cooperate with them because they had
come to the hospital. For example, Mr. Wei stated:
I thought my disease, since I trust this consultant, when he treated me, I
followed his instructions as much as possible. I would tell him if I ate
something in day to day life. At least I understand if there is any impact
or conflict. Doctor also had a better understanding of my life style. He
had a better understanding when he treated me. (We) cooperate with
each other.
Ms. Zheng also made the following comments about this issue:
Anyway I waited for doctors, whatever the doctor asked me to do, I do
it. I only need to cooperate. I then get well. Don’t think too much…

222
This is similar to Ms. Zhang thoughts:
Now, my thoughts in my mind, since we came here; (we) listened to the
doctor. These are my thoughts. Otherwise, it is uncomfortable to live
here.
The above data suggests that professional relationships are not essential in
determining perceptions of NWM and the role that such therapy plays in the
treatment of cancer. People have complex interactions with Western health care
professionals. When it comes to Western medicine treatment, cancer patients may
adhere to the directions of a doctor. However, cancer patients make decisions about
the use of NWM often regardless of a doctor’s opinion.
One study which investigated 453 outpatients in a comprehensive cancer centre
regarding the use of complementary and alternative medicine (CAM) found that
almost 74% of patients were willing to know more about CAM, and 90% of this
group preferred to source from books or pamphlets and 50% from doctors
(Richardson et al., 2000, p. 2509). Although some studies show that almost two
thirds (74%) of people do not discuss NWM with their health care professionals (Lim

223
et al.’s, 2005, p. 19), around 50% of patients in a US study stated they would like to
listen to their doctor’s opinions regarding NWM (Richardson et al., 2000, p. 2509).
In this study, professional relationships and practices do not seem to play a vital role
in cancer patients’ use of NWM. All participants in this study were treated in Western
hospitals. It is notable that no matter whether they discussed NWM with their health
care professionals or not, many decided to use NWM in some form.
While Western medicine treatment has become more institutionalised in Taiwan,
NWM exists in Taiwanese people’s day to day life and is present in the community.
People are able to share information about such therapies in informal ways, without
considerable effort. These community connections may therefore contribute to the
decisions of Taiwanese people with cancer to use NWM. Decisions about use of
these two treatments (Western medicine and NWM) appear to occur at different
levels. On the one hand, the decision to use Western medicine seems to be based on
the authority bestowed upon western trained medical professionals. On the other
hand, where decisions regarding NWM are made, this is more likely to occur within
a family or community context. We see, therefore, two quite distinct decision making
processes at work.

224
Summary
Three levels of social relationships and how they related to each other have been
discussed in this chapter. The analysis suggests why and how people with cancer use
or not use NWM. These social relationships, which include family connections and
community connections inform the decision making process of people with cancer in
using NWM. In addition, how and why professional relationships and practices are
important was also explored.
Next, the final chapter will address the core category and theoretical propositions of
this study.

225
CHAPTER 8
Taken-For-Grantedness
“Because after all we are Chinese…”
Because of the long and entrenched history of Chinese medicine in Taiwan, people
have traditionally incorporated such knowledge into their health care. As was argued
earlier, with the appearance and growing acceptance of Western medical practices,
multiple medical approaches have become more and more popular. Yet, despite the
strong foundations of Western medicine in the treatment of cancer in Taiwan, the use
of Chinese medicine has persisted and developed (Lin, 1992, p. 114).
Within this context, this study explored the processes of decision making that
underlie the use of non Western medicine by people in Taiwan with cancer. The
existence of a range of medical beliefs and systems of health care has long been
characteristic of East and Southeast Asia (Kunstadter & Kleinman, 1975, p. 739) and
particularly Hong Kong and China (Lee, 1975, pp. 231-235). An early review of a
number of studies in Asia by Kunstadter and Kleinman (1975) highlighted the

226
existence of choices for those with disease between systems of medical beliefs and
behaviours. None of these studies, however, extended to an exploration of the
processes whereby people in East and Southeast Asia make decisions on health care
therapies and regimes (p. 740). In the absence of subsequent studies on this issue
within Chinese communities, this study provides insight into the processes by which
people with cancer adopt various health practices and in particular, the use of NWM.
The core category that emerged from the study, a ‘‘taken-for-grantedness’’ in
decision making about the use of NWM, reflects the meanings as constructed and
articulated by the participants. These meanings, in turn, envelop the key categories of
philosophical beliefs and social relationships which set the conditions for the actions
of participants. The core and key categories and their constitutive knowledge thus
provide the bases for understanding how the social meanings of using NWM are
constructed and how people with cancer mediate the social processes of decision
making regarding the use of NWM.
The study analysis applied the Strauss and Corbin (1998) premise of “moving
between induction and deduction” to develop these understandings. That is, the study
sought to induce what is going on within the data by reading the data and engaging

227
with assumptions related to the data. The deductive phase constituted grounding the
interpretation of the data in existing research and literature to validate the
interpretation (pp. 136-137). Hence, from the point at which the core category
(“taken-for-grantedness”) emerged from the analysis, a deductive process has been
undertaken in theoretically linking the core category and its key categories and
subcategories.
The study findings extend knowledge on and understandings of how and why
Taiwanese people with cancer use NWM. As shown in figure 1, there are numerous
connections between the two main categories, philosophical beliefs and social
relationships and interactions which manifest in dynamic ways.
Furthermore, in seeking to explore how and why people with cancer in Taiwan use
NWM, the study concludes with some theoretical propositions about the underlying
social processes.

228
Philosophical beliefs
Social relationships
Traditional Chinese Philosophy
Professional Relationships and Practices
Religious Practices
Community Connections
Family Connections
Taken-for-Grantedness
Figure 1: Taiwanese People with Cancer and Non-Western Medicine (NWM) Use
Chinese Proverbs

229
Taken-for-Grantedness
The core category “taken-for-grantedness” encapsulates the context (or the conditions
for) and social meanings of NWM use in this study. This is well reflected in Ms.
Chu’s statement: “Because after all we are Chinese, (we) still believe in Chinese
medicine”. The context here is one where Traditional Chinese Medicine and Western
medicine coexist in Taiwan. Thus the study has sought to interpret the ways in which
people make sense of these coexisting systems and to pose a theorisation of the ways
people with cancer, as active participants in their social worlds, negotiate the various
systems of care. The findings of this study explored the context within which people
use Western medicine and NWM and the forms and patterns of NWM use. The
patterns of usage varied considerably and thus suggest that the interactions between
people with cancer and their use of NWM are complex.
The dominant tendency in this study was for the concurrent use of Western medicine
and NWM in the cancer treatment journeys. Furthermore and importantly, for many,
NWM was not understood solely as a therapy “complementary” to Western medicine
but rather as a therapy that has its own distinct value. This is so because, unlike
Western medicine, NWM was used according to views grounded in long standing

230
philosophical beliefs about health and healthcare. The coexistence of Western
medicine and NWM by people with cancer thus takes on a particular meaning.
Significantly, there is a taken-for-grantedness about the use of NWM which reflects a
level of autonomy in decision making. This contrasts notably with the use of Western
medicine which is most obviously linked to the expertise of the medical profession.
The use of NWM therapies for cancer is, therefore, a result of actions grounded in the
world of the participants far more so than the world of professionals.
Hence, the negotiations were mediated through deeply embedded and enduring belief
systems. From this study we see that the sense of taking NWM for granted is reflected
in philosophical beliefs, including traditional Chinese philosophy, religious practices
and Chinese proverbs and self destiny, all of which appear as integral to everyday life
in Taiwan.
Social relationships are also an important component of the interpretive process which
surrounds the use of NWM by people with cancer. These social relationships include
family connections and community connections. Significantly, professional
relationships with Western practitioners do not appear to be as important as family
and social relationships when it comes to decisions over the use of NWM among

231
Taiwanese people with cancer.
Interactions within different social dimensions determined how and why NWM might
or might not be used. People used NWM not simply because of its perceived
effectiveness, but more so because of a taken-for-grantedness of philosophical beliefs,
family connections and community connections. Human relationships and collectives
are essential forms of human activity and society and the individual are understood as
inseparable. Each social dimension considered in the study analysis was a different
phase of a social process that contributed to the ways in which people responded to
their diagnoses and health care.
Implications of the Findings
There are a number of potentially significant implications to be drawn from the study.
First, the study results show that health care professionals may be unaware of cancer
patient’s use of NWM. From a clinical point of view, it could thus be argued that it is
appropriate for health care professionals to have knowledge of NWM use. This view
is based on the notion that NWM may be harmful, and as such, health care
professionals will need to inform patients of potential risks. Indeed, several recent

232
studies are emphatic about the need for both instruction on NWM and the integration
of NWM into health care curricula and the health care system (Wyatt and Post-White,
2005, p. 216; Zhang, 2000, p. 139). Within this particular discourse it is a given that
the basis for regulation is evidence based research for which the randomised
controlled trial is considered the benchmark. Indeed, this is a standard that is largely
accepted uncritically as appropriate for NWM (Cardini, et al., 2006, p. 282; Feng, et
al., 2006, pp. 219-220).
However, while issues of patient safety and good clinical outcomes are important
concerns, they did not appear to predominate in this study. Participants were
concerned about doing their best in their situations and there was little concern that
NWM would compromise wellbeing. Indeed, Traditional Chinese Medicine uses a
very different structure and process from Western medicine and it may not be
appropriate to apply the same standards for evaluating the two systems (Chi, 1996, p.
1345). From this perspective, communication with patients about risks of treatments
will always be problematic since the methods used to define and determine such risks
cannot be agreed. However, promoting open communication about treatment
decisions is likely to be important to support and clarify these where requested.

233
A further and related implication points to the dominance within the current literature
of the concept of the integration of Western medicine and NWM or, in other words,
the mainstreaming of NWM within western medical system (Algier et al., 2005; Scott
et al., 2005; Wyatt and Post-White, 2005; Zhang, 2000). The findings of this study
give support to a more critical input into discussions on integration. For example, the
process of integration of NWM and Western medicine will see healthcare knowledge
increasingly become the privileged domain of health care professionals and thus
subject to the institutional constraints that characterise Western medicine. Yet, where
the authority of medical practitioners is broadened to incorporate NWM so the
autonomy of patient decision making in the use of NWM will be eroded. Furthermore,
integration implies institutionalisation, regulation and perhaps the exclusion of some
therapies. Finally, tensions may be created by efforts to integrate these two systems
and may result in, not only political struggles for dominant positions within health
care, but confusion and contradictions for individuals who already face significant
stressors.

234
Limitations of This Study
Symbolic interactionist research proposes that data and its findings are “here and
now”; “here” is located, “now” is timed. Thus, analysis of this kind is seen as
localised and concrete matter (Blumer, 1969, p. 131). In addition, a human’s social
life and formation is mediated through an interpretive process and this process is
contextualised.
But as we see from the above, the findings of this study may not be readily
generalised. Rather, this study provides a contextualised view of why and how people
with cancer act and how they interact with others in the particular social contexts of
eastern countries and associated family and community perspectives.
There is also the methodological issue in this study of saturation. It was earlier argued
that the study did not seek to achieve saturation. Rather, the concept of theoretical
saturation was applied in the analytical process and not in respect of sampling. This
may be considered a retreat from the traditional method and particularly that of
Strauss and Corbin. However, as has been argued previously, the original intent of
Glaser and Strauss (1967) was to define “saturation” as becoming possible only after

235
numerous research studies had been undertaken on the same phenomenon and within
similar contexts (p. 62). Seemingly, Glaser and Strauss well understood the
problematic of drawing a line in knowledge development, a point which has been
obscured in subsequent grounded theory texts. Clearly, one study is not able to
achieve saturation.
In addition, the participants of this study were all recruited from Western medicine
hospitals. To some degree, therefore, these participants were accepting of Western
medical treatments, even though they were using some forms of NWM. The
participants of this study did not include those who chose not to be treated in the
Western medicine system. It is noted that the processes for patients who reject western
treatments altogether may result in different emphases in terms of influences on the
construction of meaning. However, the strength of the study sample was that its
characteristics allowed for an exploration of a complex process of incorporating quite
distinct health care regimes.

236
Recommendations for Future Research
There is a dearth of qualitative research that explores the use of NWM among people
with cancer. From the findings of this study, we understand that people engage in
decision making processes regarding Western medicine and NWM in a variety of
ways. The Taiwan Public Health Report (2001) has indicated that the goal in the
development of Chinese Medicine is to reform Chinese Medicine so that it becomes a
more institutionalised process and thus encourages the integration of Chinese and
Western medicines (p. 35). It would be worthwhile to explore people’s perceptions
regarding institutionalised NWM settings, such as solely Chinese Medicine hospital
or clinics.
In addition, this study has focused only on people with cancer who were hospitalised
in Western hospitals and, therefore, an exploration of the broader population in the
community is indicated. Further, this study concentrated on Taiwanese people with
cancer. Most of the findings of the study appear to be specific to Eastern culture, such
as traditional Chinese philosophy and religious practice (Buddhism, Taoism and folk
beliefs are more Eastern oriented). Therefore, it is recommended that similar studies
be undertaken in Western countries, such as Australia, to determine if there are

237
significant differences between the two cultures that shape decision making processes
related to NWM use. It is also recommended that studies be undertaken exploring
Taiwanese health care professionals’ perspectives and understandings of the use of
NWM among people with cancer.
Conclusion
The social process that emerged from this study presents an explanation of the
conditions within which the use of NWM was interpreted by Taiwanese people with
cancer. The study explored how philosophical beliefs and social relationships and all
that these entail presented as the contexts that conditioned, although did not determine,
decision making. This study has thus provided an opportunity to explore the various
patterns of co-existence of NWM and Western medicine as experienced by Taiwanese
people with cancer and the social processes with which Taiwanese people engage
when using NWM in their cancer treatment journey.

238
References
Abraham, C., & Sheeran, P. (2000). Understanding and Changing Health Behaviour: From Health Beliefs to Self-Regulation. In P. Norman & C. Abraham & M. Conner (Eds.), Understanding and Changing Health Behaviour: from Health Beliefs to Self-Regulation (pp. 3-24). Amsterdam: Harwood Academic Publishers. Adams, J. (2000). General practitioners, complementary therapies and evidence-based medicine: the defence of clinical autonomy. Complementary Therapies in Medicine, 8(4), 248-252. Adamson, G. (2003). Patient empowerment in cancer management healing the whole person. Complementary Therapies in Nursing and Midwifery, 9(3), 109-113. Ades, T., & Yarbro, C. H. (2000). Alternative and Complementary Therapies in Cancer Management. In C. H. Yarbro & M. H. Frogge & M. Goodman & S. L. Groenwald (Eds.), Cancer Nursing-Principles and Practice (pp. 616-630). London: Jones and Bartlett. Albrecht, G., Higginbotham, N., & Freeman, S. (2001). The Hierarchy of Health Influences. In N. Higginbotham & G. Albrecht & L. Connor (Eds.), Health Social Science: A Transdisciplinary and Complexity Perspective (pp. 17-46). Melbourne: Oxford University Press. Alexander, R. D. (1990). Epigenetic Rules and Darwinian Algorithms: The Adaptive Study of Learning and Development. Ethology and Sociobiology, 11(4-5), 241-303. Algier, L. A., Hanoglu, Z., Özden, G., & Kara, F. (2005). The use of complementary and alternative (non-conventional) medicine in cancer patients in Turkey. European Journal of Oncology Nursing Complementary Therapies in Cancer, 9(2), 138-146. Allan, G., & Crow, G. (2001). Families, households and society. Basingstoke: Palgrave. Alvesson, M., & Sköldberg, K. (2000). Reflexive Methodology: New Vistas for

239
Qualitative Research. London: Sage. Ambert, A. M., Adler, P. A., Adler, P., & Detzner, D. F. (1995). Understanding and evaluating qualitative research. Journal of Marriage and the Family, 57, 879-893. American Cancer Society. (2000). American Cancer Society's Guide to Complementary and Alternative Cancer Methods. Atlanta, Ga: American Cancer Society. American Cancer Society. (2006). Guides For Using Complementary and Alternative Methods. Retrieved 29 December, 2006, from the World Wide Web: http://www.cancer.org/docroot/ETO/content/ETO Andrews, G. J. (2003). Placing the consumption of private complementary medicine: everyday geographies of older peoples' use. Health & Place, 9(4), 337-349. Annells, M. (1997). Grounded theory method, part 1: with the five moments of qualitative research. Nursing Inquiry, 4, 120-129. Annells, M. (1997). Grounded theory method, part 2: options for users of the method. Nursing Inquiry, 4, 176-180. Astin, J. A. (1998). Why Patients Use Alternative Medicine: Result of a National Study. Journal of American Medical Association (JAMA), 279(19), 1548-1553.
Baker, C., Wuest, J., & Stern, P. N. (1992). Method Slurring: The Grounded Theory/Phenomenology Example. Journal of Advanced Nursing, 17, 1355-1360. Beck, C. T. (1999). Grounded Theory Research. In J. A. Fain (Ed.), Reading, Understanding, and ApplYin Nursing Research: A Text and Workbook (pp. 205-226). Philadelphia: F. A. Davis Company. Becker, B., & Charles, N. (2006). Layered Meanings: The construction of 'the family' in the interview. Community, Work & Family, 9(2), 101-122. Behi, R., & Nolan, M. (1995). Ethical Issues in Research. British Journal of Nursing, 4(12), 712-716.

240
Benoliel, J. Q. (1996). Grounded Theory and Nursing Knowledge. Qualitative Health Research, 6(3), 406-428. Berry, D. L. (1993). Return-to-Work Experiences of People With Cancer. Oncology Nursing Forum, 20(9), 905-911. Blumer, H. (1954). What Is Wrong with Social Theory. American Sociological Review, 19(1), 3-10. Blumer, H. (1969). Symbolic Interactionism: Perspective and Method. Englewood Cliffs: Prentice-Hall, Inc. Blumer, H. (1978). Society as Symbolic Interaction. In A. Wells (Ed.), Contemporary Sociological Theories (pp. 91-98). Santa Monica: Goodyear. Boon, H., Brown, J. B., Gavin, A., Kennard, M. A., & Stewart, M. (1999). Breast Cancer Survivor's Perceptions of Complementary/ Alternative Medicine (CAM): Making the Decision to Use or Not to Use. Qualitative Health Research, 9(5), 639-653. Bottomley, J. M. (2004). Qi Gong for Health and Healing. In C. M. Davis (Ed.), Complementary Therapies in Rehabilitation (pp. 253-282). Thorofare: Slack Incorporated. Bowman, K. W., & Singer, P. A. (2001). Chinese seniors perspectives on end-of-life decisions. Social Science & Medicine, 53(4), 455-464. Bubolz, M. M. (2001). Family as source, user, and builder of social capital. Journal of Socio-Economics, 30(2), 129-131. Budenholzer, F. E. (2001). Religion and Science in Taiwan: Rethinking the Connection. Zygon, 36(4), 753-764. Burns, N. (1989). Standards for qualitative research. Nursing Science Quarterly, 2, 44-52. Cardini, F., Wade, C., Regalia, A. L., Gui, S., Li, W., Raschetti, R., & Kronenberg, F. (2006). Clinical research in traditional medicine: Priorities and methods. Complementary Therapies in Medicine, 14(4), 282-287.

241
Carone, J., Dominic A., & Barone, D. F. (2001). A social cognitive perspective on religious beliefs: their functions and impact on coping and psychotherapy. Clinical Psychology Review, 21(7), 989-1003. Carter, B. (2003). Methodological issues and complementary therapies: researching intangibles? Complementary Therapies in Nursing and Midwifery, 9, 133-139. Cassileth, B., R., & Chapman, C. C. (1996). Alternative and Complementary Cancer Therapies. Cancer, 77(6), 1026-1034. Cassileth, B., R. (1998). Resources for Alternative and Complementary Cancer Therapies. Cancer Practice, 6(5), 299-301. Castles, M. R. (1987). Organising The Literature Review. In M. R. Castles (Ed.), Primer of Nursing Research (pp. 45-53). Philadelphia: W. B. Saunders. Chan, K. (2005). Chinese medicinal materials and their interface with Western medical concepts. Journal of Ethnopharmacology, 96(1-2), 1-18. Chan, E. A., Cheung, K., Mok, E., Cheung, S., & Tong, E. (2006). A narrative inquiry into the Hong Kong Chinese adults' concepts of health through their cultural stories. International Journal of Nursing Studies, 43(3), 301-309. Chang, L. C., & Li, L. C. (2004). Patterns of complementary therapy use by homebound cancer patients in Taiwan. Applied Nursing Research, 17(1), 41-47. Chang, J. H. Y. (2004). Mead's Theory of Emergence as a Framework for Multilevel Sociological Inquiry. Symbolic Interaction, 27(3), 405-427. Chao, Y. M. (1995). Nursing's Values From a Confucian Perspective. International Nursing Review, 42(5), 147-149. Charles, C., Gafni, A., & Whelan, T. (1999). Decision making in the physician-patient encounter: revisiting the shared treatment decision making model. Social Science & Medicine, 49(5), 651-661. Charmaz, K. (1983). The grounded theory method: An explication and interpretation.

242
In R. M. Emerson (Ed.), Contemporary field research: a collection of readings (pp. 109-126). Prospect Heights, Ill: Waveland Press. Charmaz, K. (1990). 'Discovering' Chronic Illness: Using Grounded Theory. Social Science and Medicine, 30(11), 1161-1172. Charmaz, K. (2000). Grounded Theory: Objectivist and Contructivist Methods. In N. K. Denzin & Y. S. Lincoln (Eds.), Handbook of Qualitative Research (2nd ed., pp. 509-536). London: Sage. Charon, J. M. (2004). Symbolic Interactionism: An Introduction, An Interpretation, An Integration. Upper Saddle River: Pearson Prentice Hall. Cheek, J., Shoebridge, J., Willis, E., & Zadoroznyj, M. (1996). Society and Health: Social theory for health workers. Melbourne: Longman. Chen, Y. C. (2001). Chinese values, health and nursing. Journal of Advanced Nursing, 36(2), 270-273. Chenitz, W. C., & Swanson, J. M. (1986). Qualitative research using grounded theory. In W. C. Chenitz & J. M. Swanson (Eds.), From Practice To Grounded Theory: qualitative research in nursing (pp. 3-15). Menlo Park: Addison-Wesley Publishing. Chenitz, W. C. (1986). The informal interview. In W. C. Chenitz & J. M. Swanson (Eds.), From Practice To Grounded Theory: qualitative research in nursing (pp. 79-90). Menlo Park: Addison-Wesley Publishing. Cheung, C.-K., Kwan, A. Y.-H., & Ng, S. H. (2006). Impacts of filial piety on preference for kinship versus public care. Journal of Community Psychology, 34(5), 617-634. Chez, R. A., Jonas, W. B., & Eisenberg, D. (1999). The Physician and Complementary and Alternative Medicine. In W. B. Jonas & J. S. Levin (Eds.), Essentials of Complementary and Alternative Medicine (pp. 31-45). Philadelphia: Lippincott. Chi, C. (1994). Integrating Traditional Medicine into Modern Health Care System: Examining The Role of Chinese Medicine in Taiwan. Social Science and Medicine, 39(3), 307-321.

243
Chi, C., Lee, J. L., Lai, J. S., Chen, C. Y., Chang, S. K., & Chen, S. C. (1996). The practice of Chinese medicine in Taiwan. Social Science & Medicine, 43(9), 1329-1348. Chi, C., Lee, J. L., Lai, J. S., Chen, S. C., Chen, C. Y., & Chang, S. K. (1997). Utilization of Chinese Medicine in Taiwan. Alternative Therapies, 3(4), 40-53. Chiu, L. (2000). Transcending Breast Cancer, Transcending Death: A Taiwanese Population. Nursing Science Quarterly, 13(1), 64-72. Chiu, L. (2001). Spiritual resources of Chinese immigrants with breast cancer in the USA. International Journal of Nursing Studies, 38(2), 175-184. Cho, H. J. (2000). Traditional medicine, professional monopoly and structural interests: a Korean case. Social Science & Medicine, 50(1), 123-135. Clarke, A. E. (2003). Situational Analyses: Grounded Theory Mapping After the Postmodern Turn. Symbolic Interaction, 26(4), 553-576. Clavarino, A., & Yates, P. (1995). Fear, Faith or Rational Choice: Understanding the Users of Alternative Therapies. In G. M. Lupton & J. M. Najman (Eds.), Sociology of Health and Illness: Australian Readings (2nd ed., pp. 252-275). Melbourne: Macmillan Education Australia. Conrad, M. E., Brown, P., & Conrad, M. G. (1996). Fatalism and breast cancer in black women. Annual Internal Medicine, 125(11), 941-942. Corbin, J., & Strauss, A. (1990). Grounded Theory Research: Procedures, Canons, and Evaluative Criteria. Qualitative Sociology, 13(1), 3-21. Corbin, J. M. (1998). Alternative Interpretations: Valid or Not? Theory & Psychology, 8(1), 121-128. Cordova, M. J., Giese-Davis, J., Golant, M., Kronnenwetter, C., Chang, V., McFarlin, S., & Spiegel, D. (2003). Mood disturbance in community cancer support groups: The role of emotional suppression and fighting spirit. Journal of Psychosomatic Research, 55(5), 461-467.

244
Cunningham, R. S., & Herbert, V. (2000). Nutrition As A Complement of Alternative Therapy. Seminars in Oncology Nursing, 16(2), 163-169. Cutcliffe, J. R., & McKenna, H. P. (1999). Establishing The Credibility of Qualitative Research Findings: The Plot Thickens. Journal of Advanced Nursing, 30(2), 374-380. Cutcliffe, J. R. (2000). Methodological Issues in Grounded Theory. Journal of Advanced Nursing, 31(6), 1476-1484. Decker, G. M. (2000). An Overview of Complementary and Alternative Therapies. Clinical Journal of Oncology Nursing, 4(1), 49-52. DEGUI, C. (2005). AMERICAN CONFUCIANISM. Journal of Chinese Philosophy, 32(1), 123-138. DeKeyser, F. G., Cohen, B. B., & Wagner, N. (2001). Knowledge levels and attitudes of staff nurses in Israel towards complementary and alternative medicine. Journal of Advanced Nursing, 36(1), 41-48. Department of Health Taiwan, R. O. C. (2001). Taiwan Public Health Report 2001. Taipei: Department of Health Taiwan, R. O. C. Department of Health Taiwan, R. O. C. (2005). The Death Statistic (Table 1: The Major Cause of Death in Taiwan). Retrieved December 20, 2006, from the World Wide Web: http://www.doh.gov.tw/statistic/STbook.ASP Domino, G., & Lin, W. Y. (1993). Cancer Metaphors: Taiwan and the United States. International Journal of Psychology, 28(1), 45-56. Easthope, G. (2003). Alternative, Complementary, or Integrative? Complementary Therapies in Medicine, 11, 2-3. Eaves, Y. D. (2001). A Synthesis Technique for Grounded Theory Data Analysis. Journal of Advanced Nursing, 35(5), 654-663. Eguchi, K., Hyodo, I., & Saeki, H. (2000). Current status of cancer patients' perception of alternative medicine in Japan: a preliminary cross-sectional survey.

245
Supportive Care in Cancer, 8, 28-32. Eisenberg, D. M., Kessler, R. C., Foster, C., Norlock, F. E., Calkins, D. R., & Delbanco, T. L. (1993). Unconventional Medicine in the United States: Prevalence, Costs, and Pattern of Use. The New England Journal of Medicine, 328(4), 246-252. Eisenberg, D. M., Davis, R. B., & Ettner, S. L. (1998). Trends in Alternative Medicine Use in the United States, 1990-1997: Result of a Follow-up National Survey. Journal of American Medical Association (JAMA), 280(18), 1569-1575. Eisenberg, D., Kessler, R. C., Rompay, M. I. V., Kaptchuk, T. J., Wilkey, S. A., et al. (2001). Perceptions about Complementary Therapies Relative to Conventional Therapies among Adults Who Use Both: Results from a National Survey. Annals of Internal Medicine, 135(5), 344-351. Engebretson, J. (1999). Alternative and Complementary Healing: Implications for Nursing. Journal of Professional Nursing, 15(4), 214-223. Engebretson, J. (2002). Culture and complementary therapies. Complementary Therapies in Nursing and Midwifery, 8(4), 177-184. Ernst, E., & Fugh-Berman, A. (2002). Complementary and alternative medicine: What is it all about? Occupational and Environmental Medicine, 59(2), 140-144. Esposito, N. (2001). From Meaning to Meaning: The Influence of Translation Techniques on Non-English Focus Group Research. Qualitative Health Research, 11(4), 568-579. Fee, L., Cronin, A., Simmons, R., & Choudry, S. (1999). Assessing older people's health and social needs: Qualitative research investigating health beliefs and social factors relevant to older people's health. London: Health Education Authority. Feng, Y., Wu, Z., Zhou, X., Zhou, Z., & Fan, W. (2006). Knowledge discovery in traditional Chinese medicine: State of the art and perspectives. Artificial Intelligence in Medicine, 38(3), 219-236. Flick, U. (1998). An Introduction to Qualitative Research. London: Sage.
246
Flinn, M. V. (1997). Culture and the evolution of social learning. Evolution and Human Behavior, 18(1), 23-67. Fontana, A., & Frey, J. H. (2000). The Interview: From Structured Questions to Negotiated Text. In N. K. Denzin & Y. S. Lincoln (Eds.), Handbook of Qualitative Research (2nd ed., pp. 645-672). London: Sage. Franks, P., Campbell, T. L., & Shields, C. G. (1992). Social relationships and health: The relative roles of family functioning and social support. Social Science & Medicine, 34(7), 779-788. Gecsedi, R., & Decker, G. (2001). Incorporating Alternative Therapies into Pain Management. American Journal of Nursing, 101(4), 35-39. Gilbert, D. A. (2002). Culture and Holistic Nursing. In M. A. Bright (Ed.), Holistic Health and Healing (pp. 71-80). Philadelphia: F. A. Davis Company. Glaser, B. G. (1965). The constant comparative method of qualitative analysis. Social Problems, 12, 436-445. Glaser, B. G., & Strauss, A. L. (1965). Awareness of Dying. New York: Aldine Publishing Co. Glaser, B. G., & Strauss, A. L. (1967). The Discovery of Grounded Theory. Chicago: Aldine. Glaser, B. G. (1978). Theoretical Sensitivity. Mill Valley: The Sociology Press. Glaser, B. G. (1992). Emergence vs Forcing: Basics of Grounded Theory Analysis. Mill Valley: Sociology Press. Graham, H. (1999). Complementary Therapies in Context: The Psychology of Healing. London: Jessica Kingsley Publishers. Gurm, B. K., Stephen, J., MacKenzie, G., Doll, R., Barroetavena, M. C., & Cadell, S. Understanding Canadian Punjabi-speaking South Asian women's experience of breast cancer: A qualitative study. International Journal of Nursing Studies, In Press, Corrected Proof.

247
Gusfield, J. R. (2003). A Journey with Symbolic Interaction. Symbolic interaction, 26(1), 119-139. Hammersley, M. (1989). The Dilemma of Qualitative Method: Herbert Blumer and the Chicago Tradition. New York: Routledge. Harmsworth, K., & Lewith, G. T. (2001). Attitudes to traditional Chinese medicine amongst Western trained doctors in the People’s Republic of China. Social Science & Medicine, 52(1), 149-153. Harrell, S. (1977). Modes of Belief in Chinese Folk Religion. Journal for the Scientific Study of Religion, 16(1), 55-65. Haworth-Hoeppner, S. (2005). A Sociological Account of the Persistence of Invalidated Anorexic Identities. Symbolic Interaction, 28(1), 1-23. Hollenberg, D. (2006). Uncharted ground: Patterns of professional interaction among complementary/alternative and biomedical practitioners in integrative health care settings. Social Science & Medicine, 62(3), 731-744. Holloway, I., & Wheeler, S. (2002). Qualitative Research in Nursing (2nd ed.). Melbourne: Blackwell Publishing. Holroyd, E. (2002). Health-Seeking Behaviors and Social Change: The Experience of the Hong Kong Chinese Elderly. Qualitative Health Research, 12(6), 731-750. Hsieh, Y. W. (1967). Filial Piety and Chinese Society. In C. A. Moore & A. V. Morris (Eds.), The Chinese Mind: Essentials of Chinese Philosophy and Culture (pp. 167-187). Honolulu: East-West Center Press. Huang, Y. H. (2000). The personal influence model and Gao Guanxi in Taiwan Chinese public relations. Public Relations Review, 26(2), 219-236. Hufford, D. J. (2002). CAM and Culture Diversity: Ethics and Epistemology Coverge. In D. Callahan (Ed.), The Role of Complementary & Alternative Medicine: accommodating pluralism (pp. 15-35). Washington, D. C.: Georgetown University Press.

248
Hunt, A., & Millar, R. (2000). As Science for Public Understanding. Chicago: Heinemann. Hwang, K.-K. (1999). Filial Piety and Loyalty: Two Types of Social Identification in Confucianism. Asian Journal of Social Psychology, 2(1), 163-183. Hwu, Y. J., Coates, V. E., & Boore, J. R. P. (2001). The health behaviours of Chinese people with chronic illness. International Journal of Nursing Studies, 38(6), 629-641. ISAY, G. C. (2005). QIAN MU AND THE MODERN TRANSFORMATION OF FILIAL PIETY. Journal of Chinese Philosophy, 32(3), 441-454. Jensen, L. M. (1997). Manufacturing Confucianism: Chinese Traditions and Universal Civilization. Durham: Duke University Press. Jiang, B. (1997). The Cultural Tradition of China and Modernization. In M. Wang & X. Yu & G. F. McLean (Eds.), Chinese Cultural Traditions and Moderization: Chinese Philosophical Studies, X. Washington, D. C.: The Council for Research in Values and Philosophy. Johnson, M. R. D. (2004). Faith, prayer, and religious observances. Clinical Cornerstone, 6(1), 17-24. Katz, P. R. (1999). Morality Books and Taiwanese Identity: The Texts of the Palace of Guidance. Journal of Chinese Religions, 27, 69-92. Katz, P. R. (2003). Religion and the State in Post-war Taiwan. The China Quarterly, 174(1), 395-412. Keats, D. M. (2000). Interviewing: A Practical Guide for Students and Professionals. Sydney: UNSW Press. Kemp, C. (2005). Cultural issues in palliative care. Seminars in Oncology Nursing, 21(1), 44-52. Kleinman, A. (1975). Social, Cultural and Historical Themes in the Study of Medicine in Chinese Societies: Problems and Prospects for the Comparative Study of Medicine

249
and Psychiatry. In A. Kleinman & P. Kunstadter & E. R. Alexander & J. L. Gale (Eds.), Medicine in Chinese Cultures: Comparative Studies of Health Care in Chinese and Other Societies (pp. 589-643). Washington, D.C.: U.S. Department of Health, Education, and Welfare Public Health Service. Kunstadter, P., & Kleinman, A. (1975). Epilogue. In A. Kleinman & P. Kunstadter & E. R. Alexander & J. L. Gale (Eds.), Medicine in Chinese Cultures: Comparative Studies of Health Care in Chinese and Other Societies (pp. 737-747). Washington, D.C.: U.S. Department of Health, Education, and Welfare Public Health Service. Kuroda, T. (1994). Family Structure and Social Change: Implications of Fertility Changes in Japan and China. In L. J. Cho & M. Yada (Eds.), Tradition and Change in the Asian Family (pp. 45-55). Honolulu: East-West Center. Lao, L. (1999). Traditional Chinese Medicine. In W. B. Jonas & J. S. Levin (Eds.), Essentials of Complementary and Alternative Medicine (pp. 216-232). Philadelphia: Lippincott Williams & Wilkins. Lee, R. P. L. (1975). Interaction between Chinese and Western Medicine in Hong Kong: Modernization and Professional Inequality. In A. Kleinman & P. Kunstadter & E. R. Alexander & J. L. Gale (Eds.), Medicine in Chinese Cultures: Comparative Studies of Health Care in Chinese and Other Societies (pp. 219-240). Washington, D.C.: U.S. Department of Health, Education, and Welfare Public Health Service. Lee, R. P. L. (1981). Chinese and Western Health Care Systems: Professional Stratification in a Modernizing Society. In A. Y. C. King & R. P. L. Lee (Eds.), Social Life and Development in Hong Kong (pp. 255-274). Hong Kong: Chinese University Press. Lee, M.-L., & Sun, T.-H. (1995). The Family and Demography in Contemporary Taiwan. Journal of Comparative Family Studies, XXVI (1), 101-115. Lee, C. H., & Liang, W. M. (2006). Attitudes and Intentions of Patients Toward Integrated Chinese and Western Medicine in Taiwan. The Journal of Alternative and Complementary Medicine, 12(3), 233-236. Lew-Ting, C. Y. (2005). Antibiomedicine belief and integrative health seeking in Taiwan. Social Science & Medicine, 60, 2111-2116.

250
Lewith, G., Kenyon, J., & Lewis, P. (1996). Complementary Medicine: An Integrated Approach. New York: Oxford University Press. Lim, M. K., Sadarangani, P., Chan, H. L., & Heng, J. Y. (2005). Complementary and alternative medicine use in multiracial Singapore. Complementary Therapies in Medicine, 13(1), 16-24. Liu-Wang, H. C. (1959). An Analysis of Chinese Clan Rules: Confucian Theories in Action. In D. S. Nivison & A. F. Wright (Eds.), Confucianism in Action (pp. 63-96). Stanford: Stanford University Press. Liu, J. M., Chu, H. C., Chin, Y. H., Chen, Y. M., Hsieh, R. K., Chiou, T. J., & Whang-Pang, J. (1997). Cross Sectional Study of Use of Alternative Medicine in Chinese Cancer Patients. Japanese Journal of Clinical Oncology, 27(1), 37-41. Locke, K. (1996). Rewriting The Discovery of Grounded Theory After 25 Years? Journal of Management Inquiry, 5(3), 239-245. Lomborg, K., & Kirkevold, M. (2003). Truth and validity in grounded theory-a reconsidered realist interpretation of the criteria: fit, work, relevance and modifiability. Nursing Philosophy, 4(3), 189-200. Low, J. (1999). The Experiences of People Who Use Alternative Therapies: A Symbolic Interactionist Analysis. McMaster University, Hamilton. Low, J. (2001). Alternative, complementary or concurrent health care? A critical analysis of the use of the concept of complementary therapy. Complementary Therapies in Medicine, 9, 105-110. Lu, L. (2002). A preliminary study on the concept of health among the Chinese. Counselling Psychology Quarterly, 15(2), 179-189. Ma, H. K. (1990). The Chinese Taoistic perspective on human development. International Journal of Intercultural Relations, 14(2), 235-249. MacLennan, A. H., Wilson, D. H., & Taylor, A. W. (1996). Prevalence and cost of alternative medicine in Australia. The Lancet, 347, 569-573.

251
Maines, D. R. (2001). The Fault line of Consciousness: A View of Interactionism in Sociology. New York: Aldine de Gruyter. Maines, D. R. (2003). Interactionism's Place. Symbolic Interaction, 26(1), 5-18. Marshall, C. (1990). Goodness criteria: Are they objective or judgement calls? In E. G. Guba (Ed.), The paradigm dialog (pp. 188-197). Newbury Park, CA: Sage. Martin, K. G. (1975). Medical Systems in A Taiwan Village: Ong-Ia-Kong, The Plague God as Modern Physician. In A. Kleinman & P. Kunstadter & E. R. Alexander & J. L. Gale (Eds.), Medicine in Chinese Cultures: Comparative Studies of Health Care in Chinese and Other Societies (pp. 115-141). Washington, D.C.: U.S. Department of Health, Education, and Welfare Public Health Service. Martin, P. Y., & Turner, B. A. (1986). Grounded Theory and Organisational Research. The Journal of Applied Behavioural Science, 22(2), 141-157. Maxwell, J. A. (1992). Understanding and validity in qualitative research. Harvard Educational Review, 62, 279-299. Maxwell, J. A. (1996). Qualitative research design: An interactive approach. Thousand Oaks, CA: Sage. McCabe, P., & Kenny, A. (2003). Complementary Therapies. In M. O'Connor & S. Aranda (Eds.), Palliative Care Nursing: A Guide to Practice (2 ed., pp. 259-270). Melbourne: Ausmed Publications. McCabe, P. (2005). Complementary and alternative medicine in Australia: a contemporary overview. Complementary Therapies in Clinical Practice, 11(1), 28-31. McCraken, G. (1988). The Long Interview. Newbury Park: Sage. Mead, G. H. (1932). The Philosophy of the Present. Chicago: The University of Chicago Press. Mead, G. H. (1956). George Herbert Mead on Social Psychology: Selected Papers Edited and with an Introduction by Anselm Strauss. London: The University of

252
Chicago Press. Meeker, W. C. (2000). Public demand and the integration of complementary and alternative medicine in the US health care system. Journal of Manipulative and Physiological Therapeutics, 23(2), 123-126. Melchart, D., Linde, K., Fischer, P., White, A., Allais, G., Vickers, A., & Berman, B. (1999). Acupuncture for recurrent headaches: a systematic review of randomised controlled trials. Cephalalgia, 19, 779-786. Melia, K. M. (1996). Rediscovering Glaser. Qualitative Health Research, 6(3), 368-378. Millers, D. E., & Hintz Jr., R. A. (1997). The Structure of Social Interaction. Studies in Symbolic Interaction, Supplement 3, 87-107. Moldoveanu, M., & Stevenson, H. (2001). The self as a problem: the intra-personal coordination of conflicting desires. Journal of Socio-Economics, 30(4), 295-330. Morrione, T. J. (1998). Persistence and change: fundamental elements in Herbert Blumer's metatheoretical perspective. In L. Tomasi (Ed.), The Tradition of the Chicago School of Sociology (pp. 191-216). Aldershot Hants: Ashgate. Mulvaney-Day, N. E., Alegria, M., & Sribney, W. (2007). Social cohesion, social support, and health among Latinos in the United States. Social Science & Medicine, 64(2), 477-495. Nam, R. K., Fleshner, N., Rakovitch, E., Klotz, L., Trachtenberg, J., & Choo, R. (1999). Prevalence and patterns of the use of complementary therapies among prostate cancer patients: an epidemiological analysis. Journal of Urology, 161, 1521-1524. National Breast Cancer Centre. (2003). Clinical practice guidelines for the psychosocial care of adults with cancer. Camperdown: National Breast Cancer Centre. National Centre for Complementary and Alternative Medicine. (2001). Expanding Horizons of Healthcare: Five Year Strategic Plan 2001-2005. Washington DC: National Institutes of Health.

253
National Centre for Complementary and Alternative Medicine. (2003). National Centre for Complementary and Alternative Medicine. Retrieved October 7, 2003, from the World Wide Web: http://nccam.hin.gov National Council Against Health Fraud. (1998). Survey finds increased use of alternative healthcare. NCAHF Newsletter, 21(2), 1-2. National Health and Medical Research Council. (2006). Complementary and Alternative Medicine Special Call for Research Applications. Retrieved December 20, 2006, from the World Wide Web: http://www.nhmrc.gov.au/funding/types/granttype/strategic/cam.htm Nelson McDermott, M. A., & Palchances, K. (1994). A literature review of the critical elements in translation theory. Journal of Nursing Scholarship, 26(2), 113-116. Ni, P. (1999). Confucian Virtues and Personal Health. In R. Fan (Ed.), Confucian Bioethics (pp. 27-44). Dordrecht: Kluwer Academic Publishers. O'Callaghan, F. V., & Jordan, N. (2003). Postmodern values, attitudes and the use of complementary medicine. Complementary Therapies in Medicine, 11(1), 28-32. O'Connor, B. B. (2000). Conceptions of the Body in Complementary and Alternative Medicine. In M. Kelner & B. Wellman & B. Pescosolido & M. Saks (Eds.), Complementary and Alternative Medicine: Challenge and Change (pp. 39-60). Amsterdam: Harwood Academic Publishers. Ott, M. J. (2002). Complementary and Alternative Therapies in Cancer Symptom Management. Cancer Practice, 10(3), 162-166. Parkman, C. (2001). Alternative Therapies Are Here to Stay. Nursing Management, 32(2), 36-39. Parry, K. W. (1998). Grounded Theory and Social Process: A New Direction for Leadership Research. Leadership Quarterly, 9(1), 85-105. Patton, M. Q. (1990). Qualitative evaluation and research methods. Newbury Park, CA: Sage.

254
Peace, G., & Simons, D. (1996). Completing The Whole. Nursing Times, 92(25), 52-54. Peters, D., Chaitow, L., Harris, G., & Morrison, S. (2002). Integrating Complementary Therapies in Primary Care. London: Churchill Livingstone. Phillips, D. L. (1993). Looking backward: A critical appraisal of communitarian thought. Princeton, NJ: Princeton University Press. Pidgeon, N. (1996). Grounded theory: theoretical background. In J. T. E. Richardson (Ed.), Handbook of Qualitative Research Methods: for Psychology and the Social Sciences (pp. 75-85). Leicester: BPS Books. Popay, J., Rogers, A., & Williams, G. (1998). Rationale and standards for the systematic review of qualitative literature in health services research. Qualitative Health Research, 8, 341-351. Powe, B. D., & Finnie, R. (2003). Cancer Fatalism: The State of the Science. Cancer Nursing, 26(6), 454-465. Powell, C. B., Dibble, S. L., Dall'Era, J. E., & Cohen, I. (2002). Use of herbs in women diagnosed with ovarian cancer. International Journal of Gynecological Cancer, 12(2), 214-217. Quah, S. R. (2003). Traditional healing systems and the ethos of science. Social Science & Medicine, 57(10), 1997-2012. Rao, J. K., Mihaliak, K., Kroenke, K., Bradley, J., Tierney, W. M., & Weinberger, M. (1999). Use of Complementary Therapies for Arthritis among Patients of Rheumatologists. Annual Internal Medicine, 131(6), 409-416. Rennie, D. L. (1998). Reply to Corbin: From One Interpreter to Another. Theory & Psychology, 8(1), 129-135. Rice, P. L., & Ezzy, D. (1999). Qualitative Research Methods: A Health Focus. Melbourne: Oxford University Press. Richardson, M. A., Sanders, T., Palmer, J. L., Greisinger, A., & Singletary, S. E.

255
(2000). Complementary/Alternative Medicine Use in a Comprehensive Cancer Center and Implications for Oncology. Journal of Clinical Oncology, 18(13), 2505-2514. Robinson, A., & McGrail, M. R. (2004). Disclosure of CAM use to medical practitioners: a review of qualitative and quantitative studies. Complementary Therapies in Medicine, 12(2-3), 90-98. Rodgers, B. L., & Yen, W.-J. (2002). Re-thinking nursing science through the understanding of Buddhism. Nursing Philosophy, 3(3), 213-221. Sandelowski, M. (1986). The problem of rigour in qualitative research. Advances in Nursing Science, 8, 27-37. Schroën, J. H. T. (2002). Non-linear dynamics and Chinese medicine: an essay on research models, TCM, and recent changes in modern scientific philosophy. Clinical Acupuncture and Oriental Medicine, 3(2), 92-98. Scott, J. A., Kearney, N., Hummerston, S., & Molassiotis, A. (2005). Use of complementary and alternative medicine in patients with cancer: A UK survey. European Journal of Oncology Nursing, 9(2), 131-137. Seidman, I. (1998). Interviewing as Qualitative Research: A Guide for Researchers in Education and Social Sciences. New York: Teachers College Press. Sheldon, L. (1998). Grounded Theory: Issues for Research in Nursing. Nursing Standard, 12(52), 47-50. Sharp, S. A. (1986). Folk medicine practices: Women as keepers and carriers of knowledge. Women’s Studies International Forum, 9(3), 243-249. Shen, J., & Glaspy, J. (2001). Acupuncture: Evidence and Implications for Cancer Supportive Care. Cancer Practice, 9(3), 147-150. Shih, F. J. (1996). Concepts related to Chinese patients' perceptions of health, illness and person: issues of conceptual clarity. Accident and Emergency Nursing, 4(4), 208-215. Simpson, P. B. (2003). Family Beliefs About Diet and Traditional Chinese Medicine

256
for Hong Kong Women With Breast Cancer. Oncology Nursing Forum, 30(5), 834-840. Smith-Fassler, M. E., & Lopez-Bushnell, K. (2001). Acupuncture as complementary therapy for back pain. Holistic Nursing Practice, 15(3), 35-44. Spencer, J. W. (1999). Essential Issues in Complementary/Alternative Medicine. In J. W. Spencer & J. J. Jacobs (Eds.), Complementary/Alternative Medicine: An Evidence-Based Approach (pp. 3-36). St. Louis: Mosby. Stern, P. N. (1980). Grounded Theory Methodology: Its Uses and Processes. Image, XII(1), 20-23. Stevenson, C. (1997). Complementary therapies and their role in nursing care. Nursing Standard, 24(11), 49-53. Stevenson, F. A., Britten, N., Barry, C. A., Bradley, C. P., & Barber, N. (2003). Self-treatment and its discussion in medical consultations: how is medical pluralism managed in practice? Social Science & Medicine, 57(3), 513-527. Strasen, L. (1999). The Silent Health Care Revolution: The Rising Demand for Complementary Medicine. Nursing Economics, 17(5), 246-251. Straughan, P. T., & Seow, A. (1998). Fatalism reconceptualized: a concept to predict health screening behavior. Journal of Gender Cultural Health, 3(2), 85-100. Strauss, A. (1987). Qualitative Analysis for Social Scientists. Cambridge: Cambridge University Press. Strauss, A., & Corbin, J. (1990). Basics of Qualitative Research: Grounded Theory Procedures and Techniques. Newbury Park: Sage. Strauss, A., & Corbin, J. (1994). Grounded Theory Methodology: An Overview. In N. K. Denzin & Y. S. Lincoln (Eds.), Handbook of Qualitative Research (pp. 273-285). Thousand Oaks: Sage. Strauss, A., & Corbin, J. (1997). Grounded Theory in Practice. London: Sage.

257
Strauss, A., & Corbin, J. (1998). Grounded Theory Methodology: An Overview. In N. Denzin & Y. Lincoln (Eds.), Strategies of Qualitative Inquiry (pp. 158-183). Thousand Oaks: Sage. Strauss, A., & Corbin, J. (1998). Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory. Thousand Oaks: Sage. Streubert, H. J., & Carpenter, D. R. (1999). Qualitative Research in Nursing: Advancing the Humanistic Imperative (2nd ed.). Philadelphia: J. B. Lippincott. Streubert-Speziale, H. J., & Carpenter, D. R. (2003). Qualitative Research in Nursing: Advancing the Humanistic Imperative (3nd ed.). Philadelphia: J. B. Lippincott. Sun, T. H., & Liu, Y. H. (1994). Changes in Intergenerational Relations in the Chinese Family: Taiwan's experience. In L. J. Cho & M. Yada (Eds.), Tradition and Change in the Asian Family (pp. 319-361). Honolulu: East-West Center. Tatsumura, Y., Maskarinec, G., Shumay, D. M., & Kakai, H. (2003). Religious and spiritual resources, CAM, and conventional treatment in the lives of cancer patients. Alternative Therapies in Health and Medicine, 9(3), 64-71. Taylor, E. J. (2001). Spirituality, culture, and cancer care. Seminars in Oncology Nursing, 17(3), 197-205. The Research Council for Complementary Medicine. (2003). The RCCM. Retrieved 7 October, 2003, from the World Wide Web: http://www.rccm.org.uk/ Thomas, K. J., Nicholl, J. P., & Coleman, P. (2001). Use and expenditure on complementary medicine in England: a population based survey. Complementary Therapies in Medicine, 9(1), 2-11. Thomas, R. B., & Bright, M. A. (2002). Global Health Issues. In M. A. Bright (Ed.), Holistic Health and Healing (pp. 81-102). Philadelphia: F. A. Davis Company. Thomas, T. L. (2002). Culture and Health. In M. VanRooyen & T. Kirsch & K. Clem & C. J. Holliman (Eds.), Emergent Field Medicine (pp. 77-90). New York: McGraw-Hill.

258
Thorne, S., Paterson, B., Russell, C., & Schultz, A. (2002). Complementary/alternative medicine in chronic illness as informed self-care decision making. International Journal of Nursing Studies, 39(7), 671-683. Tough, S. C., Johnston, D. W., Verhoef, M. J., Arthur, K., & Bryant, H. (2002). Complementary and alternative medicine use among colorectal cancer patients in Alberta, Canada. Alternative Therapies in Health and Medicine, 8(2), 54-64. Tsai, D. F.-C. (2006). Eye on Religion: Confucianism, Autonomy and Patient Care. Southern Medical Journal, 99(6), 685-687. Tulder, M. W., Cherkin, D. C., Berman, B., Lao, L., & Koes, B. W. (2002). Acupuncture for low back pain (Cochrane Review). The Cochrane Library, 4, 1-25. Twinn, S. (1997). An exploratory study examining the influence of translation on the validity and reliability of qualitative data in nursing research. Journal of Advanced Nursing, 26(2), 418-423. Twinn, D. S. (1998). An analysis of the effectiveness of focus groups as a method of qualitative data collection with Chinese populations in nursing research. Journal of Advanced Nursing, 28(3), 654-661. Twycross, R. (1994). Pain Relief in Advanced Cancer. New York: Churchill Livingstone. Veith, I. (1972). The Yellow Emperor's Classic of Internal Medicine. Los Angeles: University of California Press. Vertheof, M., Scott, C., & Hilsden, R. (1998). A multi-method research study on the use of complementary therapies among patients with inflammatory bowel disease. Alternative Therapies in Health and Medicine, 4, 68-71. Vickers, A. (2000). Researching complementary medicine. British Journal of Therapy and Rehabilitation, 7(1), 26-29. Vickers, A. J., & Cassileth, B. R. (2001). Unconventional therapies for cancer and cancer-related symptoms. Lancet Oncology, 2(4), 226-232.
259
VoyDanoff, P. (2001). Conceptualizing community in the context of work and family. Community, Work & Family, 4(2), 133-156. Wang, Q. (1999). The Confucian Filial Obligation and Care for Aged Parents. In R. Fan (Ed.), Confucian Bioethics (pp. 235-256). Dordrecht: Kluwer Academic Publishers. Wang, S.-Y. C., & Yates, P. (2006). Nurses' responses to people with cancer who use complementary and alternative medicine. International Journal of Nursing Practice, 12(5), 288-294. Wang, S. Y., Yates, P., & Windsor, C. (2006). Exploring The Use of Non Western medicine By People With Cancer in Taiwan: A Ground Theory Study. Paper presented at the 14th International Conference on Cancer Nursing, September 27th – 1st October 2006, The Sheraton Centre, Toronto, Canada. Wang, C., Han, C., Hsu, T. H., Windsor, C., & Barnard, A. (2006). Translation in qualitative research: what is evidence? Paper presented at the 7th International Interdisciplinary Conference-Looking to the Future: Opportunities & Challenges for Qualitative Research, 14th - 16th July 2006 Gold Coast, Queensland, Australia. Wellman, B. (1995). Lay referral networks: Using conventional medicine and alternative therapies for low back pain. Research in the Sociology of Health Care, 12, 213-238. Whittemore, R., Chase, S. K., & Mandle, C. L. (2001). Validity in qualitative research. Qualitative Health Research, 11(4), 522-537. Whorton, J. C. (1999). The History of Complementary and Alternative Medicine. In W. B. L. Jonas, J. S. (Ed.), Essentials of Complementary and Alternative Medicine (pp. 16-30). Philadelphia: Lippincott. Wilson, H. S., & Hutchinson, S. A. (1996). Methodological Mistakes in Grounded Theory. Nursing Research, 45(2), 122-124. Wimpenny, P., & Gass, J. (2000). Interviewing in phenomenology and grounded theory: is there a difference? Journal of Advanced Nursing, 31(6), 1485-1492.

260
Woo, K. Y. (1997). The Modernization of Confucianism: A Discussion of the Cultural Change from Consanguineous Feeling to District Concern. In M. Wang & X. Yu & G. F. McLean (Eds.), Chinese Cultural Traditions and Moderization: Chinese Philosophical Studies, X (pp. 85-94). Washington, D. C.: The Council for Research in Values and Philosophy. Woodgate, R. (2000). Part 1: An introduction to conducting qualitative research in children with cancer. Journal of Pediatric Oncology Nursing, 17(4), 192-206. World Health Organization. (2001). Legal Status of Traditional Medicine and Complementary/Alternative Medicine: A Worldwide View. Geneva: World Health Organization. World Health Organization. (2002). WHO Traditional Medicine Strategy 2002-2005. Geneva: World Health Organization. Wright, L. M., Watson, W. L., & Bell, J. M. (1996). Beliefs: The heart of healing in families and illness. New York: Subsidiary of Perseus Books. Wyatt, G., & Post-White, J. (2005). Future Direction of Complementary and Alternative Medicine (CAM) Education and Research. Seminars in Oncology Nursing, 21(3), 215-224. Wysong, P. (1998). Many asthma patients using alternative medicine: conventional medicine seen as not treating the whole person. Medical Post, 34(35), 40. Yates, P. M., Beadle, G., Clavarino, A., Najman, J. M., Thomson, D., Williams, G., Kenny, L., Roberts, S., Mason, B., & Schlect, D. (1993). Patients with terminal cancer who use alternative therapies: their beliefs and practices. Sociology of Health and Illness, 15(2), 199-216. Yeager, D. M., Glei, D. A., Au, M., Lin, H.-S., Sloan, R. P., & Weinstein, M. (2006). Religious involvement and health outcomes among older persons in Taiwan. Social Science & Medicine, 63(8), 2228-2241. Yeh, C. H. (2001). Religious beliefs and practices of Taiwanese parents of pediatric patients with cancer. Cancer Nursing, 24(6), 476-482.

261
Yeo, S. S., Meiser, B., Barlow-Stewart, K., Goldstein, D., Tucker, K., & Eisenbruch, M. (2005). Understanding community beliefs of Chinese-Australians about cancer: Initial insights using an ethnographic approach. Psycho-Oncology, 14(3), 174-186. Zhang, X. (2000). Integration of traditional and complementary medicine into national health care systems. Journal of Manipulative and Physiological Therapeutics, 23(2), 139-140. References in Chinese:
Traditional Chinese Medicine Committee (2001) 中醫藥委員會 (民國 90,
2001).中醫醫療管理法規彙編.台北: 行政院衛生署。
(Traditional Chinese Medicine Committee, 2003) 中醫藥委員會 (民國 92,
2003).臺灣中醫藥整合與前瞻.台北: 行政院衛生署。
(Wang, 1990) 王廷輔 (民國 79, 1990).臺中地區居民中西醫療行為取向之研
究..公共衛生,17(1),21-33。
(Wang, 2001) 王愛慈 (民國 90, 2001).一位採信民俗療法的精神病患之護理經
驗.高雄護理雜誌,18(2),92-104。
(Chiou, 1999) 丘周萍 (民國 88, 1999) .台灣血液透析患者另類療法使用之研
究..護理研究,7(5),398-407。

262
(Department of Health Taiwan, R.O.C., 2003) 行政院衛生署 (民國92, 2003).
公共衛生年報.台北: 行政院衛生署。
(Du, 1997) 杜正勝 (民國 86, 1997).醫療、社會與文化-另類醫療史的思考.新
史學,8(4),143-171。
(Du, 1992) 杜異珍 (民國 81, 1992).文化對女性乳癌病患醫療行為之影響.榮
總護理, 9(2), 127-133。
(Xin et al., 1996) 辛隆士、邱太源、胡文郁、程劭儀、陳慶餘 (民國 85, 1996).
癌末病人之另類治療行為.中華家醫誌,6(3),127-137。
(Lin, 1992) 林文香 (民國 81, 1992).為推展護理本土化奠石—認識民間醫療行
為.榮總護理,9(2),110-116。
(Lin & Ji, 1998) 林正介、季瑋珠 (民國 87, 1998).了解民眾的醫療體系與求醫
行為: 基層醫療的礎石.基層醫訊,3(12) ,6-8。

263
(Lin et al., 1996) 林春香、劉雪娥、王正儀 (民國 85, 1996).大腸直腸癌症病患
民俗療法之採用及其相關因素之探討.長庚護理,7(3),30-45。
(Shih, 1999) 施欣欣 (民國 88, 1999).中醫學對人的詮釋.護理雜誌,46(3),
5-10。
(Hu, 1999) 胡幼慧 (民國 88, 1999).另類療法的社會空間.Hope,20,90-94。
(Hu, 1999) 胡幼慧 (民國 88, 1999).另類療者的社會空間一項田野研究的初步
分析.思與言,36(2),183-212。
(Liang et al., 2002) 梁靜祝、熊秉荃、劉芳怡、江杏珠、張美珠、陳淑卿 (民國
91, 2002).腹膜透析病患採用民俗醫療行為的分析研究.臺灣腎臟護理學會雜
誌,1(2),106-120。
(Xu, 1992) 許木柱 (民國 81, 1992).民俗醫療與醫護因應.榮總護理,9(2),
117-120。
(Chen et al., 2005) 陳玉萍、曾振淦、陳美伶、洪志宏、曾雁明、李弘暉 (民國

264
94, 2005).放射線治療之惡性腦瘤患者接受另類療法與食物觀念的調查分析.
放射治療與腫瘤學,12(1),59-65。
(Chen et al., 1999) 陳玉萍、曾雁明、曾振淦、林信吟、洪志宏 (民國 88, 1999).
放射線治療之癌患接受另類療法的調查.放射治療與腫瘤學,6,295-300。
(Chen, 2001) 陳春發 (民國 90, 2001).中醫在臺灣醫療體系的角色-以臺北市立
中醫醫院為例.北市中醫會刊雜誌,7(4) ,75-83。
(Chen, 1995) 陳郁夫 (民國84, 1995).人類的終極關懷.台北: 幼獅。
(Chen & Mao, 2001) 陳德人、毛家舲 (民國90, 2001).另類醫療在健康照顧體
系的興起與趨勢.臺灣醫界,44(9),39-41。
(Yang, 1992) 楊文山 (民國 81, 1992).臺灣地區民眾求醫行為之分析.榮總護
理,9(2),121-126。
(Cai, 1992) 蔡相輝 (民國 81, 1992).臺灣的祠祀與宗教.台北: 臺原。
265
(Teng et al., 1999) 鄧錦惠、汪忠川、吳茂賢、楊明仁 (民國 88, 1999).民眾求
助收驚治療之動機與需求研究.中華家醫誌,9(4),217-227。
(Lai, 1997) 賴明美 (民國 86, 1997).另類醫學.基層醫學,12(9) ,169-171。
(Xie, 1998) 謝正毅 (民國 87, 1998).爭取生命的契機: 走出另類療法的迷思.
常春月刊,184,172-174。
(Zhong, 2001) 鍾聿琳 (民國90, 2001).護理人員對另類醫療應有的認識.臺灣
醫學,5(3),343-347。

266
Appendix I: Participant Information Sheet
QUT
Participant Information Sheet
Title of Project: Exploring the use of non Western medicine by people with
cancer in Taiwan: a grounded theory study
Researcher: Wang, Shou-Yu (Cindy)
Phone: 002-61-7-32631097 (Australia)
(04) 26335636 (Taiwan)
I am an international student from Taiwan and enrolled in a Doctor of Philosophy
(PhD) study offered by Queensland University of Technology, Brisbane, Australia.
This project is being conducted as part of the course requirements for this degree. The
purpose of this study is to explore the use of non Western medicine by people with
cancer in Taiwan. The findings of this study may be published, however, no names or
information which could identify any individual or organization will be recorded.

267
If you agree to participate in this study, you will be asked to participate in an
interview conducted by the researcher. During the interview, you will be asked to
discuss your opinions about non Western medicine and views about using non
Western medicine.
The interview will be audio taped and may last up to one hour. The interview will be
conducted at a time and place convenient to you. You can stop the tape at any time if
you do not want the specific content to be audio taped. These tapes will be transcribed
without using any names or identifying features. Furthermore, the tapes will be erased
after the study. Only the researcher and her research supervisor (Associate Professor
Patsy Yates, Ms Carol Windsor and Associate Professor Chouh-Jiaun Lin) will have
access to this information, so that your confidentiality can be assured.
The potential benefits of this study are an increased understanding about cancer
patients’ uses of non Western medicine. This may assist in developing health care
professionals’ understanding of how they can more effectively care for patients with
cancer.
There are no known risks associated with beings involved in this study. If any

268
problems or concerns arise during the study, the researcher can refer you to
appropriate sources of help. If you experience any distress as a result of participation
in this project, you can contact the Hospital Counselling service on (04)
26625111-2152 (Kuang Tain Hospital), (04) 2205 2121-4252 (China Medical College
Hospital) for assistance, free of charge. In addition, you also can contact the
researcher if you have any questions about the project, or the Secretary of the QUT
Human Research Ethics Committee on 002-61-7-3864 2902 if you have concerns
about the ethical conduct of the project.

269
昆士蘭科技大學 研究說明
研究主題 臺灣地區癌症病人使用非西醫療法之探討:紮根理論研究
研究者 王守玉
電話 (04) 26335636
本人目前於澳洲布理斯本昆士蘭科技大學進修博士班課程, 此項研究計劃是本
人之博士論文主題, 此項研究計劃的目的在於探討臺灣地區癌症病人使用非
西醫療法的過程。此研究結果也許刊登於期刊或出版,但將不會出現任何名字或
機構名稱。
如果您同意參與此項研究,您將參與一次與研究者的會談。在會談當中,您將被
問及您對使用非西醫療法的看法和使用它們的觀感。會談將持續最長一小時,且
將進行錄音,會談會在您覺得方便的時間及地點舉行。當任何會談內容您不想被
錄音時,您可以隨時按下錄音停止鍵;在不提及名字的前提下,這些錄音帶的內
容將被謄寫下來作為資料分析之用。而在研究結束後這些錄音帶資料將被消除,
且在研究計畫過程中,只有研究者及其指導教授會接觸這些資料,因此您的個人

270
資料絕對保密。這項研究將有助於增加了解癌症病人使用非西醫療法的過程,
同時有助於醫療專業人員了解如何更加有效率的照顧癌症病人。
參與本研究目前沒有已知的危險,如果在參與本研究期間有任何問題發生,研究
者將會轉介您到適當的單位尋求幫助。如果您因參與本研究而導致苦惱或情緒低
潮, 您可免費聯絡光田醫院社工室,電話: (04) 26625111-2152, 或中國醫藥大
學附設醫院社工室, 電話: (04) 2205 2121-4252, 尋求協助。此外,如果您對此
研究有任何問題,您可聯絡研究者。再者,如果您對此研究有任何倫理上的問題,
您可聯絡昆士蘭科技大學倫理委員會秘書室,電話: 002-61-7-3864 2902。

271
Appendix II: Consent Form
QUT
Consent Form
Title of Project: Exploring the use of non Western medicine by people with
cancer in Taiwan: a grounded theory study
Researcher: Wang, Shou-Yu (Cindy)
Phone: 002-61-7-32631097 (Australia)
(04) 26335636 (Taiwan)
I agree to participate in Miss Wang, Shou-Yu’s (Cindy) research project entitled
“Exploring the use of non Western medicine by people with cancer in Taiwan: a
grounded theory study”.
By signing below, I am indicating that I:
• have read and understood the information sheet about this project;

272
• have had any questions answered to my satisfaction;
• understand that if I have any additional questions I can contact the researcher;
• understand that I am free to withdraw at any time, without penalty or comment;
• understand that I can contact the researcher if I have any questions about the project,
or the Secretary of the University Human Research Ethics Committee on 002-61-3864
2340 or [email protected] if I have concerns about the ethical conduct of the
project;
• if I experience any distress as a result of my participation in this project, I can
contact the Hospital Counselling service on (04) 2662 5111-2152 (Kuang Tain
Hospital), (04) 2205 2121-4252 (China Medical College Hospital) for assistance, free
of charge; and
• agree to participate in this project.
Name:
Signature:
Date:

273
昆士蘭科技大學 同意書
研究主題 臺灣地區癌症病人使用非西醫療法之探討:紮根理論研究
研究者 王守玉
電話 (04) 2633 5636
本人同意參與王守玉小姐之研究計畫 (研究主題 臺灣地區癌症病人使用非西
醫療法之探討:紮根理論研究) 。
簽署此同意書時,本人已經
∗ 閱讀並了解此研究之說明;
∗ 問及相關問題並獲得滿意答覆;
∗ 了解如果有其它問題, 本人可聯絡研究者,
∗ 了解可在任何時間無條件下退出此研究計畫,
∗ 了解如果對此研究有任何問題, 本人可聯絡研究者,
∗ 知道如果對此研究有任何倫理上的問題,本人可聯絡昆士蘭科技大學倫理委員
會秘書室,電話: 002-61-7-3864 2340 或 [email protected];

274
∗ 獲知如果因參與本研究而導致苦惱或情緒低潮,本人可免費聯絡光田醫院社工
室,電話: (04) 26625111-2152, 或中國醫藥大學附設醫院社工室, 電話: (04)
2205 2121-4252, 尋求協助;
∗ 同意參與此研究計畫。
姓名 _________________________
簽名 _________________________
日期 _________________________

275
Appendix III: The Interview Theme List
The Interview Theme List
1. History of cancer patients use of non Western medicine.
∗ Could you describe your history of using non Western medicine?
∗ Could you talk about the role of non Western medicine in your daily life?
∗ Could you talk about the non Western medicine you use?
2. The relationships between non Western medicine and cancer treatments.
∗ Could you talk about the relationship between non Western medicine and
other cancer treatment?
3. Associated events around the treatments of cancer
∗ Could you talk about what affect your decisions to use non Western
medicine?
4. Is there anything else that you think is important to understanding your experiences
of using non Western medicine during the treatment of cancer that we have not
discussed?

276
會談主題
1. 癌症病人使用非西醫療法的歷程。
∗ 您能談您使用非西醫療法的歷史嗎?
∗ 您能談一下非西醫療法在您日常生活中的角色嗎?
∗ 您能談一下您所使用的非西醫療法嗎?
2. 癌症治療與非西醫療法之間的關係。
∗ 您能說一下您決定使用非西醫療法的過程嗎?
∗ 您能談一下非西醫療法與您所使用的其它癌症治療之間的關係嗎?
∗ 您能聊一下非西醫療法與您在克服及對付癌症之間的關係嗎?
3. 與癌症治療相關的事項。
∗ 您能說一下什麼會影響您使用非西醫療法的決定嗎?
4. 有任何事件是您覺得在您癌 症 治 療 及 了 解 您使用非西醫療法時是重要的,
但我們並沒有談到的嗎?





























