Embed Size (px)
Citation preview

Taiho Oncology
A presentation by Now What
Metastatic
Colorectal Cancer:
The mCRC Patient Journey
DEC 8, 2014
Workshop Agenda
Breakfast + Introductions
Insights Deck + Journey Share-out
Journey Discussion
Lunch
Ideation Session + Breakout Groups
Winning Worksheets
8:30-9:00
9:00-11:30
11:30-12:00
12:00-12:30
12:30-2:30
2:30-3:00
2
3
Contents
Background
I
Overarching
Insights
II III
Patient
Profiles
IV
Journey
V
Now What:
Ideation

overview of project goals, methodology, and
sample
I
Background

5
Illuminate the patient journey from a functional and emotional perspective, delving
into what it’s like to live with metastatic colorectal cancer.
Explore the barriers for 3rd and 4th line treatment initiation – from a functional,
physiological, and emotional perspective.
Identify the barriers for 3rd and 4th line treatment compliance and strategic solutions for
overcoming said barriers.
Generate a series of support and/or adherence ideas to help for a more successful
mCRC patient experience.
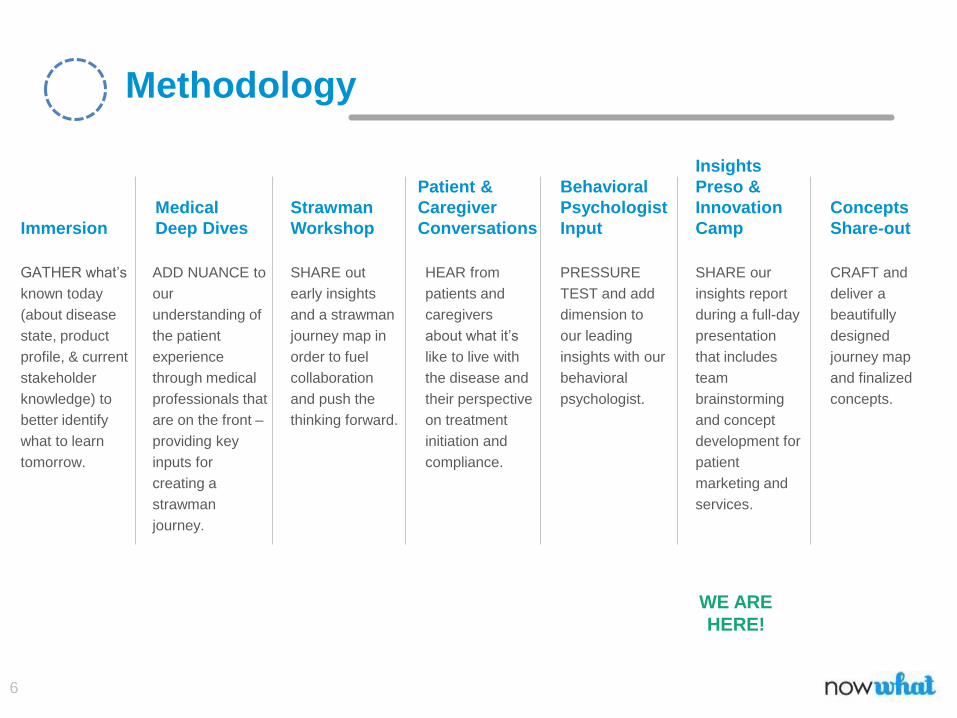
The Project Goals
6
GATHER what’s
known today
(about disease
state, product
profile, & current
stakeholder
knowledge) to
better identify
what to learn
tomorrow.
Immersion
ADD NUANCE to
our
understanding of
the patient
experience
through medical
professionals that
are on the front –
providing key
inputs for
creating a
strawman
journey.
Medical
Deep Dives
Methodology
SHARE out
early insights
and a strawman
journey map in
order to fuel
collaboration
and push the
thinking forward.
Strawman
Workshop
HEAR from
patients and
caregivers
about what it’s
like to live with
the disease and
their perspective
on treatment
initiation and
compliance.
Patient &
Caregiver
Conversations
PRESSURE
TEST and add
dimension to
our leading
insights with our
behavioral
psychologist.
Behavioral
Psychologist
Input
SHARE our
insights report
during a full-day
presentation
that includes
team
brainstorming
and concept
development for
patient
marketing and
services.
Insights
Preso &
Innovation
Camp
CRAFT and
deliver a
beautifully
designed
journey map
and finalized
concepts.
Concepts
Share-out
WE ARE
HERE!

II
Overarching Insights4 key truths about the mCRC patient experience

8
3
mCRC changes you
While each mCRC patient is unique, there are some key
commonalities among patients. There are unique
behaviors and values that set these individuals apart from
‘normal’ people. These attributes are integral to how they
operate throughout their life with cancer, and are not
specific to any point in the journey.

9
We rely on our bodies to be strong, to protect us, to allow us to live life the way we so desire. Being
diagnosed with cancer changes the way these individuals interact with their bodies. While they were
once able to rely on their body for strength, it now feels as if their body has let them down. Cancer is
seen as an intruder, taking over what was once theirs. They feel betrayed by the one thing that’s
supposed to protect them.
Betrayed by their own body
“I got diagnosed at 45 and prior to that I
was the epitome of health…160 lbs.,
5’10’’ and all my blood work was A+. I
had never really been sick.”
– Robert F
“I never had any real symptoms. I never
had blood in my stool and there were
only a few times I felt nauseous. I ran a
5K, and thought that was where my
fatigue was coming from.”
– Tiffany

10
Not all cancers are equal when it comes to what you can and can’t talk about. These patients often
feel uncomfortable openly speaking about their colon and rectum, a topic not typically discussed with
others. This makes it difficult for patients to open up to others about their symptoms, both pre- and
post-diagnosis.
Holding this in can put added emotional pressure on patients. When they need support most, they
are more concerned with stigma than opening up about this life-altering experience. This can lead
many to feel isolated and alone in their fight.
It’s not easy to talk about ‘down there’
“Since cancer, I have become much
more of an introvert. I don’t want to be
around people. I go to a weekly support
group. That is my ‘people infusion.’”
– Jeanne
“It was so taboo to talk about your butt
and your bowel movements, so I didn’t
tell anyone because I was embarrassed.
It was not acceptable for women to have
colon cancer.”
– Fran
11
As humans, we gain strength and security from the feeling of power we have over our lives. We take
for granted the ability to do seemingly simply things that enhance this sense of powerfulness. But
cancer takes this feeling away, leaving patients feeling powerless to control their illness. Previously
independent individuals are no longer in control of many other aspects of their life, as well. Side
effects, symptoms, diminished health and energy all threaten their ability to regain power. They thus
seek to gain their power back in different, seemingly insignificant ways. Being in charge of taking their
medication, doing things on their own, caring for others, and contributing to the family are all small
ways that patients seek to tip the scale of power back in their favor.
Losing their power
“At one point, I went through a
depression phase. I wasn’t working
and felt like I couldn’t help out my
family. I felt like a failure. But I help
my children out in my own way, like
with their homework, so they feel
like they can depend on me.”
– George
“I lost the person I was. I always
wanted to be in control – with work,
my home life, my family – and I don’t
feel like that person anymore. I feel
less confident, less sure. The most
confident I feel is when my husband
is with me.”
– Tammi
12
Regardless of segment type or whether the patient is still on or has made the decision to stop
treatment, a glimmer of hope is always there. No matter how realistic about their situation, every
patient leaves the possibility open for a cure, ‘miracle’ or even just a little more time, even when they
have been given no probable reason to expect it.
It is this glimmer of possibility that gets them through, that sustains them. Hope, however minimal,
allows patients to endure through the suffering, pain, and sadness of fighting cancer.
Pervasive hope
“The doctor’s view is that he has had
other patients like me that have lasted
15-17 years, and there are times that
the drugs that stopped working start
working again and you can go back to
them. And there are other drugs that
we haven’t tried. I’m not willing to give
up yet.”
– Steven
“The central hubs of support are my
children and wife. If I have just a little
longer, I can see my daughter walk at
graduation. I marked the date on my
calendar…I Google Colon Cancer
articles every morning…and I just hope I
live long enough to find the silver bullet,
the one that cures me.”
– Robert F
III
Psychographic
SegmentationUnderstanding the different mCRC patient personas
14
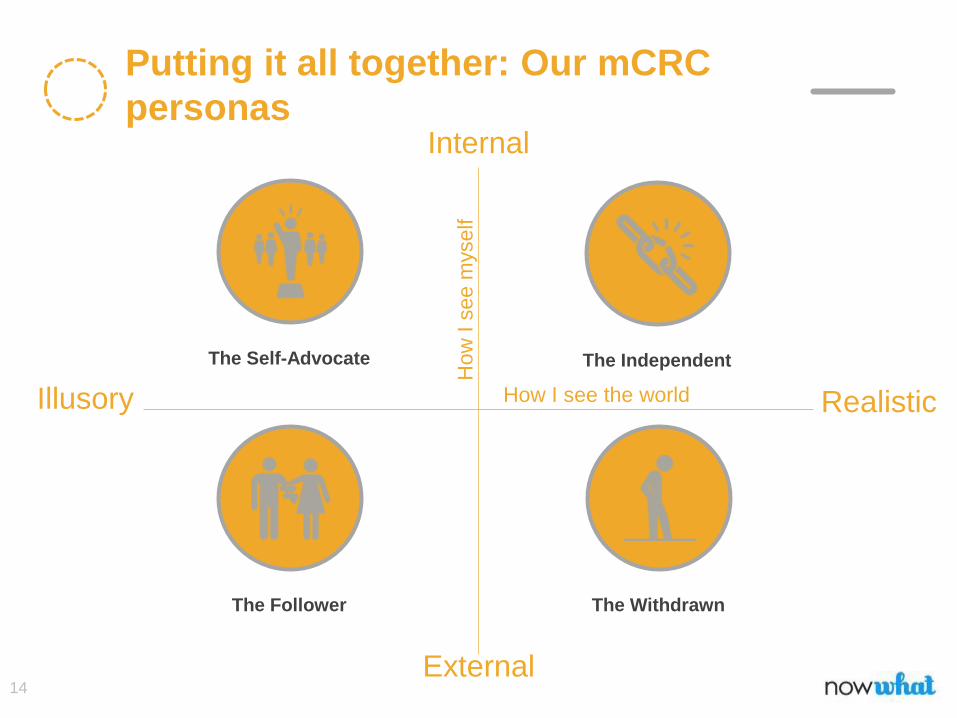
Putting it all together: Our mCRC
personas
The Independent
The WithdrawnThe Follower
The Self-Advocate
How
I s
ee m
yself
How I see the world
Internal
External
Illusory Realistic

Meet the Self-Advocates
I never thought I was an optimist, but when mortality stares you in the face it’s not worth
it to feel bad for yourself. I feel really lucky that I’ve survived this long. People use the
word ‘cancer survivor’ but I see myself more as a fighter. When it comes to treatment I
can always keep going, I’m willing to try anything if it might work. Having cancer has also
affected my relationships with other people, it’s made me a warmer person, with a
greater appreciation for the world.
ILLUSORY
INTERNAL
REALISTIC
EXTERNAL
“
“
On the Spectrum
Information Needs
Self-concept
Internal + Illusory
Outlook on Future
Relationship with Oncologist
Self-Advocates have a self-enhancing outlook on life
that makes them well equipped to fight. They view the
world with rose-colored glasses and feel confident
that they can be the exception to the rule and beat the
odds. They are driven by self-power.
This persona is optimistic about their options,
always holding out hope for a breakthrough or a
cure. Their goals for treatment are always to
either shrink or cure their cancer and they are
willing to do whatever it takes to get there.
“I have cancer, but I ultimately control what my
life looks like.”
Self-Advocates trust mainly in themselves, but
do see their doctor as a valued partner in their
treatment. A trusting relationship is important
to them, so they will switch doctors if they feel
like it’s not a good fit.
Constantly
researching to
find a cure or a
miracle.
Support Needs
Find the support
they need in
themselves.
Outlook on Cancer
Fighting Mentality
THE SELF-
ADVOCATE

Meet the Independents
Success for me means normalcy – being able to continue living the life I want, on my terms. The
goal is to live for as long as possible, as comfortable as possible. I’m pretty matter of fact about
my cancer, which can put some people off, I guess. But I’m the one in charge of my treatment,
only I know what’s best for my body. I refuse to be cattled. This is my life and I’m going to live it
on my terms. People shouldn’t be scared to have a voice – don’t let anyone push you into
anything you don’t agree with.
ILLUSORY
REALISTIC
THE
INDEPENDENT
“
“
On the Spectrum
Information Needs
Self-concept
Internal + Realistic
Outlook on Future
Relationship with Oncologist
Independents are strong and aren’t afraid to fight – but
they are also realistic. Their main focus is doing what’s
right for them, and coping by finding ways to feel
powerful. It’s very important for them to do things on their
terms to reaffirm their sense of self.
This persona is realistic about their future, and see
themselves as the rule, not the exception. They know that
death is on the horizon, but hope to maintain a sense of
normalcy and control until that time. It is important to enjoy
the time they have left.
“I have cancer, but I won’t let it take my dignity or
quality of life.”
Independents like to to be the one to call the shots.
They trust in themselves, not the oncologist, to
know what’s personally right for them. They are
focused on doing what’s best for their body, but
also for their mind and lifestyle.
Avid researchers
to stay updated
on their chances.
Support Needs
Support themselves
by trusting their
body.
Outlook on Cancer
Fighting Mentality
INTERNAL
EXTERNAL

Meet the Followers
Getting the diagnosis came as a serious blow to my family and I, but we overcame by becoming
more spiritual. Having cancer has changed every aspect of my life, but not all for the bad. I feel
very blessed because I’ve been able to learn more about myself and who my real friends are. I
try to appreciate everything I have, including my doctor who guides me. I trust what he tells me,
and simply trust that god isn’t done with me yet. I have more to do here on earth.
ILLUSORY
REALISTIC
“
“
On the Spectrum
Information Needs
Self-concept
External + Illusory
Outlook on Future
Relationship with Oncologist
Followers gain strength from their faith (whether in
religion or just spirituality), believing that there is a
reason why they have cancer. They see their fight as
a positive influence on their life, teaching them how to
be a better person and live life to the fullest.
When looking to the future, Followers hold out
hope for a cure, but trust that everything will
work out as it should. They believe that their faith
will protect them, and that there is a plan for their
life. They view the future in a positive light.
“Cancer has taken over my life, but it’s made me
a better person.”
Followers trust in their oncologist to guide them in
their treatment. They need someone else to lead
them, and will typically follow anything the doctor
says, unless they are told they our out of options –
then they will find a new doctor whose outlook
matches up more accurately with theirs.
They will research
what their doctor
prescribes them.
Support Needs
Rely on friends,
family, and doctor
for support.
Outlook on Cancer
Fighting Mentality
THE
FOLLOWER
INTERNAL
EXTERNAL

Meet the Withdrawns
I know where this leads, so I don’t get my hopes up. My husband tries not to talk too much about
my cancer, because he knows I’ll worry about it if he does – I tend to worry a lot about things. I
need someone to talk to, but support groups often make me sad. My doctor helps me a lot, as
someone to talk to and also to tell me what to do. I don’t do much research on my own because I
read something once that said I wouldn’t live more than 5 years. That got me worked up and I
don’t want to be filled with all of that fear and anxiety so I take my doctors word for it when he
tells me what to do.
ILLUSORY
REALISTIC
“
“
On the Spectrum
Information Needs
Self-concept
External + Realistic
Outlook on Future
Relationship with Oncologist
Their vision of the future is rather bleak, as they
know it’s just a matter of time. They see
themselves as the rule, and feel like they are not
in control of their own lives. Their goals are
rather small and within their realm of control.
“Cancer has taken over my life and I am
powerless against it.”
Withdrawns put a lot of stock in what their
oncologist says, and will blindly follow their
lead. Their oncologist keeps them fighting, but
when options run out this persona isn’t likely
to keep looking for new ones.
Generally withdrawn
from info sourcing, rely
predominantly on
doctor for information.
Support Needs
Generally come off
as very needy, thus
often have trouble
finding true support.
Outlook on Cancer
Fighting Mentality
THE
WITHDRAWN
INTERNAL
EXTERNAL
Withdrawns pull their strength from those around
them. They feel like they are powerless to
control their cancer, and realistically know what
the future holds. They often use avoidance to
cope, as the reality of their situation can be
overwhelming.

Meet the Caregivers
I never thought I would hear the word cancer. I had to stay strong, but I was dying inside. I try to
take things one day at a time because being a caregiver means being there 24/7. I have to be
the one to know what to do in any situation and there’s no time for emotions. I wish there was a
class on how to be a caregiver, how to treat them, how to treat the situation. There isn’t a lot of
information out there. But we’ve had a good life. I know what’s going to happen and that I’m
going to be alone. I only hope that when it comes I’ll know how to face it.
“
“
Support Needs
Information Needs
Outlook on Future
Relationship with Oncologist
Caregivers must face a future without their loved one
– a future alone. They understand that this will be
their reality, but have no way to navigate what this will
look like or how they will bear it. Caregivers fear what
this will be like, but rarely talk about it.
“Cancer has changed everything about my life,
but I don’t even have it.”
They must have a relationship with the doctor,
as well. In the oncologist’s office, caregivers
often have to be the one to take notes and ask
logistical questions, all while also processing
potentially heartbreaking news.
Caregivers are often
active researchers,
often taking over when
patients are weak.
Support Given
See themselves as the
sole supporter of
patients, bearing the
weight of their struggle.
Outlook on Cancer
Fighting Mentality
While not physically suffering from the illness, the CG’s
whole life revolves around the fight against cancer.
They fight by supporting their loved one, taking sole
responsibility of the household, providing for the family,
and keeping everyone together.
Caregivers take on a lot when their loved one is
diagnosed with cancer, and get little support in
return. They take on additional responsibility and
often feel like they’re carrying the burden of their
loved one’s care. All of this, without much in return.
They crave support in the following ways:
• An escape from cancer, a moment to
feel normal again
• Time to process their own feelings
• Information about how to give care
• Help in the day-to-day struggle
• A way to map a new course in the
future – both emotionally and logistically
IV
Journey in DetailExploring key moments in the emotional journey

21
A note on the journey
Just as every individual with mCRC is unique, so too is
their journey. While the story we tell in the following
slides is true to the overarching patient experience, it
should be noted that there are many opportunities for
difference, depending on the individual. At any point in
the journey, a patient could opt for radiation, need
surgery, or decide to stop treatment. That being said,
most individuals travel the path we’ve laid out in the
following slides.
Pre-DiagnosisTreatment Moments that Matter

“In 2006, I began noticing a change in my bowel habits, but I always attributed it to not eating very well. My doctor treated me with prescription iron for a year, but I had reoccurring hemorrhoids. I woke up tired, came home tired, and had uncontrollable gas and diarrhea. I began eating ice more than food, which my doctor just laughed at. My stomach was killing me, but he thought maybe it was just IBS and referred me to a gastroenterologist, who then scheduled a colonoscopy and took a biopsy. I called the 24-hour nurse line, who told me to go to an oncologist.”
– Fran
Patient Spotlight: Pre-diagnosis
24
Whether they had been declared cancer-free from their first
diagnosis, or not diagnosed previously, these individuals are
bright-eyed and able-bodied, thriving in their professional
and personal lives, spending time with the people they love
the most.
Though gradually they begin to experience symptoms like
rectal bleeding, abdominal pain, or constipation.
They push it to the side as a minor discomfort and self-treat
with over-the-counter medicine, diet changes, and
supplements. Active and confident, they don’t take the pain
as a serious threat to their health.
PRE-DIAGNOSIS
DISMISSIVEas symptoms appear in an
otherwise healthy individual
1
“I told my coworker how my stomach wasn’t feeling right, and she recommended Metamucil, so I took her up on that advice because it was so casual.”
– Michelle

25
With their self-treatment providing no relief, all the
abnormalities in their body steadily pile up without leave,
and they seek to find the root of the cause.
They go to their PCP, or even the ER if the pain becomes
unbearable, but they are sent off with a minor diagnosis
that misses the true culprit. As the sickness fails to
subside, they are confused by their bodies and know that
something is still not right.
PRE-DIAGNOSIS:
PERPLEXEDas they seek medical attention
“I had total blockage and hadn’t used the bathroom for weeks. I couldn’t putthe key in the door because my stomach hurt so bad. I went to the ER andthey sent me home with a diagnosis of constipation.”
– George
1

26
Due to the persistent digestive issues they experience, they
visit their general practitioner again who turns the red flags
over to a gastroenterologist.
Their gastroenterologist tells them their pain could be a
warning sign for a more serious problem and schedule a
colonoscopy to evaluate the inside of their colon.
PRE-DIAGNOSIS
CONCERNEDas they are referred to a
gastroenterologist
1
“My doctor said I was clotting and looked like he saw a ghost when herealized where it was coming from. The next day I had my firstcolonoscopy. When you’re at a [gastroenterologist’s] office, you’re not surewhat’s going to happen.”
– Michelle
27
The results can take anywhere from a couple days to a
few weeks depending on the doctor, but no time is soon
enough as they are antsy for answers.
Having spent months frantically running between
physicians, specialists, and even the ER, they desperately
want to get to the bottom of it all so they can treat what
they have and move on.
PRE-DIAGNOSIS:
ANXIOUSas they wait on results to finally
solve the mystery
“The ER tech said that maybe it was from having a uterus bleed. I knew thatwasn’t the case.”
– Michelle
1

28
Following the colonoscopy, the gastroenterologist refers
the patient to an oncologist without giving any official
diagnosis. However, the patient understand the implication
of the reference, and fears that horrible news may be on
the way.
PRE-DIAGNOSIS:
DREADwhen the doctor sends them to
an oncologist
“The GI came into the recovery room and told me I had an obstructive tumorthat needs to be surgically removed, with recovery being 4-6 weeks. He knewcertainly that I had cancer. “
– Jeanne
1

Diagnosis &
Treatment
Conversation
Treatment Moments that Matter
“I’m married with two kids, and it was not anything we had expected. There was no family history, just rectal bleeding that went on for 3-4 months. After the colonoscopy, I woke up with them telling me I had colon cancer. It was stage 4 right off the bat. It was a very emotional time and I just shut everything out. I had very scary thoughts about if I were going to die, the fear of the unknown. It put a huge strain on my marriage, work life, and kids. It was challenging from every aspect.”
– Jeanne
Patient Spotlight: Diagnosis
31
DIAGNOSIS
NUMB AND WITHDRAWNas the doctor delivers the diagnosis
“When I was diagnosed, I felt very numb and my mind shut down. I didn’tcry very much. My daughter and my pastor were with me when thishappened.”
– Tiffany
2
As they sit in the doctor’s office with their loved one awaiting the results, they have no idea what will come next. As the words “you have cancer” leave the doctor’s lips, all other words disappear and a temporary deafness takes over. Those three terrible words are all they can hear, playing over and over in their head like a broken record. Paralyzed by shock, they disconnect and disappear into themselves.
Luckily, their loved one tunes in when they tune out, and thus begins their role as the caregiver. Not being the one diagnosed means they aren’t directly affected. So although they are deeply concerned, they remain level-headed enough to absorb the information the doctor delivers. They become the eyes and the ears, and what the patient might miss, the caregiver picks up.
32
DIAGNOSIS
ANGRY AND HEARTBROKENas reality sets in
2
Hoping for a case closed, this is just the beginning. But they weren’t ready for this – they have children to raise, spouses to grow old with, and an entire world to see. After the disbelief passes and the facts processed, their emotions awaken to the life-shattering truth: this will change everything. Furious, they refuse to accept this as their new reality, but as it processes, their anger rapidly turns to deep despair.
“This is not what I planned. Cancer was never part of my plans. It was heartbreaking. Everything in life was going so perfect. I worked an amazing job, just finished school…and then they said I had stage 4 cancer.”
– Kathy
33
While everybody knows they have metastatic colorectal
cancer, there are varying perspectives on how it affects their
life expectancy.
Some believe that metastatic is a death sentence, the last
step before cancer completely takes over your body and
shuts you down.
Others view it as controllable; the tumors have spread to
other organs in your body, but you still have the ability to
shrink or maintain its size.
DIAGNOSIS
TENSION conflicting definitions of metastatic
2
“Metastatic - I had never heard that word before. I learned that this meant I was at stage 4…typically an individual with stage 4 cancer will live a maximum of two years and that’s it .”
– Michael
The more realistic segments may see it
more as a death sentence, knowing how
serious it is.
For the illusory segments, they likely see it
as controllable and maintain hope for the
best.
Segment Shift:

34
DIAGNOSIS
OVERWHELMEDby the urgency of treatment and
information overload
2
Following a lengthy diagnosis conversation, patients are typically scheduled for immediate surgery and/or chemotherapy within the same week or even the same day.
Only moments ago they were informed of their new existence as a cancer patient. Just when they try to take a breath and absorb the blow, the doctors throw even more new information their way, pulling their emotions in multiple directions without any time to process. Dizzied and shaken by all the sudden demands, everything is changing too fast, too soon.
“I could barely spell cancer before my diagnosis and suddenly everybodyis telling me all the things I need to do because my life depends on it,and that it has metastasized to my liver and lungs.”
– Robert F
35
If the doctor predicts short life expectancy and advises the
patient to “get their affairs in order,” they will end the
relationship there. Presenting death as the only choice from
the get-go implies a lack of determination and an inability to
extend their survival.
Insulted by their complacency, they are furious, aggravated,
and completely deny death. Instead, they seek out
somebody who can help them construct a brighter future, a
doctor with a fighting spirit who will lift them up and deliver
them a positive outlook and treatment options they need to
make it through. Patients do not want to put their lives in the
hands of someone who delivers the diagnosis as a death
sentence.
DIAGNOSIS
APPALLEDby the doctor’s acceptance of
their death
2
“When I heard about needing to ‘get my affairs in order,’ I did not want that to happen. The doctor was too laid back for me, as if he could only get me so far. He already had in his mind that I could only make it two to two and half years, which wasn’t good enough for me. I said, ‘doctor, I beg to differ!’ I wasn’t even 50.”
– Theresa
The Withdrawn may not have the strength to switch
doctors, even though staying with this type of physician
may lead them to become depressed.
Segment Shift:
36
DIAGNOSIS
CONFUSEDby the lack of information for long-
term living
2
The conversation between the doctor and the patient focuses solely on their diagnosis and immediate next course of action. What it does not cover, however, is the disease as a whole, from the progression of symptoms to treatment side effects to the scientific breakdown of what is happening. Receiving that kind of explanation from the doctor is vital to both the mental and physical well-being of the patient because it provides them with the reassurance they need to not only prevent death, but also live with it long-term.
At this point, they realize that it will be affecting their entire life trajectory, but they do not understand how. A more well-rounded education could have better prepared their transition from thriving to surviving.
“For those living with ‘chronic cancer’ there is a lifetime limit on how much chemo you could have. What are the things you can look forward to? What’s missing is a real understanding of how to live with cancer long-term.”
– Jeanne
The Withdrawn can only handle so much information at
once, so it may be better for them to take their fight step
by step, without too much information about the future.
Segment Shift:

37
DIAGNOSIS
PANICKEDas research reveals a bleak outlook
2
Shortly after the terminal diagnosis, Googlemania ensues. Thirsty for knowledge, the patient hysterically researches all things mCRC and realize the internet is not their friend. Massive amounts of research say they have less than five years to live, and a wave of panic washes over them as they come face to face with statistics that read “the end is near.”
“My friend who had cancer told me not to go online and read the statistics because they are about people who are older and don’t apply to me. When I researched, my anxiety went through the roof… plus there are threads about certain medications that show very few people who have had decent results.”
– Tammi
The Withdrawn do much less research on the internet
than other segments, they typically trust that their doctor
will provide them with the information they need.
Segment Shift:

SurgeryTreatment Moments that Matter

Patient Spotlight: Surgery
“After the colonoscopy, I had my operation. I told the surgeon prior that I wanted everything out of me. I didn’t want this disease to consume me. So he took the right side of my liver out, 8 inches of my colon out, and part of my rectum…Since I trusted the surgeon, I thought I was going to come out clean. The surgeon said he took out 12 lymph nodes but only 3 were positive – if only one was positive you wouldn’t need chemo. That depressed me. I was looking for 100%.”
– Michael

40
DIAGNOSTIC SURGERY: aka a colonoscopy, involves examining the inside of the colon through the insertion of a long, thin tube with a video camera at the end. The doctor can perform a biopsy and remove any visible polyps. This happens before Diagnosis.
RESECTIVE SURGERY: occurs anywhere between 1st and 4th
line. • Colectomy: involves removal of the cancerous portion of
the colon and nearby lymph node, and the two ends are joined back together. Sometimes, if they cannot reconnect the intestine a colostomy is performed, and they are given a stoma that comes out of their stomachs and leads to a bag where bowel movements are collected.
• Liver Resection: removes the cancerous part of the liver• Lung Resection: removes the cancerous part of the lungs
SURGERY TO RELIEVE A BOWEL OBSTRUCTION: removes the blocked section of the bowel. Most people will have a temporary or permanent stoma after this.
SURGERY
TYPES OF SURGERY3
41
As a very targeted plan of action, patients view surgery as the light at the end of the tunnel and a potentially curative solution to their problems. For a moment their panic ceases and their spirits lift as they begin to believe everything might just be okay. They hold onto the belief that removing the tumor means removing the cancer and are thrilled at the chance to resume their normal lives. Going into surgery, the excitement level is high, and the notion is that it is all easy from here on out.
PRE-SURGERY
OPTIMISTICwhen they meet with their
surgical oncologist
3
“Coming up to surgery, I was looking for a cure. It looked like it was doable for me. It was one little lymph node….the surgeons I met said they do this sort of thing all the time. “
– Sue
The realistic segments may not be as
optimistic before going into surgery, having a
better understanding of what could happen.
Segment Shift:
42
The smooth sailing they expected has come to a screeching halt. Anticipating complete removal of cancer, they are deeply disappointed that the surgeon was incapable of fixing them.
Nonetheless, they are forced to adapt and pursue another avenue of treatment. Their curative dreams are crushed.
POST-SURGERY
CRUSHEDwhen the surgery did not rid them of
cancer
3
“You think maybe you can get rid of the tumor in your lung with surgery, but then you realize they can’t get rid of everything. Surgery is a life extender, but it isn’t a cure. And I can’t do it anymore because it will affect my breathing and diminish the quality of my life.”
– Nathan
43
Typically following the procedure, patients stay in the hospital between 2-8 days, depending on how they heal. Many have complained of prolonged stays due to infections, ileus (paralysis of the intestines), incomplete healing where the lung has been removed, heart problems or blood clots.
When they return home, they commonly experience chronic fatigue, severe abdominal pain, sexual dysfunction, nausea, and fecal incontinence.
It can take anywhere between 4-6 weeks before they can return back to their normal lives.
Caregivers play a critical role in the healing process, acting like an in-home nurse as they tend to the patient’s wounds and rehabilitation process. However, as the patient forms an overdependence, the caregiver’s life shifts to revolve around their loved one rather than themselves.
SURGERY
TRAUMATIZED by the recovery period
3
“I thought I was dying that night. I was not supposed to have any blood transfusions and felt very light-headed. I spent a week in the hospital recovering. The recovery was rough. I went from being an athlete to not being able to get my mail.”
– Emily

First Line
Treatment Moments that Matter
“Chemotherapy sounded so terrible with the side effects. It was really scary because you just don’t know what to expect. But the nurses were great and really baby you the first time you are there.”
– Jeanne
Patient Spotlight: 1st Line
46
Since the patient is still a complete novice to medical treatments for mCRC, they put total faith in the doctor’s orders without much question. The doctor prescribes them the traditional first line of therapy and goes “by the book”, leading the treatment decision at this point as the patient follows his orders.
FIRST LINE
TRUSTING AND OPENbecause of a proven process
4
“Xeloda was the only option. My trusted doctor said ‘You are young and we have high success rates with this. You are a great candidate.’”
– Robert F

47
As they venture into unchartered territory, their pre-conceived notions of chemotherapy guide their imagination towards the worst case scenario. However, as they approach with great trepidation they also approach with great optimism, for this could be all they need to keep the cancer at bay. Fingers crossed, their hopes are high.
FIRST LINE
SCARED BUT HOPEFULas they approach chemotherapy
4
“I did a training session and they told me what the side effects were going to be. Leading up to it, I was scared, but I wanted it to start it because it was going to actively fighting the cancer.”
– Tiffany

48
The first four cycles of chemotherapy are rough. Patients experiences include flu-like symptoms, diarrhea, nausea, and fatigue. Yet, over time their bodies begin to adjust and the bad days aren’t as often as before. There is finally a calm after the storm.
FIRST LINE
RELIEVEDas reactions to chemotherapy
improve with time
4
“My biggest fear was that I was going to be deathly sick after therapy…Over time, I realized I wasn’t going to throw up and the drugs to counteract the side effects worked. I was very positive.”
– Karen
49
Having cancer is a full-time job. Suddenly all the once seamless facets in their lives are layered with friction, and they are constantly forced to factor mCRC into every decision.
They lose the ability to go on vacations at their leisure at the risk of missing chemotherapy. They aren’t as productive at work as they used to be. Going out with friends puts them at risk for getting sick in public and ruining all the fun. Even simple tasks like opening a jar become too difficult. Their placement of time and energy is very sensitive. Chemotherapy takes precedence over everything in their life.
This is a period of adaptation, and it is a difficult transition.
FIRST LINE
ADJUSTING to their new normal
4
“As chemo went through my system, I started losing my sharpness. I was less aggressive with contractors in getting the best prices, and everything began slowing down for me. This was something I never experienced, so I needed to think on my feet.”
– Michael

50
In order to evaluate the efficacy of therapy, the oncologist conducts a scan (MRI, CAT, PET, Liver) to produce a picture of the patient’s body showing if the tumors have spread or shrunk.
The scan itself is a simple enough process, but it’s the waiting process that feels most difficult. Being told they have stage 4 colorectal cancer was traumatizing enough, so another round of bad news may be too much to handle.
FIRST LINE
NERVOUSas they await their scan results
4
“It was nerve-wrecking and pretty difficult to have the prospect [of more cancer] in my face, but I tried to turn the wipers on as best as I could”. – Sue

Second Line
Treatment Moments that Matter
“The doctor decided to do a scan every 3 months. I was inremission, but really stage 4 cancer never takes a break, it justtakes a nap and comes back. Two years later I discovered itwas metastatic to my lungs, so I did Folfiri. It was pretty similarto 1st line. The sessions were the same, only the drugs changed.I knew what to expect…I had done it before, tolerated it wellthe first time, and had no reason to fear it wouldn’t go well thesecond time.”
– Jeanne
Patient Spotlight: 2nd Line

53
Just when they thought they had conquered the beast, their tumors expand or their side effects become unbearable.
Though disheartened, they know there are still plenty of options on the table. As they move into the new treatment recommended by their doctor, they keep their chins up and hold confidence that this one will be more effective.
SECOND LINE
DISCOURAGED BUT
PERSERVERANTas their body rejects treatment
5
REASONS FOR SWITCHING MEDICATION:• Side effects are unmanageable• Cancer is resistant to treatment• Doctor decides on new therapy
“The fear took my breathe away. It felt like electricity running through my body. I couldn’t sleep I was so petrified, so I took action….I thought ‘This isn’t working, but there has to be something that will.’”
– Laura

54
Having gone through several cycles of treatment, this is no longer a foreign experience to them. They have a consistent schedule where they see the same nurses and are injected with medicine that will have predictable side effects. They look forward to the warm blankets they will receive afterwards, and have even made friends with other cancer patients they met in the waiting room.
Unlike first line, when their expectations were rooted in preconceived notions, they are now at a point of familiarity and have grown accustomed to the process.
SECOND LINE
COMFORTABLEwith IV treatments
5
“At the first treatment, you have no idea of how it is going to affect your life, but as you slowly progress through you begin to plan your life around it.”
– Jeanne

55
The public persona they once knew is deteriorating. As side effects have become more visible and consistent, they have also become more difficult to mask. Being around other people is a difficult task, and they draw inward, feeling ashamed and self-conscious.
Examples of visible side effects include hair thinning, rashes, weight loss, diarrhea, memory changes, and relentless fatigue. Some patients have a colostomy done and must carry a stoma (colostomy bag) at all times in order pass bowel movements.
Not everyone around them knows they have cancer, so they worry that not everyone will understand. This may affect their adherence to medication. The way they see themselves and the way they think they are seen has completely changed for the worse.
SECOND LINE
EMBARASSEDas cancer seeps into their personal
life and alters their self-esteem
5
“The new medicine gave me acne all over my chest and face, I lost my hair, and looked like a teenager!”
– Steven

56
Undergoing chemotherapy and radiation has made cancer real. At diagnosis, they were frozen in a state of shock, but no longer is having cancer a lingering phrase, it is their life.
Everything from their relationships to their schedule to the physical state of their bodies have shifted to revolve around cancer.
Coming to terms with the fact they have cancer makes it’s first mark at this point in the journey.
Note: Everyone has their own path to acceptance, but this is typical to most
SECOND LINE
ACCEPTINGthe fact that they have cancer starts
here
5
“I grieved when I first was diagnosed and starting chemo. I was bummed out and angry and went through the normal grieving process. But after my first chemotherapy, I accepted it. Either you accept it and go on with your life or you live as a grumpy old fart. Acceptance has made everything easier…dying is going to happen to all of us. ”
– Steven
57
Back again for their routine check-up, they pray that all their hard work has paid off.
One diagnosis and two treatments later, they just want to restore their bodies to decent health. In these several days their minds race as they picture all the possible outcomes that may be. Unfortunately, there is nothing they can actively do to influence their results, so they are left helpless as they stress and think through the wait.
SECOND LINE
WORRIEDas they wait on test results
5
“The wait and see process…was a very nerve-wrecking period of time when I didn’t know what was wrong with me.”
– Sue
Third Line
Treatment Moments that Matter

“You do what the doctors say and think everything is going to be fine. Something shows up in the liver and it’s devastating. You go all the way back to square one again. It’s almost to the point of being clear and then it goes back again. You still don’t know how complicated the disease could be.”
–Jeff
Patient Spotlight: 3rd Line
60
How could this not work? A betrayed patient points an angry finger at the doctor, who recommended these medications in the first place. He boasted their scientific backings and ease of use, and the patient trusted him. But nothing turned out according to plan, and the patient is feeling frail, emotionally and physically weaker than ever before.
THIRD LINE
HEARTBROKEN AND
FRUSTRATEDthat medication has failed
6
“I felt like somebody smacked me in the face. It was hard on me, I was devastated. Words can’t really explain. I was thinking I would get rid of this; I was doing well for a year of a half and all of the sudden it spread.”
– George
REASONS FOR SWITCHING MEDICATION:• Side effects are unmanageable• Cancer is resistant to treatment• Conflict with doctor
61
Having tested several methods of treatment at this point in the journey, they have developed a stronger grasp on what their body accepts and what it rejects.
Often they start with one base therapy and interchange supplemental medications, allowing them to experiment with efficacy and side effects until they have found the perfect balance that is just right for them.
With this new understanding of their bodies, they are more vocal with their doctors and demand treatments they know will best suit their individual needs.
Note: This pertains to patients still on IVs
THIRD LINE
EMPOWEREDas they understand their body’s
responses
6
“You have to look at how you are responding to this, and your toxicity. It’s an art, you have to figure out what’s going to work. Combining chemo with radiation was an important step I made.”
– Sue
At this point in the journey, the Withdrawn do not typically
feel empowered to speak up about medications. Instead
they continue to trust their doctor over their own body.
Segment Shift:

62
Going from hospital visits to self-administering medication makes all the difference in their sense of freedom. Rather than scheduling their weeks around doctor’s visits and relying on their caretaker to bring them there, they have a portable medication that is just as simple as taking a vitamin. No more travel time or waiting time to be treated – just the pill and water whenever they decide.
Now that they don’t have to block out hours of their day, they have opened up their schedules to do more of what they want to do, when they want to do it. Plus, they don’t have to put as much mental energy into thinking about cancer. With this new release, they have authority on their lives again.
THIRD LINE
LIBERATEDas they make the switch from IVs to
oral therapy
6
“I was very excited – it was a good time for me mentally and physically. I went on vacation, spent a lot of my time with husband, and felt strong enough to go on a trip with my friend. I loved my doctors and nurse, but with the IV I would be anxiety ridden for two or three days going in.”
– Tammi

63
Since the switch to an oral medication, they must create entirely new schedules for themselves. Gone are the days when treatment times were set in stone, when caregivers drove them to appointments and nurses injecting their medicine. Instead, they self-administer it, when they decide, posing a possible barrier to adherence. With this new freedom comes accountability and the responsibility is on them to make a comfortable routine they can stick to.
Note: This applies to patients who made the switch to oral therapy.
THIRD LINE
ADAPTIVE as they adjust to a new routine
6
“Infusions are easy, you just go to the doctor. With being on Stivarga, I sometimes forget, or I don’t take them. It’s like a form of rebellion. Cancer sucks.”
– Jeanne

64
Regardless of what they are on, failed treatments and recurrences have become a life motif, and the likelihood that this could happen again is not so far off base. This is the biggest fear of their lives and it follows them everywhere they go. God forbid the lump in their neck, pain in their back, or stomach ache means the cancer has returned. They are arrested by the possibility of the disease getting worse at any second.
THIRD LINE
WALKING ON EGGSHELLSas every ache triggers fear of
cancer
6
“Having cancer, you will always live this way, so when you have pain you start panicking. Every little lump or bump will always be cancer to me, even if that’s not what it is.”
– Emily
The realistic segments are more matter of
fact at this stage, and know that their cancer
is likely growing.
Segment Shift:
65
It’s back again to the waiting game, but this time their fear of tumor growth is many months in the making. As they wait on the results, they hold their breath, frozen in fear as they are captured by cancer-phobia. If the results return bad news, it means more pain, and less life.
THIRD LINE
TERRIFIEDas they wait on scan results
6
“There is always the fear that it will be the worst possible scenario. I call it scanxiety.”
– Jeff

Fourth Line +
Treatment Moments that Matter

“Psychologically speaking, I thought I was going to beat it. Now I have to try something else and take the crap of not knowing if it is going to work. It put me in another frame of mind, and for my wife, being my caregiver, it is almost like her having the cancer. Stivarga shrunk the tumor but the side effects were too much. I had open wound blisters on my feet and have to use a wheelchair because I can’t walk. I cried bitterly. There are times I have thought to myself, ‘is it really worth it?’ But I don’t want to stop treatment. The only obstacle would be if the treatment doesn’t work anymore…I still have a soul, I still have a heart, and I still have a love for my life. I’ll be damned if I give up because a doctor says to me that they can’t treat me anymore…You have to be your own advocate.”
– Michael
Patient Spotlight: 4th Line
68
Despite all the adversity they have faced, it just isn’t getting better. They have gone through surgery, radiation, three different medications, and financial and emotional hardship only to be told they are still riddled with disease. Aggravated, they feel as if their suffering hasn’t amounted to any progress and will have to endure a new set of side effects once more.
FOURTH LINE
FRUSTRATEDwith unrelenting side effects and/or
ineffective therapy
7
REASONS FOR SWITCHING MEDICATION:• Side effects are unmanageable• Cancer is resistant to treatment• Conflict with doctor• Understanding their body’s responses to therapy
“After Xelota and Avastin gave me hand-foot syndrome, I switched to a clinical trial, and then I switched to Folfiri. But I hated Folfiri because I felt so sick, got so thin, and lost my hair. I just wanted to get off it.”
– Michelle

69
Across the board, patients begrudgingly declared that chemotherapy is poison. Intended to shrink their tumors, though sometimes with avail, the side effects are so debilitating they can barely function. Living a normal life is becoming frustratingly impossible, and it is as if the chemotherapy is harming them more than the cancer.
For instance, patients are so overcome with fatigue they could hardly stay awake. Some were bound to wheelchairs due to skin peeling caused by hand-foot syndrome. Others couldn’t even push elevator buttons or hold a pen because of the neuropathy.
The life they loved to live has been erased by the chemotherapy, and their entire existence revolves around managing side effects and adhering to a schedule.
FOURTH LINE
BITTERas toxicity builds
7
“I had enough. I was underweight. The only thing the doctor did was lower the dosage strength of the chemo. He would agree with what I said but never confirm that he was going to change it. I was so sick and felt like, in my bones, I was going to die, not from the cancer but from the side effects of the chemotherapy. It is poison.”
– Fran

70
When the going gets tough and they struggle to carry on, they ground themselves in a higher purpose. Some lean on their faith in God to carry them through, holding strong to the belief that He has a plan and will be with them in Heaven. Others are motivated by the people they love the most – if they leave this Earth, it may be too difficult for their families to go on without them. Some even say this was given to them as a necessary challenge towards growth as human beings.
No matter the reason, their incredible resilience is driven by the belief that this fight is bigger than themselves.
FOURTH LINE
MOTIVATEDby a strong sense of purpose to
keep the fight alive
2
“I will go onto a better place, but my wife is the one who will be left behind…I am doing everything I possibly can in my power to make sure I don’t leave her. She is such a motivating factor. ”
– Jeff
The Independents may be less motivated here to keep
fighting with medication, and may instead make the
choice to fight with other means, and opt for better QoL.
Segment Shift:

71
The entire mCRC journey has been a learning and growing process for them. Conflicting messages from doctors, loved ones, and statistics have been pulling them in opposite directions, influencing their treatment decisions and life perspective.
However, they are no longer novices to this game. Initially, they were insecure and in need of more guidance, but now they realize the doctors’ recommendations and predictions are not necessarily true for them. One size does not fit all. They refuse to be a statistic; their lives are important. With this heightened sense of self-worth, they speak up for themselves and challenge the doctor’s advice. They are the navigators of their journey.
FOURTH LINE
ASSERTIVEas they strengthen their voice and
define their experience
2
“You have to ask questions…If you aren’t interested in your own health, you are going down the wrong road. You have to know for yourself what you’re doing, what you’re chances are, and if you don’t like it, fire the doctor and get another one. Nobody owns my body but God”
– Michael
The Followers are less likely to take their treatment into
their own hands, but may switch doctors if they feel that
theirs is willing to give up the fight.
The Withdrawn are less likely to challenge what their
doctor says, and may still maintain some degree of
insecurity.
Segment Shift:

72
Despite the morbid statistics and cynical doctors who told them their lives should be over by now, they are still breathing. All the messages they received up through this point says the cancer should have killed them by now. Living past their life expectancy has given them strength and validated the belief that they can make it past anything.
FOURTH LINE
GRATEFULthey have made it this far
7
“In some respects, I am very fortunate that I have survived this long. The mortality rate is very high. It is not so much a challenge, but a blessing. Everyday is another day. Every year is another year. It depends on how you look at it. I’ve survived 15 years.”
– Steven
73
Despite all the trials and tribulations, their goals have stayed the same: find a cure to this disease or go into remission.
After all, they have lived past their predicted life expectancy and made it through four lines of therapy, proving to themselves that they have the resilience it takes to defy all odds. They keep their eyes peeled for the possibility of an existing cure, and settle for no less.
FOURTH LINE
STILL DETERMINEDto find the silver bullet
7
“There’s one conclusion that is satisfactory, which is complete remission, otherwise or you are circling back into a research mode for different potentials. There are no appropriate answers besides remission or cure.”
- Robert
The realistic segments’ goals revolve more
around maintenance and finding more time,
knowing that a cure is not out there.
Segment Shift:
74
Since their bodies have rejected everything so far, new science could mean promising results. Clinical trials not only advance their chances of success, but also advance science and the well-being of others in the process, giving them the extra satisfaction of using their struggles for a greater good. However, they will only consider up and coming therapies backed by evidence that show improvement and have minimal side effects. When they do find this, it tells them that maybe life isn’t over after all.
FOURTH LINE
PERSERVERANTas clinical trials and new treatments
provide a glimmer of hope
7
“Every time I sign up for a clinical trial, I trust that it might be the next successful thing…I hope I am taking an experimental drug that is the next best thing for the FDA to push through.”
- Michelle

75
Patients are at the end of their line. They can only handle so much heartbreak and failure before they fall apart. With every failed scan result, the likelihood of death becomes more real in their minds. Medically speaking, they have tried almost everything. Their well-being and the well-being of their family are at stake. The outcome of these results mark a pivotal moment in their future.
FOURTH LINE
PETRIFIEDas they wait for results to come
back
7
“I don’t care who you are, with every little thing that comes up, you will always have, with colorectal or any other cancer diagnosis, a fear that it is coming back. Your brain never lets you see no evidence of disease.”
– Fran B
The illusory segments will likely continue to
fight and exhaust all options in the hope that
something will work or give them more time.
Segment Shift:

Ending Treatment
Treatment Moments that Matter

77
ENDING TREATMENT
VARYING EMOTIONSexperienced when making the decision to end treatment
SAD & DEPRESSEDby the lack of treatment options
HELPLESS because they’ve lost power over life
FEELING INVISIBLEwhen unheard by the oncologist
DEMORALIZEDwhen treated as a number, not a
human
FEARING THE FUTUREwithout information on long-term living
RELIEVED by the support of family & friends
FEELING GUILTYfor putting their family through the ringer
RESENTFUL & DEFEATEDabout living with unbearable side effects
ENDING TREATMENT
SAD & DEPRESSEDby the lack of treatment options
Many patients will continue to fight for as long as
treatment options are readily available. Unfortunately,
there are not unlimited options and patients too often find
themselves forced to make the decision to end active
treatment even when they are mentally and physically
wanting to continue. While this lack of treatment options
may not be an adherence issue on the patient’s part,
they’re still left feeling completely depressed and betrayed
by their body – sometimes even blaming themselves for
their body’s inability to work well with the chemotherapy
options supplied by their doctors.
“It is quite a burden. You want (to be cured) so badly that you feel helpless about it. At a certain point you look back and say you’ve done everything you can.”
– Robert F.
78
Relevant
Segments:
ENDING TREATMENT
HELPLESS because they’ve lost power over life
Maintaining a sense of control over their lives is critical for
patients living with mCRC, particularly since they no longer
have power over their bodies. As individuals progress
through their mCRC journey, they feel like they’ve slowly
lost authority and seek out ways to take back the power in
their lives. Many patients feel the decision to end active
treatment gives them back this sense of power. They often
associate the decision more with making the choice to live
and live on their own terms, versus die and die under
cancer’s control.
79
“I will not let this be a death sentence. I will die on my own terms.”– Robert F
Relevant
Segments:
ENDING TREATMENT
FEELING INVISIBLEwhen unheard by the oncologist
A patient’s relationship with their oncologist plays an
extremely important role in the success of their long-term
adherence. Many patients expressed frustration and lack
of confidence in their doctors – either giving up on them
way too early and/or missing the drive to research
alternative options. Patients will often jump around from
doctor to doctor in hopes of eventually finding a good fit,
all the while unable to develop a lasting relationship
grounding in trust and equality. This inability to find a
stable medical partner means patients’ routine and
compliance suffer. If they don’t believe in their doctor they
are less likely to believe in the recommended treatment
plan.
80
“Our tiffs came from his push for chemo and alternatives weren’t his proclivity. I asked about the side effects, if they were going to be worse and he kept saying he wasn’t sure. In my mind, if he surgically removed the cancer and the only things showing up were in my nose and lung, why was he forcing poison into my body?”
– Fran
Relevant
Segments:
ENDING TREATMENT
DEMORALIZEDwhen treated as a number, not a human
Too often along their mCRC journey patients experience
the ‘cattle drive’ syndrome. From the way they engage
with doctors to how treatment processes and plans are put
into place, patients are left feeling like they’re treated more
as a statistic, than a human being with individualized
needs. In their eyes, their mCRC experience is a personal
one so therefore they require a plan of action (goal setting,
treatment dosing, information gathering, etc.) that is as
unique and particular as they are themselves. This notion
of ‘group protocol’ can often lead patients to distrust in the
healthcare system and disconnect for their treatment in an
act of rebellion.
“Many cancer patients just do what the doctor says. I refuse to be cattled.”– Fran
81
Relevant
Segments:

ENDING TREATMENT
FEARING THE FUTUREwithout information on long-term living
While physicians often refer to mCRC as a chronic
condition, this information is rarely relayed to the patients
themselves. Conversations are often focused on the here
and now with little emphasis on next steps or more
importantly, long-term living. This ‘today’ tactic may work
for some, but for most can create a sense of fear – not
knowing what to expect or how to react. It also may
generate a more immediate will to fight, but does a
disservice to patients in the long run when their cancer
becomes a more chronic battle. It’s more difficult for them
to maintain a strong will later on in the journey without a
marathon-type outlook engrained in them from the initial
point of diagnosis.
82
“Being a survivor at stage 4 and being told you have a year, I hated that. There wasn’t much discussion on what you do after, how you handle the side effects, what is your new normal is and how you prepare yourself for that. You’re not expected to survive.”
– Fran
Relevant
Segments:

ENDING TREATMENT
RELIEVED by the support of family & friends
As patients progress through lines of therapy, the support
of those around them begins to wield more influence over
their treatment decisions. Regardless of whether or not
patients themselves want to stop or continue on with
treatment, the urgings of their family, friends, and even
physicians can sway them toward one decision over
another. If a patient’s family is telling them to stop
treatment, it’s likely that they will listen and for many, even
feel relieved.
“I had a family meeting with my three children. They said, ‘Mom, we ratheryou have a full, short life than a long, hard life.’ so that is what we decided…Iwatched my dad die of cancer and suffer for a year… I don’t want my familyto watch that. My children are my world.”
–Kathy
83
Relevant
Segments:
ENDING TREATMENT
FEELING GUILTYfor putting their family through the ringer
Patients’ decision to end treatment can also be heavily
influenced by the guilt they experience from involving their
family in all the physical, emotional, logistical, and financial
burdens associated with the mCRC journey. Patients often
express the want to end treatment purely based on it
being beneficial to the ones they love. They no longer
want to put their family through the ringer and from a
personal standpoint, no longer want to feel the
responsibility of knowing that it’s all due to them and their
ongoing complications and frustrations.
“As the cancer adapts to treatment, and as your body can no longer take chemo, you begin to lose options. But I’m not going to put my family in debt for a clinical trial that may not help me. I must shelter my children from a lot of decisions.”
– Tim
84
Relevant
Segments:
ENDING TREATMENT
RESENTFUL & DEFEATEDabout living with unbearable side effects
The physical toll that patients experience while undergoing
chemotherapy can be unbearable. As patients progress
through the mCRC journey, it becomes more and more
difficult for them to focus on the positive benefits of the
treatment, and rather begin to fixate on the negative side
effects. Once patients realize that their days are
numbered, quality of daily life triumphs quantity of days.
Even for those that experience only a few bad days of side
effects at the beginning of each round of chemo, it’s
difficult for them to see through to the other side.
85
“Chemotherapy has been extremely difficult. If anything, it has extended life three to four months, yet my quality of life has been deteriorating greatly. Side effects play a huge part, but it’s not just that. You get tired of the whole state of mind. Where is the future in that? Is it going to change or get better? No. I’ll have a better quality of life without it.”
– Tammi
Relevant
Segments:

Best Supportive
Care
Treatment Moments that Matter

“My teenagers came home when I was laying on the couch and thought I was dead. They said ‘Mom, don’t do this.’ So I had a family meeting with my three children and they said ‘Mom, we rather you have a full, short life, then a long, hard life. So that is what we decided. It was the hardest decision of my life…but I was not living…this is difficult for people to process. As somebody who hasn’t gone through treatment and doesn’t know how I react to chemotherapy or how I feel, they can’t really comprehend. ”
– Kathy
Patient Spotlight: Best Supportive Care
88
Their entire journey has been an experience of loss: hair loss, weight loss, memory loss, financial loss, loss of time, loss of freedom, and loss of happiness. The decision to go off treatment is about regaining these losses and restoring their livelihood. No longer will they just be going through the motions. No longer will they have to endure the tribulations of chemo.
After serious thought, they have made the conscious decision to sacrifice a longer life in exchange for a better life. To them, time is most valuable when they can enjoy it. The trade-off is worth the price. They have made up their minds.
BEST SUPPORTIVE CARE
DECISIVEas they cut their losses
8
“I was not living. It is very much quality over quantity. I rather live six full months and truly live life then six terrible years. People disagree with my decision but is something I have to do my way. People say I am choosing to die, and I say no, I am choosing to live.”
– Kathy
For the illusory segments, it is more likely
that they ran out of viable options to treat
their mCRC, than choosing to stop
Segment Shift:

89
Everything up through this point in their journey has shaped them to be extremely time conscious. With a shortened period of time left, the little moments matter: doing homework with their children, feeling the warmth of sunshine on their face, watching a movie with their spouse. With death so near, they live in the moment, appreciating every little thing, because there is no
promise for tomorrow.
BEST SUPPORTIVE CARE
MINDFULthat there is no promise for
tomorrow, so they live day by day
8
“It’s a blessing to have this time…I am focused on making good memories with my kids. Telling them I love them, taking more family pictures, making a bucket list, teaching them how to cook.”
– Kathy
90
Although they have made the decision to stop treatment, they are not opposed to innovative alternatives that may heal their cancer, as long as it does not compromise their well-being. After all, they chose to end treatment so they could enjoy life. So if they came across a traditional medication or alternative treatment that would allow them to enjoy their lives even more than now, for even longer than they hoped, they may take it into serious consideration.
BEST SUPPORTIVE CARE
OPEN-MINDEDas they keep their eyes peeled for
new breakthroughs
8
“I get up at 6am every morning, get dressed, turn on the computer and Google colon cancer articles every morning. I am looking for a more centered attack at cancer. There’s a flash of new drugs. You just hope you live long enough to get the silver bullet, the one that cures you.”
– Robert W.
The Withdrawn typically do not engage in as much
information searching, and are therefore not on the
lookout for something new unless their doctor tells them
about it.
Segment Shift:

91
Having resigned from chemotherapy, they acknowledge their death is just around the corner. However, when they leave this Earth their loved ones will remain, coping with the uncertainty of how to carry on without them.
But as part of preparing for death is also preparing others for life, they have taken the necessary steps to set up their families for success after they die. This includes anything from writing a will to paying off the mortgage to teaching their children how to cook. Comfort is found in knowing that the family they leave behind will have something to take with them, making the end easier to accept.
BEST SUPPORTIVE CARE:
ACCEPTANCEof the inevitable, as they’ve
equipped their families for a life
without them
8
“I’ve made a whole folder of benefits that my wife will get when I pass. This has really become more about my family-life insurance, new cars for my wife and son, new furniture, decisions about our home . You get to that point of making sure the family will be secure after you’re gone.”
– Tim
LunchYum!
!

V
Now What: IdeationExploring key moments in the emotional journey
Ideation Introduction
Over the course of this journey we have identified a series
of adherence complications and barriers, spanning from
daily living to long-term compliance. Based off these
findings, we have pinpointed opportunities to ideate from
that will keep our patients on track.
94

95
Adherence Barriers + Innovation Opportunities
Barrier: Lack of Options
Opportunity: Education
Barrier: Doctor Conflict
Opportunity: Optimize
Communication
Barrier: Number, Not
Person
Opportunity:
Personalization
Barrier: Fear of Future
Opportunity: Marathon Not
Sprint
Barrier: Family Supports
Stopping
Opportunity: Provide Family
Hope
Barrier: Causing Family
Hardship
Opportunity: Generate Balance
Barrier: Intolerable Side
Effects
Opportunity: Track and
Predict
Barrier: Loss of Authority
Opportunity: Empowerment
Barrier: Lack of Routine
Opportunity: Create Mindless
Habits

Adherence
BarrierLACK OF OPTIONS. Patients find themselves at a standstill when they no longer see treatment
options on the table. Though they may still want to continue on, they give up when it seems like
nothing is left.
Innovation Opportunity
EDUCATION. Educate the patient on new treatment so that if the doctors don’t provide this
information, the patient themselves can access it. Provide a thorough breakdown of medications
they can take now or in the near future, especially ones they may have never considered before.
This will let them know they are never stuck; there are always ways to keep going.
Relevant Segments:
96
Adherence Barrier
LOSS OF AUTHORITY: As the patient progresses through their journey, they feel like they’ve slowly
lost authority and seek out ways to take back the power in their lives. Many patients feel that the
decision to end active treatment gives them back this sense of power.
Innovation Opportunity
EMPOWERMENT: Develop ways to help them regain power over their everyday lives, from the big
moments to the little things. Giving them the freedom to make decisions over even minute details
can make a huge difference in relieving their frustration and putting them back in the driver’s seat.
Relevant Segments:
97
Adherence Barrier
DOCTOR CONFLICT: Their doctors aren’t providing them the kind of care they feel like they
deserve. Conflicting opinions on next steps of treatment lead to a lack of trust, resulting in a lack of
compliance.
Innovation Opportunity
OPTIMIZE COMMUNICATION: Develop programs and materials that enable stronger
doctor/patient relationships and improve communication. Connect them to doctors that suit their
preferences and needs.
Relevant Segments:
98
Adherence Barrier
NUMBER NOT PERSON: The patient is treated like a statistic, rather than a person with individual
needs.
Innovation Opportunity
PERSONALIZATION: Provide them with treatment and support that is tailored to their personal
experience, acknowledging them as a human being who needs specialized care. One size does
not fit all.
Relevant Segments:
99
Adherence Barrier
FEAR OF THE FUTURE: There is plenty of conversation on how to deal with fighting cancer right
now, but nothing about how to live with it forever.
Innovation Opportunity
MARATHON NOT SPRINT: Create resources that eliminate fear of the future and lend insights on
how to deal with everyday life as a cancer patient. Restructure the conversation so it is framed as a
marathon, not a sprint.
Relevant Segments:
100

Adherence Barrier
FAMILY SUPPORTS STOPPING: Their families, one of the main drivers for continuing the fight,
give them the okay to let go of treatment.
Innovation Opportunity
PROVIDE FAMILY HOPE: Deliver hope and support for families so they have the tools and
emotional means they need to carry on as caregivers. Empowered families equal empowered
patients.
Relevant Segments:
101

Adherence Barrier
CAUSING FAMILY HARDSHIP: The patient feels like a burden to their families as their loved ones
sacrifice money, time, and energy to keep them alive.
Innovation Opportunity
GENERATE BALANCE: Provide outlets, support systems, and tools for family members to generate
balance in their lives so that they don’t feel over-impacted. Having these resources will relieve the
guilt the patient carries and lessen everyone’s hardship.
Relevant Segments:
102
Adherence Barrier
INTOLERABLE SIDE EFFECTS: The patient is fed up and exhausted by side effects that never go
away.
Innovation Opportunity
TRACK AND PREDICT: Provide a snapshot for the patient to track and predict side effects. We’ve
heard that side effects are worse in the beginning then they are towards the end, demonstrating
what to expect will help them see the light at the end of the tunnel.
Relevant Segments:
103
Adherence Barrier
LACK OF ROUTINE: Switching from an IV to an oral means a change in their routine and has a
completely new set of implications. With an IV, they could compartmentalize cancer, whereas orals
stay with them as a constant reminder. Orals are also self-administered, so they must rely on
themselves to take it.
Innovation Opportunity
CREATE MINDLESS HABITS: Create a new structure so that taking orals becomes a mindless
habit, freeing up their mental energy and preventing further stress or exhaustion.
Relevant Segments:
104

NOW WHAT: Patient Role Play
The Self-Advocate The Independent The Follower The Withdrawn
The Caregiver
105

www.nowwhat.com
THANK YOU!Now What
155 Avenue of the Americas
7th floor
New York, New York 10013