-
Tack Optimized Balloon Angioplasty
George Adams, MD, MHS, FACC, FSCAIUniversity of North Carolina –
Rex Healthcare
Raleigh, North Carolina, USA
-
Dissections Occur Frequently…
• Dissection is a result of plaque disruption during
angioplasty
• DCB may not be a stand-alone therapy in mechanically
challenging SFA/popliteal lesions:• CTO
• Lesions >15 cm
Study Dissection Rate
PACIFIER 47.4% PTA73.5% DCB
THUNDER 56%
LEVANT 2 72.3% PTA63.7% DCB
Metzger C. Multicenter Global Registry Report of the Two-year
Outcomes with a Paclitaxel-Coated Balloon in Patients with Complex
Femoropopliteal Lesions, TCT 2016Scheinert D. Strengths and
Weakness of DCBs: Insights from the Global Registries, VIVA
2016
DCB Registry Dissection/Stent Rate
Lutonix® Global Registry1
34.3% in lesions 140 – 500mm(35.7% stent rate)
IN.PACT® Global Registry1
26.2% in lesions ≥ 15cm(40.4% stent rate)
-
…Often Worse Than We Think
0
10
20
30
40
50
60
70
AB
CD
ENone
TOBA: Baseline Dissection Grade
Site
Core Lab
Major disparity between site reported and core lab dissection
grade
Bosiers M et al. J Vasc Surg 64(1):109-16.
-
• Chronic inflammation
• In-stent restenosis
• Limit future treatment options
• Fracture
Stent (study) Re-stenosisStent Fracture
Rate
ZilverZilver PTX
16% @ 1yr10% @ 1yr
0.9% RCT1.5% SAT
Supera (SUPERB) 13% @ 1yr 0.0% @ 1yr
Wallstent Up to 19%
SMART (SIROCCO) 18% @ 6m 18.2% @ 6m
EverFlex (Durability) 28% @ 1yr 0.4%
LifeStent (Resilient) 19% @ 1yr 3.1% @ 1yr
Luminexx (FAST) 32% @ 1yr 12% @ 1yr
Dynalikn-E (STRIDES) 32% @ 1yr 2% @ 1 yr
Stents Have Limitations
-
Tack Endovascular System®
Tack® Implant
Nitinol with gold radiopaque markers
Unique anchoring minimizes migration
Pin-and-pull delivery technique
Over-the-wire system
Pre-loaded 6mm implants
Delivery System
CAUTION: Investigational device. Tack Endovascular System is
limited by Federal (United States) law to investigational use. Not
approved for sale in the United States. Tack Endovascular System is
CE Mark authorized under EC Directive 93/42/EEC.Tack Endovascular
System® and Tack® are registered trademarks of Intact Vascular,
Inc.
Sizing:4F – 1.5mm-4.5mm RVD6F – 2.5mm-6mm RVD
-
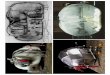
Minimal Metal
Short, open cell design
Low Radial Force
Minimizes vessel trauma
Focal Treatment
Treat only where needed
Typical Stent
6Fr Tack Implant
4Fr Tack Implant
Better Healing1 by Design
1Schneider PA et al. JACC Cardiovasc Interv 8(2):347-54.
-
Evidence
Study Design Status Key Findings
TOBA(N=138)
Prospective, single arm13 European sites
Completed Published in Journal of Vascular Surgery 2016• 89.5%
K-M freedom from CD-TLR• 76.4% K-M patency rate• 98.5% technical
success rate
TOBA II(N=210)
Prospective, single arm40 US and European sites
Enrolling Actively enrollingPOBA or Lutonix® DCB
TOBA III(N=200)
Prospective, single arm20 European sitesLong lesion subset (≤250
mm)
Enrolling Actively enrollingIN.PACT® Admiral® DCB
ABOVE THE KNEE
Bosiers M et al. J Vasc Surg 64(1):109-16.
-
TOBA II/TOBA III: Endpoints
Primary Safety Endpoint:
Freedom from any new-onset MAE:
Index limb amputation (above the ankle)
CEC adjudicated clinically-driven target lesion
revascularization (CD-TLR)
All-cause death at 30 days
Primary Efficacy Endpoint:
Primary patency:
Freedom from CEC adjudicated CD-TLR
Freedom from core lab-adjudicated DUS binary restenosis at 12
months (PSVR >2.5)
-
It’s a different disease
• Small vessel diameters
• Diffuse calcium
…with poor treatment options
• PTA• POBA, DCB • Poor long-term outcomes• Dissection
• Stents• BMS, DES• In-stent restenosis
• Alternatives• Atherectomy• Invasive bypass surgery
Challenges in BTK Treatment
-
Evidence
Study Design Status Key Findings
TOBA BTK(N=35)
BTK - Prospective, single arm6 Europe/New Zealand sites
Completed Presented at SCAI 2016• 100% 30-day patency• 84.5%
amputation-free survival at 12m• 93.5% freedom from CD-TLR at
12m
BELOW THE KNEE
Bosiers M et al. J Vasc Surg 64(1):109-16.
-
TOBA BTK Demographics and Lesion Characteristics
SubjectsSafety(n=35)
Performance(n=32)
Age (Y) 76.1 ± 9.3 76.1± 9.5
Gender:Female
Male48.6%51.4%
43.8%56.3%
Diabetes 77.1% 81.3%
Hypertension 91.4% 90.6%
Smoking:CurrentRemote
5.9%29.4%
6.5%32.3%
Rutherford:45
11.4%88.6%
12.5%87.5%
Core Lab Baseline Lesion Characteristics(Safety Sample)
Lesion length (mm) 51.4 ± 28.0 (34)
Total occlusion 22.2% (8/36)
Dissection Grade: ABC
21.2% (7/33)60.6% (20/33)18.2% (6/33)
Proximal Lesion Location:Anterior tibial
Tibioperoneal trunkPeroneal
Posterior tibial
38.9% (14/36)27.8% (10/36)16.7% (6/36)16.7% (6/36)
Calcification: None/mildModerate
Severe
36.1% (13/36)61.1% (22/36)2.8% (1/36)
• Broad anatomical distribution• >60% moderate/severe
calcification• 1/5th of patients had total occlusions• Lesion
lengths up to 8cm• ~80% Grade B+ dissections
• ~90% were Rutherford 5
• ~80% had diabetes
-
Safety and Performance
ParameterSafety Sample
N=35
Performance
Sample; N=32
Device Success1 32/35 (91.4%) NA
Procedure Success2 34/35 (97.1%) 31/32 (96.9%)
1Successful delivery and deployment of the study device(s) at
the intended target site(s) and successful withdrawal of the
delivery catheter2Demonstrated vessel patency as reported by the
physician (visual estimate) without the occurrence of MALE + POD on
the date of procedure
Primary Safety at 30 Days Safety Sample Perf. Sample
Composite Primary Safety Endpoint 1/35 (2.9%) 1/32 (3.1%)
Major Amputation 0/35 (0.0%) 0/32 (0.0%)
Re-intervention 1/35 (2.9%) 1/32 (3.1%)
Death 0/35 (0.0%) 0/32 (0.0%)
-
Twelve-month Results
Days Since Index Procedure
Pri
mary
Pate
ncy P
er
Pati
ent
0
10
20
30
40
50
60
70
80
90
100
Days Since Index Procedure
0 30 60 90 120 150 180 210 240 270 300 330 360
Primary Patency by Vessel at 12m = 78.4%
Primary Patency by Subject at 12m = 77.4%P
rim
ary
Pat
en
cy
Observational Endpoint 30 Days 3 Months 6 Months 12 Months
Amputation-free survival
(above the ankle)100% 96.8% 96.8% 84.5%
Freedom from CD-TVR 100% 100% 93.5% 93.5%Freedom from CD-TLR
100% 100% 93.5% 93.5%
-
What’s Next?
TOBA II BTKPivotal study of the Tack device in the treatment of
patients with critical limb ischemia
Study Design Prospective, single-arm, multi-center
Population • Subjects with CLI (RCC 3-5) and angiographic
evidence of a dissection post-PTA
• Patients will be assessed using the WIfI risk stratification
system
• No lesion length maximum
Subjects/Sites 232 subjects at up to 50 global sites (~40 US
sites)
-
TOBA II BTK
Primary Endpoints
Safety MALE + POD at 30 days
Efficacy MALE at 12 months + POD at 30 days
Secondary Endpoints
Target lesion(s) tacked segment(s) patency at 12 months defined
as the presence of blood flow using duplex ultrasound (flow vs. no
flow)
Target Limb Salvage defined as freedom from any above-ankle
target limb amputation at 12 months
Enrollment to begin Q1 2017Enrollment projected to be complete
in Q1 2019
-
Summary
• Tack Endovascular System offers new paradigm in treating
post-PTA dissections
• Preserves future treatment options
• Rigorous clinical development program both above and below the
knee
-
Tack Optimized Balloon Angioplasty
George Adams, MD, MHS, FACC, FSCAIUniversity of North Carolina –
Rex Healthcare
Raleigh, North Carolina, USA