Embed Size (px)
Citation preview

The Evolution of the 2‐Midnight Rule
Rose M. Turner, RN, BSN, ACM
Wednesday, September 17th, 2014
The information provided in AHC Media Webinars does not, and is not intended to constitute medical or legal advice. Opinions, references and links provided by our speakers are provided for your convenience and do not represent our endorsement of such opinions, products or services.

2
Rose M. Turner, RN, BSN, ACM, is President of Rose M. Turner Consulting, a hospital case management consulting firm where she uses over 20 years of expertise to design programs that are patient focused and easy to operationalize. She has worked in hospital case management for over 20 years managing the most complex cases on the front lines and designing programs and processes for difficult patient populations as a special projects case manager. Her hospital work also includes developing policy, astute knowledge of government regulations affecting case management, and implementing case management education & orientation programs.
22
Speaker
Learning Objectives1. Describe the development of the 2MN Rule.
2. Review the change in using medical necessity for admission.
3. Explain the effect of the 2MN Rule on the hospital revenue cycle.
4. Explain new and revised case management standards, regulations, and laws put forth by CMS, TJC and the federal government.
5. Evaluate case management protocols and penalties.
Key Concepts
• The history behind the 2 MN Rule development• Changes to hospital processes regarding billing level of care
• Debate on how to interpret and document the physician’s order & certification
• Legislative and court battles shaping the rule• How the voice of the provider now influences CMS
• The financial impact to the hospital revenue cycle
H.R. Bill 6675Medicare Act
• Created under Title XVIII of the Social Security Act
• Signed into law by Lyndon B. Johnson July 30, 1965
• Designed for Americans 65 and over who could not get health insurance to cover costly hospital bills
• President Harry S. Truman received the very first Medicare card
• Crafted to mirror major commercial plans at the time – the Blues
• Developed as an 80/20 policy –plan pays 80%, patient pays 20% with copays & deductibles
• Financed by payroll taxes
Billing Level of Care
• Clinical level of care – ICU– Intermediate Care– Med‐Surg
• Billing level of care– Inpatient– Outpatient (Observation)
HR 611 Tax Relief & Healthcare Act of 2006 (Section 302)
8
Assumption: 5‐6% of payments to hospitals are errors
Medicare Trust Fund running out of money
Demonstration project – a first for Medicare to go to outside contractors
Recovery of over $10 billion in 3 years, 3 states
How we got here
9
What is the RAC? (the official definition)
Recovery Audit Contractors = private companies using proprietary data mining software to review Medicare billed claims for potential errors ‐ both overpayments and underpayments
“CMS designed the RAC program to:1) Detect and correct past improper payments in the
Medicare FFS program; and
2) Provide information to CMS & Medicare contractors that could help protect the Medicare Trust Funds by preventing future improper payments thereby lowering the Medicare FFS Claims payment error rate.”1
They get a percentage of all monies successfully retracted1Medicare RAC Program Update, June 2010
The Complexity of CMS RAC Program
• Contractors data mining claims
• Claims look back 3 years• Routine denials• Long time intervals• Volume nation‐wide is choking
the appeal process• No additional resources for
CMS entities• Recoupment of money from
providers• Contractors incentivized
financially• Automated denials (mostly
coding)• Complex denials (medical
necessity)

12
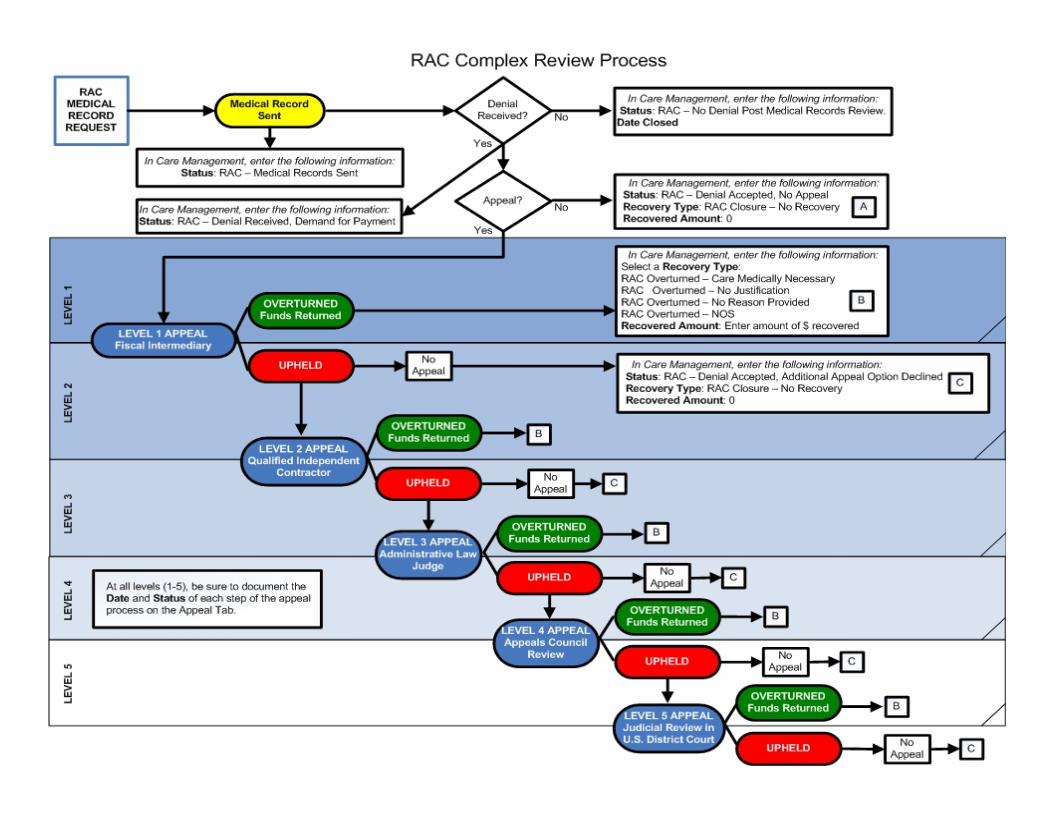
Medicare Levels of Appeal – nothing new
Level 1: Fiscal Intermediary (FI) Level 2: Qualified Independent Contractor (QIC) Level 3: Administrative Law Judge (ALJ)Level 4: DAB/MAC (Medicare Appeals Council)Level 5: US District Court
Medicare Appeals Council Review (CMS can pursue if they disagree with the ALJ findings)
14
Initial RAC Targets
Level of care – short stays
3 day stay with transfer toSNF
Code 44
Discharge Disposition Codes
Cardiac Procedures
“Retrospectoscope”
Dr. Ronald HirschMedical Director, Case ManagementSherman HospitalElgin, IL
ACMA Learning Link
“In recent years, the number of cases of Medicare beneficiaries receiving observation services for more than 48 hours, while still small, has increased from approximately 3 percent in 2006 to approximately 8 percent in 2011. This trend concerns us because of the potential financial impact on Medicare beneficiaries…‖ …in only rare and exceptional cases do reasonable and necessary outpatient observation services in the hospital span more than 48 hours.”
2014 IPPS Final Rule
Over the next 3 years CMS found an increasing use of Observation as RAC Program Continues………
………….and the volume of claims appealed by hospitals is now in the 100’s of thousands……..
It was a hot, muggy afternoon in Washington, D.C. The date was August 2nd 2013 at 5 pm EST.As all of Washington was hitting the beltway for the drive home to Arlington, VA or to the airport to fly to the Hamptons for the weekend…CMS posted the new FINAL Inpatient Prospective Payment System (IPPS) for FY14………
The 2 MN Rule • First published in the IPPS
FY14 effective October 1, 2013• Dramatically changed hospital
admission determination for IP vs. OP
• Gave little time to operationalize a change with new regulatory requirements
• Did not address many “real” scenarios that hospital personnel face every day
• Time trumps criteria• Days were calculated by MNs
not hours • Rules for physician
documentation was very specific
• ED physicians could no longer write billing level of care orders
The 24 Hour Benchmark
The 24 hours benchmark now applies to the 24 hours that start at MN of the first calendar day the patient is in a hospital bed to the following
MN.
Each MN time period is called a “Medical Utilization Day” or affectionately known as a ‘MUD’
Benchmark vs. Presumption
• Benchmark of 2 midnights– “decision to admit should be based on the cumulative time spent at the hospital beginning with the initial outpatient service”, i.e. physician should consider the time already spent (ED, OBS services)
Benchmark vs. Presumption
• Presumption of 2 midnights– inpatient claims with LOS>2 MNs after formal admission will be presumed appropriate and will not be the focus of medical review (ex., systematic abuse or delays in provision of care)
Time‐based INPT Admission
• An INPT admission is defined by a patient requiring a hospitalization encompassing 2 MNs.
• The physician should order INPT admission “if he or she expects the beneficiary’s length of stay will exceed a 2‐MN benchmark or if the beneficiary requires a procedure specified as ‘INPT ONLY’.”
“Physicians should use a 24‐hour period as a benchmark, i.e., they should order admission for patients who are expected to need hospital care for 24 hours or more, and treat other patients on an outpatient basis.‖ Admissions…are not covered or non‐covered solely on the basis of the length of time the patient actually spends in the hospital.”
Medicare Benefit Policy Manual, Pub 100‐2, Chapter 1, Section 10
Expectation of 2 MN’s must be determined on admission by the Physician:
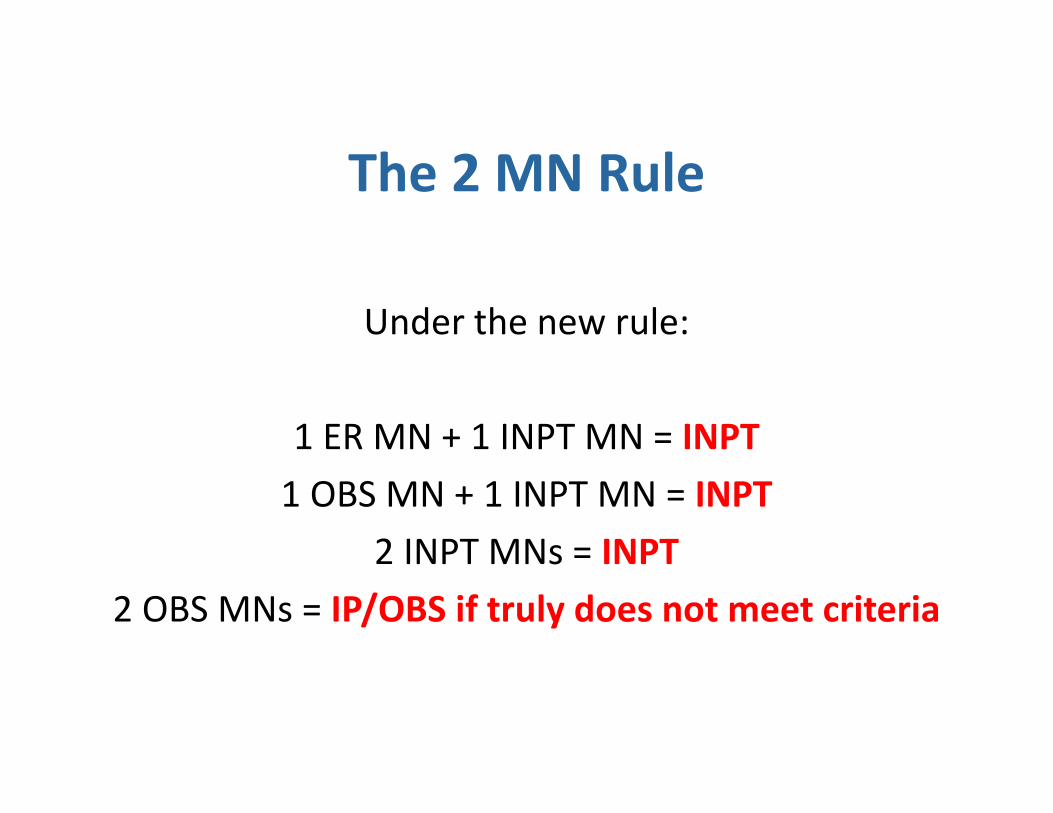
The 2 MN Rule
Under the new rule:
1 ER MN + 1 INPT MN = INPT1 OBS MN + 1 INPT MN = INPT
2 INPT MNs = INPT2 OBS MNs = IP/OBS if truly does not meet criteria
Severity of Illness is 2ndary to the time element
• Severity of illness must be met for the required 2 MNs in the hospital for IP LOC.
• An overnight ICU stay would be OBS unless the patient stays for a 2nd MN or clearly meets IP for that single MN.
• Deaths, transfers, and miracle cures depend on documentation.
Medical Necessity is not going away
• “…in order for payment to be provided under Medicare Part A, the care must be reasonable and necessary.”
• “The factors that lead a physician to admit a particular beneficiary based on the physician’s clinical expectation…must be clearly and completely documented in the medical record.”
• Any nationally recognized criteria can be used26
Observation Changes
OBS still <24 hours but:
• After 1 MN all OBS patients must be dischargedor advanced to INPT
• An OBS MN counts towards INPT• There should not be any 2 MN OBS – unless the medical necessity is not there for IP
SNF 3 Day Stay Rule ‐ Not Changed
• 3 medically necessary nights under inpatient status are still necessary for short term SNF coverage
• The inpatient stay is still calculated from the time of the IP admission order
• Even though a midnight spent as an outpatient may factor into a physician’s 2 midnight calculation and benchmark for inpatient status, it does not count as one of the medically necessary 3 inpatient nights to qualify for SNF or Subacute Rehab.
28
Physician Orders
• ED physicians can no longer writing a level of care holding order on MEDICARE patients (this does not apply to any other insurance) {later changed with provider pushback}
• Level of Care orders for MEDICARE patients can only be written by Attending/Hospitalist with staff privileges
• Residents in a teaching facility/GME program can write the order
• A verbal order can be received from the attending
Physician Order – Specific Language Required
For payment of hospital INPT services under Medicare Part A, the order must specify “admit to INPT”, “admit as an INPT”, “admit for INPT services” or similar language.
“Admit to ICU”, “Admit to PCU” are no longer acceptable – default to OBS.
Physician Documentation
• Physicians must document expectation of care spanning 2 midnights
• Certification of care (42 CFR§424.13)
• Appropriate order is required
• Reasons for hospitalization stated
• Diagnosis• Expected time the
patient will remain in the hospital
Inpatient order is critical under the new rule
• The rule emphasizes the need for a formal order• Unless a treating physician has written an order to admit the
patient as an inpatient, the patient is considered to be a hospital outpatient
• The order must specify the admitting practitioner’s recommendation to admit “to inpatient,” “as an inpatient,” “for inpatient services” or similar language. The words “admit” and “inpatient” must appear
• The order must be furnished by a qualified and licensed practitioner who has admitting privileges at the hospital as permitted by State law. The practitioner may not delegate the decision to another individual who is not authorized by the State to admit patients, or has not been granted admitting privileges by the hospital
32
The Case Manager’s Role
• Monitoring the patient for medical necessity while watching the clock
• Ensuring the correct MD order is in place as soon as possible (delay can cause loss of day for SNF transfer)
• Working with physicians to ensure documentation of the order and care is on the chart
Certification/Recertification
• Clarity in documentation is key:– Admission orders must be specific– H&Ps must certify the need for – INPT status– Progress Notes must recertify the continued need for INPT status
CMS Warning
CMS will assume that a hospital stay of at least 2 MNs qualifies as an INPT but…
…they have instructed their auditors to look for physicians/facilities who are “gaming” the system to generate INPT stays.
36
The healthcare community fights back
• Hospital and other professional associations have lobbied to influence the regulatory process
• Organizational feedback has influenced the regulatory language of the RAC process
• Case Management organizations have been on Capitol Hill lobbying for clarifications of the regulations
Open Door Forum Calls and Email
• Provider questions are many• Operationalizing the new rules are difficult• CMS responds with Open Door Forum Calls (ODF)
• Flooded with questions on the calls (literally thousands listening in)
• Provides an email address for questions
Providers Make a Difference• CMS keeps making changes:
• September 5, 2013• January 30, 2014• February 24, 2014
• Return to ED physicians OK to write LOC orders
• Increase number of exceptions for less than 2 MN inpatient stay
• Hold on RAC auditors reviewing claims
• Addition of “Probe & Educate” for CMS to review claims and provide feedback to providers
• Occurrence Span Code 72 remains optional – providers still trying to operationalize in coding process
• Clarification on physician documentation

Bills in Congress
• HR 1179 – Improving Access to Medicare Coverage Act of 2013 (Obsdays count towards SNF stay)
• S. 2082 – Two‐Midnight Rule Coordination and Improvement Act of 2014 (separate payment methodology for 2 MN stays)
• S. 1012 – Medicare Audit Improvement Act of 2013 (limits documentation requests by RACs)
Every one is talking about it…..
OIG: Hearings on Capitol Hill July 30, 2014 – “Admitted or Not? The Impact of Medicare Observation Status on Seniors”
American Hospital Association files federal lawsuits April 2014 challenging the rule and it’s reduction in payments to hospitals
The Center for Medicare Advocacy files a federal class action lawsuit in early 2014 on behalf of Medicare beneficiaries
Except….
Joint Commission – surveys for quality issues in hospitals, not payment issues
Impact on Hospital Revenues• CMS thought that IP stays would increase with the 2 MN
Rule….research is showing the opposite.
• “Observation and Inpatient Status: Clinical Impact of the 2‐Midnight Rule” published January 2014 in the Journal of Hospital Medicine found that the new rules have caused a net loss of 14.9% IP stays.
• A Obs. stay can average $4‐5K less than an IP stay decreasing hospital revenues.
• A procedure that does not appear on the CMS IP Only list is now more likely to be billed as OP regardless of associated risk to avoid RAC recoupment
“Observation care is a well‐defined set of specific, clinically appropriate services, which include ongoing short‐ term treatment, assessment, and reassessment before a decision can be made regarding whether patients will require further treatment as hospital inpatients or if they are able to be discharged from the hospital.”
Section 20.6, Chapter 6 of the Medicare Benefit Policy Manual (MBPM) (Pub. 100–02)
Resource: CMS definition of Observation Care

“An inpatient is a person who has been admitted to a hospital for bed occupancy for purposes of receiving inpatient hospital services. Generally, a patient is considered an inpatient if formally admitted as inpatient with the expectation that he or she will remain at least overnight and occupy a bed…”
Medicare Benefit Policy Manual, Pub 100‐2, Chapter 1, Section 10
Resource: CMS Definition of Inpatient

“The decision to admit a patient is a complex medical judgment which can be made only after the physician has considered a number of factors, including the patient's medical history and current medical needs, the types of facilities available to inpatients and to outpatients, the hospital's by‐laws and admissions policies, and the relative appropriateness of treatment in each setting.”
Medicare Benefit Policy Manual – Chapter 1, Section 10
Resource: Physician’s Decision to Admit as Inpatient
The 2014 IPPS Final Rule Federal Register / Vol. 78, No. 160 / Monday, August 19, 2013 / Rules and Regulations Section XI (pp. 1645 – 1851) Final Rule Home Page: http://www.cms.gov/Medicare/Medicare‐Fee‐for‐Service‐Payment/AcuteInpatientPPS/FY2014‐IPPS‐Final‐Rule‐Home‐Page.html
Resource: Internet Link for the 2 MN Rule
47
ALJ – Administrative Law Judge
DPP – Duplicate primary payment
CMS – Center for Medicare and Medicaid Services
CMD – Contractor Medical Director
MMA Medicare Monderization Act
FI – Fiscal Intermediary
CERT – Comprehensive Error Rate Testing
CMS Acronyms
48
HAC – Hospital Acquired Condition
MAC – Medicare Administrative Contractor
MAC – Medicare Appeals Council
MSP – Medicare Secondary Payor
RAP – Requested (for) Anticipated payment
PSC – Program Safeguard Contractor
ZPIC – Zone Program Intermediary Contractor
PIP – Periodic Intermediate Payment
CMS Acronyms
49
PPR – Potentially Preventable Readmission
OIG – Office of Inspector General
TIN – Tax Identification Number
NCD – National Coverage Determination
LCD – Local Coverage Determination
QIO – Quality Improvement Organization
VBP – Value Based Purchasing
CMS Acronyms
50
DCA – Documentation & Coding Adjustment
DAB – Departmental Appeals Board
ADR – Alternative Dispute Resolution
MOD – Medicare Operations Division
HIM – Health Information Management
DOJ – Department of Justice
ERRP – Error Rate Reduction Plan
CMS Acronyms
51
PPR – Potentially Preventable Readmission
OIG – Office of Inspector General
TIN – Tax Identification Number
NCD – National Coverage Determination
LCD – Local Coverage Determination
QIO – Quality Improvement Organization
VBP – Value Based Purchasing
CMS Acronyms
52
FFS – Fee for Service
HCPCS – Healthcare Common Procedure Coding System
NPI – National Provider Identifier
OMB – Office of Management and Budget
CMS Acronyms
53
This presentation is intended solely to provide general information and does not constitute legal advice. Attendance at the presentation or later review of these printed materials
does not create an attorney-client relationship with the presenter(s). You should not take any action based upon any information in this presentation without first consulting legal
counsel familiar with your particular circumstances.
54
Thank you for attending!
Questions??
Rose M. Turner, RN, BSN, ACM
5454