Embed Size (px)
Citation preview



To my mother Filijay T Sawo, and her mother Binta Touray (Kunjur),and her mother Touréngding Jamba,and her mother Bintou Danso, andher mother Khadija “Banna” and her mother Mai Touray.


List of Papers
This thesis is based on the following papers, which are referred to in the text by their Roman numerals. I Dabo F, Nyberg F, Qin Z, Sundström-Poromaa I, Åkerud H. Plasma
levels of beta-endorphin during pregnancy and use of labor analgesia. Reprod Sci. 2010; 17: 742-747.
II Dabo F, Grönbladh A, Nyberg F, Sundström-Poromaa I, Åkerud H.
Different SNP combinations in the GCH1 gene and use of labor analgesia. Mol Pain. 2010;6:41.
III Dabo Pettersson F, Grönbladh A, Nyberg F, Sundström-Poromaa I,
Åkerud H. The A118G Single nucleotide polymorphism of human µ-opioid receptor gene and use of labor analgesia. Submitted.
IV Dabo Pettersson F, Hellgren C, Nyberg F, Åkerud H, Sundström-
Poromaa I. Anxiety, depressed mood and the use of labor analgesia. Submitted.
Reprints were made with permission from the respective publishers.


Contents
Introduction ..................................................................................................... 9 Labor pain .................................................................................................. 9 Physiological response to pain during labor ............................................. 10 Labor pain and mental health ................................................................... 10 Labor analgesia ........................................................................................ 11 Measurement of pain ................................................................................ 13 Endogenous pain modulators ................................................................... 14 Single nucleotide polymorphism .............................................................. 19
Aims .............................................................................................................. 22
Material and Methods ................................................................................... 23 Study populations ..................................................................................... 23 Methods .................................................................................................... 25 Statistics ................................................................................................... 26
Results ........................................................................................................... 28 Study I ...................................................................................................... 28 Study II ..................................................................................................... 29 Study III ................................................................................................... 32 Study IV ................................................................................................... 34
Discussion ..................................................................................................... 36 Methodological considerations................................................................. 36
-endorphin and labor .............................................................................. 37 Studies of candidate genes; GCH1 and OPRM1 ...................................... 39 Mental health during pregnancy and labor ............................................... 41
Sammanfattning på svenska .......................................................................... 43
General Conclusions ..................................................................................... 45
Acknowledgements ....................................................................................... 46
References ..................................................................................................... 49

Abbreviations
ACTH Adrenocorticotrophic hormone ANCOVA Analysis of covariance ANOVA Analysis of variance BE -Endorphin BH4 6(R)-L-erythro-5,6,7,8-tetrahydrobiopterin (BH4) BMI Body mass index COMT Catechol-O-methyltransferase DNIC Diffuse noxious inhibitory control EDA Epidural analgesia GCH1 Guanosine triphosphate cyclohydrolase gene 1 GWA Genome wide association MADRS-S Montgomery-Åsberg depression rating scale (self- rated version) MC1R Melanocortin-1 receptor gene MOR Human -opioid receptor N2O Nitrous oxide OPRM1 Opioid receptor 1 gene (human) PAG Periaqueductal grey PBI Present behavioral intensity PCB Paracervical block PDB Pudendal nerve block POMC Pro-opio-melanocortin SIA Stress induced analgesia SNP Single nucleotide polymorphism STAI-T Spielberger state-trait anxiety inventory (trait version) TENS Transcutaneous electrical nerve stimulation VAS Visual analogue scale

9
Introduction
Labor pain Labor is considered to be one of the most painful events in human expe-rience and women often underestimate the pain they will experience (1). Many factors might influence the actual perception of pain i.e.; the size of the fetus, the duration of labor, cultural influences, previous painful expe-riences and the support the woman in labor receives. Endogenous pain mod-ulators are also involved in the overall experience of labor pain, both in phy-siological and psychological response to the exposure of pain (2, 3).
The character of labor pain changes across the first and second stage of labor (4). In the first stage of labor the pain mainly emerges from mechanical dis-tension of the lower uterine segment, mechanical dilation of the cervix and uterine-muscle contractions (5). Neurally, the uterus and the cervix are sup-plied by afferent neurons accompanying the sympathetic nerves, the uterine and cervical plexus, the aortic plexus, the middle, superior and inferior hy-pogastric plexus. Small unmyelinated visceral C-fibers (slow transmitters) conduct nociception (6). Contraction pain is referred to the dermatomes sup-plied by T10, T11, T12 and L1 (5).
Labor pain in the second stage of labor is caused by mechanical distension of the lower uterine segment and cervix (similar to the first stage) but pressure from the presenting part of the fetus within the pelvis is also of importance. Neuropathic pain is thought to develop from contact pressure by the present-ing part to the lumbosacral plexus (5). The second stage labor pain is charac-terized by a sharp, localized sensation in the perineal and recto-anal area, sometimes also in the lower extremities. A possible explanation to this sen-sation is traction and pressure in the urogenital organs, ligaments, muscles and fascia of the pelvic floor. This in turn stimulates the pudendal nerve originating from S2-S4. The stretching of vagina and perineum is transferred by myelinated rapidly transmitting A-delta fibers (6).

10
Physiological response to pain during labor Physiological responses to labor pain include hyperventilation and metabolic changes with increased catabolic activity based on rising levels of glucagon and growth hormone, and decreases in anabolic hormones such as insulin and testosterone (7). Other hormonal changes that follow as a response to labor pain are increased release of cortisol, adrenocorticotrophic hormone (ACTH) and -endorphin (BE) (8, 9). Moreover, in response to maternal stress increased levels of noradrenaline and adrenaline have been found (9-11). The importance of plasma catecholamines and cortisol for maternal stress during labor has been proven since epidural or spinal analgesia result in decreased levels (12). Other evidence of augmented sympathetic activity includes a progressive rise in peripheral resistance and increased cardiac output (10, 11). Furthermore, increased levels of circulating free fatty acids and lactate during labor has been reported (13).
Labor pain and mental health Emotional wellbeing and pain processing are intimately linked but has thus far most commonly been studied in the area of chronic pain. Longstanding and chronic pain has been shown to result in social isolation, depression and hopelessness (14, 15). Depression can render otherwise tolerable pain un-bearable (16), and notably, antidepressants acting on the monoaminergic systems are commonly used to treat chronic pain (17).
Numerous psychological factors, however, have been associated with la-bor pain including expectations (18, 19), coping strategies (20), partner or doula support (21, 22), support from caregivers, and involvement in decision making throughout labor (23).
However, few studies have evaluated antenatal depression and anxiety as possible predictors of labor pain experience. It has been hypothesized that anxious women may fear that pain experiences per se are threatening and harmful thus influencing the labor pain experience (24). A number of studies have suggested that prenatal anxiety or anxiety sensitivity is associated with expected, experienced and recalled pain during labor (18, 24, 25). Women with high scores of anxiety appear to be more inclined to use labor analgesia during the second stage of labor (26), whereas women with high depression scores received overall more pain relief during labor (27). In addition, preg-nant women with anxiety and/or depressive disorders appear to be more inclined to use epidural analgesia during labor (28). However, none of these studies adjusted for all factors that may influence use of labor analgesia.

11
Labor analgesia There are a number of different techniques for labor analgesia available and in Sweden almost all women are offered similar techniques, independent of where they give birth. Regional differences are, however, found for frequen-cy of use for some of the analgesics. The analgesic treatment during labor can briefly be categorized into the following groups; non pharmaceutical, inhalation, local anesthetic and neuraxial techniques.
Non-pharmaceutical techniques The non pharmaceutical techniques are analgesic treatments that do not in-volve any pharmaceutical products and are thought to act through the pa-tient’s endogenous pain relieving pathways. The non pharmaceutical me-thods used are transcutaneous electrical nerve stimulation (TENS), massage (29), water bath (30), intradermal sterile water injections, acupuncture and continuous support in labor.
Transcutaneous electrical nerve stimulation TENS is a low electric current administered through electrodes attached to the skin. It acts on the posterior roots of the nerves supplying the uterus (31). The mechanism of nociceptive neurons contending each other is called “counter irritation” (32), which is explained by stimulation of nerves in the skin sharing the same dermatomal distribution as the uterus. It might offer some pain relief in the first stage of labor but is scarcely sufficient as the only analgesia used (33-36).
Intradermal sterile water injections The intradermal sterile water injections entails that sterile water or saline is injected sub- or intracutaneously in the lower back and the sacrum. This offers the woman a stout but brief analgesia in the back or perineal area (37). The mechanism causing analgesia is thought to be based on pain inhibition from the periaqueductal grey (PAG) (32).
Acupuncture Acupuncture is a technique for pain relief based on ancient Chinese medi-cine. The technique is to manually insert acupuncture needles into acupunc-ture points and applying manipulations; twisting, pushing and pulling of the needle until the patient and acupuncturist both experiences the “De Qi” sen-sation (38, 39). Acupuncture is thought to work through mechanisms of en-dorphin release due to hypothalamic activation and altered levels of neuro-transmitters in the body (40). Acupuncture appears to be most effective in the first stage of labor (38, 39), but has a definite role in reducing pain (41) and may reduce the need of epidural analgesia (42).

12
Inhalation techniques Some centuries ago different inhalation methods were common for labor analgesia, but today there is only one left in use, nitrous oxide (N2O). N2O is administered through a mask held over the nose and mouth and is co-distributed with 50 – 70 % oxygen. N2O may be quite effective if the correct inhalation technique is used and if side effects as nausea and vomiting can be avoided. N2O is often used when neuraxial methods cannot be offered or when progress in labor is rapid. It is used by approximately 81.5 % of wom-en in labor (43).
Local anesthetic techniques
Paracervical nerve block Paracervical nerve block (PCB) offers pain relief by blocking the sensory and sympathetic nerves in cervix (44). It is applied as an injection of local anesthetics into the paracervical tissue and it is mainly used during the first stage of labor. PCB has a relatively short duration and the injection can be repeated once. The use of PCB is 1.2 % in laboring women (43).
Pudendal nerve block The pudendal nerve block (PDB) is used during the second stage of labor or after delivery when perineal injuries are sutured. Usage of PDB during the second stage of labor has decreased due to the increased use of EDA. PDB is used by 2.8% of women in labor (43).
Neuraxial anesthesia A number of different neuraxial techniques are available; i.e. continuous epidural anesthesia (EDA), combined spinal-epidural analgesia, patient con-trolled epidural analgesia and spinal anesthesia (45).
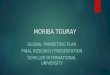
Epidural anesthesia EDA (Figure 1) is the most potent neuraxial anesthesia available. EDA acts through blocking the spinal segments of T11 and T12 and the sacral plexus (45). The woman in labor is commonly not offered EDA as the primary op-tion for labor analgesia. It is given as the second or third alternative after the effect of N2O has been evaluated.
It is the labor analgesia technique that provides the best pain relief and maternal satisfaction (46, 47). According to a relatively recent Cochrane review, epidural analgesia is associated with an increased risk of instrumen-tal vaginal birth but not caesarean delivery, long-term backache or low neo-natal Apgar scores at five minutes (46). However, in the Swedish context,

13
the introduction of bupivacaine and sufentanil EDA was associated with decreased rates of both instrumental vaginal deliveries and caesarean sec-tions (48-50). EDA is used by 30.2% of all Swedish women in vaginal deli-very (43), but the user frequency differs across the country, with most fre-quent use in Stockholm and middle-north of Sweden (51). Use of epidural analgesia in Sweden is associated with nulliparity, birth weight and a prenat-al belief that epidural analgesia will be needed (51, 52).
Figure 1. Epidural analgesia technique. Reproduced from Findley and Chamberlain, BMJ, 1999; 318: 927-930 with permission from BMJ Publishing Group Ltd.
Measurement of pain Pain is a highly subjective experience influenced by learning, context, atten-tion, and other psychological variables. Various methods are used to meas-ure pain including verbal and numeric self-rating scales, behavioral observa-tion scales, and physiologic responses, but none of them detain all the as-pects or dimensions of pain (53). Because pain is subjective, it has been ar-gued that self-reported pain provides the most valid measure of the experience (53, 54).
In clinical practice perhaps the most commonly used approach is the visu-al analogue scale (VAS). It consists of a 100 mm line, with descriptions of the pain attached to it. The scale ranges between “no pain” (0 mm) to “worst imaginable pain” (100 mm). The patient is instructed to put a mark on the

14
100 mm line, corresponding to how she rates the pain (54-56). VAS is an ordinal scale, meaning that a score of 4.0 is not necessarily twice as painful as the score of 2.0. Usually the rating is done before or after an event i.e. pain relief. The major limitation with the VAS is that is has to be done on paper, a ruler or electronically (57), but it is simple and can be used and as-sessed promptly.
Other self-reported methods available to measure pain are the verbal rat-ing scale and the McGill pain questionnaire. The verbal rating scale is also ordinal and includes adjectives to describe pain intensity; no pain, mild pain, moderate pain and severe pain (54, 58). The McGill pain questionnaire in-cludes not only questions concerning pain but also queries about the socioe-conomic situation. Moreover, the patient is asked to rank words describing the pain (59). Within the field of chronic pain the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials has recommended that additional core outcome domains should be assessed including physical and emotional functioning and patient satisfaction (60). Specific self-reported questionnaires for use in chronic pain have been developed but will not be addressed in this thesis.
Behavioral observation scales are most often used in patients who other-wise cannot express pain (patients with profound intellectual and severe motor disabilities, patients in anesthetic or intensive care, and neonatal in-fants) and include the Pain Behavior Checklist (61), the Iowa Pain Thermo-meter, Checklist of Nonverbal Pain Indicators (62), The Critical Care Pain Observation Tool (63), Pain Observation Scale for Young Children, Prema-ture Infant Pain Profile, the COMFORT behavior scale (64) and many more. The Present Behavioral Intensity Scale (PBI) can be assessed by the attend-ing midwife or obstetrician (65).
Physiologic responses to pain include blood pressure, heart rate, respirato-ry rate, and oxygen saturation. More recently, skin conductance has been introduced as an objective measure of pain in the neonatal (66) and post-operative units (67-70). The skin conductance level depends on the activity of the eccrine sweat glands (which reflects the output of the sympathetic nervous system) but has thus far only been sparsely used during labor (71). More advanced methods for establishing pain sensitivity and pain thresholds include, for instance, quantitative sensory testing with thermometry or pres-sure (72).
Endogenous pain modulators The physiological mechanisms of endogenous anti-nociception have been subject to numerous studies but are still not fully understood. Endogenous pain modulation is in part explained by the endorphins, but numerous other substances are of importance as well. Among the most well-known sub-

15
stances are found endocannabinoids (73), norepinephrine (74), substance P (75), neuropeptide Y (76), serotonin (77), dopamine (78), N2O (beyond ongoing use) (79) and oxytocin (80, 81).
The endorphins are anti-nociceptives that are released intra-cerebrally and spinally (80). Endorphins bind to the same receptors as and share similar analgesic effects with the opiates i.e. morphine, fentanyl and methadone (82). The endogenous opioids are of importance in regulating the organism’s response to physical and psychological stress. More than ten opioid peptides that derive from three different precursors of endorphin; pro-opiomelanocortin (POMC), pro-enkephalin and pro-dynorphin have been described (83). The opioid peptides bind with high affinity to the opioid receptors; -, - and -receptors.
-endorphin BE derives from POMC. The main production of BE takes place in the pitui-tary (anterior lobe) (84-86), the medial basal hypothalamus and nucleus commisuralis (87, 88). BE and ACTH are released simultaneously into the blood in response to stress and other ACTH-releasing stimuli. In peripheral tissue ACTH opposes the effects of BE and vice versa, but ACTH has in experimental studies, administered into brain tissue been shown to evoke analgesia (89).
BE binds to the - (also called the morphine receptor) and the -receptor, and in vitro it has a higher affinity for -receptors (89). The -receptor is found in the hypothalamic and thalamic nuclei, the PAG, and the median raphe nucleus. The -receptors are more prominent in the amygdala, nucleus accumbens, olfactory tubercle and the pontine nuclei (90).
-endorphin in labor and pregnancy It has been suggested that BE is of importance for pain modulation during pregnancy and labor (91). Furthermore, a study has indicated that women who exercise during pregnancy respond with increased BE levels and also report lower scores of pain during labor (92), whereas low BE levels were detected in patients with chronic stress and major depression (93, 94).
Few attempts have been made to relate BE levels at the end of pregnancy to clinical outcomes. A number of previous cross-sectional studies have as-sessed BE levels during pregnancy, (95-99) but only a few have included women longitudinally throughout pregnancy (100, 101). Both of the two latter longitudinal studies have reported gradual increases in BE plasma le-vels across pregnancy (100, 101), but sample size and time-frames for sam-pling were limited. The reason why BE levels increase during pregnancy (if they do) is not known, but it has been speculated that BE levels reflect in-creased stress at the end of a pregnancy or increased production from placen-tal tissue (92, 102).

16
Furthermore, a pronounced elevation of BE has been described during la-bor and the early postpartum period (99, 103). High levels of BE during labor has been hypothesized to relate to increased use of analgesia, increased distress, and vaginal delivery (as opposed to caesarean section) (92, 104).
Enkephalins and dynorphins Enkephalins are present in the anterior and posterior lobe of the pituitary, they are widely distributed in the central nervous system (i.e. the retina, vag-al nerve and the brain), the adrenal medulla and the gastrointestinal tract (105-107). Six opioid peptides derive from pro-enkephalin; [Met]enkephalyl-Arg-Phe, [Met]enkephalyl-Arg-Gly-Leu, [Met]enkephalyl-Arg-Arg-Val- NH2, leucine-enkephaline and methionine-enkephalin (83). They are present in the adrenals but in a smaller quantity also in the brain (82). The enkephalins have affinity for both - and -receptors (83).
Five opioid peptides arise from pro-dynorphin; -neo-endorphin, - neo-endorphin, dynorphin A, dynorphin B and dynorphin A (83). Dynorphins are mainly found in the anterior and posterior lobe of the pituitary, PAG and substantia nigra and analgesia is induced experimentally when injected into the spinal cord of rats (108). The dynorphins bind preferably to -receptors but unlike the other endorphins their effect is only partially reversible by naloxone (an opiate antagonist), indicating that their actions are not only mediated by opioid receptors (83).
Anti-nociceptive mechanisms mediated by the endorphins Endogenous modulation of pain is often described by the central descending regulation from the PAG, but also as stress-induced analgesia (SIA), diffuse noxious inhibitory control (DNIC), and placebo response. Endorphins are thought to be involved in all of these mechanisms. Placebo response, SIA and DNIC are completely or in part reversible by naloxone, thus indicating the involvement of the opioid-receptors (109-111). BE is the most potent endorphin and believed to be an important element in PAG-induced analge-sia, SIA, DNIC and placebo response.
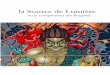
Pain is modulated via a descending tract (Figure 2) from the midbrain in the PAG via the rostral ventral medulla down to the dorsal horn of the spinal cord (80). The PAG is also interconnected with the cerebral cortex and the amygdala (Figure 2), areas that are of importance for experience and fear of pain (112). Afferent nociceptive fibers from peripheral parts of the body are relayed in the spinal dorsal horn. Impulses from the afferent nociceptors are inhibited by axons from PAG at the spinal level. In this descending tract (top-down pain modulation) -receptors are thought to be part of the inhibi-tory influence on the afferent nociceptors in the spinal cord. The effects of non steroid anti-inflammatory drugs and opioids are thought to act through the top-down pain modulation (111, 113). The PAG-induced analgesia has

17
been reproduced experimentally through electric stimulation of the neurons in the PAG where an increased level of endorphins in the cerebrospinal fluid is subsequently seen (89).
SIA is the term for a strong analgesia evoked by endorphins that are re-leased in response to a profound noxious stimulus. In order for SIA to be induced, the individual has to be under an extremely stressful condition and the pain stimulus has to exceed a certain threshold (80). The underlying me-chanism is unknown but it can be reproduced in experimental pain studies and is thought to explain painlessness in certain conscious multi-trauma pa-tients (89, 114).
DNIC corresponds to a peripheral noxious stimuli suppressing neuronal response to pain (115, 116). DNIC is believed to be inhibited in patients with chronic pain syndrome (117).

18
Figure 2. Top-down endogenous pain modulation. Reproduced from Ossipov et al, J Clin Invest. 2010; 120: 3779 – 3787, with permission of American Society for Clin-ical Investigation. LA-lateral amygdala, BLA - basolateral amygdala, CeA - central nucleus amygdala, PAG - periaqueductal gray, LC - locus coeruleus, RVM - rostral ventromedial medulla, DRt - dorsal reticular nucleus

19
Single nucleotide polymorphism Besides the role of endogenous pain modulation, a number of recent studies strongly suggest that genetic factors play an important role in the mechan-isms underlying the experience of pain (118-120).
Single-nucleotide polymorphisms (SNPs) are single base-pair alterations in the deoxyribonucleic acid (DNA) sequence and represent a major source of genetic heterogeneity. This heterogeneity will influence how people differ in their risk of disease or their response to drugs. About 10 million SNPs exist in human populations, where the rarer SNP allele has a frequency of < 5% (121).
In general, SNPs occur less often in coding regions of the genome than in non coding regions (122, 123). SNPs located in the regulatory sites of a gene can affect the rate of transcription, ultimately affecting the production of the specific encoded protein. When present in the coding regions, SNPs can cause alterations in protein structure and hence its function (124). The genet-ic variance due to a SNP may vary between different ethnic groups, because of population stratification, i.e. Africans and ethnic groups with proximity to Africa have more SNPs than some populations in North America, Asia and Europe (121).
An allele corresponds to a viable part of the DNA sequence located at a given locus on the chromosome. A set of associated SNP alleles in a region of a chromosome is called a haplotype. These closely linked genes are usual-ly inherited as a unit. The international HapMap project (http://hapmap.ncbi.nlm.nih.gov/whatishapmap.html.en) "tag" SNPs that uniquely identify these haplotypes are monitored with the purpose of identi-fying regions in the chromosomes that associate with specific diseases or behaviors.
SNP and pain sensitivity in humans Besides one genome-wide association (GWA) study in post-surgical pain (118), most interest has been devoted to candidate gene association studies. These candidate genes mainly fall into two categories; neurotransmission modulators and mechanisms that affect inflammation (119). Some of the most studied genes include the guanosine triphosphate cyclohydrolase 1 (GCH1) gene, the human opioid receptor 1 (OPRM1) gene, the melano-cortin-1 receptor gene (MC1R) and the catechol-O-methyltransferase (COMT) (125).
The opioid receptor -1 gene The OPRM1 gene encodes for the human -opioid receptor (MOR). The MOR is of importance in pain modulation, through stimuli from both endo-genous and exogenous substances. As the main receptor for BE, it is of im-

20
portance for the physiological and psychological response to stress, trauma and pain. The MOR also serves as a main receptor for opiates, in clinical practice morphine and other opiates, which are widely used for pain relief. Due to large individual differences in doses needed for pain relief and toler-ance of opiates, there is a need for increased knowledge about the mechan-isms regulating that.
A number of SNPs in OPRM1 has been hypothesized to be of importance for inter-individual differences in morphine-induced analgesia and pain sen-sitivity (126, 127). The OPRM1 A118G SNP has been shown to be of main relevance and in this specific polymorphism an adenine nucleotide is re-placed by guanine, which results in a change of asparagine to aspartate at position 40 in the µ-opioid receptor protein and a putative glycosylation site at the N-terminal part is eliminated (128). The gene is located on chromo-some 6, contains 4 exons and is 236371 base pairs (http://genome.ucsc.edu/). In vitro studies of the OPRM1 A118G SNP have indicated a three-fold in-crease in affinity and potency of BE on homozygous G allelic receptors (128). It has thus, been hypothesized that wild type OPRM1 carriers need more analgesia for pain relief and have lower pain thresholds and tolerance than the G-allele carriers (homozygous and heterozygous for A/G). In clini-cal studies, the specific polymorphism affects both subjective pain reporting and objective pain-related cortical activity (129). Opioid analgesic needs in chronic pain could also be affected by this polymorphism (130) and the re-quirement of intrathecal fentanyl analgesia in laboring women is influenced where the 118G allele carriers used lower levels of fentanyl suggesting that they are more responsive to opioids than wild-type A118 allele carriers (131). On the contrary, Wong et al could though not identify any association between duration of analgesia and treatment for breakthrough pain based on intrathecal opioid analgesia during labor and the A118G polymorphism of OPRM1 (132). Furthermore, individuals homozygous for the wild-type A118 allele required less morphine to manage early pain after total abdo-minal hysterectomy (133). Hence, the role of this polymorphism in influen-cing pain perception and analgesic requirement is controversial and not fully elucidated.
Guanosine triphosphate cyclohydrolase 1 It has been reported by Tegeder and colleagues that the pain-protective SNP combination of guanosine triphosphate cyclohydrolase gene 1 (GCH1) is associated with reduced pain sensitivity in humans (134). Guanosine tri-phosphate cyclohydrolase 1 is the rate limiting enzyme in the biosynthesis of 6(R)-L-erythro-5,6,7,8-tetrahydrobiopterin (BH4) (135, 136). BH4, in turn, is an essential cofactor in the synthesis of many pain modulators including catecholamines, serotonin and N20 (137) and feed-forward activation via phenylalanine and feedback inhibition through BH4 regulates the activity of GCH1 (138). The identified pain-protective SNP combination of GCH1 is

21
composed of 15 SNPs found at different locations on the gene (134). Recent-ly, screening for the combination of three SNPs has been shown to be suffi-cient for definition of the pain-protective haplotype with high sensitivity and specificity: c.-9610G > A, c343+8900A > T, and c.*4279 > G (139). The literature on the pain-protective SNP combination of GCH1 is conflicting and the pain-protective effect appears to be most evident in patients with neuropathic rather than nociceptive pain. Tegeder and colleagues (134) suggested that the pain-protective SNP combination of GCH1 is associated with less pain following discectomy for persistent radicular low back pain and their results have later been reproduced both by themselves (140) and by others (141). Further studies on the pain-protective SNP combination of GCH1 have been more discouraging.

22
Aims
I. to measure how plasma levels of BE vary during normal preg-nancy and to investigate whether plasma levels of BE in late pregnancy are associated with a number of pain related behaviors during labor.
II. to investigate if there is a clinically relevant association between the pain-protective SNP combination in the guanosine triphos-phate cyclohydrolase 1 (GCH1) gene and a number of pain re-lated behaviors during labor.
III. to investigate whether there is a clinically relevant association be-
tween the A118G polymorphism of the human opioid receptor -1 gene (OPRM1) and a number of pain related behaviors during labor.
IV. to assess if self-rated antenatal depressed mood and anxiety are
associated with pain related behaviors and self-reported pain dur-ing labor.

23
Material and Methods
Study populations
Study I Study I was based on a random sample from a cohort of healthy pregnant women (n = 469) with singleton pregnancies enrolled in gestational weeks 8 to 12, at five antenatal healthcare centers in Värmland County, Sweden. The women were followed longitudinally during pregnancy and plasma samples were collected at scheduled routine visits at the antenatal health care centers at gestational weeks 10, 25, 28, 33 and 37. The random sample consisted of women (n=45) with at least 4 blood samples (and at least 1 blood sample from gestational week 37) throughout pregnancy. Exclusion criteria were pregnancy complications such as hypertension or preeclampsia, known mal-formation of the fetus, premature labor, late onset of labor (after week 42 + 0), planned or acute caesarean section and induced start of labor or chronic diseases. In addition, women with subjective reports of pelvic pain in early pregnancy, daily use of analgesics, or drug abuse were excluded.
Study II-III Between March 1, 2007 and May 31, 2007 all women (age > 18 years) at-tending the 2nd trimester routine ultrasound screening at Uppsala University Hospital were approached for study participation. In Uppsala County, all routine ultrasound examinations are performed at Uppsala University Hos-pital which also is the only available delivery ward within the county. Hence, the study subjects represent a population-based sample. Among all eligible women, 814 (approximately 65% of eligible pregnant women during the inclusion period) accepted to participate in the study. Exclusion criteria at this point of the study were 1) detection of malformation or missed abor-tion at the ultrasound examination, 2) inability to read and understand the study information due to language difficulties, and 3) not providing informed consent.
Following the review of the medical records additional exclusion criteria were applied: Women delivering elsewhere, with intrauterine fetal death or gestational length < 30 weeks (< 33 weeks in paper III), planned or emer-gency caesarean section before onset of labor and non-Caucasian origin. The patient population of paper II-III is described in figure 3.

24
Figure 3. Flow-chart of the patient population of papers II and III. Numbers in parentheses refer to paper III where women delivering prior to gestational week 33 were excluded. One non-Caucasian women delivered prior to gestational week 33, thus reducing the number of non-Caucasians left to exclude in the flow-chart.
Study IV In the fourth and final study, 99 women in gestational weeks 37 to 40 were recruited through public maternity health care units in Uppsala County and through local newspaper advertisement. Healthy primiparous and multi-parous women above 18 years of age with an uncomplicated singleton preg-nancy were eligible for inclusion. The exclusion criteria were severe preg-nancy complications (pre-eclampsia, intrauterine growth retardation) and planned caesarean section.
In all studies demographic data and information on analgesia use during labor, together with other obstetric and delivery variables, were retrieved from the medical records of the parturients. Each participating woman gave her written informed consent and the studies were approved by the Indepen-dent Ethical Review Board at Uppsala University, Sweden.

25
Methods Sample collection In study I blood samples were collected in Litium/Heparin containing tubes and centrifuged for 10 min at 3000 rpm. Plasma was transferred into tubes and stored at -70ºC. In study II-IV blood samples were collected in tubes containing EDTA and the samples were centrifuged for 10 minutes at 5000 rpm. Plasma and buffy coat were separated and stored in new tubes at -70ºC.
Measurement of -endorphin in plasma To analyze levels of BE in plasma the radioimmunoassay (RIA) EURIA-beta-Endorphin kit (Euro-Diagnostica AB, Sweden) was used. This RIA is based on double-antibody precipitation. No levels were below the detection limits at any time point during pregnancy. All samples from each woman were run in duplicate and in the same assay to reduce variability. No levels were below the detection limit (10 pg/mL) at any time point during pregnan-cy.
DNA isolation study II-IV Total genomic DNA was extracted from whole blood using the Magtration 12GC system (Precision System Science, Chiba, Japan) and the Magazorb® DNA Common Kit-200 (Precision System Science, Chiba, Japan) as de-scribed earlier (142).
SNP analysis The different SNPs were determined by the TaqMan SNP genotyping assay (Applied Biosystems, Foster City, CA, USA). Applied Biosystems designed the target specific PCR primers and allele-specific TaqMan MGB probes (assay numbers GCH-1; C_25800745, C_1545138 and C_3044867, respec-tively, and OPRM-1; C 8950074 1) labeled with FAM and VIC. The assays were performed according to the manufacturer’s instructions. Administration of labor analgesia Labor analgesia (N2O, TENS, acupuncture, sterile water blocks, PCB, PDB and EDA) was administered according to the routines at the delivery ward. All types of analgesia were at available for the women in labor at all times. Details concerning the different kinds of analgesia used are presented in the manuscripts.
Labor Pain-Related Outcomes The primary labor pain-related behavior outcomes for the entire thesis were 1) stage of cervical dilation on arrival at the delivery unit and 2) use of any type of second line analgesia. Second line labor analgesia was defined as any use of more than one form of analgesia during labor. Following review of

26
paper I, it was specifically asked that we should use a slightly different out-come instead of second line analgesia i.e. need for additional pain medica-tion beyond N2O during labor (the change of outcome measure did not alter the results). Additional pain-related outcomes have been added in paper II and III, based on the request of the reviewers.
Visual Analogue Scores In study II-IV, each woman was asked to retrospectively rate labor pain (within 24 hours of delivery). Due to organizational difficulties and as wom-en were recruited while still pregnant, it was considered unfeasible to per-form prospective pain ratings during labor. On two visual analogue scales women rated labor pain prior to labor analgesia and during the last two hours of labor, irrespective of analgesia use. The scale measured from 0 to 100 mm where 0 equaled no pain and 100 represented worst possible pain. However, VAS scores were only returned by 337 of 676 women in study II –III (re-sponse rate 49.8 %), and for this reason, were not included in papers II – III. The results of the VAS scores have been added to the thesis as they provide valuable information of the outcome measures that were used and to the difficulties of measuring pain in the labor ward.
MADRS-S and STAI-T Women who participated in paper IV filled out the self-rated version of the Montgomery-Åsberg Depression Rating Scale (MADRS-S) (143) and the trait version of the Spielberger State-Trait Anxiety Inventory (STAI-T) (144) 14 days prior to expected delivery. Depressed mood was defined as a score
11 on the MADRS-S scale (143). A STAI-T score > 40 was used to indi-cate increased anxiety levels (144, 145). Both of these scales are commonly used in studies of pregnant women, and are available in validated Swedish versions (the MADRS-S was originally made in Sweden).
Statistics
Study I Comparisons of BE plasma levels between different gestational weeks were made with repeated measures analysis of variance (ANOVA). Two different ANOVAs were made, one including all samples throughout pregnancy and the other including the third trimester samples. Multivariate logistic regres-sion analysis was used to calculate adjusted odds ratios (AOR) for need for additional pain medication beyond N2O during labor, with third trimester BE levels, together with a number of confounding variables, as independent variables.

27
Study II-III Demographic and obstetric variables were compared between homozygous, heterozygous and non-carriers of the pain-protective SNP combination of GCH1 by one-way ANOVA and Tukey HSD or Chi-square tests. Any sig-nificant differences between groups were adjusted for relevant confounders by analysis of covariance (ANCOVA) or multivariate logistic regression. Demographic and obstetric variables were compared between non-carriers and G-allele carriers of the OPRM1 A118G SNP using Student’s T-test and Chi-square tests.
Multivariate linear (cervical dilation at arrival to the delivery unit) and lo-gistic (use of second line analgesia) regression models were composed to address the influence of the different SNPs.
Study IV MADRS-S and STAI-T scores were analyzed by Mann-Whitney U-test, as assumption of normal distribution was not met. Multivariate linear (cervical dilation at arrival to the delivery unit) and logistic (use of second line anal-gesia) regression models were composed.
The statistical analyses are described in further detail in each paper. All statistical analyses were performed by the Statistical Package for the Social Sciences (SPSS) 18.0 for Windows software package.

28
Results
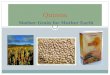
Study I Levels of BE during pregnancy decreased significantly in gestational weeks 28 and 33 compared to gestational week 10 (14.4 and 14.4 pg/mL compared to 16.6 pg/mL, p< 0.001 and p < 0.01, respectively, Figure 4). A significant increase in BE level between week 28 and 37 was noted, p < .01. However, there was no difference in plasma concentrations of BE between gestational weeks 10 and 37.
Stepwise multivariate logistic regression of the results with use of labor analgesia other than N2O as the outcome variable and BE levels and possible confounders as predictor variables were performed. The
Figure 4. Mean ± SD levels of BE at different gestational weeks among women with complete blood sampling (n = 38). *** Significant decrease in gestational week 28 compared to gestational week 10, p<0.001. **Significant decrease in gesta-tional week 33 compared to gestational week 10, p<0.001. # Significant increase in BE levels between gestational week 28 and week 37, <0.01.

29
Table 1. Factors associated with need for additional pain medication beyond N2O during labor Variables Unadjusted OR
(95 % CI) Adjusted OR
(95 % CI) Parity Primipara 1 1 Multipara 0.20 (0.06 – 0.72) 0.39 (0.06 – 2.52) Age, years 1.00 (0.88 – 1.14) Pre-pregnancy BMI < 25.0 kg/m2 1 1 > 25.0 kg/m2 4.64 (1.24 – 17.4) 3.88 (0.54 – 28.0) Dilation of cervix at arrival to labor ward, cm
0.62 (0.44 – 0.89) 0.53 (0.31 – 0.91)
Duration of labor, hours 1.92 (1.28 – 2.89) Use of oxytocin during deliv-ery
No 1 1
Yes 1.49 ( 1.01 – 2.07) 1.44 (0.82 – 2.50) Gestational week, weeks 1.50 (0.80 – 2.82) Smoking No 1 Yes 0.79 (0.19 – 3.31) Low BE levels 1 Reference 1 1 LQ 11.5 (2.12 – 62.3) 18.67 (1.53 – 227) 1 Subjects in the lowest quartile (LQ) of BE levels compared to the other quartiles at gestational week 37. Marital status, ethnicity, labor onset, fetal presentation, delivery were not considered in the model because of the homogenous study group. Duration of labor was not entered in the final model as it correlated with cervical dilation at arrival to the labor ward. However, the odds ratio for low BE levels was not significantly altered by entering or not entering duration of labor to the final model. multivariable logistic regression analysis indicated that women within the lowest quartile of BE levels at gestational week 37 required labor analgesia other than N2O to a significantly higher extent, and this finding remained after adjustment for possible confounders such as parity, duration of labor, cervical opening upon arrival at the delivery unit and use of oxytocin during labor (Table 1).
Study II Among the 676 Caucasian subjects who had complete data on the SNP ana-lyses in the study population, 15 (2.2%) were homozygous carriers, 180 (26.6%) heterozygous carriers and 481 (71.1%) were non-carriers of the pain-protective SNP combination of GCH1. Homozygous carriers, hetero-zygous carriers and non-carriers of the 3 SNPs used were in accord with the Hardy-Weinberg equilibrium. There were no major differences in socio-demographic and clinical variables between groups.

30
Table 2. Labor pain related behavioral outcomes according to GCH1 SNP combina-tions
Non-carriers
(n = 481)
Heterozyg-ous
(n = 180)
Homozygous
(n = 15)
Cervical dilation at arrival to the delivery unita, cm
4.3 ± 2.5
4.1 ± 2.3
5.7 ± 2.2*
Cervical dilation at request of epidural analgesiab, cm
5.8 ± 1.9 5.3 ± 2.0 6.3 ± 2.3
Use of labor analgesia, n (%) No use 44 (9.1 %) 17 (9.4 %) 1 (6.7 %) N2O 396 (82.3 %) 143 (79.4 %) 12 (80.0 %) Acupunc-
ture 155 (32.2 %) 62 (34.4 %) 6 (40.0 %)
Epidural analgesia
159 (33.1 %) 52 (28.9 %) 7 (46.7 %)
Second line analgesia
249 (51.8 %) 92 (51.1 %) 11 (73.3 %)
*p = 0.033 in comparison to heterozygous carriers and non-carriers of the GCH1 SNP combination, ANOVA adjusted for parity. a Data missing in 81 subjects. b Data based on 159 non-carriers, 52 heterozygous and 7 homozygous carriers of the GCH1 SNP combination.
Homozygous carriers of the pain-protective SNP combination of GCH1 ar-rived in the delivery ward with a more advanced stage of cervical dilation than subjects heterozygous for the pain-protective SNP combination of GCH1 and non-carriers did, adjusted for parity (Table 2).
A possible association between the pain-protective SNP combination of GCH1 and use of second line analgesia was suggested by the bivariate anal-ysis (p = 0.10). This possible association was further analyzed with adjust-ment for confounders in a multivariate logistic regression model. In the biva-riate analyses nulliparity, induced labor, cervical dilation upon arrival in the delivery unit, and duration of labor were associated with second line labor analgesia. Independent explanatory factors for use of second line labor anal-gesia use were nulliparity, dilation of cervix < 2 cm at arrival to the delivery unit and duration of labor for more than 2 hours.
Multivariate logistic regression indicated that homozygous carriers of the pain-protective SNP combination of GCH1 had an increased risk of using second line labor analgesia (OR 5.1, 95% CI, 1.09-23.96), whereas hetero-zygous carriers did not differ in this aspect from non-carriers (Table 3).

Tab
le 3
. Fac
tors
ass
ocia
ted
wit
h us
e of
sec
ond
line
labo
r an
alge
sia
Use
of
seco
nd li
ne
labo
r an
alge
sia
U
nadj
uste
d O
R
95
% C
I
Adj
uste
d O
R
95
% C
I
Par
ity
Par
ous
130
(34.
9 %
) 1
1
Nul
lipa
rous
22
2 (7
3.3
%)
5.12
***
3.67
– 7
.14
2.68
***
1.73
– 4
.16
H
eigh
t
0.
98
0.96
– 1
.00
0.98
0.
96 –
1.0
0
Sta
rt o
f la
bor
Spo
ntan
eous
29
1 (5
0.2
%)
1
1
In
duce
d 61
(63
.5 %
) 1.
73*
1.11
– 2
.70
0.63
0.
32 –
1.2
3
Cer
vica
l dil
atio
n at
arr
ival
to th
e de
live
ry u
nit,
cma
> 5
83
(36
.9 %
) 1
1
0.79
– 0
.97
2-
4 17
8 (5
6.9
%)
2.26
***
1.59
– 3
.20
1.34
0.
85 –
2.1
3
0-1
45 (
78.9
%)
6.42
***
3.21
– 1
2.82
2.
46*
1.05
– 5
.76
Dur
atio
n of
labo
rb 0-
2 ho
urs
32 (
17.6
%)
1
1
2-
5 ho
urs
74 (
45.1
%)
3.85
***
2.36
– 6
.29
3.33
***
1.92
– 5
.80
5-
10 h
ours
10
9 (6
6.1
%)
9.12
***
5.54
– 1
5.03
7.
13**
* 3.
87 –
13.
13
>
10
hour
s 13
4 (8
7.0
%)
31.4
1***
17
.14
– 57
.53
16.5
3***
7.
68 –
35.
62
G
CH
1 pa
in p
rote
ctin
g ge
noty
pe
Abs
ent
249
(51.
8 %
) 1
1
Het
eroz
ygou
s 92
(51
.1 %
) 0.
97
0.69
– 1
37
1.25
0.
80 –
1.9
7
Hom
ozyg
ous
11 (
73.3
%)
2.56
0.
80 –
8.1
6 5.
11*
1.09
– 2
3.96
a
Mis
sing
cas
es 8
1, b
Mis
sing
cas
es 1
1

32
Study III Genotyping was successful in 672 of 675 included cases. Of these, 541 (80.5%) were homozygous carriers of AA, 119 (17.7%) were heterozygous carriers (AG) and 12 (1.8%) were homozygous carriers of GG. The number of homozygous carriers, heterozygous carriers and non-carriers of the OPRM1 A118G SNP were in accord with the Hardy-Weinberg equilibrium. All women included, were assigned to two groups according to genotype. Non-carriers (n = 541) corresponded to homozygous carriers of the wild-type allele (AA), and the G-allele group (n = 131) were heterozygous and homozygous carriers of the 118G allele.
No significant differences in socio-demographic variables or obstetric outcomes were found between non-carriers and G-allele carriers. However, induced labor tended to be more common in G-allele carriers, why subse-quent analyses on pain-related outcomes only have included subjects with spontaneous start of labor.
Labor pain-related outcomes for non-carriers and G-allele carriers with spontaneous start of labor are shown in Table 4 and 5. Following adjustment for parity, no differences in cervical dilation on arrival at the delivery unit or cervical dilation at request of epidural analgesia were detected.
A multivariate logistic regression model was performed and odds ratios adjusted for parity, height and duration of labor were calculated. As seen in Table 5, no association between G-allele carriers and use of N2O, acupunc-ture, epidural, morphine, second or third line analgesia was identified.
Table 4. Labor pain behavior related outcomes and the OPRM1 A118G SNP of in the 577 women with spontaneous onset of labor
Non-carriers
G-allele carriers
pa
Cervical dilation at arrival to the
delivery unit, cm
4.5 ± 2.4 4.7 ± 2.6 0.02 0.62
Cervical dilation at request of epi-
dural analgesia, cm
5.9 ± 2.0 5.9 ± 1.3 -0.02 0.83
aLinear regression, adjusted for parity

33
Table 5. Use of labor analgesia and the OPRM1 A118G SNP
Non-carriers
(n=471) G-allele carriers
(n=106) OR (95% CI)
No use 46 (9.8 %) 10 (9.4%) 1.23 (0.55 – 2.78 ) Nitrous oxide 391 (83.0 %) 85 (80.2 %) 0.84 (0.48 – 1.49) Acupuncture 149 (31.6 %) 33 (31.1 %) 1.04 (0.64 – 1.69) Epidural analgesia 147 (30.2 %) 33 (31.1 %) 1.23 (0.69 – 2.20) Second line analgesia 218 (46.3 %) 51 (48.1 %) 1.31 (0.77 – 2.24) Third line analgesia 61 (13.0%) 12 (11.3%) 0.99 (0.48 – 2.05)
OR; Odds ratio (adjusted for parity, height and duration of labor), n.c. not calculated
Addendum to study II and III Median VAS ratings prior to labor analgesia and during the last two hours of labor were 74 mm (0 – 100 mm) and 81 mm (2 – 100 mm), respectively. Both scores, but especially the VAS scores during the last two hours of la-bor, were highly skewed towards the higher end of the scale. Self-rated pain prior to labor analgesia was significantly higher among women who subse-quently used second-line analgesia (first line analgesia users median 71 mm (0 – 100 mm) vs. second line analgesia users median 77 mm (16 – 100 mm), p < 0.05), but there was no difference between these groups during the last two hours (median 80 (9 – 100 mm) vs. 83 (2 – 100 mm), respectively). The latter finding, however, was significantly influenced by the use of epidural analgesia during the final stage of labor, Table 6.
No differences in self-rated pain between carriers or non-carriers of the pain-protective SNP combination of GCH1 or 118G allele of OPRM1 were found. Table 6. Retrospectively self-reported pain according to use of labor analgesia, median (range) None or first-line
analgesia only
n = 177
Second-line analge-sia other than epidur-
al analgesia n = 65
Epidural analgesia
n = 100 Pain during last two hours of labor, mm
80 (9 – 100)
90 (31 – 100)***
80 (2 – 100)

34
*** p < 0.001 in comparison with none or first-line analgesia users and epidural analgesia users, Kruskal-Wallis followed by Mann-Whitney U-test.
Study IV Of the 99 women included in the paper IV, one subsequently underwent a planned caesarean section and one woman was lost to follow-up as she deli-vered elsewhere. Among included women, 83 (85.6 %) had a spontaneous onset of labor and were evaluated in the analysis on cervical dilation at ar-rival to the delivery department, whereas the entire study group were in-cluded in the aims on second line analgesia. Sixteen (16.5 %) subjects had MADRS-S scores 11, indicating depressed mood but none scored above 20 which would indicate possible major depression. Only ten (10.3 %) sub-jects had STAI-T scores > 40, indicating increased anxiety.
Explanatory factors for stage of cervical dilation at arrival to the delivery unit are displayed in Table 7. Following adjustment for BMI and parity the MADRS-S score was significantly associated with cervical dilation at arrival to the delivery department.
Women who used second line analgesia reported higher scores on the MADRS-S (7.1 ± 4.1 vs. 5.4 ± 4.1 in none or first line users, p < 0.05) but did not differ in anxiety ratings. However, when adjusted for parity, BMI, gestational length, duration of labor and the pain-protective SNP combina-tion of GCH1, the association between MADRS-S score and use of second line analgesia was lost, Table 8. Together with body mass index and duration of labor, GCH1 remained a significant explanatory variable for use of second line analgesia.
No differences in visual analogue ratings of pain were found between women with depressed mood (MADRS-S 11) and women with MADRS-S scores in the normal range. Women with high anxiety levels (STAI-T > 40) reported increased self-rated pain prior to labor analgesia in comparison with women who had anxiety scores in the normal range (88 mm (61 – 100 mm) vs. 72 (11 – 100 mm) in non-anxious women).

35
Table 7. Multivariate linear regression analysis on factors associated with cervical opening at arrival to the delivery department in 83 women with spontaneous onset of labor Model 1 Model 2
P
p
Parous subjects
0.213 0.053 0.196 0.07
BMI -0.234 0.034 -0.165
0.14
MADRS-S scores -0.254 0.021
Model 1: R2 = 0.08, Model 2 R2 = 0.14 Table 8. Multivariate logistic regression of variables increasing the risk of using second line analgesia (n = 97)
Odds ratio
95 % CI
p
Nulliparity
1.47
0.44 – 4.92
ns
BMI 1.17 1.01 – 1.36 0.05 Gestational week at labor 0.99 0.65 - 1.54 ns Duration of labor < 5 hours 1 > 5 hours 2.82 1.56 – 5.10 0.001 MADRS-S (total) 1.05 0.94 - 1.19 ns pain-protective SNP combi-nation of GCH1
Non-carriers 1
Heterozyg-ous/homozygous
3.51
1.18 – 10.4 0.05
Nagelkerke R2 = 0.38, CI confidence interval

36
Discussion
Methodological considerations Safe pain relief with the highest maternal satisfaction for each parturient is central in obstetric care. Labor analgesia is nowadays, in our country, avail-able for all women at the delivery units, but not all women are satisfied and do suffer from labor pain. To enable individual counseling on labor analge-sia the possibility to identify candidate genes or genetic variants that regulate endogenous pain mechanisms would be of importance. In our work we have investigated a number of labor pain related outcomes and their association with endogenous pain modulation, different genes and SNPs of interest.
Labor pain-related behavior Pain is a highly subjective experience. Various methods can be used to measure pain, but no single measurement will cover all aspects of pain (53). For this thesis, two primary pain-related endpoints were used, namely stage of cervical dilation on arrival at the delivery unit and use of any type of second line analgesia. These outcomes were chosen as information was rea-dily available in the majority of the medical records. Vaginal palpation for assessment of cervical dilation, effacement and fetal station is performed at the arrival to the labor ward or before induction of labor. It is furthermore often done when epidural analgesia is requested. Amount and type of labor analgesia used is documented in the medical records and our definition of second line analgesia was any use of more than one type of analgesia during labor. By using this definition a larger cohort than women who ask for EDA was included in the analysis. However, these measures are confounded by a number of variables, some of which may not have been accounted for in this work.
Cervical stage at arrival to the delivery department was in our studies af-fected by parity, depressed mood, and (in one of the study populations also by BMI in the bivariate analysis). Besides the fact that data on depressed mood was not available for subjects in paper II and III, residual confounding may have included distance from the hospital, family support, and previous experience of rapid labor or history of obstetric complications. The useful-ness of cervical stage as a measure of pain is, however, supported by a prior study where prospective pain ratings on the short form of the McGill pain

37
questionnaire were used (4). According to the findings of Capogna and col-leagues, mean intensity of pain increased as cervical dilation increased in both nulliparous and multiparous women.
Second line analgesia was influenced by parity, height (BMI in paper IV), labor, cervical stage at arrival to the delivery department, duration of labor, onset of and use of oxytocin. The latter four variables are confounded and in paper III and IV, only duration of labor was used in the final analysis. The usefulness of second line analgesia as a measure of pain is strengthened by the visual analogue scores, where women in need of second line analgesia rated more severe pain prior to labor analgesia than women who used no or only first line analgesia. Clearly, the studies would have been improved if prospective and subjective measures of pain, at defined stages of labor (on admittance, before first line analgesia, before second line analgesia and so forth) had been included. In addition, behavioral observation scales, such as the PBI can be assessed by the attending mid-wife (65).
All women in this thesis were included while still pregnant. This proce-dure precluded the use of the visual analogue ratings in paper II and III, as more than half of women forgot to bring their pain-scales to the delivery unit when labor started. Clearly, in paper IV, where women were included much later in pregnancy, the visual analogue scores were remembered and filled out by the majority of subjects. Although the usefulness of the visual analo-gue scales were hampered, the inclusion of subjects already during pregnan-cy may have its’ advantages. Had women been included at admittance to the delivery unit, informed consent would have been taken while women were in pain, which may not be ethical. In addition, inclusion upon admittance would presumably target women with less behavioral pain.
Arbitrary power analyses were conducted prior to each of the studies. However, in the case of paper II, the sample size nevertheless became insuf-ficient as the homozygous carriers of the pain protective SNP combination of GCH1 were few. The study population of paper II and III is also far more heterogeneous (in terms of the labor variables) than the other two study pop-ulations, and in retrospect, it would have been wise to apply more strict in-clusion criteria for the study such as nulliparity and planned vaginal deli-very.
-endorphin and labor Although a large part of the research regarding BE has decreased in recent years, they are as ever present in the discussion of endogenous pain modula-tion(146), mood (93, 94) and consequently in labor (92).
In our study, where women were included prospectively and followed longitudinally during pregnancy, we confirmed prior results indicating an increase in plasma levels of BE during the third trimester (100, 147), but

38
failed to detect any difference in BE between the first and third trimester. Furthermore, our findings also indicated that low levels of BE at the end of pregnancy are associated with increased usage of second line analgesia.
A number of previous cross-sectional studies have assessed BE levels throughout pregnancy (95-99), but only two of them have used a longitudin-al design (100, 101). In a small study comprising 10 pregnant women, Browning and co-workers reported gradually increasing levels of BE throughout the course of pregnancy, with the increase starting already at gestational week 16-20 (100). We were unable to replicate the findings of Browning and colleagues but, in line with two previous studies (101, 148), we found a subsequent increase during the third trimester. Given the sub-stantially larger sample size of the present study, our estimates of BE levels throughout the course of pregnancy are more valid than prior cross-sectional and relatively small longitudinal studies.
The significant decrease of BE levels in gestational weeks 28 and 33 compared to gestational week 10 is in line with previous cross-sectional studies (97) and could possibly be due to the successive increase in blood volume of pregnant women, which is known to occur at the end of the second trimester. The subsequent increase of BE in late pregnancy might, in turn, be a result of increased stress at the end of pregnancy but could also be due to increased production of BE from placental tissue (101, 149). Very few attempts have been made to relate BE levels at the end of pregnan-cy to clinical outcomes. The association between low levels of BE in plasma at gestational week 37 and increased use of second line analgesia is in agreement with a previous study by Sandman and colleagues (147), who reported that plasma levels of ACTH and BE increase in the third trimester of pregnancy and that these factors are co-released from gestational week 27-29 until delivery. However, this co-release pattern between ACTH and BE was disrupted in women who subsequently used conduction analgesia during labor (147). An even more pronounced elevation of endorphins has been described during labor (99, 103) and high BE levels during labor has been related to increased use of analgesia (94, 104). In addition, a negative correlation has observed between self-reported pain in labor and the post-partum BE levels (150). However, the relationship between low BE levels in gestational week 37 and increased use of second line labor analgesia is most likely mediated through factors, other than pain-modulation, of importance for labor analgesia use such as general level of physical activity during preg-nancy (92, 151) or BMI (152-154).
While there appears to be an association between BE and major depres-sion, it is rarely demonstrated as a simple deficit or excess (93, 155). In con-trast, high levels of BE throughout pregnancy is associated with increased risk for postpartum depression (156), hypothetically mediated through a more pronounced BE withdrawal following delivery (27, 157, 158).

39
Studies of candidate genes; GCH1 and OPRM1 Two categories of potential genetic pain-perception pathways have been described, where neurotransmission modulators and mechanisms that affect inflammation are of main importance. The pain-related genes mainly dis-cussed in the literature interact with specific receptors and signaling down-stream of the receptor, modulation of opioid effects, metabolism and trans-port (119). The genes studied by us are pain-related genes known to be of interest in the clinic and they were specifically chosen as they have been proposed to be candidate genetic markers for pain perception and for indi-vidual sensitivity to analgesics.
The results from study II indicated that the pain-protective SNP combina-tion of GCH1 may be of importance in a limited number of homozygous carriers during the initial dilation of cervix, but upon arrival at the delivery unit these women are more inclined to use second line labor analgesia. Intri-guingly, the latter finding was partly replicated in paper IV where hetero- and homozygous carriers more often used second line analgesia than non-carriers.
Previous studies of the pain-protective SNP combination of GCH1 have been conflicting. The pain-protective effect appears to be most evident in patients with neuropathic rather than nociceptive pain. Tegeder and col-leagues (134) suggested that the pain-protective SNP combination of GCH1 is associated with less pain following discectomy for persistent radicular low back pain and their results were later been reproduced both by themselves (140) and by others (141, 159). Further studies on the pain-protective SNP combination of GCH1 have been more discouraging. Kim and colleagues (160) found no association between rated pain severity after surgical remov-al of molar teeth and the pain-protective SNP combination of GCH1, and similar negative findings were obtained in patients with chronic pancreatitis (161). The pain-protective SNP combination of GCH1 may also have a role in chronic pain as it has been shown to delay the need of opioid treatment in cancer patients (162). The negative results in our study could be due to the fact that labor pain is mainly nociceptive or that pain modulating pathways affected by BH4 are not the primary ones during labor (134). A more spe-culative explanation is, however, that the pain-protective SNP combination of GCH1 has a bimodal effect. In situations with low-intensity pain, patients are less sensitive, whereas in situations with intense pain (as labor) the pain-protecting effect conferred by the SNP combination is altered. Yet another alternative speculation is that women with inherited pain protection have been less exposed and used to pain, and are thus more inclined to request analgesia when pain intensity exceeds a certain threshold.
In study III no association between homozygous OPRM1 G-allele carriers and labor pain-related behavior was detected. Previous research findings in

40
this field are diverse and the relevance of this polymorphism seems to be most evident in studies dealing with exogenously supplied opiates and pain perception (131, 163-165). This might partially explain our negative results but another reason for the lack of results in our study could be due to the somewhat blunt measures of pain perception and pain behavior that were used. Obviously, a difference in pain-related behavior depending on a geno-type related to the function of the µ-opioid receptor is bound to involve treatment response to opioids. When this study was planned, additional out-come measures were incorporated, including the total sufentanil dose (or dose rate). However, this information turned out to be difficult to ascertain in many cases and could thus not be used. However, the relevance of positive findings in studies dealing with genetic polymorphisms in clinical settings is sometimes at risk of being overestimated (166, 167). The nature and range of genetic modulation of pain has thus far not been adequately addressed. Due to the limited number of patients in the studies (126, 127, 141, 159) per-formed as well as the limited number of genes and genetic variants investi-gated, the complete understanding of the relevance of genetic variants for personalized analgesic treatments is not ruled out. More studies in this area are needed and hopefully collaborations in larger research groups or consortia might allow projects where a large number of patients can be included and projects as part of i.e. the HapMap project might improve the capacity. Complex physiological mechanisms such as pain modulation might be subject to GWA studies where 1 000 000 markers or more markers in the genome is analyzed instead of one specific SNP or haplotype. The advantage of GWA studies are that the influence of linkage disequilibrium is taken into consideration, since genes that are in close prox-imity of the studied gene also are observed (168). Thus far, the only genome-wide approach in acute pain research (118) has focused on response to non-steroidal anti-inflammatory analgesics in post-surgical pain (for GWA stu-dies in chronic pain, see for instance (169, 170)). The study revealed a can-didate SNP associated with analgesic onset, which was in linkage disequili-brium with a gene encoding a zinc finger protein (118). The study, however, included an extremely limited number of patients (n = 112), that it may be expected that further studies in this area is underway.
Obvious strengths in study II-IV are that the cohort is relatively homo-genous study population where Caucasians dominate and the population-based design. In fact, the population based model is considered more robust when studying specific genes of interest, whereas case-control models are recommended only when a larger sample size is included (171). The homo-genous population reduces the risk of incorrect genetic associations since population stratification is avoided (118).
There is a need for increased information on how labor pain is regulated, and possibly the 8 - 10% of all women who seem to endure labor without

41
any exogenous analgesia at all, should be specifically studied in future stu-dies.
Mental health during pregnancy and labor The main finding of study IV was that antenatal self-rated depressed mood is associated with early arrival to the delivery department. Women with in-creased STAI-T scores reported higher self-rated pain prior to labor analge-sia, which might indicate that antenatal anxiety is associated with increased self-rated pain prior to labor analgesia.
Previous studies regarding mental health and pregnant women has mainly focused on antenatal depression and perinatal outcomes such as preterm labor and low birth weight (172, 173). Depression and anxiety during preg-nancy will also impact on a number of health-related behaviors and obstetric outcomes. For instance, it has previously been shown that antenatal depres-sion and/or anxiety is associated with nausea, sick-leave, premature contrac-tions, planned caesarean section, use of epidural analgesia, and self-experienced longer duration of labor (28). The current study also emphasizes that pain-related behavior and self-reported pain during labor may be af-fected by antenatal depressed mood and anxiety. Antenatal depressed mood was primarily associated with a less advanced stage of cervical dilation at arrival to the delivery department, but as discussed previously, this pain-related behavior may be confounded by factors which were not accounted for. We were not able to replicate prior findings that depressive disorders are associated with increased use of epidural analgesia or second line analge-sia (28). Previous studies in this area have, however, had a different focus with obstetric complications as primary outcome in relation to depression or depressed mood, and relevant adjustment for factors contributing to use of labor analgesia (such as duration of labor) were not considered (26, 27).
Antenatal anxiety, measured as trait anxiety levels near term pregnancy did not influence any of the pain-related behaviors but women with high anxiety scores experienced more severe pain before labor analgesia was ad-ministered. This finding adds to previous literature suggesting a direct corre-lation between anxiety sensitivity and maximum pain during labor (24, 25). Although a few women reported very low scores for pain during labor, the clear majority indicated that pain was closer to worst imaginable pain and variability in pain scorings in this sample was limited. In addition, pain scor-ings were collected retrospectively, i.e. within 24 hours of delivery, and re-trospective recall biases may have influenced the pain severity. Based on prior studies (24), it seems that anxiety sensitivity was the best predictor of maximum pain during labor. Anxiety sensitivity in a parturient refers to an-xiety related symptoms due to belief (in this context) that the labor pains will harm her or her fetus. The relationship between anxiety sensitivity and

42
STAI-T has been explored by Curzik and Begic (18) who concluded that there is no reason to expect greater labor pain intensity in women with high levels of trait anxiety whereas it can be expected in women with high anxiety sensitivity. In our study we have not addressed the phenomenon of anxiety sensitivity.
A general concern with studies regarding depression and pregnancy is that the discrimination between psychosocial stress, subclinical depression and true depression is often inconsistent, i.e. women (especially of high socioe-conomic status) tend to report what is expected of them rather than how they feel (172). Thus, underreporting of depressed mood may be expected during pregnancy, why conclusions of labor pain related outcomes and depression may be hard to interpret. The issue of the pregnancy itself influencing the MADRS-S score was taken into consideration (174, 175), but given the rela-tively high socioeconomic status of the study group the two confounders might balance each other.

43
Sammanfattning på svenska
Smärtupplevelsen och användning av smärtstillande behandling under en förlossning varierar mellan olika kvinnor. Det finns en mängd förklaringar till detta; där tidigare förlossningserfarenhet, förlossningens duration, barnets vikt och psykologiska faktorer förefaller vara de mest inflytelserika. Den här avhandlingen har studerat såväl biologiska (effekter av kroppseget morfin (endorfin) och genetiska polymorfier) som psykologiska faktorers (depres-sions- och ångestsymtom) betydelse för smärtrelaterade beteenden under förlossningen. De två genpolymorfier som studerats härrör från specifika förändringar av basparen i OPRM1- respektive GCH1 genen och har tidigare associerats med bättre svar på smärtstillande behandling respektive minskad smärtkänslighet.
Det som kom att bli vår första studie rörde -endorfin (BE) som är ett kroppseget ämne med en morfinliknande effekt vars frisättning påverkas av stress. Vi kunde visa att BE nivåerna var oförändrade under graviditet, men att de efter en sänkning i den andra trimestern ökade under graviditetens senare del. Låga nivåer av BE under graviditeten var dessutom associerat med större behov av smärtlindring under förlossningen.
Kvinnor som var bärare i dubbel uppsättning av den förändrade GCH1 genen kom till förlossningen med mer öppen livmoderhals jämfört med icke-bärare. Vidare efterfrågade de, i motsats till vad vi hade förväntat oss, i hög-re utsträckning minst två sorters smärtlindring. Motsvarande genetiska ana-lys för OPRM1 genen påvisade ingen skillnad mellan bärare och icke-bärare avseende livmoderhalsstatus vid tid för ankomst till förlossningen eller be-hov av smärtlindring. Självrapporterad smärta påverkades inte av bärarskap av någondera av genpolymorfierna. Våra studier bekräftar att förstföderskor och kvinnor med långdragna förlossningar har ett större behov av smärtlind-ring.
Det är känt att orsakerna till behov av smärtlindring och skillnader i smärtupplevelsen under förlossningen är multifaktoriella. För att ta reda på betydelsen av faktorer som nedstämdhet, ångest och kroppens eget morfin (endorfiner) för upplevelse av förlossningssmärta, gjordes fördjupade studier på området. Vår 4:e och sista studie rörde huruvida ångest och nedstämdhet under graviditeten kan ha betydelse för hur tidigt man söker i förlossnings-förloppet och behovet av smärtlindring. Kvinnor med mer uttalade depres-sionssymtom visade sig söka tidigare i förloppet med värkar än motsvarande kvinnor med låg poäng på depressionsskalan MADRS-S. Vidare skattar

44
kvinnor med hög poäng på ångestskalan (STAI-T) sin förlossningssmärta högre innan de får bedövning av barnmorskan än motsvarande kvinnor med låg eller ingen ångest. Vår slutsats blev att kvinnans psykiska hälsa under graviditeten har betydelse för smärtupplevelse men att det inte ensamt kan förklara eller förutse smärtupplevelsen hos enskilda kvinnor. Det behövs dock fortsatta studier inom fältet för att komma närmare en bättre förklar-ingsmodell av födande kvinnors olika behov av smärtlindring.

45
General Conclusions
Levels of BE in plasma remain unchanged between early and late pregnancy except for a nadir in the beginning of the third trimester. Low levels of BE in gestational week 37 is associated with increased need second line labor analgesia. The pain-protective SNP combination of GCH1 may be of importance in homozygous carriers during the initial phase of labor. However these women are more inclined to use second line labor analgesia than corresponding hete-rozygous women and non-carriers. There is no association between the OPRM1 A118G SNP regarding pain-related behavior measured as stage of cervical dilation on arrival to the deli-very unit or use of any type of second line labor analgesia.
Depressed mood during pregnancy is associated with early arrival to the delivery department, whereas antenatal anxiety is associated with increased self-rated pain prior to labor analgesia.

46
Acknowledgements
This thesis was conducted at the Department of Women’s and Children’s Health and the Department of Pharmaceutical Biosciences, Division of Bio-logical Research on Drug Dependence both at Uppsala University, Uppsala, Sweden.
I would like to give my sincere thanks to everyone who supported, as-sisted and encouraged me during this process. I especially wish to express my gratitude to: My main supervisor, Assistant Professor Helena Åkerud, for sharing your knowledge and aptitude as a researcher and always focusing on what was important to get to the next level. I have been lucky to have you as my su-pervisor! My co-supervisor Professor Inger Sundström-Poromaa, for recruiting me to this fantastic project and sharing your tremendous knowledge with us. Thanks for supporting me in times of hardship, which kept me thinking posi-tive at all times. To my second co-supervisor in the Pharmaceutical department, Professor Fred Nyberg, for inspiring meetings and for sharing your great knowledge and large network with us. I would also like to thank the heads of the Department of Women’s and Children’s health Professor Emeritus Ove Axelsson and Professor Jan Gustafsson, and the Head of the Department of Pharmaceutical Biosciences Professor Eva Brittebo. Assistant Professor Elisabeth Darj, Dr Gunilla Hallberg and Dr Bo Sul-tan past and present directors of the Department of Obstetrics and Gynecol-ogy in Uppsala, for your support and generosity. My co-authors Alfhild Grönbladh and Qin Zhou thank you for valuable assistance.

47
To our whole research group but in particular my co-author and fellow PhD student Charlotte Hellgren, thank you for helping me with the recruitment of women to paper IV, interesting scientific discussions and a very good teamwork. Dr Susanne Ledin Eriksson, anesthetist (the County Hospital in Gävle) for valuable input at the mid-term seminar and assistance in co-authoring the chapter on neuraxial anesthesia. Britt-Marie Johansson, technician at BMC and the Uppsala Genome Centre, both in Uppsala, for valuable assistance. All my colleagues, midwifes and co-workers at the Department of Obste-trics and Gynecology in Uppsala, especially Professor Tord Naessén, Peter Lindgren and my roommates Sarah Nordqvist and Katarina Lind-borg Kösenlioglu, thank you for your support and friendly talks. To all midwifes and obstetricians in the labor ward in Karlstad Central Hospital. Professor Matts Olovsson, who invited me to join the research community in our department. The Åkerud family for your generosity thanks to all of you! Thanks to all the participating mothers from Uppsala and Värmland Coun-ty.
Mam Foon (from Addicted to Base), for drawing the beautiful cover of this thesis.
Birgitta Wikmark Carlsson, for our fruitful meetings and helping me real-ize what to do with my proficiencies! To mr. Dudo Touray for help to get into the field of Obstetrics and Gyne-cology, I nïn mbara! Dr Charlotta Sävblom my dear friend and colleague for all your good ad-vice and pep talk when I needed it the most! My in laws Gunnel and Åke Pettersson for supporting me and Kalle in the very tough late stages of this work!

48
My brothers and sisters; Majula Dabo, Aija Dabo, Muhammad L Dabo and Mustafa K Dabo, and my nephews Muhammad and Ahmed-Yusuf Jawara thank you for your love and support!
To my beloved husband Karl Gustav Pettersson, you are also my best friend and my son Jonas Kalil Pettersson, you are what it is all about! My parents; Filijay Tamara Sawo och Lamin S Dabo, thank you for be-lieving in me and always nagging on me to do my homework and never to settle – I think it helped! This project was financed by grants from the Söderström-Königska Foun-dation, the Uppsala-Örebro Regional Research Council, Precision Sys-tem Science (PSS), General Maternity Hospital Foundation and from the Swedish Science Research Council.

49
References
1. Lally JE, Murtagh MJ, Macphail S, Thomson R. More in hope than expectation: a systematic review of women's expectations and experience of pain relief in labour. BMC Med. 2008;6:7.
2. Mason P. Deconstructing endogenous pain modulations. J Neurophysiol. 2005 Sep;94(3):1659-63.
3. Robertson A. The pain of labour. Midwifery Today Childbirth Educ. 1996 Spring(37):19-21, 40-2.
4. Capogna G, Camorcia M, Stirparo S, Valentini G, Garassino A, Farcomeni A. Multidimensional evaluation of pain during early and late labor: a comparison of nulliparous and multiparous women. Int J Obstet Anesth. 2010 Apr;19(2):167-70.
5. Rowlands S, Permezel M. Physiology of pain in labour. Baillieres Clin Obstet Gynaecol. 1998 Sep;12(3):347-62.
6. Ward ME. Acute pain and the obstetric patient: recent developments in analgesia for labor and delivery. Int Anesthesiol Clin. 1997 Spring;35(2):83-103.
7. Bonica JJ, editor. The nature of pain in parturition. New York: Churchill Livingstone; 1996.
8. Bacigalupo G, Riese S, Rosendahl H, Saling E. Quantitative relationships between pain intensities during labor and beta-endorphin and cortisol concentrations in plasma. Decline of the hormone concentrations in the early postpartum period. J Perinat Med. 1990;18(4):289-96.
9. Mahomed K, Gulmezoglu AM, Nikodem VC, Wolman WL, Chalmers BE, Hofmeyr GJ. Labor experience, maternal mood and cortisol and catecholamine levels in low-risk primiparous women. J Psychosom Obstet Gynaecol. 1995 Dec;16(4):181-6.
10. Lederman RP, Lederman E, Work B, Jr., McCann DS. Anxiety and epinephrine in multiparous women in labor: relationship to duration of labor and fetal heart rate pattern. Am J Obstet Gynecol. 1985 Dec 15;153(8):870-7.
11. Lederman RP, Lederman E, Work BA, Jr., McCann DS. The relationship of maternal anxiety, plasma catecholamines, and plasma cortisol to progress in labor. Am J Obstet Gynecol. 1978 Nov 1;132(5):495-500.
12. Neumark J, Hammerle AF, Biegelmayer C. Effects of epidural analgesia on plasma catecholamines and cortisol in parturition. Acta Anaesthesiol Scand. 1985 Aug;29(6):555-9.

50
13. Pearson JF, Davies P. The effect on continuous lumbar epidural analgesia on maternal acid-base balance and arterial lactate concentration during the second stage of labour. J Obstet Gynaecol Br Commonw. 1973 Mar;80(3):225-9.
14. Carr JL, Moffett JA. The impact of social deprivation on chronic back pain outcomes. Chronic Illn. 2005 Jun;1(2):121-9.
15. Nicholson B, Verma S. Comorbidities in chronic neuropathic pain. Pain Med. 2004 Mar;5 Suppl 1:S9-S27.
16. Gureje O. Psychiatric aspects of pain. Curr Opin Psychiatry. 2007 Jan;20(1):42-6.
17. Kroenke K, Krebs EE, Bair MJ. Pharmacotherapy of chronic pain: a synthesis of recommendations from systematic reviews. Gen Hosp Psychiatry. 2009 May-Jun;31(3):206-19.
18. Curzik D, Jokic-Begic N. Anxiety sensitivity and anxiety as correlates of expected, experienced and recalled labor pain. J Psychosom Obstet Gynaecol. 2011 Dec;32(4):198-203.
19. McCrea H, Wright ME, Stringer M. Psychosocial factors influencing personal control in pain relief. Int J Nurs Stud. 2000 Dec;37(6):493-503.
20. Escott D, Slade P, Spiby H. Preparation for pain management during childbirth: the psychological aspects of coping strategy development in antenatal education. Clin Psychol Rev. 2009 Nov;29(7):617-22.
21. Berg M, Terstad A. Swedish women's experiences of doula support during childbirth. Midwifery. 2006 Dec;22(4):330-8.
22. Waldenstrom U, Bergman V, Vasell G. The complexity of labor pain: experiences of 278 women. J Psychosom Obstet Gynaecol. 1996 Dec;17(4):215-28.
23. Hodnett ED. Pain and women's satisfaction with the experience of childbirth: a systematic review. Am J Obstet Gynecol. 2002 May;186(5 Suppl Nature):S160-72.
24. Lang AJ, Sorrell JT, Rodgers CS, Lebeck MM. Anxiety sensitivity as a predictor of labor pain. Eur J Pain. 2006 Apr;10(3):263-70.
25. Reading AE, Cox DN. Psychosocial predictors of labor pain. Pain. 1985 Jul;22(3):309-15.
26. Perkin MR, Bland JM, Peacock JL, Anderson HR. The effect of anxiety and depression during pregnancy on obstetric complications. Br J Obstet Gynaecol. 1993 Jul;100(7):629-34.
27. Smith R, Cubis J, Brinsmead M, Lewin T, Singh B, Owens P, et al. Mood changes, obstetric experience and alterations in plasma cortisol, beta-endorphin and corticotrophin releasing hormone during pregnancy and the puerperium. J Psychosom Res. 1990;34(1):53-69.
28. Andersson L, Sundstrom-Poromaa I, Wulff M, Astrom M, Bixo M. Implications of antenatal depression and anxiety for obstetric outcome. Obstet Gynecol. 2004 Sep;104(3):467-76.

51
29. Kimber L, McNabb M, Mc Court C, Haines A, Brocklehurst P. Massage or music for pain relief in labour: a pilot randomised placebo controlled trial. Eur J Pain. 2008 Nov;12(8):961-9.
30. Ohlsson G, Buchhave P, Leandersson U, Nordstrom L, Rydhstrom H, Sjolin I. Warm tub bathing during labor: maternal and neonatal effects. Acta Obstet Gynecol Scand. 2001 Apr;80(4):311-4.
31. Findley I, Chamberlain G. ABC of labour care. Relief of pain. BMJ. 1999 Apr 3;318(7188):927-30.
32. Melzack R. Prolonged relief of pain by brief, intense transcutaneous somatic stimulation. Pain. 1975 Dec;1(4):357-73.
33. Chia YT, Arulkumaran S, Chua S, Ratnam SS. Effectiveness of transcutaneous electric nerve stimulator for pain relief in labour. Asia Oceania J Obstet Gynaecol. 1990 Jun;16(2):145-51.
34. Kaplan B, Rabinerson D, Lurie S, Bar J, Krieser UR, Neri A. Transcutaneous electrical nerve stimulation (TENS) for adjuvant pain-relief during labor and delivery. Int J Gynaecol Obstet. 1998 Mar;60(3):251-5.
35. van der Ploeg JM, Vervest HA, Liem AL, Schagen van Leeuwen JH. Transcutaneous nerve stimulation (TENS) during the first stage of labour: a randomized clinical trial. Pain. 1996 Nov;68(1):75-8.
36. van der Spank JT, Cambier DC, De Paepe HM, Danneels LA, Witvrouw EE, Beerens L. Pain relief in labour by transcutaneous electrical nerve stimulation (TENS). Arch Gynecol Obstet. 2000 Nov;264(3):131-6.
37. Hutton EK, Kasperink M, Rutten M, Reitsma A, Wainman B. Sterile water injection for labour pain: a systematic review and meta-analysis of randomised controlled trials. BJOG. 2009 Aug;116(9):1158-66.
38. Wang SM, Kain ZN, White P. Acupuncture analgesia: I. The scientific basis. Anesth Analg. 2008 Feb;106(2):602-10.
39. Wang SM, Kain ZN, White PF. Acupuncture analgesia: II. Clinical considerations. Anesth Analg. 2008 Feb;106(2):611-21, table of contents.
40. Tournaire M, Theau-Yonneau A. Complementary and alternative approaches to pain relief during labor. Evid Based Complement Alternat Med. 2007 Dec;4(4):409-17.
41. Smith CA, Collins CT, Crowther CA, Levett KM. Acupuncture or acupressure for pain management in labour. Cochrane Database Syst Rev. 2011(7):CD009232.
42. Ramnero A, Hanson U, Kihlgren M. Acupuncture treatment during labour--a randomised controlled trial. BJOG. 2002 Jun;109(6):637-44.
43. Swedish Official Statistics S. Pregnancies, deliveries and newborn infants. The Swedish Medical Birth Register 1973 - 2008. wwwsocialstyrelsense. 2009.
44. Davis JE. Paracervical block in obstetrics and gynecology. Calif Med. 1966 Dec;105(6):421-3.

52
45. Loubert C, Hinova A, Fernando R. Update on modern neuraxial analgesia in labour: a review of the literature of the last 5 years. Anaesthesia. 2011 Mar;66(3):191-212.
46. Anim-Somuah M, Smyth R, Howell C. Epidural versus non-epidural or no analgesia in labour. Cochrane Database Syst Rev. 2005(4):CD000331.
47. Dickinson JE, Paech MJ, McDonald SJ, Evans SF. Maternal satisfaction with childbirth and intrapartum analgesia in nulliparous labour. Aust N Z J Obstet Gynaecol. 2003 Dec;43(6):463-8.
48. Amer-Wahlin I, Christoffersson M, Dahlgren N, Rydhstroem H. Epidural analgesia with sufentanil during labor and operative delivery. Acta Obstet Gynecol Scand. 2000 Jul;79(7):538-42.
49. Eriksson SL, Olausson PO, Olofsson C. Use of epidural analgesia and its relation to caesarean and instrumental deliveries-a population--based study of 94,217 primiparae. Eur J Obstet Gynecol Reprod Biol. 2006 Sep-Oct;128(1-2):270-5.
50. Lindeberg SN, Thoren T, Hanson U. A high rate of epidural analgesia with bupivacaine-sufentanil is consistent with a low rate of caesarean section and instrumental deliveries. Eur J Obstet Gynecol Reprod Biol. 2001 Oct;98(2):193-8.
51. Schytt E, Waldenstrom U. Epidural analgesia for labor pain: whose choice? Acta Obstet Gynecol Scand. 2010;89(2):238-42.
52. Ekeus C, Hjern A, Hjelmstedt A. The need for epidural analgesia is related to birthweight - a population-based register study. Acta Obstet Gynecol Scand. 2009;88(4):397-401.
53. Katz J, Melzack R. Measurement of pain. Surg Clin North Am. 1999 Apr;79(2):231-52.
54. Williamson A, Hoggart B. Pain: a review of three commonly used pain rating scales. J Clin Nurs. 2005 Aug;14(7):798-804.
55. Aun C, Lam YM, Collett B. Evaluation of the use of visual analogue scale in Chinese patients. Pain. 1986 May;25(2):215-21.
56. Scott J, Huskisson EC. Accuracy of subjective measurements made with or without previous scores: an important source of error in serial measurement of subjective states. Ann Rheum Dis. 1979 Dec;38(6):558-9.
57. Kremer E, Atkinson JH, Ignelzi RJ. Measurement of pain: patient preference does not confound pain measurement. Pain. 1981 Apr;10(2):241-8.
58. Jensen TS. Self-report scales and procedures for assessing pain in adults. Turk DC MR, editor. New York: The Guildford Press; 1992.
59. Melzack R, Taenzer P, Feldman P, Kinch RA. Labour is still painful after prepared childbirth training. Can Med Assoc J. 1981 Aug 15;125(4):357-63.
60. Turk DC, Dworkin RH, Revicki D, Harding G, Burke LB, Cella D, et al. Identifying important outcome domains for chronic pain clinical trials: an IMMPACT survey of people with pain. Pain. 2008 Jul 15;137(2):276-85.
61. van der Putten A, Vlaskamp C. Pain assessment in people with profound intellectual and multiple disabilities; a pilot study into the use of the Pain

53
Behaviour Checklist in everyday practice. Res Dev Disabil. 2011 Sep-Oct;32(5):1677-84.
62. Ersek M, Polissar N, Neradilek MB. Development of a composite pain measure for persons with advanced dementia: exploratory analyses in self-reporting nursing home residents. J Pain Symptom Manage. 2011 Mar;41(3):566-79.
63. Tousignant-Laflamme Y, Bourgault P, Gelinas C, Marchand S. Assessing pain behaviors in healthy subjects using the Critical-Care Pain Observation Tool (CPOT): a pilot study. J Pain. 2010 Oct;11(10):983-7.
64. de Jong A, Baartmans M, Bremer M, van Komen R, Middelkoop E, Tuinebreijer W, et al. Reliability, validity and clinical utility of three types of pain behavioural observation scales for young children with burns aged 0-5 years. Pain. 2010 Sep;150(3):561-7.
65. Bonnel AM BF. Labor pain assessment: validity of a behavioral index. . Pain 1985;22(1):81-90.
66. Hellerud BC, Storm H. Skin conductance and behaviour during sensory stimulation of preterm and term infants. Early Hum Dev. 2002 Dec;70(1-2):35-46.
67. Choo EK, Magruder W, Montgomery CJ, Lim J, Brant R, Ansermino JM. Skin conductance fluctuations correlate poorly with postoperative self-report pain measures in school-aged children. Anesthesiology. 2010 Jul;113(1):175-82.
68. Hullett B, Chambers N, Preuss J, Zamudio I, Lange J, Pascoe E, et al. Monitoring electrical skin conductance: a tool for the assessment of postoperative pain in children? Anesthesiology. 2009 Sep;111(3):513-7.
69. Ledowski T, Ang B, Schmarbeck T, Rhodes J. Monitoring of sympathetic tone to assess postoperative pain: skin conductance vs surgical stress index. Anaesthesia. 2009 Jul;64(7):727-31.
70. Ledowski T, Bromilow J, Wu J, Paech MJ, Storm H, Schug SA. The assessment of postoperative pain by monitoring skin conductance: results of a prospective study. Anaesthesia. 2007 Oct;62(10):989-93.
71. Jonsson M, Hellgren C, Wiberg-Itzel E, Akerud H. Assessment of pain in women randomly allocated to speculum or digital insertion of the Foley catheter for induction of labor. Acta Obstet Gynecol Scand. 2011 Sep;90(9):997-1004.
72. Soderberg K, Sundstrom Poromaa I, Nyberg S, Backstrom T, Nordh E. Psychophysically determined thresholds for thermal perception and pain perception in healthy women across the menstrual cycle. Clin J Pain. 2006 Sep;22(7):610-6.
73. Guindon J, Beaulieu P. The role of the endogenous cannabinoid system in peripheral analgesia. Curr Mol Pharmacol. 2009 Jan;2(1):134-9.
74. Zhou XJ, Yang J, Yan FL, Wang DX, Li XY, Fan XQ, et al. Norepinephrine plays an important role in antinociceptive modulation of hypothalamic paraventricular nucleus in the rat. Int J Neurosci. 2010 Jun;120(6):428-38.

54
75. Kream RM, Kato T, Shimonaka H, Marchand JE, Wurm WH. Substance P markedly potentiates the antinociceptive effects of morphine sulfate administered at the spinal level. Proc Natl Acad Sci U S A. 1993 Apr 15;90(8):3564-8.
76. Li JJ, Zhou X, Yu LC. Involvement of neuropeptide Y and Y1 receptor in antinociception in the arcuate nucleus of hypothalamus, an immunohistochemical and pharmacological study in intact rats and rats with inflammation. Pain. 2005 Nov;118(1-2):232-42.
77. Lopez-Garcia JA. Serotonergic modulation of spinal sensory circuits. Curr Top Med Chem. 2006;6(18):1987-96.
78. Potvin S, Grignon S, Marchand S. Human evidence of a supra-spinal modulating role of dopamine on pain perception. Synapse. 2009 May;63(5):390-402.
79. Bessiere B, Laboureyras E, Chateauraynaud J, Laulin JP, Simonnet G. A single nitrous oxide (N2O) exposure leads to persistent alleviation of neuropathic pain in rats. J Pain. 2010 Jan;11(1):13-23.
80. Basbaum AI, Fields HL. Endogenous pain control systems: brainstem spinal pathways and endorphin circuitry. Annu Rev Neurosci. 1984;7:309-38.
81. Yang J, Liang JY, Li P, Pan YJ, Qiu PY, Zhang J, et al. Oxytocin in the periaqueductal gray participates in pain modulation in the rat by influencing endogenous opiate peptides. Peptides. 2011 Jun;32(6):1255-61.
82. Dalayeun JF, Nores JM, Bergal S. Physiology of beta-endorphins. A close-up view and a review of the literature. Biomed Pharmacother. 1993;47(8):311-20.
83. Kosterlitz HW. The Wellcome Foundation lecture, 1982. Opioid peptides and their receptors. Proc R Soc Lond B Biol Sci. 1985 Jul 22;225(1238):27-40.
84. Bloom F, Battenberg E, Rossier J, Ling N, Leppaluoto J, Vargo TM, et al. Endorphins are located in the intermediate and anterior lobes of the pituitary gland, not in the neurohypophysis. Life Sci. 1977 Jan 1;20(1):43-7.
85. Moon HD, Li CH, Jennings BM. Immunohistochemical and histochemical studies of pituitary beta-lipotrophs. Anat Rec. 1973 Mar;175(3):529-37.
86. Pelletier G, Leclerc R, Labrie F, Cote J, Chretien M, Lis M. Immunohistochemical localization of beta-lipotropic hormone in the pituitary gland. Endocrinology. 1977 Mar;100(3):770-6.
87. Schwartzberg DG, Nakane PK. Ontogenesis of adrenocorticotropin-related peptide determinants in the hypothalamus and pituitary gland of the rat. Endocrinology. 1982 Mar;110(3):855-64.
88. Schwartzberg DG, Nakane PK. ACTH-related peptide containing neurons within the medulla oblongata of the rat. Brain Res. 1983 Oct 16;276(2):351-6.
89. Akil H, Richardson DE, Barchas JD, Li CH. Appearance of beta-endorphin-like immunoreactivity in human ventricular cerebrospinal fluid upon analgesic electrical stimulation. Proc Natl Acad Sci U S A. 1978 Oct;75(10):5170-2.

55
90. Goodman RR, Snyder SH, Kuhar MJ, Young WS, 3rd. Differentiation of delta and mu opiate receptor localizations by light microscopic autoradiography. Proc Natl Acad Sci U S A. 1980 Oct;77(10):6239-43.
91. Gintzler. Endorphin-mediated Increases in pain threshold during pregnancy. Science. 1980 193-5
92. Varrassi G, Bazzano C, Edwards WT. Effects of physical activity on maternal plasma beta-endorphin levels and perception of labor pain. Am J Obstet Gynecol. 1989 Mar;160(3):707-12.
93. Hegadoren KM, O'Donnell T, Lanius R, Coupland NJ, Lacaze-Masmonteil N. The role of beta-endorphin in the pathophysiology of major depression. Neuropeptides. 2009 Oct;43(5):341-53.
94. Vogl SE, Worda C, Egarter C, Bieglmayer C, Szekeres T, Huber J, et al. Mode of delivery is associated with maternal and fetal endocrine stress response. BJOG. 2006 Apr;113(4):441-5.
95. Csontos K, Rust M, Hollt V, Mahr W, Kromer W, Teschemacher HJ. Elevated plasma beta-endorphin levels in pregnant women and their neonates. Life Sci. 1979 Sep 3;25(10):835-44.
96. Genazzani AR, Facchinetti F, Parrini D. beta-lipotrophin and beta-endorphin plasma levels during pregnancy. Clin Endocrinol (Oxf). 1981 Apr;14(4):409-18.
97. Goebelsmann U, Abboud TK, Hoffman DI, Hung TT. Beta-endorphin in pregnancy. Eur J Obstet Gynecol Reprod Biol. 1984 May;17(2-3):77-89.
98. Goland RS, Wardlaw SL, Stark RI, Frantz AG. Human plasma beta-endorphin during pregnancy, labor, and delivery. J clin Endocrinol Metab. 1981 Jan;52(1):74-8.
99. Hoffman DI, Abboud TK, Haase HR, Hung TT, Goebelsmann U. Plasma beta-endorphin concentrations prior to and during pregnancy, in labor, and after delivery. Am J Obstet Gynecol. 1984 Nov 1;150(5 Pt 1):492-6.
100. Browning AJ, Butt WR, Lynch SS, Shakespear RA. Maternal plasma concentrations of beta-lipotrophin, beta-endorphin and gamma-lipotrophin throughout pregnancy. Br J Obstet Gynaecol. 1983 Dec;90(12):1147-51.
101. Sandman CA, Wadhwa PD, Chicz-DeMet A, Porto M, Garite TJ. Third trimester POMC disregulation predicts use of anesthesia at vaginal delivery. Peptides. 1995;16(2):187-90.
102. Glamsta EL, Morkrid L, Lantz I, Nyberg F. Concomitant increase in blood plasma levels of immunoreactive hemorphin-7 and beta-endorphin following long distance running. Regul Pept. 1993 Nov 19;49(1):9-18.
103. McLean M, Thompson D, Zhang HP, Brinsmead M, Smith R. Corticotrophin-releasing hormone and beta-endorphin in labour. Eur J Endocrinol. 1994 Aug;131(2):167-72.
104. Hofmeyr GJ, Gulmezoglu AM, Nikodem VC, Van der Spuy ZM, Hendricks MS. Labor experience and beta-endorphin levels. Int J Gynaecol Obstet. 1995 Sep;50(3):299-300.

56
105. Beaumont A, Hughes J. Biology of opioid peptides. Annu Rev Pharmacol Toxicol. 1979;19:245-67.
106. Humbert J, Pradelles P, Gros C, Dray F. Enkephalin-like products in embryonic chicken retina. Neurosci Lett. 1979 May;12(2-3):259-63.
107. Lundberg JM, Hamberger B, Schultzberg M, Hokfelt T, Granberg PO, Efendic S, et al. Enkephalin- and somatostatin-like immunoreactivities in human adrenal medulla and pheochromocytoma. Proc Natl Acad Sci U S A. 1979 Aug;76(8):4079-83.
108. Tung AS, Yaksh TL. In vivo evidence for multiple opiate receptors mediating analgesia in the rat spinal cord. Brain Res. 1982 Sep 9;247(1):75-83.
109. Beecher HK. The powerful placebo. J Am Med Assoc. 1955 Dec 24;159(17):1602-6.
110. Levine JD, Gordon NC, Fields HL. The mechanism of placebo analgesia. Lancet. 1978 Sep 23;2(8091):654-7.
111. Ossipov MH, Dussor GO, Porreca F. Central modulation of pain. J Clin Invest. 2010 Nov 1;120(11):3779-87.
112. Bingel U, Tracey I. Imaging CNS modulation of pain in humans. Physiology (Bethesda). 2008 Dec;23:371-80.
113. Ossipov MH, Dussor GO, Porreca F. Central modulation of pain. J Clin Invest. Nov 1;120(11):3779-87.
114. Fields HL, Basbaum, A I, Heinricher, MM, editor. Central nervous system mechanisms of pain modulation. 5 ed. Burlington, Massachusetts, USA: Elsevier Health Sciences; 2005.
115. Le Bars D, Dickenson AH, Besson JM. Diffuse noxious inhibitory controls (DNIC). II. Lack of effect on non-convergent neurones, supraspinal involvement and theoretical implications. Pain. 1979 Jun;6(3):305-27.
116. Le Bars D, Dickenson AH, Besson JM. Diffuse noxious inhibitory controls (DNIC). I. Effects on dorsal horn convergent neurones in the rat. Pain. 1979 Jun;6(3):283-304.
117. Villanueva L. Diffuse Noxious Inhibitory Control (DNIC) as a tool for exploring dysfunction of endogenous pain modulatory systems. Pain. 2009 Jun;143(3):161-2.
118. Kim H, Ramsay E, Lee H, Wahl S, Dionne RA. Genome-wide association study of acute post-surgical pain in humans. Pharmacogenomics. 2009 Feb;10(2):171-9.
119. Shi Q, Cleeland CS, Klepstad P, Miaskowski C, Pedersen NL. Biological pathways and genetic variables involved in pain. Qual Life Res. 2010 Dec;19(10):1407-17.
120. Tremblay J, Hamet P. Genetics of pain, opioids, and opioid responsiveness. Metabolism. 2010 Oct;59 Suppl 1:S5-8.
121. Altshuler DM, Gibbs RA, Peltonen L, Dermitzakis E, Schaffner SF, Yu F, et al. Integrating common and rare genetic variation in diverse human populations. Nature. 2010 Sep 2;467(7311):52-8.

57
122. Li WH, Sadler LA. Low nucleotide diversity in man. Genetics. 1991 Oct;129(2):513-23.
123. Nickerson DA, Taylor SL, Weiss KM, Clark AG, Hutchinson RG, Stengard J, et al. DNA sequence diversity in a 9.7-kb region of the human lipoprotein lipase gene. Nat Genet. 1998 Jul;19(3):233-40.
124. Sachidanandam R, Weissman D, Schmidt SC, Kakol JM, Stein LD, Marth G, et al. A map of human genome sequence variation containing 1.42 million single nucleotide polymorphisms. Nature. 2001 Feb 15;409(6822):928-33.
125. Oertel B, Lotsch J. Genetic mutations that prevent pain: implications for future pain medication. Pharmacogenomics. 2008 Feb;9(2):179-94.
126. Fillingim RB, Kaplan L, Staud R, Ness TJ, Glover TL, Campbell CM, et al. The A118G single nucleotide polymorphism of the mu-opioid receptor gene (OPRM1) is associated with pressure pain sensitivity in humans. J Pain. 2005 Mar;6(3):159-67.
127. Huang CJ, Liu HF, Su NY, Hsu YW, Yang CH, Chen CC, et al. Association between human opioid receptor genes polymorphisms and pressure pain sensitivity in females*. Anaesthesia. 2008 Dec;63(12):1288-95.
128. Bond C, LaForge KS, Tian M, Melia D, Zhang S, Borg L, et al. Single-nucleotide polymorphism in the human mu opioid receptor gene alters beta-endorphin binding and activity: possible implications for opiate addiction. Proc Natl Acad Sci U S A. 1998 Aug 4;95(16):9608-13.
129. Oertel BG, Preibisch C, Wallenhorst T, Hummel T, Geisslinger G, Lanfermann H, et al. Differential opioid action on sensory and affective cerebral pain processing. Clin Pharmacol Ther. 2008 Apr;83(4):577-88.
130. Janicki PK, Schuler G, Francis D, Bohr A, Gordin V, Jarzembowski T, et al. A genetic association study of the functional A118G polymorphism of the human mu-opioid receptor gene in patients with acute and chronic pain. Anesth Analg. 2006 Oct;103(4):1011-7.
131. Landau R, Kern C, Columb MO, Smiley RM, Blouin JL. Genetic variability of the mu-opioid receptor influences intrathecal fentanyl analgesia requirements in laboring women. Pain. 2008 Sep 30;139(1):5-14.
132. Wong CA, McCarthy RJ, Blouin J, Landau R. Observational study of the effect of mu-opioid receptor genetic polymorphism on intrathecal opioid labor analgesia and post-cesarean delivery analgesia. Int J Obstet Anesth. 2010 Jul;19(3):246-53.
133. Chou WY, Yang LC, Lu HF, Ko JY, Wang CH, Lin SH, et al. Association of mu-opioid receptor gene polymorphism (A118G) with variations in morphine consumption for analgesia after total knee arthroplasty. Acta Anaesthesiol Scand. 2006 Aug;50(7):787-92.
134. Tegeder I, Costigan M, Griffin RS, Abele A, Belfer I, Schmidt H, et al. GTP cyclohydrolase and tetrahydrobiopterin regulate pain sensitivity and persistence. Nat Med. 2006 Nov;12(11):1269-77.
135. Frank S, Madlener M, Pfeilschifter J, Werner S. Induction of inducible nitric oxide synthase and its corresponding tetrahydrobiopterin-cofactor-

58
synthesizing enzyme GTP-cyclohydrolase I during cutaneous wound repair. J Invest Dermatol. 1998 Dec;111(6):1058-64.
136. Thony B, Auerbach G, Blau N. Tetrahydrobiopterin biosynthesis, regeneration and functions. Biochem J. 2000 Apr 1;347 Pt 1:1-16.
137. Laufs S, Blau N, Thony B. Retrovirus-mediated double transduction of the GTPCH and PTPS genes allows 6-pyruvoyltetrahydropterin synthase-deficient human fibroblasts to synthesize and release tetrahydrobiopterin. J Neurochem. 1998 Jul;71(1):33-40.
138. Maita N, Okada K, Hatakeyama K, Hakoshima T. Crystal structure of the stimulatory complex of GTP cyclohydrolase I and its feedback regulatory protein GFRP. Proc Natl Acad Sci U S A. 2002 Feb 5;99(3):1212-7.
139. Lotsch J, Belfer I, Kirchhof A, Mishra BK, Max MB, Doehring A, et al. Reliable screening for a pain-protective haplotype in the GTP cyclohydrolase 1 gene (GCH1) through the use of 3 or fewer single nucleotide polymorphisms. Clin Chem. 2007 Jun;53(6):1010-5.
140. Tegeder I, Adolph J, Schmidt H, Woolf CJ, Geisslinger G, Lotsch J. Reduced hyperalgesia in homozygous carriers of a GTP cyclohydrolase 1 haplotype. Eur J Pain. 2008 Nov;12(8):1069-77.
141. Campbell CM, Edwards RR, Carmona C, Uhart M, Wand G, Carteret A, et al. Polymorphisms in the GTP cyclohydrolase gene (GCH1) are associated with ratings of capsaicin pain. Pain. 2009 Jan;141(1-2):114-8.
142. Ginya H, Asahina J, Yoshida M, Segawa O, Asano T, Ikeda H, et al. Development of the Handy Bio-Strand and its application to genotyping of OPRM1 (A118G). Anal Biochem. 2007 Aug 1;367(1):79-86.
143. Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry. 1979 1979 Apr;134:382-9.
144. Spielberger CD, Gorsuch RL, R.E. L, Vagg PR, Jacobs GA. Manual for the State-Trait Anxiety Inventory (Form Y1-Y2). Consulting Psychology Press. 1983.
145. Weinstein AM. Visual ERPs evidence for enhanced processing of threatening information in anxious university students. Biol Psychiatry. 1995 Jun 15;37(12):847-58.
146. Nakagawasai O, Tadano T, Tan No K, Niijima F, Sakurada S, Endo Y, et al. Changes in beta-endorphin and stress-induced analgesia in mice after exposure to forced walking stress. Methods Find Exp Clin Pharmacol. 1999 Sep;21(7):471-6.
147. Sandman C A GL, Wadhwa PD, Chicz-DeMet A, Porto M, Garite T. Third Trimester POMC Disregulation Predicts Use of Anesthesia at Vaginal Delivery. Petides 1995;16(2):187-90.
148. Chan EC, Smith R, Lewin T, Brinsmead MW, Zhang HP, Cubis J, et al. Plasma corticotropin-releasing hormone, beta-endorphin and cortisol inter-relationships during human pregnancy. Acta Endocrinol (Copenh). 1993 Apr;128(4):339-44.

59
149. Krieger DT. Placenta as a source of 'brain' and 'pituitary' hormones. Biol Reprod. 1982 Feb;26(1):55-71.
150. Newnham JP, Dennett PM, Ferron SA, Tomlin S, Legg C, Bourne GL, et al. A study of the relationship between circulating beta-endorphin-like immunoreactivity and post partum 'blues'. Clin Endocrinol (Oxf). 1984 Feb;20(2):169-77.
151. Schwarz L, Kindermann W. Changes in beta-endorphin levels in response to aerobic and anaerobic exercise. Sports Med. 1992 Jan;13(1):25-36.
152. Appleyard SM, Hayward M, Young JI, Butler AA, Cone RD, Rubinstein M, et al. A role for the endogenous opioid beta-endorphin in energy homeostasis. Endocrinology. 2003 May;144(5):1753-60.
153. Giugliano D, Paolisso G, Pizza G, Saccomanno F, Torella R. Hormonal and metabolic effects of beta-endorphin in the elderly. Horm Metab Res. 1991 Jul;23(7):351-2.
154. Giugliano D, Lefebvre PJ. A role for beta-endorphin in the pathogenesis of human obesity? Horm Metab Res. 1991 Jun;23(6):251-6.
155. Merenlender-Wagner A, Dikshtein Y, Yadid G. The beta-endorphin role in stress-related psychiatric disorders. Curr Drug Targets. 2009 Nov;10(11):1096-108.
156. Yim IS, Glynn LM, Schetter CD, Hobel CJ, Chicz-Demet A, Sandman CA. Prenatal beta-endorphin as an early predictor of postpartum depressive symptoms in euthymic women. J Affect Disord. 2010 Sep;125(1-3):128-33.
157. Fajardo MC, Florido J, Villaverde C, Oltras CM, Gonzalez-Ramirez AR, Gonzalez-Gomez F. Plasma levels of beta-endorphin and ACTH during labor and immediate puerperium. Eur J Obstet Gynecol Reprod Biol. 1994 Jun 15;55(2):105-8.
158. Halbreich U, Endicott J. Possible involvement of endorphin withdrawal or imbalance in specific premenstrual syndromes and postpartum depression. Med Hypotheses. 1981 Aug;7(8):1045-58.
159. Kim DH, Dai F, Belfer I, Banco RJ, Martha JF, Tighiouart H, et al. Polymorphic variation of the guanosine triphosphate cyclohydrolase 1 gene predicts outcome in patients undergoing surgical treatment for lumbar degenerative disc disease. Spine (Phila Pa 1976). 2010 Oct 1;35(21):1909-14.
160. Kim H, Dionne RA. Lack of influence of GTP cyclohydrolase gene (GCH1) variations on pain sensitivity in humans. Mol Pain. 2007;3:6.
161. Lazarev M, Lamb J, Barmada MM, Dai F, Anderson MA, Max MB, et al. Does the pain-protective GTP cyclohydrolase haplotype significantly alter the pattern or severity of pain in humans with chronic pancreatitis? Mol Pain. 2008;4:58.
162. Lotsch J, Klepstad P, Doehring A, Dale O. A GTP cyclohydrolase 1 genetic variant delays cancer pain. Pain. 2010 Jan;148(1):103-6.

60
163. Oertel BG, Kettner M, Scholich K, Renne C, Roskam B, Geisslinger G, et al. A common human mu-opioid receptor genetic variant diminishes the receptor signaling efficacy in brain regions processing the sensory information of pain. J Biol Chem. 2009 Mar 6;284(10):6530-5.
164. Sia AT, Lim Y, Lim EC, Goh RW, Law HY, Landau R, et al. A118G single nucleotide polymorphism of human mu-opioid receptor gene influences pain perception and patient-controlled intravenous morphine consumption after intrathecal morphine for postcesarean analgesia. Anesthesiology. 2008 Sep;109(3):520-6.
165. Zhang W, Chang YZ, Kan QC, Zhang LR, Lu H, Chu QJ, et al. Association of human mu-opioid receptor gene polymorphism A118G with fentanyl analgesia consumption in Chinese gynaecological patients. Anaesthesia. 2009 Feb;65(2):130-5.
166. Ioannidis JP. Large scale evidence and replication: insights from rheumatology and beyond. Ann Rheum Dis. 2005 Mar;64(3):345-6.
167. Ioannidis JP. Molecular bias. Eur J Epidemiol. 2005;20(9):739-45. 168. Attia J, Ioannidis JP, Thakkinstian A, McEvoy M, Scott RJ, Minelli C, et al.
How to use an article about genetic association: B: Are the results of the study valid? JAMA. 2009 Jan 14;301(2):191-7.
169. Galvan A, Skorpen F, Klepstad P, Knudsen AK, Fladvad T, Falvella FS, et al. Multiple Loci modulate opioid therapy response for cancer pain. Clin Cancer Res. 2011 Jul 1;17(13):4581-7.
170. Klepstad P, Fladvad T, Skorpen F, Bjordal K, Caraceni A, Dale O, et al. Influence from genetic variability on opioid use for cancer pain: a European genetic association study of 2294 cancer pain patients. Pain. 2011 May;152(5):1139-45.
171. Attia J, Ioannidis JP, Thakkinstian A, McEvoy M, Scott RJ, Minelli C, et al. How to use an article about genetic association: C: What are the results and will they help me in caring for my patients? JAMA. 2009 Jan 21;301(3):304-8.
172. Alder J, Fink N, Bitzer J, Hosli I, Holzgreve W. Depression and anxiety during pregnancy: a risk factor for obstetric, fetal and neonatal outcome? A critical review of the literature. J Matern Fetal Neonatal Med. 2007 Mar;20(3):189-209.
173. Grote NK, Bridge JA, Gavin AR, Melville JL, Iyengar S, Katon WJ. A meta-analysis of depression during pregnancy and the risk of preterm birth, low birth weight, and intrauterine growth restriction. Arch Gen Psychiatry. 2010 Oct;67(10):1012-24.
174. Kamysheva E, Skouteris H, Wertheim EH, Paxton SJ, Milgrom J. A prospective investigation of the relationships among sleep quality, physical symptoms, and depressive symptoms during pregnancy. J Affect Disord. 2010 Jun;123(1-3):317-20.
175. Nicholls JA, Grieve DW. Posture, performance and discomfort in pregnancy. Appl Ergon. 1992 Apr;23(2):128-32.