Embed Size (px)
Citation preview

PaediatricsRespiratory system
T. CymesStage 3 student doctorUniversity of Cambridge

Plan
Examination tips differences from adults red flags
Asthma Bronchiolitis Pneumonia Cystic fibrosis
Other diseases

Examination – how to survive
Get to their level! Let young children play with your stethoscope
Great toy! Lets them get used to it
Let parents undress the child only when needed Start with least invasive examination Show on parents, toy etc Auscultate early Save percussion until the end
▪ Start on arm or knee – they get used to it!
Examination – difference from adults
Position Infants – lying on couch Toddler – on parent's lap Pre-school – while at play
Initial impression important ?unwell child
Look for dysmorphic features Percussion can be omitted
Little information in infants

Accessory muscles
Wheeze
Stridor
Grunting
Silent chest
Examination – respiratory distress Tachypnoea / tachycardia
Intercostal recessions
Harrison’s sulcus
Cyanosis
Nasal flaring
Source: BMJSource: Wikipedia Source: englishclass.jp
Source: gponline.com
Source: lumen.luc.eduSource:
quickbase.intuit.com
Asthma
Epidemiology 15% prevalence Associated with atopy
History Wheeze & cough Worse a night Ask about▪ Triggers▪ Frequency▪ Interval symtpoms
Examination out of attack ± wheeze Reduced PEFR
Examination during attack Signs of respiratory distress Hyperexpansion Ascultate Reduced PEFR SpO2

Asthma management
Acute attack – O SHIT! Oxygen Salbutamol Hydrocortisone Ipratropium Theophylline ! – get help!
Monitor SpO2 and PEFR
Chronic management ladderMild • SABA
≥3 week• Inhaled steroids at
conventional dosage
Poor control• LABA• Reasses
No response• Leukotriene antagonists• Theophylline
Poor control •Maximise inhaled steroids•Refer
Poor control •Oral steroids•Immunosuppression / immunomodulation
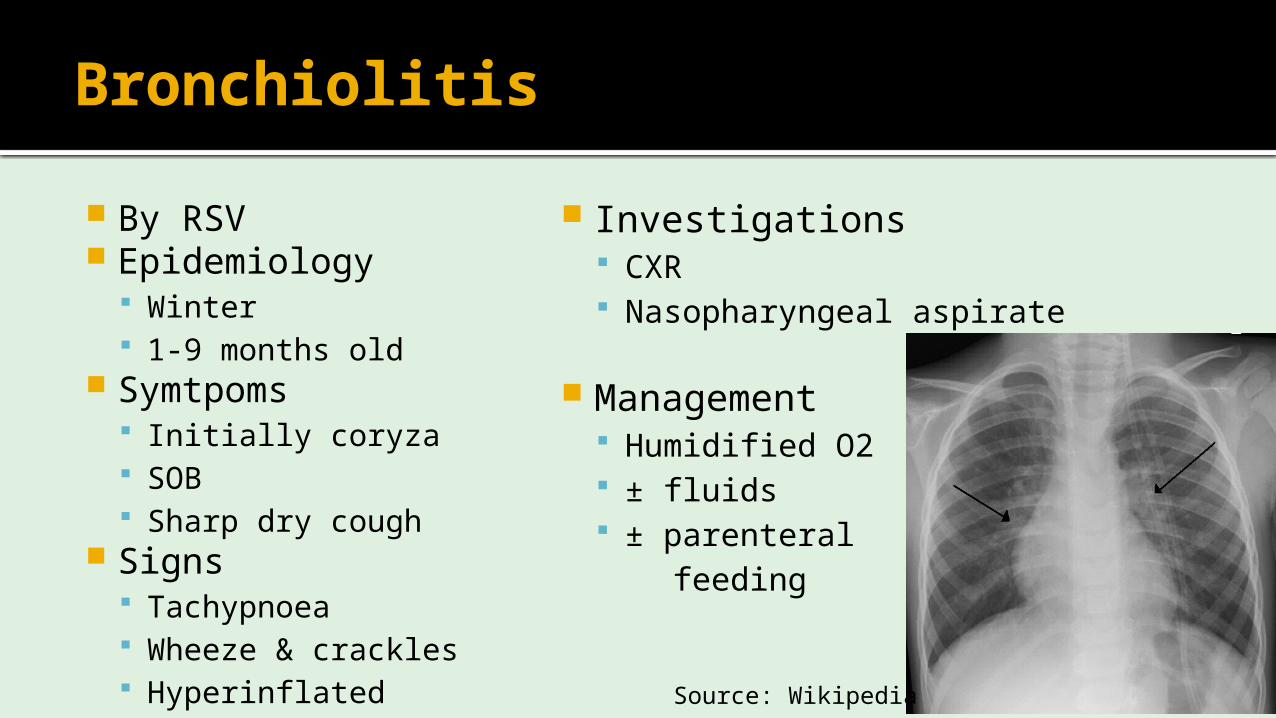
Bronchiolitis
By RSV Epidemiology
Winter 1-9 months old
Symtpoms Initially coryza SOB Sharp dry cough
Signs Tachypnoea Wheeze & crackles Hyperinflated
Investigations CXR Nasopharyngeal aspirate
Management Humidified O2 ± fluids ± parenteral feeding
Source: Wikipedia

Pneumonia
History Often URTI Cough Poor feeding “Unwell child”
Examination Tachypnoea Nasal flare Chest indrawing
Investigations CXR Nasopharyngeal aspirate
Management Usually at home Oxygen & anaelgesia as
neededAge Pathogens Empirical antibiotics
Neonate GBSE. coli
Ampicillin + gentamicin
> 5 years old
ViralStrep. pneumoniaeH. influenzaeB. pertussis
AmpicillinCeftriaxone
> 5 years old
Strep. pneumoniaeH. influenzaeGASMycoplasma
AmoxicillinErythromycin

Cystic fibrosis
Part of Guthrie test
Autosomal recessive 1:2500 live births 1:25 are carriers
History Meconium ileus (10-20%) Persistent cough Recurrent/chronic chest infection Bronciectasis in children Malabsorption failure to thrive Male infertility
Signs Hyperinflated Wheeze Coarse crackles
Management Monitor lung function Prophylactic + rescue antibiotics Physiotherapy Bilateral lung transplant when end-
stage
Nutrtional▪ Pancreatic enzyme supplements▪ 150% healthy calorie intake
Other diseases
Croup Parainfluenza virus URTI barking cough +
stridor Improve over 24h Symptomatic management ?Steroids
Acute epiglottitis H. influenzae type b Very painful throat Sits up with open mouth Drooling DON’T examine throat Intubate, then:▪ Blood culture▪ Cefuroxime IV
Other diseases
Whooping cough B. pertussis Coryza Coughing paroxysms▪ Inspiratory whoop
Erythromycin
Acute otitis media RSV, pneumococci, Hib, GBS Earache in older children Fever Exclude via otoscopy in any
ill oddler Management▪ Symptomatic▪ amoxicillin

Thank you!





![[d], [o] If one doctor doctors another doctor does the doctor who doctors the doctor doctor the doctor the way the doctor he is doctoring doctors? Or](https://img.pdfslide.us/doc/110x75/56649e995503460f94b9c732/d-o-if-one-doctor-doctors-another-doctor-does-the-doctor-who-doctors-the.jpg)