Embed Size (px)
Citation preview

T-cell Receptors and their importance in Organ Transplant and HIV-mediated Cell Death
Alex Guan, Henry Vo, Terence Chi Lok Cheung, Nicholas Loy Son Leslie Dan Faculty of Pharmacy, University of Toronto
1
PHM142 Fall 2014 Instructor: Dr. Jeffrey Henderson

Can be referred as T lymphocytes, part of the adaptive immune system2
From bone marrow -> develop receptors in thymus (gene rearrangement)3
Two main types: Helper T Cells and Cytotoxic T Cells
Cytotoxic T cells kills infected cells via toxins such as perforins and granzymes that cause the infected cell to undergo apoptosis1
Helper T cells secrete cytokines that activate cells involved in immune response such as macrophages (phagocytosis). They are also involved in the antibody production process of B cells1
What are T cells?

Heterodimer embedded in T cells2
Two polypeptide chains: α and β (more common) or γ and δ (less common)2
α polypeptide weighs 40-50kDa, and β weighs 40-45kDa2
Each polypeptide chain has a variable region and constant region (domains)3
Variable regions contain different sequences of amino acids which creates different binding sites for a variety of antigens3
T-cell Receptors

T-cell Receptor Structure

Dendritic cells phagocytize invading pathogens and use protease to break the proteins into peptides (antigens)3
This process is referred to as antigen processing3
peptides combine with MHC (major histocompatibility complex) and migrate to the surface of dendritic cells where they bind to specific T cell receptor3
Antigen-presenting cells3
How are receptors activated?

What Are MHCs?
Major Histocompatibility Complex
Cell surface molecules that bind to peptides from processed antigens4
Can act as antigen presenters to the corresponding T-cell receptors4
Two classes of MHC: 1 and 24

MHC Class 1 bind with intracellular antigenic peptides May signify that something is wrong with the cell itself (i.e.
tumours or bacteria/virally infected cells)4
These are found on all nucleated cells4
MHC Class 2 bind with extracellular-origin antigenic peptides These bind to peptides of pathogens to basically trigger an
immune response from certain immune cells by activating them4
These are found on very specific cells (such as B-cells or macrophages)4
Cytotoxic T cells (CD8+) are specific for MHC-14
Helper T cells (CD4+) are specific for MHC-24
MHC Binding Restriction

CD8 T-cells release cytokines such as IFN-γ and TNF-α to kill the target cell while CD4 T-cells release cytokines for activation4

In order to trigger a response, the MHC-peptide complex must4
Be able to bind perfectly to the TCR4
MHC Binding Restriction

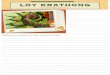
T cells are infected by HIV in a receptor mediated fashion
Gp120 (on HIV) binds to CD4 (on the T cell), inducing a conformational change in gp120 allowing secondary interaction with co-receptor CCXR3 or CCR5.6
Subsequently, gp41 (on HIV) inserts into the plasma membrane of the T cell, undergoing a conformational change, ultimately fusing the HIV and T cell membranes together, allowing the viral contents to be injected into the cell. 6
Background: Receptor mediated entry of HIV into T helper cells
Image taken from http://upload.wikimedia.org/wikipedia/commons/c/c7/HIV_attachment.gif

When infected by HIV, there are two signature events which take place.5 Depletion of CD4 t-cell Inflammatory events
Human Immunodeficiency Virus (HIV)
Image taken http://labs.gladstone.ucsf.edu/greene/sites/default/files/imagecache/os_modal_image_500/greene/files/inflammation_cycle.png
Up until 2009, the mechanism of T cell death and the cause of inflammation was unclear.

Where does the Inflammation come from?
How is that related to cell death? Majority of cells die by a process called pyroptosis, a
Caspase-1 mediated response.5
Releases a large amount of inflammatory cytokines.5
Attraction of other T-cells “Vicious Cycle”
New drugs: Caspase-1 inhibitors
Mechanism of CD4 T-helper cell death by HIV-1 virus and possible new treatments

Organ Transplants: Allogeneic Grafting
In 2013, more than 4,500 Canadians needed an organ transplant7
Isogeneic Grafting Considerations ABO blood type compatibility8
TCR-MHC compatibility9
Low chances of compatibility, and high rates of rejection9
Hyperacute Rejection Acute Rejection Chronic Rejection
13Image taken from reference 10

Organ Transplants: Rejection Mechanism
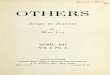
T-Cell-mediated response to MHC 1 CD8+ cell TCRs recognize the foreign MHC 1on donor
cells9
CD8+ cells induce cytotoxic effects causing donor cells to undergo apoptosis
T-Cell-mediated response to MHC 2 CD4+ cell TCRs recognize foreign MHC 2 on donor cells9
CD4+ cells proliferate and secrete cytokines that activate macrophages
Antibody-mediated response to MHC 2 CD4+ cells communicate with B lymphocytes, which
create antibodies against MHC 2 and associated antigens9
14

R. CD8+
CD8
TCR
15
R. CD8+
CD8
TCRDonor APC
MHC 1
MH
C 2
T-Cell-mediated response to MHC 1

16
R. CD4
+
CD4
TCRDonor APCMHC 1
MH
C 2
Antibody and T-Cell-mediated response to MHC 2
Proliferation
R. CD4
+
CD4
TCR
R. CD4
+
CD4
TCR
Cytokine Production
IFN-γ
Activated Macrophages
B Lymphocytes
Humoral ImmuneResponse

17Image taken from reference 9

Summary T-cells are part of the adaptive immune system, The cells are produced in bone marrow and develop receptors in the thymus.
There exists helper T cells and cytotoxic T cells
The receptor is a heterodimer with two polypeptide chains, usually α and β although γ and δ exists as well The variable region provides different binding sites for the receptor to bind to different antigens
Dendritic cells break down pathogen to create antigens that bind to MHC in a process called antigen processing The MHC bound peptide is called antigen presenting cell and it then binds to T cell receptor MHCs are membrane molecules that act to bind antigen peptides in order to present them to T-cells for a variety of functions
2 classes: MHC-1/2; MHC-1 can be found on all cells, MHC-2 only on some CD8 binds to MHC-1, releases cytokines and triggers cell death CD4 binds to MHC-2, releases cytokines that trigger responses in a variety of different immune cells
In order for a T-cell to bind, the MHC and antigen peptide must be specific Even if one of the two doesn’t correspond, there will be no reaction
HIV depletes T-helper Cell (CD4+) populations and creates inflammation events HIV enters the cell in a receptor mediated fashion, using gp120 and gp41 glycoproteins to bind and insert viral contents,
respectively. CD4+ Cell death via pyproptosis releases pro-inflammatory cytokines, attracting other T cells which become infected,
propagating the infection as well as chronic inflammation. New drug prospect: Caspase-1 inhibitors.
It is important to consider both ABO blood type and MHC compatibility when discussing organ transplants. Incompatibility leads to either Hyperacute (preformed antibodies, within minutes), acute (days-months), or chronic rejection
(months-years). Rejection Mechanisms: T-Cell-mediated (CD8) response to MHC 1,T- Cell-mediated (CD4) response to MHC 2, and Antibody-
mediated response to MHC 2 + associated antigen Immunosuppression drugs + steroids can be used to treat rejection, however none target T-cell receptors

1. Kimball, J.W. (2011, April 5). Cytotoxic T Lymphocytes. Retrieved from http://users.rcn.com/jkimball.ma.ultranet/BiologyPages/C/CTL.html
2. Owen, J.A., Punt J., Stranford S.A. (2013). Kuby Immunology. New York, NY: W.H. Freeman and Company.
3. Parham, P. (2009). The immune system. New York, NY: Garland Science, Taylor & Francis Group, LLC.
4. Murphy, K., Travers, P., Walport, M., & Janeway, C. (2012). Janeway's Immunobiology (8th ed.). New York: Garland Science.
5. Doitsh, G., Galloway, N. L., Geng, X., Yang, Z., Monroe, K. M., Zepeda, O., ... & Greene, W. C. (2014). Cell death by pyroptosis drives CD4 T-cell depletion in HIV-1 infection. Nature, 505(7484), 509-514.
6. Ray, N., & Doms, R. W. (2006). HIV-1 coreceptors and their inhibitors. In Chemokines and Viral Infection (pp. 97-120). Springer Berlin Heidelberg.
7. Government of Canada. (2013, December 13). Organ & tissue donation. Retrieved from http://www.healthycanadians.gc.ca/diseases-conditions-maladies-affections/donation-contribution-eng.ph
8. West, L. J., Karamlou, T., Dipchand, A. I., Pollock-Barziv, S. M., Coles, J. G., & McCrindle, B. W. (2006). Impact on outcomes after listing and transplantation, of a strategy to accept ABO blood group-incompatible donor hearts for neonates and infants. The Journal of Thoracic and Cardiovascular Surgery, 131(2), 455–461
9. Kumar, V., Abbas, A., Mitchell, R., & Fausto, N. (2007) Robbins Basic Pathology (8th ed.). Philadelphia: Elsevier - Health Sciences Division.
10. Welsh, R. M., & Selin, L. K. (2002). No one is naive: the significance of heterologous T-cell immunity. Nature Reviews Immunology 2(6), 417-426.
References