Embed Size (px)
Citation preview

Systolic Phases of the Cardiac Cyclein Children
BY DAvm GOLDE, M.D., AND LuIs BURSTIN, M.D.
SUMMARYThe duration of the systolic phases of the cardiac cycle in 390 normal children
was determined from high-speed simultaneous recordings of the electrocardiogram,phonocardiogram, apexcardiogram, and carotid pulse. Data were obtained on chil-dren 1 mo to 13 years of age and analyzed to define the independent effects ofaging and heart rate on the systolic intervals. Electromechanical systole (Q-II) wasfound to prolong with increasing age in children with the same heart rate. Pre-ejec-tion period was also prolonged in older children and occupied an increased percentageof total systole. The interval from onset of contraction to first sound varied inverselywith heart rate and was independent of age. Electromechanical delay and isometriccontraction time were directly related to age and independent of rate. Ejection timevaried directly with age and inversely with heart rate but occupied a smaller per-
centage of systole in older children. Alterations in systolic phase duration occurringwith maturation reflect the normal functional adaptation of the developing heart.Measurement of these phases can provide useful information relative to cardiac func-tion in children.
Additional Indexing Words:Polycardiography Systolic time intervals Ejection timeIsometric contraction time Pre-ejection periodElectromechanical delay
NONINVASIVE technics have becomeincreasingly important in the study of
cardiovascular disease. With these methodsprecise hemodynamic data may be obtainedwithout risk or discomfort to the patient, andstudies can be repeated frequently and undervarious test conditions. Simultaneous externalpolycardiography is an atraumatic technic thatpermits the measurement of the various
From the Department of Medicine, University ofCalifornia School of Medicine, San Francisco,California, and the Department of Physiopathology,University of Costa Rica School of Medicine, SanJose, Costa Rica.
Presented in part at the 18th Annual ScientificSession, American College of Cardiology, March 1,1969.Address for reprints: David Golde, M.D., Depart-
ment of Medicine, University of Califomia Hospitals,San Francisco Medical Center, San Francisco,California 94122.
Received May 4, 1970; revision accepted forpublication August 25, 1970.
Circulation, Volume XLII, December 1970
PhonocardogramApexcardiogram
phases of cardiac systole. The duration ofthese phases correlates well with the patho-physiology in many abnormal cardiac states,and measurement of the phases can provideuseful clinical information relative to cardiacfunction.
Considerable data have been accumulatedon the normal temporal correlations of thephases of systole in adults.' Specific alterationsin systolic phase duration have been shown tooccur with congestive heart failure,2 thyroiddisease,3 digitalis therapy,4 and hypercal-cemia,5 as well as with various congenital" andvalvular defects.7 Data on the normal tem-poral relationships of the systolic phases inchildren are sparse, however, and age-raterelationships remain ill defined.-10 It isdifficult in children to separate the effects ofage and heart rate on the systolic intervalsbecause of the normal inverse relationshipbetween these variables. Cardiovascular mat-uration presumably involves a series of
1029
by guest on April 27, 2018
http://circ.ahajournals.org/D
ownloaded from

GOLDE, BURSTIN
adaptive processes which are reflected by age-dependent alterations in systolic phase dura-tion.The purpose of the present study was to
determine the independent effects of agingand heart rate on the systolic phases inchildren and to delineate the pattern of phasealteration occurring with normal cardiovascu-lar maturation.
MethodsThree hundred and ninety children (202 male
and 188 female) were studied. The subjectsranged in age from I mo to 13 years and were ingood health and free of heart disease. Each childwas normal on cardiovascular examination whichincluded blood pressure determination (in chil-dren over 2 years), auscultation of the heart andlungs, and a standard 12-lead electrocardiogram.Studies were conducted in the morning with thechildren recumbent and in the postabsorptivestate. Only cooperative subjects were included,and no sedation was used.
Simultaneous recordings were taken of theelectrocardiogram (lead II), phonocardiogram,apexcardiogram, and carotid pulse. Tracings were
c--
:: lox
@
:E iS ::::E :E
;::
.:G e|of F F
_ W
|_ |
E5P K:
:::
:E;
:::::::::::: :E
::i:::: i:::D;
:::
::
i:
Z
1s,i: 5
8'# E:x fflg tK
:; i;
i:
v_,-,_. .>
::: :E:>
/
...heOtrkcontraction
recorded on a Siemens Cardirex-6 direct-writingapparatus (linear frequency response 0.07 to 500Hz, 30% amplitude reduction at 650 Hz) utilizingthe Maass-Weber filter system. Boucke-Brechttype transducers were used for the carotid pulsepickup and apexcardiogram. The phonocardio-gram was recorded with an electromagneticmicrophone placed over the left ventricle at alocation giving the clearest reception of the firstand second heart sounds. All wave forns weredisplayed oscillographically, and recordings weretaken at paper speeds of 200 mm/ sec whenoptimal reception was achieved. The phases weremeasured by hand (with the aid of magnifica-tion) in five consecutive cycles at end expiration,and the average was recorded. Only tracings withclear wave forms and inflection points wereutilized. Though the usual limit of readingaccuracy for these types of recordings was takenas 5 msec,2 smaller units were interpolated inestimating phases of extremely short duration.
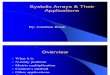
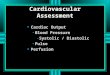
Six phases of cardiac systole were studied (fig.1) . Total electromechanical systole (hereafterreferred to as systole) was taken to comprise theQ-second sound interval (Q-II). The Q-first soundperiod (Q-I) was separated into two phases,electromechanical delay (EMD) and the intervalfrom the onset of contraction to the first sound
::I
N.-FdAs dekzy
Crtdpulse
Ape
Figure 1
Simultaneous recording of the electrocardiogram,cardiogram demonstrating method of calculatingmm/sec; time intervals, 5 msec).
phonocardiogram, carotid pulse, and apex-systolic phase duration (paper speed, 200
Circulation, Volume XLlI, Decembef 1970
1030
f
*-*--Eiection- ll.l.
by guest on April 27, 2018
http://circ.ahajournals.org/D
ownloaded from

CARDIAC CYCLE IN CHILDREN
Table 1Mean Values for Phase Duration in Five Age Groups (30 Children in Each)
HeartSex Yr/mo rate Q-II PEP Q-I EMD C-I ICT ET SQ
F 1/7 120 0.220 0.034 0.021 0.002 0.018 0.014 0.186 5.48M 1/6 119 0.220 0.034 0.021 0.002 0.018 0.014 0.186 5.43F 5/3 106 0.256 0.048 0.031 0.006 0.026 0.018 0.207 4.21M 5/6 104 0.257 0.050 0.031 0.006 0.026 0.018 0.207 4.15F 6/8 105 0.265 0.056 0.036 0.011 0.025 0.020 0.209 3.70M 6/7 90 0.294 0.063 0.043 0.014 0.029 0.021 0.232 3.71F 8/7 94 0.321 0.(060 0.035 0.012 0.023 0.025 0.260 4.30M 8/6 92 0.320 0.061 0.037 0.014 0.023 0.024 0.260 4.28F 13/8 84 0.367 0.093 0.060 0.029 0.031 0.033 0.274 2.97M 13/6 87 0.357 0.089 0.057 0.028 0.029 0.032 0.268 3.01
Abbreviations: Yr/mo = mean age in years and months; heart rate = beats/min; Q-II =
electromechanical systole; PEP = pre-ejection period; Q-I = transformation time; EMD =electromechanical delay; C-I = onset of contraction to 1st sound; ICT = isometric contraction;ET = ejection time; SQ = systolic quotient.
(C-I).1 EMD was measured from the Q wave ofthe electrocardiogram (lead II) to the onset ofthe systolic wave of the apexcardiogram (Cpoint). Q-I was read directly from the Q wave ofthe ECG to the first high frequency vibrations ofthe first heart sound, and C-I was calculated bysubtracting EMD from Q-I. Isometric contractiontime (ICT) was determined by measuring theinterval from the first heart sound to the onset ofthe upstroke of the carotid pulse wave andcorrecting for pulse transmission delay." Pulsedelay time was taken as the interval between thesecond heart sound and the trough of the carotidincisura. The pre-ejection phase (PEP) was
calculated by summing Q-I and ICT. Ejectiontime (ET) was measured from the onset of thecarotid upstroke to the trough of the incisura.12The systolic quotient (SQ) was calculated as theratio of ET and PEP. The data were stored on
magnetic tape and analyzed with the aid of an
IBM 360-50 computer. Preliminary plots were
made directly from taped data using the Cal-Comp apparatus.* Standard computer programswere used for regression analysis and tests ofstatistical significance. To determine possible sex
differences in systolic phase duration, t-tests were
performed on the entire population, on datacomparing children of various ages with the same
heart rate, and on children of the same age withvarious heart rates.
ResultsThe mean values obtained for the phases of
systole in five age groups are presented in
table 1. All phases of systole were found toprolong with increasing age, and the heartrate was progressively slower in older chil-dren. Linear regression equations relatingphase duration to age and heart rate are givenin table 2. F values for all equations weresignificant at P < 0.001. No significant differ-ences (P <0.05) were found between malesand females in the complete population forthe phases studied. In the group of 6 yearolds, however, systole (Q-II), PEP, and ETwere significantly shorter in girls (table 1).This was accounted for by the higher meanheart rate in girls in that age group ( 105 vs.90). In comparing boys and girls of similar
Table 2Regression Equations for Calculating SystolicPhase Duration* Based on Data from 390 Children1 Month to 13 Years of Age
Equation r SE
Systole (Q-II) = 0.65 M - 1.66 R + 402 0.97 14PEP = 0.30 M - 0.32 R + 65 0.94 6ET = 0.35 M- 1.35 R + 337 0.94 13EMD = 0.21 M-5.6 0.90 4C-I = 47-0.23 R 0.77 5Q-I = 0.18 M-0.31 R + 53 0.91 5ICT = 0.12 M + 11 0.89 3SQ = 5.47 - 0.015 M 0.78
*Interval in milliseconds.Abbreviations: M = age in months; R = rate in
beats per minute; r = correlation coefficient; SE =standard error.
*CaifoniaComputer Products, Inc., Anaheim,California.Circulation, Volume XLII, December 1970
1031
by guest on April 27, 2018
http://circ.ahajournals.org/D
ownloaded from

GOLDE, BURSTIN
heart rates, no differences were present forany of the phases.
Systole
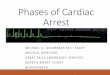
A direct and linear relationship was foundto exist between the duration of systole (Q-II)and age for all of the children studied (fig. 2).Though a linear regression equation withacceptable fit may be written for this relation-ship, age and rate effects cannot be separatedfrom these data. When systole is plottedagainst heart rate for 13-year-old children (fig.3), the expected inverse relationship is seen.To determine possible independent effects ofage, duration of systole was compared for allchildren in the study (48) who coincidentlyhad a heart rate of 100 + 2.5 beats/min.Systole was found to prolong with increasingage apart from any rate considerations (fig.
410
380 _
350
,320
-290...'* .,
o 260 _- ,, a -;
>230 _
200 -
170
2 3 4 5 6 7 8 9 10 12 13 14AGE: (years)
Figure 2
Duration of systole (Q-II) vs. age for entire population(390 children).
lCHILDREN THIRTEEN YEARS OLD4IO0
390
@ 370E
-j 350
0
>- 330
310
iI
I
. I
I
II70 75 80 85 90 95 100 105 1o
RAT E (per min)
Figure 3
Duration of systole (Q-II) vs. heart rate for 13-year-oldchildren.
330K
310H_jn
E 290
270(n
cn
00
0 -o
0*.
0.
* * *@
250K
230
II I22 4 6 8 10 12
AGE (yeor) RATE a 100
Figure 4
14
Duration of systole (Q-II) vs. age for all children inthe study with a heart rate of 100 ± 2.5 beats/min.
4). The regression equation for calculatingtotal systole, therefore, contains two vanrablesand reflects the independent relationship ofsystole to age. This type of analysis wasapplied to all of the phases studied.
Electromechanical DelayEMD was found to prolong with increasing
age (fig. -5) but was relatively independentof heart rate (fig. 6). The regression equationfor EMD contains only one variable. When thephases are expressed as a percentage of totalsystole (table 3), EMD is seen to occupy anincreasing percentage of total systole in older
Table 3Mean Duration of Systolic Phases for Each AgeGroup Expressed as a Percentage of Systole (Q-II)
Age (yr) EMD C-I Q-I ICT PEP ET
<1 8.8 6.9 15.8 84.21 0.8 8.2 9.0 6.5 15.6 84.42 0.8 8.7 9.5 6.5 15.9 84.13 0.9 9.6 10.6 6.6 16.8 83.24 2.1 9.8 11.9 6.8 18.7 81.35 2.3 9.9 12.3 7.0 19.3 80.76 4.4 9.6 14.0 7.3 21.3 78.77 4.6 8.5 13.2 7.6 20.7 79.38 4.1 7.2 11.3 7.6 19.1 80.99 5.2 7.8 12.9 7.6 20.5 79.510 5.1 7.8 12.9 7.5 20.4 79.711 7.7 7.0 14.5 7.4 21.9 78.112 8.5 7.5 15.9 8.5 24.4 75.713 7.8 8.4 16.2 9.0 25.1 75.9
Abbreviations: Same as in table 1.
Circulation, Volume XUL, December 1970
1032
350 r
* 0
.
by guest on April 27, 2018
http://circ.ahajournals.org/D
ownloaded from

CARDIAC CYCLE IN CHILDREN
S-J
E
-j
Uz
I
ULU
0Iru
-iLU
* e
2 4 6 8 10 12 14AGE ( year) RATE - 100
Figure 5Electromechanical delay vs. age for children with aheart rate of 100 ± 2.5 beats/min.
is dependent on both age and heart ratealterations and was found to prolong withboth increasing age and decreasing rate. Thecomposition of the Q-I period also changedmarkedly with aging. In children 1 to 3 yearsold the Q-I interval largely reflected theduration of C-I, whereas in 13 year olds EMDaccounted for approximately half of Q-I.
Isometric Contraction Time
ICT was found to prolong with increasingage and was independent of heart rate withinthe range studied. The duration of isometriccontraction increased approximately two anda half times between the ages of 1 and 13years and occupied a slightly increasedpercentage of systole in older children.
CHILDREN EIGHT YEARS OLD
4- 25
< 20
z
I 10
5
hJ
i70 75 80 85 90 95 100 105 10 115
HEART RATE (per min)
Figure 6Electromechanical delay vs. heart rate for 8-year-oldchildren.
children. EMD was not measurable in chil-dren under 1 year with our technics and is lessthan 5 msec through the first 4 years of life.Approximately a sixfold increase in EMD isnoted between 4 and 13 years.
Contraction to First Sound (C-I)The C-I period was found to prolong with
decreasing heart rate but was largely inde-pendent of age. Rate-dependent alterations inthe C-I period roughly approximated those ofsystole; C-I, therefore, occupied a relativelyconstant percentage of systole in all agegroups (table 3).
Q-I IntervalThe Q-I interval (transformation time)
comprises both the EMD and C-I periods. It
Circulation, Volume XLII, December 1970
Pre-ejection PeriodPEP comprises the Q-I and ICT phases and
therefore relates twice to age and once to rate.PEP was prolonged in older children due to adirect relationship with age and indirectrelationship with rate. PEP occupied a pro-gressively greater percentage of systole withmaturation.
Ejection TimeET was found to relate independently to
age and heart rate. Though ET prolongedwith increasing age, it occupied a progressive-ly smaller percentage of total systole (table3).
Systolic QuotientThe systolic quotient was inversely related
to age and relatively independent of rate (fig.7). The quotient reflects the relative durationof PEP and ET and decreases with aging.
DiscussionThe duration of the various systolic phases
in children differs markedly from thoseobserved in adults.-10 Though some of thesedifferences may be explained by the morerapid heart rates of childhood, age per se is animportant determinant of phase duration. Thisis illustrated (table 4) by comparing valuesfor systolic phase duration in adults (based ondata from 121 normal males studied byWeissler and associates2) with values derived
1033
*e
00 0 0
00 0
0 0a 0
*0
..
0
0
by guest on April 27, 2018
http://circ.ahajournals.org/D
ownloaded from

1034
CHILDREN NINE YEARS OLD
K
* 0
0
.
jF
3.0
75 80 85 90 95 100 105 110 115
RATE (per min)
Figure 7
Systolic quotient vs. heart rate for 9-year-old children.
GOLDE, BURSTIN
Rate Age % Systole
Systole tElectromechanical
Delay - t 1C-1 -_Isometric
Contraction - tEjection time i t ISystolic Quotient - I
Figure 8Relationship of systolic phase duration, age, andheart rate; absolutely and as a percentage of systole.f = Direct relationship; 4 = inverse relaionship.
in this study for 3-year-old children, bothassuming a heart rate of 100 beats/min. Inorder to define the relative contribution ofage and heart rate to systolic phase duration,a large sample was studied permitting a com-parison of children of different ages withsimilar heart rates and children with varyingheart rates within a single age group. Usingthis type of analysis, a consistent pattern ofphase alteration was observed with matura-tion. The precise maturation factors responsi-ble for these alterations were not identified,though it seems likely that heart size, bloodpressure, and blood volume, are importantin this regard. Theoretically, some of the ob-served changes in phase duration could relateto extracardiac factors such as thoracic de-velopment. Autonomic activity must also beconsidered a significant factor.'3 Figure 8summarizes the relationships among the
Table 4Comparison of Systolic Phase Duration in Adultsand 3-Year-Old Children Based on a Heart Rateof 100 Beats/Min: Adult Values Calculated fromthe Regression Data of Weissler and Associates2
Adults Children (3 yr old)msec % of systole msee % of systole
Cycle 600 600Diastole 264 341Systole (Q-II) 336 259PEP 91 27 44 17ET 243 72 215 83Q-I 50 15 28 11ICT 38 11 16 6
Abbreviations: Same as in table 1.
duration of the systolic phases and age andrate.
Systole (Q-II) was found to relate inverselyto heart rate and indirectly to age. For a givenrate, systole was prolonged in older childrenand diastole was abbreviated. Diastole, there-fore, occupied a smaller percentage of thecardiac cycle, though in absolute terms itsduration increased in older children becauseof a slower heart rate. Interestingly, aprolongation of systole has been reported tooccur in old age.14 In our study, theprolongation of systole with age was largelydue to a long PEP, and ET, though alsolengthened, occupied a progressively smallerpercentage of systole in older children. Thelong systole found in old age was thought tobe due primarily to an increase in PEP.14 Arecent study,'5 however, has shown that ETalso is prolonged in old age independently ofchanges in heart rate and blood pressure. Theobserved alterations in systole, PEP, and EToccurring with maturation in children are,
therefore, qualitatively similar to those seen inold age.The duration of PEP has been taken as an
index of myocardial contractility and iscorrelated with ejection fraction,16 17 leftventricular end-diastolic pressure,18 cardiacoutput, and stroke volume.19' 20 Weissler hasshown that congestive heart failure in adultsresults in a prolongation of PEP and an
abbreviated ET.2 Digitalis will reverse theseeffects and cause a shortening of total systole.4The changes in PEP and ET which occur with
Circxation, Volxme XLI, December 1970
5.0
z 4.5
0na 4.0
u)o 3.5
0t 0
00
a0
by guest on April 27, 2018
http://circ.ahajournals.org/D
ownloaded from

CARDIAC CYCLE IN CHILDREN
aging in children could reflect alterations inmyocardial contractility or primarily relate tochanges in preload and afterload consequentto increased ventricular volume and highermean aortic pressures. The relative duration ofET and PEP is reflected by the SQ which islargely independent of rate and decreaseswith aging in childhood.9 In adults thequotient is constant over a wide age and raterange and is reported to be decreased inpatients with congestive failure2 and coronaryartery disease.21No significant sex differences in phase
duration were found in our study, though bothsystole (Q-II) and ET have been found to belonger in adult females than in males.2 Thissex differential may only become apparentafter puberty. Galstian9 reported ET to beshorter and the heart rates more rapid in girls7 to 15 years old. The decreased ET seems tobe a rate phenomenon, as no significantdifferences were found in our study for theentire population or when children withsimilar heart rates were compared. In the onlyage group in which a sex differential existed(6 year olds) there was also a marked differ-ence in heart rate between boys and girls.The shortened PEP found in young children
was due largely to decreased duration ofEMD and ICT. These two phases wereindependent of heart rate and directly relatedto age. ICT has been reported to beindependent of rate in both adults22 andchildren.4 EMD represents the time intervalbetween excitation and the onset of precordialmovement as measured from the Q wave ofthe electrocardiogram (lead II) to the onsetof the systolic wave of the apexcardiogramand is less than 5 msec in children under 4years. EMD prolongs with aging in childrenbut is relatively constant in adults, with 38msec frequently taken as a mean value.23Since EMD and ICT do not alter with ratechanges, they occupy an increased percentageof systole at more rapid heart rates. Thesephases would appear to be theoretically rate-limiting; however, our study includes onlyphysiologic rate changes and different phaserelationships may be operative with markedCirculation, Volume XLII, December 1970
bradycardia or tachycardia. Willems andKesteloot,24 for example, found ET to relatelinearly to heart rate, but exponential orpolynomial relationships existed in paroxysmalatrial tachycardia or with complete A-Vblock.The C-I interval was not related to age and
varied inversely with heart rate. This periodparalleled rate changes both absolutely and asa percentage of systole. Some of the difficultyin utilizing the Q-I interval clinically mayrelate to the disparity in the physiologiccorrelations of its component phases, EMDand C-I. For example, C-I has been found tobe a good index of the severity of mitralstenosis, whereas Q-I is poorly correlated.7The measurement of the systolic phases in
children by external graphic recordings can bepotentially useful in the diagnosis and quanti-tation of congenital defects, assessment ofmyocardial function, and screening for pediat-ric heart disease. Clinical application, how-ever, is predicated on an understanding of thenormal phase relationships in childhood.External recordings lend themselves to com-puter applications in which wave forms can bedigitized and phase duration calculateddirectly.25 Such a system could provideinstantaneous data on phase alterations andwould eliminate the subjective errors inherentin determining phase duration by handreading.The changes in systolic phase duration
occurring with maturation presumably repre-sent the normal functional adaptation of thedeveloping heart. This is manifested by anorderly redistribution of systolic intervalsresulting in a characteristic phase structure foreach age group and heart rate. Further studyof the precise maturation factors responsiblefor these changes is necessary. Measurement ofthe systolic phases in various childhood diseasestates can provide valuable information rela-tive to the effect of these diseases on cardiacfunction.
AcknowledgmentThe authors wish to express their appreciation to
Dr. Carlos Brenes Pereira for assistance with theclinical studies and Mr. George Shakargi for statisticalconsultation.
1035"
by guest on April 27, 2018
http://circ.ahajournals.org/D
ownloaded from

GOLDE, BURSTIN
References1. FiSHLuEDER BL: Las fases del ciclo cardiaco. Su
estudio grafico y su valor clinico. PrincipiaCardiologica 6: 123, 1959
2. WEissLER AM, HAmuS WS, Scuo.NFED CD:Systolic time intervals in heart failure in man.Circulation 37: 149, 1968
3. AIDI , LEON DF, DEGROOT WJ, ET AL: Effectof the thyroid state on myocardial contractilityand ventricular ejection rate in man. Circula-tion 23: 229, 1968
4. WmSSLsR AM, KAMEN AR, BORNSTEiN RS, ETAL: The effect of Deslanoside on the durationof the phases of ventricular systole in man.Amer J Cardiol 15: 153, 1965
5. SHINER P, HAPRms W, WEISSLER A: Effects ofacute changes in serum calcium levels onsystolic time intervals. Amer J Cardiol 24: 42,1969
6. BURSTIN L: Estimacion cuantitativa del cortocir-cuito sanguineo arteriovenoso en la communi-cacion interauricular por registros graficosexternos. Arch Inst Cardiol Mex 25: 479, 1965
7. ORESHKOV V: Q-I or C-I interval in the diagnosisof mitral stenosis. Brit Heart J 29: 778, 1967
8. HARRIS L, WEISSLER AM, MANSKE AO, ET AL:Duration of the phases of mechanical systole ininfants and children. Amer J Cardiol 14: 449,1964
9. GALSTIAN AA: Determination of tempoxal cor-relations of systolic phases in children. Pedia-triia 40: 49, 1962 (Russian)
10. FoRATTINI. C, SELMI W, GIACOMELLI F, ET AL:Le varie fasi della rivoluzione cardiaca studiatecon il metodo poligrafico in bambini dell'etascolare. Boll Soc Trivenata Med Int 3: 37,1955
11. ORE:sHKov V: Indirect measurement of isovolu-metric contraction time on the basis ofpolygraphic tracings. Cardiologia 47: 315, 1965
12. SPODICK DH, KUMAR S: Left ventricular ejectionperiod. Amer Heart J 76: 70, 1968
13. RAAB W, DEPAULA E SILVA P, STARCHESKA YK:Adrenergic and cholinergic influences on thedynamic cycle of the normal human heart.Cardiologia 33: 350, 1958
14. SLODKI SJ, HUSSIAN AT, LUISADA AA: The Q-II
interval: III. A study of the second heart soundin old age. J Amer Geriat Soc 17: 673, 1969
15. WILLEMs JL, ROELANDT J, DE GEEST H, ET AL:
The left ventricular ejection time in elderlysubjects. Circulation 42: 37, 1970
16. SUrrON R, HooD W, CRAIGE E: Correlation ofpre-ejection period with left ventricular ejec-tion fraction. (Abstr) Clin Res 38: 23, 1970
17. KRAETZ F, KRoscus M, MOZENA D, ElT AL:
Correlation of left ventricular pre-ejectionperiod with left ventricular ejection fraction inpatients with heart disease. (Abstr) Proc CentSoc Clin Res 42: 70, 1969
18. TALLEY R, MEYER J, McNAY J: Effect of heartrate, left ventricular end-diastolic pressure, anddiastolic pressure, on the pre-ejection period asan index of myocardial contractile state.(Abstr) J Clin Invest 48: 82a, 1969
19. BRAUNWALD E, SARNOFF SJ, STAINSKY WN:-Determinants of duration and mean rate ofventricular ejection. Circulation Research 6:319, 1958
20. WALLACE AG, MITCELL JH, SKINNER SN, ETAL: Duration of the phases of left ventricularsystole. Circulation Research 12: 611, 1963
21. MARGOLIS C: The significance of ejectionperiod/tension period as a factor in theassessment of cardiac function and as apossible diagnostic tool for the uncovering ofsilent coronary heart disease. Dis Chest 46:706, 1964
22. FRANK MN, KINLAW WB: Indirect measurementof isovolumetric contraction time and tensionperiod in normal subjects. Amer J Cardiol 10:800, 1962
23. HARRISON TR, DIXON K, RUSSELL RP JR, ET AL:
The relation of age to the duration ofcontraction, ejection, and relaxation of thenormal human heart. Amer Heart J 67: 189,1964
24. WILLEMS J, KESTELOOT H: The left ventricularejection time: Its relation to heart rate,mechanical systole and some anthropometricdata. Acta Cardiol 22: 401, 1967
25. GILBERT D: Digital analysis of hemodynamicdata. National Institutes of Health, U. S.Public Health Service, November, 1968
Circulation, Volume XLII, December 1970
1036
by guest on April 27, 2018
http://circ.ahajournals.org/D
ownloaded from

DAVID GOLDE and LUIS BURSTINSystolic Phases of the Cardiac Cycle in Children
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1970 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.42.6.1029
1970;42:1029-1036Circulation.
http://circ.ahajournals.org/content/42/6/1029located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on April 27, 2018
http://circ.ahajournals.org/D
ownloaded from











![Ultrasound backscatter tensor imaging (BTI): analysis of ... · cardiac function such as cardiac output, derived from the measure of diastolic and systolic ventricular volume [16]](https://img.pdfslide.us/doc/110x75/60633fcb9adee63abc71437b/ultrasound-backscatter-tensor-imaging-bti-analysis-of-cardiac-function-such.jpg)